professor john strang national addiction centre, king’s ... · pdf filenovel...
TRANSCRIPT
Novel buprenorphine oral lyophilisate (EspranorTM/XprenorTM) vs sublingual buprenorphine in opioid‐dependent patients:
‘first‐in‐patient’
Phase II safety study
Professor John Strang
National Addiction Centre, King’s College London, UK
Novel buprenorphine oral lyophilisate (EspranorTM/XprenorTM) vs sublingual buprenorphine in opioid‐dependent patients:
‘first‐in‐patient’
Phase II safety study
Authorship: John Strang a,b,+, Kylie Reed a,b,*, Karolina Bogdanowicz b, James Bell a,b, Rob VanderWaal a, Jenny Keen a,b, Pete Beavan a, Shelagh Baillie c and Alastair Knight d.
a King’s College London, National Addiction Centre (Institute of Psychiatry, Psychology and Neuroscience), Denmark Hill, London SE5 8BB, UK; b Addictions Services, South London & Maudsley NHS Foundation Trust, London; c Martindale Pharma, Buckinghamshire, UK; d Evicom, Twickenham, UK.
Declaration (personal & institutional)• DH, NTA, Home Office, NACD, EMCDDA, WHO, UNODC, FDA, NIDA.
• NHS provider (community & in‐patient); history with Phoenix House, Lifeline, Clouds House,
KCA (Kent Council on Addictions).
• Consultation and work with pharmaceutical companies re actual or
potential development of
new medicines for use in the addiction treatment field, including (past 3 years) Martindale
Pharma, Reckitt‐Benkiser/Indivior, UCB, MundiPharma, Lundbeck, Alkermes, Rusan/iGen,
Braeburn and also discussions with Lightlake, Lanacher, Fidelity
International and Titan.
• Principal Investigator and (through the university) retained consultant for the UK Espranor
Safety Study for Martindale Pharma.
• UKDPC (UK Drug Policy Commission), SSA (Society for the Study of
Addiction); and two
Masters degrees (taught MSc and IPAS) and an Addictions MOOC.
• Work also with several charities (and received support) including Action on Addiction, and
also with J Paul Getty Charitable Trust (JPGT) and Pilgrim Trust.
• The university (King’s College London) has registering intellectual property on a novel
naloxone formulation, and JS has been named in a patent registration by a Pharma company
as inventor of another naloxone formulation.
Funding for this study
• Exclusive financial support for this study from Martindale Pharma
• Funding through the King’s Health Partners Clinical Trials Office (and thence to Clinical Research Facility, King’s College Hospital and to clinical sites within SLaM (South London & Maudsley) NHS
Foundation Trust and to the university King’s College London
• Funding through the university (King’s College London) for consultancy advice and input from Professor Strang (funding to
the university)
• Supplementary support from the BRC (Biomedical Research Centre) for Mental Health, Institute of Psychiatry, Psychology &
Neuroscience, King’s College London
Thanks
• Patients who consented to participate
• Colleagues within CRF (Clinical Research Facility), AAU (Acute Assessment Unit), referring teams and Clinical Trials Office
(KHP‐CTO)
• Martindale Pharma
Introduction – why is it interesting?
• Buprenorphine maintenance – now widely used (variably internationally); individual and public benefit; Cochrane‐tested;
NICE‐approved (TA 114)
• Problem of abuse of diverted supplies; existing tablets liable to concealment due to slow dispersal; impedes wider utilisation and
completely obstructs use in some less supervised settings
• Can we have new forms of buprenorphine without this problem? Yes ‐
Buprenorphine/naloxone Suboxone ‘film’
(US, Oz, S E Asia);
orally‐disintegrating tablet lyophilised buprenorphine (this study)
Study design (1)
Aims: to test safety and efficacy of a new buprenorphine oral lyophilisate (‘Espranor’) compared to standard sublingual
buprenorphine (‘Subutex’, reference product), covering dose induction and maintenance.
