promoting regular exercise in organizational fitness programs: health-related differences in...
TRANSCRIPT

PERSONNEL PSYCHOJJJGY 1994,41
PROMOTING REGULAR EXERCISE IN ORGANIZATIONAL FITNESS PROGRAMS:
BUILDING BLOCKS HEALTH-RELATED DIFFERENCES IN MOTIVATIONAL
DAVID A. HARRISON Department of Management
University of Texas at Arlington
LAURIE Z. LISKA School of Management
University of Rxas at Dallas
Hypotheses are proposed about relations among “building block” com- ponents of the motivation to attain exercise goals in an organizational fitness program, as well as about health-related individual differences in those components. The hypotheses are tested in a longitudinal field study involving questionnaire, physiological, and behavioral data from 107 participants in such a program. In support of the componential hy- potheses, goal attainment was a positive function of goal commitment. Goal commitment was an additive function of goal attractiveness and goal-specific self-efficacy/perceived control. In support of the individ- ual difference hypotheses, physiological variables were associated with work- and health-related perceived bamers to goal attainment. Em- ployees with high health risks ranged from .5 to 1.2 SDs higher in per- ceived barriers than employees with low risks. Evidence suggests that for goal setting to succeed as a program intervention, managers must concentrate on reducing the perceived work- and health-related bar- riers to exercise participation and goal attainment, especially for em- ployees with high health risks.
In response to a dramatically rising burden of health care costs, orga- nizations have begun to sponsor their own health promotion programs. The number of such programs has increased exponentially over the past decade, both in the United States and internationally (Cox, 1984; Geb- hardt & Cnunp, 1990, Leatt, Hattin, West, & Shephard, 1988; Terborg,
Portions of this paper were presented at the August 1991 Academy of Management Meetings in Miami, Florida. This research was supported, in part, by a grant to the first author from the University of Texas System (UT 15-330). Special thanks to Margie Lazarine and John Weis for their administrative support, and to Maria Carrington, Kris Diede, Janis Joplin, and Mary McLaughlin for their assistance in data collection. We are also grateful to Patrick Wright, Jerry Wofford, and several anonymous colleagues for helpful comments on earlier versions of this paper.
Correspondence and requests for reprints should be addressed to David A. Harrison, Department of Management, College of Business Administration, UTA Box 19467, Ar- lington, TX 76019-0467.
COPYRIGHT 0 1994 PERSONNEL PSYCHOLOCY, INC.
47
48 PERSONNEL PSYCHOLOGY
1986). Participation in such programs can have many beneficial health outcomes for individual participants, such as lowered risk of cardiovas- cular disease, increased alertness, improved muscle tone, mitigation of the negative effects of stress, and elevated mood states (Falkenberg, 1987; Jick & Mitz, 1985; Lichtman & Poser, 1983). The programs can also have a number of beneficial outcomes to organizations that sponsor them, such as providing a competitive advantage in recruiting skilled em- ployees, generating a shared “worker-oriented” perception of the firm, improving employee attitudes, lowering turnover, and reducing discre- tionary absenteeism (Baun, Bernacki, & IIsai, 1986; Bernacki & Baun, 1984, Bowne, Russell, Morgan, Optenberg, & Clark, 1984; Dishman & Gettman, 1980; Falkenberg, 1987; Shephard, Corey, Renzland, & Cox, 1982; Bai, Baun, & Bernacki, 1987). However, the primary reason that organizations implement such programs is the strong connection between these organizational and individual outcomes: Organizational savings in health care costs clearly depend on individual improvements in health (Erfurt, Foote, & Heirich, 1992; Gebhardt & Crump, 1990; Ilgen, 1990).
Therefore, motivating individual employees to change health-related behaviors in a health promotion program (whether the program involves on-site exercise, regular health screening, health education, or changes in health-related behaviors outside work) is necessary for ensuring the program’s organizational-level success (Terborg, 1986). As several au- thors have recently pointed out, it is important to establish sound moti- vational principles on which to base a successful program (Gebhardt & Crump, 1990; Guthrie & Olian, 1990; Ilgen, 1990, Terborg, 1986). One purpose of this paper is to propose and test some of those principles.
Another purpose is to identify individual differences in the “build- ing blocks” or components of the motivation to participate in such pro- grams, and especially, to achieve health-related goals. Large increases in program participation for specific sets of individuals, such as those with health risks, can be more vital and cost-effective than moderate in- creases in participation for all employees (Erfurt et al., 1992). For exam- ple, high stress levels are associated with increased risk of cardiovascu- lar disease and other physiological problems (Glasgow & Terborg, 1988; Kahn, 1981; Kasl, 1984). Exercise can decrease the severity of physi- ological responses to stress-related situations (Falkenberg, 1987). Mo- tivating exercise and fitness-related behaviors for individuals with high health risks may be more important than motivating exercise behaviors for individuals without such risks (Davis, Jackson, Kronenfeld, & Blair, 1987). Therefore, it is critical to identify how the basic components of fitness motivation vary in strength across individuals, especially across levels and categories of health risk.

HARRISON AND LISKA 49
Motivational Building Blocks
There are many “levels” of workplace health promotion and orga- nizational fitness programs. Each level addresses increasingly broad classes of health-related behaviors, including dietary choices, hygienic habits, stress reduction, and exercise (O’Donnell, 1986). In this paper, we deal with one class: exercise behaviors. Therefore, we hereafter use the term “fitness program.” We also assume that the mechanisms under- lying work motivation are parallel to those underlying exercise motiva- tion at work. We discuss those mechanisms in the sections below, even- tually concentrating on a set of motivational “building blocks.” Rather than developing a fully specified theory of fitness motivation, we argue for the inclusion of a central set of components. We then examine how levels of those components are associated with health-related individ- ual differences. Although many constructs are viable as components in the fitness motivation process (e.g., health locus of control), we focus on those supported in existing theory and research on goal commitment in organizations.
Goal Setting and Goal Commitment
It is likely that difficult, specific goals would help to instigate or in- crease the motivation to exercise in an employee fitness program. Diffi- cult, specific exercise goals should be easy to assemble and assign. And, although continuing an exercise regimen requires multiple behaviors over months or years, those behaviors are not too complex or too novel to fall outside the purview of simple goal-setting techniques (’hbbs, 1986; Wood, Mento, & Locke, 1987). Evidence comes from successful goal- setting interventions in health and exercise-related contexts outside the workplace (e.g., Alexy, 1985; Garland, Weinberg, Bruya, & Jackson, 1988; Locke & Latham, 1990; Seidman, Sevelius, & Ewald, 1984).
It is clear from past research, however, that exercise goals in an em- ployee fitness program would not influence actual exercise levels without sufficient employee commitment to those goals (Hollenbeck & Klein, 1987; Locke & Latham, 1990). Therefore, in addition to assigning diffi- cult and specific goals, managers of organizational fitness programs must generate goal commitment. In most goal-setting theories, commitment and goal difficulty (level) interact in their effects on goal attainment. In the present study, however, goal level was held constant across partici- pants, yielding our first hypothesis:
Hypothesis I: Exercise goal commitment is a direct, positive antecedent of the attainment of exercise goals (in an organizational fitness program).
50 PERSONNEL PSYCHOLOGY
Different components of goal commitment, the fundamental “build- ing blocks” of goal-directed motivation, have been proposed in overlap- ping theories by Ajzen (1991), Hollenbeck and Klein (1987), and Locke, Latham, and Erez (1988). W o classes of these components include the attractiveness of goal attainment and task-specific self-eficaq/perceived control over goal attainment. We discuss each component in more detail below.
Attractiveness: Instrunentalities and Wlences
Hollenbeck and Klein (1987) have proposed that attractiveness and expectancy of goal attainment are interactive components of commit- ment to attain work goals. Expectancy is quite similar to task specific self-efficacy and is discussed in a section below. Attractiveness is quite similar to the overall valence of a goal, the positive or negative evaluation of goal attainment. A model of valence/attractiveness was developed by Vroom (1964) in the original version of VIE theory. Vroom explains that the attractiveness of reaching a particular level of task performance is a summed set of cross-products of two parallel factors: instrumentali- ties (Ii), strengths of perceptions that positive or negative outcomes will be received once the performance level is attained; and, specific valences (K), the anticipated affect or perceived utility of those outcomes. Sim- ilar to a subjective expected utility, the Ii x V , couplets sum over all perceived outcomes to generate the overall attractiveness of attaining a goal.
