project pearls objectives - ichp - residency... · residency project pearls ... objectives •...
TRANSCRIPT

8/29/2012
1
Residency Project Pearls
Adherence to and Outcomes Associated with a Clostridium difficile Infection Guideline at a
Large Teaching Institution
RaeAnna C. Zatarski, Pharm.D.September 15, 2012
Speaker has no conflicts of interest to disclose.
Objectives
• Select a treatment plan for a patient with Clostridium difficile infection based on the severity of illness.
• Identify potential barriers to adherence to the Clostridium difficile infection treatment guidelines.
Advocate Lutheran General Hospital (ALGH)
• Academic research institution
• Level 1 trauma center
• 645 bed capacity
• Located in Park Ridge, Illinois
Clostridium difficile Infection (CDI)
Causes 20 – 30% of antibiotic associated diarrhea
• Risk factors for CDI– Prior antimicrobial or proton pump inhibitor use
Recent immunosuppressive therapy– Recent immunosuppressive therapy
• Epidemiology – Incidence: 85,700 in 1993 → 301,200 in 2005 – Mortality: 5.7 / million in 1999 → 23.7 / million in 2004– Incidence at ALGH: 400 patient cases annually
Schroeder MS. Am Fam Physician. 2005 March 1;71(5):921‐8.Cohen SH, et al. Infect Control Hosp Epidemiol. 2010 May;31(5):431‐55.
Treatment
• Early treatment of CDI– Metronidazole designated as first line agent– Vancomycin limited to failures or intolerance
• Increased incidence of metronidazole failures causedIncreased incidence of metronidazole failures caused shift in clinical practice
• Zar trial (2007)– Mild‐moderate: metronidazole noninferior to vancomycin– Severe: vancomycin superior to metronidazole
Jung KS, et al. Gut Liver. 2010 Sept;4(3):332‐7.Zar FA, et al. Clin Infect Dis. 2007 Aug 1;45(3):302‐7.
Treatment
• ALGH approved physician‐managed CDI treatment guidelines in July 2009– Stratified patients into severity categories according to clinical signs and symptoms
– Recommended specific treatment regimens based on severity category
• SHEA / IDSA published their revised CDI treatment guidelines in May 2010
Cohen SH, et al. Infect Control Hosp Epidemiol. 2010 May;31(5):431‐55.

8/29/2012
2
ALGH Recommendations for Initial Treatment
Clinical Severity Supportive Clinical Data Recommended Treatment
Mild‐moderateWBC < 15,000 cell/mcL and a serum creatinine level < 1.5
times premorbid level
Metronidazole 500mg PO q8h for 10 ‐ 14 days
SevereWBC ≥ 15,000 cell/mcL orserum creatinine level ≥ 1.5
times premorbid level
Vancomycin 125 mg PO q6hfor 10 ‐ 14 days
Severe ‐complicated
Hypotension, shock, ileus, megacolon
Vancomycin 500 mg PO q6h + metronidazole 500 mg IV q8h
Current Study
• Rationale– Anecdotal evidence suggested physician non‐adherence– Concern regarding undertreatment of patients
• Purpose– To determine if physicians were adherent to the ALGH CDI guidelines
– To determine if adherence to the guidelines improved patient outcomes
Methods• Descriptive, retrospective chart review
• Subject population– Age ≥ 18 years diagnosed July 1, 2009 – June 30, 2011– CDI treatment initiated at LGH– CDI treatment initiated at LGH
• Assessment – Severity categorized based on clinical signs and symptoms– Initial treatment compared to recommended therapy
• Evaluated for adherence • Classified as under, appropriate, or overtreatment
Endpoints
• Primary endpoint: percentage of subjects who were treated in accordance with CDI guidelines
S d d i t• Secondary endpoints– Incidence of under, appropriate, and overtreatment– Incidence of clinical outcomes in treatment groups– Impact of proton pump inhibitor or prior antimicrobial use on CDI severity
Definitions
• Clinical cure: no need for therapy escalation; resolution of diarrhea by day 6; and subject survival
• Recurrence: positive stool toxin assay within 90 days of initial positive stool toxin assaypositive stool toxin assay
• Mortality: subject expired from any cause within 90 days of positive stool toxin assay
• Antimicrobial use: use of at least one dose of an antimicrobial in the eight weeks prior to the positive stool toxin assay
Statistics
• Descriptive study required 130 subjects for 80% power for the primary endpoint
• Pearson Chi‐Square / Fisher’s exact tests used to analyze q / ygroup differences– Two‐tailed p value < 0.05 considered statistically significant for
single comparisons– Two‐tailed p value < 0.02 considered statistically significant for
multiple comparisons (Bonferroni’s method)

8/29/2012
3
Results
650 subjects id tifi d
250 subjects randomly 324 encounters
l t didentified randomly selected evaluated
Baseline Characteristics: Subjects
Characteristics [n = 250]
Female [no (%)] 141 (56.4)
Age [mean (SD), range] 67.83 ± 17.36 (18 – 100)
Ethnicity [no (%)]CaucasianAfrican‐AmericanAsianHispanic
210 (84)13 (5.2)12 (4.8)7 (2.8)
History of CDI [no (%)] 18 (7.2)
Baseline Characteristics: Encounters
Encounters [n = 324] No (%)
Initial Episode 220 (67.7)
1st recurrence 56 (17.3)
Severity [n = 324] No (%)
Mild‐moderate 163 (50.3)1 recurrence 56 (17.3)
2nd recurrence 10 (3.1)
3rd recurrence 5 (1.5)
Reinfection 33 (10.2)
Mild moderate 163 (50.3)
Severe 105 (32.4)
Severe‐complicated 56 (17.3)
Adherence Rates
No (%)
Overall [n = 324] 137 (42.3)
Mild‐moderate [n = 163] 86 (52.8)
Severe [n = 105] 41 (39)
Severe‐complicated [n = 56] 10 (17.9) p < 0.001
Mild‐moderate Treatment Regimens
Regimen [n = 163] No (%)
Metronidazole 500 mg PO q8h 66 (40.5)
Metronidazole 500 mg IV q8h 22 (13.5)
Vancomycin 125 mg PO q6h * 51 (31.3)
Metronidazole 500 mg IV q8h +vancomycin 125 mg PO q6h 13 (8)
Other 11 (6.7)
* Appropriate depending onsubject’s history of illness.
Mild‐moderate Treatment Regimens

8/29/2012
4
Severe Treatment Regimens
Regimen [n = 105] No (%)
Metronidazole 500 mg PO q8h 19 (18.1)
Metronidazole 500 mg IV q8h 17 (16.2)
i h ( )Vancomycin 125 mg PO q6h 41 (39)
Metronidazole 500 mg IV q8h + vancomycin 125 mg PO q6h 15 (14.3)
Metronidazole 500 mg IV q8h + vancomycin 250 mg PO q6h 7 (6.7)
Other 6 (5.7)
Severe Treatment Regimens
Severe‐complicated Treatment Regimens
Regimen [n = 56] No (%)
Metronidazole 500 mg IV q8h 8 (14.3)
Vancomycin 125 mg PO q6h 12 (21.4)
Metronidazole 500 mg IV q8h + 16 (28 6)g qvancomycin 125 mg PO q6h 16 (28.6)
Metronidazole 500 mg IV q8h + vancomycin 250 mg PO q6h 5 (8.9)
Metronidazole 500 mg IV q8h + vancomycin 500 mg PO q6h 10 (17.9)
Other 5 (8.9)
Severe‐complicated Treatment Regimens
Overall Treatment Regimens Undertreatment versus Appropriate Treatment
Overall [n = 324]No (%)
Undertreatment[n = 85]No (%)
Appropriate treatment[n = 149]No (%)
Percent difference
Escalation required 83 (25.6) 29 (34.1) 41 (27.5) + 6.6
Clinical cure 178 (54.9) 35 (41.2) 83 (55.7) ‐ 14.5 *
Mortality 43 (13.3) 21 (24.7) 15 (10.1) + 14.6
Recurrence free 224 (69.1) 47 (55.3) 112 (75.2) ‐ 19.9
p < 0.02* p = 0.033