Design: randomised (2:1) open label study in opioid dependent subjects; with subsequent partial cross‐over of group on experimental
oral lyophilisate. Personalised dose titration. [Pharmacokinetics on volunteer sub‐set].
Settings: specialised clinical trials facility and specialised outpatient addictions treatment facility on same campus.
Study design (2)
Participants:
•opioid dependent subjects (n=36)
•commencing buprenorphine maintenance treatment (maintenance dose to be flexibly titrated)
•includes patients also using alcohol and/or cocaine and/or benzodiazepines at levels below specified thresholds
Materials – study medications
The two buprenorphine formulations studied:
•new buprenorphine oral lyophilisate (‘Espranor’)
•sub‐lingual buprenorphine (‘Subutex’, reference product)
Measures• Respiratory function (respiratory rate, pulse‐oximetry);
• retention in treatment;
• medication hold and dose adequacy (VAS);
• opiate withdrawal signs and symptoms (OOWS, SOWS);
• tablets disintegration time (disintegration; completely dissolved).
• [also, for PK volunteer subjects, plasma buprenorphine and norbuprenorphine – in analysis, to be reported separately].
Patient population & doses achieved
• 36 patients (2:1 randomisation); 23 buprenorphine oral lyophilisate
(Espranor), 13 sublingual buprenorphine (Subutex)
• Generally well‐matched across the two groups; Age – mean 42 years; Gender –
14% female
• Retained well through the intensive study period
• Adequate personalised maintenance doses achieved (means of 11mg and 10mg for oral lyophilisate
