prof paul emery and dr juan jover - fit for work europe summit 2013.pdf
DESCRIPTION
Prof Paul Emery and Dr Juan Jover - Fit for Work Europe Summit 2013TRANSCRIPT

Investing in Healthcare: breaking down
the silos
Brussels, 16 October 2013
With the endorsement of the Lithuanian Presidency of the Council of the EU
In partnership with the European Economic and Social Committee
Co-chaired by Antonyia Parvanova MEP & Gianni Pittella, Vice-President, EP
Follow us on Twitter @FfWEurope
Check our website www.fitforworkeurope.eu
Take a look at our blog www.blog.fitforworkeurope.eu
Professor Paul Emery and Professor Juan Jover
Social Return on Investment:
The results of the Early Intervention Clinic in Spain.
The concept of the Fit for Work Early Intervention
framework In Europe.
Rheumatic and Musculoskeletal Diseases
More than 200 diseases
• Joints
• Connective Tissue
• Spine
• Soft tissue
• Bone
High Disease Burden
• High incidence and prevalence
• Chronic course
• High use of Health System resources
• High impact in quality of life: Pain and Disability

Burden of diseases in Canada, 2000
http://www.phac-aspc.gc.ca/ph-sp/preveco-01-eng.php#fig1
Adapted from IHE, 2008; data from the Public Health Agency of Canada

Spain´s National Budget. 2005
20%
Musculoskeletal
Temporary Work Disability
Temporary Work Disability
Subsidies an Other Economic
Benefits of Social Security
10.000.000.000 euros