With regard to exercise goals for instance, an employee might per- ceive that attaining a particular goal in a fitness program could “give me more energy and stamina.” The strength of that perception is an instru- mentality; the subjective evaluation of that gain in energy and stamina is a corresponding valence. Some of these ideas have already been applied in exercise and fitness contexts. For example, the subjective expected utility or attractiveness of participating in a fitness program has been shown to be related to actual participation levels (Godin & Shephard, 1986; Marcus & Owen, 1992; Steinhardt & Young, 1992; Zavela, Davis, Cottrell, & Smith, 1988). This leads to the ensuing hypothesis:
Hypothesis 2u: Commitment to an exercise goal (in an organizational fit- ness program) is a positive function of the attractiveness of goal attain- ment, which itself is a sum of products of instrumentalities and valences associated with perceived consequences of goal attainment.
HARRISON AND LISKA 51
Task Specific SewEficacy or Perceived Control: Sum of Perceived Barnsen
Although attractiveness and its instrumentality-valence building blocks are important, they do not span the entire range of factors that affect goal commitment. Social cognitive theory (Bandura, 1986) rec- ognizes the distinct impact of perceived behavioral constraints on goal- directed motivation, using the notion of self-efficacy. Dsk specific self- efficacy can be construed as a perceived connection between attempting to and successfully completing a task, or as perceived (behavioral) con- trol over getting a task accomplished once it is initiated (Ajzen, 1987; Bandura, 1982). As such, it is similar to Vroom’s (1964) expectancy link between effort and performance, and Naylor, Pritchard, and Ilgen’s (1980) act-to-product contingency.
As with attractiveness, task-specific self-efficacy or perceived behav- ioral control can be broken down into constituent components. Ajzen (1987; Ajzen & Madden, 1986) terms these components control beliefs: perceptions that one can control or overcome obstacles toward reach- ing a goal. In one of Ajzen’s formulations (Ajzen & Madden, 1986), task-specific self-efficacy or perceived control over goal attainment is a sum of k = 1,. . . K salient control beliefs. In the health and fitness literature, researchers focus on the converse of these components, per- ceived barriers (PBk) to goal attainment. The perceived barrier construct is one of the four dimensions defined in the health belief model (Jam & Becker, 1984). Indeed, it is the dimension that consistently accounted for the most variance in preventive health and sick role behavior (Jam & Becker, 1984) and it was the only dimension significantly related to exercise compliance in a study by Tirrell and Hart (1980).
To illustrate, some perceived barriers to attaining exercise goals could reflect a perceived lack of physical ability: “I’m too out of shape to exer- cise”; others could reflect a perceived lack of resources: “My work sched- ule just doesn’t allow it.” These perceptions can flow from long-standing attributional styles, from unsuccessful past experiences, or from envi- ronmental events (e.g., the onset of an illness) that trigger self-efficacy or control-related cognitions. Ironically and importantly, employees who could benefit most by actively exercising in an organizational fit- ness program might perceive the strongest barriers to exercise goals, because they feel too obese, exhausted, or chronically ill. Dsk-specific self-efficacy and/or perceived control (and the barrier-related cognitions they comprise) have already been shown to contribute to the motivation to attain many types of health- and fitness-related goals (Chambliss & Murray, 1979; Condiotte & Lichtenstein, 1981; Kanfer & Phillips, 1970; Kaplan, Atkins, & Reinsch, 1984; Mahoney, Moura, & Wade, 1973; Mar- cus & Owen, 1992; McAuley & Courneya, 1992; Melnyk, 1988; Pong

52 PERSONNEL PSYCHOLOGY
& McAuley, 1992; Schifter & Ajzen, 1985). Also, Strecher, DeVel- lis, Becker, and Rosenstock (1986) review much correlational and ex- perimental evidence for the relationship between self-efficacy and such hedth-related behaviors. Their results suggested that self-efficacy was strongly related to both short- and long-term health behavior modifi- cation and health maintenance. Based on this research, we submit the following hypothesis:
Hypothesis 2b: Commitment to an exercise goal (in an organizational fit- ness program) is a positive function of the perceived control/task-specific self-efficacy regarding goal attainment, which itself is the converse of a sum of perceived barriers to goal attainment.
Health-Related Individual Differences
If the factors described above are fundamental building blocks of the motivation to attain fitness goals, they probably contribute to that mo- tivation in different ways for different individuals. That is, it is likely that some groups or individuals will see certain instrumentalities as es- pecially large and consequential, or will be especially cognizant of spe- cific barriers to their goal attainment. Other groups and individuals will not. These differences may be systematic. We outline propositions about them below.
Health-related differences are particularly critical in a fitness pro- gram context because employees who have some form of health-related risk are the most important and cost-effective candidates to bring into the program. A fundamental purpose of any employee exercise pro- gram is to reduce the health risk of the high risk employees (Terborg, 1986). Health-related factors not only help determine who is at risk but may also provide a guide for determining who is or is not motivated to exercise.
Several kinds of perceived barriers have been related to various health-related variables, in reciprocal causation (Ajzen, 1987; Bandura, 1986; Kobasa, Maddi, & Khan 1982; O’Leary, 1985). This reciprocity of influence can lead to a downward spiral of high perceived barriers to per- forming healthy behaviors (such as exercise), fewer healthy behaviors, poorer health outcomes, external or low-control attributions about the ability to perform healthy behaviors in the future, then higher perceived barriers, and so on. Researchers have observed that those employees who need to participate in fitness programs most, do it least (Gebhardt & Crump, 1990; O’Leary, 1985; Settergen, Wilbur, Hartwell, & Rass- weiller, 1983; Zavela et al. 1988). From this evidence, we propose:
HARRISON AND LISKA 53
Hypothesis 3a: Past health-related factors, such as smoking, somatic prob- lems, frequent sick leave, high cholesterol levels, high resting heart rates, high blood pressure rates, and/or a great percentage of body fat are posi- tively related to perceived health-related bamers to attaining fitness goals.
Research in social psychology, particularly attribution research, can explain some of the variance in these perceived barriers. According to the revised learned helplessness theory (Peterson & Seligman, 1984; Seligman, 1986), attributions have potent effects on a number of impor- tant types of consequences, including general health states, achievement, and performance. When making attributions for negative outcomes, such as poor health states, individuals may shift responsibility from an internal, “central,” source to an external, “peripheral,” source (Snyder & Higgins, 1988). This systematic shift can eventually form an attribu- tional style in which a wide variety of negative outcomes are described as having situational and/or unstable causes. In other words, people may focus on a broad scope of information in a self-protective manner (6. Bylor & Brown, 1988). Thus, people who consistently make external attributions or see perceived bamers in the health and exercise context, might have the same attributions and perceptions in work- and family- related contexts, in a kind of perceptual or judgmental spillover.
This reasoning is consistent with the development of the health locus of control construct (Lau, 1982). A person’s health locus of control is considered a relatively stable individual difference. It is a more specific form of the general construct, locus of control, and is positively related to other components of it. That is, those who have an external locus for health also tend to have such beliefs in other, non-health-related areas (Rotter, 1975).
Likewise, the reverse causal ordering may be operating. People with more work- and family-related barriers to exercise might develop a high health risk. For example, constraints on the time available to exercise may be greater for those whose work demands longer hours or those who have more family responsibilities (Blegen, Mueller, & Price, 1988), leading to lowered health states. Accordingly, the following hypothesis is proposed:
Hjpothesis 36: Individual differences in health-related factors will be pos- itively related to other (not health-related) types of perceived bamers to attaining fitness goals.
That is, we predict that people who take more sick leave, overeat more often, smoke more often, experience more somatic problems, and so on, will also be likely to perceive lower controVefficacy over other kinds of

54 PERSONNEL PSYCHOLOGY
barriers to attaining fitness goals, such as family problems, workload, and scheduling conflicts.
Summaly
A variety of motivational factors might affect an individual’s attain- ment of exercise goals in an employee fitness program. The immedi- ate determinant of goal attainment is goal commitment. We examine two sets of proposed motivational components or “building blocks” of such goal commitment. These building blocks are (a) instrumentalities and valences that make up the attractiveness of goal attainment, and (b) perceived barriers that make up perceived control or task-specific self-efficacy regarding goal attainment. In this study, we are also con- cerned with health-related individual differences in these motivational components. If such differences are shown, this study could provide the rudiments for an approach to managing participation of high-risk versus low-risk employees.
