“progenitor cell therapy in ami after meta-analyses results ? pro“ “progenitor cell therapy in...
TRANSCRIPT

““Progenitor Cell Therapy in AMIProgenitor Cell Therapy in AMIAfter Meta-Analyses Results ? Pro“After Meta-Analyses Results ? Pro“
““Progenitor Cell Therapy in AMIProgenitor Cell Therapy in AMIAfter Meta-Analyses Results ? Pro“After Meta-Analyses Results ? Pro“
Andreas M. Zeiher, MDDept. of Internal Medicine IIIUniversity of FrankfurtGermany
Andreas M. Zeiher, MDDept. of Internal Medicine IIIUniversity of FrankfurtGermany
Disclosure information: Guidant (research support)t2cure (co-founder, advisor)

The Heart is a Regenerating OrganUndisputable Evidence from DNA Integration of C-14
– generated during nuclear bomb testing during cold war -
Bergmann O et al., Science 2009; 324:98-102

Cells for functional cardiac repairCells for functional cardiac repair
Embyronic-likestem cells
(iPS)
somatic cells(skin fibroblasts)
4 genes:Oct4, Klf4, Sox2, myc
Cardiacstem cellsCardiacstem cells
Modified from Dimmeler et al, JCI 2005

Metaanalysis of randomized and
cohort studies of progenitor cell
therapy in ischemic heart disease
N = 976; overall treatment effect
+ 3.7 percentage points increase
in LV-EF ( p < 0.001 )
Abdel-Latif, Arch Intern Med 2007; 167:989
Vascularization Apoptosis
Vascularization Apoptosis
Paracrine factorsParacrine factors
CardiacRegenerationCardiacRegeneration
AcuteAcuteMyocardialMyocardialInfarctionInfarction
AcuteAcuteMyocardialMyocardialInfarctionInfarction
ChronicChronicHeart Heart FailureFailure
ChronicChronicHeart Heart FailureFailure
chronicchronicLV- dilatationLV- dilatation
infarctinfarctexpansionexpansion
Adverse LV RemodelingAdverse LV Remodeling
Cell Therapy in Ischemic Heart Failure: Cell Therapy in Ischemic Heart Failure: therapeutic targetstherapeutic targets
Cell Therapy in Ischemic Heart Failure: Cell Therapy in Ischemic Heart Failure: therapeutic targetstherapeutic targets

Cell Therapy for Ischemic Heart FailureCell Therapy for Ischemic Heart FailureCell Therapy for Ischemic Heart FailureCell Therapy for Ischemic Heart Failure
The patient population at risk post-AMIThe patient population at risk post-AMI
Effects of cell therapy in patients at riskEffects of cell therapy in patients at risk
Derivation of the clinical benefitDerivation of the clinical benefit

Volpi et al., Circulation 1993; 88: 416-429
LV contractile recovery within 1 week after successful LV contractile recovery within 1 week after successful reperfusion determines clinical outcome in STEMIreperfusion determines clinical outcome in STEMIThere is no linear correlation between mortality and ejection fraction after AMI !

VALIANTVALIANTValValsartan sartan iin n AAcute Myocardial Icute Myocardial Innfarction farction TTrialrial
• 14703 patients14703 patients• STEMISTEMI • 0.5 - 10 days0.5 - 10 days• EF < 40%EF < 40%• Killlip I-III Killlip I-III • Diuretics 60%, Diuretics 60%, • Beta-Blocker 71%Beta-Blocker 71%
Pro
bab
ility
of
ca
rdia
c d
eath
, re
-MI
reh
os
pit
alis
atio
n f
or
hea
rt f
ailu
re
NEJM 2003, 349: 1893-1906
23% in23% in 1 year1 year23% in23% in 1 year1 year
30 % in30 % in 2 years2 years30 % in30 % in 2 years2 years

0 6 12 18 24 30 36 42 48
0.0
0.05
0.10
0.15
0.20
0.25
Months from Randomization
Cum
ulat
ive
Ris
k
318 305 272 217 172 124 79 31 Cntrl315 299 258 211 172 123 82 25 ICD
Number at Risk
ICDControl
Cumulative risk of death from any cause
p=0.66
Hohnloser at al., N Engl J Med 2004
Defibrillator IN Acute Myocardial Infarction Trial (DINAMIT)
STEMISTEMI 6- 40 days6- 40 daysEF < 35%EF < 35%

