product guide - cyramzahcp.comcyramzahcp.com/img/pdf/cyramza_product_guide.pdf · product guide...
TRANSCRIPT

P R O D U C T G U I D E
WARNING: HEMORRHAGE, GASTROINTESTINAL PERFORATION, AND IMPAIRED WOUND HEALINGHemorrhage: CYRAMZA increased the risk of hemorrhage and gastrointestinal hemorrhage, including severe and sometimes fatal hemorrhagic events. Permanently discontinue CYRAMZA in patients who experience severe bleeding.Gastrointestinal Perforation: CYRAMZA can increase the risk of gastrointestinal perforation, a potentially fatal event. Permanently discontinue CYRAMZA in patients who experience a gastrointestinal perforation. Impaired Wound Healing: Impaired wound healing can occur with antibodies inhibiting the VEGF pathway. Discontinue CYRAMZA therapy in patients with impaired wound healing. Withhold CYRAMZA prior to surgery and discontinue CYRAMZA if a patient develops wound healing complications.
CYRAMZA® (ramucirumab) as a single agent, or in combination with paclitaxel, is indicated for the treatment of patients with advanced or metastatic gastric or gastroesophageal junction (GEJ) adenocarcinoma with disease progression on or after prior fluoropyrimidine- or platinum-containing chemotherapy.
CYRAMZA, in combination with docetaxel, is indicated for the treatment of patients with metastatic non-small cell lung cancer (NSCLC) with disease progression on or after platinum-based chemotherapy. Patients with epidermal growth factor receptor (EGFR) or anaplastic lymphoma kinase (ALK) genomic tumor aberrations should have disease progression on FDA-approved therapy for these aberrations prior to receiving CYRAMZA.
CYRAMZA, in combination with FOLFIRI (irinotecan, folinic acid, and 5-fluorouracil), is indicated for the treatment of patients with metastatic colorectal cancer (mCRC) with disease progression on or after prior therapy with bevacizumab, oxaliplatin, and a fluoropyrimidine.
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.

2
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
TA
BL
E O
F C
ON
TE
NT
SDosing and Administration ....................................................................................................... 3
CYRAMZA Overview ...................................................................................................... 10
Advanced Gastric and Gastroesophageal Junction (GEJ) Adenocarcinoma .............. 12
Metastatic Non-Small Cell Lung Cancer (mNSCLC) ................................................... 33
Metastatic Colorectal Cancer (mCRC) ......................................................................... 46
Lilly Resources ............................................................................................................ 55
Important Safety Information ..................................................................................... 57
3
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
DOSING AND ADMINISTRATION
RECOMMENDED DOSE
Treatment Regimen Interval Dosage Infusion Time
Monotherapy
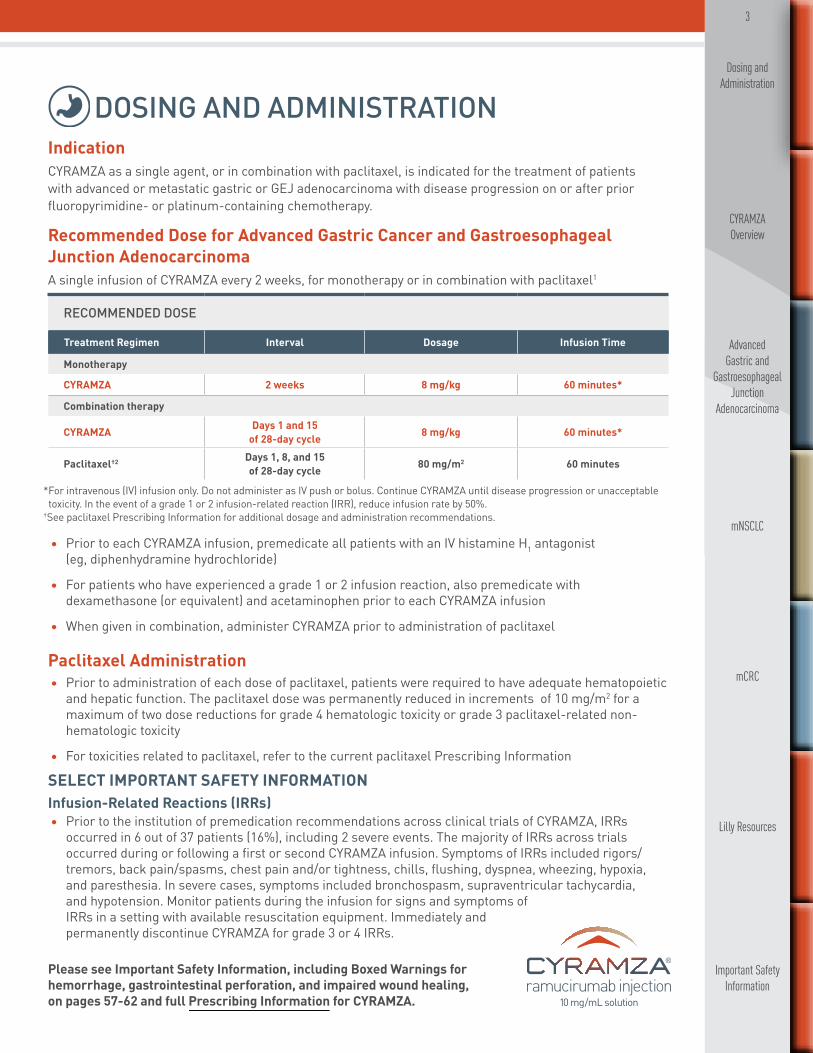
CYRAMZA 2 weeks 8 mg/kg 60 minutes*
Combination therapy
CYRAMZA Days 1 and 15 of 28-day cycle 8 mg/kg 60 minutes*
Paclitaxel†2 Days 1, 8, and 15 of 28-day cycle 80 mg/m2 60 minutes
SELECT IMPORTANT SAFETY INFORMATIONInfusion-Related Reactions (IRRs)• Prior to the institution of premedication recommendations across clinical trials of CYRAMZA, IRRs
occurred in 6 out of 37 patients (16%), including 2 severe events. The majority of IRRs across trials occurred during or following a first or second CYRAMZA infusion. Symptoms of IRRs included rigors/tremors, back pain/spasms, chest pain and/or tightness, chills, flushing, dyspnea, wheezing, hypoxia, and paresthesia. In severe cases, symptoms included bronchospasm, supraventricular tachycardia, and hypotension. Monitor patients during the infusion for signs and symptoms of IRRs in a setting with available resuscitation equipment. Immediately and permanently discontinue CYRAMZA for grade 3 or 4 IRRs.
IndicationCYRAMZA as a single agent, or in combination with paclitaxel, is indicated for the treatment of patients with advanced or metastatic gastric or GEJ adenocarcinoma with disease progression on or after prior fluoropyrimidine- or platinum-containing chemotherapy.
Recommended Dose for Advanced Gastric Cancer and Gastroesophageal Junction AdenocarcinomaA single infusion of CYRAMZA every 2 weeks, for monotherapy or in combination with paclitaxel1
* For intravenous (IV) infusion only. Do not administer as IV push or bolus. Continue CYRAMZA until disease progression or unacceptable toxicity. In the event of a grade 1 or 2 infusion-related reaction (IRR), reduce infusion rate by 50%.
†See paclitaxel Prescribing Information for additional dosage and administration recommendations.
• Prior to each CYRAMZA infusion, premedicate all patients with an IV histamine H1 antagonist (eg, diphenhydramine hydrochloride)
• For patients who have experienced a grade 1 or 2 infusion reaction, also premedicate with dexamethasone (or equivalent) and acetaminophen prior to each CYRAMZA infusion
• When given in combination, administer CYRAMZA prior to administration of paclitaxel
Paclitaxel Administration• Prior to administration of each dose of paclitaxel, patients were required to have adequate hematopoietic
and hepatic function. The paclitaxel dose was permanently reduced in increments of 10 mg/m2 for a maximum of two dose reductions for grade 4 hematologic toxicity or grade 3 paclitaxel-related non-hematologic toxicity
• For toxicities related to paclitaxel, refer to the current paclitaxel Prescribing Information

4
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
DOSING AND ADMINISTRATION, CONTINUED
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
EVENT DOSE MODIFICATIONS
Infusion-related reactions• Reduce infusion rate by 50% for grade 1 or 2• Permanently discontinue for grade 3 or 4
Hypertension• Interrupt CYRAMZA for severe hypertension until controlled with medical management• Permanently discontinue if severe hypertension cannot be controlled with
antihypertensive therapy
Proteinuria
• Interrupt CYRAMZA for urine protein levels ≥2 g/24 h. Reinitiate treatment at a reduced dose of 6 mg/kg every 2 weeks once the urine protein level returns to <2 g/24 h. If the protein level ≥2 g/24 h reoccurs, interrupt CYRAMZA and reduce the dose to 5 mg/kg every 2 weeks once the urine protein level returns to <2 g/24 h
• Permanently discontinue if urine protein level >3 g/24 h or in the setting of nephrotic syndrome
Wound healing complications • Interrupt CYRAMZA prior to scheduled surgery until the wound is fully healed
Arterial thromboembolic events • Permanently discontinue
Gastrointestinal perforation • Permanently discontinue
Grade 3 or 4 bleeding • Permanently discontinue
Dose Modifications for CYRAMZA1
SELECT IMPORTANT SAFETY INFORMATIONHemorrhage• CYRAMZA increased the risk of hemorrhage and gastrointestinal hemorrhage including severe and
sometimes fatal hemorrhagic events. In study 1, which evaluated CYRAMZA as a single agent in advanced gastric cancer, the incidence of severe bleeding was 3.4% for CYRAMZA and 2.6% for placebo. In study 2, which evaluated CYRAMZA plus paclitaxel in advanced gastric cancer, the incidence of severe bleeding was 4.3% for CYRAMZA plus paclitaxel and 2.4% for placebo plus paclitaxel. Patients with gastric cancer receiving nonsteroidal anti-inflammatory drugs (NSAIDs) were excluded from enrollment in studies 1 and 2; therefore, the risk of gastric hemorrhage in CYRAMZA-treated patients with gastric tumors receiving NSAIDs is unknown. In study 3, which evaluated CYRAMZA plus docetaxel in metastatic non-small cell lung cancer (NSCLC), the incidence of severe bleeding was 2.4% for CYRAMZA plus docetaxel and 2.3% for placebo plus docetaxel. Patients with NSCLC receiving therapeutic anticoagulation or chronic therapy with NSAIDs or other antiplatelet therapy other than once-daily aspirin or with radiographic evidence of major airway or blood vessel invasion or intratumor cavitation were excluded from study 3; therefore, the risk of pulmonary hemorrhage in these groups of patients is unknown. In study 4, which evaluated CYRAMZA plus FOLFIRI in metastatic colorectal cancer, the incidence of severe bleeding was 2.5% for CYRAMZA plus FOLFIRI and 1.7% for placebo plus FOLFIRI. Permanently discontinue CYRAMZA in patients who experience severe bleeding.
5
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
DOSING AND ADMINISTRATION, CONTINUED
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
RECOMMENDED DOSE
Treatment Regimen Interval Dosage Infusion Time
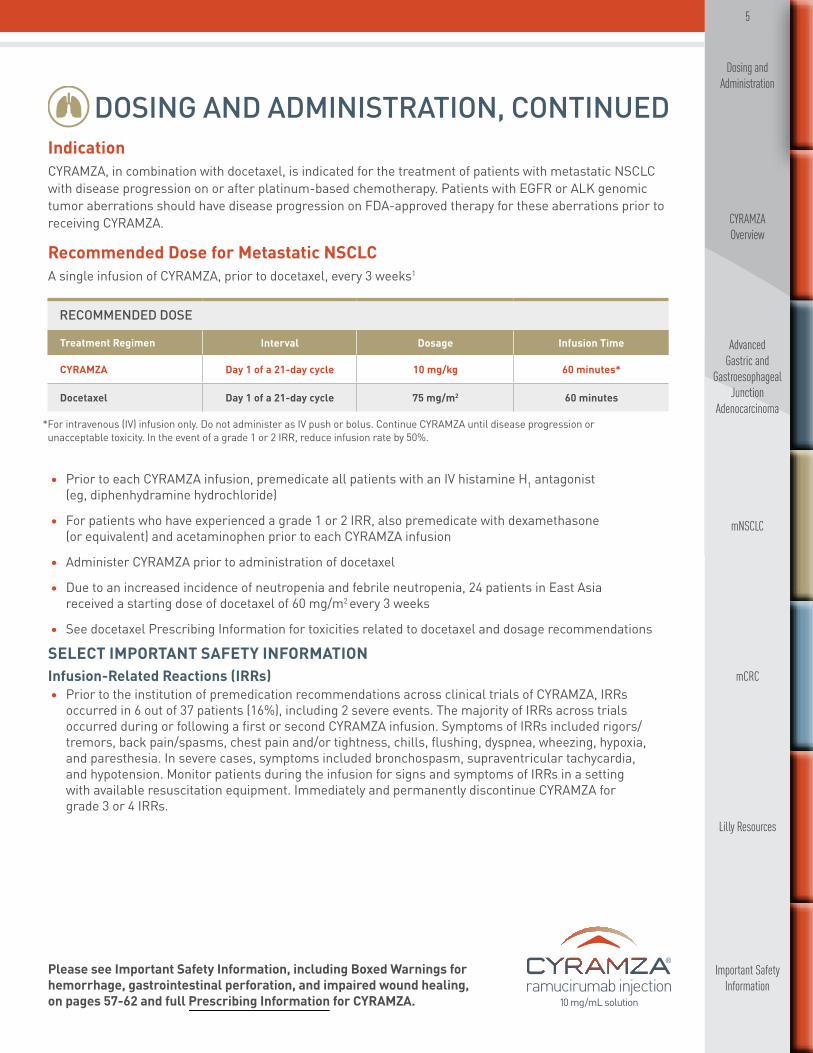
CYRAMZA Day 1 of a 21-day cycle 10 mg/kg 60 minutes*
Docetaxel Day 1 of a 21-day cycle 75 mg/m2 60 minutes
IndicationCYRAMZA, in combination with docetaxel, is indicated for the treatment of patients with metastatic NSCLC with disease progression on or after platinum-based chemotherapy. Patients with EGFR or ALK genomic tumor aberrations should have disease progression on FDA-approved therapy for these aberrations prior to receiving CYRAMZA.
Recommended Dose for Metastatic NSCLCA single infusion of CYRAMZA, prior to docetaxel, every 3 weeks1
* For intravenous (IV) infusion only. Do not administer as IV push or bolus. Continue CYRAMZA until disease progression or unacceptable toxicity. In the event of a grade 1 or 2 IRR, reduce infusion rate by 50%.
• Prior to each CYRAMZA infusion, premedicate all patients with an IV histamine H1 antagonist (eg, diphenhydramine hydrochloride)
• For patients who have experienced a grade 1 or 2 IRR, also premedicate with dexamethasone (or equivalent) and acetaminophen prior to each CYRAMZA infusion
• Administer CYRAMZA prior to administration of docetaxel
• Due to an increased incidence of neutropenia and febrile neutropenia, 24 patients in East Asia received a starting dose of docetaxel of 60 mg/m2 every 3 weeks
• See docetaxel Prescribing Information for toxicities related to docetaxel and dosage recommendations
SELECT IMPORTANT SAFETY INFORMATIONInfusion-Related Reactions (IRRs)• Prior to the institution of premedication recommendations across clinical trials of CYRAMZA, IRRs
occurred in 6 out of 37 patients (16%), including 2 severe events. The majority of IRRs across trials occurred during or following a first or second CYRAMZA infusion. Symptoms of IRRs included rigors/tremors, back pain/spasms, chest pain and/or tightness, chills, flushing, dyspnea, wheezing, hypoxia, and paresthesia. In severe cases, symptoms included bronchospasm, supraventricular tachycardia, and hypotension. Monitor patients during the infusion for signs and symptoms of IRRs in a setting with available resuscitation equipment. Immediately and permanently discontinue CYRAMZA for grade 3 or 4 IRRs.

6
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
DOSING AND ADMINISTRATION, CONTINUED
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
Dose Modifications for CYRAMZA1
EVENT DOSE MODIFICATIONS
Infusion-related reactions• Reduce the infusion rate by 50% for grade 1 or 2• Permanently discontinue for grade 3 or 4
Hypertension• Interrupt CYRAMZA for severe hypertension until controlled with medical management• Permanently discontinue if severe hypertension cannot be controlled with
antihypertensive therapy
Proteinuria
• Interrupt CYRAMZA for urine protein levels ≥2 g/24 h. Reinitiate treatment at a reduced dose of 8 mg/kg every 3 weeks once the urine protein level returns to <2 g/24 h. If the urine protein level ≥2 g/24 h reoccurs, interrupt CYRAMZA and reduce the dose to 6 mg/kg every 3 weeks once the urine protein level returns to <2 g/24 h
• Permanently discontinue if urine protein level >3 g/24 h or in the setting of nephrotic syndrome
Wound healing complications • Interrupt CYRAMZA prior to scheduled surgery until the wound is fully healed
Arterial thromboembolic events • Permanently discontinue
Gastrointestinal perforation • Permanently discontinue
Grade 3 or 4 bleeding • Permanently discontinue
SELECT IMPORTANT SAFETY INFORMATIONArterial Thromboembolic Events (ATEs)• Serious, sometimes fatal, ATEs including myocardial infarction, cardiac arrest, cerebrovascular accident,
and cerebral ischemia occurred in clinical trials including 1.7% of 236 patients who received CYRAMZA as a single agent for gastric cancer in study 1. Permanently discontinue CYRAMZA in patients who experience a severe ATE.
7
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
DOSING AND ADMINISTRATION, CONTINUED
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
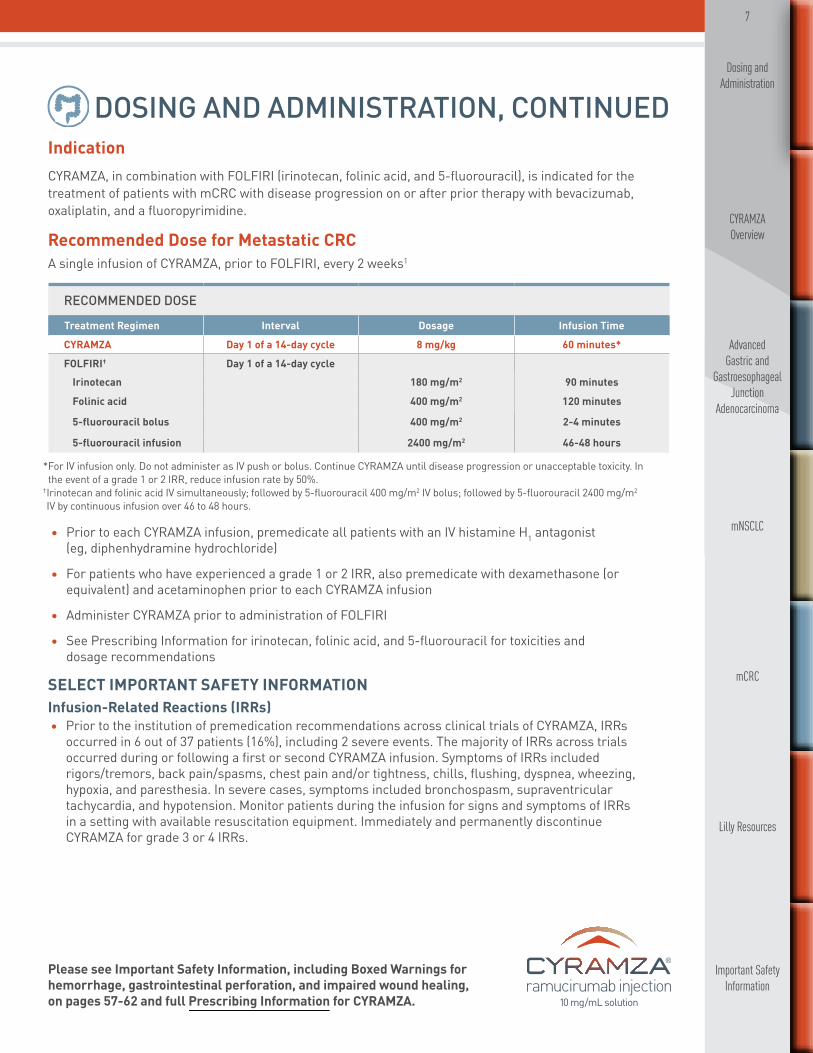
IndicationCYRAMZA, in combination with FOLFIRI (irinotecan, folinic acid, and 5-fluorouracil), is indicated for the treatment of patients with mCRC with disease progression on or after prior therapy with bevacizumab, oxaliplatin, and a fluoropyrimidine.
Recommended Dose for Metastatic CRCA single infusion of CYRAMZA, prior to FOLFIRI, every 2 weeks1
* For IV infusion only. Do not administer as IV push or bolus. Continue CYRAMZA until disease progression or unacceptable toxicity. In the event of a grade 1 or 2 IRR, reduce infusion rate by 50%.
† Irinotecan and folinic acid IV simultaneously; followed by 5-fluorouracil 400 mg/m2 IV bolus; followed by 5-fluorouracil 2400 mg/m2 IV by continuous infusion over 46 to 48 hours.
• Prior to each CYRAMZA infusion, premedicate all patients with an IV histamine H1 antagonist (eg, diphenhydramine hydrochloride)
• For patients who have experienced a grade 1 or 2 IRR, also premedicate with dexamethasone (or equivalent) and acetaminophen prior to each CYRAMZA infusion
• Administer CYRAMZA prior to administration of FOLFIRI
• See Prescribing Information for irinotecan, folinic acid, and 5-fluorouracil for toxicities and dosage recommendations
RECOMMENDED DOSE
Treatment Regimen Interval Dosage Infusion Time
CYRAMZA Day 1 of a 14-day cycle 8 mg/kg 60 minutes*
FOLFIRI† Day 1 of a 14-day cycleIrinotecan 180 mg/m2 90 minutes
Folinic acid 400 mg/m2 120 minutes
5-fluorouracil bolus 400 mg/m2 2-4 minutes
5-fluorouracil infusion 2400 mg/m2 46-48 hours
SELECT IMPORTANT SAFETY INFORMATIONInfusion-Related Reactions (IRRs)• Prior to the institution of premedication recommendations across clinical trials of CYRAMZA, IRRs
occurred in 6 out of 37 patients (16%), including 2 severe events. The majority of IRRs across trials occurred during or following a first or second CYRAMZA infusion. Symptoms of IRRs included rigors/tremors, back pain/spasms, chest pain and/or tightness, chills, flushing, dyspnea, wheezing, hypoxia, and paresthesia. In severe cases, symptoms included bronchospasm, supraventricular tachycardia, and hypotension. Monitor patients during the infusion for signs and symptoms of IRRs in a setting with available resuscitation equipment. Immediately and permanently discontinue CYRAMZA for grade 3 or 4 IRRs.

8
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
DOSING AND ADMINISTRATION, CONTINUED
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
Dose Modifications for CYRAMZA1
EVENT DOSE MODIFICATIONS
Infusion-related reactions• Reduce the infusion rate by 50% for grade 1 or 2• Permanently discontinue for grade 3 or 4
Hypertension• Interrupt CYRAMZA for severe hypertension until controlled with medical management• Permanently discontinue if severe hypertension cannot be controlled with
antihypertensive therapy
Proteinuria
• Interrupt CYRAMZA for urine protein levels ≥2 g/24 h. Reinitiate treatment at a reduced dose of 6 mg/kg every 2 weeks once the urine protein level returns to <2 g/24 h. If the urine protein level ≥2 g/24 h reoccurs, interrupt CYRAMZA and reduce the dose to 5 mg/kg every 2 weeks once the urine protein level returns to <2 g/24 h
• Permanently discontinue if urine protein level >3 g/24 h or in the setting of nephrotic syndrome
Wound healing complications • Interrupt CYRAMZA prior to scheduled surgery until the wound is fully healed
Arterial thromboembolic events • Permanently discontinue
Gastrointestinal perforation • Permanently discontinue
Grade 3 or 4 bleeding • Permanently discontinue
SELECT IMPORTANT SAFETY INFORMATIONHypertension• An increased incidence of severe hypertension occurred in patients receiving CYRAMZA as a single
agent (8%) as compared to placebo (3%), in patients receiving CYRAMZA plus paclitaxel (15%) as compared to placebo plus paclitaxel (3%), and in patients receiving CYRAMZA plus docetaxel (6%) as compared to placebo plus docetaxel (2%), and in patients receiving CYRAMZA plus FOLFIRI (11%) as compared to placebo plus FOLFIRI (3%). Control hypertension prior to initiating treatment with CYRAMZA. Monitor blood pressure every 2 weeks or more frequently as indicated during treatment. Temporarily suspend CYRAMZA for severe hypertension until medically controlled. Permanently discontinue CYRAMZA if medically significant hypertension cannot be controlled with antihypertensive therapy or in patients with hypertensive crisis or hypertensive encephalopathy.