Method
Overview
We employed the ideas discussed above in a field study of 107 full- time employees taking part in a fully developed employee fitness pro- gram. During individual interviews we asked these participants to con- sider a specific goal: 30 or more minutes of vigorous mrcise, an aver- age of three or more times per week for 8-12 weeks (depending on what point in the semester the participant was interviewed). Not only was the goal specific, it was difficult for most subjects-the mean level of indi- vidual participation before the interviews was about 1.7 exercise sessions per week. During the interviews, we measured several individual differ- ences, as well as instrumentalities and valences of outcomes of attaining the assigned goal, and perceived bamers to successful goal attainment. As our hypotheses dictated, we then related the individual differences to the motivational components, and the motivational components to subsequent exercise behavior in the fitness program.
Background and Features of the Employee Fitness Program
The setting for this investigation was a large, urban university in the southwestern United States. An organization-wide fitness program had been in place for two semesters before our study began. Requirements for initial enrollmenit in the program were full-time employment at the
HARRISON AND LISKA 55
university, a semi-annual physical, and a $5 blood test. Organized ac- tivities included low-impact and water aerobics, swimming, walking, jog- ging, tennis, racquetball, basketball, volleyball, and softball. The uni- versity granted all program members 90 minutes of paid release time each week to participate in the fitness program, provided that members matched the release time spent exercising with an identical amount of non-work time. Participants were repeatedly encouraged by the pro- gram staff, in oral and written messages throughout each semester, to try to attain a goal of exercising vigorously an average of three or more times per week, at least 30 minutes each time. Supplementary seminars were also offered at various times on health and wellness topics such as preventive health care, low-calorie diet, stress reduction, and smoking cessation.
When our study began, there were 341 participants in the fitness program, 19% of all full-time employees. This is slightly higher than rates reported for white-collar employees in other studies (Gebhardt & Crump, 1990). The program was administered jointly by the univer- sity’s personnel department, by the fitness program director (who had additional responsibilities as an instructor of recreational sports), and by part-time staff. Organized activities were offered on weekdays: in the early morning, during the noon hour, and in the late afternoon. Profes- sional instructors led aerobics classes, which also required a small fee ($lohemester). Other activities did not require a fee and were less for- mally organized.
Participants signed on-site log books for activities taking place on or starting at the university’s exercise facilities. Exercise activities per- formed off-site were recorded by participants on special forms and re- turned each month to the program coordinator. The coordinator devel- oped monthly archival reports of individual exercise levels from the log books and these forms.
Elicitation Study
To ensure that the motivational building blocks used in our study were grounded in the population at hand, we conducted an elicitation study. We sent a one-page survey to all fitness program members 2 months prior to the beginning of the main study. Elicitation questions were open-ended and asked participants to (a) list all positive, negative, or neutral outcomes of vigorously exercising 30 minutes or more, an av- erage of three or more times per week in the fitness program, for the up- coming semester; and (b) list other things the respondent associated with the goal, including factors that might keep them from reaching it. The first question elicited relevant outcomes; the second, perceived barriers.
56 PERSONNEL PSYCHOLOGY
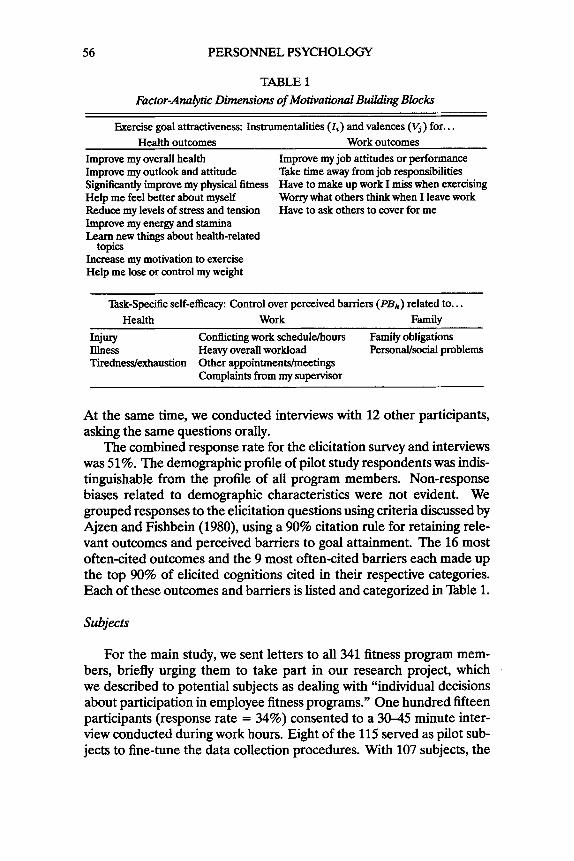
TABLE 1 Factor-Analytic Dimensions of Motivational Building Blocks
Exercise goal attractiveness: Instrumentalities ( I i ) and valences (Vj ) for.. . Health outcomes Work outcomes
Improve my overall health Improve my job attitudes or performance Improve my outlook and attitude T&e time away from job responsibilities Significantly improve my physical fitness Have to make up work I miss when exercising Help me feel better about myself Worry what others think when I leave work Reduce my levels of stress and tension Have to ask others to cover for me Improve my energy and stamina Learn new things about health-related
Increase my motivation to exercise Help me lose or control my weight
topics
’hk-Specific self-efficacy: Control over perceived barriers (P&) related to.. . Health Work Family
Injury Conflicting work schedulehours Family obligations Illness Heavy overall workload Personal/social problems Tuednedexhaustion Other appointmenWmeetings
Complaints from my supervisor
At the same time, we conducted interviews with 12 other participants, asking the same questions orally.
The combined response rate for the elicitation survey and interviews was 51%. The demographic profile of pilot study respondents was indis- tinguishable from the profile of all program members. Non-response biases related to demographic characteristics were not evident. We grouped responses to the elicitation questions using criteria discussed by Ajzen and Fishbein (1980), using a 90% citation rule for retaining rele- vant outcomes and perceived barriers to goal attainment. The 16 most often-cited outcomes and the 9 most often-cited barriers each made up the top 90% of elicited cognitions cited in their respective categories. Each of these outcomes and barriers is listed and categorized in Bble 1.
Subjects
For the main study, we sent letters to all 341 fitness program mem- bers, briefly urging them to take part in our research project, which we described to potential subjects as dealing with “individual decisions about participation in employee fitness programs.” One hundred fifteen participants (response rate = 34%) consented to a 30-45 minute inter- view conducted during work hours. Eight of the 115 served as pilot sub- jects to fine-tune the data collection procedures. With 107 subjects, the
HARRISON AND LISKA 57
power of observing a large (r = 5 0 ) effect size = .99, a medium (r = .30) effect size = .92, and smali (r = .lo) effect size = .26 (Cohen, 1977).
Twenty (19%) of the final 107 subjects were male. Most subjects were married (64%). The median number of children living at each partici- pant’s home was 1.0 (Z = .89; max. = 4). The mean age in the sam- ple was 41.4 years (SD = 9.6; min. = 24, max. = 62). The mean num- ber of years of education was 15.8 (SD = 2.8). The program appealed mainly to employees in clerical and para-professional jobs as indicated by the percentage of those employees in our sample (75%). Some sub- jects held managerial or administrative positions (13%)’ and others were faculty members (12%). Thirty-six percent of the participants did aero- bic walking as their chief fitness activity and 31% took part in organized aerobics classes. Once again, the demographic profile of the sample in the main study closely matched the demographic profile of all members; non-response bias was not detected for these and other demographic and organizational variables.
Data-Collection Procedure
On-site interviews were conducted during the 4th-8th weeks of the fall, 1990 semester (allowing 8-12 weeks of possible fitness program par- ticipation after the interview). The first part of each interview was oral, containing questions about how the participant evaluated the adminis- tration and features of the fitness program. These questions were de- signed to maximize the face validity of the interview session, and to ease subjects into later forced choice questions.
In the second part of the interview, motivational constructs were measured using interactive questionnaire items presented by a laptop computer. Those items were followed by self-reports of health vari- ables. No computer knowledge was needed to complete the question- naire. The computer afforded us the opportunity to quickly tailor ques- tionnaire items to individual respondents via “branching” of questions. It also eliminated much of the error introduced by manual data coding and data entry procedures, and helped to assure the respondents of their confidentiality. IIb further assure confidentiality, the interviewer could not see the subject’s answers as he or she answered the computer survey. However, the interviewer was available to answer questions and make requested clarifications about the computer-presented items. Question- naire responses were eventually linked with exercise and physiological data using a unique, scrambled code provided by each respondent.
58 PERSONNEL PSYCHOLOGY
Measures
The computer provided sample items and instructions on how to re- spond to the various item formats in the questionnaire. Because of time constraints and the breadth of constructs covered, most constructs were measured with only one or two items. Most of the constructs were mea- sured with reference to attaining the exercise goal: “vigorously exercis- ing at least 30 minutes, for an average of 3 or more times per week, dur- ing the rest of this semester.”
