prognostic implication of the p53 protein and ki-67 antigen immunohistochemistry in malignant...
TRANSCRIPT

618
Prognostic Implication of the p53 Protein and Ki-67 Antigen lmmunohistochemistry in Malignant Fibrous Histiocytoma Peng Yang, M.D.,*,t Takanori Hirose, M.D.,* Tadashi Hasegawa, M.D.,* Kunihiko Seki, M.D.,* Toshiaki Sano, M.D.,* and Kazuo Hizawa, M.D.*
Background. Mounting evidence indicates that p53 regulates cell growth and abnormal p53 immunopheno- typic expression is associated with an unfavorable prog- nosis for patients with some types of carcinoma. The prognostic significance of p53 overexpression in malig- nant fibrous histiocytomas (MFHs) of soft tissue has not yet been elucidated.
Methods. Expressions of p53 protein and Ki-67 anti- gen in 54 primary MFHs of soft tissue were investigated immunohistochemically and indexed quantitatively by counting the number of immunoreactive nuclei versus the total neoplastic nuclei in the representative fields of each tumor to evaluate their prognostic implications and interrelations with other clinicopathologic parameters.
Results. The percentages (labeling indices [LIs]) of p53 and Ki-67-immunoreactive nuclei versus the total neoplastic nuclei were 0.1-93.Z0/0 (mean + standard devi- ation [SD], 40.6% k 21.8%) and 5.3-90.8% (mean k SD, 42.7% f 29.4%), respectively. The Ki-67 LI correlated with histologic grade (P = 0.01498), primary tumor size (P = 0.04985), disease free interval (reverse correlation, P =
0.00776), and recurrence and metastasis (P = 0.00360). The p53 LI correlated with primary tumor size (P = 0.00431) but did not show any significant correlation with histologic grade, Ki-67 LI, primary tumor size, disease free interval, or recurrence and metastasis. Other sig- nificant correlations included histologic grade and dis- ease free interval (P = O.OOo~O), primary tumor size and disease free interval (reverse correlation, P = 0.00869), histologic grade and recurrence (P = 0.02714), and pri- mary tumor size and primary tumor location ( P = 0.00028). In the grouped survival analysis, patients with
From the 'First Department of Pathology, University of Tok- ushima School of Medicine, Tokushima, Japan; tVisiting Doctor from Department of Pathology. Shandong Provincial Qianfoshan Hospi- tal, Jinan, Shandong, China.
Address for reprints: Kazuo Hizawa, M.D., First Department of Pathology, University of Tokushima School of Medicine, Tokushima 770, Japan.
Received March 30,1995; accepted April 20,19Y5.
recurrence or metastasis or with tumors of larger size (27 cm), high histologic grade, or higher Ki-67 LI (>25%) had a significantly reduced survival (P < 0.05). The different p53 immunohistochemical expression and the different histologic types did not reflect different cumulative sur- vival (P > 0.05). Regression analysis revealed that the pri- mary tumor size and histologic grade, but not Ki-67 or p53 LIs, were independent statistical variables for prognosti- cation.
Conclusions. These results indicate that (1) primary tumor size and histologic grade are two important prog- nostic factors, (2) Ki-67 LI should be used in adjunct with other main prognostic factors for patients with MFHs, and (3) nuclear p53 overexpression in MFHs of soft tissue is a comparatively common event that has no prognostic implication. Cancer 1995; 76:618-25.
Key words: malignant fibrous histiocytoma, prognosis, p53 protein, Ki-67 antigen, immunohistochemistry.
The p53 gene, located on the region of chromosome 17~13.1, encodes a protein product that is required to restrain cell growth. In vitro studies revealed that under y-irradiation or actinomycin-D inhibition of DNA syn- thesis, cells showed accumulation of p53 protein in nu- clei that correlated with cell arrest in G , phase.' Consis- tent with this finding, Lane' proposed that p53 regu- lates the cell growth cycle by activating transcription of genes that cause arrest in GI phase when the genome is damaged. The regulatory function may be lost by dele- tion of both wild-type alleles or by a dominant mutation in one allele. In the latter event, the dysfunction may be of dominant negative type when the mutant protein overrides the function of wild-type protein; alterna- tively, p53 mutation may result in production of mutant protein, which functions as a tumor pr~moter .~ Muta- tions of the p53 gene result in the production of mutant protein that loses its tumor-suppressing property and

p53 and Ki-67 in Malignant Fibrous Histiocytoma/Yang et al. 619
holds a prolonged half-life (4 hours) that permits im- munohistochemical de te~t ion .~ ,~ Recent studies indi- cated that p53 abnormalities existed among a large va- riety of human malignan~ies~,~ and were associated with an unfavorable prognosis of patients with colon and breast carcinoma^.',^
Although several investigations showed that p53 abnormalities existed in 19-36% of malignant fibrous histiocytomas (MFHs),"-13 the prognostic significance of p53 overexpression in MFHs has not been elucidated. A few previous studies evaluated the prognostic sig- nificance of Ki-67 antigen in MFHs and yielded contro- versial These data prompted us to perform the current study of MFHs of soft tissue, using a novel antibody, D07, which recognizes an epitope on the amino acids 35-45 of the N-terminus of both wild and mutant p53 protein and was found to be superior to other similar antibodies in detecting mutant protein.I6 We analyzed the immunohistochemical expressions of the p53 protein and Ki-67 antigen in MFHs of soft tissue and their interrelations with patient prognosis and other established clinicopathologic parameters.