Cell Therapy for Ischemic Heart FailureCell Therapy for Ischemic Heart FailureCell Therapy for Ischemic Heart FailureCell Therapy for Ischemic Heart Failure
The patient population at risk post-AMIThe patient population at risk post-AMI
Effects of cell therapy in patients at risk Effects of cell therapy in patients at risk

0
2
4
6
8
10
EF below medianEF below median(( 48.9 %) 48.9 %)
Baseline LVEFBaseline LVEFby QLVAby QLVA
EF above medianEF above median((>> 48.9 %) 48.9 %)
Ab
solu
te c
han
ge
in g
lob
al L
VE
F (%
)A
bso
lute
ch
ang
e in
glo
bal
LV
EF
(%
)
Enhanced contractile recovery by BMC is confined to patients with failed initial recovery
Enhanced contractile recovery by BMC is confined to patients with failed initial recovery
2.52.5 1.11.1 7.5 1.17.5 1.1 3.73.7 0.70.7
p = 0.002p = 0.002p = 0.002p = 0.002 p = 0.81p = 0.81p = 0.81p = 0.81
4.0 0.64.0 0.6
PlaceboPlacebo BMCBMC PlaceboPlacebo BMCBMCn =n = 5252 4141 4040 5454
p for interaction = p for interaction = 0.0200.020p for interaction = p for interaction = 0.0200.020
Schächinger et al., N Engl J Med 2006

REGENTREGENT
Courtesy of M Tendera, ESC Congress Munich, 9/2008
39 39 37 40
Controls N=20
10
20
30
40
50
60
70
80
BMCN=46
10
20
30
40
50
60
70
80
p=0.73 p=0.01
0 6 months 0 6 months
REGENT trialREGENT trial
36
31
0 6 months10
20
30
40
50
60
p=0.007
< median
-5
0
5
10
15
20
25
30
FINNCELL trialFINNCELL trial
< median > median
Ch
ang
e in
EF
(%
)
BMC
Placebo
Courtesy of H. Huikuri, European Heart Journal, 2008
p = 0.04
Enhanced contractile recovery by BMC in patients with failed initial recovery – results of recent controlled trialsEnhanced contractile recovery by BMC in patients with failed initial recovery – results of recent controlled trials

En
dsy
sto
lic
volu
me
(ml)
EF < median
Baseline 4 months 12 months
EF > median
BMC
Placebo
Baseline EF: 39 + 1.9 % Baseline EF: 56 + 2.3 %
Adverse remodeling is confined to patients with failed Adverse remodeling is confined to patients with failed initial recovery of EF and abrogated by BMC therapyinitial recovery of EF and abrogated by BMC therapy
Dill et al., AHJ 2009
Change of endsystolic volumes over time (MRI)
0
20
40
60
80
100
120
140
Baseline 4 months 12 months
p = 0.7
p = 0.06
p = 0.01
p = 0.9 p = 0.7 p = 0.5

Change in endsystolic volume (ml)Change in endsystolic volume (ml)
-10-10 -5-5 00 55 1010 1515 2020
Ch
an
ge
in E
F (
%)
Ch
an
ge
in E
F (
%)
00
22
44
66
88
1010
EF EF 48.9% 48.9%p = 0.007p = 0.007
BMCBMC
PlaceboPlacebo
Intracoronary BMC Administration Profoundly Modifies LV RemodelingIntracoronary BMC Administration
Profoundly Modifies LV Remodeling
- 4- 4
- 2- 2
Interaction between LV ejection fraction and endsystolic volumeInteraction between LV ejection fraction and endsystolic volume
no therapyno therapy
ReperfusionReperfusion ++pharmac. Rxpharmac. Rx

Cell Therapy for Ischemic Heart FailureCell Therapy for Ischemic Heart FailureCell Therapy for Ischemic Heart FailureCell Therapy for Ischemic Heart Failure
The patient population at risk post-AMIThe patient population at risk post-AMI
Effects of cell therapy in patients at risk Effects of cell therapy in patients at risk
Derivation of the clinical benefitDerivation of the clinical benefit

Do beneficial effects of BMC therapy on adverse remodeling translate into clinical benefit ?
Do beneficial effects of BMC therapy on adverse remodeling translate into clinical benefit ?
??
Therapies preventingadverse remodelling…Therapies preventingadverse remodelling…
… reduce adverse cardiovascular events… reduce adverse cardiovascular events
ACEI , ARB, ß-Blocker, Aldosteron-Ant.