9
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
1 Calculate the dose and required volume of CYRAMZA for infusion. Formula for dose calculation: Patient weight (kg) x Recommended dose (mg/kg) = Dose
• Vials contain either 100 mg/10 mL or 500 mg/50 mL at a concentration of 10 mg/mL solution of CYRAMZA
2 Inspect the vial
• Inspect vial contents for particulate matter and discoloration prior to dilution— CYRAMZA is a sterile, preservative-free, clear to slightly opalescent and colorless to slightly yellow solution
• If visible particulate matter or discolorations are seen, discard the vial
Step-by-step Preparation of the CYRAMZA InfusionUse aseptic technique to prepare the CYRAMZA infusion solution. Each vial is intended for single use only. The product contains no preservatives. Any unused product should be discarded.1
DOSING AND ADMINISTRATION, CONTINUED
4Administer the solution
• Visually inspect the diluted solution—If particulate matter or discolorations are seen, discard the solution
• Administer via infusion pump over 60 minutes through a separate infusion line. Use of a protein sparing 0.22 micron filter is recommended
• At the end of the infusion, flush the line with sterile sodium chloride (0.9%) solution for injection
3
Dilute the infusion solution. DO NOT FREEZE OR SHAKE the infusion solution
• Withdraw the required volume of CYRAMZA and further dilute with only 0.9% sodium chloride injection in an IV infusion container to a final volume of 250 mL —DO NOT use dextrose-containing solutions—DO NOT dilute with other solutions or co-infuse with other electrolyte medications
• Gently invert the IV container to ensure adequate mixing• Store diluted infusion for no more than 24 hours at 2°C to 8°C (36°F to 46°F) or 4 hours at room
temperature (below 25°C [77°F])• Discard vial with any unused portion of CYRAMZA
Storage RequirementsDO NOT FREEZE OR SHAKE1
• Store vials in a refrigerator at 2°C to 8°C (36°F to 46°F) until time of use• Protect from light—keep the vial in the outer carton• Store diluted infusion for no more than 24 hours at 2°C to 8°C (36°F to 46°F) or 4 hours at room
temperature (below 25°C [77°F])
SELECT IMPORTANT SAFETY INFORMATIONGastrointestinal Perforations• CYRAMZA is an antiangiogenic therapy that can increase the risk of gastrointestinal perforation, a
potentially fatal event. Four of 570 patients (0.7%) who received CYRAMZA as a single agent in advanced gastric cancer clinical trials experienced gastrointestinal perforation. In study 2, the incidence of gastrointestinal perforation was 1.2% for CYRAMZA plus paclitaxel as compared to 0.3% for placebo plus paclitaxel. In study 3, the incidence of gastrointestinal perforation was 1% for CYRAMZA plus docetaxel as compared to 0.3% for placebo plus docetaxel. In study 4, the incidence of gastrointestinal perforation was 1.7% for CYRAMZA plus FOLFIRI and 0.6% for placebo plus FOLFIRI. Permanently discontinue CYRAMZA in patients who experience a gastrointestinal perforation.

10
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
CYRAMZA OVERVIEW
* FDA standard NDC has been “zero-filled” to ensure creation of an 11-digit code that meets HIPAA standards. The zero-fill location is indicated in bold. NDC=National Drug Code; HIPAA=Health Insurance Portability and Accountability Act.
VIAL TYPE NDC*
100 mg/10 mL (10 mg/mL) 00002-7669-01
500 mg/50 mL (10 mg/mL) 00002-7678-01
Vials not actual size.
How SuppliedCYRAMZA is available in 100 mg/10 mL and 500 mg/50 mL (10 mg/mL) solution, single-dose vials.1
SELECT IMPORTANT SAFETY INFORMATIONImpaired Wound Healing• Impaired wound healing can occur with antibodies inhibiting the VEGF pathway. CYRAMZA has not
been studied in patients with serious or nonhealing wounds. CYRAMZA, an antiangiogenic therapy, has the potential to adversely affect wound healing. Discontinue CYRAMZA therapy in patients with impaired wound healing. Withhold CYRAMZA prior to surgery. Resume CYRAMZA following the surgical intervention based on clinical judgment of adequate wound healing. If a patient develops wound healing complications during therapy, discontinue CYRAMZA until the wound is fully healed.
11
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
CYRAMZA OVERVIEW, CONTINUED
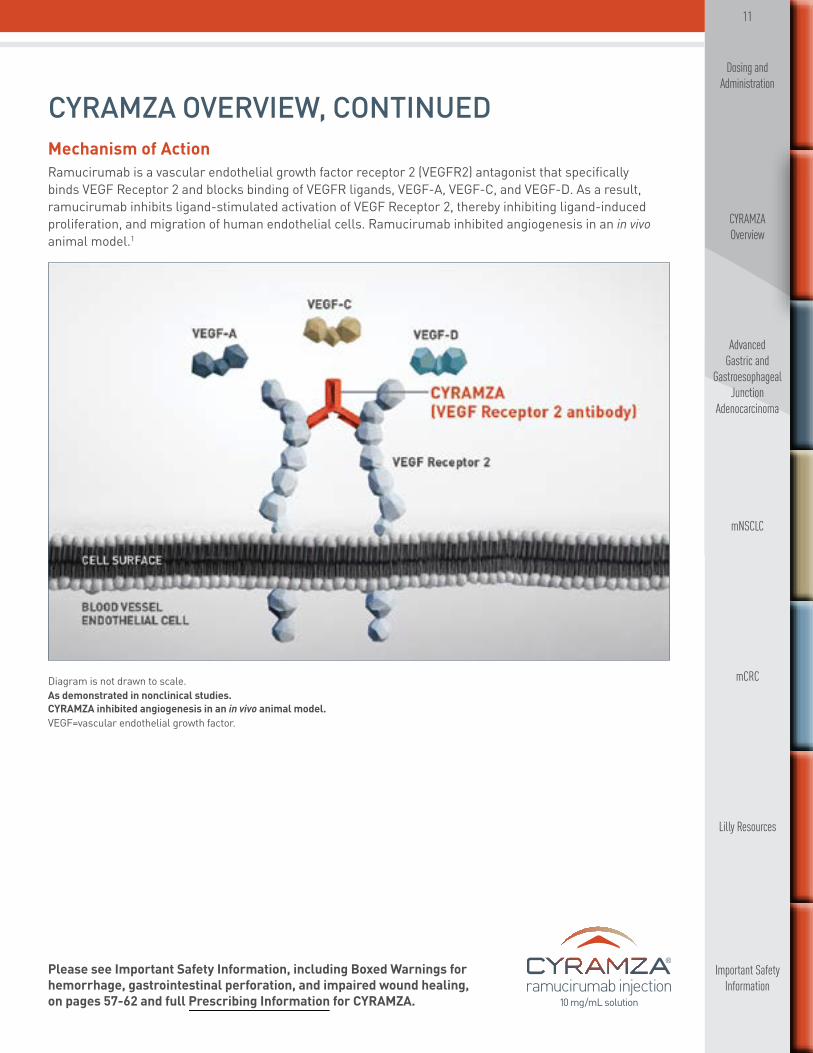
Diagram is not drawn to scale. As demonstrated in nonclinical studies. CYRAMZA inhibited angiogenesis in an in vivo animal model.VEGF=vascular endothelial growth factor.
Mechanism of ActionRamucirumab is a vascular endothelial growth factor receptor 2 (VEGFR2) antagonist that specifically binds VEGF Receptor 2 and blocks binding of VEGFR ligands, VEGF-A, VEGF-C, and VEGF-D. As a result, ramucirumab inhibits ligand-stimulated activation of VEGF Receptor 2, thereby inhibiting ligand-induced proliferation, and migration of human endothelial cells. Ramucirumab inhibited angiogenesis in an in vivo animal model.1
12
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
ADVANCED GASTRIC AND GASTROESOPHAGEAL JUNCTION ADENOCARCINOMA
IndicationCYRAMZA as a single agent, or in combination with paclitaxel, is indicated for the treatment of patients with advanced or metastatic gastric or GEJ adenocarcinoma with disease progression on or after prior fluoropyrimidine- or platinum-containing chemotherapy.
* Category 1 recommendation is based on high-level evidence and there is uniform NCCN consensus that the intervention is appropriate.NCCN Guidelines=NCCN Clinical Practice Guidelines in Oncology; NCCN=National Comprehensive Cancer Network.
Category 1 Recommendation*
Monotherapy Combination therapy
NCCN Guidelines® recommend single-agent ramucirumab (CYRAMZA) as a preferred second-line treatment option (with a category 1 recommendation) for locally advanced or metastatic gastric or GEJ adenocarcinoma.
NCCN Guidelines recommend ramucirumab (CYRAMZA) in combination with paclitaxel as a preferred second-line treatment option (with a category 1 recommendation) for locally advanced or metastatic gastric or GEJ adenocarcinoma.
SELECT IMPORTANT SAFETY INFORMATIONClinical Deterioration in Child-Pugh B or C Cirrhosis • Clinical deterioration, manifested by new onset or worsening encephalopathy, ascites, or hepatorenal
syndrome, was reported in patients with Child-Pugh B or C cirrhosis who received single-agent CYRAMZA. Use CYRAMZA in patients with Child-Pugh B or C cirrhosis only if the potential benefits of treatment are judged to outweigh the risks of clinical deterioration.
NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) Recommend ramucirumab (CYRAMZA) for Second-line Treatment of Locally Advanced or Metastatic Gastric and GEJ Adenocarcinoma3,4

13
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
ADVANCED GASTRIC AND GASTROESOPHAGEAL JUNCTION ADENOCARCINOMA, CONTINUED
SELECT IMPORTANT SAFETY INFORMATIONReversible Posterior Leukoencephalopathy Syndrome (RPLS)• RPLS has been reported at a rate of <0.1% in clinical studies with CYRAMZA. Confirm the diagnosis
of RPLS with MRI and discontinue CYRAMZA in patients who develop RPLS. Symptoms may resolve or improve within days, although some patients with RPLS can experience ongoing neurologic sequelae or death.
Proteinuria Including Nephrotic Syndrome • In study 4, severe proteinuria occurred more frequently in patients treated with CYRAMZA plus FOLFIRI
compared to patients receiving placebo plus FOLFIRI. Severe proteinuria was reported in 3% of patients treated with CYRAMZA plus FOLFIRI (including 3 cases [0.6%] of nephrotic syndrome) compared to 0.2% of patients treated with placebo plus FOLFIRI. Monitor proteinuria by urine dipstick and/or urinary protein creatinine ratio for the development of worsening of proteinuria during CYRAMZA therapy. Withhold CYRAMZA for urine protein levels that are ≥2 g over 24 hours. Reinitiate CYRAMZA at a reduced dose once the urine protein level returns to <2 g over 24 hours. Permanently discontinue CYRAMZA for urine protein levels >3 g over 24 hours or in the setting of nephrotic syndrome.
Placebo (n=117)Every 2 weeks + BSC
CYRAMZA monotherapy (n=238)8 mg/kg every 2 weeks (60-minute infusion) + BSC• Progression during treatment or within†:
− 4 months after last dose of first-line chemotherapy OR − 6 months after last dose of adjuvant chemotherapy
• ECOG PS 0-1
Locally Advanced or MetastaticGastric/GEJ Adenocarcinoma (N=355)
2:1Randomization‡
ECOG=Eastern Cooperative Oncology Group; PS=performance status; BSC=best supportive care. Major Efficacy Outcome Measure: Overall survival (OS). Supportive Efficacy Outcome Measure: Progression-free survival (PFS).
* Patients received prior platinum/fluoropyrimidine combination therapy (81%), fluoropyrimidine-containing regimens without platinum (15%), or platinum-containing regimens without fluoropyrimidine (4%).
†85% of patients received prior first-line chemotherapy for metastatic disease and 15% received prior adjuvant chemotherapy. ‡Stratification factors: weight loss over prior 3 months (≥10% vs <10%), geographic region, and location of primary tumor.
• For full inclusion and exclusion criteria, please see pages 19-21
REGARD Trial Design
REGARD: A phase III trial of single-agent CYRAMZA (N=355)1
A multicenter, randomized, placebo-controlled, double-blind trial of patients with locally advanced or metastatic gastric or GEJ adenocarcinoma previously treated with fluoropyrimidine- or platinum-containing chemotherapy.*1

14
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
ADVANCED GASTRIC AND GASTROESOPHAGEAL JUNCTION ADENOCARCINOMA, CONTINUED
REGARD Trial Design, Continued
Treatment monitoring and patient management• Patients had a urinalysis (UA) dipstick every 6 weeks5
• There was not a mandatory observation period after the CYRAMZA infusion to monitor for IRRs6 • The following were performed every 2 weeks (every infusion)7:
— Vital sign measurements, including temperature, pulse rate, respiration rate, and blood pressure (obtained before and at the completion of each infusion)
— Hematology profile (complete blood count with differential and platelet count) — Chemistry and liver function profiles (sodium, potassium, chloride, carbon dioxide, BUN, creatinine,
glucose, total protein, albumin, uric acid, AST, ALT, alkaline phosphatase, total bilirubin, lactate dehydrogenase, calcium, magnesium, and phosphorus)
— Toxicity/AE assessment — Physical examination — ECOG PS evaluation
• The following were additionally performed every 6 weeks7: — Coagulation profile (International Normalized Ratio [INR], prothrombin time, and partial
thromboplastin time [PTT]) — Urinalysis — Pregnancy test — Imaging studies/tumor assessments
• In the REGARD protocol, all subsequent doses were modified/reduced if dose modification/rate reduction was needed because of an IRR8
• For infusion-related reactions after giving dexamethasone and acetaminophen, protocols included9: — A grade 1 IRR did not require stopping the infusion — A grade 2 IRR the infusion was stopped, but the site could resume the infusion at 50% of the prior rate
once the infusion reaction had resolved or decreased to grade 1. The infusion duration could not have exceeded 2 hours
— For grade 3 or 4 IRRs, the infusion should be stopped and CYRAMZA permanently discontinued• For patients on CYRAMZA, major surgery (including major dental procedures) was postponed until at
least 28 days after the last dose of CYRAMZA (when possible) and CYRAMZA was not restarted for at least 28 days after surgery along with the wound being fully healed. If subcutaneous venous access device placement was required during the course of therapy, it was recommended that a 7-day treatment-free period occur both prior to and following placement10
SELECT IMPORTANT SAFETY INFORMATION Infusion-Related Reactions (IRRs) • Prior to the institution of premedication recommendations across clinical trials of CYRAMZA, IRRs
occurred in 6 out of 37 patients (16%), including 2 severe events. The majority of IRRs across trials occurred during or following a first or second CYRAMZA infusion. Symptoms of IRRs included rigors/tremors, back pain/spasms, chest pain and/or tightness, chills, flushing, dyspnea, wheezing, hypoxia, and paresthesia. In severe cases, symptoms included bronchospasm, supraventricular tachycardia, and hypotension. Monitor patients during the infusion for signs and symptoms of IRRs in a setting with available resuscitation equipment. Immediately and permanently discontinue CYRAMZA for grade 3 or 4 IRRs.

15
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
ADVANCED GASTRIC AND GASTROESOPHAGEAL JUNCTION ADENOCARCINOMA, CONTINUED
REGARD Patient Population
Demographic and baseline characteristics were similar between treatment arms in the REGARD trial1,11
SELECT IMPORTANT SAFETY INFORMATIONImpaired Wound Healing• Impaired wound healing can occur with antibodies inhibiting the VEGF pathway. CYRAMZA has not
been studied in patients with serious or nonhealing wounds. CYRAMZA, an antiangiogenic therapy, has the potential to adversely affect wound healing. Discontinue CYRAMZA therapy in patients with impaired wound healing. Withhold CYRAMZA prior to surgery. Resume CYRAMZA following the surgical intervention based on clinical judgment of adequate wound healing. If a patient develops wound healing complications during therapy, discontinue CYRAMZA until the wound is fully healed.
Thyroid Dysfunction• Monitor thyroid function during treatment with CYRAMZA. In study 4, the incidence of hypothyroidism
reported as an adverse event was 2.6% in the CYRAMZA plus FOLFIRI treated patients and 0.9% in the placebo plus FOLFIRI treated patients.
REGARD: DEMOGRAPHIC AND BASELINE CHARACTERISTICS
CYRAMZA (n=238)
Placebo (n=117)
Age, median (range) 60 (52-67) 60 (51-71)
Male 71% 68%
Caucasian 76% 78%
Previous line of chemotherapy
First-line 84% 88%
Adjuvant 16% 12%
ECOG PS
0 28% 26%
1 72% 73%
Measurable disease 92% 91%
Location of primary tumor
Gastric 75% 74%
GEJ 25% 26%

16
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
ADVANCED GASTRIC AND GASTROESOPHAGEAL JUNCTION ADENOCARCINOMA, CONTINUED
CI=confidence interval.
• The percentage of deaths at the time of analysis was 75% (179 patients) and 85% (99 patients) in the CYRAMZA and placebo arms, respectively
Placebo + paclitaxel(n=335)
CYRAMZA + paclitaxel (n=330)
1.0
0.8
0.6
0.4
0.2
0.0
PFS
PROB
ABIL
ITY
TIME FROM RANDOMIZATION (MONTHS)
70
34
8
104
50
6
188
124
4
259
214
2
330
335
0
43
21
10
28
12
12
15
8
14
11
5
16
7
3
18
3
3
20
1
3
22
-
24TIME FROM RANDOMIZATION (MONTHS)
86420 10 12 14 16 18 20 22 24 26 28
-
CYRAMZA + paclitaxelPlacebo+ paclitaxel
Number at Risk
CYRAMZA+ paclitaxelPlacebo+ paclitaxel
4.4CYRAMZA+ paclitaxel
(n=330)
2.9Placebo+ paclitaxel(n=335)
Supportive Outcome MeasureProgression-Free Survival:
Hazard Ratio=0.64 (0.54, 0.75); P<0.001
Median—Months (95% CI)
1.0
0.8
0.6
0.4
0.2
0.0
OS P
ROBA
BILI
TY
330
335
308
294
267
241
228
180
185
143
148
109
116
81
1
78
64
60
47
41
30
24
22
13
13
6
5
1
2
0
0
0
Number at Risk
CYRAMZA + paclitaxelPlacebo+ paclitaxel
CYRAMZA
Placebo+ paclitaxel
+ paclitaxel
9.6CYRAMZA+ paclitaxel
(n=330)
7.4Placebo+ paclitaxel(n=335)
Hazard Ratio=0.81 (0.68, 0.96); P=0.017
Major Outcome MeasureOverall Survival:
Median—Months (95% CI)
% ORR (COMPLETE + PARTIAL RESPONSE)
P<0.001
28%(23, 33)
0 20 40 60 80 100
16%(13, 20)
Supportive Outcome MeasureObjective Response Rate:
Percent of Patients (95% CI)
OS P
ROBA
BILI
TY
0 1 3 5 7 9 11 13 15 17 19 272 4 6 8 10 12 14 16 18 20 26 28
49154238 92 17 7 3 0 0117
CYRAMZAPlacebo 66 34 20 7 4 2
Number at Risk
0.0
0.2
0.4
0.6
0.8
CYRAMZAPlacebo
5.2MONTHS MONTHS
CYRAMZA(n=238)
3.8MONTHS Placebo
(n=117)
1.0
TIME FROM RANDOMIZATION (MONTHS)
Hazard Ratio=0.78 (0.60, 0.998); P=0.047
Major Outcome Measure Overall Survival:
Median—Months (95% CI)
Supportive Outcome MeasureProgression-Free Survival:
Median—Months (95% CI)
PFS
PROB
ABIL
ITY
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17
238 213 113 65 61 45 30 18 18 11 5 4 2 1 1 1 1 0117 92 27 11 7 4 2 2 2 2 2 1 1 0 0 0 0 0
CYRAMZAPlacebo
1.0
0.8
0.6
0.4
0.2
0.0
Hazard Ratio=0.48 (0.38, 0.62); P<0.001
TIME FROM RANDOMIZATION (MONTHS)
CYRAMZA Placebo
Number at Risk
1.3Placebo(n=117)
CYRAMZA(n=238)
2.1(4.4, 5.7)
(2.8, 4.7)
MONTHS(8.5, 10.8)
MONTHS(4.2, 5.3)
(1.5, 2.7)
MONTHS(6.3, 8.4)
MONTHS(2.8, 3.0)
(1.3, 1.4)MONTHS
REGARD Efficacy
CYRAMZA monotherapy significantly extended overall survival1
SELECT IMPORTANT SAFETY INFORMATIONEmbryofetal Toxicity• Based on its mechanism of action, CYRAMZA can cause fetal harm when administered to pregnant
women. Animal models link angiogenesis, VEGF, and VEGF Receptor 2 (VEGFR2) to critical aspects of female reproduction, embryofetal development, and postnatal development. Advise pregnant women of the potential risk to a fetus. Advise females of reproductive potential to use effective contraception during treatment with CYRAMZA and for at least 3 months after the last dose of CYRAMZA.
The phase III REGARD trial evaluated the efficacy and safety of CYRAMZA vs placebo in patients with locally advanced or metastatic gastric or GEJ adenocarcinoma with disease progression on or after prior fluoropyrimidine- or platinum-containing chemotherapy. Major efficacy outcome measure was OS. Supportive efficacy outcome measure was PFS. All patients were ECOG PS 0 or 1. Prior to enrollment, 85% of patients had progressed during treatment or within 4 months after the last dose of first-line chemotherapy for metastatic disease, and 15% of patients progressed during treatment or within 6 months after the last dose of adjuvant chemotherapy. Patients were randomized 2:1 to CYRAMZA 8 mg/kg every 2 weeks + BSC (n=238) or placebo + BSC (n=117).1
17
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
ADVANCED GASTRIC AND GASTROESOPHAGEAL JUNCTION ADENOCARCINOMA, CONTINUED
REGARD Efficacy, Continued
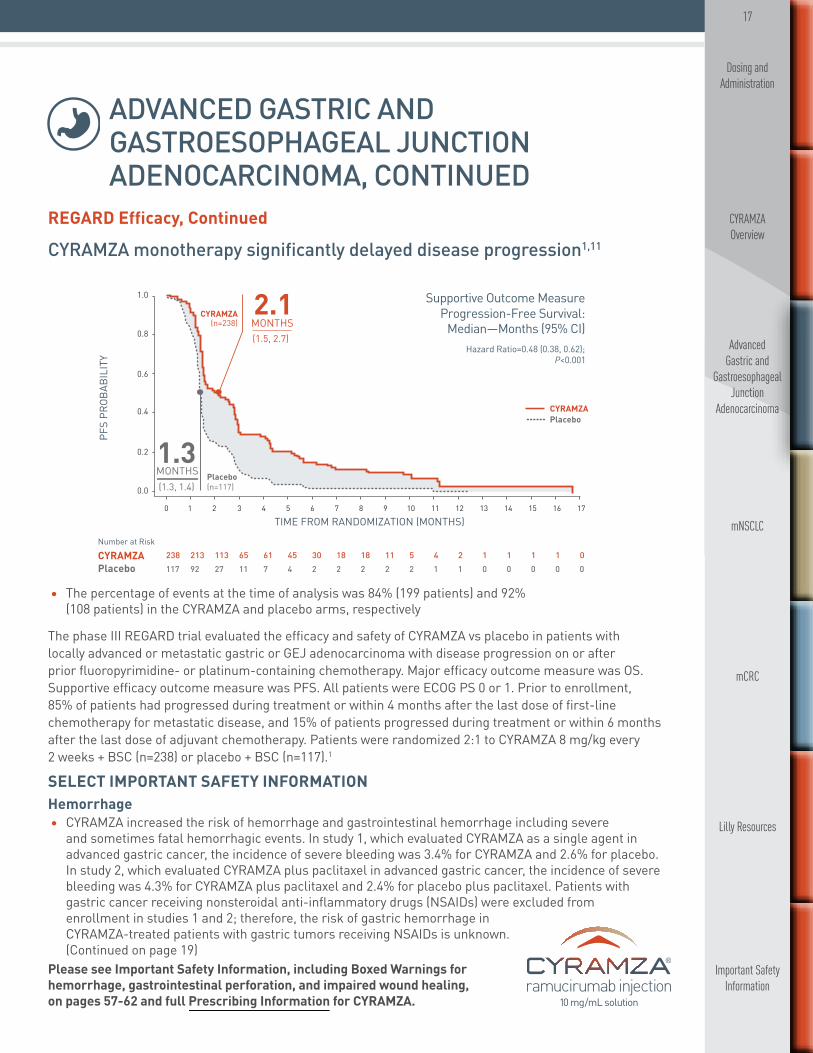
CYRAMZA monotherapy significantly delayed disease progression1,11
• The percentage of events at the time of analysis was 84% (199 patients) and 92% (108 patients) in the CYRAMZA and placebo arms, respectively
The phase III REGARD trial evaluated the efficacy and safety of CYRAMZA vs placebo in patients with locally advanced or metastatic gastric or GEJ adenocarcinoma with disease progression on or after prior fluoropyrimidine- or platinum-containing chemotherapy. Major efficacy outcome measure was OS. Supportive efficacy outcome measure was PFS. All patients were ECOG PS 0 or 1. Prior to enrollment, 85% of patients had progressed during treatment or within 4 months after the last dose of first-line chemotherapy for metastatic disease, and 15% of patients progressed during treatment or within 6 months after the last dose of adjuvant chemotherapy. Patients were randomized 2:1 to CYRAMZA 8 mg/kg every 2 weeks + BSC (n=238) or placebo + BSC (n=117).1
Placebo + paclitaxel(n=335)
CYRAMZA + paclitaxel (n=330)
1.0
0.8
0.6
0.4
0.2
0.0
PFS
PROB
ABIL
ITY
TIME FROM RANDOMIZATION (MONTHS)
70
34
8
104
50
6
188
124
4
259
214
2
330
335
0
43
21
10
28
12
12
15
8
14
11
5
16
7
3
18
3
3
20
1
3
22
-
24TIME FROM RANDOMIZATION (MONTHS)
86420 10 12 14 16 18 20 22 24 26 28
-
CYRAMZA + paclitaxelPlacebo+ paclitaxel
Number at Risk
CYRAMZA+ paclitaxelPlacebo+ paclitaxel
4.4CYRAMZA+ paclitaxel
(n=330)
2.9Placebo+ paclitaxel(n=335)
Supportive Outcome MeasureProgression-Free Survival:
Hazard Ratio=0.64 (0.54, 0.75); P<0.001
Median—Months (95% CI)
1.0
0.8
0.6
0.4
0.2
0.0
OS P
ROBA
BILI
TY
330
335
308
294
267
241
228
180
185
143
148
109
116
81
1
78
64
60
47
41
30
24
22
13
13
6
5
1
2
0
0
0
Number at Risk
CYRAMZA + paclitaxelPlacebo+ paclitaxel
CYRAMZA
Placebo+ paclitaxel
+ paclitaxel
9.6CYRAMZA+ paclitaxel
(n=330)
7.4Placebo+ paclitaxel(n=335)
Hazard Ratio=0.81 (0.68, 0.96); P=0.017
Major Outcome MeasureOverall Survival:
Median—Months (95% CI)
% ORR (COMPLETE + PARTIAL RESPONSE)
P<0.001
28%(23, 33)
0 20 40 60 80 100
16%(13, 20)
Supportive Outcome MeasureObjective Response Rate:
Percent of Patients (95% CI)
OS P
ROBA
BILI
TY
0 1 3 5 7 9 11 13 15 17 19 272 4 6 8 10 12 14 16 18 20 26 28
49154238 92 17 7 3 0 0117
CYRAMZAPlacebo 66 34 20 7 4 2
Number at Risk
0.0
0.2
0.4
0.6
0.8
CYRAMZAPlacebo
5.2MONTHS MONTHS
CYRAMZA(n=238)
3.8MONTHS Placebo
(n=117)
1.0
TIME FROM RANDOMIZATION (MONTHS)
Hazard Ratio=0.78 (0.60, 0.998); P=0.047
Major Outcome Measure Overall Survival:
Median—Months (95% CI)
Supportive Outcome MeasureProgression-Free Survival:
Median—Months (95% CI)
PFS
PROB
ABIL
ITY
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17
238 213 113 65 61 45 30 18 18 11 5 4 2 1 1 1 1 0117 92 27 11 7 4 2 2 2 2 2 1 1 0 0 0 0 0
CYRAMZAPlacebo
1.0
0.8
0.6
0.4
0.2
0.0
Hazard Ratio=0.48 (0.38, 0.62); P<0.001
TIME FROM RANDOMIZATION (MONTHS)
CYRAMZA Placebo
Number at Risk
1.3Placebo(n=117)
CYRAMZA(n=238)
2.1(4.4, 5.7)
(2.8, 4.7)
MONTHS(8.5, 10.8)
MONTHS(4.2, 5.3)
(1.5, 2.7)
MONTHS(6.3, 8.4)
MONTHS(2.8, 3.0)
(1.3, 1.4)MONTHS
SELECT IMPORTANT SAFETY INFORMATIONHemorrhage• CYRAMZA increased the risk of hemorrhage and gastrointestinal hemorrhage including severe
and sometimes fatal hemorrhagic events. In study 1, which evaluated CYRAMZA as a single agent in advanced gastric cancer, the incidence of severe bleeding was 3.4% for CYRAMZA and 2.6% for placebo. In study 2, which evaluated CYRAMZA plus paclitaxel in advanced gastric cancer, the incidence of severe bleeding was 4.3% for CYRAMZA plus paclitaxel and 2.4% for placebo plus paclitaxel. Patients with gastric cancer receiving nonsteroidal anti-inflammatory drugs (NSAIDs) were excluded from enrollment in studies 1 and 2; therefore, the risk of gastric hemorrhage in CYRAMZA-treated patients with gastric tumors receiving NSAIDs is unknown. (Continued on page 19)