Materials and Methods
The study population consisted of 54 patients with MFHs of soft tissue registered in the First Department of Pathology, University of Tokushima School of Med- icine. All the tumor specimens were obtained at the ini- tial surgical excision of primary tumors and fixed in 10% neutral formalin. The original pathologic materials from each case were reviewed for diagnostic conformation to the known diagnostic riter ria.'^ For computerized sta- tistical analysis of the interrelations between the histo- logic grade and other parameters used in the study, a 9- point scoring system was developed to reflect quantita- tively the histologic grade of each primary tumor. The score is recorded according to the cellularity (1 point, low cellularity; 2 points, moderate cellularity; 3 points, high cellularity), the nuclear pleomorphism (1 point, uniform spindle nuclei; 3 points, greatly varied nuclei; otherwise, 2 points), and the mitotic activity (1 point, 0- 9; 2 points, 10-19, 3 points, 20 or more mitotic figures per 10 high-power fields) of each tumor,
For optimal detection of the p53 protein and Ki-67 antigen, representative tissues displaying the maximal score for the histologic grade were chosen for immuno- staining. Paraffin sections of 4-pm thickness were de- paraffinized, rehydrated in graded alcohol, inhibited for endogenous peroxidase activity in 0.03% hydrogen per- oxide (H202) in methanol, and antigenetically retrieved in a microwave oven for 10 minutes at 9OoC as de- scribed.18 Sections were then incubated with normal goat serum for 20 minutes at room temperature, pri-
mary antibodies against p53 protein (D07, immuno- globulin G, 1:25, Dako Corp., Glostrup, Denmark) and Ki-67 antigen (MIB1,immunoglobulin G, 1 : 100, Immu- notech S.A., Maseille, Cedex, France) for 12-18 hours at 4OC, biotinylated rabbit antimouse immunoglobulin G for 45 minutes at room temperature, and avidin-bio- tinylated horseradish peroxidase complex (Vector Lab- oratories, Burlingame, CA) for 50 minutes at room temperature. Sections were washed thoroughly in phosphate buffered saline between each of the immu- nostaining procedures. Final reaction product was visu- alized with diaminobenzidine (Sigma, St. Louis, MO). After immunohistochemical reactions, sections were counterstained with hematoxylin for nuclear detection. Positive and negative controls were performed in each batch of the staining. For positive controls, neoplastic tissues known to be positive for p53 were used. For neg- ative controls, primary antibody was substituted with phosphate buffered saline in duplicate sections.
Immunohistochemical results were interpreted ac- cording to the intensity of immunoreactive product in nuclei of tumor cells. Any definite nuclear immuno- staining was considered to be positive. To obtain the percentages (labeling indexes) of p53 and Ki-67-immu- noreactive nuclei versus the total neoplastic nuclei in a tumor, five color microphotos at a 200x magnification in each tumor were taken from the unoverlapped rep- resentative fields (displaying the highest degree of im- munoreactivity). For statistical analysis, the labeling in- dexes for p53 and Ki-67 expressions were obtained by counting the number of positive nuclei versus the num- ber of the total neoplastic nuclei. The ungrouped quan- titative values of p53 and Ki-67 labeling indexes were entered into correlation and regression analyses. The values entering into grouped p53 and Ki-67-related sur- vival analysis were stratified at 10% and 25% of p53 and Ki-67 labeling indexes, respectively, considering the fact that some benign fibrous lesions could have a low percentage of immunoreactive cells."
For the other grouped survival comparison, the fol- lowing paired subgroups were divided and compared statistically: storiform-pleomorphic MFHs and myxoid MFHs, tumors of the extremities and tumors of the trunk and retroperitoneal region, tumors larger than or equal to 7 cm and tumors smaller than 7 cm, the high histologic grade (scored 2 7 points) and the low histo- logic grade (scored <7 points), patients without recur- rent disease and patients with recurrent diseases, pa- tients without metastatic disease and patients with met- astatic diseases, patients with neither recurrent nor metastatic disease and patients with recurrent and/or metastatic diseases.
Statistical correlation between independent vari- ables was tested by Kendall tau analysis, which does not
620 CANCER August 15,2995, Volume 76, No. 4
require normal distribution.” Survival curve of overall survival distribution was plotted by Kaplan-Meier product limit method.” Prognostic significance of difference between grouped distributions was analyzed by Gehan’s generalized Wilcoxon test.” Comparative statistical prognostic significance of variables was deter- mined by a multivariate regression analysis using Cox’s proportional hazards model.” Probability value P < 0.05 is considered statistically significant.