Health System Process
- Individual factors
- Collective
- Public Health
- Health Care System - Primary Care
- Specialized Care
- Inspection
Occupational Process
- Economic Activity
- Employers
- Unions
- Occupational Health Administrative Process
Social Security Institute
- Compensation
- Laws
- Control
- Fraud
- Inspection TWD
PWD What if…?
The complexity of Work Disability
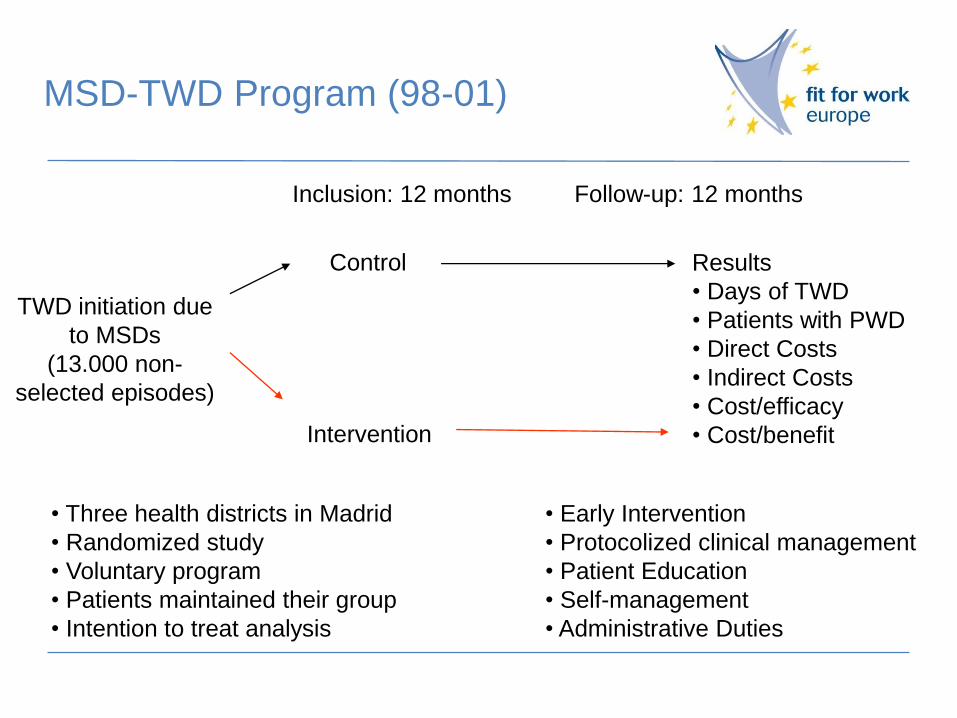
Inclusion: 12 months Follow-up: 12 months
• Three health districts in Madrid
• Randomized study
• Voluntary program
• Patients maintained their group
• Intention to treat analysis
MSD-TWD Program (98-01)
• Early Intervention
• Protocolized clinical management
• Patient Education
• Self-management
• Administrative Duties
Control
Intervention
Results
• Days of TWD
• Patients with PWD
• Direct Costs
• Indirect Costs
• Cost/efficacy
• Cost/benefit
TWD initiation due
to MSDs
(13.000 non-
selected episodes)
Control Intervention
Days
0
25
50
75
100
0 30 60 90 120 150 180 210 240 270 300 330 360
% o
f p
atie
nts
ba
ck to
wo
rk
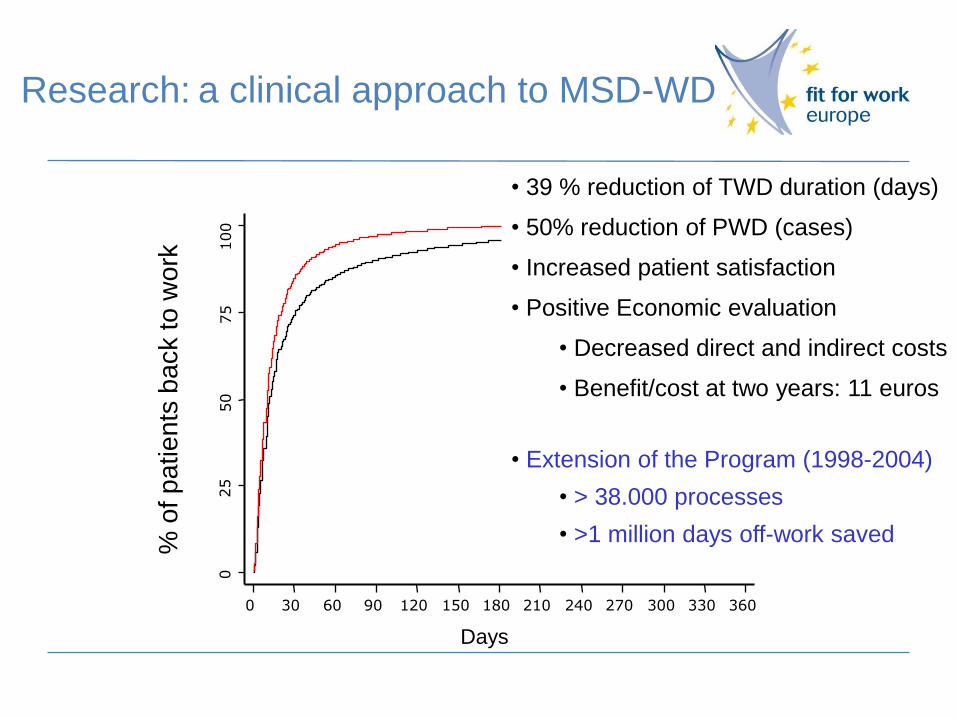
Research: a clinical approach to MSD-WD
• 39 % reduction of TWD duration (days)
• 50% reduction of PWD (cases)
• Increased patient satisfaction
• Positive Economic evaluation
• Decreased direct and indirect costs
• Benefit/cost at two years: 11 euros
• Extension of the Program (1998-2004)
• > 38.000 processes
• >1 million days off-work saved