Goal attainment was measured using the archival exercise records discussed above (in the Background and Features.. . section). Goal com- mitment was measured in a straightforward way by averaging responses to the statement: “I am strongly committed to.. . ” (the goal stated above). Responses were measured on two 7-point semantic differential scales. One ranged from “extremely unlikely” (-3) to “extremely likely” (+3); the other ranged from “extremely strong commitment” (+3) to “extremely weak commitment” (-3). Estimated reliability of this 2-item scale was CY = -87.
Instrumentalities of goal attainment (Ii) were measured by present- ing the exercise goal at the top of the computer screen, and asking partic- ipants to answer on semantic differential scales how likely each of the 16 elicited outcomes would be if the participant attained the exercise goal him- or herself. Following Vroom (1964), the scales were anchored by - 1 = “extremely unlikely” and + 1 = “extremely likely.” Valences (K) were also measured on semantic differential scales, asking participants how good or bad each of the 16 outcomes would be for them personally. Responses ranged from “extremely bad” (- 1) to “extremely good” ( + 1). For example, one instrumentality item read, “How likely is it that vigor- ously exercising at least 30 minutes. . . will improve your overall health?” The parallel valence item read, “Improving my overall health would be
Perceived barriers were measured by asking questions such as, “How likely is it that an injury will keep you from attaining the goal?” Similar to Ajzen and Madden (1986), the response format for these questions was a 7-point semantic differential scale, ranging from “extremely unlikely” (-3) to “extremely likely” (+3). Note that for these questions, respond- ing “likely” reflected a higher perceived obstacle to, and presumably, a lower motivation to attain the exercise goal.
Health-related individual differences were measured using self- reports obtained in the interview and physiological records obtained in a health screening session at the beginning of the semester. The self- reports included somatic complaints, amount of smoking, number of sickness absences taken in the previous 12 months, height, and weight.
7,

HARRISON AND LISKA 59
A 10-item index of somatic complaints, patterned after Caplan, Cobb, French, Van Harrison, and Pinneau (1980), had an estimated reliabil- ity of a = .82. The index contained frequencies of such health symp- toms as backaches, headaches, sleeping trouble, and labored breathing. Subjects also estimated the number (of packs) of cigarettes they smoked each week; responses were converted to a smoking rate of cigarettes per day. Self-reported height and weight estimates correlated well (both TS
= .96, p < .01) with corresponding archival records available for 70 of the subjects. An obesity index was computed from the height and weight data using a formula validated by Florey (1970).
Physiological data from the participants’ health screenings were used to reduce potential mono-measurement bias in tests of Hypotheses 3a and 3b, and to provide possible evidence of a link between physiological and motivational constructs. Blood chemistry measures included levels of high-density lipoproteins (HDL), low-density lipoproteins (LDL), and triglycerides. HDL is often referred to as “good” cholesterol and LDL as “bad” cholesterol. To gauge their relative levels, we created a cholesterol ratio: LDWDL. Each of the blood components has well-established connections to the risks of cardiovascular disease-risks that can be re- duced by regular exercise (American Heart Association, 1991). Other physiological measures included percentage of body fat (using a caliper procedure), diastolic and systolic blood pressure, and resting heart rate. The test-retest stabilities for these last four measures ranged from T = .68 to T = .94.
Results
Motivational Building Blocks
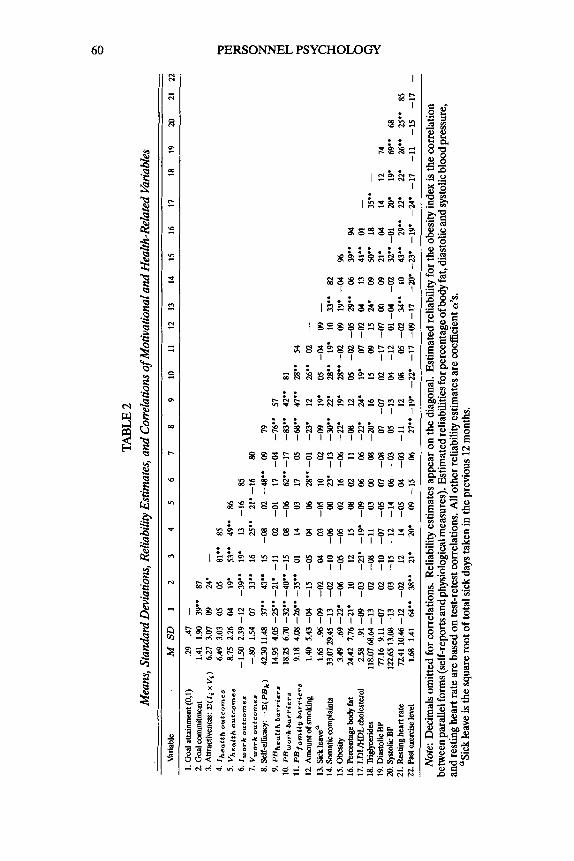
To reduce the number of motivational building blocks to a smaller set of content-based dimensions, we conducted several exploratory factor analyses with oblique rotations. In a preparatory analysis that included all the instrumentality (I i ) , valence (V,), and perceived barrier (PBk) items, two dominant factors were easily and clearly distinguished: attrac- tiveness (composed of the Ii and V, items) and self-efficacy/perceived control (composed of the PBk items). Separate factor analyses were then performed on each of these broad dimensions. Parallel analysis (Humphreys & Montanelli, 1975), scree plot, and interpretability crite- ria converged in identieing two factors for Ii and V , items: health and work outcomes. Three factors were identified in the PBk items: health-, work-, and family-related barriers. See Table 1 for the specific items in each factor. Table 2 shows means, standard deviations, and intercorre- lations of a11 of the motivational and health-related variables, along with
TABL
E 2
Mea
ns, S
tand
ard D
evia
tions
, Rel
iabi
lity E
stim
ates
, and
Cor
rela
tions
of M
otiv
atio
nal a
nd H
ealth
-Rel
ated
Var
iabl
es
Var
iabl
e M
SD
1
2 3
4 5
6 7
8 9
10
11
12
13
14
15
16
17
18
19
20
2
12
2
1. G
oal a
ttain
men
t (0.
1)
29
.47 -
2. G
oal w
mm
ibne
nt
1.41
1.90
39
.. 87
3.
Attr
activ
enes
s: C
(lix
v,)
6.2
7 3.0
7 09
24
' -
4. Ih
ea[t
ho
utc
om
er
6.49
3.03
05
05
81.'
85
5. V
heo
[th
outc
omes
8.7
5 2.
26
04
19'
53..
49"
86
6. I
wo
rk
ou
tco
mes
-150
2.3
9 -1
2 -39
'. 19
. 13
-1
6 85
7. vw
ork
ou
tcom
e.
-.80
1.54
M
33.'
16
25''
21'
-16
80
8.Se
lf-ef
fiCaq
: -C
(PB
k)
42.3
011.
48
37"
43.'
15
-08
02 -48"
09
79
9. P
Bh
eolt
hb
arr
iers
14
.95
4.05
-25
'. -2
1' -1
1 02
-01
17
-04
-76.'
57
10. P
Bw
o,k
bo
rr;e
ra
18.2
5 6.
70 -3
2"
-40"
-15
08
-06
62..
-17
-83'.
42
'. 81
12. A
mou
nt of
Sm
oLing
1.
40
5.43
-04
-15
-05
04
06
28'. -0
1 -2
3.
12
26'. 02
-
13. S
ick
leav
eo
1.65
.%
-09
-02
04
03
-05
10
02
-09
19.
05
-04
09 -
14. S
omat
ic am
plai
nts
33.0
729.
45 -
13
-02
-10
-06
00
23.
-13
-30"
22.
28.' 19
' 10
33
" 82
15
. Obe
sity
3.4
9 .6
9 -2
2. -0
6 -0
5 -0
5 02
16
-0
6 -2
2. 19
' 28..
-02
09
19'
-04
%
11.
PB
~~
,~
~~
~~
~~
~~
~~
9.
18
4.08
-26.
. -35
.. 01
14
o3
17
05
-68..
47.0
28.. 54
16.F
'em
ntag
ebod
yfat
24
.42
7.76
-21.
10
12
15
08
02
11
-0
8 12
05
-02
-05
29.. 06
39
.' 94
17
.LD
UH
DLc
hole
ster
ol
2.58
.9
1 -0
9 -0
3 -2
3' -1
9' -0
9 06
M
-22.