Results
Clinicopathologic Features
The study involved 28 men and 26 women, age 32-95 years (median age, 64.5 years). The tumors were mea- sured from 2 to 22 cm (median, 10.5 cm) and located in the lower extremities (n = 30), trunk (n = 9), retroperi- toneal region (n = 7), upper extremities (n = 6), and head and neck region (n = 2). Histologic subclassifica- tion included storiform-pleomorphic (n = 40), myxoid (n = 9), giant cell (n = 3), and inflammatory (n = 2) types of MFHs. Thirty-seven of 54 (68%) tumors were classified as high histologic grade, with the designated score of 7, 8, or 9. The follow-up time expanded from 2 to 174 months (median, 40.8 months). The disease free interval was from 3 to 70 months (median, 20.1 months). At the conclusion of the study, 9 patients were alive without disease, 10 patients were alive with dis- ease, 3 patients died of unrelated diseases, and 32 pa- tients died of the diseases. The 5- and 10-year survival rates were 37% and 24%, respectively. Twenty-one of 50 (42%) patients had recurrent diseases, 21 of 50 (42%) patients had metastatic diseases, and 36 of 50 (72%) pa- tients had recurrent and/or metastatic diseases.
Immunohistochemistry
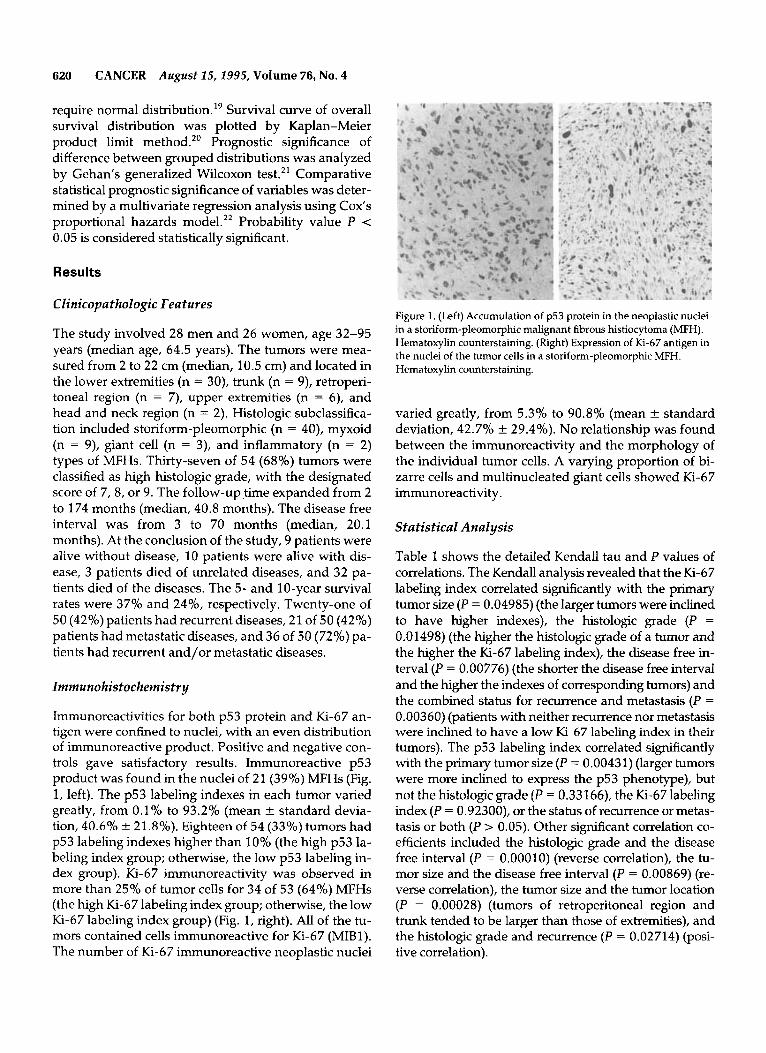
Immunoreactivities for both p53 protein and Ki-67 an- tigen were confined to nuclei, with an even distribution of immunoreactive product. Positive and negative con- trols gave satisfactory results. Immunoreactive p53 product was found in the nuclei of 21 (39%) MFHs (Fig. 1, left). The p53 labeling indexes in each tumor varied greatly, from 0.1% to 93.2% (mean f standard devia- tion, 40.6% k 21.8%). Eighteen of 54 (33%) tumors had p53 labeling indexes higher than 10% (the high p53 la- beling index group; otherwise, the low p53 labeling in- dex group). Ki-67 immunoreactivity was observed in more than 25% of tumor cells for 34 of 53 (64%) MFHs (the high Ki-67 labeling index group; otherwise, the low Ki-67 labeling index group) (Fig. 1, right). All of the tu- mors contained cells immunoreactive for Ki-67 (MIB1). The number of Ki-67 immunoreactive neoplastic nuclei
Figure 1. (Left) Accumulation of p53 protein in the neoplastic nuclei in a storiform-pleomorphc malignant fibrous histiocytoma (MFH). Hematoxylin counterstaining. (Right) Expression of Ki-67 antigen in the nuclei of the tumor cells in a storiform-pleomorphic MFH. Hematoxylin counterstaining.
varied greatly, from 5.3% to 90.8% (mean f standard deviation, 42.7% f 29.4%). No relationship was found between the immunoreactivity and the morphology of the individual tumor cells. A varying proportion of bi- zarre ceIls and multinucleated giant cells showed Ki-67 immunoreactivity .