Scientific Publications
Rheum Int . 2012 Dec; 32(12)3831-9
Rheum Int . 2011 Dec; 31(12) 1549-54 Diagnostic concordance between primary care physicians
and rheumatologists in patients with work disability related
to musculoskeletal disorders.
Candelas G, Abásolo L, León L, Lajas C, Loza E, Revenga M,
Bachiller J, Collado P, Richi P, Blanco M, Jover JA.
Prognostic Factors for Long-Term Disability Due to
Musculoskeletal Disorders LYDIA ABÁSOLO, LETICIA LEÓN, LORETO CARMONA, CRISTINA LAJAS, GLORIA
CANDELAS, MARGARITA BLANCO, AND JUAN A. JOVER1
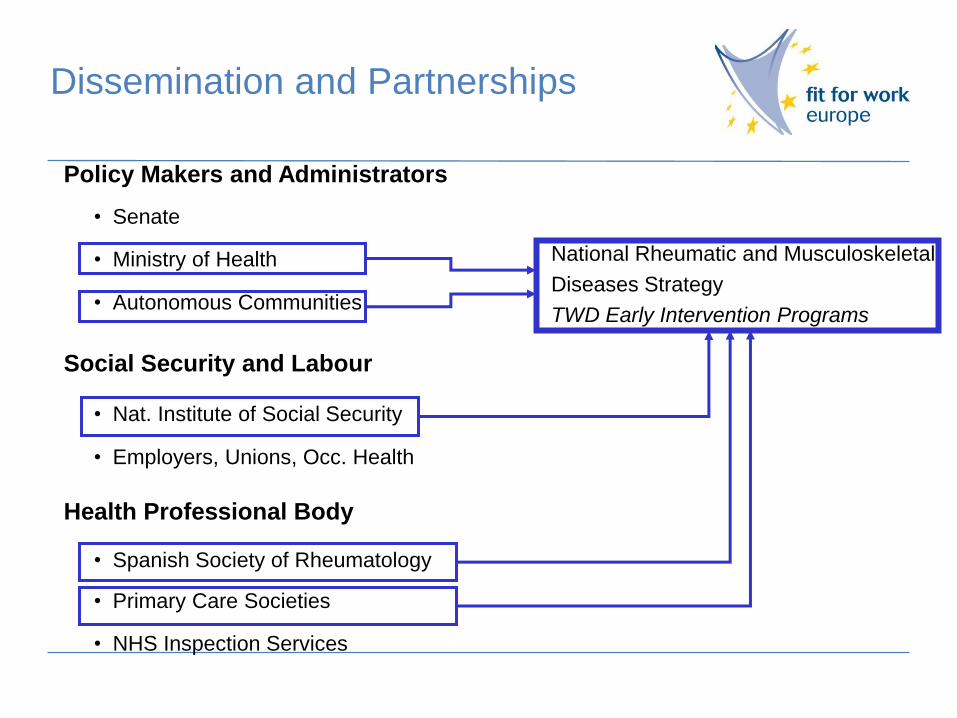
Policy Makers and Administrators
• Senate
• Ministry of Health
• Autonomous Communities
Social Security and Labour
• Nat. Institute of Social Security
• Employers, Unions, Occ. Health
Health Professional Body
• Spanish Society of Rheumatology
• Primary Care Societies
• NHS Inspection Services
Dissemination and Partnerships
National Rheumatic and Musculoskeletal
Diseases Strategy
TWD Early Intervention Programs
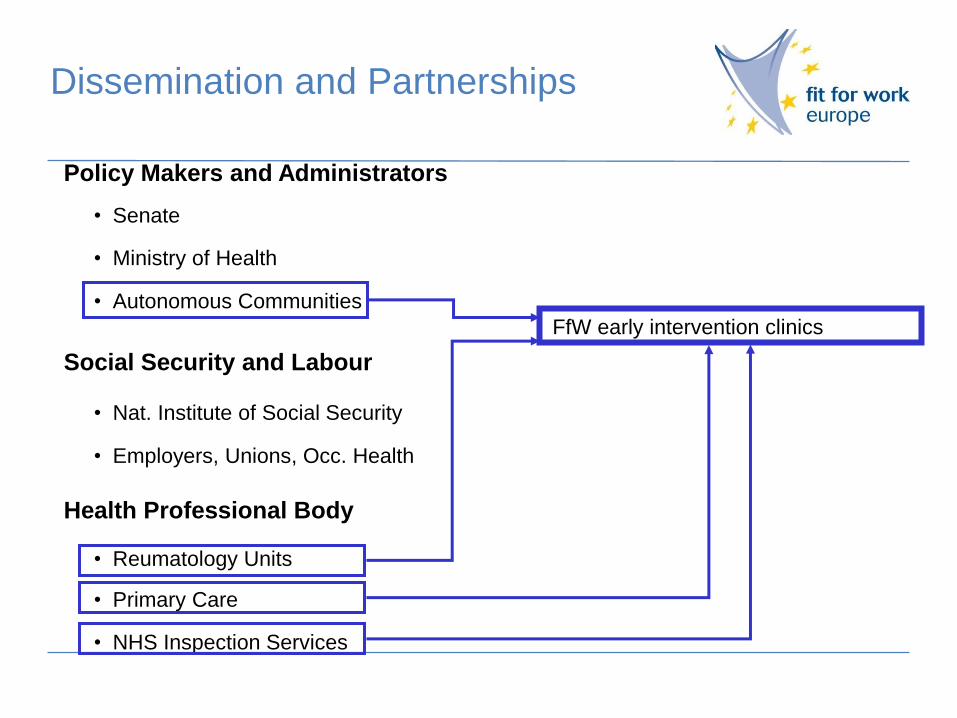
Policy Makers and Administrators
• Senate
• Ministry of Health
• Autonomous Communities
Social Security and Labour
• Nat. Institute of Social Security
• Employers, Unions, Occ. Health
Health Professional Body
• Reumatology Units
• Primary Care
• NHS Inspection Services
FfW early intervention clinics
Dissemination and Partnerships
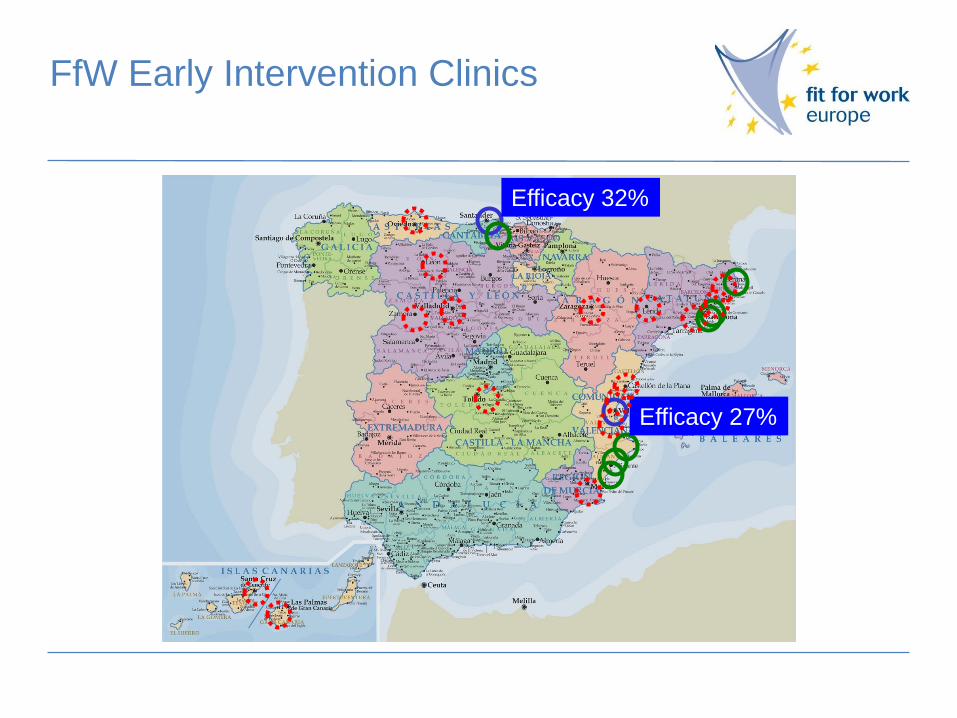
FfW Early Intervention Clinics
Efficacy 32%
Efficacy 27%