18
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
ADVANCED GASTRIC AND GASTROESOPHAGEAL JUNCTION ADENOCARCINOMA, CONTINUED
SELECT IMPORTANT SAFETY INFORMATIONThe most common serious adverse events with CYRAMZA were anemia (3.8%) and intestinal obstruction (2.1%). Red blood cell transfusions were given to 11% of CYRAMZA-treated patients vs 8.7% of patients who received placebo. Clinically relevant adverse reactions reported in ≥1% and <5% of CYRAMZA-treated patients in the REGARD trial were: neutropenia (4.7% CYRAMZA vs 0.9% placebo), epistaxis (4.7% CYRAMZA vs 0.9% placebo), rash (4.2% CYRAMZA vs 1.7% placebo), intestinal obstruction (2.1% CYRAMZA vs 0% placebo), and ATEs (1.7% CYRAMZA vs 0% placebo). Across clinical trials of CYRAMZA administered as a single agent, clinically relevant adverse reactions (including grade ≥3) reported in CYRAMZA-treated patients included proteinuria, gastrointestinal perforation, and infusion-related reactions (IRRs). In the REGARD trial, according to laboratory assessment, 8% of CYRAMZA-treated patients developed proteinuria vs 3% of placebo-treated patients. Two patients discontinued CYRAMZA due to proteinuria. The rate of gastrointestinal perforation in the REGARD trial was 0.8% and the rate of IRRs was 0.4%.
Adverse Reaction Profile for CYRAMZA Monotherapy1
REGARD: ADVERSE REACTIONS OCCURRING WITH CYRAMZA AT INCIDENCE RATE ≥5% AND ≥2% HIGHER THAN PLACEBO
ALL GRADES GRADE 3/4
Adverse ReactionsCYRAMZA 8 mg/kg (n=236)
Placebo (n=115)
CYRAMZA 8 mg/kg (n=236)
Placebo (n=115)
Hypertension 16% 8% 8% 3%
Diarrhea 14% 9% 1% 2%
Headache 9% 3% 0% 0%
Hyponatremia 6% 2% 3% 1%
• The most common adverse reactions (all grades) observed in CYRAMZA-treated patients at a rate ≥10% and ≥2% higher than placebo in the REGARD trial were hypertension (16% vs 8%) and diarrhea (14% vs 9%)
• Red blood cell transfusions were given to 11% of CYRAMZA-treated patients vs 8.7% of patients who received placebo

19
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
ADVANCED GASTRIC AND GASTROESOPHAGEAL JUNCTION ADENOCARCINOMA, CONTINUED
REGARD Trial Inclusion Criteria12
Each patient must have met the following criteria to be enrolled in this study:1. Histologically- or cytologically-confirmed gastric carcinoma, including gastric adenocarcinoma or GEJ
adenocarcinoma (patients with adenocarcinoma of the distal esophagus were eligible if the primary tumor involved the GEJ)
2. Metastatic disease or locally recurrent, unresectable disease with measurable lymph node metastases • Nonregional lymph node metastases were eligible; lymph node metastases must have been measurable as defined by the Response Evaluation Criteria in Solid Tumors (RECIST)
• Locally recurrent, unresectable disease was eligible if there were at least one measurable lymph node metastasis (regional or nonregional) as defined by RECIST
• Received prior radiation therapy, measurable or evaluable lesions must have been outside the radiation field, or (for lesions within the radiation field) there must have been documented progression following radiation therapy
3. Measurable disease and/or evaluable disease. Measurable disease was defined as at least one unidimensionally measurable target lesion (≥20 mm with conventional techniques or ≥10 mm by spiral CT), as defined by RECIST. Examples of evaluable, nonmeasurable disease include gastric, peritoneal, or mesenteric thickening in areas of known disease, or peritoneal nodules that were too small to be considered measurable by RECIST
4. Experienced disease progression during or within 4 months after the last dose of first-line therapy for metastatic disease, or during or within 6 months after the last dose of adjuvant therapy
• Acceptable first-line regimens for this study were combination chemotherapy regimens that included platinum or fluoropyrimidine components (acceptable prior platinum agents were cisplatin, carboplatin, or oxaliplatin; acceptable prior fluoropyrimidine agents were 5-FU, capecitabine, or S-1)
• Elevations in CEA or other tumor markers without radiographic evidence of progression did not constitute satisfactory evidence of progression on first-line therapy
• Intolerant to first-line chemotherapy regimens were eligible provided there was disease progression within 4 months after the last dose of first-line therapy
• Had one or more component(s) of first-line chemotherapy discontinued because of toxicity, but continued to receive the other component(s) of first-line therapy (eg, a FOLFOX regimen in which the oxaliplatin was stopped and the 5-FU/leucovorin was continued), were eligible following disease progression
• Prior adjuvant therapy was permitted, and patients with disease progression during adjuvant chemotherapy were eligible, provided that disease progression occurred within 6 months after the completion of adjuvant therapy. Patients who experienced disease progression more than 6 months after the last dose of adjuvant therapy should have received first-line therapy for metastatic disease, with subsequent progression on first-line therapy a requirement for eligibility
SELECT IMPORTANT SAFETY INFORMATIONHemorrhage, Continued • In study 3, which evaluated CYRAMZA plus docetaxel in metastatic non-small cell lung cancer (NSCLC),
the incidence of severe bleeding was 2.4% for CYRAMZA plus docetaxel and 2.3% for placebo plus docetaxel. Patients with NSCLC receiving therapeutic anticoagulation or chronic therapy with NSAIDs or other antiplatelet therapy other than once-daily aspirin or with radiographic evidence of major airway or blood vessel invasion or intratumor cavitation were excluded from study 3; therefore, the risk of pulmonary hemorrhage in these groups of patients is unknown. In study 4, which evaluated CYRAMZA plus FOLFIRI in metastatic colorectal cancer, the incidence of severe bleeding was 2.5% for CYRAMZA plus FOLFIRI and 1.7% for placebo plus FOLFIRI. Permanently discontinue CYRAMZA in patients who experience severe bleeding.
20
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
ADVANCED GASTRIC AND GASTROESOPHAGEAL JUNCTION ADENOCARCINOMA, CONTINUED
REGARD Trial Inclusion Criteria, Continued12
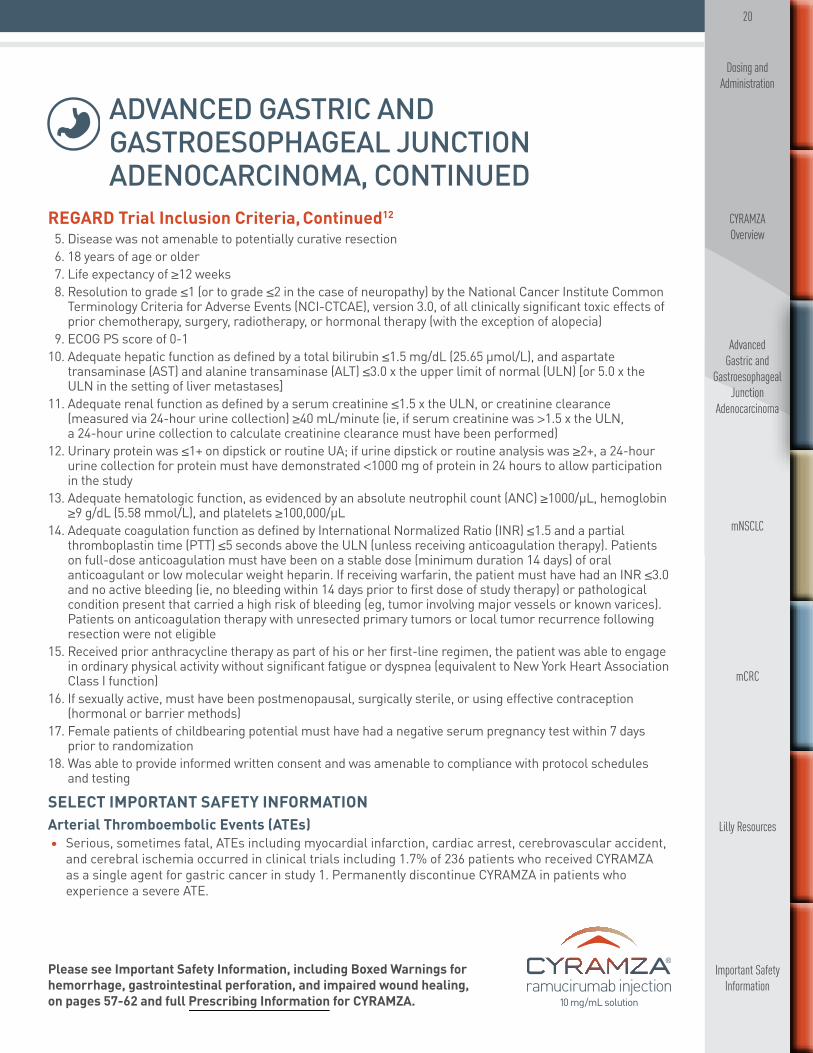
5. Disease was not amenable to potentially curative resection6. 18 years of age or older7. Life expectancy of ≥12 weeks 8. Resolution to grade ≤1 (or to grade ≤2 in the case of neuropathy) by the National Cancer Institute Common
Terminology Criteria for Adverse Events (NCI-CTCAE), version 3.0, of all clinically significant toxic effects of prior chemotherapy, surgery, radiotherapy, or hormonal therapy (with the exception of alopecia)
9. ECOG PS score of 0-110. Adequate hepatic function as defined by a total bilirubin ≤1.5 mg/dL (25.65 μmol/L), and aspartate
transaminase (AST) and alanine transaminase (ALT) ≤3.0 x the upper limit of normal (ULN) [or 5.0 x the ULN in the setting of liver metastases]
11. Adequate renal function as defined by a serum creatinine ≤1.5 x the ULN, or creatinine clearance (measured via 24-hour urine collection) ≥40 mL/minute (ie, if serum creatinine was >1.5 x the ULN, a 24-hour urine collection to calculate creatinine clearance must have been performed)
12. Urinary protein was ≤1+ on dipstick or routine UA; if urine dipstick or routine analysis was ≥2+, a 24-hour urine collection for protein must have demonstrated <1000 mg of protein in 24 hours to allow participation in the study
13. Adequate hematologic function, as evidenced by an absolute neutrophil count (ANC) ≥1000/μL, hemoglobin ≥9 g/dL (5.58 mmol/L), and platelets ≥100,000/μL
14. Adequate coagulation function as defined by International Normalized Ratio (INR) ≤1.5 and a partial thromboplastin time (PTT) ≤5 seconds above the ULN (unless receiving anticoagulation therapy). Patients on full-dose anticoagulation must have been on a stable dose (minimum duration 14 days) of oral anticoagulant or low molecular weight heparin. If receiving warfarin, the patient must have had an INR ≤3.0 and no active bleeding (ie, no bleeding within 14 days prior to first dose of study therapy) or pathological condition present that carried a high risk of bleeding (eg, tumor involving major vessels or known varices). Patients on anticoagulation therapy with unresected primary tumors or local tumor recurrence following resection were not eligible
15. Received prior anthracycline therapy as part of his or her first-line regimen, the patient was able to engage in ordinary physical activity without significant fatigue or dyspnea (equivalent to New York Heart Association Class I function)
16. If sexually active, must have been postmenopausal, surgically sterile, or using effective contraception (hormonal or barrier methods)
17. Female patients of childbearing potential must have had a negative serum pregnancy test within 7 days prior to randomization
18. Was able to provide informed written consent and was amenable to compliance with protocol schedules and testing
SELECT IMPORTANT SAFETY INFORMATION Arterial Thromboembolic Events (ATEs)• Serious, sometimes fatal, ATEs including myocardial infarction, cardiac arrest, cerebrovascular accident,
and cerebral ischemia occurred in clinical trials including 1.7% of 236 patients who received CYRAMZA as a single agent for gastric cancer in study 1. Permanently discontinue CYRAMZA in patients who experience a severe ATE.
21
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
ADVANCED GASTRIC AND GASTROESOPHAGEAL JUNCTION ADENOCARCINOMA, CONTINUED
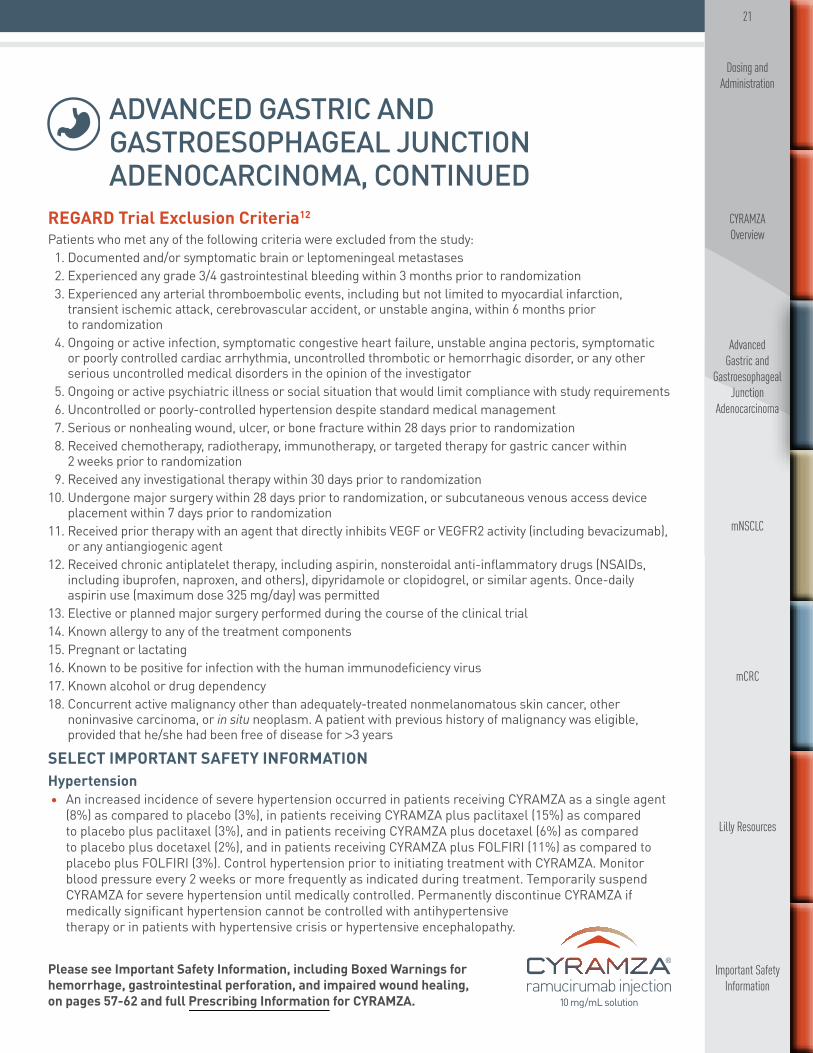
REGARD Trial Exclusion Criteria12
Patients who met any of the following criteria were excluded from the study:1. Documented and/or symptomatic brain or leptomeningeal metastases2. Experienced any grade 3/4 gastrointestinal bleeding within 3 months prior to randomization3. Experienced any arterial thromboembolic events, including but not limited to myocardial infarction,
transient ischemic attack, cerebrovascular accident, or unstable angina, within 6 months prior to randomization
4. Ongoing or active infection, symptomatic congestive heart failure, unstable angina pectoris, symptomatic or poorly controlled cardiac arrhythmia, uncontrolled thrombotic or hemorrhagic disorder, or any other serious uncontrolled medical disorders in the opinion of the investigator
5. Ongoing or active psychiatric illness or social situation that would limit compliance with study requirements6. Uncontrolled or poorly-controlled hypertension despite standard medical management7. Serious or nonhealing wound, ulcer, or bone fracture within 28 days prior to randomization8. Received chemotherapy, radiotherapy, immunotherapy, or targeted therapy for gastric cancer within
2 weeks prior to randomization9. Received any investigational therapy within 30 days prior to randomization
10. Undergone major surgery within 28 days prior to randomization, or subcutaneous venous access device placement within 7 days prior to randomization
11. Received prior therapy with an agent that directly inhibits VEGF or VEGFR2 activity (including bevacizumab), or any antiangiogenic agent
12. Received chronic antiplatelet therapy, including aspirin, nonsteroidal anti-inflammatory drugs (NSAIDs, including ibuprofen, naproxen, and others), dipyridamole or clopidogrel, or similar agents. Once-daily aspirin use (maximum dose 325 mg/day) was permitted
13. Elective or planned major surgery performed during the course of the clinical trial14. Known allergy to any of the treatment components15. Pregnant or lactating16. Known to be positive for infection with the human immunodeficiency virus17. Known alcohol or drug dependency18. Concurrent active malignancy other than adequately-treated nonmelanomatous skin cancer, other
noninvasive carcinoma, or in situ neoplasm. A patient with previous history of malignancy was eligible, provided that he/she had been free of disease for >3 years
SELECT IMPORTANT SAFETY INFORMATIONHypertension• An increased incidence of severe hypertension occurred in patients receiving CYRAMZA as a single agent
(8%) as compared to placebo (3%), in patients receiving CYRAMZA plus paclitaxel (15%) as compared to placebo plus paclitaxel (3%), and in patients receiving CYRAMZA plus docetaxel (6%) as compared to placebo plus docetaxel (2%), and in patients receiving CYRAMZA plus FOLFIRI (11%) as compared to placebo plus FOLFIRI (3%). Control hypertension prior to initiating treatment with CYRAMZA. Monitor blood pressure every 2 weeks or more frequently as indicated during treatment. Temporarily suspend CYRAMZA for severe hypertension until medically controlled. Permanently discontinue CYRAMZA if medically significant hypertension cannot be controlled with antihypertensive therapy or in patients with hypertensive crisis or hypertensive encephalopathy.