Statistical Analysis
Table 1 shows the detailed Kendall tau and P values of correlations. The Kendall analysis revealed that the Ki-67 labeling index correlated significantly with the primary tumor size (P = 0.04985) (the larger tumors were inclined to have higher indexes), the histologic grade (P = 0.01498) (the higher the histologic grade of a tumor and the higher the Ki-67 labeling index), the disease free in- terval (P = 0.00776) (the shorter the disease free interval and the higher the indexes of corresponding tumors) and the combined status for recurrence and metastasis (P =
0.00360) (patients with neither recurrence nor metastasis were inclined to have a low Ki-67 labeling index in their tumors). The p53 labeling index correlated significantly with the primary tumor size (P = 0.00431) (larger tumors were more inclined to express the p53 phenotype), but not the histologic grade (P = 0.33166), the Ki-67 labeling index (P = 0.92300), or the status of recurrence or metas- tasis or both (P > 0.05). Other significant correlation co- efficients included the histologic grade and the disease free interval (P = 0.00010) (reverse correlation), the tu- mor size and the disease free interval (P = 0.00869) (re- verse correlation), the tumor size and the tumor location (P = 0.00028) (tumors of retroperitoneal region and trunk tended to be larger than those of extremities), and the histologic grade and recurrence (P = 0.02714) (posi- tive correlation).

Tab
le 1
. Ken
dall
Cor
rela
tion I
and
PV
alue
s B
etw
een
the
Var
iabl
es T
este
d in
the
Stud
v*
Ken
dall
7
and
P va
lue
Typ
e L
ocat
ion
Size
G
rade
R
ecur
renc
e M
etas
tasi
s R
eMe
P53
K
i67
Loca
tion
Size
Gra
de
Rec
urre
nce
Met
asta
sis
ReM
e
P53
Ki-6
7
Dis
ease
-fre
e in
terv
al
7 P 7 P P P P 7
7
7
7 P 7 P P 7 T P
0.05
786
(-)
0.53
677
0.21
458
0.07
433
0.50
566
0.07
965
0.41
439
0.10
319
(-)
0.29
030
0.54
354
0.02
235
0.8 2
2 6 8
0.08
493
(-)
0.38
929
0.05
592
0.55
047
0.06
234
(-)
0.05
928
(-)
0.43
645
(-)
0.00
028t
0.
0038
7 (-
) 0.
9670
7 0.
0281
5 0.
7730
2 0.
1576
5 0.
1062
3 0.
0216
0 0.
8248
6 0.
1496
7 (-
) 0.
1136
4 0.
0809
6 (-
) 0.
3874
2 0.
0443
6
0.04
424
0.71
293
0.05
526
(-)
0.66
228
0.09
444
0.45
538
0.07
157
(-)
0.54
354
0.33
784
0.00
431t
0.
2321
0 0.
0498
5t
0.31
549
(-)
0.21
561
0.02
714t
0.11
286
0.01
871
0.84
794
0.11
673
(-)
0.33
166
0.22
790
0.01
498t
0.
3644
0 (-
)
0.15
472
(-)
0.16
537
(-)
0.09
015
0.17
331
0.07
574
0.1 1
752
0.22
360
0.05
062
0.05
538
0.12
525
0.57
456
0.20
422
0.03
673
(-)
0.35
007
0.00
915
(-)
0.70
661
0.00
360t
0.
9230
0 0.
0294
3 (-
) 0.
0338
2 0.
1788
4 0.
4198
2 (-
) 0.
6039
3 ~ .. . .
0.63
582
0.00
869t
0.
0001
0t
.
~~~
~ 0.
7289
3 0.
8851
6 0.
0077
67
0.76
292
Type
: 1 =
stor
ifor
m-p
leom
orph
ic M
HFs
; 2 =
myx
oid
mal
igna
nt fi
brou
s his
tiocy
tom
a (M
FH);
Loc
atio
n: 1
= tu
mor
s of
trun
k an
d re
trop
erito
neal
reg
ion;
2 =
tum
ors
of ex
trem
ities
; ReM
e: 1
= p
atie
nt s
tatu
s of
havi
ng
neith
er re
curr
ence
nor
met
asta
sis;
2 =
recu
rren
ce or
met
asta
sis o
nce;
3 =
recu
rren
ce o
r met
asta
sis
twic
e, e
tc. T
he n
umbe
rs e
nter
into
the
Ken
dall
corr
elat
ion.
(-):
rev
erse
cor
rela
tion.
t S
tatis
tical
ly s
igni
fican
t cor
rela
tion.

622 CANCER August 25,2995, Volume 76, No. 4
KAPLAN-MEIER METHOD GEHANS TEST GEHAN'S TEST
.8 : ........................... i . .:. ........I .......
.7 . . ..:. ....... 1... ..... : ...............
.6,, ~ . . . . . . . . . . . . .
.s ; i.. ,~~ i~~ ...,......
.4 ; ....... i ..............
.3j . . . j - I ! . 2 . . .