24'
19'
07
-02
04
13
41..
01
-
18. T
iigfy
cerid
es
118.
0768
.64
-13
02
-08
-11
03
00
08
-20'
16
15
09
I5
24'
09
50..
18
35'.
-
19. D
iasto
lic B
P n.16 9
.11
-07
02
-10
-07
-05
07
-08
07
-07
02
-17
-07
00
09
21.
04
14
12
74
20. S
ysto
lic BP
122.
65 1
3.08
-13
03
-1
5 -1
2 -1
4 06
-o3
05
-13
04
-12
01 -0
4 -02
32"
-01
20' 19
. 69"
68
21. Resting h
eart
rate
72
.41
10.4
6 -1
2 -0
2 12
14
-0
5 04
-0
3 -1
1 12
08
05
-0
2 34"
10
43"
29"
22'
22.
26.. 25
'' Bf,
22. P
ast e
xerc
ise le
vel
1.68
1.
41
64.' 38
.. 21
. 20
' 09
-1
5 06
27
" -1
9. -2
2'
-17
-09
-17
-20'
-23.
-19.
-24.
-17
-11
-15
-17
-
Not
e: D
ecim
als o
mitt
ed fo
r cor
rela
tions
. Rel
iabi
lity e
stim
ates
appe
ar o
n th
e di
agon
al. E
stim
ated
relia
bilit
y for
the
obes
ity in
dex
is th
e co
rrel
atio
n be
twee
n pa
ralle
l for
ms (
self-
repo
rts an
d ph
ysio
logi
cal m
easu
res)
. Est
imat
ed re
liabi
litie
s for
perc
enta
ge of
bod
y fat
, dia
stol
ic an
d sy
stolic
bloo
d pr
essu
re,
and
rest
ing h
eart
rate
are
bas
ed o
n te
st-r
etes
t cor
rela
tions
. All
othe
r rel
iabi
lity e
stim
ates
are
coef
ficie
nt a
's.
?Sic
k le
ave
is th
e sq
uare
root
of t
otal
sick
day
s tak
en in
the
prev
ious
12 m
onth
s.
HARRISON A N D LISKA 61
estimated reliabilities. The somewhat low reliabilities for PBhealth and PBfamily will tend to yield underestimates of the relations between these factors and other variables.
Goal Commitment-Goal Attainment Relation
IIfiventy-nine percent of the participants attained the exercise goal. The theories of Locke et A. (1988) and Hollenbeck and Klein (1987) both propose interactive effects of goal commitment with goal difficulty (or level) on performance. When only a single goal level is set (i.e., goal difficulty is a constant), goal commitment will have a main effect, as stated in Hypothesis 1. Supporting that hypothesis, the correlation of goal attainment (scored “1” if the employee exercised an average of 2 3 timesiweek after the interview and “0” if < 3 timesiweek) with goal commitment was significant (T = .39, p < .01). When the continuous variable, average amount of exercise per week (performance), was sub- stituted for the dichotomous variable, goal attainment, the correlation increased to T = .45 (p < .01).
It was also possible to test for the unique contribution of goal com- mitment to future exercise performance, by including it in a regression equation containing a measure of past performance. Using archival data, we computed the average amount of exercise per week (performance) each individual had before the interviews were conducted. Using fu- ture performance as the dependent variable, we conducted a hierarchical multiple regression analysis, entering goal commitment after past exer- cise. The incremental contribution of goal commitment was significant, despite a substantial carryover of exercise rates over time ( initial AR2 for past exercise = .65, p < .01; incremental AR2 for goal commitment = .07, p < .01; correlations of past exercise with other variables in the study are given in Bble 2).
Other Correlates of Goal Attainment
Although we did not have explicit hypotheses about variables other than commitment that might have zero-order correlations with goal at- tainment, it may be of interest to examine some of those correlations in nble 2. For instance, as we noted above, there is considerable stability in exercise rates over the 16 weeks of the study. Past (pre-interview) ex- ercise levels correlated strongly with future (post-interview) goal attain- ment: T = .64 (p < .05), and both performance indices shared the same covanates. Self-efficacy and each of its perceived barrier components also had significant correlations with goal attainment, underscoring the importance of these variables in the motivational process (all ps < .05).

62 PERSONNEL PSYCHOLOGY
Finally, both obesity and percentage of body fat, which are substantially intercorrelated, had significant relations with goal attainment (T = .22, .21, respectively; p < -05 for both).
Components of Goal Commitment
In keeping with Hypotheses 2a and 2b, indices of goal attractiveness and task-specific self-efficacy/perceived control were created by sum- ming their elements (C[& x K], and -C[PBk], respectively). As Tmble 2 shows, zero-order correlations of these proposed components of goal commitment with commitment itself were all significant. Goal attrac- tiveness and perceived controytask-specific self-efficacy were also fairly independent (T = .15, p > .lo), suggesting that whether or not the goal seemed attractive had little bearing on one’s judgments about barriers to achieving it. We used hierarchical multiple regression analyses to see if each of these components explained unique variance in goal commit- ment. Supporting Hypotheses 2a and 2b, both attractiveness and task- specific self-efficacy had significant weights in a full regression equation (standardized weights were .23 and .40, respectively; p < .01). Goal at- tractiveness explained a unique 8% of the variance in goal commitment; perceived controytask-specific self-efficacy explained a unique 15%. To test the interactive contribution of these components proposed by Hol- lenbeck and Klein (1987), we performed another moderated multiple re- gression analysis. In this case, however, the contribution of a C[& x K] x - C[PBk] multiplicative term did not improve the prediction of goal com- mitment (AR2 = .007, p > .lo).
Additionally, the factor-analytic dimensions within attractiveness and task-specific self-efficacy were correlated with goal commitment, as shown in Table 2. Both instrumentalities and valences of the “hassle” type work outcomes had significant relations with goal commitment (T
= -.39, .33, respectively; ps < .Ol), suggesting that organizational inter- ventions related to such outcomes might be effective. Valence, but not instrumentality of the health-related outcomes, was also related to goal commitment (T = .19, p < .05). All three of the perceived barrier factors had significant correlations with goal commitment (health-related bar- riers: T = -.21, p < .01; work-related barriers: T = -.40, p < .01; and family-related barriers: T = -.35, p < .Ol). The correlation involving work-related barriers suggests that at least some portion of self-efficacy regarding attaining exercise goals might be enhanced by an organiza- tional intervention. This takes on added importance if one notes that work-related instrumentalities and perceived barriers were strongly con- nected (. = .62). Recalling that most of the elicited work outcomes were
HARRISON AND LISKA 63
negative (e.g., “have to ask others to cover for me”), the results imply that such outcomes are also seen as barriers to goal attainment.
Health-Related Individual Differences
As indicated in Table 2, Hypotheses 3a and 3b were strongly sup- ported by the health data. Employees who complained more about aches and pains, took more sick leave, were more obese, or smoked, all per- ceived less controVefficacy than their healthier counterparts over health- and work-related barriers to attaining the exercise goal. The canonical correlation between the three perceived barrier factors and these four health variables was R = .48 (p < .01).
Relations between cardiovascular health data and perceived barriers are also displayed in Table 2. Only the LDUHDL cholesterol ratio was sigmficantly correlated with any of the perceived barrier factors. Em- ployees with higher cholesterol ratios perceived both stronger health- related (T = .24, p < .05) and work-related barriers (T = .19, p < .05) to attaining the exercise goal. Although the self-reported or physiologi- cal health variables were generally positively related to one another, the cholesterol ratio and especially the obesity measure stand out as hav- ing significant correlations with nearly every other health state (except smoking). This supports the construct validity of the self-reported obe- sity (based on height and weight estimates) index and argues for its use in future studies.
Discussion
Implications of Motivatioml Principles
A principle contribution of this study is the demonstration that mo- tivational principles applied in work performance contexts can also be applied in the context of organizational fitness programs. For example, some of the strongest components of exercise goal commitment were in- strumentalities and valences associated with work-related outcomes of attaining an exercise goal. If these are truly causal determinants of goal commitment, the implications to fitness program managers are similar to those that flow from Vroom’s (1964) VIE theory. To motivate employ- ees to reach an exercise goal, a fitness program manager must (a) try to strengthen the instrumentality linking goal attainment to positively va- lenced outcomes (e.g., provide work-related rewards such as increased health insurance premium sharing), (b) weaken the instrumentalities that link goal attainment to negatively valenced outcomes (e.g., arrange schedules so that employees need not ask co-workers to “cover for them”

64 PERSONNEL PSYCHOLOGY
while they take part in organized exercise activities), (c) add positively valenced outcomes to the perceived set of outcomes (e.g., praise and social recognition for attaining the goal), and (d) remove negatively va- lenced outcomes from the perceived set (e.g., enforce a managerial sup- port policy that would eliminate work “piling up” while the employee uses release time to exercise). Erfurt et al. (1992) provide evidence for the cost-effectiveness of such an approach, especially one that provides a variety of health improvement strategies, and one-to-one outreach and follow-up counseling. Both of these factors stress the importance of ad- dressing individual differences in valued outcomes and perceived barri- ers, which are discussed below.