22
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
ADVANCED GASTRIC AND GASTROESOPHAGEAL JUNCTION ADENOCARCINOMA, CONTINUED
1:1Randomization†
• Progression during treatment or within 4 months after last dose of first-line fluoropyrimidine- and platinum-containing regimen*
• ECOG PS 0-1
Locally Advanced or MetastaticGastric/GEJ Adenocarcinoma (N=665)
CYRAMZA + paclitaxel(n=330)
28-day cycle
CYRAMZA 8 mg/kg days 1, 15 + paclitaxel 80 mg/m2 days 1, 8, 15
Placebo days 1, 15+ paclitaxel 80 mg/m2 days 1, 8, 15 28-day cycle
Placebo + paclitaxel(n=335)
Major efficacy outcome measure: overall survival (OS). Supportive efficacy outcome measures: progression-free survival (PFS), objective response rate (ORR). Patients received treatment until disease progression or unacceptable toxicity.
* 75% of patients randomized in the study received prior platinum/fluoropyrimidine combination therapy without anthracycline; 25% received platinum/fluoropyrimidine combination therapy with anthracycline.
† Stratification factors were geographic region, time to progression on first-line therapy (<6 months vs ≥6 months), and disease measurability (measurable vs nonmeasurable disease).
• For full inclusion and exclusion criteria, please see pages 29-32
RAINBOW Trial Design
RAINBOW: A phase III trial of CYRAMZA in combination with paclitaxel as second-line therapy for locally advanced or metastatic gastric cancer (N=665)1,13
A large, multicenter, randomized, double-blind trial of patients with locally advanced or metastatic gastric or GEJ adenocarcinoma previously treated with fluoropyrimidine- and platinum-containing chemotherapy.*13
SELECT IMPORTANT SAFETY INFORMATIONInfusion-Related Reactions (IRRs)• Prior to the institution of premedication recommendations across clinical trials of CYRAMZA, IRRs
occurred in 6 out of 37 patients (16%), including 2 severe events. The majority of IRRs across trials occurred during or following a first or second CYRAMZA infusion. Symptoms of IRRs included rigors/tremors, back pain/spasms, chest pain and/or tightness, chills, flushing, dyspnea, wheezing, hypoxia, and paresthesia. In severe cases, symptoms included bronchospasm, supraventricular tachycardia, and hypotension. Monitor patients during the infusion for signs and symptoms of IRRs in a setting with available resuscitation equipment. Immediately and permanently discontinue CYRAMZA for grade 3 or 4 IRRs.

23
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
ADVANCED GASTRIC AND GASTROESOPHAGEAL JUNCTION ADENOCARCINOMA, CONTINUED
RAINBOW Trial Design, Continued
Treatment monitoring and patient management• A UA dipstick was performed every 2 weeks. If a patient had proteinuria ≥2+, a 24-hour urine collection
was conducted per the protocol14
• There was a mandatory 60-minute observation period after the first two infusions of CYRAMZA to monitor for IRRs. The observation period was eliminated from further infusions if there was no evidence of an IRR15
• At every infusion, the following were performed16: — Vital signs — Hematology profile (complete blood count with differential, white blood cell count, and platelet count) — Liver function profile (ALT, AST, bilirubin) — A urinalysis was required on days 1 and 15 only
• On day 1 of each new cycle, the following were performed16: — Physical examination — ECOG PS evaluation — Chemistry profile (sodium, potassium, blood urea nitrogen, phosphorous, creatinine, glucose, total
protein, albumin, uric acid, AST, ALT, alkaline phosphatase, total bilirubin, lactate dehydrogenase, calcium, and magnesium)
• Every 2 cycles, the following were performed16: — Pregnancy test — Coagulation profile (INR or PT, and PTT) — Heart monitoring (ECG and echocardiogram)
• Every 6 weeks, the imaging studies/tumor assessments were completed16
• In the RAINBOW protocol, all subsequent doses were modified/reduced if dose modification/rate reduction was needed because of an IRR8
• For infusion-related reactions after giving dexamethasone and acetaminophen, protocols included9: — A grade 1 IRR did not require stopping the infusion — A grade 2 IRR the infusion was stopped, but the site could resume the infusion at 50% of the prior rate
once the infusion reaction had resolved or decreased to grade 1. The infusion duration could not have exceeded 2 hours
— For grade 3 or 4 IRRs, the infusion should be stopped and CYRAMZA permanently discontinued• For patients on CYRAMZA, major surgery (including major dental procedures) was postponed until at
least 28 days after the last dose of CYRAMZA (when possible) and CYRAMZA was not restarted for at least 28 days after surgery along with the wound being fully healed. If subcutaneous venous access device placement was required during the course of therapy, it was recommended that a 7-day treatment-free period occur both prior to and following placement10
SELECT IMPORTANT SAFETY INFORMATIONImpaired Wound Healing• Impaired wound healing can occur with antibodies inhibiting the VEGF pathway. CYRAMZA has not been
studied in patients with serious or nonhealing wounds. CYRAMZA, an antiangiogenic therapy, has the potential to adversely affect wound healing. Discontinue CYRAMZA therapy in patients with impaired wound healing. Withhold CYRAMZA prior to surgery. (Continued on next page)

24
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
ADVANCED GASTRIC AND GASTROESOPHAGEAL JUNCTION ADENOCARCINOMA, CONTINUED
* By self-report.
RAINBOW Patient Population
Demographic and baseline characteristics were similar between treatment arms1,13,17
RAINBOW: DEMOGRAPHIC AND BASELINE CHARACTERISTICS
CYRAMZA + paclitaxel
(n=330)
Placebo + paclitaxel
(n=335)
Age, median (range) 61 (25-83) 61 (24-84)
Male 69% 73%
Ethnic origin*
Caucasian 63% 59%
Asian 33% 36%
Black or other 4% 4%
Previous line of chemotherapy
First-line 100% 100%
Adjuvant 9% 10%
ECOG PS
0 35% 43%
1 65% 57%
Measurable disease 81% 81%
Location of primary tumor
Gastric 80% 79%
GEJ 20% 21%
SELECT IMPORTANT SAFETY INFORMATIONImpaired Wound Healing, Continued• Resume CYRAMZA following the surgical intervention based on clinical judgment of adequate wound
healing. If a patient develops wound healing complications during therapy, discontinue CYRAMZA until the wound is fully healed.

25
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
ADVANCED GASTRIC AND GASTROESOPHAGEAL JUNCTION ADENOCARCINOMA, CONTINUED
RAINBOW Efficacy
CYRAMZA plus paclitaxel significantly extended overall survival1
• The percentage of deaths at the time of analysis was 78% (256 patients) and 78% (260 patients) in the CYRAMZA plus paclitaxel and placebo plus paclitaxel treatment arms, respectively
Placebo + paclitaxel(n=335)
CYRAMZA + paclitaxel (n=330)
1.0
0.8
0.6
0.4
0.2
0.0
PFS
PROB
ABIL
ITY
TIME FROM RANDOMIZATION (MONTHS)
70
34
8
104
50
6
188
124
4
259
214
2
330
335
0
43
21
10
28
12
12
15
8
14
11
5
16
7
3
18
3
3
20
1
3
22
-
24TIME FROM RANDOMIZATION (MONTHS)
86420 10 12 14 16 18 20 22 24 26 28
-
CYRAMZA + paclitaxelPlacebo+ paclitaxel
Number at Risk
CYRAMZA+ paclitaxelPlacebo+ paclitaxel
4.4CYRAMZA+ paclitaxel
(n=330)
2.9Placebo+ paclitaxel(n=335)
Supportive Outcome MeasureProgression-Free Survival:
Hazard Ratio=0.64 (0.54, 0.75); P<0.001
Median—Months (95% CI)
1.0
0.8
0.6
0.4
0.2
0.0
OS P
ROBA
BILI
TY
330
335
308
294
267
241
228
180
185
143
148
109
116
81
1
78
64
60
47
41
30
24
22
13
13
6
5
1
2
0
0
0
Number at Risk
CYRAMZA + paclitaxelPlacebo+ paclitaxel
CYRAMZA
Placebo+ paclitaxel
+ paclitaxel
9.6CYRAMZA+ paclitaxel
(n=330)
7.4Placebo+ paclitaxel(n=335)
Hazard Ratio=0.81 (0.68, 0.96); P=0.017
Major Outcome MeasureOverall Survival:
Median—Months (95% CI)
% ORR (COMPLETE + PARTIAL RESPONSE)
P<0.001
28%(23, 33)
0 20 40 60 80 100
16%(13, 20)
Supportive Outcome MeasureObjective Response Rate:
Percent of Patients (95% CI)
OS P
ROBA
BILI
TY
0 1 3 5 7 9 11 13 15 17 19 272 4 6 8 10 12 14 16 18 20 26 28
49154238 92 17 7 3 0 0117
CYRAMZAPlacebo 66 34 20 7 4 2
Number at Risk
0.0
0.2
0.4
0.6
0.8
CYRAMZAPlacebo
5.2MONTHS MONTHS
CYRAMZA(n=238)
3.8MONTHS Placebo
(n=117)
1.0
TIME FROM RANDOMIZATION (MONTHS)
Hazard Ratio=0.78 (0.60, 0.998); P=0.047
Major Outcome Measure Overall Survival:
Median—Months (95% CI)
Supportive Outcome MeasureProgression-Free Survival:
Median—Months (95% CI)
PFS
PROB
ABIL
ITY
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17
238 213 113 65 61 45 30 18 18 11 5 4 2 1 1 1 1 0117 92 27 11 7 4 2 2 2 2 2 1 1 0 0 0 0 0
CYRAMZAPlacebo
1.0
0.8
0.6
0.4
0.2
0.0
Hazard Ratio=0.48 (0.38, 0.62); P<0.001
TIME FROM RANDOMIZATION (MONTHS)
CYRAMZA Placebo
Number at Risk
1.3Placebo(n=117)
CYRAMZA(n=238)
2.1(4.4, 5.7)
(2.8, 4.7)
MONTHS(8.5, 10.8)
MONTHS(4.2, 5.3)
(1.5, 2.7)
MONTHS(6.3, 8.4)
MONTHS(2.8, 3.0)
(1.3, 1.4)MONTHS
The phase III RAINBOW trial evaluated the efficacy and safety of CYRAMZA plus paclitaxel vs placebo plus paclitaxel in patients with locally advanced or metastatic gastric or GEJ adenocarcinoma with disease progression on or after prior fluoropyrimidine- and platinum-containing chemotherapy. Major efficacy outcome measure was OS. Supportive efficacy outcome measures were PFS and ORR. All patients were ECOG PS 0 or 1. Prior to enrollment, 97% of patients had progressed during treatment or within 4 months after the last dose of first-line chemotherapy for metastatic disease. Twenty-five percent of patients had received anthracycline in combination with platinum/fluoropyrimidine therapy, while 75% did not. Patients were randomized 1:1 to CYRAMZA 8 mg/kg (n=330) or placebo (n=335) every 2 weeks (on days 1 and 15) of each 28-day cycle. Patients in both arms received paclitaxel 80 mg/m2 on days 1, 8, and 15 of each 28-day cycle.1,18
SELECT IMPORTANT SAFETY INFORMATIONGastrointestinal Perforations• CYRAMZA is an antiangiogenic therapy that can increase the risk of gastrointestinal perforation, a
potentially fatal event. Four of 570 patients (0.7%) who received CYRAMZA as a single agent in advanced gastric cancer clinical trials experienced gastrointestinal perforation. In study 2, the incidence of gastrointestinal perforation was 1.2% for CYRAMZA plus paclitaxel as compared to 0.3% for placebo plus paclitaxel. (Continued on next page)

26
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
ADVANCED GASTRIC AND GASTROESOPHAGEAL JUNCTION ADENOCARCINOMA, CONTINUED
• The percentage of events at the time of analysis was 85% (279 patients) and 88% (296 patients) in the CYRAMZA plus paclitaxel and placebo plus paclitaxel treatment arms, respectively
Placebo + paclitaxel(n=335)
CYRAMZA + paclitaxel (n=330)
1.0
0.8
0.6
0.4
0.2
0.0
PFS
PROB
ABIL
ITY
TIME FROM RANDOMIZATION (MONTHS)
70
34
8
104
50
6
188
124
4
259
214
2
330
335
0
43
21
10
28
12
12
15
8
14
11
5
16
7
3
18
3
3
20
1
3
22
-
24TIME FROM RANDOMIZATION (MONTHS)
86420 10 12 14 16 18 20 22 24 26 28
-
CYRAMZA + paclitaxelPlacebo+ paclitaxel
Number at Risk
CYRAMZA+ paclitaxelPlacebo+ paclitaxel
4.4CYRAMZA+ paclitaxel
(n=330)
2.9Placebo+ paclitaxel(n=335)
Supportive Outcome MeasureProgression-Free Survival:
Hazard Ratio=0.64 (0.54, 0.75); P<0.001
Median—Months (95% CI)
1.0
0.8
0.6
0.4
0.2
0.0
OS P
ROBA
BILI
TY
330
335
308
294
267
241
228
180
185
143
148
109
116
81
1
78
64
60
47
41
30
24
22
13
13
6
5
1
2
0
0
0
Number at Risk
CYRAMZA + paclitaxelPlacebo+ paclitaxel
CYRAMZA
Placebo+ paclitaxel
+ paclitaxel
9.6CYRAMZA+ paclitaxel
(n=330)
7.4Placebo+ paclitaxel(n=335)
Hazard Ratio=0.81 (0.68, 0.96); P=0.017
Major Outcome MeasureOverall Survival:
Median—Months (95% CI)
% ORR (COMPLETE + PARTIAL RESPONSE)
P<0.001
28%(23, 33)
0 20 40 60 80 100
16%(13, 20)
Supportive Outcome MeasureObjective Response Rate:
Percent of Patients (95% CI)OS
PRO
BABI
LITY
0 1 3 5 7 9 11 13 15 17 19 272 4 6 8 10 12 14 16 18 20 26 28
49154238 92 17 7 3 0 0117
CYRAMZAPlacebo 66 34 20 7 4 2
Number at Risk
0.0
0.2
0.4
0.6
0.8
CYRAMZAPlacebo
5.2MONTHS MONTHS
CYRAMZA(n=238)
3.8MONTHS Placebo
(n=117)
1.0
TIME FROM RANDOMIZATION (MONTHS)
Hazard Ratio=0.78 (0.60, 0.998); P=0.047
Major Outcome Measure Overall Survival:
Median—Months (95% CI)
Supportive Outcome MeasureProgression-Free Survival:
Median—Months (95% CI)
PFS
PROB
ABIL
ITY
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17
238 213 113 65 61 45 30 18 18 11 5 4 2 1 1 1 1 0117 92 27 11 7 4 2 2 2 2 2 1 1 0 0 0 0 0
CYRAMZAPlacebo
1.0
0.8
0.6
0.4
0.2
0.0
Hazard Ratio=0.48 (0.38, 0.62); P<0.001
TIME FROM RANDOMIZATION (MONTHS)
CYRAMZA Placebo
Number at Risk
1.3Placebo(n=117)
CYRAMZA(n=238)
2.1(4.4, 5.7)
(2.8, 4.7)
MONTHS(8.5, 10.8)
MONTHS(4.2, 5.3)
(1.5, 2.7)
MONTHS(6.3, 8.4)
MONTHS(2.8, 3.0)
(1.3, 1.4)MONTHS
RAINBOW Efficacy, Continued
CYRAMZA plus paclitaxel significantly delayed disease progression1,13
The phase III RAINBOW trial evaluated the efficacy and safety of CYRAMZA plus paclitaxel vs placebo plus paclitaxel in patients with locally advanced or metastatic gastric or GE junction adenocarcinoma with disease progression on or after prior fluoropyrimidine- and platinum-containing chemotherapy. Major efficacy outcome measure was OS. Supportive efficacy outcome measures were PFS and ORR. All patients were ECOG PS 0 or 1. Prior to enrollment, 97% of patients had progressed during treatment or within 4 months after the last dose of first-line chemotherapy for metastatic disease. Twenty-five percent of patients had received anthracycline in combination with platinum/fluoropyrimidine therapy, while 75% did not. Patients were randomized 1:1 to CYRAMZA 8 mg/kg (n=330) or placebo (n=335) every 2 weeks (on days 1 and 15) of each 28-day cycle. Patients in both arms received paclitaxel 80 mg/m2 on days 1, 8, and 15 of each 28-day cycle.1,18
SELECT IMPORTANT SAFETY INFORMATIONGastrointestinal Perforations, Continued• In study 3, the incidence of gastrointestinal perforation was 1% for CYRAMZA plus docetaxel as compared
to 0.3% for placebo plus docetaxel. In study 4, the incidence of gastrointestinal perforation was 1.7% for CYRAMZA plus FOLFIRI and 0.6% for placebo plus FOLFIRI. Permanently discontinue CYRAMZA in patients who experience a gastrointestinal perforation.

27
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
ADVANCED GASTRIC AND GASTROESOPHAGEAL JUNCTION ADENOCARCINOMA, CONTINUED
RAINBOW Efficacy, Continued
CYRAMZA plus paclitaxel provided significantly greater objective response rate compared with placebo plus paclitaxel1
Objective response rate was defined as complete plus partial response. Disease progression and tumor response were assessed by investigators in accordance with Response Evaluation Criteria in Solid Tumors (RECIST) 1.1.13
Placebo + paclitaxel(n=335)
CYRAMZA + paclitaxel (n=330)
1.0
0.8
0.6
0.4
0.2
0.0
PFS
PROB
ABIL
ITY
TIME FROM RANDOMIZATION (MONTHS)
70
34
8
104
50
6
188
124
4
259
214
2
330
335
0
43
21
10
28
12
12
15
8
14
11
5
16
7
3
18
3
3
20
1
3
22
-
24TIME FROM RANDOMIZATION (MONTHS)
86420 10 12 14 16 18 20 22 24 26 28
-
CYRAMZA + paclitaxelPlacebo+ paclitaxel
Number at Risk
CYRAMZA+ paclitaxelPlacebo+ paclitaxel
4.4CYRAMZA+ paclitaxel
(n=330)
2.9Placebo+ paclitaxel(n=335)
Supportive Outcome MeasureProgression-Free Survival:
Hazard Ratio=0.64 (0.54, 0.75); P<0.001
Median—Months (95% CI)
1.0
0.8
0.6
0.4
0.2
0.0
OS P
ROBA
BILI
TY
330
335
308
294
267
241
228
180
185
143
148
109
116
81
1
78
64
60
47
41
30
24
22
13
13
6
5
1
2
0
0
0
Number at Risk
CYRAMZA + paclitaxelPlacebo+ paclitaxel
CYRAMZA
Placebo+ paclitaxel
+ paclitaxel
9.6CYRAMZA+ paclitaxel
(n=330)
7.4Placebo+ paclitaxel(n=335)
Hazard Ratio=0.81 (0.68, 0.96); P=0.017
Major Outcome MeasureOverall Survival:
Median—Months (95% CI)
% ORR (COMPLETE + PARTIAL RESPONSE)
P<0.001
28%(23, 33)
0 20 40 60 80 100
16%(13, 20)
Supportive Outcome MeasureObjective Response Rate:
Percent of Patients (95% CI)
OS P
ROBA
BILI
TY
0 1 3 5 7 9 11 13 15 17 19 272 4 6 8 10 12 14 16 18 20 26 28
49154238 92 17 7 3 0 0117
CYRAMZAPlacebo 66 34 20 7 4 2
Number at Risk
0.0
0.2
0.4
0.6
0.8
CYRAMZAPlacebo
5.2MONTHS MONTHS
CYRAMZA(n=238)
3.8MONTHS Placebo
(n=117)
1.0
TIME FROM RANDOMIZATION (MONTHS)
Hazard Ratio=0.78 (0.60, 0.998); P=0.047
Major Outcome Measure Overall Survival:
Median—Months (95% CI)
Supportive Outcome MeasureProgression-Free Survival:
Median—Months (95% CI)
PFS
PROB
ABIL
ITY
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17
238 213 113 65 61 45 30 18 18 11 5 4 2 1 1 1 1 0117 92 27 11 7 4 2 2 2 2 2 1 1 0 0 0 0 0
CYRAMZAPlacebo
1.0
0.8
0.6
0.4
0.2
0.0
Hazard Ratio=0.48 (0.38, 0.62); P<0.001
TIME FROM RANDOMIZATION (MONTHS)
CYRAMZA Placebo
Number at Risk
1.3Placebo(n=117)
CYRAMZA(n=238)
2.1(4.4, 5.7)
(2.8, 4.7)
MONTHS(8.5, 10.8)
MONTHS(4.2, 5.3)
(1.5, 2.7)
MONTHS(6.3, 8.4)
MONTHS(2.8, 3.0)
(1.3, 1.4)MONTHS
The phase III RAINBOW trial evaluated the efficacy and safety of CYRAMZA plus paclitaxel vs placebo plus paclitaxel in patients with locally advanced or metastatic gastric or GEJ adenocarcinoma with disease progression on or after prior fluoropyrimidine- and platinum-containing chemotherapy. Major efficacy outcome measure was OS. Supportive efficacy outcome measures were PFS and ORR. All patients were ECOG PS 0 or 1. Prior to enrollment, 97% of patients had progressed during treatment or within 4 months after the last dose of first-line chemotherapy for metastatic disease. Twenty-five percent of patients had received anthracycline in combination with platinum/fluoropyrimidine therapy, while 75% did not. Patients were randomized 1:1 to CYRAMZA 8 mg/kg (n=330) or placebo (n=335) every 2 weeks (on days 1 and 15) of each 28-day cycle. Patients in both arms received paclitaxel 80 mg/m2 on days 1, 8, and 15 of each 28-day cycle.1,18
SELECT IMPORTANT SAFETY INFORMATIONClinical Deterioration in Child-Pugh B or C Cirrhosis• Clinical deterioration, manifested by new onset or worsening encephalopathy, ascites, or hepatorenal
syndrome, was reported in patients with Child-Pugh B or C cirrhosis who received single-agent CYRAMZA. Use CYRAMZA in patients with Child-Pugh B or C cirrhosis only if the potential benefits of treatment are judged to outweigh the risks of clinical deterioration.