8/29/2012
5
Overtreatment versus Appropriate Treatment
Overall [n = 324]No (%)
Appropriate treatment[n = 149]No (%)
Overtreatment [n = 90]No (%)
Percent difference
Escalation required 83 (25.6) 41 (27.5) 13 (14.4) ‐ 13.1
Clinical cure 178 (54.9) 83 (55.7) 60 (66.7) + 11.0
Mortality 43 (13.3) 15 (10.1) 7 (7.8) ‐ 2.3
Recurrence free 224 (69.1) 112 (75.2) 65 (72.2) ‐ 3.0
p < 0.02
Proton Pump Inhibitor Use
SeverityUsed proton
pump inhibitorNo (%)
Overall [n = 324] 235 (72.5)[ ] ( )
Mild‐moderate [n = 162] 116 (71.6)
Severe [n = 105] 73 (69.5)
Severe‐complicated [n = 56] 46 (82.1) p = 0.16
Prior Antimicrobial Use
SeverityAntimicrobial use in previous 8 weeks
No (%)
Overall [n = 324] 239 (73.8)[ ] ( )
Mild‐moderate [n = 162] 121 (74.7)
Severe [n = 105] 79 (75.2)
Severe‐complicated [n = 56] 39 (69.6) p = 0.81
Limitations
• Retrospective study
• Researcher bias
• Strict adherence to guideline definitions
• Study not powered to analyze secondary endpoints
Conclusions: Primary Endpoint
• 42 % overall adherence to CDI guideline
• Adherence lower in severe and severe‐complicated CDI
• Barriers to adherence– Lack of awareness among hospital staff– Subjects unable to take medications by mouth– Barriers to using rectal vancomycin– Clinically severe subjects with low WBC count
Conclusions: Secondary Endpoints
• Undertreatment versus appropriate treatment– Significantly increased incidence of mortality and recurrence– Lower incidence of clinical cure
• Overtreatment versus appropriate treatment• Overtreatment versus appropriate treatment – Failed to show significant improvement in clinical outcomes– Potentially leads to increased medication costs and adverse
effects
• Proton pumps inhibitor and prior antimicrobial use was not significantly different between severity groups

8/29/2012
6
Patient Case
RW is a 37‐year old female with no significant past medical history who is admitted to the hospital for three days of diarrhea after a seven day treatment course of moxifloxacin for community‐acquired
pneumonia. RW’s symptoms include a white blood cell count of 13.0 cells/mm3, serum creatinine (Scr) of 0.7 g/dL, and a positive stool toxin assay for CDI.
Based on RW’s symptoms, what is her severity of illness?
A. Mild‐moderateB. Mild‐moderate, ,
complicatedC. SevereD. Severe, complicated
Mild‐moderate
Mild‐moderate, compli...
Severe
Severe, complicated
0% 0%0%0%
Based on RW’s severity of illness, please select the most appropriate treatment option from the list below.
A. Oral vancomycin 125 mg every 6 hours for 14 days
B. Oral metronidazole 500 mg every 8 hours for 14 daysevery 8 hours for 14 days
C. Oral vancomycin 250mg every 6 hours for 14 days
D. Intravenous metronidazole500 mg every 8 hours PLUS oral vancomycin 500 mg every 6 hours for 14 days
Oral vancomycin 125 m
g...
Oral metronidazo
le 500 ..
Oral vancomycin 250mg ...
Intravenous metronidazo..
0% 0%0%0%
Residency Project Pearls
Adherence to and Outcomes Associated with a Clostridium difficile Infection Guideline at a
Large Teaching Institution
RaeAnna C. Zatarski, Pharm.D.September 15, 2012

Adherence to and Outcomes Associated with a Clostridium difficile Infection Guideline at a Large Teaching Institution
RaeAnna C. Zatarski, Pharm.D.
Background: The incidence and severity of Clostridium difficile infection (CDI) is on the rise with reports of devastating health outcomes. National CDI treatment guidelines stratify patients based on clinical symptoms and recommend specific treatment based on severity of illness. In 2009, Advocate Lutheran General Hospital adopted guidelines with identical treatment algorithms. The purpose of this project was to determine if patients were being treated in accordance with the CDI guidelines and whether adherence affected patient outcomes.
Methods: This was a retrospective, descriptive study. Subjects were identified by CDI‐associated ICD‐9 codes from July 1, 2009 to June 30, 2011. Subjects were stratified by disease severity based on laboratory values and symptoms. Guideline adherence was assessed based on initial treatment selection and subjects were categorized as undertreated (UT), overtreated (OT), or appropriately treated (AT) accordingly. Secondary endpoints included need for therapeutic escalation, clinical cure, recurrence rates, 90‐day all‐cause mortality, proton pump inhibitor (PPI) and antimicrobial use.
Results: Two hundred fifty subjects with 324 encounters were analyzed. Overall guideline adherence rate was 42.3%. Adherence rates by severity: mild‐moderate, 52.8%; severe, 39.0%; and severe‐complicated, 17.9% (p < 0.001). 46% of subjects were AT, 27.8% were OT, and 26.2% were UT. Clinical outcomes between UT versus AT subjects: therapeutic escalation required, 34.1% vs. 27.5%; clinical cure, 41.2% vs. 55.7%; mortality, 24.1% vs. 10.1%; and recurrence, 44.7% vs. 24.8%. Clinical outcomes between OT versus AT subjects: therapeutic escalation required 14.4% vs. 27.5%; clinical cure, 66.7% vs. 55.7%; mortality, 7.8% vs. 10.1%; recurrence, 27.8% vs. 24.8%. PPI or antimicrobial use did not affect severity of illness.
Conclusions: The majority of subjects were not treated in accordance with the CDI guidelines, particularly those with severe and severe‐complicated illness. UT subjects had worse clinical outcomes compared to their AT counterparts whereas, OT subjects failed to show significant improvements in clinical outcomes compared to AT subjects. Emphasis should be placed on CDI guideline adherence as this results in improved outcomes.
8/29/2012
1
Residency Project PearlsResidency Project Pearls
A pilot multidisciplinary team to monitor A pilot multidisciplinary team to monitor controlled substance documentation in a controlled substance documentation in a
community hospitalcommunity hospital
Tim Humlicek, PharmDPGY2 Solid Organ Transplant Pharmacy Resident
Rush University Medical CenterChicago, IL
DisclosureDisclosure
The author of this presentation has no actual or potential conflicts of interest.
Learning ObjectivesLearning Objectives
• Outline the process of interpreting controlled substance reports generated from automated dispensing machines that can identify hig risk usersusers.
• Recognize potential controlled substance diversion episodes using electronic medication administration documentation
NorthShore University HealthSystemNorthShore University HealthSystem
• Four acute care hospitals– Evanston Hospital: 354 beds– Glenbrook Hospital: 169 bedsHighland Park Hospital: 149 beds– Highland Park Hospital: 149 beds
– Skokie Hospital: 195 beds
• NorthShore Medical Group• NorthShore Research Institute• NorthShore Foundation
RegulationsRegulations• Drug Enforcement Administration (DEA)
– Enforces the Controlled Substance Act– Employee pilferage and units lost in transit:
• 22.7% of all unaccounted oxycodone in 2000‐2003
• Joint Commission Standard MM.4.80– Requires processes to address diversion prevention and account for all unused, expired, or returned medications.
1. Drug Enforcement Administration. Oxycodone theft & loss incidents: January 2000 through June 2003. http://www.deadiversion.usdoj.gov/drugs_concern/oxycodone/oxylosses_oct2003_1.pdf. Accessed July 28, 2011
2. Keenly P, Uselton JP. Maintain Compliance with Joint Commission Medication Management Standards. http://www.psqh.com/julaug08/medication.html. Accessed July 28, 2011.
Health System DiversionHealth System Diversion
• Diversion: unlawful channeling of regulated pharmaceuticals from legal sources to illicit
•• OpportunitiesOpportunities–– Destruction/WasteDestruction/Waste–– IntrahospitalIntrahospital transfertransfer–– LargeLarge‐‐volume removalsvolume removals
market –– MultiMulti‐‐dose vialsdose vials–– Patient specific itemsPatient specific items–– Point of purchasePoint of purchase–– Unauthorized removalsUnauthorized removals
Inciardi JA et al. Mechanisms of Prescription Drug Diversion Among Drug-Involved Club-and Street-Based Populations..Pain Med. 2007;8(2):171-183
O’Neal B, Siegel J. Diversion in the Pharmacy. Hosp Pharm. 2007;42(2):145-148
.