Death, Re-MI, Heart Failure at 4-6 MonthsDeath, Re-MI, Heart Failure at 4-6 Monthsin randomized, (placebo)-controlled BMC trialsin randomized, (placebo)-controlled BMC trials
Death, Re-MI, Heart Failure at 4-6 MonthsDeath, Re-MI, Heart Failure at 4-6 Monthsin randomized, (placebo)-controlled BMC trialsin randomized, (placebo)-controlled BMC trials
0
2
4
6
8
REPAIR
Jans
sens
FINNCELL
REG
ENT
Placebo
BMC
Dea
th,
re-M
I, h
osp
ital
isat
ion
fo
r h
eart
fai
lure
* (
%)
N=204 N=67 N=80 N=120
* after hospital discharge
TOTAL
N=471
13 / 217
3 / 254
p<0.005

BMC therapy is associated with improved clinical outcome at 2 years
BMC therapy is associated with improved clinical outcome at 2 years
daysdays00 100100 200200 300300 400400 500500 600600 7007000
60
70
80
90
100
p = 0.009p = 0.009(log rank)
PlaceboPlacebo
BMCBMC
Eve
nt-
free
su
rviv
al (
%)
Eve
nt-
free
su
rviv
al (
%)
(dea
th,
myo
card
ial i
nfar
ctio
n,(d
eath
, m
yoca
rdia
l inf
arct
ion,
reh
osp
italiz
atio
n f
. h
eart
fai
lure
)re
hosp
italiz
atio
n f
. h
eart
fai
lure
)
# exposedto risk
Placebo 103 93 90 86 86
BMC 101 99 98 97 95
- Death, MI, Rehospitalization for heart failure -- Death, MI, Rehospitalization for heart failure -

Do potential effects persist ?Do potential effects persist ?
Cell Therapy for Ischemic Heart FailureCell Therapy for Ischemic Heart Failure
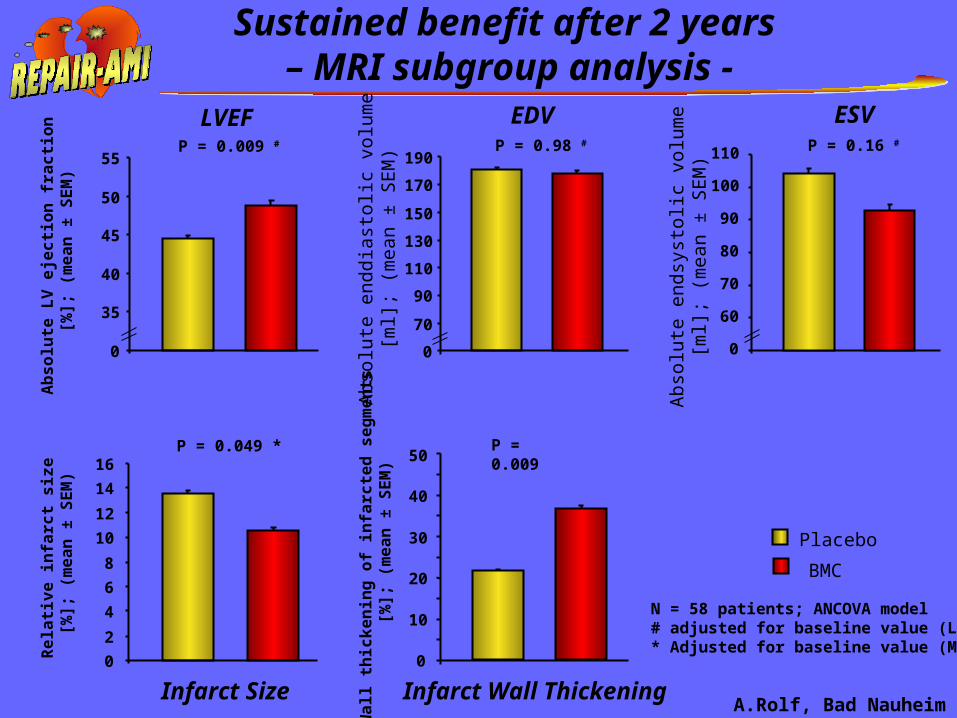
Sustained benefit after 2 years – MRI subgroup analysis -
P = 0.98 #
0
70
90
110
130
150
170
190
Abs
olu
te e
nddi
asto
lic v
olum
e[m
l]; (
mea
n ±
SE
M)
P = 0.049 *
0
2
4
6
8
10
12
14
16
Re
lati
ve
in
farc
t s
ize
[%
]; (
me
an
± S
EM
)
0
10
20
30
40
50P = 0.009
Wa
ll t
hic
ke
nin
g o
f in
farc
ted
se
gm
en
ts [
%];
(m
ea
n ±
SE
M)
Placebo
BMC
P = 0.16 #
0
60
70
80
90
100
110
Abs
olu
te e
ndsy
stol
ic v
olu
me
[ml];
(m
ean
± S
EM
)
P = 0.009 #
0
35
40
45
50
55
Ab
so
lute
LV
eje
cti
on
fra
cti
on
[%
]; (
me
an
± S
EM
)
N = 58 patients; ANCOVA model# adjusted for baseline value (LVA)* Adjusted for baseline value (MRI)
LVEF EDV ESV
Infarct Size Infarct Wall ThickeningA.Rolf, Bad Nauheim