To increase contro4task-specific self-efficacy over barriers to attain- ing an exercise goal, it might be prudent for fitness program managers to treat the barriers as real rather than perceived. For example, employ- ees in our sample often thought their work requirements conflicted with attaining exercise goals, despite getting a weekly allocation of 90 min- utes of paid release time from the organization. In fact, of all motiva- tional constructs, workload- and work-related cognitions were the most consistently related to exercise goal commitment. Flexible work and ex- ercise schedules can reduce this (perceived) interference. Participant “choice” is significantly related to self-efficacy (Mathieu, Martineau, & lbnebaum, 1993), which further underscores the importance of a menu of available participation options. Some of those options might involve less vigorous exercise (such as very low-impact aerobics), which could help to remove injury- or fatigue-related perceived barriers (see Table 1). Baining programs might be helpful to aid supervisors in coordinating schedules and workloads of employees in and out of sponsored fitness programs. Allowing an employee’s spouse and family members to exer- cise at on-site fitness facilities might decrease some of the family-related barriers to participation. All of these interventions require commitment from managers at all levels, both in resources allocated and in their par- ticipation in the program (perhaps as social models).
A goal-setting intervention itself often increases perceived control/ efficacy over barriers to performing healthy behaviors. As long as goals are reasonable and employees experience a “success77 in their first few goal strivings, the motivational change brought about by this enactive w t e r y (Bandura, 1986) involves increasingly higher levels of perceived contro4self-efficacy, especially over work-related barriers (Locke & Latham, 1990). Through a gradually building program, the self-efficacy of a group of smokers who had high outcome expectations (i.e., per- ceived the benefits of smoking cessation) but initially low efficacy expec- tations was significantly improved (Strecher, Becker, Kirscht, Eraker, &
HARRISON AND LISKA 65
Graham-Tomasi, 1985). Chambliss and Murray (1979) noted that ma- nipulating the self-efficacy of subjects with internal locus of control be- liefs contributed to sustained weight loss. In the area of exercise be- havior, Ewart, Thylor, Reese, and Debusk (1984) found that, through professional counseling efforts, task-specific self-efficacy (e.g., aerobic activities such as treadmill usage and walking) could be generalized to broader exercise behaviors (e.g., to nonaerobic activities such as weight- lifting). Similar programs could be developed and used to initially get high-risk employees into fitness programs and keep them in the pro- gram for the long term. Success in getting “at risk” people into future programs should show almost immediate health care savings to the firm involved (Terborg, 1986), and might serve to break the unhealthy moti- vational cycle linking low perceived control to fewer exercise behaviors to lower perceived control and so on.
This focus on efficacy expectations and control perceptions views in- dividuals as active participants in the modification of their own unhealthy behaviors. This is a departure from traditional models of health be- havior change that focus on individuals as passive recipients of medical treatments (e.g., drug therapies). Through the step-by-step mastery of increasingly difficult health behaviors, the locus of control should shift from external to internal sources and the downward spiral of unhealthy behaviors should be reversed.
Implications of Health-Related Individual Differences
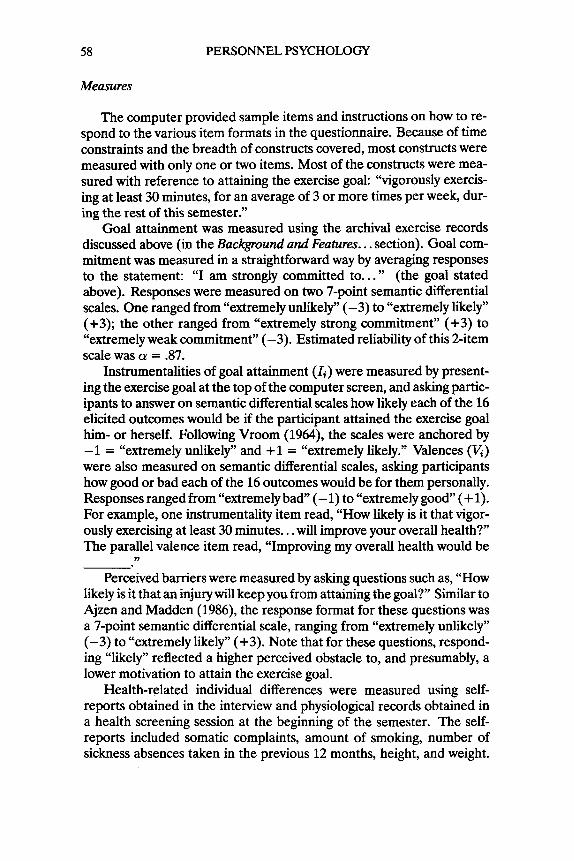
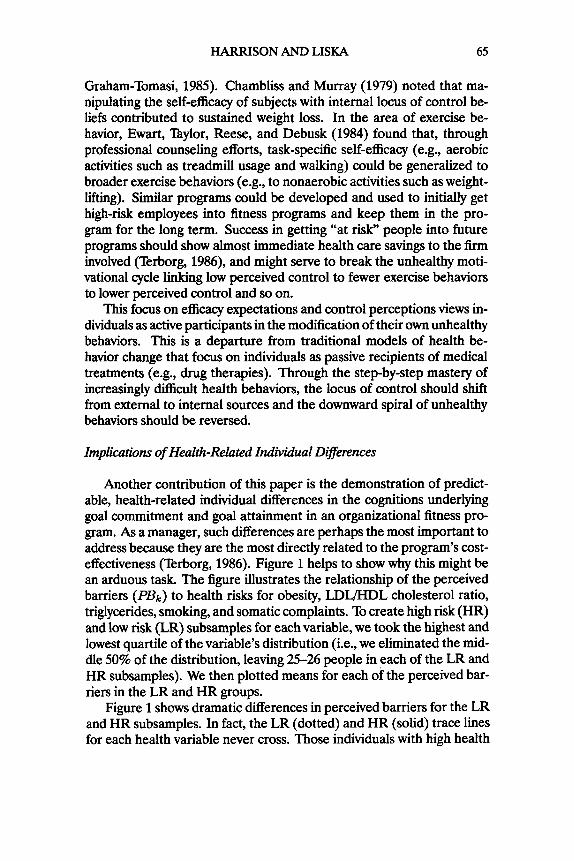
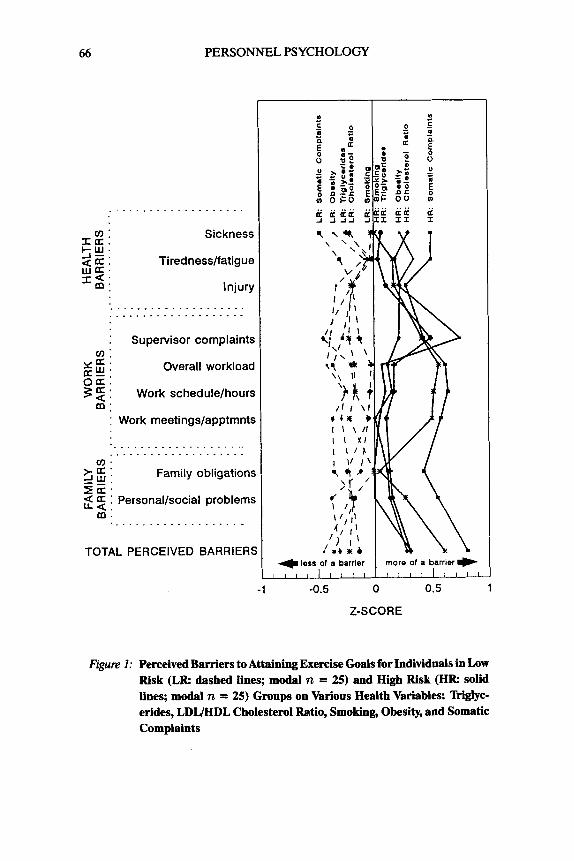
Another contribution of this paper is the demonstration of predict- able, health-related individual differences in the cognitions underlying goal commitment and goal attainment in an organizational fitness pro- gram. As a manager, such differences are perhaps the most important to address because they are the most directly related to the program’s cost- effectiveness (Terborg, 1986). Figure 1 helps to show why this might be an arduous task. The figure illustrates the relationship of the perceived barriers (PBk) to health risks for obesity, LDUHDL cholesterol ratio, triglycerides, smoking, and somatic complaints. To create high risk (HR) and low risk (LR) subsamples for each variable, we took the highest and lowest quartile of the variable’s distribution (i.e., we eliminated the mid- dle 50% of the distribution, leaving 25-26 people in each of the LR and HR subsamples). We then plotted means for each of the perceived bar- riers in the LR and HR groups.