8/29/2012
2
BackgroundBackground
• Lack of comprehensive published guidelines– Available recommendations:
• Multidisciplinary teams• Monitoring in operating rooms• Investigative process• Drug diversion software• Intervention process
O’Neal B, Siegel J. Diversion in the Pharmacy. Hosp Pharm. 2007;42(2):145-148Siegel J, Wierwille C, O’neal B. The Investigative Process. Hosp Pharm. 2007:42(2);466469Siegel J, O’Neal B. Code N: Multidisciplinary Approach to Proactive Drug Diversion Prevention. Hosp Pharm. 2007:42(2);244-248
BackgroundBackground
• University Health System Consortium Survey– Operating Room Practices: 44‐63% reconciled against dispensing records
– Use of diversion software: 79%• “Sometimes” or “Always” investigate flagged individuals identified by software: 88‐99%
– Discrepancies “always” investigated: 92‐98%
McClure SR, O’Neal BC, Grauer D, Couldry RJ, King AR. Compliance with Recommendations for Prevention and Detection of Controlled-substance Diversion in Hospitals. Am J Health-Syst Pharm. 2011;68(8):689-94.
Project ObjectivesProject Objectives
• Primary::– Develop and implement a standardized process to identify users with risk of controlled substance diversion
Project ObjectivesProject Objectives
• Secondary:– Quantify potential controlled substance diversion opportunities in users with identified risk of controlled substance diversion
– Assess the type of controlled substance discrepancies occurring based on controlled substance documentation
MethodsMethods
Monthly Report
• Pharmacist to upload monthly ADM data to vendor• Pharmacist organizes vendor report to identify high risk users
U A di
• Pharmacist prints controlled substance removals from previous 30 days for identified usersN M di i f i d iUser Audit • Nurse Manager audits transactions for appropriate documentation
Follow Up
• Users with potential diversion episodes are assessed by pharmacist and nurse manager for further diversion risks
Methods: Identifying UsersMethods: Identifying UsersReport 1: Compares removals of all controlled substances
by one user to all users
Report 2: Compares all removals of given controlled substance by one user to all users of same ADM
Report 3: Compares removals of given controlled substance by one user to all
users of that class/medicationusers of that class/medication
Report 4: Compares daily average removals for one user for
given controlled substance to all users of same
ADM

8/29/2012
3
Methods: Identifying UsersMethods: Identifying Users• Report 1: Users with >3 SDs (SD) above the mean removal of any controlled
substance
AND
• Report 2: Users with >2 SD above mean compared to station level peers for given class of controlled medications
AND
• Report 3: Users with >2 SD above mean compared to all hospital users for given class of controlled medications
AND
• Report 4: Users with >2 SD above mean compared to station level peers on a daily basis for given class of controlled medications
Methods: User AuditMethods: User Audit
• Users had all removals of controlled substances in previous 30 days audited for documentation and potential diversion episodes:– Removal without order– Removal without documented administration– Removal in excess of order that does not require waste– Removal in excess of order that requires waste without appropriate
waste documentation
Methods: User AuditMethods: User Audit
Behavioral Indicators• Isolates self• Frequent disappearances• Unscheduled visits
V l t f dditi l hift
Patient Care Indicators• Incorrect charting• Inconsistent work quality• Offers to help other nurses’
patients• Volunteers for additional shifts• Frequently spills/wastes narcotics• Chaotic home life• Refused compliance with
investigations
patients• Removes excessive amounts of
narcotics• Requests specific patients• Inadequate pain control with
patients
Siegel J, O’Neal B. Code N: Multidisciplinary Approach to Proactive Drug Diversion Prevention. Hosp Pharm. 2007:42(2);244-248
Methods: User AuditMethods: User AuditNumber marked “Yes” Level of Risk
0‐2 Points Low
3‐4 Points Medium
>5 Points High
Siegel J, O’Neal B. Code N: Multidisciplinary Approach to Proactive Drug Diversion Prevention. Hosp Pharm. 2007:42(2);244-248
Methods: Discrepancy AuditMethods: Discrepancy Audit
• Controlled substance discrepancies were reviewed over the same period assessing for type and severity– Level 1: Miscounting– Level 2: Mechanical error– Level 3: Inappropriate documentationpp p– Level 4: Incorrect administration– Level 5: Inadequate resolution
ResultsResultsIndicator Nov. 2011 Dec. 2011 Jan. 2012 Feb. 2012
Doses Dispensed‐ ADM 62,016 60,049 59,784 54,918
Average Daily Doses‐ADM 2,067 1,937 1,929 1,894
C‐II to C‐V Dispense 5,208 4,348 3,788 3,649% C‐II to C‐V 8.40% 7.24% 6.34% 6.64%
Total C‐II to C‐V Discrepancies
42 36 29 13
% C‐II to C‐V Discrepancies 0.81% 0.83% 0.77% 0.36%
Total Overrides 2,938 3,137 3,015 1,995C‐II to C‐V Overrides 891 931 897 623
% C‐II to C‐V Overrides 1.44% 1.55% 1.50% 1.13%
8/29/2012
4
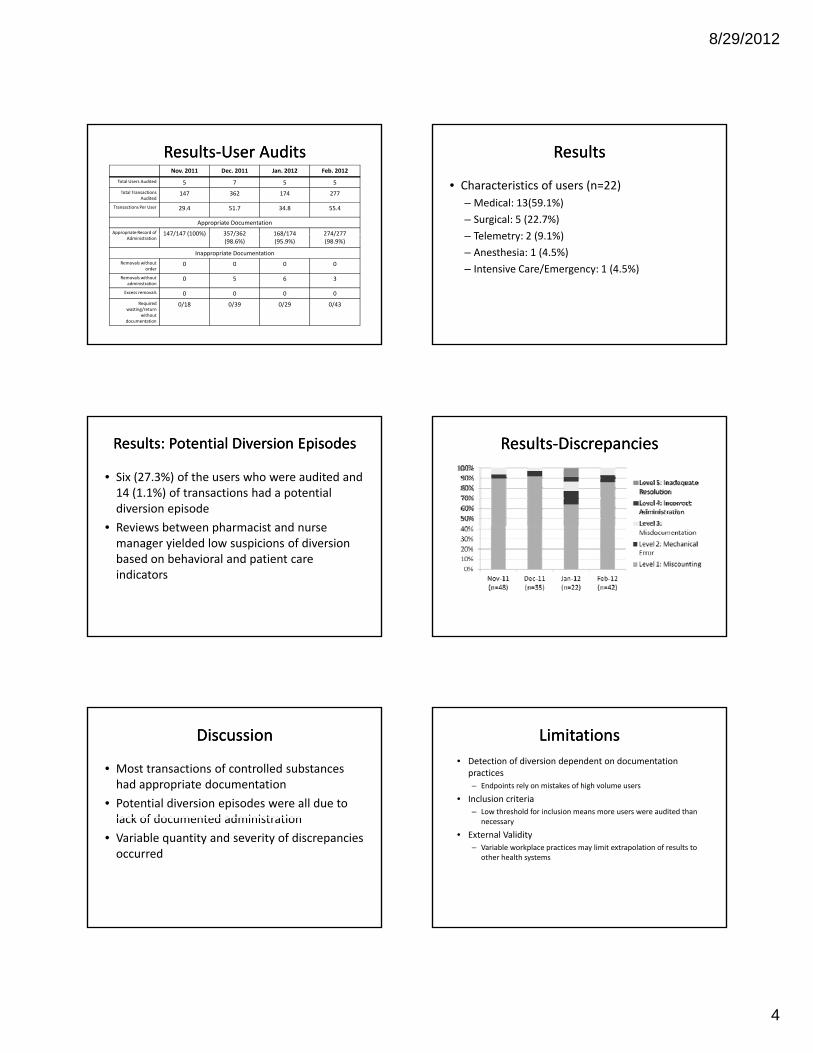
ResultsResults‐‐User AuditsUser AuditsNov. 2011 Dec. 2011 Jan. 2012 Feb. 2012
Total Users Audited 5 7 5 5Total Transactions
Audited147 362 174 277
Transactions Per User 29.4 51.7 34.8 55.4
Appropriate DocumentationAppropriate Record of 147/147 (100%) 357/362 168/174 274/277pp p
Administration147/147 (100%) 357/362
(98.6%)168/174 (95.9%)
274/277 (98.9%)
Inappropriate DocumentationRemovals without
order0 0 0 0
Removals without administration
0 5 6 3
Excess removals 0 0 0 0Required
wasting/return without
documentation
0/18 0/39 0/29 0/43
ResultsResults
• Characteristics of users (n=22)– Medical: 13(59.1%)– Surgical: 5 (22.7%)Telemetry: 2 (9 1%)– Telemetry: 2 (9.1%)
– Anesthesia: 1 (4.5%)– Intensive Care/Emergency: 1 (4.5%)
Results: Potential Diversion EpisodesResults: Potential Diversion Episodes
• Six (27.3%) of the users who were audited and 14 (1.1%) of transactions had a potential diversion episode
• Reviews between pharmacist and nurse• Reviews between pharmacist and nurse manager yielded low suspicions of diversion based on behavioral and patient care indicators
ResultsResults‐‐DiscrepanciesDiscrepancies
DiscussionDiscussion
• Most transactions of controlled substances had appropriate documentation
• Potential diversion episodes were all due to lack of documented administrationlack of documented administration
• Variable quantity and severity of discrepancies occurred
LimitationsLimitations• Detection of diversion dependent on documentation
practices– Endpoints rely on mistakes of high volume users
• Inclusion criteria– Low threshold for inclusion means more users were audited than
necessary
• External Validity– Variable workplace practices may limit extrapolation of results to
other health systems
8/29/2012
5
Future DirectionsFuture Directions
• Specify audits for users with highest removals• Establish protocol for investigating potential diversion
episodes in users with medium‐high risk:– Establish level of suspicion for prioritizing further interventions
• Implement use of refined methods across health system• Implement use of refined methods across health‐system
ConclusionsConclusions
• Using objective criteria from usage reports is capable of identifying users with disproportionate removals of controlled substances
• Subjective knowledge of employees is another important aspect of diversion monitoringaspect of diversion monitoring
• Appropriate documentation occurred most frequently• Potential diversion episodes lacked an documented
administration, but could have been administered by another user
• Discrepancy quantity and severity may be useful as a benchmark to track documentation practices
SELF ASSESSMENT QUESTIONSELF ASSESSMENT QUESTION#1#1
Which of the following users meets at least one criteria to be eligible for a controlled substance transaction audit?
a) A user with a monthly average of removals less than 3 SDs of the mean for a particular controlled substance compared to all hospital users
b) A user with a daily average removals less than 2 SDs above the mean for a particular controlled substance compared to all users of a specific automated dispensing machine
c) A user with a monthly average of removals less than 2 SDs above the meanc) A user with a monthly average of removals less than 2 SDs above the mean compared to all users of a particular automated dispensing machine
d) A user with a monthly average of removals greater than 3 SDs of the mean for a particular controlled substance compared to all hospital users
SELF ASSESSMENT QUESTIONSELF ASSESSMENT QUESTION#2#2
Which of the following could be considered a potential controlled substance diversion episode?
a) Removal of a controlled substance and a documented patient refusal and an appropriate record of return
b) Removal of a controlled substance without an order
c) Removal of a controlled substance with a documented administration to a patientp
d) Canceled removal of a controlled substance with subsequent documented administration
8/29/2012
6
Special thanks to:• Carol Heunisch, PharmD, BCPS• Nancy Lechowicz, RN, MS• Monica Sherlock RN MSN• Monica Sherlock, RN, MSN• Rita Walter, RN, MS• Mary Keegan, RN, MS
ReferencesReferences1. Drug Enforcement Administration. http://www.justice.gov/dea/ . Accessed July 31, 2011.2. Drug Enforcement Administration. Oxycodone theft & loss incidents: January 2000 through June
2003. http://www.deadiversion.usdoj.gov/drugs_concern/oxycodone/oxylosses_oct2003_1.pdf. Accessed July 28, 2011
3. Keenly P, Uselton JP. Maintain Compliance with Joint Commission Medication Management Standards. http://www.psqh.com/julaug08/medication.html. Accessed July 28, 2011.
4. Inciardi JA et al. Mechanisms of Prescription Drug Diversion Among Drug‐Involved Club‐and Street‐Based Populations..Pain Med. 2007;8(2):171‐183
5. O’Neal B, Siegel J. Diversion in the Pharmacy. Hosp Pharm. 2007;42(2):145‐1486 McClure SR O’neal BC Grauer D Couldry RJ King AR Compliance with Recommendations for6. McClure SR, O neal BC, Grauer D, Couldry RJ, King AR. Compliance with Recommendations for
Prevention and Detection of Controlled‐substance Diversion in Hospitals. Am J Health‐Syst Pharm. 2011;68(8):689‐94.
7. Siegel J, Wierwille C, O’neal B. The Investigative Process. Hosp Pharm. 2007:42(2);466‐4698. Siegel J, O’Neal B. Code N: Multidisciplinary Approach to Proactive Drug Diversion Prevention.
Hosp Pharm. 2007:42(2);244‐248
Questions?Questions?
Contact Information:Tim Humlicek, PharmD
Rush University Medical Centertimothy j humlicek@rush [email protected]