90
80
70
60
50
40
30
Baseline 4 months 1 year
MR
I L
VE
F (
%)
2 years
p < 0.001 p = 0.008 p = 0.04
5 years
p < 0.001
p = 0.03
Improvement of MRI - determined LVEF isImprovement of MRI - determined LVEF issustained 5 years after progenitor cell therapysustained 5 years after progenitor cell therapy
Mean ± SDN
46 ± 10N = 31
52 ± 11N = 30
57 ± 13N = 30
62 ± 11N = 28
59 ± 8N = 31

Persistently low NT-pro BNP serum levels at 5 years Persistently low NT-pro BNP serum levels at 5 years indicate absence of adverse LV remodelingindicate absence of adverse LV remodeling
1.000
500
0
Baseline 4 months 1 year 2 years 5 years
Mean ± SDN
917 ± 920N = 39
283 ± 283N = 34
285 ± 346N = 25
304 ± 602N = 19
213 ± 308N = 39
NT
-pro
BN
P s
eru
m l
evel
s[p
g/m
l]
p < 0.001 p = 0.20 p = 0.97
p = 0.03
p = 0.97
2.500

Bone Marrow Cell Therapy for Post-Infarction Heart Failure
Bone Marrow Cell Therapy for Post-Infarction Heart Failure
Intracoronary administration of BMC …Intracoronary administration of BMC …
abrogates adverse left ventricular remodeling abrogates adverse left ventricular remodeling in patients at risk in patients at risk - - failure of initial contractile recovery after reperfusionfailure of initial contractile recovery after reperfusion- persistently elevated NT-proBNP acutely- persistently elevated NT-proBNP acutely
abrogates adverse left ventricular remodeling abrogates adverse left ventricular remodeling in patients at risk in patients at risk - - failure of initial contractile recovery after reperfusionfailure of initial contractile recovery after reperfusion- persistently elevated NT-proBNP acutely- persistently elevated NT-proBNP acutely
is associated with enhanced LV contractile is associated with enhanced LV contractile recovery and improved coronary flow reserverecovery and improved coronary flow reserveis associated with enhanced LV contractile is associated with enhanced LV contractile recovery and improved coronary flow reserverecovery and improved coronary flow reserve
is associated with improved clinical is associated with improved clinical outcome at 2 yearsoutcome at 2 yearsis associated with improved clinical is associated with improved clinical outcome at 2 yearsoutcome at 2 years
demonstrates a cell bioactivity - contractile demonstrates a cell bioactivity - contractile recovery response relationship recovery response relationship demonstrates a cell bioactivity - contractile demonstrates a cell bioactivity - contractile recovery response relationship recovery response relationship
prevents adverse remodelling over 5 yearsprevents adverse remodelling over 5 yearsprevents adverse remodelling over 5 yearsprevents adverse remodelling over 5 years

ConclusionConclusion
In patients with acute post-infarction heart failure In patients with acute post-infarction heart failure despite successful reperfusion therapydespite successful reperfusion therapy
a large-scale clinical endpoint trial is a large-scale clinical endpoint trial is warranted to document the effects on warranted to document the effects on mortality and morbiditymortality and morbidity
a large-scale clinical endpoint trial is a large-scale clinical endpoint trial is warranted to document the effects on warranted to document the effects on mortality and morbiditymortality and morbidity

Stefanie DimmelerStefanie DimmelerBirgit AssmusBirgit AssmusVolker SchächingerVolker Schächingerwww.REPAIR-AMI.org