and sublingual respectively)
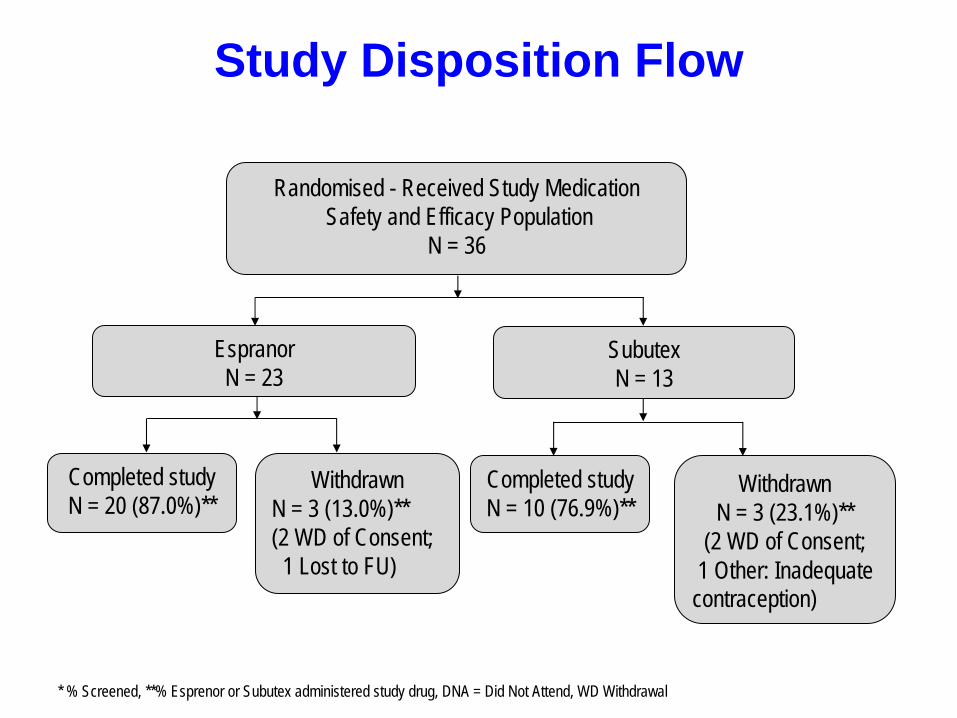
Study Disposition Flow
Randomised - Received Study MedicationSafety and Efficacy Population
N = 36
WithdrawnN = 3 (13.0%)** (2 WD of Consent;
1 Lost to FU)
Completed studyN = 20 (87.0%)**
WithdrawnN = 3 (23.1%)**
(2 WD of Consent;1 Other: Inadequate contraception)
Completed studyN = 10 (76.9%)**
EspranorN = 23
SubutexN = 13
* % Screened, **% Esprenor or Subutex administered study drug, DNA = Did Not Attend, WD Withdrawal
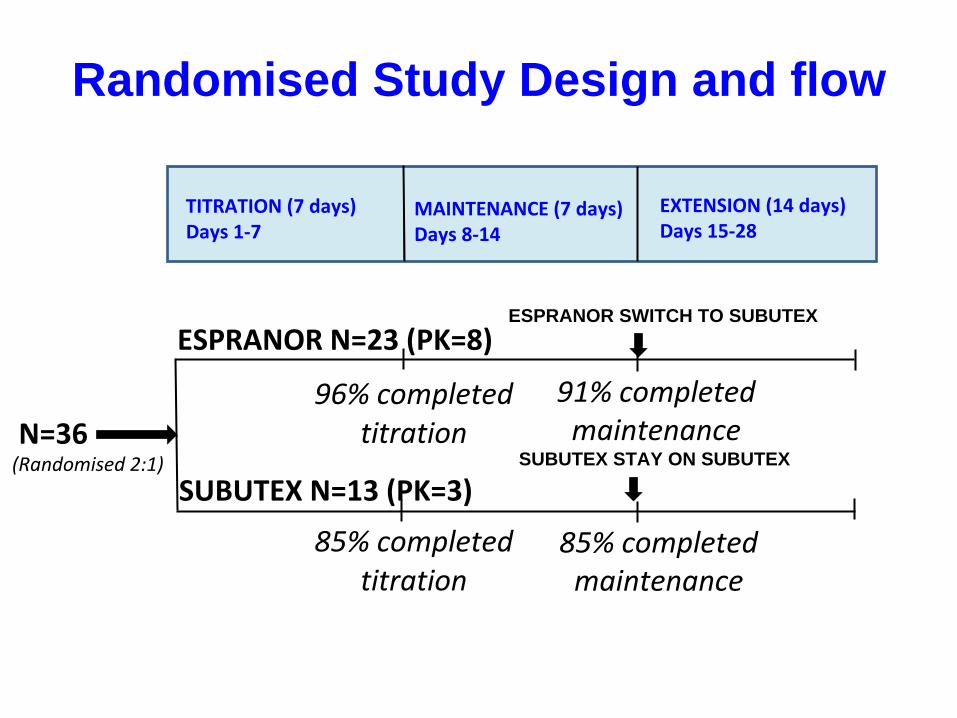
Randomised Study Design and flow
TITRATION (7 days)Days 1‐7
MAINTENANCE (7 days)Days 8‐14
EXTENSION (14 days)Days 15‐28
ESPRANOR N=23 (PK=8)
SUBUTEX N=13 (PK=3)
N=36
ESPRANOR SWITCH TO SUBUTEX
SUBUTEX STAY ON SUBUTEX
96% completed titration
85% completed titration
91% completed maintenance
85% completed maintenance
(Randomised 2:1)
Results – selected excerpts
• Full paper to follow in journal format –
hopefully soon
• Separate analyses and presentation of cross‐over sample at a future meeting
• Separate analyses and presentation of hypoxic response at a future meeting
Results – overall observations
• Buprenorphine oral lyophiliate ‐
completely disintegrating within 2 minutes in 58% of administrations (vs 5% for sublingual bup).
• Individual tailoring of doses resulted in similar dosing regimes (mean maintenance daily doses of 11mg and 10mg respectively).
• No significant between‐group differences were detected in retention in treatment, opiate withdrawal phenomena, craving,
adequacy of ‘hold’
and measures of respiratory function.