8/29/2012
1
Residency Project Pearls
Prolonged Antibiotic Prophylaxis After Cardiovascular Implantable Electronic Device Implantation and Its Effect on
Device‐Related InfectionsDevice‐Related Infections Natasha Lopez, PharmD, BCPS
Critical Care PharmacistRush University Medical Center
Chicago, IL
Disclosure Statement
The speaker has no actual or potential conflict of interest in relation to this
presentation
Background
• Cardiac implantable electronic device (CIED) infections have remained a major complication after implantation
• The incidence of infection related to CIED implantation ranges from 0.13% to 19.9%
• Variations in the populations and practices at different sites account for this range of incidence rates
• With the expanded indications for CIED implantation and higher risk patient population receiving therapy, the prevention and management of CIED infections continues to be studied
DiMarco, et al. NEJM. 2003;349:1836‐1847.
Microbiology of CIED Infections
Sohail MR, et al. J Am Coll Cardiol. 2007;49:1851‐1859.
Risk FactorsPatient Factors Procedural Characteristics
•Diabetes mellitus
•Heart failure
•Malignancy
R l d f i ( l l
•Fever within 24 hours of implant
•Pre‐procedural temporary pacing
•Device revision/replacement
P f h 2 i•Renal dysfunction (glomerularfiltration rate <60 mL/min)
•Corticosteroid use
•Oral anticoagulant use
•Presence of more than 2 pacing leads
•Failure to receive preoperative antibiotic prophylaxis
•Physician experience
Klug D, et al. Circulation.2007;166:1349‐1355.Nery P, et al.J Cardiovasc Electrophysiol. 2010; 21:786‐790.Sohail, M, et al. CID. 2007;45:166‐173.
Study Agent/Dose/Regimen No. of Patients
Follow‐up in Months (range)
Results
Jacobson et al Cloxacillin 2 g IV 1 hr before and 1 g IV q6h for 2 days and by mouth for 8 days after
N= 100 Abx= 50Control= 50
NA (1‐43) Infection: Abx= 1 Control= 7Death: Abx= 0 Control= 1
Ramsdale et al Cloxacillin 1 g with amoxicillin 1 g IV 1 hr before and ampicillin/flucloxacillin by mouth 500 mg q6h for 48 hrs
N= 500Abx= 244Control= 256
NA (3‐12) Infection: Abx= 2 Control= 1Death: Abx= 19 Control= 15
Antibiotic Prophylaxis for Pacemakers
Bluhm et al Flucloxacillin 2 g IV 1 hr before and 1 g by mouth q8h for 5 days
N= 106Abx= 52Control= 54
NA (7‐35) Infection: Abx= 0 Control= 0Death: Abx= 1 Control= 1
Glieca et al Cefazolin 4 g IV daily for 5 days N= 200Abx= 100Control= 100
NA Infection: Abx= 0 Control= 12Death: Abx= 0 Control= 0
Mounsey et al Flucloxacillin 1 g IV before, 500 mg by mouth q6h for 48 hrs
N= 473Abx= 224Control= 249
19 (9‐26) Infection: Abx= 0 Control= 9Death: Abx= 0 Control= 0
Da Costa, et al. Circulation. 1998;97:1796‐1801.
8/29/2012
2
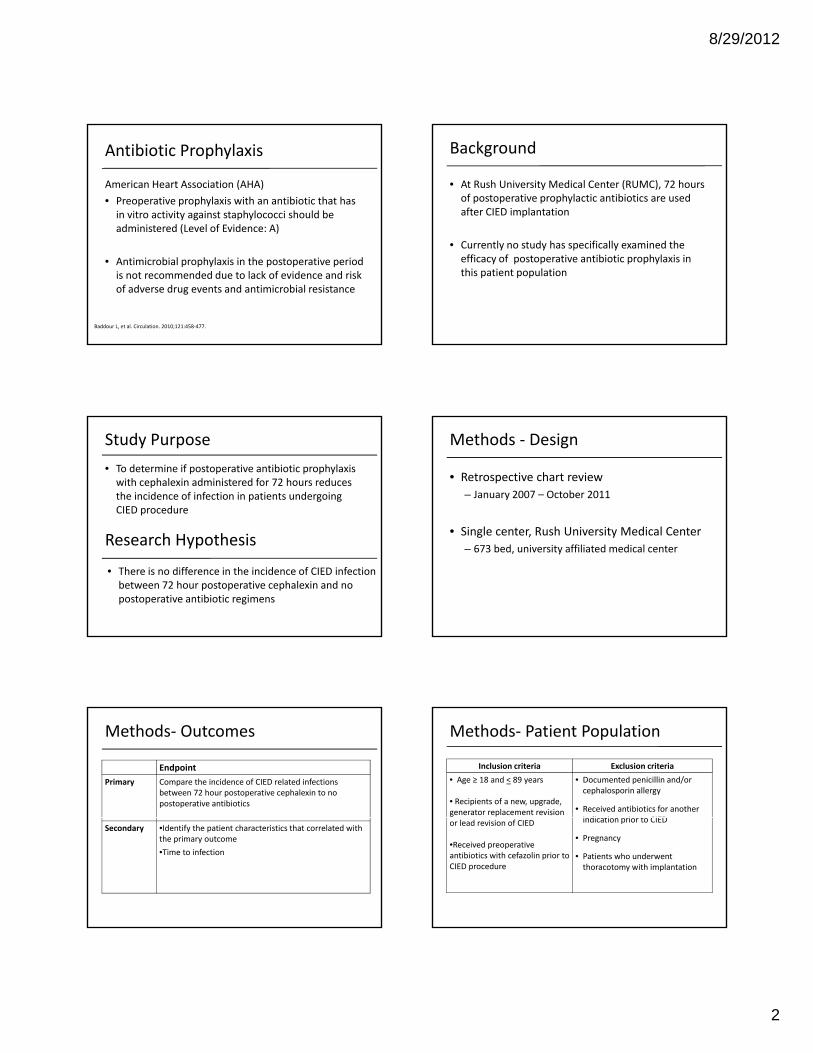
Antibiotic Prophylaxis
American Heart Association (AHA)• Preoperative prophylaxis with an antibiotic that has in vitro activity against staphylococci should be administered (Level of Evidence: A)
• Antimicrobial prophylaxis in the postoperative period is not recommended due to lack of evidence and risk of adverse drug events and antimicrobial resistance
Baddour L, et al. Circulation. 2010;121:458‐477.
• At Rush University Medical Center (RUMC), 72 hours of postoperative prophylactic antibiotics are used after CIED implantation
Background
• Currently no study has specifically examined the efficacy of postoperative antibiotic prophylaxis in this patient population
• To determine if postoperative antibiotic prophylaxis with cephalexin administered for 72 hours reduces the incidence of infection in patients undergoing CIED procedure
Study Purpose
• There is no difference in the incidence of CIED infection between 72 hour postoperative cephalexin and no postoperative antibiotic regimens
Research Hypothesis
• Retrospective chart review– January 2007 – October 2011
Methods ‐ Design
• Single center, Rush University Medical Center– 673 bed, university affiliated medical center
Methods‐ Outcomes
EndpointPrimary Compare the incidence of CIED related infections
between 72 hour postoperative cephalexin to no postoperative antibiotics
Secondary •Identify the patient characteristics that correlated with the primary outcome•Time to infection
Methods‐ Patient Population
Inclusion criteria Exclusion criteria• Age ≥ 18 and < 89 years
• Recipients of a new, upgrade, generator replacement revision
• Documented penicillin and/or cephalosporin allergy
• Received antibiotics for another i di ti i t CIEDor lead revision of CIED
•Received preoperative antibiotics with cefazolin prior to CIED procedure
indication prior to CIED
• Pregnancy
• Patients who underwent thoracotomy with implantation