Steering CommitteeSteering Committee
HamburgHamburg
LeipzigLeipzigBad BerkaBad Berka
SuhlSuhl
Bad OeynhausenBad Oeynhausen
LippeLippe
Homburg/SaarHomburg/Saar
ZürichZürich
MannheimMannheim
LudwigshafenLudwigshafen Frankfurt(2 centers)Frankfurt(2 centers)
BadNauheimBadNauheimGiessenGiessen
MainzMainz
KasselKassel
Study Centers and Core FacilitiesStudy Centers and Core Facilities
S. Erbs / R. HambrechtS. Erbs / R. Hambrecht
V. Schächinger /V. Schächinger /B. Assmus / S. DimmelerB. Assmus / S. Dimmeler
A. M. Zeiher (PI)A. M. Zeiher (PI)
A. Elsässer / M. Stanisch /A. Elsässer / M. Stanisch /T. Dill / Ch. HammT. Dill / Ch. Hamm
W. HaberboschW. Haberbosch
H. Hölschermann /H. Hölschermann /H. TillmannsH. Tillmanns
J. Yu / B. LauerJ. Yu / B. Lauer
R. Corti / T. LüscherR. Corti / T. Lüscher
D. Mathey / T. TüblerD. Mathey / T. Tübler
T. Süselbeck / M. Brückmann /T. Süselbeck / M. Brückmann /K. HaaseK. Haase
G. Nickenig / N. Werner /G. Nickenig / N. Werner /M. BöhmM. Böhm
J. HaaseJ. Haase
C. Hansen / J. NeuznerC. Hansen / J. Neuzner
A. Germing / A. MüggeA. Germing / A. Mügge
B. Mark / J. SengesB. Mark / J. Senges
C. Hoffmann / M. Farr /C. Hoffmann / M. Farr /D. HorstkotteD. Horstkotte
A. Cuneo / U. TebbeA. Cuneo / U. Tebbe
S. Genth-Zotz /S. Genth-Zotz /T. MünzelT. Münzel
BochumBochum
Cell Processing CenterCell Processing Center
T. Tonn / N. Krzossok/T. Tonn / N. Krzossok/E. SeifriedE. Seifried
Safety CommitteeSafety CommitteeT. Bonzel / W. KasperT. Bonzel / W. Kasper
Coordinating CenterCoordinating Center
H. BraunH. Braun
MRI Core LabMRI Core Lab
Doppler Core LabDoppler Core Lab
Echo Core LabEcho Core Lab
Angio Core LabAngio Core Lab
www.REPAIR-AMI.orgwww.REPAIR-AMI.org400 km400 km

Klinikum derKlinikum derJohann Wolfgang Goethe UniversitätJohann Wolfgang Goethe Universität
Frankfurt am MainFrankfurt am Main
Dept. of HematologyDept. of Hematology
H. Martin / W. HofmannH. Martin / W. HofmannD. HoelzerD. Hoelzer
Dept. of RadiologyDept. of Radiology
N. Abolmaali / J. SchmittN. Abolmaali / J. SchmittT. VoglT. Vogl
Experimental StudiesExperimental StudiesC. Urbich, C. Urbich, A. KühbacherA. KühbacherM. Potente M. Potente A. AicherA. Aicher E. Chavakis, G. CarmonaE. Chavakis, G. CarmonaL. Rössig, D. Scharner L. Rössig, D. Scharner M. Koyanagi, M. IwasakiM. Koyanagi, M. IwasakiTh. Ziebart, C. YoonTh. Ziebart, C. Yoon
& technical help (Andrea, Nicole,& technical help (Andrea, Nicole,Ariane, Marion, Tino)Ariane, Marion, Tino)
Red Cross FrankfurtRed Cross Frankfurt
T. Tonn / SeifriedT. Tonn / SeifriedT. Brühl, M. Vasa,T. Brühl, M. Vasa,K. Sasaki, C. Badorff, C. HeeschenK. Sasaki, C. Badorff, C. Heeschen
Clinician Scientists:Clinician Scientists:J. Honold, R. Lehmann J. Honold, R. Lehmann U. Fischer-RasokatU. Fischer-RasokatS. Fichtlscherer S. Fichtlscherer F. Seeger, C.KisselF. Seeger, C.KisselK.SpyridopoulosK.SpyridopoulosN. Bellera GotardaN. Bellera Gotarda
Kerckhoff ClinicKerckhoff Clinic
C. Hamm / T. DillC. Hamm / T. Dill