. 2 / . . . , , < i . ! . . ! . b ...+
. I ; . . . . , + . ! . * . . . . . . . . 0 : . . . . . . . . ..i .... : . . . . . . .
o m 40 M 80 100. 120 140 IM 180
. . . . . . . . , . . . . . . . . . . . . ....... , . . , , . .
, . .
. . . . I : '
. . , . . , . .
...... ...... .... ...........
~ . . . . . . . . . . . . . . .........
...... .............. ...... ..... M . . ...........
..... ..... 10
. . .... i i . i ..: , 2-21.111 59.333 97X4 131.78 174
40.222 78A44 116.67 1S4.89
. .! ...] ...! ....... i ........... 90 ..., < ..... , 4 ~ , , S ? . W . j
.......
....
...... ........
L : .... 2 21.111 59.333 97.556 135.78 174
40.222 78.444 11667 154.89
GEHAN'S TEST GEHANS TEST GEHAN'S TEST
. 10
0
10 L- YL- 1 ot&o~-rk.mnm7cy&-' 1
2 21 111 59333 97.556 13578 174 221111 59333 97556 13578 174 40222 70444 11667 15489 40222 7 8 W 11667 15489
GEHAN'S TEST
70 I..
.... ...... ....
..........
10
2 21.111 59.333 W.556 135.78 174 40.222 78.444 11667 lS4.89
GEHAN'S TEST
2 21.111 59.333 97.556 135.78 174 40.222 78444 116.67 154.89
.I .. -...... ............. : I . . : L .- . .................. . . .+\i , . .
..: \ + i . :..i . .* ... d . . . . . ;..id& ...... j ..... ................. i.. i ...... ......
, . . ...................
, . I ,
........ ........... ......... .... ........ . . . . . . . . ..,...... ~. ...... .....
. . 2 21.111 59.333 97.556 135.78 174
40222 78.444 116.67 154.89
Figure 2. X axis represents follow- up time (months), with the digits indicating interval beginning; Y axis represents proportion survival. (Top left) The overall survival of this cohort of patients with malignant fibrous histiocytomas (MFHs) of soft tissue. (Top middle) Patients in the p53 positive group and negative group have no significant difference on cumulative survival. (Top right) Patients in the high Ki- 67 index group have a significantly reduced cumulative survival compared with those in low Ki-67 index group. (Middle left) Patients with tumors greater than or equal to 7 cm have a significantly reduced cumulative survival compared with those with tumors less than 7 cm. (Center) Patients with storiform- pleomorphic MFHs and with myxoid MFHs have no significant Qfference on cumulative survival. (Middle right) Patients with high grade MFHs (scored 7, 8, or 9) have a significantly reduced cumulative survival compared with those with low grade MFHs. (Bottom left) Patients with metastatic MFHs have a significantly reduced cumulative survival compared with those with no metastasis. (Bottom
middle) Patients with recurrence and without recurrence have no sipticant difference on cumulative survival. (Bottom right) Patients with recurrent and/or metastatic MFHs have a sigruficantly reduced cumulative survival compared with those with neither recurrence nor metastasis.
Figure 2 illustrates the overall survival (top left) and the grouped cumulative survivals (top middle through bottom right) with corresponding probability values and group indications. Gehan's generalized Wilcoxon test revealed that patients of the high p53 labeling index group and the low p53 labeling index group had no sig- nificant difference on the cumulative survival ( P = 0.27020) (Fig. 2, top middle). Patients of the high Ki-67 labeling index group had a significantly worse progno- sis than those of the low Ki-67 labeling index group ( P = 0.00008) (Fig. 2, top right). The other prognostic com- parisons included the following: patients with tumors greater than or equal to 7 cm had a significantly reduced cumulative survival compared with those with tumors less than 7 cm (P = 0.00080) (Fig. 2, middle left); pa- tients with storiform-pleomorphic MFHs and with myxoid MFHs had no statistical difference on prognosis ( P = 0.05418) (Fig. 2, center); patients with low histo- logic grade tumors had a better prognosis than patients with high histologic grade tumors (P = 0.00018) (Fig. 2,
middle right); patients without metastatic diseases showed a better prognosis than patients with metastasis (P = 0.02014) (Fig. 2, bottom left); patients with and without recurrent diseases were not significantly different on prognosis (P = 0.20774) (Fig. 2, bottom middle); and patients with tumors of different locations had no significant difference on survival. Patients with- out recurrence and metastasis had a significantly better prognosis than those with either recurrence or metasta- sis or both ( P = 0.03316) (Fig. 2, bottom right).
The multivariate regression analysis based on Cox's proportional hazards model revealed that the primary tumor size and the histologic grade were two statisti- cally significant independent indicators for patient prognosis ( P = 0.00012). The other variables, including the p53 labeling index, Ki-67 labeling index, histologic type, recurrence and metastasis, disease free interval, primary tumor location, and patient age had no inde- pendent significance in the prognostication of the cur- rent cohort of patients (t < 2.0).