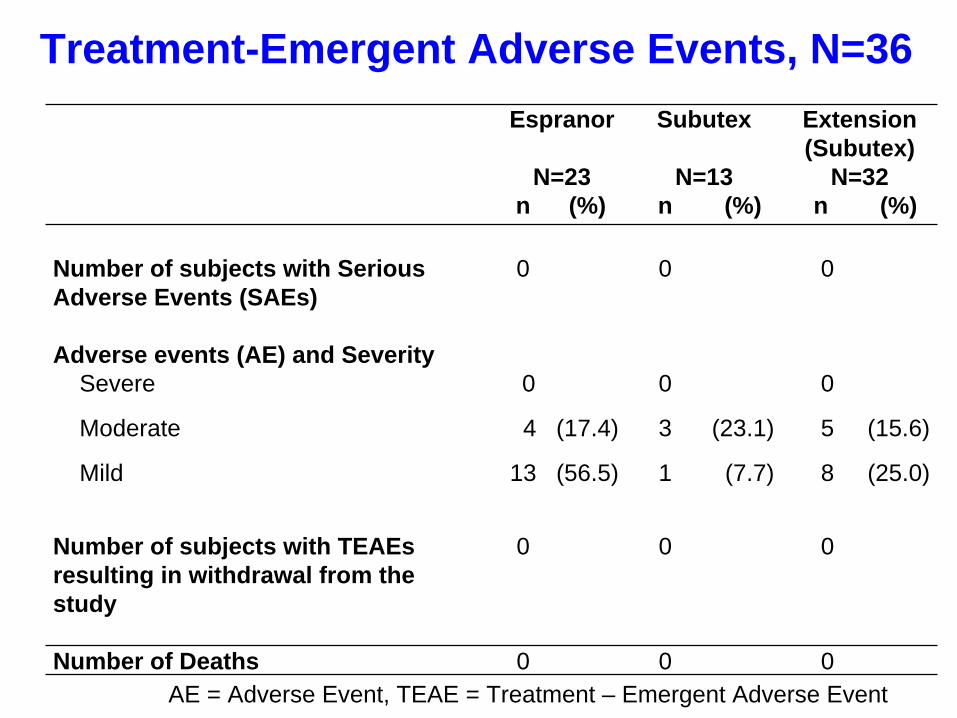
• No SAEs, nor ‘severe’
AEs. More AEs and TEAEs with Espranor (mostly ‘mild’
with similar proportions for ‘moderate’).
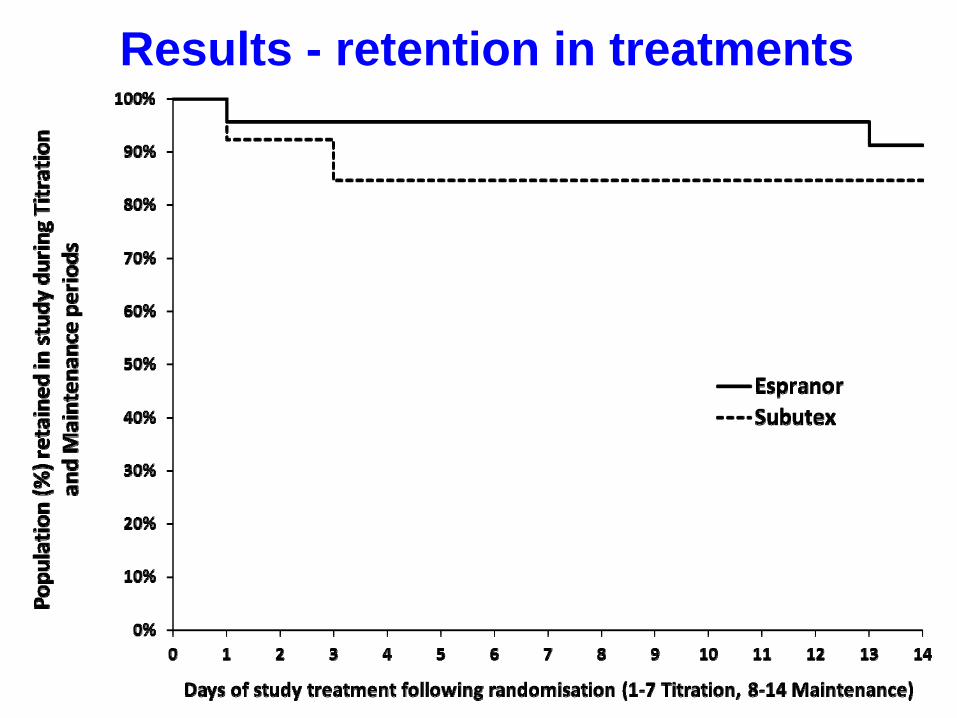
Results - retention in treatments
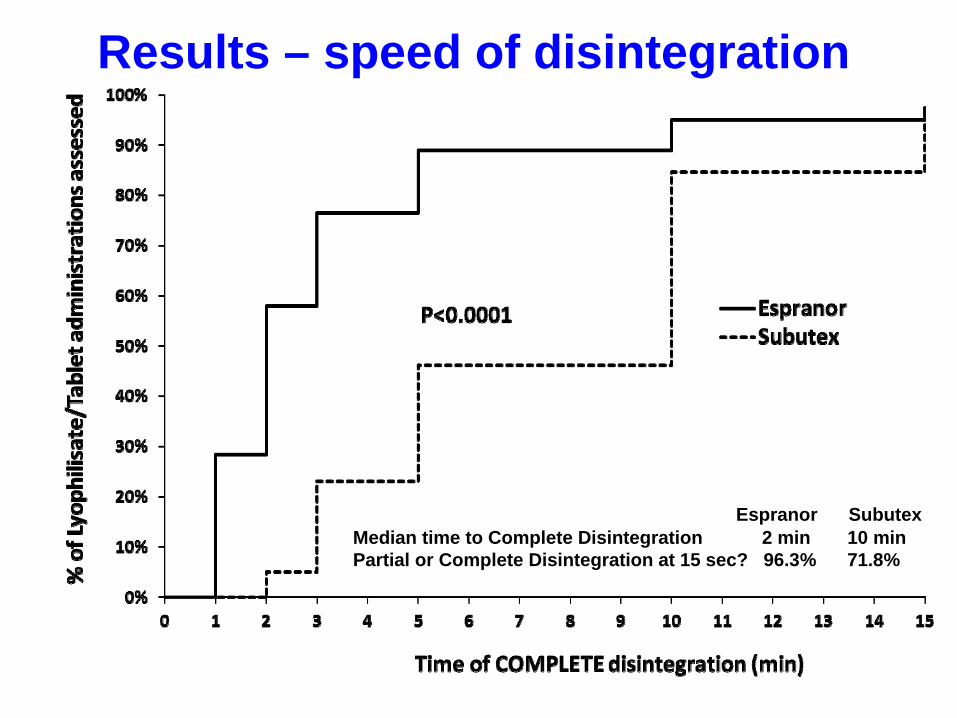
Results – speed of disintegration