Health
Service
Research
Access Health
Results Health Care Reengineering
Very early Specific and Specialized Decreased
TWD-PWD
TWD
FfW EIC Concept

Professor Paul Emery
FfW Early Intervention
European Task Force
European Early Intervention for RMDs
Task Force Working Group
• Chaired by Professor Paul Emery and Professor Juan Jover
• Membership applies to European clinicians committed and interested
in developing early intervention programmes/clinics in their country for
people with RMDs
• Secretariat: Patient Central contracted by The Work Foundation
• Current Membership: Professor Emery (UK), Professor Jover
(Spain), Professor Matucci (Italy), Professor Faustino (Portugal),
Professor Fitzgerald (Ireland), Dr Steve Brennan (UK)
Task Force
Purpose and short-term objectives
• Support the production and expert endorsement of material that allows
the development of early intervention for RMDS:
• Produce Evidence Base (in short-term based on Spanish early
intervention programme with input in longer term from UK model)
• Clinical and financial analysis of Jover data: Key principles, learnings
and outcomes
• Collation and analysis of data and activity from wider Spanish Early
Intervention Programme

Early Intervention Toolkit
For clinicians interested in setting up EI clinics:
• The rationale for early intervention – key principles
• How to set-up early intervention clinics – lessons from
Spain and UK
• Further elements to be informed by:
- The Working Group’s meeting at EULAR 2014
- Follow-up from Summit and FfW ambassadors – their needs