28
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
ADVANCED GASTRIC AND GASTROESOPHAGEAL JUNCTION ADENOCARCINOMA, CONTINUED
Adverse Reaction Profile for CYRAMZA in Combination With Paclitaxel1,19
• The most common adverse reactions (all grades) observed in patients treated with CYRAMZA plus paclitaxel at a rate of ≥30% and ≥2% higher than placebo plus paclitaxel were fatigue (57% vs 44%), neutropenia (54% vs 31%), diarrhea (32% vs 23%), and epistaxis (31% vs 7%)
• The incidence of febrile neutropenia was 2.4% vs 1.2% in the CYRAMZA plus paclitaxel and placebo plus paclitaxel treatment arms, respectively1,19
• 19% of patients treated with CYRAMZA plus paclitaxel received granulocyte colony-stimulating factors vs 8.5% of patients treated with paclitaxel alone20
SELECT IMPORTANT SAFETY INFORMATION• The most common serious adverse events with CYRAMZA plus paclitaxel in study 2 were neutropenia
(3.7%) and febrile neutropenia (2.4%); 19% of patients treated with CYRAMZA plus paclitaxel received granulocyte colony-stimulating factors.
• Adverse reactions resulting in discontinuation of any component of the CYRAMZA plus paclitaxel combination in 2% or more patients in study 2 were neutropenia (4%) and thrombocytopenia (3%).
• Clinically relevant adverse reactions reported in ≥1% and <5% of the CYRAMZA plus paclitaxel-treated patients in study 2 were sepsis (3.1% for CYRAMZA plus paclitaxel vs 1.8% for placebo plus paclitaxel) and gastrointestinal perforations (1.2% for CYRAMZA plus paclitaxel vs 0.3% for placebo plus paclitaxel).
RAINBOW: ADVERSE REACTIONS OCCURRING AT INCIDENCE RATE ≥5% AND A ≥2% DIFFERENCE BETWEEN ARMS IN PATIENTS RECEIVING CYRAMZA IN COMBINATION WITH PACLITAXEL
ALL GRADES GRADE 3/4
Adverse ReactionsCYRAMZA + paclitaxel
(n=327)
Placebo + paclitaxel
(n=329)
CYRAMZA + paclitaxel
(n=327)
Placebo + paclitaxel
(n=329)
Fatigue/Asthenia 57% 44% 12% 6%
Neutropenia 54% 31% 41% 19%
Diarrhea 32% 23% 4% 2%
Epistaxis 31% 7% 0% 0%
Hypertension 25% 6% 15% 3%
Peripheral edema 25% 14% 2% 1%
Stomatitis 20% 7% 1% 1%
Proteinuria 17% 6% 1% 0%
Thrombocytopenia 13% 6% 2% 2%
Hypoalbuminemia 11% 5% 1% 1%
Gastrointestinal hemorrhage events 10% 6% 4% 2%
29
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
ADVANCED GASTRIC AND GASTROESOPHAGEAL JUNCTION ADENOCARCINOMA, CONTINUED
RAINBOW Trial Inclusion Criteria21
Each patient must have met the following criteria to be enrolled in this study:1. Histologically- or cytologically-confirmed gastric carcinoma, including gastric adenocarcinoma or GEJ
adenocarcinoma (patients with adenocarcinoma of the distal esophagus were eligible if the primary tumor involved the GEJ)
2. Metastatic disease or locally recurrent, unresectable disease with measurable lymph node metastases • Nonregional lymph node metastases were eligible; lymph node metastases must have been measurable as defined by the Response Evaluation Criteria in Solid Tumors (RECIST)
• Locally-recurrent, unresectable disease was eligible if there was at least one measurable lymph node metastasis (regional or nonregional) as defined by RECIST
• Received prior radiation therapy, measurable or evaluable lesions must have been outside the radiation field, or (for lesions within the radiation field) there must have been documented progression following radiation therapy
3. Measurable disease and/or evaluable disease. Measurable disease was defined as at least one unidimensionally measurable target lesion (≥20 mm with conventional techniques or ≥10 mm by spiral CT), as defined by RECIST. Examples of evaluable, nonmeasurable disease include gastric, peritoneal, or mesenteric thickening in areas of known disease, or peritoneal nodules that were too small to be considered measurable by RECIST
4. Experienced disease progression during or within 4 months after the last dose of first-line therapy for metastatic disease, or during or within 6 months after the last dose of adjuvant therapy
• Acceptable first-line regimens for this study were combination chemotherapy regimens that included platinum or fluoropyrimidine components (acceptable prior platinum agents were cisplatin, carboplatin, or oxaliplatin; acceptable prior fluoropyrimidine agents were 5-FU, capecitabine, or S-1)
• Elevations in CEA or other tumor markers without radiographic evidence of progression did not constitute satisfactory evidence of progression on first-line therapy
• Intolerant to first-line chemotherapy regimens were eligible provided there was disease progression within 4 months after the last dose of first-line therapy
• Patients who had one or more component(s) of first-line chemotherapy discontinued because of toxicity, but continued to receive the other component(s) of first-line therapy (eg, a FOLFOX regimen in which the oxaliplatin was stopped and the 5-FU/leucovorin was continued), were eligible following disease progression
• Prior adjuvant therapy was permitted, and patients with disease progression during adjuvant chemotherapy were eligible, provided that disease progression occurred within 6 months after the completion of adjuvant therapy. Patients who experienced disease progression more than 6 months after the last dose of adjuvant therapy should have received first-line therapy for metastatic disease, with subsequent progression on first-line therapy a requirement for eligibility
SELECT IMPORTANT SAFETY INFORMATIONReversible Posterior Leukoencephalopathy Syndrome (RPLS)• RPLS has been reported at a rate of <0.1% in clinical studies with CYRAMZA. Confirm the diagnosis
of RPLS with MRI and discontinue CYRAMZA in patients who develop RPLS. Symptoms may resolve or improve within days, although some patients with RPLS can experience ongoing neurologic sequelae or death.

30
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
ADVANCED GASTRIC AND GASTROESOPHAGEAL JUNCTION ADENOCARCINOMA, CONTINUED
RAINBOW Trial Inclusion Criteria, Continued21
5. Disease was not amenable to potentially curative resection6. 18 years of age or older7. Life expectancy of ≥12 weeks 8. Resolution to grade ≤1 (or to grade ≤2 in the case of neuropathy) by the National Cancer Institute Common
Terminology Criteria for Adverse Events (NCI-CTCAE), Version 3.0, of all clinically significant toxic effects of prior chemotherapy, surgery, radiotherapy, or hormonal therapy (with the exception of alopecia)
9. ECOG PS score of 0-110. Adequate hepatic function as defined by a total bilirubin ≤1.5 mg/dL (25.65 μmol/L), and aspartate
transaminase (AST) and alanine transaminase (ALT) ≤3.0 x the upper limit of normal (ULN) [or 5.0 x the ULN in the setting of liver metastases]
11. Adequate renal function as defined by a serum creatinine ≤1.5 x the ULN, or creatinine clearance (measured via 24-hour urine collection) ≥40 mL/minute (ie, if serum creatinine was >1.5 x the ULN, a 24-hour urine collection to calculate creatinine clearance must have been performed)
12. Urinary protein was ≤1+ on dipstick or routine UA; if urine dipstick or routine analysis was ≥2+, a 24-hour urine collection for protein must have demonstrated <1000 mg of protein in 24 hours to allow participation in the study
13. Adequate hematologic function, as evidenced by an absolute neutrophil count (ANC) ≥1000/μL, hemoglobin ≥9 g/dL (5.58 mmol/L), and platelets ≥100,000/μL
14. Adequate coagulation function as defined by International Normalized Ratio (INR) ≤1.5 and a partial thromboplastin time (PTT) ≤5 seconds above the ULN (unless receiving anticoagulation therapy). Patients on full-dose anticoagulation must have been on a stable dose (minimum duration 14 days) of oral anticoagulant or low molecular weight heparin. If receiving warfarin, the patient must have had an INR ≤3.0 and no active bleeding (ie, no bleeding within 14 days prior to first dose of study therapy) or pathological condition present that carried a high risk of bleeding (eg, tumor involving major vessels or known varices). Patients on anticoagulation therapy with unresected primary tumors or local tumor recurrence following resection were not eligible
15. Received prior anthracycline therapy as part of his or her first-line regimen, the patient was able to engage in ordinary physical activity without significant fatigue or dyspnea (equivalent to New York Heart Association Class I function)
16. If sexually active, must have been postmenopausal, surgically sterile, or using effective contraception (hormonal or barrier methods)
17. Female patients of childbearing potential must have had a negative serum pregnancy test within 7 days prior to randomization
18. Able to provide informed written consent and was amenable to compliance with protocol schedules and testing
SELECT IMPORTANT SAFETY INFORMATIONProteinuria Including Nephrotic Syndrome• In study 4, severe proteinuria occurred more frequently in patients treated with CYRAMZA plus FOLFIRI
compared to patients receiving placebo plus FOLFIRI. Severe proteinuria was reported in 3% of patients treated with CYRAMZA plus FOLFIRI (including 3 cases [0.6%] of nephrotic syndrome) compared to 0.2% of patients treated with placebo plus FOLFIRI. Monitor proteinuria by urine dipstick and/or urinary protein creatinine ratio for the development of worsening of proteinuria during CYRAMZA therapy. (Continued on next page)

31
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
ADVANCED GASTRIC AND GASTROESOPHAGEAL JUNCTION ADENOCARCINOMA, CONTINUED
RAINBOW Trial Exclusion Criteria21
Patients who met any of the following criteria were excluded from the study:1. Squamous cell or undifferentiated gastric cancer2. Undergone major surgery within 28 days prior to randomization, or central venous access device
placement within 7 days prior to randomization 3. Received any chemotherapy other than platinum and fluoropyrimidine with or without anthracycline for
advanced gastric or GEJ adenocarcinoma 4. Received previous systemic chemotherapy with a cumulative dose of >900 mg/m2 of epirubicin or >400 mg/m2 of doxorubicin
5. Received any previous systemic therapy (including investigational agents) targeting VEGF or the VEGFR signaling pathways. Other previous targeted therapies were permitted, if stopped at least 28 days prior to randomization
6. A history of deep vein thrombosis, pulmonary embolism, or any other significant thromboembolism (venous port or catheter thrombosis or superficial venous thrombosis were not considered "significant”) during the 3 months prior to randomization
7. Received therapeutic anticoagulation with warfarin, low-molecular weight heparin or similar agents. Patients who received prophylactic, low-dose anticoagulation therapy were eligible provided that the coagulation parameters defined in the inclusion criteria (INR ≤1.5 and PTT/aPTT ≤1.5 ULN) or (PT ≤1.5 ULN and PTT/aPTT ≤1.5 ULN) were met
8. Received chronic therapy with nonsteroidal anti-inflammatory agents (NSAIDs, eg, indomethacin, ibuprofen, naproxen or similar agents) or other anti-platelet agents (eg, clopidogrel, ticlopidine, dipyridamole, anagrelide). Aspirin use at doses up to 325 mg/day was permitted
9. Significant bleeding disorders, vasculitis, or had a significant bleeding episode from the gastrointestinal tract within 3 months prior to study entry
10. History of gastrointestinal perforation and/or fistulae within 6 months prior to randomization11. Symptomatic congestive heart failure (New York Heart Association II-IV) or symptomatic or poorly
controlled cardiac arrhythmia12. Experienced any arterial thrombotic event, including myocardial infarction, unstable angina,
cerebrovascular accident, or transient ischemic attack, within 6 months prior to randomization 13. Uncontrolled arterial hypertension ≥150/≥90 mm Hg despite standard medical management 14. Serious or nonhealing wound or peptic ulcer or bone fracture within 28 days prior to randomization 15. Bowel obstruction, history or presence of inflammatory enteropathy or extensive intestinal resection
(hemicolectomy or extensive small intestine resection with chronic diarrhea), Crohn’s disease, ulcerative colitis, or chronic diarrhea
SELECT IMPORTANT SAFETY INFORMATIONProteinuria Including Nephrotic Syndrome, Continued• Withhold CYRAMZA for urine protein levels that are ≥2 g over 24 hours. Reinitiate CYRAMZA at a reduced
dose once the urine protein level returns to <2 g over 24 hours. Permanently discontinue CYRAMZA for urine protein levels >3 g over 24 hours or in the setting of nephrotic syndrome.

32
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
ADVANCED GASTRIC AND GASTROESOPHAGEAL JUNCTION ADENOCARCINOMA, CONTINUED
RAINBOW Trial Exclusion Criteria, Continued21
16. Serious illness or medical condition(s) including, but not limited to the following: • Known human immunodeficiency virus infection or acquired immunodeficiency syndrome- related illness
• Active or uncontrolled clinically serious infection • Previous or concurrent malignancy except for basal or squamous cell skin cancer and/or in situ carcinoma of the cervix, or other solid tumors treated curatively and without evidence of recurrence for at least 3 years prior to the study
• Uncontrolled metabolic disorders or other nonmalignant organ or systemic diseases or secondary effects of cancer that induce a high medical risk and/or make assessment of survival uncertain
• Other severe acute or chronic medical or psychiatric condition or laboratory abnormality that may have increased the risk associated with study participation or study drug administration, or may have interfered with the interpretation of study results, and in the judgment of the Investigator would have made the patient ineligible for entry into this study
• History or evidence of known central nervous system metastases or carcinomatous meningitis • Known allergy or hypersensitivity to monoclonal antibody treatment or any components used in the ramucirumab DP preparation
• Known allergy or hypersensitivity to paclitaxel or any components used in the paclitaxel preparation or other contraindication for taxane therapy
17. Pregnant or breastfeeding 18. Was enrolled in, or had discontinued within the last 28 days from a clinical trial involving an investigational
product or non-approved use of a drug, or concurrently was enrolled in any other type of medical research judged not to be scientifically or medically compatible with this study. Patients participating in surveys or observational studies were eligible to participate in this study
SELECT IMPORTANT SAFETY INFORMATIONThyroid Dysfunction• Monitor thyroid function during treatment with CYRAMZA. In study 4, the incidence of hypothyroidism
reported as an adverse event was 2.6% in the CYRAMZA plus FOLFIRI treated patients and 0.9% in the placebo plus FOLFIRI treated patients.

33
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
METASTATIC NON-SMALL CELL LUNG CANCER
NCCN Guidelines Recommend ramucirumab (CYRAMZA) Plus Docetaxel as a Subsequent Therapy Option in Patients With Metastatic NSCLC22
IndicationCYRAMZA, in combination with docetaxel, is indicated for the treatment of patients with metastatic NSCLC with disease progression on or after platinum-based chemotherapy. Patients with EGFR or ALK genomic tumor aberrations should have disease progression on FDA-approved therapy for these aberrations prior to receiving CYRAMZA.
Category 2A Recommendation*
RAMUCIRUMAB (CYRAMZA) PLUS DOCETAXEL
NCCN Guidelines recommend ramucirumab (CYRAMZA) in combination with docetaxel as a subsequent therapy option (with a category 2A recommendation)* in patients with nonsquamous or squamous metastatic NSCLC.
* Category 2A recommendation is based on lower-level evidence and there is uniform NCCN consensus that the intervention is appropriate.
SELECT IMPORTANT SAFETY INFORMATIONEmbryofetal Toxicity• Based on its mechanism of action, CYRAMZA can cause fetal harm when administered to pregnant
women. Animal models link angiogenesis, VEGF, and VEGF Receptor 2 (VEGFR2) to critical aspects of female reproduction, embryofetal development, and postnatal development. Advise pregnant women of the potential risk to a fetus. Advise females of reproductive potential to use effective contraception during treatment with CYRAMZA and for at least 3 months after the last dose of CYRAMZA.
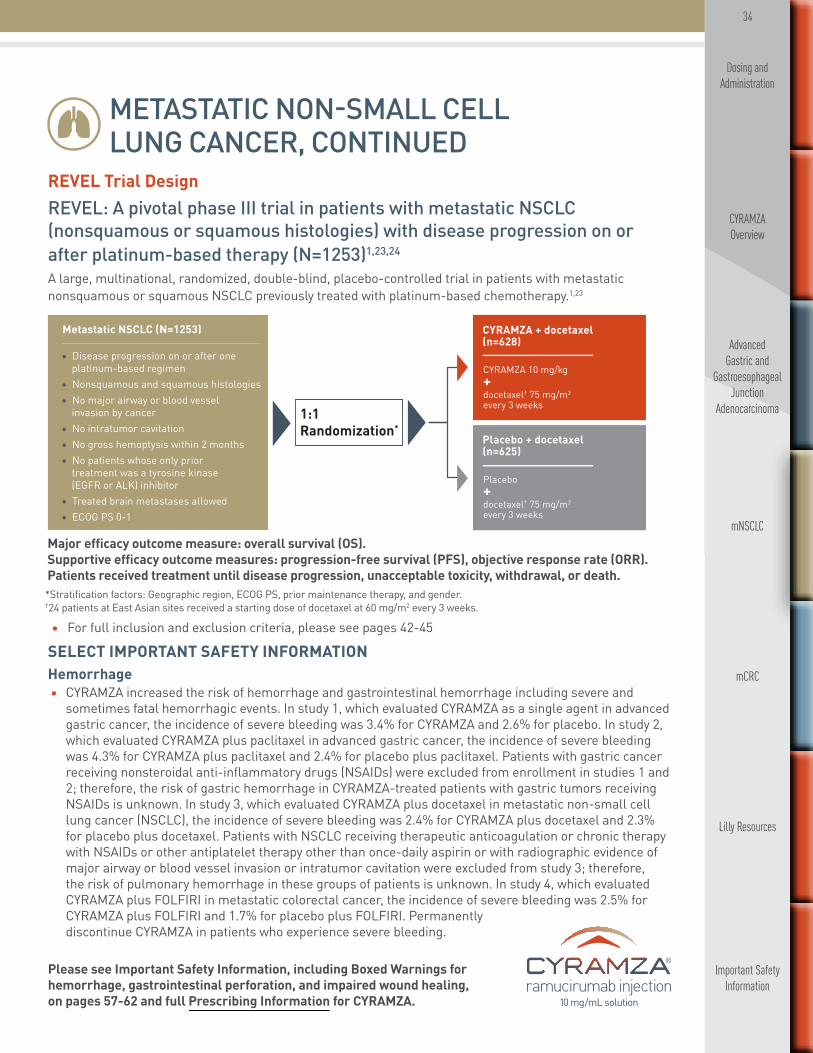
34
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
METASTATIC NON-SMALL CELL LUNG CANCER, CONTINUED
REVEL Trial DesignREVEL: A pivotal phase III trial in patients with metastatic NSCLC (nonsquamous or squamous histologies) with disease progression on or after platinum-based therapy (N=1253)1,23,24 A large, multinational, randomized, double-blind, placebo-controlled trial in patients with metastatic nonsquamous or squamous NSCLC previously treated with platinum-based chemotherapy.1,23
1:1Randomization*
• Disease progression on or after one platinum-based regimen• Nonsquamous and squamous histologies• No major airway or blood vessel invasion by cancer• No intratumor cavitation• No gross hemoptysis within 2 months• No patients whose only prior treatment was a tyrosine kinase (EGFR or ALK) inhibitor• Treated brain metastases allowed• ECOG PS 0-1
Metastatic NSCLC (N=1253) CYRAMZA + docetaxel(n=628)
CYRAMZA 10 mg/kg +docetaxel† 75 mg/m2 every 3 weeks
Placebo + docetaxel(n=625)
Placebo + docetaxel† 75 mg/m2 every 3 weeks
Major efficacy outcome measure: overall survival (OS).Supportive efficacy outcome measures: progression-free survival (PFS), objective response rate (ORR). Patients received treatment until disease progression, unacceptable toxicity, withdrawal, or death.
*Stratification factors: Geographic region, ECOG PS, prior maintenance therapy, and gender. †24 patients at East Asian sites received a starting dose of docetaxel at 60 mg/m2 every 3 weeks.
• For full inclusion and exclusion criteria, please see pages 42-45
SELECT IMPORTANT SAFETY INFORMATIONHemorrhage • CYRAMZA increased the risk of hemorrhage and gastrointestinal hemorrhage including severe and
sometimes fatal hemorrhagic events. In study 1, which evaluated CYRAMZA as a single agent in advanced gastric cancer, the incidence of severe bleeding was 3.4% for CYRAMZA and 2.6% for placebo. In study 2, which evaluated CYRAMZA plus paclitaxel in advanced gastric cancer, the incidence of severe bleeding was 4.3% for CYRAMZA plus paclitaxel and 2.4% for placebo plus paclitaxel. Patients with gastric cancer receiving nonsteroidal anti-inflammatory drugs (NSAIDs) were excluded from enrollment in studies 1 and 2; therefore, the risk of gastric hemorrhage in CYRAMZA-treated patients with gastric tumors receiving NSAIDs is unknown. In study 3, which evaluated CYRAMZA plus docetaxel in metastatic non-small cell lung cancer (NSCLC), the incidence of severe bleeding was 2.4% for CYRAMZA plus docetaxel and 2.3% for placebo plus docetaxel. Patients with NSCLC receiving therapeutic anticoagulation or chronic therapy with NSAIDs or other antiplatelet therapy other than once-daily aspirin or with radiographic evidence of major airway or blood vessel invasion or intratumor cavitation were excluded from study 3; therefore, the risk of pulmonary hemorrhage in these groups of patients is unknown. In study 4, which evaluated CYRAMZA plus FOLFIRI in metastatic colorectal cancer, the incidence of severe bleeding was 2.5% for CYRAMZA plus FOLFIRI and 1.7% for placebo plus FOLFIRI. Permanently discontinue CYRAMZA in patients who experience severe bleeding.

35
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
METASTATIC NON-SMALL CELL LUNG CANCER, CONTINUED
REVEL Trial Design, Continued
Treatment monitoring and patient management• Patients had a UA dipstick every 6 weeks25
• There was a mandatory 60-minute observation period after the first two infusions of CYRAMZA to watch for IRRs. The observation period was eliminated from further infusions if there was no evidence of an IRR26
• The following were performed27: — Vital sign measurements, including temperature, pulse rate, respiration rate, and blood pressure (at
every infusion, obtained before and at the completion of each infusion) — Hematology profile (complete blood count with differential and platelet count) was checked
every infusion — Clinical chemistry (sodium, potassium, chloride, carbon dioxide, BUN, creatinine, glucose, total
protein, albumin, uric acid, AST/SGOT, ALT/SGPT, alkaline phosphatase, total bilirubin, direct bilirubin, lactate dehydrogenase, calcium, magnesium, and phosphorus) - every infusion
— Coagulation profile (INR, prothrombin time, and PTT) - every infusion — Urinalysis - every 6 weeks — Pregnancy test - every 6 weeks — Imaging studies/tumor assessments - every 6 weeks
• In the REVEL protocol, all subsequent doses were modified/reduced if dose modification/rate reduction was needed because of an IRR8
• For infusion-related reactions after giving dexamethasone and acetaminophen, protocols included9: — A grade 1 IRR did not require stopping the infusion — A grade 2 IRR the infusion was stopped, but the site could resume the infusion at 50% of the prior rate
once the infusion reaction had resolved or decreased to grade 1. The infusion duration could not have exceeded 2 hours
— For grade 3 or 4 IRRs, the infusion should be stopped and the CYRAMZA permanently discontinued
• For patients on CYRAMZA, major surgery (including major dental procedures) was postponed until at least 28 days after the last dose of CYRAMZA (when possible) and CYRAMZA was not restarted for at least 28 days after surgery along with the wound being fully healed. If subcutaneous venous access device placement was required during the course of therapy, it was recommended that a 7-day treatment-free period occur both prior to and following placement10
SELECT IMPORTANT SAFETY INFORMATIONInfusion-Related Reactions (IRRs)• Prior to the institution of premedication recommendations across clinical trials of CYRAMZA, IRRs
occurred in 6 out of 37 patients (16%), including 2 severe events. The majority of IRRs across trials occurred during or following a first or second CYRAMZA infusion. Symptoms of IRRs included rigors/ tremors, back pain/spasms, chest pain and/or tightness, chills, flushing, dyspnea, wheezing, hypoxia, and paresthesia. In severe cases, symptoms included bronchospasm, supraventricular tachycardia, and hypotension. Monitor patients during the infusion for signs and symptoms of IRRs in a setting with available resuscitation equipment. Immediately and permanently discontinue CYRAMZA for grade 3 or 4 IRRs.