8/29/2012
3
Methods‐ Data Collection • Demographics
– Age– Gender– Comorbidities– LVEF
• Procedure factors
• Outcomes
– Device Infection
– Cultures
• Culture positive
• Culture negativeProcedure factors – CIED type– Leads – Length of procedure
• Medication – Anticoagulants – Immunosuppressants
• Culture negative
– Time to infection
– Organism identified
• Gram positive
• Gram negative
– Susceptibilities
Patient Population ICD 9 Codes
CIED implants (n=615 )
Inclusion‐Age >18 and < 89 years‐Recipient of new implanted CIED *revised, upgrade, generator replaced
Erx code: cephalexin
Cephalexin x72 hours(n= 155 )
No post‐operative cephalexin(n= 0)
•No preoperative abx or received vancomycin•Documented penicillin and/or cephalosporin allergy •Received antibiotics for another indication•Pregnancy
Exclusion N= 460
Patient CharacteristicsCharacteristics CIED
(n=155)
Age (years), median (IQR) 63 (54‐74)
Male sex, no. (%) 95 (61.3)
Weight (kg), median (IQR) 81.6 (68.9‐97.1)
Ethnicity, no. (%)African American
Caucasian80 (51.6)51 (32 9)Caucasian 51 (32.9)
LVEF (%), median (IQR) 25 (15‐35)SCr (mcg/dL), median (IQR) 1.1 (0.9‐1.4)
Co‐morbidities, no. (%)Atrial fibrillation/flutter
COPDCHF CKD
DiabetesHTN
54 (34.8)32 (20.6)108 (69.7)47 (30.3)49 (31.6)128 (82.5)
Patient CharacteristicsCharacteristics CIED
(n=155)
Length of procedure (mins), median 78:52
Cefazolin preoperative dose (grams), median (IQR) 1 (1‐2)
Cumulative cefazolin (grams), median (IQR) 3 (3‐5)
•New CIED , no. (%)PPM ICD
CRT D
112 (72.3)37(23.9)53(34.2)22( 14 2)CRT‐D 22( 14.2)
•Lead Revision •Upgrade •Generator replacement •Lead revision and Generator replacement
4 (2.6)16 (10.3)15(9.7)8 ( 5.2)
•Temporary pacing wire, no. (%) 11 (7.1)
•Leads placed, no. (%)<2>2
111 (71.6)42 (27.7)
PPM= Permanent pacemaker ICD= implantable cardiac defibrillator CRT‐D= Cardiac resynchronization therapy with defibrillator
Results‐ Infections• Incidence of Infection= 2.6 %Infection (n=4)
Time to infection(days)
Organism Procedure(prior to infection)
Device Treatment
1 28 Culture negative Upgrade CRT‐D‐3 leads
Levofloxacin &clindamycin x14 d
2 48 Culture negative Generatorreplacement
ICD‐2 leads
Vancomycin + piperacillin/tazoreplacement 2 leads piperacillin/tazo
x14 d
3 24 Staphylococcus aureus(MSSA)
Atrial lead revision & generator
replacement
PPM‐2 leads
Cefazolin x14 d
4 128 •Pseudomonasaeruginosa•Klebsiella pneumoniae(pan‐susceptible)
Upgrade ICD‐2 leads
Vancomcyin + Cefepime x14 dLevofloxacin x7 dDuration= 21 d
Results‐ Characteristics of Patients with CIED Infection
Infection (n=4)
Age, yr
Sex DM CKD COPD History of Valverepair
Oral anticoagulant
Immunosuppressant
1 62 M _ _ _ + + _
2 29 M _ _ _ _ _ _
3 85 M + + _ _ + _
4 53 F _ _ + + + _
_ , Absent; +, PresentM= male; F= female

8/29/2012
4
• Dependent on consistency and completeness of medical charts
9 d d d id ifi i f
Study Limitations
• ICD‐9 code dependent identification of patients with new CIED and infection
• Selection and dosing of medications by prescriber bias
19
Conclusion
• Previous studies utilizing only preoperative antibiotic prophylaxis document a 0.5‐1% incidence of infection
• Currently data are insufficient to confidently assess postoperative antibiotic prophylaxis after CIED procedures
• The existing data does not allow definitive recommendations for clinical practice
Future Application
• Vancomycin comparison group
• Review of postoperative antibiotic prophylaxis regimen prior to 2007regimen prior to 2007
• Prospective evaluation of infection rate
Self‐Assessment Questions
Which of the following is recommended by the 2010 American Heart Association Guidelines to prevent CIED infections at time of device implantation?
A. Preoperative antibiotic prophylaxis B. Preoperative and 72 hour postoperative antibiotic
prophylaxis C. 72 hour postoperative antibiotic prophylaxisD. No antibiotic prophylaxis
Self‐Assessment Questions
Common organisms responsible for CIED infections include all of the following, EXCEPT?
A C l ti St h lA. Coagulase‐negative Staphylococcus B. Methicillin resistant Staphylococcus aureusC. Methicillin sensitive Staphylococcus aureusD. Candida species
Residency Project Pearls
Prolonged Antibiotic Prophylaxis After Cardiovascular Implantable Electronic Device Implantation and Its Effect on
Device‐Related Infections Researcher:
Natasha Lopez, PharmD, BCPS
Research Committee:Christopher Crank, PharmD, Ms, AQ‐ID Payal Gurnani, PharmD, BCPS