p53 and Ki-67 in Malignant Fibrous Histiocytoma/Yung et ul. 623
Discussion
Several previous reports described the p53 and/or Ki- 67 expressions in adult soft tissue sarcoma^.^'-^^,^^ In these studies, the different histologic types of soft tissue sarcomas were mixed together, and only a few of them correlated the p53 and Ki-67 immunophenotypic data with clinicopathologic manifestat i~ns. '~~ ' '~~~ Further- more, to the best of our knowledge, none of these stud- ies performed correlation study using the straight label- ing indexes for p53 and Ki-67 expressions. In the current study, to maximally avoid the possible nonob- jective effect, we analyzed a clinicopathologically well characterized cohort of 54 adult patients with a single type of primary soft tissue sarcoma MFH to test the prognostic effects of the p53 and Ki-67 immunopheno- typic expressions by using the straight labeling index methodology, the 9-point scoring system for histologic grade and the natural values for other clinicopathologic variables. Our results indicate that nuclear p53 accumu- lation is a relatively common immunophenotypical phenomenon in MFHs of soft tissue, being 39% (21 of 54) in the current series, an incidence slightly higher than those reported ( 19-36%).'0-'3 The higher inci- dence seems to be caused by the straight labeling index used in the current study, which is contrasted with the previous studies in which the thresholds of 5-20% were set for the designation of p53 positivity; alternatively, it could be caused by the various antibodies and immu- nostaining methods used in the different studies.
Recently, Latres et al. found in a study of 48 pri- mary, 14 recurrent, and 11 metastatic adult soft tissue sarcomas of diverse histologic types that allelic deletion of 17p and p53 overexpression were common events in adult soft tissue sarcomas, being 53% and 34%, respec- t i~ely. '~ They observed that p53 overexpression oc- curred more often in tumors of high histologic grade, large tumor size and metastasis, but the statistical differences between the positive and negative groups were not significant. Although, like Latres et al.,23 we achieved a similar statistical result, the trends obtained by Latres et al. for p53 prognostic effects contradict the results obtained in the current study; we did not observe any inclination of p53 labeling index correlating with the primary histologic grade, status of recurrence and/ or metastasis, or overall survival using the methodology described above. These discrepancies are perhaps ex- plained by the differences of the antibodies and the methodologies for immunohistochemistry and statisti- cal analysis used in the previous study and the current one. More importantly, the compositions of the two co- horts are different. In the study by Latres et al.,23 52% of patients had either liposarcomas (n = 25) or leiomy- osarcomas (n = 13), and only 12% (n = 9) patients had
MFHs. This difference could be significant, because ei- ther liposarcoma or leiomyosarcoma is tumorigeneti- cally and cytogenetically different from MFH; the latter usually exhibits more pronounced phenotypic and ge- notypic di~ersities.'~
In our study, except regarding primary tumor size, the nuclear accumulation of p53 protein had no signifi- cant correlations with the other clinicopathologic pa- rameters tested. The cumulative survival between the high p53 index group and the low p53 index group were not significantly different, nor was there such a trend, indicating that overexpression of p53 protein is not a prognostic indicator for patients with MFHs of soft tis- sue. This conclusion is concordant with the finding of Kawai et al.," who found in a study of 96 soft tissue sarcomas that the difference of cumulative survivals of 40 patients with MFHs with and without p53 nuclear accumulation was not statistically significant. Drobnjak et a1.I' recently investigated the p53 expression in 174 adult soft tissue sarcomas and found that the patients with a p53 positive phenotype displayed a significantly reduced survival. Although their conclusion is consis- tent with the overall result obtained by Kawai et al.," it may not be applicable to MFH, because among their 174 tumors, 110 (63%) cases were either liposarcomas or leiomyosarcomas, which were known to be clinico- pathologically different from MFHs. Moreover, the p53 accumulation was not a significant, histologic grade-in- dependent predictor of survival, as suggested repeat- edly by the Cox's regression model used in their" and our studies, respectively. These results indicate that there is no linear correlation between p53 expression and survival of patients with MFH.
Whether the dissociation between p53 status and clinicopathologic parameters is caused by the overex- pression of wild-type p53 protein or another mecha- nism is unclear. In a comparative molecular genetic and immunohistochemical study of 113 sarcomas of bone and soft tissue, Wadayama et al.13 noted that among the 42 detected gene alternations, all the missense muta- tions showed p53 immunoreactivities in cells quantified from less than 10% to more than 50% and that no im- munoreactivity was observed in the 21 (50%) cases with gross rearrangements, frame-shift mutation, nonsense mutation, or mutation at splicing site. Comparing re- sults of p53 immunohistochemistry and single-strand conformational polymorphism analysis as well as DNA sequencing of 58 squamous cell carcinomas of head and neck, Xu et al.24 observed a 60% concordance between the results of the different methodologies. Among the remaining 24 (40%) cases, 20 showed p53 overex- pression without apparent mutations, and only 4 cases had mutations without detectable p53 immunostaining. They also found that there were no significant differ-

624 CANCER August 25,1995, Volume 76, No. 4
ences between p53 status and tumor staging, tumor site, metastasis, and patholop features. Conversely, Oliner et al.25 detected that 7 of 22 (31.8%) MFHs showed MDM2 gene amplification. Based on the finding that among 24 sarcomas (1 1 MFHs and 13 liposarcomas), 8 tumors showed alterations of p53 gene, 8 tumors had MDM2 amplifications, and no tumor contained alter- ation of both genes, Leach et a1.26 suggested that p53 and MDM2 genetic alterations are alternative mecha- nisms for inactivating the same regulatory pathway for suppressing cell growth. Therefore, the MFHs with MDM2 amplification will lack mutant p53 immunophe- notype but will have similar biologic aggressiveness, as do the p53 positive ones, a proportion that may account for the prognostic nullification of the p53 labeling index in the adult soft tissue MFHs.