Early Intervention Clinic Principles
• Rapid referral
• Rapid assessment
• Expert assessment:
- Confirm diagnosis
- Confirm appropriate management
- Simple intervention for 90% of patients referred
- Patient education and engagement
- Early discharge to return to work
Model: Early Intervention for RA
• Early intervention now established as effective in
preventing disability and work loss
• Early arthritis clinics routine
• Ambition remission-induction
• Disease prevention now on agenda
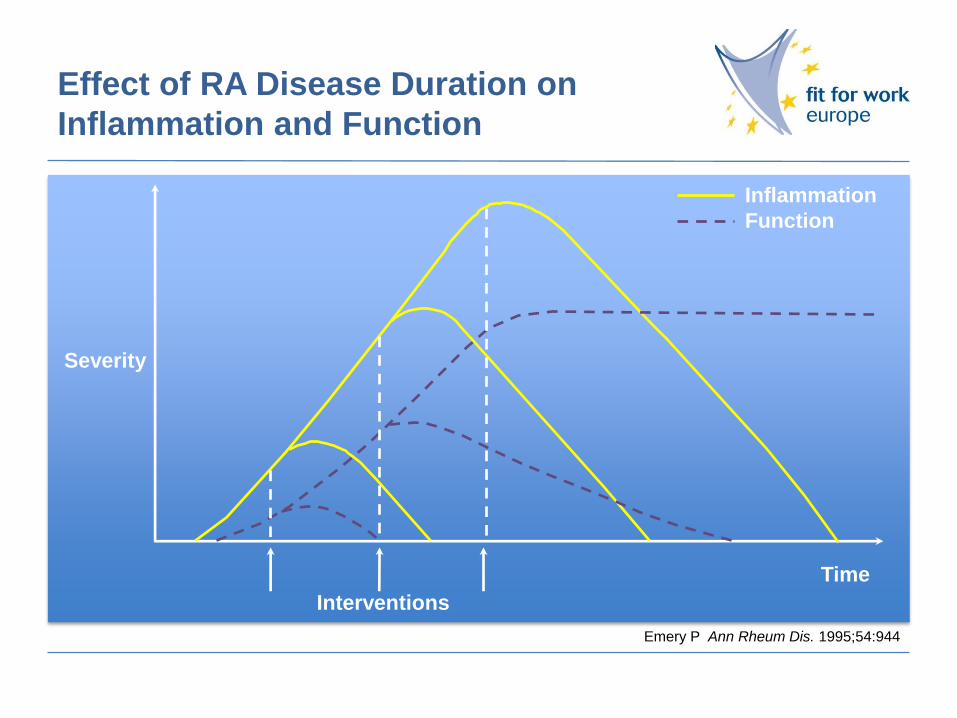
Effect of RA Disease Duration on
Inflammation and Function
Interventions
Time
Severity
Inflammation
Function
Emery P. Ann Rheum Dis. 1995;54:944

Early Intervention: UK

Introduction
• Project to
• demonstrate early intervention reduces work disability
in musculoskeletal patients
• demonstrate early intervention improves patient
outcomes and increases patient satisfaction
• deliver unique UK data on early intervention and work
disability to drive a cost-effectiveness model
• deliver a model for treating high volume
musculoskeletal problems and associated work
disability
Enhancing the MSK Service: Leeds
Current Service
Leeds Musculoskeletal Service receives 25,000 referrals
per year; 90% are seen by physiotherapists.
• Accessed by three CCGs (450 GPs in Leeds)
• 6-8 weeks waiting time to see a physiotherapist
• No strict criteria or protocols relating to referral – based
on GP judgement