Figure 1 shows dramatic differences in perceived barriers for the LR and HR subsamples. In fact, the LR (dotted) and HR (solid) trace lines for each health variable never cross. Those individuals with high health
66 PERSONNEL PSYCHOLOGY
....................
Sickness
Tirednesslfatigue
Injury . . . . . . . . . . . . . . . . . . ...................
: Supervisor complaint: a:
x a * Overall workloac a:: o a t 3 3 : Work schedulelhour:
m : : Work meetings/apptmnts
. . . . . . . . . . . . . . . . . . . . .................... v ) . SG: Family obligation:
Z-a. 4 a : Personal/social problem: L a .
m . . . . . . . . . . . . . . . . . . . . -
TOTAL PERCEIVED BARRIER! mora of a barrier .) &
-1 -0.5 0 0.5 1
Z-SCORE
Figure 1: Perceived Barriers to Attaining Exercise Goals for Individuals in Low Risk (LR dashed lines; modal n = 25) and High Risk (HR solid lines; modal n = 25) Groups on Various Health Variables: "iglyc- erides, LDIJHDL Cholesterol Ratio, Smoking, Obesity, and Somatic Complaints
HARRISON A N D LISKA 67
risks always perceived greater barriers to attaining the exercise goal, regardless of the type of barrier or the type of risk. Furthermore, the HR-LR differences in total perceived barriers are very large by behav- ioral science standards. For each health risk variable, the difference in total perceived barriers is at least .5 standard deviations. For obesity, smoking, and somatic complaints, the differences range from .8 to 1.2 standard deviations. In other words, employees with high health risks were from .5 to nearly 1.2 standard deviations higher in perceived barriem than employees with low health risks. Thus, a major first step in any approach to employee fitness motivation might be to change or remove these per- ceived obstacles. This suggestion is further supported by the significant zero-order correlations perceived barriers had with goal attainment (see ’Iiible 2).
Limitations and Research Directions
As with any single investigation, the results and conclusions pre- sented here need to be replicated before they are generally applicable. The ecological validity of these results is limited by the uniqueness of the sampled organization, the predominantly white-collar sample, and the small proportion of males. Replications over time and across organi- zational and demographic contexts would be especially useful. Indeed, our sample contains only 6% of the employees in the entire organiza- tion, which greatly limits generalizations to those program participants who were not in our study, and especially to those who never joined the program. There is a clear need to study those individuals in future re- search, as they are often the employees at highest health risk (Zavela et al., 1988).
Applied research is also needed to test the effectiveness of various change strategies on perceived barriers to fitness goals. For example, experimental or quasi-experimental field research might compare the ef- fectiveness of education-based interventions that only passively involve high-risk employees, to example-based interventions that involve care- fully chosen social models, key employees, or managers in work groups, to exercise-based interventions that enjoin active involvement. Longi- tudinal “laboratory” experiments involving random assignment of un- dergraduate students to such change conditions in their (typically man- dated) physical education courses are a useful but seldom used possibil- ity.
Within the attractiveness component, the cognitions that are easiest to manipulate are the instrumentalities, as valences tend to be more sta- ble and deep-rooted. This study reinforces that notion, in that there is less disagreement about how good it would be to attain positive health
68 PERSONNEL PSYCHOLOGY
outcomes (Z, h2 of VheQlth outcomes = 8.75,5.11, respectively) than there is about how reaching the exercise goal would help one to attain those outcomes (T, h2 of Iwork outcomes = 6.75,9.18, respectively; both I s and Vs are measured on the same -1 to + 1 summated scale). We have also noted that the best instrumentalities for change involve work-related outcomes, because they have the strongest connection to goal commit- ment. Of all the components of goal attractiveness, a unit change in IWmk outcomes would yield the largest change in goal commitment.
That prediction, however, is predicated on a causal connection be- tween the constructs. Our results are merely correlational. Stronger experimental tests (such as those we have suggested above) of these relations are necessary. Furthermore, the largest correlations we ob- served involved motivational constructs that were measured via self- report. Common method variance is a distinct concern, and can only be overcome with less obtrusive, but yet-to-be developed measures of commitment, attractiveness, and perceived control.
Longitudinal studies over longer time intervals are also needed. Though often stated, such a recommendation in the fitness program con- text is neither empty nor trite. For example, the results involving health states and perceived barriers beg an important question (although in this study many of the health variables were measured weeks before the per- ceptual constructs). Are the perceptions rationalizations (external at- tributions)? That is, are they the consequences of one’s own unhealthy behaviors in the past? Or, are the health states antecedents-the rea- sons that the unhealthy behaviors initially developed? Future studies must include multi-wave designs that help to map that time-dependent causal chain.
Other important time-based questions also come to mind. For in- stance, how is the initial motivation to sign-up similar to and different from the motivation to adhere to an exercise regimen? How are par- ticipation levels maintained? Finally, further identification of motiva- tional patterns for employees at risk of major health problems should be a paramount concern. If effective motivational principles can be used with these persons, virtually all parties involved would benefit: organi- zations, program managers, and individual employees.
REFERENCES
Ajzen I. (1987). Attitudes, traits, and actions: Dispositional prediction of behavior in personality and social psychology. In Berkowitz L (Ed.), Advances in qerimental sociulpvchology, Vol. 20 (pp. 1-63). Hillsdale, NJ: Erlbaum.
Ajzen I. (1991). The theory of planned behavior. Olganizational Behavior and Human Decision Processes, 50,179-21 1.
Ajzen I, Fishbein M. (1980). Understanding attitudes andpredicting social behavior. Engle- wood Cliffs, NJ Prentice-Hall.

HARRISON AND LISKA 69
Ajzen I, Madden TJ. (1986). Prediction of goal-directed behavior: Attitudes, intentions, and perceived behavioral control. J o m l of Experimental Social Psychology, 22, 453474.
Alw B. (1985). Goal-setting and health risk reduction. Numhg Research, 34,283-288. American Heart Association. (1991). Exercise and your heart. Dallas, Tx: Author. Bandura A. (1982). Self-efficacy mechanism in human agency. American ~sychok@St, 37,
122-147. Bandura A. (1986). Social foundations of thought and action: A social cognitive theory.
Englewood C W , N J Prentice-Hall. Baun WB, Bernacki El, Tsai SI? (1986). A preliminary investigation: Effect of a corpo-
rate fitness program on absenteeism and health care cost. Joumalof Occupational Medicine, 28,lS-22.
Bernacki El, Baun WB. (1984). The relationship of job performance to exercise adherence in a corporate fitness program. Journal of Occupational Me&&, 26,529-531.
Blegen MA, Mueller CW, Price JL. (1988). Measurement of kinship responsibility for organizational research. Journal ofApplied Psychology, 73,402-409.
Bowne DW, Russell ML, Morgan JL, Optenberg SA, Clark AE. (1984). Reduced disability and health care costs in an industrial fitness program. Journal of Occupational Medic&, 26,809416.
Caplan RD, Cobb S, French JRP Jr, Van Harrison R, Pinneau SR. (1980). Job demands and worker health. Institute for social Research: Ann Arbor, MI.
Chambliss CA, Murray El. (1979). Efficacy attribution: Locus of control and weight loss. Cognitive Thempy Research, 3,349-353.
Cohen J. (1977). Statistical power analyses for the behavwml sciences. San Diego, CA: Academic Press.
Condiotte MM, Lichtenstein E. (1981). Self-efficacy and relapse in smoking cessation: A replication and extension. Journal of Consulzing and Clinical Psychology, 49,648- 658.
Cox MH. (1984). Fitness and lifestyle programs for business and industry: Problems in recruitment and retention. J o m l of Cardiac Rehabilitation, 4,136-142.
Davis KE, Jackson KL, Kronenfeld JJ, Blair SN. (1987). Determinants of participation in worksite health promotion activities. Health Education Quarterly, 14,195-205.