36
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
METASTATIC NON-SMALL CELL LUNG CANCER, CONTINUED
SELECT IMPORTANT SAFETY INFORMATION Arterial Thromboembolic Events (ATEs)• Serious, sometimes fatal, ATEs including myocardial infarction, cardiac arrest, cerebrovascular accident,
and cerebral ischemia occurred in clinical trials including 1.7% of 236 patients who received CYRAMZA as a single agent for gastric cancer in study 1. Permanently discontinue CYRAMZA in patients who experience a severe ATE.
REVEL Patient Population
Demographic and baseline characteristics were similar between treatment arms1,23,28
*Data not available for one patient in the CYRAMZA plus docetaxel group.†Data not available for one patient in each group.CR=complete response; PR=partial response; SD=stable disease; PD=progressive disease.
REVEL: DEMOGRAPHIC AND BASELINE CHARACTERISTICS
CYRAMZA + docetaxel
(n=628)
Placebo + docetaxel
(n=625)
Age, median (range) 62 (21-85) 61 (25-86)
Male, n (%) 419 (67%) 415 (66%)
Race (self-reported), n (%)*
Caucasian 526 (84%) 503 (80%)Asian 74 (12%) 86 (14%)
Histology, n (%)
Nonsquamous 465 (74%) 447 (72%)
Squamous 157 (25%) 171 (27%)ECOG PS†
1 420 (67%) 425 (68%)Smoking history, n (%)
Ever 518 (82%) 483 (77%)Prior Treatment
Prior taxane, n (%) 153 (24%) 149 (24%)Prior bevacizumab, n (%) 88 (14%) 92 (15%)Prior pemetrexed, n (%) 233 (37%) 249 (40%)Prior gemcitabine, n (%) 157 (25%) 152 (24%)Prior maintenance therapy, n (%) 135 (21%) 143 (23%)
Best response to platinum, n (%)CR/PR/SD 420 (67%) 417 (67%)PD 178 (28%) 182 (29%)
Time since previous therapy, n (%)<9 months 400 (64%) 374 (60%)≥9 months 226 (36%) 251 (40%)

37
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
METASTATIC NON-SMALL CELL LUNG CANCER, CONTINUED
REVEL Efficacy
CYRAMZA plus docetaxel demonstrated a statistically significant improvement in overall survival vs docetaxel1,29
• The percentage of deaths at the time of analysis was 68% (428 patients) and 73% (456 patients) in the CYRAMZA plus docetaxel and placebo plus docetaxel arms, respectively
OS P
ROBA
BILI
TY
1.0
0.8
0.6
0.4
0.2
0.00 3 6 9 12 15 18 21 24 27 30 33 36
TIME FROM RANDOMIZATION (MONTHS)
527 415 329 231 156 103628
625
CYRAMZA+ docetaxelPlacebo+ docetaxel 501 386 306 197 129 86
Number at Risk
70 45 23 11 2 0
56 36 23 9 0 0
CYRAMZA+ docetaxelPlacebo+ docetaxel
Hazard Ratio (95% CI)=0.86 (0.75, 0.98); P=0.024
10.5MONTHS
CYRAMZA+ docetaxel
(n=628)
Placebo+ docetaxel(n=625)
(9.5, 11.2)
MONTHS9.1
(8.4, 10.0)
Major Outcome MeasureOverall Survival:
Median—Months (95% CI)
PFS
PROB
ABIL
ITY
1.0
0.8
0.6
0.4
0.2
0.00 3 6 9 12 15 18 21 24 27 30
TIME FROM RANDOMIZATION (MONTHS)
383 204 120 59 38 11
301 172 95 37 17 9
7 3 3 0
4 3 2 0
Hazard Ratio (95% CI)=0.76 (0.68, 0.86); P<0.001
4.5MONTHS
628
625
CYRAMZA+ docetaxelPlacebo+ docetaxel
Number at Risk
CYRAMZA+ docetaxelPlacebo+ docetaxel
(4.2, 5.4)
CYRAMZA+ docetaxel
(n=628)
MONTHS Placebo+ docetaxel(n=625)
3.0(2.8, 3.9)
Supportive Outcome MeasureProgression-Free Survival:
Median—Months (95% CI)
% ORR (COMPLETE + PARTIAL RESPONSE)
P<0.001
0 20 40 60 80 100
Placebo + docetaxel (n=625)
14%(11, 17)
CYRAMZA + docetaxel (n=628)
23%(20, 26)
Supportive Outcome Measure Objective Response Rate: Percent of Patients (95% CI)
The phase III REVEL trial evaluated the efficacy and safety of CYRAMZA plus docetaxel vs placebo plus docetaxel in patients with metastatic NSCLC with disease progression on or after platinum-based chemotherapy. Major efficacy outcome measure was OS. Supportive efficacy outcome measures were PFS and ORR. All patients were required to have ECOG PS 0 or 1. Patients were randomized 1:1 (N=1253) to receive either CYRAMZA 10 mg/kg or placebo, in combination with docetaxel at 75 mg/m2 every 21 days.1
SELECT IMPORTANT SAFETY INFORMATION Hypertension• An increased incidence of severe hypertension occurred in patients receiving CYRAMZA as a single agent
(8%) as compared to placebo (3%), in patients receiving CYRAMZA plus paclitaxel (15%) as compared to placebo plus paclitaxel (3%), and in patients receiving CYRAMZA plus docetaxel (6%) as compared to placebo plus docetaxel (2%), and in patients receiving CYRAMZA plus FOLFIRI (11%) as compared to placebo plus FOLFIRI (3%). Control hypertension prior to initiating treatment with CYRAMZA. Monitor blood pressure every 2 weeks or more frequently as indicated during treatment. Temporarily suspend CYRAMZA for severe hypertension until medically controlled. Permanently discontinue CYRAMZA if medically significant hypertension cannot be controlled with antihypertensive therapy or in patients with hypertensive crisis or hypertensive encephalopathy.

38
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
METASTATIC NON-SMALL CELL LUNG CANCER, CONTINUED
• The percentage of events at the time of analysis was 89% (558 patients) and 93% (583 patients) in the CYRAMZA plus docetaxel and placebo plus docetaxel arms, respectively
The phase III REVEL trial evaluated the efficacy and safety of CYRAMZA plus docetaxel vs placebo plus docetaxel in patients with metastatic NSCLC with disease progression on or after platinum-based chemotherapy. Major efficacy outcome measure was OS. Supportive efficacy outcome measures were PFS and ORR. All patients were required to have ECOG PS 0 or 1. Patients were randomized 1:1 (N=1253) to receive either CYRAMZA 10 mg/kg or placebo, in combination with docetaxel at 75 mg/m2 every 21 days.1
OS P
ROBA
BILI
TY
1.0
0.8
0.6
0.4
0.2
0.00 3 6 9 12 15 18 21 24 27 30 33 36
TIME FROM RANDOMIZATION (MONTHS)
527 415 329 231 156 103628
625
CYRAMZA+ docetaxelPlacebo+ docetaxel 501 386 306 197 129 86
Number at Risk
70 45 23 11 2 0
56 36 23 9 0 0
CYRAMZA+ docetaxelPlacebo+ docetaxel
Hazard Ratio (95% CI)=0.86 (0.75, 0.98); P=0.024
10.5MONTHS
CYRAMZA+ docetaxel
(n=628)
Placebo+ docetaxel(n=625)
(9.5, 11.2)
MONTHS9.1
(8.4, 10.0)
Major Outcome MeasureOverall Survival:
Median—Months (95% CI)
PFS
PROB
ABIL
ITY
1.0
0.8
0.6
0.4
0.2
0.00 3 6 9 12 15 18 21 24 27 30
TIME FROM RANDOMIZATION (MONTHS)
383 204 120 59 38 11
301 172 95 37 17 9
7 3 3 0
4 3 2 0
Hazard Ratio (95% CI)=0.76 (0.68, 0.86); P<0.001
4.5MONTHS
628
625
CYRAMZA+ docetaxelPlacebo+ docetaxel
Number at Risk
CYRAMZA+ docetaxelPlacebo+ docetaxel
(4.2, 5.4)
CYRAMZA+ docetaxel
(n=628)
MONTHS Placebo+ docetaxel(n=625)
3.0(2.8, 3.9)
Supportive Outcome MeasureProgression-Free Survival:
Median—Months (95% CI)
% ORR (COMPLETE + PARTIAL RESPONSE)
P<0.001
0 20 40 60 80 100
Placebo + docetaxel (n=625)
14%(11, 17)
CYRAMZA + docetaxel (n=628)
23%(20, 26)
Supportive Outcome Measure Objective Response Rate: Percent of Patients (95% CI)
REVEL Efficacy, Continued
CYRAMZA plus docetaxel delayed disease progression1,30
SELECT IMPORTANT SAFETY INFORMATIONInfusion-Related Reactions (IRRs)• Prior to the institution of premedication recommendations across clinical trials of CYRAMZA, IRRs
occurred in 6 out of 37 patients (16%), including 2 severe events. The majority of IRRs across trials occurred during or following a first or second CYRAMZA infusion. Symptoms of IRRs included rigors/tremors, back pain/spasms, chest pain and/or tightness, chills, flushing, dyspnea, wheezing, hypoxia, and paresthesia. In severe cases, symptoms included bronchospasm, supraventricular tachycardia, and hypotension. Monitor patients during the infusion for signs and symptoms of IRRs in a setting with available resuscitation equipment. Immediately and permanently discontinue CYRAMZA for grade 3 or 4 IRRs.
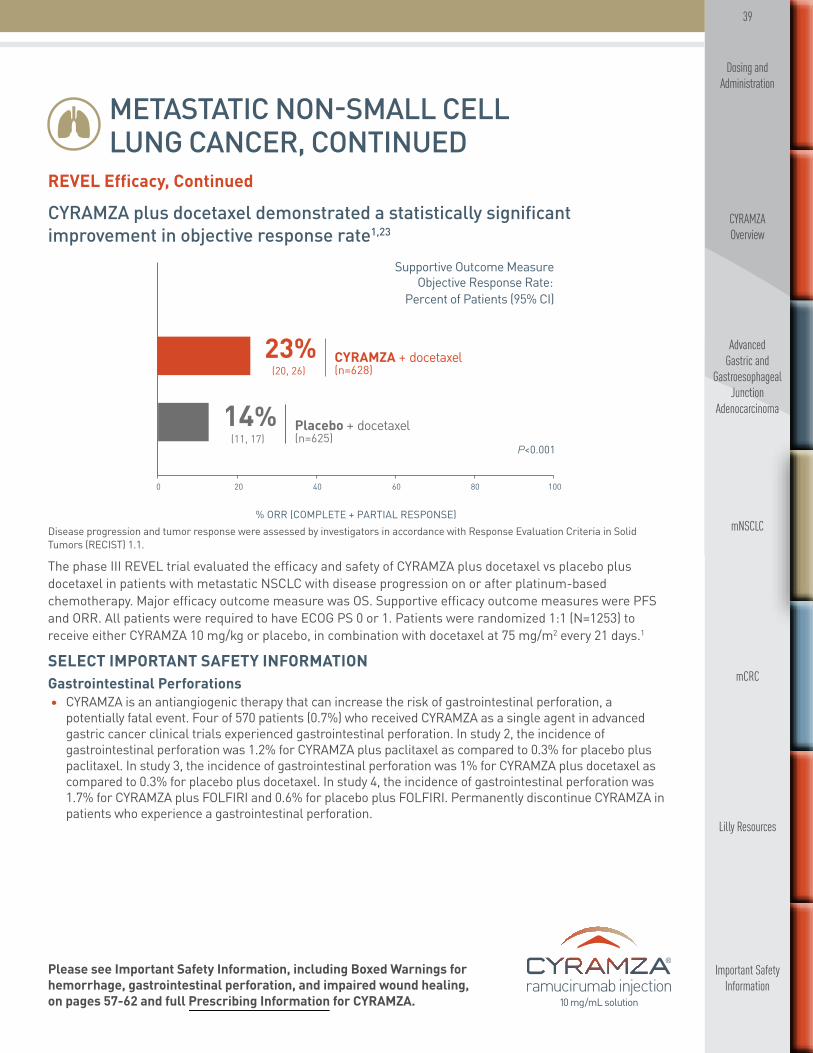
39
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
METASTATIC NON-SMALL CELL LUNG CANCER, CONTINUED
The phase III REVEL trial evaluated the efficacy and safety of CYRAMZA plus docetaxel vs placebo plus docetaxel in patients with metastatic NSCLC with disease progression on or after platinum-based chemotherapy. Major efficacy outcome measure was OS. Supportive efficacy outcome measures were PFS and ORR. All patients were required to have ECOG PS 0 or 1. Patients were randomized 1:1 (N=1253) to receive either CYRAMZA 10 mg/kg or placebo, in combination with docetaxel at 75 mg/m2 every 21 days.1
REVEL Efficacy, Continued
CYRAMZA plus docetaxel demonstrated a statistically significant improvement in objective response rate1,23
Disease progression and tumor response were assessed by investigators in accordance with Response Evaluation Criteria in Solid Tumors (RECIST) 1.1.
OS P
ROBA
BILI
TY
1.0
0.8
0.6
0.4
0.2
0.00 3 6 9 12 15 18 21 24 27 30 33 36
TIME FROM RANDOMIZATION (MONTHS)
527 415 329 231 156 103628
625
CYRAMZA+ docetaxelPlacebo+ docetaxel 501 386 306 197 129 86
Number at Risk
70 45 23 11 2 0
56 36 23 9 0 0
CYRAMZA+ docetaxelPlacebo+ docetaxel
Hazard Ratio (95% CI)=0.86 (0.75, 0.98); P=0.024
10.5MONTHS
CYRAMZA+ docetaxel
(n=628)
Placebo+ docetaxel(n=625)
(9.5, 11.2)
MONTHS9.1
(8.4, 10.0)
Major Outcome MeasureOverall Survival:
Median—Months (95% CI)
PFS
PROB
ABIL
ITY
1.0
0.8
0.6
0.4
0.2
0.00 3 6 9 12 15 18 21 24 27 30
TIME FROM RANDOMIZATION (MONTHS)
383 204 120 59 38 11
301 172 95 37 17 9
7 3 3 0
4 3 2 0
Hazard Ratio (95% CI)=0.76 (0.68, 0.86); P<0.001
4.5MONTHS
628
625
CYRAMZA+ docetaxelPlacebo+ docetaxel
Number at Risk
CYRAMZA+ docetaxelPlacebo+ docetaxel
(4.2, 5.4)
CYRAMZA+ docetaxel
(n=628)
MONTHS Placebo+ docetaxel(n=625)
3.0(2.8, 3.9)
Supportive Outcome MeasureProgression-Free Survival:
Median—Months (95% CI)
% ORR (COMPLETE + PARTIAL RESPONSE)
P<0.001
0 20 40 60 80 100
Placebo + docetaxel (n=625)
14%(11, 17)
CYRAMZA + docetaxel (n=628)
23%(20, 26)
Supportive Outcome Measure Objective Response Rate: Percent of Patients (95% CI)
SELECT IMPORTANT SAFETY INFORMATIONGastrointestinal Perforations• CYRAMZA is an antiangiogenic therapy that can increase the risk of gastrointestinal perforation, a
potentially fatal event. Four of 570 patients (0.7%) who received CYRAMZA as a single agent in advanced gastric cancer clinical trials experienced gastrointestinal perforation. In study 2, the incidence of gastrointestinal perforation was 1.2% for CYRAMZA plus paclitaxel as compared to 0.3% for placebo plus paclitaxel. In study 3, the incidence of gastrointestinal perforation was 1% for CYRAMZA plus docetaxel as compared to 0.3% for placebo plus docetaxel. In study 4, the incidence of gastrointestinal perforation was 1.7% for CYRAMZA plus FOLFIRI and 0.6% for placebo plus FOLFIRI. Permanently discontinue CYRAMZA in patients who experience a gastrointestinal perforation.
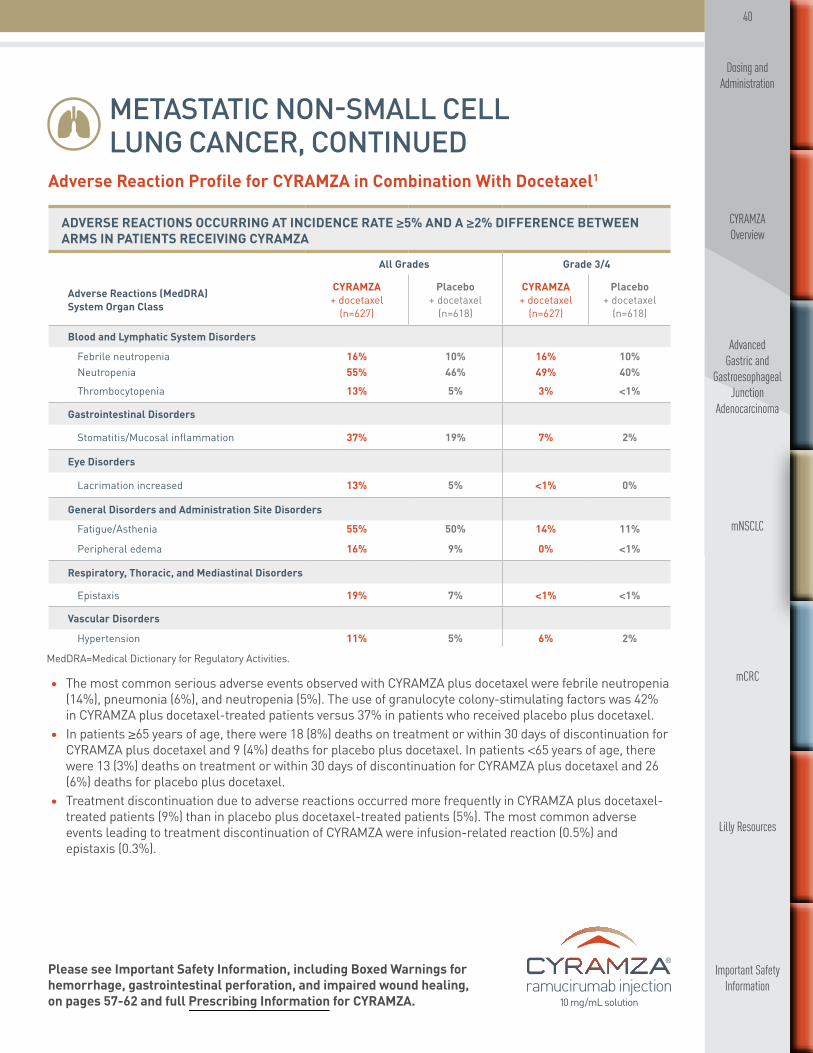
40
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
METASTATIC NON-SMALL CELL LUNG CANCER, CONTINUED
Adverse Reaction Profile for CYRAMZA in Combination With Docetaxel1
• The most common serious adverse events observed with CYRAMZA plus docetaxel were febrile neutropenia (14%), pneumonia (6%), and neutropenia (5%). The use of granulocyte colony-stimulating factors was 42% in CYRAMZA plus docetaxel-treated patients versus 37% in patients who received placebo plus docetaxel.
• In patients ≥65 years of age, there were 18 (8%) deaths on treatment or within 30 days of discontinuation for CYRAMZA plus docetaxel and 9 (4%) deaths for placebo plus docetaxel. In patients <65 years of age, there were 13 (3%) deaths on treatment or within 30 days of discontinuation for CYRAMZA plus docetaxel and 26 (6%) deaths for placebo plus docetaxel.
• Treatment discontinuation due to adverse reactions occurred more frequently in CYRAMZA plus docetaxel-treated patients (9%) than in placebo plus docetaxel-treated patients (5%). The most common adverse events leading to treatment discontinuation of CYRAMZA were infusion-related reaction (0.5%) and epistaxis (0.3%).
MedDRA=Medical Dictionary for Regulatory Activities.
ADVERSE REACTIONS OCCURRING AT INCIDENCE RATE ≥5% AND A ≥2% DIFFERENCE BETWEEN ARMS IN PATIENTS RECEIVING CYRAMZA
All Grades Grade 3/4
Adverse Reactions (MedDRA) System Organ Class
CYRAMZA + docetaxel
(n=627)
Placebo + docetaxel
(n=618)
CYRAMZA + docetaxel
(n=627)
Placebo + docetaxel
(n=618)
Blood and Lymphatic System Disorders
Febrile neutropenia 16% 10% 16% 10%Neutropenia 55% 46% 49% 40%Thrombocytopenia 13% 5% 3% <1%
Gastrointestinal Disorders
Stomatitis/Mucosal inflammation 37% 19% 7% 2%
Eye Disorders
Lacrimation increased 13% 5% <1% 0%
General Disorders and Administration Site Disorders
Fatigue/Asthenia 55% 50% 14% 11%
Peripheral edema 16% 9% 0% <1%
Respiratory, Thoracic, and Mediastinal Disorders
Epistaxis 19% 7% <1% <1%
Vascular Disorders
Hypertension 11% 5% 6% 2%

41
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
METASTATIC NON-SMALL CELL LUNG CANCER, CONTINUED
CLINICALLY RELEVANT ADVERSE EVENTS ASSOCIATED WITH ANTIANGIOGENIC THERAPY
All Grades Grade ≥3
EventCYRAMZA + docetaxel
(n=627)
Placebo + docetaxel
(n=618)
CYRAMZA + docetaxel
(n=627)
Placebo + docetaxel
(n=618)
Bleeding/Hemorrhaging 29% 15% 2% 2%
Epistaxis 19% 6% <1% <1%
Gastrointestinal hemorrhage 3% 2% 1% <1%Pulmonary hemorrhage 8% 7% 1% 1%
– Hemoptysis 6% 5% 1% 1%
Hypertension 11% 5% 6% 2%
Infusion-related reaction 4% 4% 1% 1%
Proteinuria 3% 1% <1% 0%
Venous thromboembolic event 3% 6% 2% 3%
Renal failure 2% 2% <1% <1%
Arterial thromboembolic event 2% 2% 1% 1%
Congestive heart failure 1% 1% 1% <1%
Gastrointestinal perforation 1% <1% 1% <1%
CLINICALLY RELEVANT ADVERSE EVENTS ASSOCIATED WITH ANTIANGIOGENIC THERAPY
Additional Adverse Events to Consider With CYRAMZA as an Antiangiogenic Therapy23
• For patients with nonsquamous histology, the overall incidence of pulmonary hemorrhage was 7% and the incidence of grade ≥3 pulmonary hemorrhage was 1% for CYRAMZA plus docetaxel compared to 6% overall incidence and 1% for grade ≥3 pulmonary hemorrhage for placebo plus docetaxel. For patients with squamous histology, the overall incidence of pulmonary hemorrhage was 10% and the incidence of grade ≥3 pulmonary hemorrhage was 2% for CYRAMZA plus docetaxel compared to 12% overall incidence and 2% for grade ≥3 pulmonary hemorrhage for placebo plus docetaxel.
• Clinically relevant adverse reactions reported in ≥1% and <5% of CYRAMZA plus docetaxel-treated patients in study 3 were hyponatremia (4.8% CYRAMZA plus docetaxel versus 2.4% for placebo plus docetaxel) and proteinuria (3.3% CYRAMZA plus docetaxel versus 0.8% placebo plus docetaxel).