Ki-67 antigen is a nuclear protein present in GI , S, G2, and M phases, but not in GO phase of the cell cycle.27 Several studies indicate that cell proliferative activity defined by Ki-67 labeling index correlates with cell growth fraction and radiothymidine labeling i n d e ~ . ~ ~ , ~ ~ The prognostic role of Ki-67 index in MFH is controver- ~ i a l , ' ~ , ' ~ although all of the studies had concordant re- sults on the covariation of Ki-67 index and histologic grade. The current study also revealed that the Ki-67 labeling index of MFHs correlated significantly with the histologic grade. We found that the high Ki-67 labeling index was associated significantly with the reduced cu- mulative survival, but it is not an independent signifi- cant predictor of patient prognosis, as suggested by the Cox's regression analysis. Our finding in this regard is similar to that of Drobnjak et al.," indicating that Ki-67 index may become useful when it is used in combina- tion with other main prognostic factors in predicting the prognosis of patients with MFHs.
A few previous clinicopathologic studies revealed that the primary tumor size significantly contributed to the metastasis3' and the prognosis of MFHs and other sarcoma^.^^,^^ Furthermore, a covariation between the tumor size and the histologic grade of MFHs was noted.33 In the current study, the primary tumor size contributed significantly to the prognosis (t = 2.95, Cox's model) and did not covary with the histologic grade, indicating its statistical independence and prac- tical value in the prognostication of patients with MFHs. Consistent with results of previous investiga- t i o n ~ , ~ ~ - ~ ~ the histologic grade defined by cellularity, nuclear pleomorphism, and mitotic activity was sig- nificantly related with the patient prognosis. We con- clude from the current study that (1) tumor size and his- tologic grade are two important independent prognostic factors; (2) Ki-67 index correlates significantly with his- tologic gr?de, recurrence and metastasis, disease free in- terval, anu survival and should be used in adjunct with
other main prognostic factors in prognostication of pa- tients with MFHs; and (3) nuclear p53 overexpression in MFHs of soft tissue is a comparatively common event that has no prognostic implication.
References
1.
2. 3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
Kastan MB, Onyekwere 0, Sidransky D, Vogelstein B, Craig RW. Participation of p53 protein in the cellular response to DNA damage. Cancer Re5 1991;51:6304-11. Lane DP. p53, guardian of the genome. Nature 1992;358:15-6. Milner J, Medcalf EA, Cook A. Tumor suppressor gene p53: analysis of wild-type and mutant p53 complexes. Mol Cell Biol
Finlay CA, Hinds PW, Tan TH, Eliyahu D, Oren M, Levine AJ. Activating mutations for transformation by p53 produce a gene product that forms an hsc 700-p53 complex with an altered half- life. Mol Cell B i d 1988;8:531-9. Hesketh R. The oncogene handbook. London: Academic Press,
Bartek J, Bartkowa J, Vojtesek B, Staskova Z, Lukas J, Rejthar A, et al. Aberrant expression of the p53 oncoprotein is a common feature of a wild spectrum of human malignancies. Oncogene
Hollstein M, Sidransky D, Vogelstein B, Harris CC. p53 Muta- tions in human cancer. Science 1991;253:49-53. Isola J, Visakorpi T, Holli K, Kallioniemi OP. Association of ex- pression of tumor suppressor protein p53 with rapid cell prolif- eration and poor prognosis in node-negative breast cancer pa- tients. ] Natl Cancer Inst 1992;84:1109-14. Kikuchi-Yanoshita R, Konishi M, Ito S, Seki M, Tanaka K, Maeda Y, et al. Genetic changes of both p53 alleles associated with the conversion from colorectal adenoma to early carcinoma in famil- ial adenomatous polyposis and non-familial adenomatous polyposis patients. Cancer Res 1992;52:3965-71. Drobnjak M, Latres E, Pollack D, Karpeh M, Dudas M, Woodrruff JM, et al. Prognostic implications of p53 nuclear over- expression and high proliferation index of Ki-67 in adult soft- tissue sarcomas. ] Natl Cancer Znst 1994;86:549-54. Kawai A, Noguchi M, Beppu Y, Yokoyama R, Mukai K, Hiro- hashi S, et al. Nuclear immunoreaction of p53 protein in soft tissue sarcomas: a possible prognostic factor. Cancer 1994; 73:
Soini Y, Vahakangas K, Nuorva K, Kame1 D, Lane DP, Paakko P. p53 immunohistochemistry in malignant fibrous histiocytoma and other mesenchymal tumors. JPathoI 1992; 168:29-33. Wadayama 8, Toguchida J, Yamaguchi T, Sasaki MS, Kotoura Y, Yamamuro T. p53 Expression and its relationship to DNA al- ternations in bone and soft tissue sarcomas. BrJ Cancer 1993; 68: 1134-9. Ueda T, Aozasa K, Tsujimoto M, Ohsawa M, Uchida A, Aoki Y, et al. Prognostic significance of Ki-67 reactivity in soft tissue sarcomas. Cancer 1989;63:1607-11. Zehr RJ, Bauer TW, Marks KE, Weltevreden A. Ki-67 and grad- ing of malignant fibrous histiocytomas. Cancer 1990;66:1984- 90. Baas 10, Mulder JWR, Offerhaus JA, Vogelstein B, Hamilton SR. An evaluation of six antibodies for immunohistochemistry of mutant p53 gene product in archival colorectal neoplasms. J PQ-
Enzinger FM, Weiss SW. Soft tissue tumors. 3rd ed. St. Louis:
Shi S-R, Key ME, Kalra KL. Antigen retrieval in formalin-fixed,
1991; 11:12-9.