Espranor SubutexMedian time to Complete Disintegration 2 min 10 minPartial or Complete Disintegration at 15 sec? 96.3% 71.8%
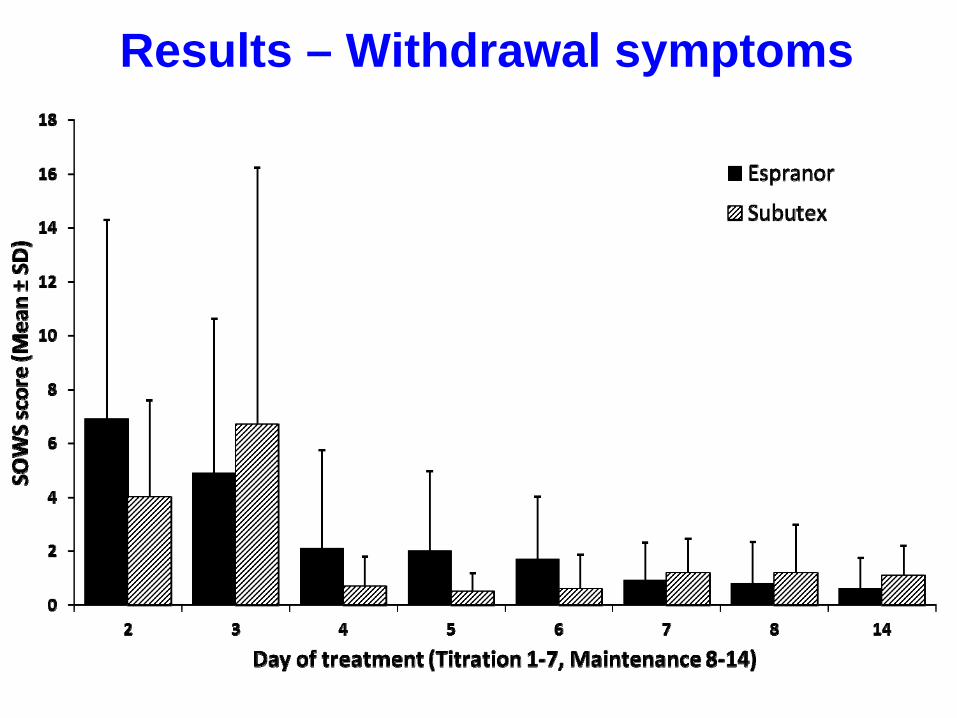
Results – Withdrawal symptoms
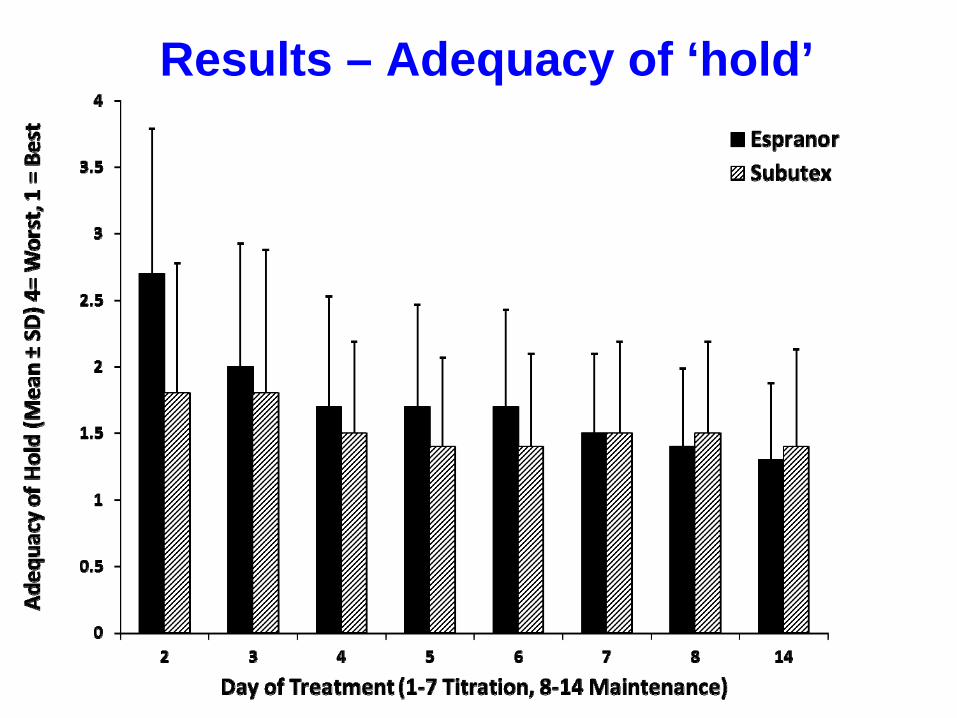
Results – Adequacy of ‘hold’
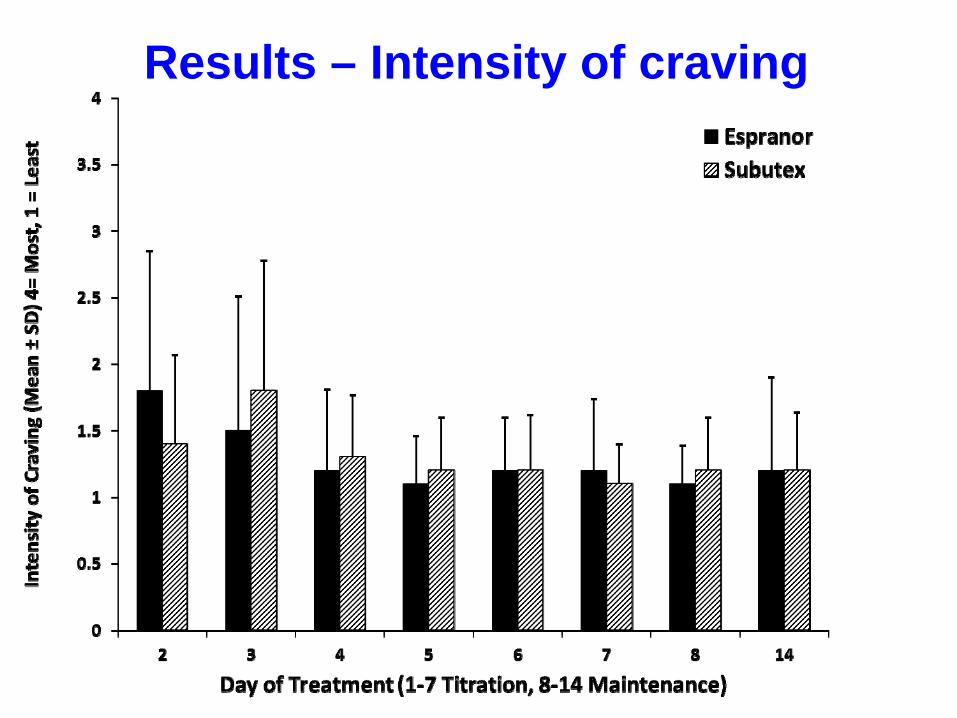
Results – Intensity of craving
Espranor Subutex Extension(Subutex)
N=23 N=13 N=32n (%) n (%) n (%)