42
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
METASTATIC NON-SMALL CELL LUNG CANCER, CONTINUED
REVEL Trial Inclusion Criteria24
Patients were eligible for the study only if all of the following criteria were met:1. Disease progression during or after one and only one prior first-line platinum-based chemotherapy regimen
with or without maintenance therapy for advanced/metastatic disease • Recurrent disease after adjuvant or neoadjuvant therapy or patients who had received combined chemotherapy and radiation for locally advanced disease were eligible, if
— Patient had progressive disease within 6 months after completion of adjuvant or neoadjuvant platinum-based therapy (adjuvant therapy was to be considered the patient’s one and only prior first-line, platinum-based chemotherapy); or
— Patient had progressive disease more than 6 months after completion of therapy AND had developed progressive disease on or after one subsequent chemotherapy regimen for advanced/metastatic disease
• Maintenance chemotherapy was defined as therapy given within 42 days after the last dose of platinum-based chemotherapy in patients with ongoing clinical benefit (complete response [CR], partial response [PR], or stable disease [SD]) after platinum-based, first-line induction chemotherapy
• Prior bevacizumab as first-line and/or maintenance therapy was allowed2. Provided signed informed consent and was amenable to compliance with protocol schedules and testing3. Males or females at least 18 years of age4. ECOG PS of 0 or 1 at the time of randomization5. Histologically or cytologically confirmed NSCLC. Mixed NSCLC tumors were categorized by the predominant
cell type • NSCLC tumors that were not otherwise specified (NOS) with regard to histology or could not be sub-classified as squamous, adenocarcinoma, or large cell histology were categorized as nonsquamous
— For squamous cell histology or for centrally located mediastinal masses (<30 mm from the carina) identified by CT scan or chest X-ray, the patient underwent an MRI of the chest or intravenous contrast CT scan within 21 days prior to randomization, to exclude major airway or blood vessel invasion by cancer
6. Stage IV NSCLC disease at the time of randomization (based on the American Joint Committee on Cancer [AJCC], Seventh Edition)
7. Measurable or nonmeasurable disease at the time of randomization documented by CT scan or MRI as defined by RECIST, Version 1.1
8. Resolution to grade ≤1 by the National Cancer Institute Common Terminology Criteria for Adverse Events (NCI-CTCAE), Version 4.0, of all clinically significant toxic effects of prior locoregional therapy, surgery, or other anticancer therapy
SELECT IMPORTANT SAFETY INFORMATIONImpaired Wound Healing• Impaired wound healing can occur with antibodies inhibiting the VEGF pathway. CYRAMZA has not been
studied in patients with serious or nonhealing wounds. CYRAMZA, an antiangiogenic therapy, has the potential to adversely affect wound healing. Discontinue CYRAMZA therapy in patients with impaired wound healing. Withhold CYRAMZA prior to surgery. Resume CYRAMZA following the surgical intervention based on clinical judgment of adequate wound healing. If a patient develops wound healing complications during therapy, discontinue CYRAMZA until the wound is fully healed.
43
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
METASTATIC NON-SMALL CELL LUNG CANCER, CONTINUED
REVEL Trial Inclusion Criteria, Continued24
9. Adequate organ function, defined as: • Total bilirubin less than or equal to the upper limit of normal value (ULN), aspartate aminotransferase (AST) and alanine aminotransferase (ALT) ≤2.5 x ULN, or ≤5 x ULN if the transferase elevation was due to liver metastases • Did not have:
— Cirrhosis at a level of Child-Pugh B (or worse) or — Cirrhosis (any degree) and a history of hepatic encephalopathy or clinically meaningful ascites resulting from cirrhosis. Clinically meaningful ascites was defined as ascites resulting from cirrhosis and requiring ongoing treatment with diuretics and/or paracentesis
• Serum creatinine ≤1.5 x ULN or calculated creatinine clearance ≥50 mL/min (per the Cockcroft-Gault formula or equivalent and/or 24-hour urine collection [Cockcroft-Gault glomerular filtration rate = (140-age) * (Wt in kg) * (0.85 if female)/(72 * Cr) where “Cr” is serum creatinine]) • Absolute neutrophil count (ANC) ≥1.5 x 103/μL (≥1.5 x 109/L), hemoglobin ≥10.0 g/dL (≥6.2 mmol/L), and platelets ≥100 x 103/μL (≥100 x 109/L) • Must have had adequate coagulation function as defined by International Normalized Ratio (INR) ≤1.5 or prothrombin time (PT) ≤1.5 x ULN, and partial thromboplastin time (PTT/aPTT) ≤1.5 x ULN
10. Urinary protein was ≤1+ on dipstick or routine UA. If urine dipstick or routine analysis indicated proteinuria ≥2+, then a 24-hour urine was to be collected and demonstrated <1000 mg of protein in 24 hours to allow participation in the study
11. Eligible patients of reproductive potential (both sexes) agreed to use reliable methods of birth control (hormonal or barrier methods) during the study period and at least 12 weeks after the last dose of study therapy. The label (eg, Summary of Product Characteristics, US package insert, etc) requirements with regard to the methods and duration of contraception during and after treatment with docetaxel can differ between countries. Country-specific requirements applied only if they were more stringent than those already stipulated in the protocol
12. Female patients of childbearing potential must have had a negative serum or urine pregnancy test within 7 days prior to randomization
13. Life expectancy of ≥3 months14. Prior radiation therapy was allowed if:
• In the case of chest radiotherapy at least 28 days had elapsed from the completion of radiation treatment prior to randomization
• In the case of focal or palliative radiation treatment at least 7 days had elapsed from last radiation treatment prior to randomization (and provided that 25% or less of total bone marrow had been irradiated)
• In the case of central nervous system (CNS) radiation (see Exclusion Criteria) at least 14 days had elapsed from the completion of radiation treatment prior to randomization
SELECT IMPORTANT SAFETY INFORMATIONClinical Deterioration in Child-Pugh B or C Cirrhosis• Clinical deterioration, manifested by new onset or worsening encephalopathy, ascites, or hepatorenal
syndrome, was reported in patients with Child-Pugh B or C cirrhosis who received single-agent CYRAMZA. Use CYRAMZA in patients with Child-Pugh B or C cirrhosis only if the potential benefits of treatment are judged to outweigh the risks of clinical deterioration.
44
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
METASTATIC NON-SMALL CELL LUNG CANCER, CONTINUED
REVEL Trial Exclusion Criteria24
Patients were excluded from the study if they met any of the following criteria:1. Disease progression on more than one prior chemotherapy regimen (with or without maintenance therapy)
for advanced and/or metastatic disease2. Only prior treatment for advanced disease was a tyrosine kinase inhibitor (eg, erlotinib)3. Tumor wholly or partially contained small cell lung cancer4. Undergone major surgery within 28 days prior to randomization, or subcutaneous venous access device
placement within 7 days prior to randomization. Furthermore, any patient with postoperative bleeding complications or wound complications from a surgical procedure performed in the last 2 months was to be excluded
5. Had an elective or a planned major surgery during the course of the trial6. Received concurrent treatment with other anticancer therapy, including other chemotherapy,
immunotherapy, hormonal therapy, chemoembolization, or targeted therapy • The last dose of bevacizumab must have been at least 28 days from the time of randomization • The last dose of cytotoxic chemotherapy must have been at least 14 days from the time of randomization
7. Untreated CNS metastases. Patients with treated brain metastases were eligible if they were clinically stable with regard to neurologic function, off steroids after cranial irradiation (whole brain radiation therapy, focal radiation therapy, and stereotactic radiosurgery) ending at least 2 weeks prior to randomization, or after surgical resection performed at least 28 days prior to randomization. The patient may have had no evidence of grade ≥1 CNS hemorrhage based on pretreatment MRI or IV contrast CT scan (performed within 21 days before randomization)
8. Radiologically documented evidence of major blood vessel invasion or encasement by cancer9. Radiographic evidence of intratumor cavitation, regardless of tumor histology
10. A history of uncontrolled hereditary or acquired thrombotic disorder11. Received therapeutic anticoagulation with warfarin, low-molecular weight heparin, or similar agents.
Patients receiving prophylactic, low-dose anticoagulation therapy were eligible provided that the coagulation parameters defined in the inclusion criteria (INR ≤1.5 or PT ≤1.5 x ULN, and PTT/aPTT ≤1.5 x ULN) were met
12. Received chronic therapy with nonsteroidal anti-inflammatory drugs (NSAIDs; eg, indomethacin, ibuprofen, naproxen, or similar agents) or other antiplatelet agents (eg, clopidogrel, ticlopidine, dipyridamole, and anagrelide). Aspirin use at doses up to 325 mg/day was permitted
13. History of gross hemoptysis (defined as bright red blood or ≥1/2 teaspoon) within 2 months prior to randomization
SELECT IMPORTANT SAFETY INFORMATION Reversible Posterior Leukoencephalopathy Syndrome (RPLS)• RPLS has been reported at a rate of <0.1% in clinical studies with CYRAMZA. Confirm the diagnosis
of RPLS with MRI and discontinue CYRAMZA in patients who develop RPLS. Symptoms may resolve or improve within days, although some patients with RPLS can experience ongoing neurologic sequelae or death.
45
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
METASTATIC NON-SMALL CELL LUNG CANCER, CONTINUED
REVEL Trial Exclusion Criteria, Continued24
14. Clinically relevant congestive heart failure (CHF; NYHA II-IV) or symptomatic or poorly controlled cardiac arrhythmia
15. Experienced any arterial thrombotic event, including myocardial infarction, unstable angina, cerebrovascular accident, or transient ischemic attack, within 6 months prior to randomization
16. Uncontrolled arterial hypertension ≥150/≥90 mm Hg despite standard medical management 17. Had a serious or nonhealing wound, ulcer, or bone fracture within 28 days prior to randomization18. Had significant bleeding disorders, vasculitis, or experienced grade 3/4 gastrointestinal (GI) bleeding within
3 months prior to randomization19. History of GI perforation and/or fistulae within 6 months prior to randomization20. Had a bowel obstruction, history or presence of inflammatory enteropathy or extensive intestinal resection
(hemicolectomy or extensive small intestine resection with chronic diarrhea), Crohn's disease, ulcerative colitis, or chronic diarrhea
21. Had peripheral neuropathy grade ≥2 (NCI-CTCAE v 4.0)22. Had a serious illness or medical condition(s) including, but not limited to, the following:
• Known human immunodeficiency virus (HIV) infection or acquired immunodeficiency syndrome (AIDS)-related illness
• Active or uncontrolled clinically serious infection • Previous or concurrent malignancy except for basal or squamous cell skin cancer and/or in situ carcinoma of the cervix, or other solid tumors treated curatively and without evidence of recurrence for at least 3 years prior to randomization
• Uncontrolled metabolic disorders or other nonmalignant organ or systemic diseases or secondary effects of cancer that induced a high medical risk and/or made assessment of survival uncertain
• Other severe acute or chronic medical or psychiatric condition or laboratory abnormality that might have increased the risk associated with study participation or study drug administration, or might have interfered with the interpretation of study results, and in the judgment of the investigator made the patient ineligible for entry into this study
• The patient had significant third-space fluid retention (eg, ascites or pleural effusion), and was not amenable for required repeated drainage
• Known allergy or hypersensitivity reaction to any of the treatment components • Known history of active drug abuse
23. Was pregnant (confirmed by urine or serum beta human chorionic gonadotropin [β-HCG] test within 7 days prior to randomization), or breastfeeding
24. Was enrolled in or discontinued study drug (within 28 days prior to randomization) from a clinical trial involving an investigational drug or device, or concurrently enrolled in any other type of medical research judged not to be scientifically or medically compatible with this study. Patients participating in surveys or observational studies were eligible to participate in this study
25. Prior therapy with docetaxel
SELECT IMPORTANT SAFETY INFORMATION Proteinuria Including Nephrotic Syndrome• In study 4, severe proteinuria occurred more frequently in patients treated with CYRAMZA plus FOLFIRI
compared to patients receiving placebo plus FOLFIRI. Severe proteinuria was reported in 3% of patients treated with CYRAMZA plus FOLFIRI (including 3 cases [0.6%] of nephrotic syndrome) compared to 0.2% of patients treated with placebo plus FOLFIRI. Monitor proteinuria by urine dipstick and/or urinary protein creatinine ratio for the development of worsening of proteinuria during CYRAMZA therapy. (Continued on next page)

46
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
Category 2A Recommendation*
RAMUCIRUMAB† (CYRAMZA) PLUS FOLFIRI
NCCN Guidelines recommend ramucirumab (CYRAMZA) in combination with FOLFIRI as a second-line treatment option† (with a category 2A recommendation)* for metastatic colorectal cancer.
METASTATIC COLORECTAL CANCER
NCCN Guidelines Recommend ramucirumab (CYRAMZA) Plus FOLFIRI as a Second-line Treatment Option in Patients With Metastatic Colorectal Cancer31,32
IndicationCYRAMZA, in combination with FOLFIRI (irinotecan, folinic acid, and 5-fluorouracil), is indicated for the treatment of patients with mCRC with disease progression on or after prior therapy with bevacizumab, oxaliplatin, and a fluoropyrimidine.
* Category 2A recommendation is based on lower-level evidence and there is uniform NCCN consensus that the intervention is appropriate.
†Bevacizumab is the preferred anti-angiogenic agent based on toxicity and/or cost.
SELECT IMPORTANT SAFETY INFORMATIONProteinuria Including Nephrotic Syndrome, Continued• Withhold CYRAMZA for urine protein levels that are ≥2 g over 24 hours. Reinitiate CYRAMZA at a
reduced dose once the urine protein level returns to <2 g over 24 hours. Permanently discontinue CYRAMZA for urine protein levels >3 g over 24 hours or in the setting of nephrotic syndrome.
Thyroid Dysfunction• Monitor thyroid function during treatment with CYRAMZA. In study 4, the incidence of hypothyroidism
reported as an adverse event was 2.6% in the CYRAMZA plus FOLFIRI treated patients and 0.9% in the placebo plus FOLFIRI treated patients.

47
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
METASTATIC COLORECTAL CANCER, CONTINUED
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
mCRC (N=1072)
• Disease progression during or after bevacizumab, oxaliplatin, and a fluoropyrimidine
• ECOG PS 0-1
Placebo
FOLFIRI +
CYRAMZA + FOLFIRI*(n=536)
CYRAMZA 8 mg/kg
FOLFIRI+every 2 weeks
every 2 weeks
STRATIFICATIONFACTORS
Placebo + FOLFIRI*(n=536)
• Geographic region
• KRAS mutation status (mutant vs wild-type)
• Time to disease progression afterbeginning first-line treatment (<6months vs ≥6 months)
1:1Randomization
RAISE Trial Design
RAISE: A pivotal phase III trial of second-line therapy in patients with mCRC with progressive disease (N=1072)1,33
A large, multinational, randomized, double-blind, placebo-controlled trial in patients with disease progression on or after prior therapy with bevacizumab, oxaliplatin, and a fluoropyrimidine.
Major Efficacy Outcome Measure: Overall survival (OS).Supportive Efficacy Outcome Measure: Progression-free survival (PFS). Patients received treatment until disease progression or unacceptable toxicity.
* Irinotecan 180 mg/m2 IV over 90 minutes and folinic acid 400 mg/m2 IV simultaneously over 120 minutes; followed by 5-fluorouracil 400 mg/m2 IV bolus over 2 to 4 minutes; followed by 5-fluorouracil 2400 mg/m2 IV by continuous infusion over 46 to 48 hours.KRAS=Kirsten rat sarcoma oncogene homolog.
• For full inclusion and exclusion criteria, please see pages 53-54
SELECT IMPORTANT SAFETY INFORMATIONEmbryofetal Toxicity• Based on its mechanism of action, CYRAMZA can cause fetal harm when administered to pregnant
women. Animal models link angiogenesis, VEGF, and VEGF Receptor 2 (VEGFR2) to critical aspects of female reproduction, embryofetal development, and postnatal development. Advise pregnant women of the potential risk to a fetus. Advise females of reproductive potential to use effective contraception during treatment with CYRAMZA and for at least 3 months after the last dose of CYRAMZA.
Hemorrhage• CYRAMZA increased the risk of hemorrhage and gastrointestinal hemorrhage including severe and
sometimes fatal hemorrhagic events. In study 1, which evaluated CYRAMZA as a single agent in advanced gastric cancer, the incidence of severe bleeding was 3.4% for CYRAMZA and 2.6% for placebo. In study 2, which evaluated CYRAMZA plus paclitaxel in advanced gastric cancer, the incidence of severe bleeding was 4.3% for CYRAMZA plus paclitaxel and 2.4% for placebo plus paclitaxel. Patients with gastric cancer receiving nonsteroidal anti-inflammatory drugs (NSAIDs) were excluded from enrollment in studies 1 and 2; therefore, the risk of gastric hemorrhage in CYRAMZA-treated patients with gastric tumors receiving NSAIDs is unknown. (Continued on page 49)

48
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
METASTATIC COLORECTAL CANCER, CONTINUED
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
RAISE Trial Design, ContinuedTreatment monitoring and patient management34
• Patients had a urinalysis (UA) every 6 weeks. If a patient had proteinuria ≥2+, a 24-hour urine collection was conducted per the protocol
• There was a mandatory 60-minute observation period after the first two infusions of CYRAMZA to monitor for IRRs. The observation period was eliminated from further infusions if there was no evidence of an IRR
• In the RAISE protocol, all subsequent doses were modified/reduced if dose modification/rate reduction was needed because of an IRR
• At every infusion, the following were performed: — Physical examination, including height (at baseline only) and weight measurements — Vital signs, including blood pressure, pulse rate, respiration rate, and temperature — Liver function tests — Toxicity/AE assessment — Concomitant medication assessment — Hematology profile — Chemistry profile
• Every 2 cycles, the following was performed: — ECOG performance status
• Every 3 cycles, the following were performed: — Coagulation profile — Urinalysis testing, including routine dipstick measurements and, if clinically indicated, microscopic analysis — TSH levels, including a complete thyroid evaluation using an investigator-designated (local) laboratory — Imaging studies/tumor assessment — Serum CEA — β-HCG pregnancy test
• Alterations in CYRAMZA administration, dependent upon the infusion-related reaction grade: — For a grade 1 IRR, it was not required to stop the infusion. For subsequent infusions, patients were premedicated with diphenhydramine hydrochloride 50 mg IV (or equivalent); additional premedication could be administered at the investigator’s discretion
— For a grade 2 IRR, the infusion was stopped, but the site could resume the infusion at 50% of the prior rate once the infusion reaction had resolved or decreased to grade 1. The infusion duration could not have exceeded 2 hours. For subsequent infusions, patients were premedicated with diphenhydramine hydrochloride 50 mg IV (or equivalent); additional premedication could be administered at the investigator’s discretion
— For grade 3 or 4 IRRs, the infusion was stopped and CYRAMZA permanently discontinued — For any infusion-related reaction, other medications could be administrated based upon clinical discretion
• For patients on CYRAMZA, major surgery was postponed until at least 28 days after the last dose of CYRAMZA (when possible), and CYRAMZA was not restarted for at least 28 days after surgery along with the wound being fully healed.35 If subcutaneous venous access device placement was required during the course of therapy, it was recommended that a 7-day treatment-free period occur both prior to and following placement34
SELECT IMPORTANT SAFETY INFORMATIONInfusion-Related Reactions (IRRs)• Prior to the institution of premedication recommendations across clinical trials of CYRAMZA, IRRs occurred
in 6 out of 37 patients (16%), including 2 severe events. The majority of IRRs across trials occurred during or following a first or second CYRAMZA infusion. Symptoms of IRRs included rigors/tremors, back pain/spasms, chest pain and/or tightness, chills, flushing, dyspnea, wheezing, hypoxia, and paresthesia. In severe cases, symptoms included bronchospasm, supraventricular tachycardia, and hypotension. Monitor patients during the infusion for signs and symptoms of IRRs in a setting with available resuscitation equipment. Immediately and permanently discontinue CYRAMZA for grade 3 or 4 IRRs.

49
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
METASTATIC COLORECTAL CANCER, CONTINUED
RAISE: DEMOGRAPHIC AND BASELINE CHARACTERISTICS
CYRAMZA + FOLFIRI
(n=536)
Placebo + FOLFIRI
(n=536)Age, median (range) 62 (21-83) 62 (33-87)
Male* 54% 61%
Ethnic origin*Caucasian 76% 77%Asian 21% 19%
ECOG PS0 49% 48%1 50% 51%
Disease stage at initial diagnosis, n (%)
Stages I-IIIC 24% 24%Stage IV 76% 76%
KRAS status at study entry, n (%)Mutant 50% 49%Wild-type 50% 51%
<6 months from time to disease progression after beginning first-line treatment† 23% 24%
Prior therapyPrior bevacizumab use ≥3 months 85% 80%Prior oxaliplatin use ≥3 months 87% 85%Prior fluoropyrimidine use ≥3 months 93% 90%
RAISE Patient Population
Demographics and baseline characteristics were similar between treatment arms in the RAISE trial1,36-38
RAISE: DEMOGRAPHIC AND BASELINE CHARACTERISTICS
Based on intent-to-treat population.*Percentages are based on the total population size (N=1072).†Based on case report form (CRF) data if present, or interactive voice response system (IVRS) value if CRF data were missing for the parameter.
SELECT IMPORTANT SAFETY INFORMATIONHemorrhage, Continued• In study 3, which evaluated CYRAMZA plus docetaxel in metastatic non-small cell lung cancer (NSCLC),
the incidence of severe bleeding was 2.4% for CYRAMZA plus docetaxel and 2.3% for placebo plus docetaxel. Patients with NSCLC receiving therapeutic anticoagulation or chronic therapy with NSAIDs or other antiplatelet therapy other than once-daily aspirin or with radiographic evidence of major airway or blood vessel invasion or intratumor cavitation were excluded from study 3; therefore, the risk of pulmonary hemorrhage in these groups of patients is unknown. (Continued on next page)

50
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
METASTATIC COLORECTAL CANCER, CONTINUED
RAISE Efficacy
CYRAMZA plus FOLFIRI demonstrated a statistically significant improvement in overall survival1
OS P
ROBA
BILI
TY
0 3 6 9 12 15 18 21 24 27 30 33 36 39 42
TIME (MONTHS)
497 421 345 269 195 114536
536
CYRAMZA+ FOLFIRIPlacebo+ FOLFIRI 486 400 329 228 166 108
Number at Risk
78 53 34 22 12 4
66 44 22 10 2 2
0
1
0
0
CYRAMZA+ FOLFIRIPlacebo+ FOLFIRI
Hazard Ratio (95% CI)=0.85 (0.73, 0.98); P=0.023
13.3MONTHS
CYRAMZA+ FOLFIRI
(n=536)
(12.4, 14.5)
Placebo+ FOLFIRI(n=536)
MONTHS11.7
(10.8, 12.7)
1.0
0.8
0.6
0.4
0.2
0.0
Major Outcome Measure Overall Survival:
Median—Months (95% CI)
Supportive Outcome Measure Progression-Free Survival:
Median—Months (95% CI)
PFS
PROB
ABIL
ITY
1.0
0.8
0.6
0.4
0.2
0.0
0 3 6 9 12 15 18 21 24 27 30 33 36 39 42
TIME (MONTHS)
381 234 142 77 38 20536
536
CYRAMZA+ FOLFIRIPlacebo+ FOLFIRI 345 182 92 52 31 17
Number at Risk
11 6 5 2 1 1
10 3 1 0 0 0
0
0
0
0
CYRAMZA+ FOLFIRIPlacebo+ FOLFIRI
Hazard Ratio (95% CI)=0.79 (0.70, 0.90); P<0.001
CYRAMZA+ FOLFIRI(n=536) 5.7
MONTHS(5.5, 6.2)
Placebo+ FOLFIRI(n=536)
MONTHS4.5(4.2, 5.4)
• The treatment effect was consistent across prespecified stratification factors
• The percentage of deaths at the time of analysis was 69% (372 patients) and 74% (397 patients) in the CYRAMZA plus FOLFIRI and placebo plus FOLFIRI arms, respectively
The phase III RAISE trial evaluated the efficacy and safety of CYRAMZA plus FOLFIRI vs placebo plus FOLFIRI in patients with mCRC with disease progression on or after prior therapy with bevacizumab, oxaliplatin, and a fluoropyrimidine. Major efficacy outcome measure was OS. Supportive efficacy outcome measure was PFS. All patients were required to have ECOG PS 0 or 1. Patients were stratified by geographic region, KRAS mutation status, and time to disease progression after the beginning of first-line treatment (<6 months vs ≥6 months). Patients were randomized 1:1 (N=1072) to receive either CYRAMZA 8 mg/kg or placebo, in combination with FOLFIRI every 14 days.1
SELECT IMPORTANT SAFETY INFORMATION Hemorrhage, Continued • In study 4, which evaluated CYRAMZA plus FOLFIRI in metastatic colorectal cancer, the incidence of
severe bleeding was 2.5% for CYRAMZA plus FOLFIRI and 1.7% for placebo plus FOLFIRI. Permanently discontinue CYRAMZA in patients who experience severe bleeding.
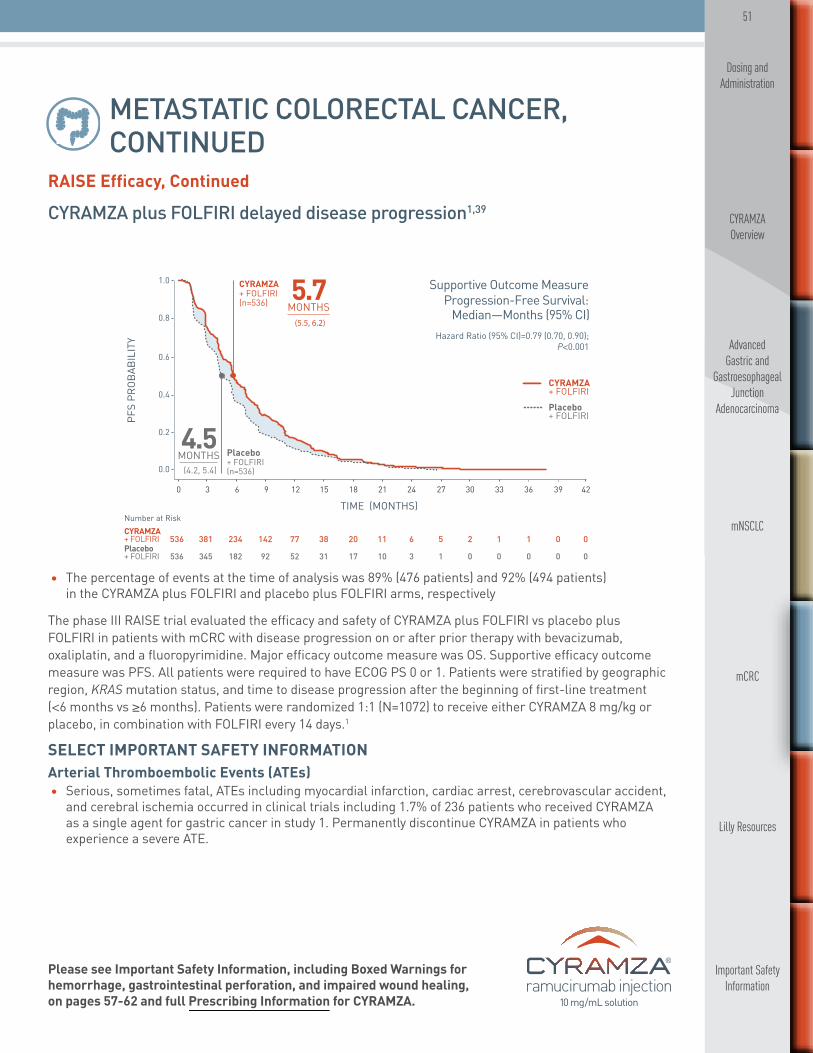
51
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
METASTATIC COLORECTAL CANCER, CONTINUED
OS P
ROBA
BILI
TY
0 3 6 9 12 15 18 21 24 27 30 33 36 39 42
TIME (MONTHS)
497 421 345 269 195 114536
536
CYRAMZA+ FOLFIRIPlacebo+ FOLFIRI 486 400 329 228 166 108
Number at Risk
78 53 34 22 12 4
66 44 22 10 2 2
0
1
0
0
CYRAMZA+ FOLFIRIPlacebo+ FOLFIRI
Hazard Ratio (95% CI)=0.85 (0.73, 0.98); P=0.023
13.3MONTHS
CYRAMZA+ FOLFIRI
(n=536)
(12.4, 14.5)
Placebo+ FOLFIRI(n=536)
MONTHS11.7
(10.8, 12.7)
1.0
0.8
0.6
0.4
0.2
0.0
Major Outcome Measure Overall Survival:
Median—Months (95% CI)
Supportive Outcome Measure Progression-Free Survival:
Median—Months (95% CI)
PFS
PROB
ABIL
ITY
1.0
0.8
0.6
0.4
0.2
0.0
0 3 6 9 12 15 18 21 24 27 30 33 36 39 42
TIME (MONTHS)
381 234 142 77 38 20536
536
CYRAMZA+ FOLFIRIPlacebo+ FOLFIRI 345 182 92 52 31 17
Number at Risk
11 6 5 2 1 1
10 3 1 0 0 0
0
0
0
0
CYRAMZA+ FOLFIRIPlacebo+ FOLFIRI
Hazard Ratio (95% CI)=0.79 (0.70, 0.90); P<0.001
CYRAMZA+ FOLFIRI(n=536) 5.7
MONTHS(5.5, 6.2)
Placebo+ FOLFIRI(n=536)
MONTHS4.5(4.2, 5.4)
RAISE Efficacy, Continued
CYRAMZA plus FOLFIRI delayed disease progression1,39
• The percentage of events at the time of analysis was 89% (476 patients) and 92% (494 patients) in the CYRAMZA plus FOLFIRI and placebo plus FOLFIRI arms, respectively
The phase III RAISE trial evaluated the efficacy and safety of CYRAMZA plus FOLFIRI vs placebo plus FOLFIRI in patients with mCRC with disease progression on or after prior therapy with bevacizumab, oxaliplatin, and a fluoropyrimidine. Major efficacy outcome measure was OS. Supportive efficacy outcome measure was PFS. All patients were required to have ECOG PS 0 or 1. Patients were stratified by geographic region, KRAS mutation status, and time to disease progression after the beginning of first-line treatment (<6 months vs ≥6 months). Patients were randomized 1:1 (N=1072) to receive either CYRAMZA 8 mg/kg or placebo, in combination with FOLFIRI every 14 days.1
SELECT IMPORTANT SAFETY INFORMATION Arterial Thromboembolic Events (ATEs)• Serious, sometimes fatal, ATEs including myocardial infarction, cardiac arrest, cerebrovascular accident,
and cerebral ischemia occurred in clinical trials including 1.7% of 236 patients who received CYRAMZA as a single agent for gastric cancer in study 1. Permanently discontinue CYRAMZA in patients who experience a severe ATE.