Dishman RK, Gettman LR. (1980). Psychobiologic influence of exercise adherence. Jour-
Erfurt JC, Fmte A, Heirich MA. (1992). The cost-effectiveness of worksite wellness programs for hypertension control, weight loss, smoking cessation, and exercise.
Ewart CK, Taylor CB, Reese LB, Debusk RE (1984). Effects of early postmyocardial infar- cation exercise testing on self-perception and subsequent physical activity. Amen- can Joumal of Cardiology, 41,10761080.
Fakenberg LE. (1987). Employee fitness programs: Their impact on the employee and the organization. Academy of Management Review, 12,511-522.
Florey C du V (1970). The use and interpretation of ponderal index and other weight- height ratios in epidemiological studies. Journal of Chronic Diseases, 23,93-103.
Garland H, Weinberg R, Bruya L, Jackson A. (1988). Self-efficacy and endurance perfor- mance: A longitudinal field test of cognitive mediation theory. Applied Psychology: An International Rwiew, 37,381-394.
Gebhardt DL, Crump CE. (1990). Employee fitness and wellness programs in the work- place. American Psychologist, 45,262-272.
Glasgow RE, Terborg JR. (1988). Occupational health promotion programs to reduce cardiovascular risk. Journal of Comulting and Clinical Psychology, 56,365-373.
nal Of Sport PsychologY, 2,295-310.
PERSONNEL PSYCHOLQGY, 45,5-27.

70 PERSONNEL PSYCHOLOGY
Godin G, Shephard RJ. (1986). Importance of type of attitude to the study of exercise- behavior. Psychological Reports, 58,991-1000.
Guthrie Jp, Olian JD. (1990). Using psychological constructs to improve health and safety: The HRM niche. In Fems GW (Ed.), Research in personnel and human resources management, Vol. 8 (pp. 141-201). Greenwich, CT: JAI Press.
Hollenbeck JR, Klein HJ. (1987). Goal commitment and the goal-setting process: Prob- lems, prospects, and proposals for future research. Journal of Applied Psychology, 2,212-220.
HumphreF LG, Montanelli RG Jr. (1975). An investigation of the parallel analysis cri- terion for determining the number of common factors. Multivariate Behavioral Re- search, 10,193-205.
Ilgen DR. (1990). Health issues at work Opportunities for industriaUorganizational psy- chology. American Psychologist, 45,273-283.
Janz NK, Becker MH. (1984). h e health belief model: A decade later. Health Education Quarterly, I I , 1-47.
Jick TD, Mitz LF. (1985). Sex differences in work stress. Academy of Management Review, 10,408-420.
Kahn FU. (1981). Work and health. New York Wiley. Kanfer FH, Phillips JS. (1970). Learning foundations of behavior therapy. New York Wiley. Kaplan RM, Atkins CJ, Reinsch S. (1984). Specific efficacy expectations mediate exercise
Kasl SV. (1984). Stress and health. Annual Review of Public Health, 5,319-342. Kobasa SC, Maddi SR, Kahn S. (1982). Hardiness and health: Aprospective study. Journal
Lau RR. (1982). Origins of health locus of control beliefs. Journal of Personality and Social
Lean P, Hanin J, West C, Shephard RJ. (1988). Seven year follow-up of an employee fitness program. Canadian Journal of Public Health, 79,2045.
Lichtman S, Poser EG. (1983). The effects of exercise on mood and cognitive functioning. Journal of Pychosomatic Research, 27,43-52.
Locke EA, Latham GI? (1990). A theory of goal setting and task perjomnce. Englewood Cliffs, N J Prentice-Hall.
Locke EA, Latham GP, Erez M. (1988). The determinants of goal commitment. Academy of Management Review, 13,-39.
Mahoney MJ, Moura NG, Wade TC. (1973). The relative efficacy of self-reward, self- punishment, and self-monitoring techniques for weight loss. Journal of Consulting and Clinical Psychology, 40,404407.
Marcus BH, Owen N. (1992). Motivational readiness, self-efficacy, and decision-making for exercise. Journal ofApplied Social Psychobg~, 22,3-16.
Mathieu JE, Martineau JW, lhnebaum SI. (1993). Individual and situational influences on the development of self-efficacy: Implications for training effectiveness. PER-
McAuley E, Coumeya KS. (1992). Self-efficacy relationships with affective and exertion
Melnyk KAM. (1988). Barriers: A critical review of the literature. Nursing Research, 37,
Naylor JC, Pritchard RD, Ilgen DR. (1980). A theory of behavior in organizations. New
ODonnell MI? (1986). Definition of health promotion: Part I 1 Levels of programs.
OLeary A. (1985). Self-efficacy and health. Behavior Research and Thempy, 23,437451.
compliance in patients with COPD. Health Psychology, 3,223-242.
of Personality and Social Psychology, 42,168-177.
Psychology, 42,322-334.
sONNELPSYCHOLOGY, 46,125-147.
responses to exercise. Journal ofApplied Social Psychology, 22,312-326.
196-201.
York Academic Press.
American Journal of Health Promotion, 1, fj-9.

HARRISON AND LISKA 71
Peterson C, Seligman ME€? (1984). Causal explanations as a risk factor for depression: Theory and evidence. Psychological Review, 91,347-374.
Pong K, McAuley E. (1992). Goal setting, self-efficacy, and exercise behavior. Journal of S p r t & Ewrcrie Psychoogy, 14,352-360.
Rotter JB. (1975). Some problems and misconceptions related to the construct of internal versus external locus of control of reinforcement. Journal of Consultingand Clinical
Schifter DB, Ajzen I. (1985). Intention, perceived control, and weight loss: An application of the theory of planned behavior. Journal of Personaliy and Social Psychology, 49, 843-851.
Seidman Is, Sevelius CG, Ewald F! (1984). A cost-effective weight loss program at the worksite. J o m l of Occupational Medicine, 29,884-891.
Seligman ME€? (1986). Ekphnatory styk: Depresswn, Lyndon Baines Johnson and the Baseball Hall of Fame. Paper presented at the Ninety-Fourth Annual Convention of the American Psychological Association. Washington, DC.
Settergen SK, Wilbur CS, Hartwell TD, Rassweiller JH. (1983). Comparison of respon- dents and nonrespondents to a worksite health screen. J o m l of Occupational Medicine, 25,475-480.
Shephard FU, Corey P, Renzland P, Cox M. (1982). The influence of an employee fitness and lifestyle modification program upon medical care costs. Canadian Journal of Pubkc Health, 73,259-263.
Snyder CR, Higgins RL. (1988). Excuses: Their role in the negotiation of reality. Psycho- logical Bulktin, I#, 23-35.
Steinhardt MA, Young DR. (1992). Psychological attributes of participants and nonpar- ticipants in a worksite health and fitness center. BehuvwmlMedicine, 18,4046.
Strecher VJ, Becker MH, Kirscht JP, Eraker SA, Graham-Tomasi Rp. (1985). Psychosocial
Psychology, 43,56-67.
aspects of changes in cigarette-smoking behavior. Patient Education Co&seling, 7, 249-262.
Strecher VJ, DeVellis BM, Becker MH, Rosenstwk IM. (1986). The role of self-efficacy in achieving health behavior change. Health Education Quarte& 13,73-91.
Thylor SE, Brown JD. (1988). Illusion and well-being: A social psychological perspective on mental health. Psrchological Bulletin, 103,193-210.
Terborg JR. (1986). Health promotion at the worksite: A research challenge for personnel and human resources management. In Fems G, Rowland K (Eds.), Research in personnel and human resources management, VoL 4 (pp. 225-267). Greenwich, CT: JAI Press.
Tirrell BE, Hart LK (1980). The relationship of health beliefs and knowledge to exercise compliance in patients after coronary bypass. Heart Lung, 9,487-493.
Tsai SP, Baun WB, Bernacki EJ. (1987). Relationship of employee turnover to exercise adherence in a corporate fitness program. Journal of Occupational Medicine, 29,
'hbbs ME. (1986). Goal setting: A meta-analytic investigation of the empirical evidence. Journal of Applied Psychology, 71,474432.
Vrmm VH. (1964). Work motivation. New York: Wiley. Wood RE, Mento AJ, Locke EA. (1987). Task complexity as a moderator of goal effects:
A meta-analysis. Journal ofApplied Psychology, 72,416-425. Zavela KJ, Davis LG, Cottrell RR, Smith WE. (1988). Do only the healthy intend to
participate in worksite health promotions? Health Education Quarterly, IS, 259- 267.
572-575.