Number of subjects with Serious Adverse Events (SAEs)
0 0 0
Adverse events (AE) and Severity Severe 0 0 0
Moderate 4 (17.4) 3 (23.1) 5 (15.6)
Mild 13 (56.5) 1 (7.7) 8 (25.0)
Number of subjects with TEAEs resulting in withdrawal from the study
0 0 0
Number of Deaths 0 0 0AE = Adverse Event, TEAE = Treatment – Emergent Adverse Event
Treatment-Emergent Adverse Events, N=36
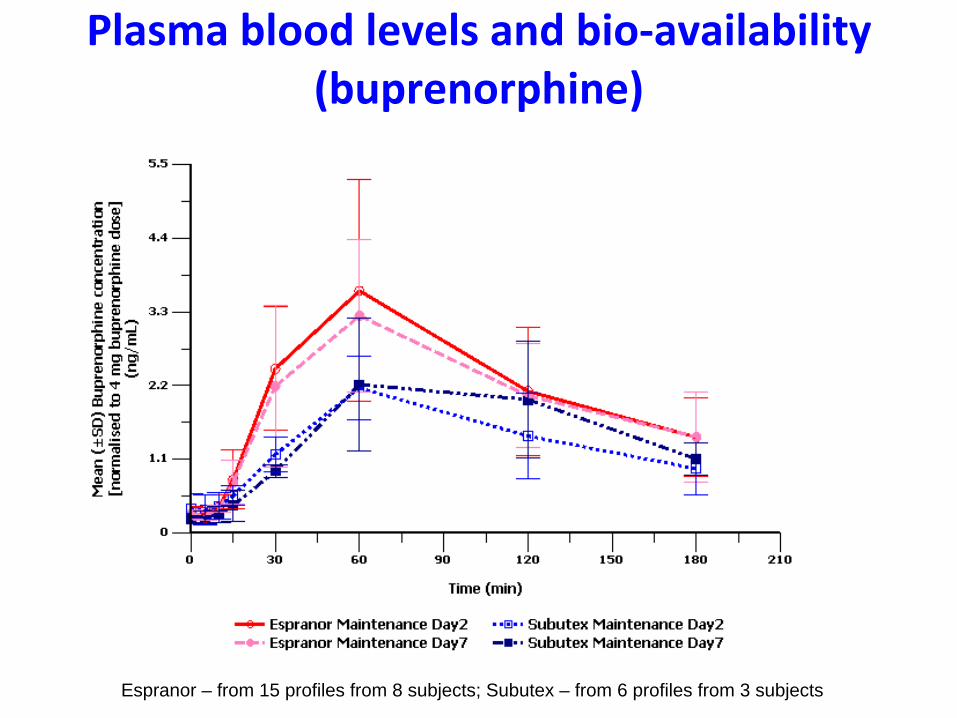
Plasma blood levels and bio‐availability (buprenorphine)
Espranor – from 15 profiles from 8 subjects; Subutex – from 6 profiles from 3 subjects
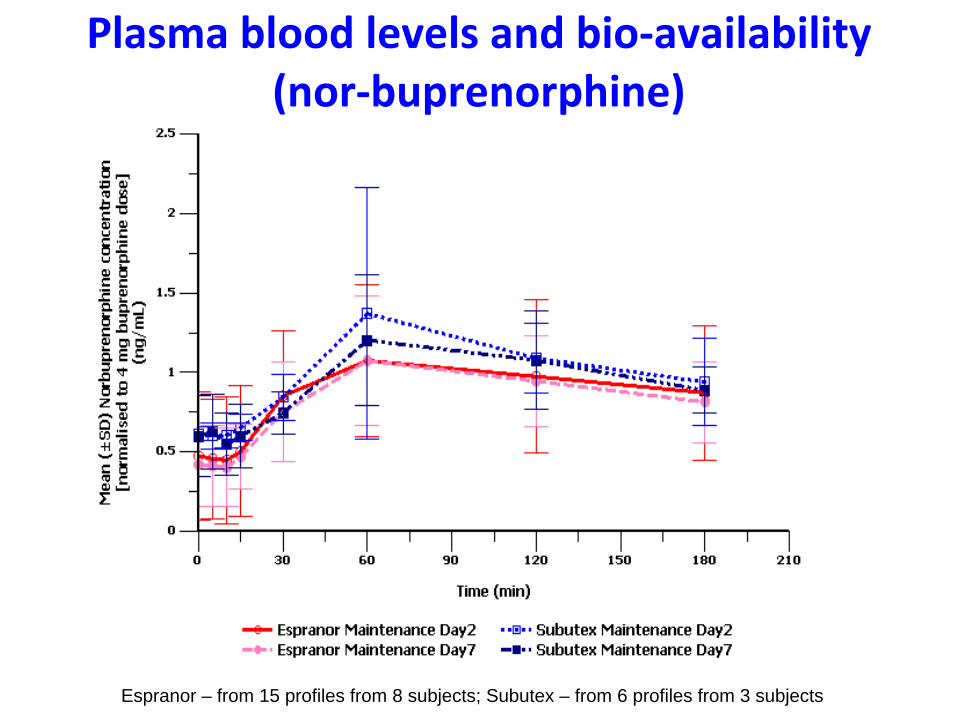
Plasma blood levels and bio‐availability (nor‐buprenorphine)
Espranor – from 15 profiles from 8 subjects; Subutex – from 6 profiles from 3 subjects
Discussion and possible implications
• New buprenorphine
product (recent license approval UK, Sweden)
• Mono‐product – implications?
• Safety, efficacy; treatment retention
• Patient and service‐provider perspectives
• Patient experience – is it different?
• Scope for wider applications?
Thank you