Enhancing the MSK Service: Leeds
Enhanced service
• Rapid confirmation of diagnosis (within 5 days of being signed
off sick)
• Rapid assessment and initiation of appropriate management
(within 5 days of being signed off sick from work)
• Earlier and structured initiation of patient education, self-
management/coping strategies plan
• Provision of simple, psychological assessment
• The small numbers who may need further specialist assessment
and investigations will get earlier referral
• Discharge plan based on fit for work status or permanent disability
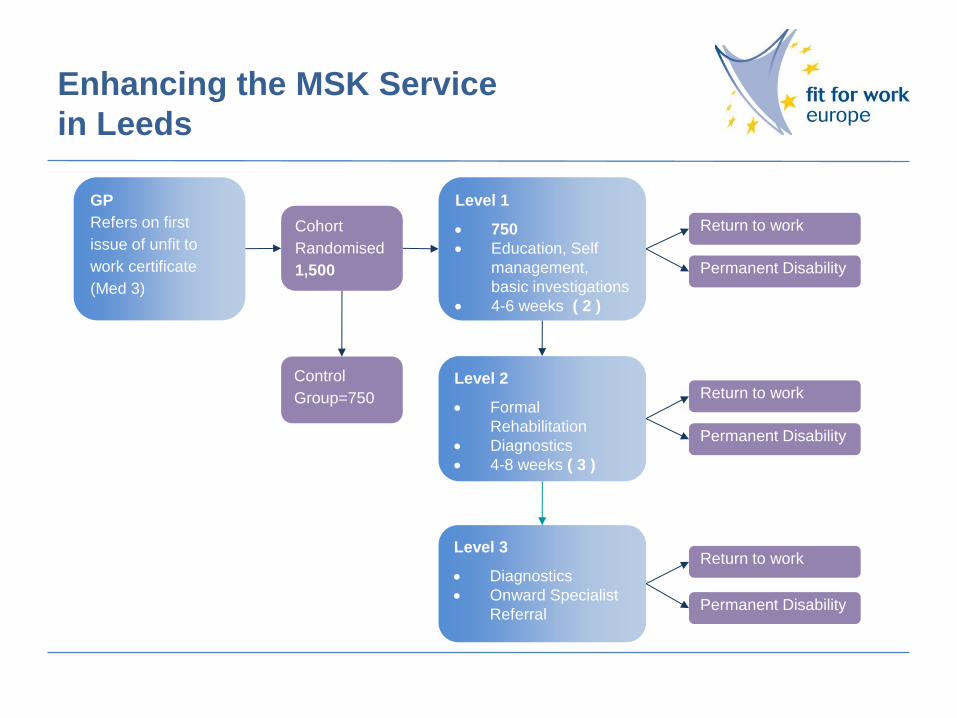
Enhancing the MSK Service
in Leeds
GP
Refers on first
issue of unfit to
work certificate
(Med 3)
Cohort
Randomised
1,500
Level 2
Formal
Rehabilitation
Diagnostics
4-8 weeks ( 3 )
Level 3
Diagnostics
Onward Specialist
Referral
Level 1
750
Education, Self
management,
basic investigations
4-6 weeks ( 2 )
Control
Group=750
Permanent Disability
Return to work
Permanent Disability
Return to work
Permanent Disability
Return to work

Enhancing the MSK Service in Leeds
Local-Buy In and Project Steering Group
• Service Enhancement Project Steering Group formed (supported by
the Director of Public Health, Dr Ian Cameron). A process of
stakeholder engagement undertaken to identify and confirm support
and contribution of the necessary collaborators to deliver project
• Managerial Representatives of Leeds Community Health Care Trust
• Transformational Lead for 3 CCGs in Leeds – Dr Chris Mills
• Clinical Lead: Dr Steve Brennan
• Academic Lead: Professor Paul Emery
• Project Lead: Rhonda Siddall
Project Phases
Phase I:
Configuring an enhanced service
Phase II:
Delivering an enhanced service
Phase III:
Assessing the value of an
enhanced service
Phase IV:
Producing the service
enhancement model template +
communicating the results
Phase II: Delivering an enhanced
service
Service Model:
• 6 dedicated clinics per week over 2-3 sites owned by Leeds
Community Healthcare Trust
• Clinics run by MSK Physician Steve Brennan (Leeds Community
Healthcare Trust)
• IT and Administrative Support Provided by Leeds Community
Healthcare Trust
• Service Data System compatible with GP system (System 1) via a
shared access agreement
Phase III: Assessing the value of
an enhanced service
• Project Period: 18 months
• Number of Patients: 750 (compared to control group of 750;
control managed by GPs)
• Process:
- Data Capture: Integrated System 1
- Interrogation and Analysis: done by Leeds Community Healthcare Trust and
Dr Steve Brennan
• Outcomes Assessed:
- Impact on temporary work disability (TD)
- Impact on permanent work disability (PD)
- Patient Satisfaction
- Impact on onward referral and investigation costs

Thank you for attending the Fit for Work
Summit 2013.
Follow us on Twitter @FfWEurope
Check our website www.fitforworkeurope.eu
Take a look at our blog www.blog.fitforworkeurope.eu