1994; 536-53.
1991 ; 6:1699-703.
2499-505.
thol 1994;172:5-12.
Mosby; 1995:1-16,89-118,351-80.
p53 and Ki-67 in Malignant Fibrous Histiocytoma/Yang et al. 625
19.
20.
21 t
22.
23.
24.
25.
26.
27.
paraffin embedded tissues: an enhancement method for immu- nohistochemical staining based upon microwave oven heating of tissue sections. 1 Histochem Cytochem 1991;39:741-8. Siege1 S , Castellan NJ. Nonparametric statistics for the behav- ioral sciences. 2nd ed. New York: McGraw-Hill, 1965. Kaplan EL, Meier P. Non-parametric estimation from incom- plete observation. A m Stat AssocJ 1985;53:457-81. Gehan EA. A generalized Wilcoxon test for comparing arbitrarily singly-censored samples. Biometrica 1965;52:202-33. Cox DR. Regression models and life tables. 1 R Stat Soc 1972;84: 1035-44. Latres E, Drobnjak M, Pollack D, Oliva MR, Ramos M, Karpeh M, et al. Chromosome 17 abnormalities and TP53 mutations in adult soft tissue sarcomas. Am PathoI 1994; 145:334-55. Xu L, Chen Y-T, Huvos A, Zlotolow IM, Rettig WJ, Old LJ, et al. Overexpression of p53 protein in squamous cell carcinomas of head and neck without apparent gene mutations. Diagn Mol Pa- thol 1994; 3:83-92. Oliner JD, Kinzler KW, Meltzer PS, George DL, Vogelstein B. Amplification of a gene encoding a p53-associated protein in hu- man sarcomas. Nature 1992;358:80-3. Leach FS, Tokino T, Meltzer P, Burrell M, Oliner JD, Smith S, et a]. p53 mutation and mdm2 amplification in human soft tissue sarcomas. Cancer Res 1993; 53:2231-4. Gerdes J, Lemke H, Baisch H, Wacker H-If, Schwab U, Stein H. Cell cycle analysis of a cell proliferation associated human nuclear antigen defined by the monoclonal antibody Ki-67.1 Zm- nlutlol 1984; 133~1710-7
28.
29.
30.
31.
32.
33.
34.
35.
36.
Kame1 OW, Frankin WA, Ringus JC, Meyer JS. Thymidine label- ing index and Ki-67 growth fraction in lesions of the breast. Am \Pathof 1989; 134:107-13. Sasaki K, Matsumura K, Tsuji T, Shinozaki F, Takahashi M. Re- lationship between labeling indices of Ki-67 and BrdUrd in hu- man malignant tumors. Cancer 1988; 62:989-93. Weiss SW, Enzinger FM. Malignant fibrous histiocytoma: an analysis of 200 cases. Cancer 1978;41:2250-66. Bertoni F, Capanna R, Biagini R, Bacchini P, Guerra A, Ruggieri P, et al. Malignant fibrous histiocytoma of soft tissue: an analysis of 78 cases located and deeply seated in the extremities. Cancer
Gustafson P. Soft tissue sarcoma: epidemiology and prognosis in 508 patients. Acta Orthopaedica Scandinavica 1994; 259
Rydholm A, Syk I . Malignant fibrous histiocytoma of soft tissue: correlation between clinical variables and histologic malignancy grade. Cancer 1986;57:2323-4. Coindre JM, Trojani M, Contesso G, David M, Rouesse J, Bui NB, et al. Reproducibility of a histopathologic grading system for adult soft tissue sarcoma. Cancer 1986;58:306-9. Costa J, Wesley RA, Glatstein E, Rosenberg SA. The grading of soft tissue sarcomas: results of a clinicopathologic correlation in a series of 163 cases. Cancer 1984;53:530-41. Trojani M, Contesso G, Coindre JM, Rouesse J, Bui NB, de Mascarel A, et al. Soft tissue sarcomas of adults; study of pathological prognostic variables and definition of a histopatho- logic grading system. J n f Cancer 1984;33:37-42.
1985;56:356-67.
(SUPPI): 1-3 1.