8/29/2012
1
Residency Project Pearls
From Dabigatran to Warfarin: A Change in Progress
Ashley Jacobs, Pharm.D.Clinical‐Staff PharmacistLutheran Health Network
Fort Wayne, INSeptember 2012
Disclosure: The speaker has no actual or potential conflict of interest in relation to this presentation.
• Warfarin: A vitamin‐K antagonist whose indications include prevention of thromboembolic events in atrial fibrillation
• Dabigatran: A direct thrombin inhibitor
Common Oral Anticoagulants
• Dabigatran: A direct thrombin inhibitor approved to reduce the risk of systemic embolism and stroke in patients with non valvular atrial fibrillation
Warfarin [Prescribing Information]. Haifa Bay, Israel: Taro Pharmaceutical Industries Ltd; 2009. Pradaxa® [Prescribing Information]. Ridgefield, CT: Boehringer Ingelheim Pharmaceuticals, Inc.; 2012.
Dabigatran and Warfarin
Dabigatran Warfarin• Pros
– No routine monitoring requiredS d d d il bl
• Pros– Therapy can be tailored to
patient specific needs– Long history of use– Standard dosages available
• Cons– No antidote available– Post‐marketing reports of
bleeding
Long history of use– Antidote available
• Cons– Routine monitoring required– Difficulty managing unstable
INRs– Bleeding
Heartwire. Available at: http://www.theheart.org/article/1324923.doWarfarin [Prescribing Information]. Haifa Bay, Israel: Taro Pharmaceutical Industries Ltd; 2009.
Pradaxa® [Prescribing Information]. Ridgefield, CT: Boehringer Ingelheim Pharmaceuticals, Inc.; 2012
• The Randomized Evaluation of Long‐Term Anticoagulation Therapy (RE‐LY) study compared dabigatran 110 mg BID and 150 mg BID to dose‐adjusted warfarin
RE‐LY: Warfarin vs. Dabigatran
BID to dose adjusted warfarin– Primary outcome event was stroke or systemic embolism
– Dabigatran 150 mg BID had lower rates of stroke or systemic embolism, but similar rates of major hemorrhage, when compared to warfarin
Connolly SJ, et al. N Engl J Med 2009; 361:1139-51
Adverse Events in the RE‐LY Study
•In the RE-LY study, bleeding and gastrointestinal events (ex: dyspepsia and gastrointestinal hemorrhage) were the most frequent causes of dabigatran treatment
Connolly SJ, Ezekowitz MD, et al. N Engl J Med 2009; 361:1139‐51. Pradaxa® [Prescribing Information]. Ridgefield, CT: Boehringer Ingelheim
Pharmaceuticals, Inc.; 2012.
discontinuation
• Approved in the Fall of 2010 with the following dosing recommendations:
• CrCl >30: 150 mg PO BID• CrCl 15 to 30: 75 mg PO BID
Dabigatran
• CrCl <15 or patients on dialysis: No recommendation can be provided
• In patients 75 years old and older, there is an increased risk for bleeding
Pradaxa® [Prescribing Information]. Ridgefield, CT: Boehringer Ingelheim Pharmaceuticals, Inc.; 2012.Boehringer Ingelheim Pharmaceuticals, Inc. Available at: http://www.pradaxa.com/
8/29/2012
2
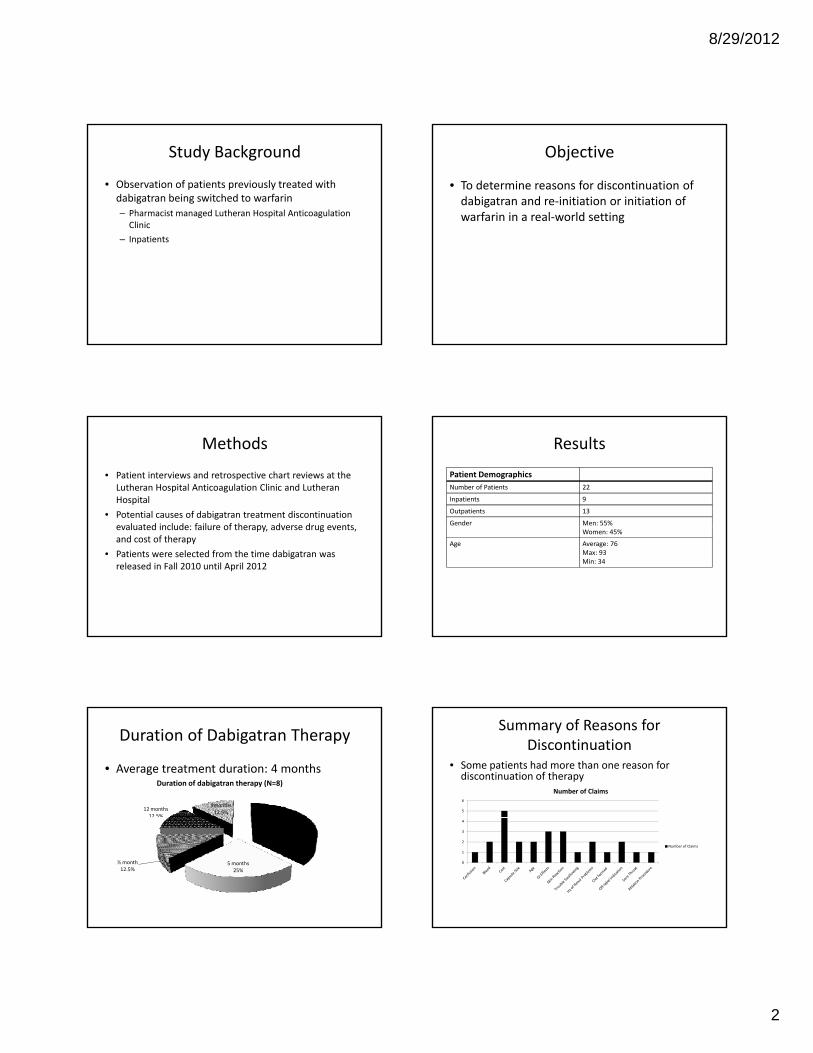
• Observation of patients previously treated with dabigatran being switched to warfarin– Pharmacist managed Lutheran Hospital Anticoagulation Clinic
Study Background
– Inpatients
• To determine reasons for discontinuation of dabigatran and re‐initiation or initiation of warfarin in a real‐world setting
Objective
• Patient interviews and retrospective chart reviews at the Lutheran Hospital Anticoagulation Clinic and Lutheran Hospital
• Potential causes of dabigatran treatment discontinuation evaluated include: failure of therapy adverse drug events
Methods
evaluated include: failure of therapy, adverse drug events, and cost of therapy
• Patients were selected from the time dabigatran was released in Fall 2010 until April 2012
ResultsPatient DemographicsNumber of Patients 22
Inpatients 9
Outpatients 13
Gender Men: 55%Women: 45%
Age Average: 76Max: 93Min: 34
• Average treatment duration: 4 months
Duration of Dabigatran Therapy
1 month12 months12.5%
9months 12.5%
Duration of dabigatran therapy (N=8)
37.5%
5 months25%
½ month12.5%
%
• Some patients had more than one reason for discontinuation of therapy
Summary of Reasons for Discontinuation
5
6
Number of Claims
0
1
2
3
4
Number of Claims
8/29/2012
3
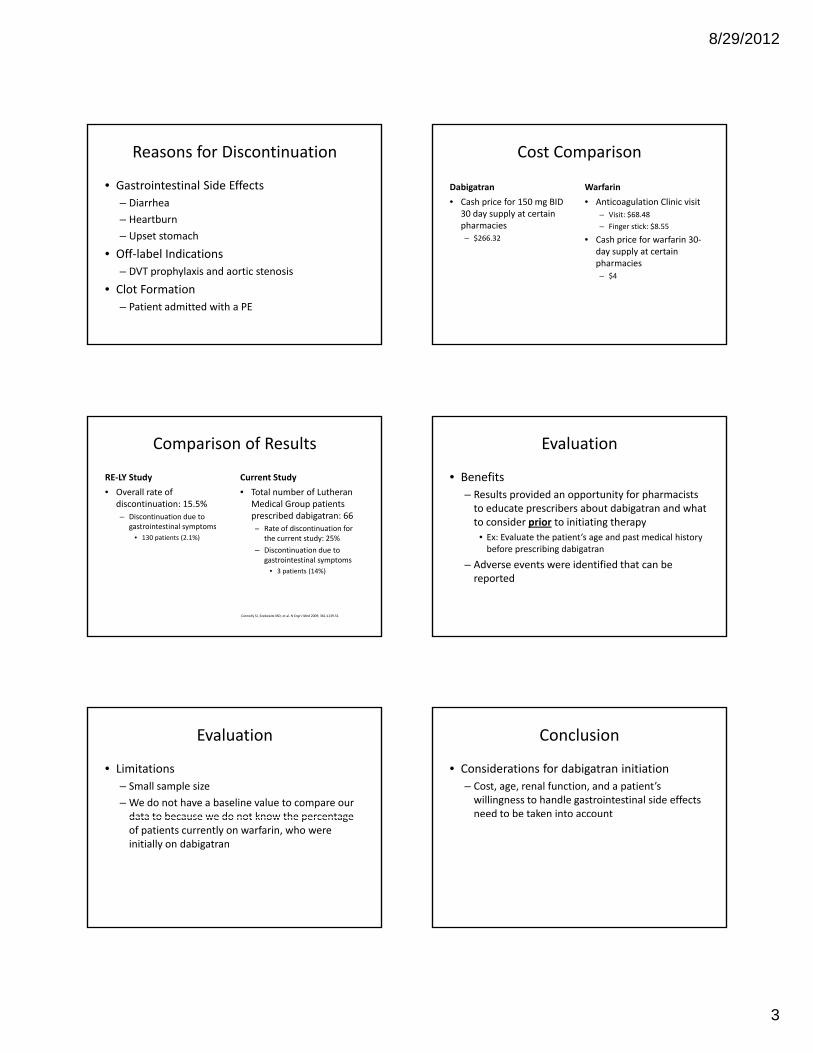
Reasons for Discontinuation
• Gastrointestinal Side Effects– Diarrhea– HeartburnUpset stomach– Upset stomach
• Off‐label Indications– DVT prophylaxis and aortic stenosis
• Clot Formation– Patient admitted with a PE
Cost Comparison
Dabigatran• Cash price for 150 mg BID
30 day supply at certain pharmacies
Warfarin• Anticoagulation Clinic visit
– Visit: $68.48– Finger stick: $8.55
– $266.32 • Cash price for warfarin 30‐day supply at certain pharmacies– $4
Comparison of Results
RE‐LY Study Current Study• Overall rate of
discontinuation: 15.5%– Discontinuation due to
gastrointestinal symptoms
• Total number of Lutheran Medical Group patients prescribed dabigatran: 66
R t f di ti ti fgastrointestinal symptoms• 130 patients (2.1%)
– Rate of discontinuation for the current study: 25%
– Discontinuation due to gastrointestinal symptoms
• 3 patients (14%)
Connolly SJ, Ezekowitz MD, et al. N Engl J Med 2009; 361:1139‐51
• Benefits – Results provided an opportunity for pharmacists to educate prescribers about dabigatran and what to consider prior to initiating therapy
Evaluation
p g py• Ex: Evaluate the patient’s age and past medical history before prescribing dabigatran
– Adverse events were identified that can be reported
• Limitations– Small sample size– We do not have a baseline value to compare our data to because we do not know the percentage
Evaluation
data to because we do not know the percentage of patients currently on warfarin, who were initially on dabigatran
• Considerations for dabigatran initiation– Cost, age, renal function, and a patient’s willingness to handle gastrointestinal side effects need to be taken into account
Conclusion
8/29/2012
4
A patient has a CrCl of 25 mL/min. Which dose of dabigatran should be prescribed for this patient?
– A: 150 mg PO daily – B: 75 mg PO BID – C: 150 mg PO BID – D: Dabigatran is– D: Dabigatran is contraindicated in this patient
A: 150 m
g PO daily
B: 75 mg PO B
ID
C: 150 m
g PO BID
D: Dabigatran is contrai...
0% 0%0%0%
Which organ system is commonly associated with dabigatran side effects?
– A: Respiratory system – B: Endocrine system – C: Excretory system – D: Digestive system– D: Digestive system
A: Respiratory system
B: Endocrine system
C: Excretory system
D: Digestive system
0% 0%0%0%
• 1. MayoClinic. Atrial Fibrillation. Available at: http://www.mayoclinic.com/health/atrial‐fibrillation/DS00291 Accessed November 27, 2011.
• 2. Boehringer Ingelheim Pharmaceuticals, Inc. How AFib can cause a stroke. Available at: https://www.afibstroke.com/blood‐clot‐causes‐stroke.jsp?sc=PRDACQWEBGGLDDG1203103&utm_source=google&utm_medium=cpc&utm_term=afib&utm_campaign=Afib_UnbrandedAccessed April 7, 2012.
• 3. Warfarin [Prescribing Information]. Haifa Bay, Israel: Taro Pharmaceutical Industries Ltd; 2009. • 4. Pradaxa® [Prescribing Information]. Ridgefield, CT: Boehringer Ingelheim Pharmaceuticals, Inc.; 2012.• 5. Connolly SJ, Ezekowitz MD, Yusuf S, et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med 2009;
References
y g p g361:1139‐51.
• 6. Boehringer Ingelheim Pharmaceuticals, Inc. Pradaxa. Available at: http://www.pradaxa.com/ Accessed April 7, 2012.
http://www.vietvaluetravel.com/blog/2012/02/21/most‐asked‐questions‐about‐vietnam/
Residency Project Pearls
From Dabigatran to Warfarin: A Change in Progress g g
Ashley Jacobs, Pharm.D.Clinical‐Staff PharmacistLutheran Health Network
Fort Wayne, INSeptember 2012
Disclosure: The speaker has no actual or potential conflict of interest in relation to this presentation.
8/29/2012
1
Residency Project Pearls
Extended Stability of Intravenous Acetaminophen in Syringes and Opened
Glass Bottles
J if L K i k ki Ph DJennifer L. Kwiatkowski, Pharm.D.Pediatric Specialist at St. John’s Hospital, Springfield, ILSeptember 2012
Great Lakes Presentation from PGY2 Pediatric Pharmacy Residency at the University of Michigan
The speaker has no actual or potential conflict of interest in relation to this presentation.
• Unable to tolerate oral or rectal drug administration
• Potential reduction in opioid or NSAID related
Therapeutic Uses
adverse effects
• Insufficient response to IV opioids or NSAIDs
• Contraindication to IV NSAIDs
Babl FE et al. Pediatr Emerg Care. 2011;27(6):496‐9.
• Intravenous acetaminophen approved for use in Europe in 2001
• Marketed in over 80 countries
Drug Development
• Food and Drug Administration (FDA) approved in November 2010
Jahr JS et al. Anesthesiol Clin. 2010;28(4):619‐45.
• Limited water solubility
– Higher at room temperature compared to refrigeration
Product Formulation
• Stability in aqueous solution
Martindale 35th ed. 2007. Koshy KT et al. J Pharm Sci. 1961;50:113‐8.
Aqueous Decomposition
Acetaminophen
p‐aminophenol and acetic acid
Hydrolysis
p‐benzoquinoneime
p‐benzoquinoneKoshy KT et al. J Pharm Sci. 1961;50:113‐8.Menezes HA et al. J Electroanal Chem. 2006; 586(1):39‐48.
Oxidation
Hydrolysis
• Target pH 5‐6– Reported half life 19‐22 years
• Acidic environment– Reported half life <1 year at pH 2
Influence of pH
p y p
• Basic environment– Reported half life 2 years at pH 9
• Product formulation– Sodium hydroxide or hydrochloric acid with buffer dibasic sodium phosphate
Koshy KT et al. J Pharm Sci. 1961;50:113‐8.Ofirmev package insert. Cadence; 2010.

8/29/2012
2
• Cysteine hydrochloride: antioxidant
• Nitrogen gas in vial to reduce oxidation
• Mannitol: isotonicity
Excipients
Mannitol: isotonicity
• No preservatives
Ofirmev package insert. Cadence; 2010.Rowe RC et al. Handbook of pharmaceutical excipients. 5th ed. 2006. Schmitt E et al. EJHP 2003 6:96‐102.
• Intravenous acetaminophen supplied as 1 gram, 100 mL bottle with 6‐hour usage guideline
Usage Guideline
Ofirmev package insert. Cadence; 2010.
Which of the following is a limitation of the current 6‐hour usage guideline for intravenous acetaminophen?
A. Potential for infusion related reactions due to administration guidelines
B. Potential for dosing errors when dispensing the 1000 mg bottle of intravenous acetaminophen
Audience Question
C. Potential for increased cost in adult patients receiving a 1000 mg dose of intravenous acetaminophen
D. Potential for product waste for pediatric patients who require only a portion of the 1000 mg bottle
• Weight‐based dosing
• Use of a fraction of the bottle
• Product waste
Pediatric Limitations
Product waste
• Increased costs
• Disruption in pharmacy workflow
• USP 797 guidelines for sterile compounding• Low‐risk level
– Sterile for 48 hours at room temperatureA i i l i i hi ISO Cl i
Beyond Use Dating
– Aseptic manipulations within ISO Class 5 air quality or better
– Institutional specifications for final dating
USP <797> Guidebook to Pharmaceutical Compounding—Sterile Preparations.
Extended Stability of Intravenous Acetaminophen in Syringes and Opened Glass Bottles
Jennifer Kwiatkowski, PharmDCary Johnson, Pharm.D., FASHPDeb Wagner, Pharm.D., FASHPUniversity of Michigan Hospitals and Health Centers
8/29/2012
3
• Specific aim – Determine if intravenous acetaminophen is stable over an 84 hour time period over a range of doses stored in syringes and a range of volumes remaining in the original opened bottle
Specific Aim
opened bottle
• Hypothesis– Intravenous acetaminophen will maintain at least 90% of the original concentration over an 84 hour time period at room temperature
High Performance Liquid Chromatography (HPLC)
http://www.comsol.com/stories/waters_corp_hplc_systems/full
• Stationary phase
– C‐18 reverse phase column
– 5‐µm particle size (250 mm x 4.6 mm)
HPLC Components
µ p ( )
• Mobile phase
– Mixture of acetonitrile and deionized‐distilled water (20:80 v/v) containing 0.15% formic acid
Acetaminophen. USP 34 NF 29.
• UV light detector– λ set at 243 nm
• Flow rate– 1 mL/min
Sample Detection
1 mL/min
• Samples – Diluted to 50 µg/mL expected concentration with mobile phase
– Prepared in triplicate, each sample assayed in duplicate
AJHP 2000;57:1150‐69.
• Analytical grade acetaminophen powder
• 5‐point standard curve
– 40, 45, 50, 55, 60 µg/mL
Acetaminophen Standard Curve
40, 45, 50, 55, 60 µg/mL
• Standard was run after every 10th assay sample as an external control
According to ASHP guidelines for conducting a drug stability experiment, drug samples must be assayed how many times?
A Once
Audience Question
A. OnceB. TwiceC. Three timesD. Four times

8/29/2012
4
• Intravenous acetaminophen supplied as 10 mg/mL, 100 mL bottle
• Doses in syringes (triplicate)– 100 mg (10 mL in 10 mL syringe)
Sample Preparation
100 mg (10 mL in 10 mL syringe)– 250 mg (25 mL in 30 mL syringe)– 500 mg (50 mL in 60 mL syringe)
• Volumes in original opened bottle (triplicate)– 250 mg (25 mL in bottle)– 900 mg (90 mL in bottle)
• Visually inspected for color change and precipitate formation
• pH measured
Sample Analysis
• Microbiological testing not performed
• Forced decomposition of intravenous acetaminophen– 3% hydrogen peroxide1 N sodium hydroxide (pH 12)
Stability‐Indicating Assays
– 1 N sodium hydroxide (pH 12)– 1 N hydrochloric acid (pH 2)
• Procedure– Heat to 90ºC for 2 hours– Neutralized to pH 7
Sample Acetaminophen Chromatogram
Results
Acetaminophen peakAcetaminophen peak at 4.05 minutes
Time
HPLC Peak Height
Results
y = 131692.3000x + 1067843.7000R² = 0.9996
Results
DegradationSolution
Degradation Peaks (minutes)
Acetaminophen Degradation (%)
3% hydrogen 2 46 5
Stability-Indicating Capability of HPLC Assay
peroxide 2.46 5
1 N hydrochloric acid (pH 2) 2.70, 6.08, 7.35 8
1 N sodium hydroxide (pH 12) 2.64, 5.23, 7.35 25
Acetaminophen peak: 4 minutesp‐aminophenol peak: 7.35 minutes

8/29/2012
5
Stability of Intravenous Acetaminophen (10 mg/mL) at Room Temperature in Varying Storage Containers
Sample Actual Initial Drug
Concentrationa
(mg/mL)
% Initial Concentration Remaining24 hours 48 hours 72 hours 84 hours
100 mg(syringe) 9.94 ± 0.05 99.11 ± 0.52 100.54 ± 0.69 100.08 ± 0.38 100.02 ± 0.53
250 mg(syringe) 9.96 ± 0.02 99.66 ± 1.11 99.61 ± 0.68 99.83 ± 0.89 99.80 ± 0.35
500 mg(syringe) 9.96 ± 0.03 100.13 ± 0.37 99.83 ± 0.64 99.92 ± 058 99.68 ± 0.55
250 mg(bottle) 9.98 ± 0.03 99.67 ± 0.36 100.07 ± 1.26 99.37 ± 0.24 99.53 ± 0.41
900 mg(bottle) 9.93 ± 0.04 99.76 ± 0.33 100.03 ± 0.59 100.54 ± 0.58 100.31 ± 1.22
aMean ± S.D. of duplicate determinants for three samples (n = 3).
• No detectable change in sample color
• No visible drug precipitation
• No appreciable change in the initial pH (5.77 ± 0.02)
Results
• Interday coefficient of variation: 1.8%
• Intraday coefficient of variation: 1%
• Intravenous acetaminophen (10 mg/mL) was physically and chemically stable in a range of volumes for up to 84 hours in the opened bottles and in polypropylene syringes
Conclusion
• Benefits of extending the stability of intravenous acetaminophen
– Decreased product waste
Significance
– Cost savings to patients and the healthcare system
– Pharmacy workflow optimized by minimizing need for urgent dose preparation
1. Babl FE, Theophilos T, Palmer GM. Is there a role for intravenous acetaminophen in pediatric emergency departments? Pediatr Emerg Care. 2011;27(6):496‐9.
2. Jahr JS, Lee VK. Intravenous acetaminophen. Anesthesiol Clin. 2010;28(4):619‐45.
3. Martindale – The Complete Drug Reference. 35th ed. London: Pharmaceutical Press; 2007.
References
4. Koshy KT, Lach JL. Stability of aqueous solutions of N‐acetyl‐p‐aminophenol. J Pharm Sci. 1961;50:113‐8.
5. Menezes HA, Maia G. Films formed by the electrooxidation of p‐aminophenol (p‐APh) in aqueous medium: What do they look like? J Electroanal Chem. 2006; 586(1):39‐48.
6. OFIRMEV (intravenous acetaminophen) package insert. San Diego, CA: Cadence Pharma; 2010 Nov.
7. Rowe RC, Sheskey PJ, Owen SC. Handbook of pharmaceutical excipients. American Pharmacists Associations. 5th ed. London; Pharmaceutical Press; 2006.
8. Schmitt E, Vainchtock A, Nicoloyannis N et al. Ready to use injectable paracetamol: easier, safer, lowering workload and costs. EJHP 2003 6:96‐102.
9. USP <797> Guidebook to Pharmaceutical Compounding— Sterile
References
Preparations. The United States Pharmacopeia, 34th revision, and The National Formulary, 29th ed. Rockville, MD: United States Pharmacopeial Convention; 2010:336‐73.
10. ASHP guidelines on quality assurance for pharmacy‐prepared sterile products. American Society of Health System Pharmacists. Am J Health Syst Pharm. 2000;57(12):1150‐69.
11. Acetaminophen. The United States Pharmacopeia, 34th revision, and The National Formulary, 29th ed. Rockville, MD: United States Pharmacopeial Convention; 2010:1720‐3.

8/29/2012
6
Questions? Residency Project Pearls
Extended Stability of Intravenous Acetaminophen in Syringes and Opened
Glass BottlesJennifer L. Kwiatkowski, Pharm.D.Pediatric Specialist at St. John’s Hospital, Springfield, ILSeptember 2012
Great Lakes Presentation from PGY2 Pediatric Pharmacy Residency at the University of Michigan
32