52
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
METASTATIC COLORECTAL CANCER, CONTINUED
Adverse Reaction Profile for CYRAMZA in Combination With FOLFIRI1,40
ADVERSE REACTIONS OCCURRING AT INCIDENCE RATE ≥5% AND A ≥2% DIFFERENCE BETWEEN ARMS IN PATIENTS RECEIVING CYRAMZA
All Grades Grade ≥3
Adverse Reactions (MedDRA) System Organ Class
CYRAMZA+FOLFIRI (n=529)
Placebo +FOLFIRI (n=528)
CYRAMZA+FOLFIRI (n=529)
Placebo +FOLFIRI (n=528)
Blood and Lymphatic System DisordersNeutropenia 59% 46% 38% 23%Thrombocytopenia 28% 14% 3% <1%
Gastrointestinal Disorders
Gastrointestinal hemorrhage events 12% 7% 2% 1%
Decreased appetite 37% 27% 2% 2%
Diarrhea 60% 51% 11% 10%
Stomatitis 31% 21% 4% 2%
General Disorders and Administration Site Disorders
Peripheral edema 20% 9% <1% 0%
Metabolism and Nutrition Disorders
Hypoalbuminemia 6% 2% 1% 0%
Renal and Urinary DisordersProteinuria* 17% 5% 3% <1%
Respiratory, Thoracic, and Mediastinal Disorders
Epistaxis 33% 15% 0% 0%
Skin and Subcutaneous Tissue DisordersPalmar-plantar erythrodysesthesia syndrome 13% 5% 1% <1%
Vascular Disorders
Hypertension 26% 9% 11% 3%
*Includes 3 patients with nephrotic syndrome in the CYRAMZA plus FOLFIRI treatment group.
• The most common serious adverse events with CYRAMZA plus FOLFIRI were diarrhea (3.6%), intestinal obstruction (3.0%), and febrile neutropenia (2.8%).
• Treatment discontinuation of any study drug due to adverse reactions occurred more frequently in CYRAMZA plus FOLFIRI-treated patients (29%) than in placebo plus FOLFIRI-treated patients (13%). The most common adverse reactions leading to discontinuation of any component of CYRAMZA plus FOLFIRI as compared to placebo plus FOLFIRI, were neutropenia (12.5% versus 5.3%) and thrombocytopenia (4.2% versus 0.8%). The most common adverse reactions leading to treatment discontinuation of CYRAMZA were proteinuria (1.5%) and gastrointestinal perforation (1.7%).
• Clinically relevant adverse reactions reported in ≥1% and <5% of CYRAMZA plus FOLFIRI-treated patients in study 4 consisted of gastrointestinal perforation (1.7% CYRAMZA plus FOLFIRI versus 0.6% for placebo plus FOLFIRI).
53
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
METASTATIC COLORECTAL CANCER, CONTINUED
RAISE Trial Inclusion Criteria41
Each patient must have met the following criteria to be enrolled in this study:1. Histologically or cytologically confirmed colorectal cancer, excluding primary tumors of appendiceal origin
(participants were eligible to enroll irrespective of KRAS mutation status)2. Confirmed metastatic colorectal cancer (stage IV)3. The participant had received first-line combination therapy of bevacizumab, oxaliplatin, and a
fluoropyrimidine for metastatic disease and (a) experienced radiographic disease progression during first-line therapy, or (b) experienced radiographic disease progression ≤6 months after the last dose of first-line therapy, or (c) discontinued part or all of first-line therapy due to toxicity and experienced radiographic disease progression ≤6 months after the last dose of first-line therapy. Note that a participant must have received a minimum of two doses of bevacizumab as part of a first-line regimen containing chemotherapy; in addition, a participant must have received at least one cycle of first-line therapy that included bevacizumab, oxaliplatin and a fluoropyrimidine in the same cycle. Note that a participant must not have received more than two different fluoropyrimidines as part of a first-line regimen; disease progression was not an acceptable reason for discontinuing one fluoropyrimidine and starting a second fluoropyrimidine
4. Receipt of no more than two prior systemic chemotherapy regimens in any setting (only one prior regimen for metastatic disease was permitted); for participants with rectal cancer, sequential neoadjuvant and adjuvant therapy counted as a single systemic regimen. Note that rechallenge with oxaliplatin was permitted and was considered part of the first-line regimen for metastatic disease, both initial oxaliplatin treatment and subsequent rechallenge were considered as one regimen
5. Measurable or nonmeasurable disease based on the Response Evaluation Criteria in Solid Tumors, Version 1.1 (RECIST v 1.1)
6. ECOG PS score of 0 or 17. Adequate hematologic, renal and hepatic function8. Adequate coagulation function (International Normalized Ratio [INR] ≤1.5 and Partial Thromboplastin Time
[PTT] or activated PTT [aPTT] ≤1.5 x upper limit of normal [ULN]). Participants on full-dose anticoagulation must have been on a stable dose of anticoagulant therapy and if on oral anticoagulation, must have had an INR ≤3 and no clinically significant active bleeding or pathological condition that carried a high risk of bleeding
9. Consent to provide a historical colorectal cancer tissue sample for assessment of biomarkers and the tumor tissue sample was available
10. Ability to provide signed informed consent
SELECT IMPORTANT SAFETY INFORMATIONHypertension • An increased incidence of severe hypertension occurred in patients receiving CYRAMZA as a single agent
(8%) as compared to placebo (3%), in patients receiving CYRAMZA plus paclitaxel (15%) as compared to placebo plus paclitaxel (3%), and in patients receiving CYRAMZA plus docetaxel (6%) as compared to placebo plus docetaxel (2%), and in patients receiving CYRAMZA plus FOLFIRI (11%) as compared to placebo plus FOLFIRI (3%). Control hypertension prior to initiating treatment with CYRAMZA. Monitor blood pressure every 2 weeks or more frequently as indicated during treatment. Temporarily suspend CYRAMZA for severe hypertension until medically controlled. Permanently discontinue CYRAMZA if medically significant hypertension cannot be controlled with antihypertensive therapy or in patients with hypertensive crisis or hypertensive encephalopathy.

54
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
METASTATIC COLORECTAL CANCER, CONTINUED
RAISE Trial Exclusion Criteria41
Patients who met any of the following criteria were excluded from the study:1. Receipt of bevacizumab ≤28 days prior to randomization2. Receipt of any investigational therapy for nononcology clinical indication ≤28 days prior to randomization3. Receipt of any previous systemic therapy, other than a combination of bevacizumab, oxaliplatin, and a
fluoropyrimidine, for first-line treatment of metastatic colorectal cancer4. Known leptomeningeal disease or brain metastases or uncontrolled spinal cord compression (currently or
in the past)5. Experienced any arterial thrombotic or arterial thromboembolic events, including, but not limited to,
myocardial infarction, transient ischemic attack, or cerebrovascular accident, ≤12 months prior to randomization
6. Pregnant (confirmed by serum beta human chorionic gonadotropin [ß HCG] test ≤7 days prior to randomization) or lactating
7. History of inflammatory bowel disease or Crohn's disease requiring medical intervention (immunomodulatory or immunosuppressive medications or surgery) ≤12 months prior to randomization
8. Acute or subacute bowel obstruction or history of chronic diarrhea that was considered clinically significant in the opinion of the investigator
9. Grade 3 or higher bleeding event ≤3 months prior to randomization10. Experienced any of the following during first-line therapy with a bevacizumab containing regimen: an
arterial thrombotic/thromboembolic event, grade 4 hypertension, grade 3 proteinuria, a grade 3/4 bleeding event, or bowel perforation
11. Known history or clinical evidence of Gilbert's Syndrome, or was known to have any of the following genotypes: UGT1A1*6/*6, UGT1A1*28/*28, or UGT1A1*6/*28
12. Known allergy to any of the study treatment components, including any components used in the preparation of ramucirumab, or other contraindication to receive the study treatments
13. Cirrhosis at a level of Child-Pugh B (or worse) or cirrhosis (any degree) and a history of hepatic encephalopathy or clinical meaningful ascites resulting from cirrhosis; clinically meaningful ascites was defined as ascites resulting from cirrhosis and requiring ongoing treatment with diuretics and/ or paracentesis
SELECT IMPORTANT SAFETY INFORMATIONInfusion-Related Reactions (IRRs)• Prior to the institution of premedication recommendations across clinical trials of CYRAMZA, IRRs occurred
in 6 out of 37 patients (16%), including 2 severe events. The majority of IRRs across trials occurred during or following a first or second CYRAMZA infusion. Symptoms of IRRs included rigors/tremors, back pain/spasms, chest pain and/or tightness, chills, flushing, dyspnea, wheezing, hypoxia, and paresthesia. In severe cases, symptoms included bronchospasm, supraventricular tachycardia, and hypotension. Monitor patients during the infusion for signs and symptoms of IRRs in a setting with available resuscitation equipment. Immediately and permanently discontinue CYRAMZA for grade 3 or 4 IRRs.
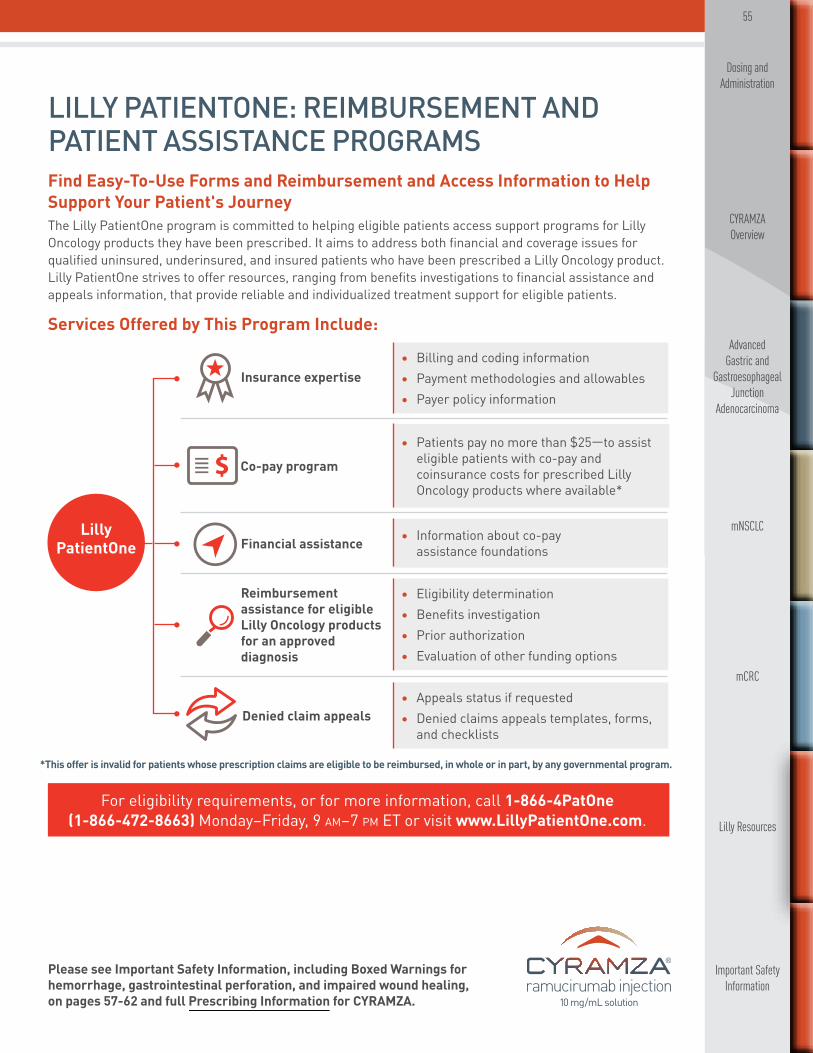
55
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
LILLY PATIENTONE: REIMBURSEMENT AND PATIENT ASSISTANCE PROGRAMSFind Easy-To-Use Forms and Reimbursement and Access Information to Help Support Your Patient's Journey The Lilly PatientOne program is committed to helping eligible patients access support programs for Lilly Oncology products they have been prescribed. It aims to address both financial and coverage issues for qualified uninsured, underinsured, and insured patients who have been prescribed a Lilly Oncology product. Lilly PatientOne strives to offer resources, ranging from benefits investigations to financial assistance and appeals information, that provide reliable and individualized treatment support for eligible patients.
Services Offered by This Program Include:
*This offer is invalid for patients whose prescription claims are eligible to be reimbursed, in whole or in part, by any governmental program.
Insurance expertise• Billing and coding information • Payment methodologies and allowables • Payer policy information
Reimbursement assistance for eligible Lilly Oncology products for an approved diagnosis
• Eligibility determination • Benefits investigation • Prior authorization • Evaluation of other funding options
Denied claim appeals• Appeals status if requested • Denied claims appeals templates, forms,
and checklists
Financial assistance • Information about co-pay assistance foundations
Co-pay program
• Patients pay no more than $25—to assist eligible patients with co-pay and coinsurance costs for prescribed Lilly Oncology products where available*
Lilly PatientOne
For eligibility requirements, or for more information, call 1-866-4PatOne (1-866-472-8663) Monday–Friday, 9 am–7 pm ET or visit www.LillyPatientOne.com.

56
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
Please see Important Safety Information, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing, on pages 57-62 and full Prescribing Information for CYRAMZA.
LILLY RESOURCESLilly MedicalContact Lilly Medical for Answers to Additional Medical Questions
56
For product supply questions, please call 1-800-821-0538 Monday–Friday, 8 am–5 pm ET or visit www.LillyTrade.com.
Visit www.LillyMedical.com, where you can submit a written question or chat electronically with a medical professional.
Call the Lilly Answers Center (TLAC) 1-800-LillyRx (1-800-545-5979) to speak with a medical professional by phone.
LillyTrade.com Contact Lilly Trade for Information on Product Ordering or ReturnsThe website is designed to provide helpful information on purchasing, dispensing, or returning Lilly products.
57
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
Please see Important Safety Information continued on pages 58-62 and full Prescribing Information for CYRAMZA, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing.
IMPORTANT SAFETY INFORMATION FOR CYRAMZA
Warnings and PrecautionsHemorrhage • CYRAMZA increased the risk of hemorrhage and gastrointestinal hemorrhage including severe
and sometimes fatal hemorrhagic events. In study 1, which evaluated CYRAMZA as a single agent in advanced gastric cancer, the incidence of severe bleeding was 3.4% for CYRAMZA and 2.6% for placebo. In study 2, which evaluated CYRAMZA plus paclitaxel in advanced gastric cancer, the incidence of severe bleeding was 4.3% for CYRAMZA plus paclitaxel and 2.4% for placebo plus paclitaxel. Patients with gastric cancer receiving nonsteroidal anti-inflammatory drugs (NSAIDs) were excluded from enrollment in studies 1 and 2; therefore, the risk of gastric hemorrhage in CYRAMZA-treated patients with gastric tumors receiving NSAIDs is unknown. In study 3, which evaluated CYRAMZA plus docetaxel in metastatic non-small cell lung cancer (NSCLC), the incidence of severe bleeding was 2.4% for CYRAMZA plus docetaxel and 2.3% for placebo plus docetaxel. Patients with NSCLC receiving therapeutic anticoagulation or chronic therapy with NSAIDs or other antiplatelet therapy other than once-daily aspirin or with radiographic evidence of major airway or blood vessel invasion or intratumor cavitation were excluded from study 3; therefore, the risk of pulmonary hemorrhage in these groups of patients is unknown. In study 4, which evaluated CYRAMZA plus FOLFIRI in metastatic colorectal cancer, the incidence of severe bleeding was 2.5% for CYRAMZA plus FOLFIRI and 1.7% for placebo plus FOLFIRI. Permanently discontinue CYRAMZA in patients who experience severe bleeding.
Arterial Thromboembolic Events (ATEs)• Serious, sometimes fatal, ATEs including myocardial infarction, cardiac arrest, cerebrovascular
accident, and cerebral ischemia occurred in clinical trials including 1.7% of 236 patients who received CYRAMZA as a single agent for gastric cancer in study 1. Permanently discontinue CYRAMZA in patients who experience a severe ATE.
WARNING: HEMORRHAGE, GASTROINTESTINAL PERFORATION, AND IMPAIRED WOUND HEALINGHemorrhage: CYRAMZA increased the risk of hemorrhage and gastrointestinal hemorrhage, including severe and sometimes fatal hemorrhagic events. Permanently discontinue CYRAMZA in patients who experience severe bleeding.Gastrointestinal Perforation: CYRAMZA can increase the risk of gastrointestinal perforation, a potentially fatal event. Permanently discontinue CYRAMZA in patients who experience a gastrointestinal perforation.Impaired Wound Healing: Impaired wound healing can occur with antibodies inhibiting the VEGF pathway. Discontinue CYRAMZA therapy in patients with impaired wound healing. Withhold CYRAMZA prior to surgery and discontinue CYRAMZA if a patient develops wound healing complications.

58
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
IMPORTANT SAFETY INFORMATION FOR CYRAMZA, CONTINUEDHypertension• An increased incidence of severe hypertension occurred in patients receiving CYRAMZA as a single
agent (8%) as compared to placebo (3%), in patients receiving CYRAMZA plus paclitaxel (15%) as compared to placebo plus paclitaxel (3%), and in patients receiving CYRAMZA plus docetaxel (6%) as compared to placebo plus docetaxel (2%), and in patients receiving CYRAMZA plus FOLFIRI (11%) as compared to placebo plus FOLFIRI (3%). Control hypertension prior to initiating treatment with CYRAMZA. Monitor blood pressure every 2 weeks or more frequently as indicated during treatment. Temporarily suspend CYRAMZA for severe hypertension until medically controlled. Permanently discontinue CYRAMZA if medically significant hypertension cannot be controlled with antihypertensive therapy or in patients with hypertensive crisis or hypertensive encephalopathy.
Infusion-Related Reactions (IRRs) • Prior to the institution of premedication recommendations across clinical trials of CYRAMZA, IRRs
occurred in 6 out of 37 patients (16%), including 2 severe events. The majority of IRRs across trials occurred during or following a first or second CYRAMZA infusion. Symptoms of IRRs included rigors/tremors, back pain/spasms, chest pain and/or tightness, chills, flushing, dyspnea, wheezing, hypoxia, and paresthesia. In severe cases, symptoms included bronchospasm, supraventricular tachycardia, and hypotension. Monitor patients during the infusion for signs and symptoms of IRRs in a setting with available resuscitation equipment. Immediately and permanently discontinue CYRAMZA for grade 3 or 4 IRRs.
Gastrointestinal Perforations• CYRAMZA is an antiangiogenic therapy that can increase the risk of gastrointestinal perforation, a
potentially fatal event. Four of 570 patients (0.7%) who received CYRAMZA as a single agent in advanced gastric cancer clinical trials experienced gastrointestinal perforation. In study 2, the incidence of gastrointestinal perforation was 1.2% for CYRAMZA plus paclitaxel as compared to 0.3% for placebo plus paclitaxel. In study 3, the incidence of gastrointestinal perforation was 1% for CYRAMZA plus docetaxel as compared to 0.3% for placebo plus docetaxel. In study 4, the incidence of gastrointestinal perforation was 1.7% for CYRAMZA plus FOLFIRI and 0.6% for placebo plus FOLFIRI. Permanently discontinue CYRAMZA in patients who experience a gastrointestinal perforation.
Impaired Wound Healing• Impaired wound healing can occur with antibodies inhibiting the VEGF pathway. CYRAMZA has not
been studied in patients with serious or nonhealing wounds. CYRAMZA, an antiangiogenic therapy, has the potential to adversely affect wound healing. Discontinue CYRAMZA therapy in patients with impaired wound healing. Withhold CYRAMZA prior to surgery. Resume CYRAMZA following the surgical intervention based on clinical judgment of adequate wound healing. If a patient develops wound healing complications during therapy, discontinue CYRAMZA until the wound is fully healed.
Clinical Deterioration in Child-Pugh B or C Cirrhosis• Clinical deterioration, manifested by new onset or worsening encephalopathy, ascites, or hepatorenal
syndrome, was reported in patients with Child-Pugh B or C cirrhosis who received single-agent CYRAMZA. Use CYRAMZA in patients with Child-Pugh B or C cirrhosis only if the potential benefits of treatment are judged to outweigh the risks of clinical deterioration.
Please see Important Safety Information continued on pages 59-62 and full Prescribing Information for CYRAMZA, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing.
59
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
IMPORTANT SAFETY INFORMATION FOR CYRAMZA, CONTINUEDReversible Posterior Leukoencephalopathy Syndrome (RPLS)• RPLS has been reported at a rate of <0.1% in clinical studies with CYRAMZA. Confirm the diagnosis
of RPLS with MRI and discontinue CYRAMZA in patients who develop RPLS. Symptoms may resolve or improve within days, although some patients with RPLS can experience ongoing neurologic sequelae or death.
Proteinuria Including Nephrotic Syndrome• In study 4, severe proteinuria occurred more frequently in patients treated with CYRAMZA plus
FOLFIRI compared to patients receiving placebo plus FOLFIRI. Severe proteinuria was reported in 3% of patients treated with CYRAMZA plus FOLFIRI (including 3 cases [0.6%] of nephrotic syndrome) compared to 0.2% of patients treated with placebo plus FOLFIRI. Monitor proteinuria by urine dipstick and/or urinary protein creatinine ratio for the development of worsening of proteinuria during CYRAMZA therapy. Withhold CYRAMZA for urine protein levels that are ≥2 g over 24 hours. Reinitiate CYRAMZA at a reduced dose once the urine protein level returns to <2 g over 24 hours. Permanently discontinue CYRAMZA for urine protein levels >3 g over 24 hours or in the setting of nephrotic syndrome.
Thyroid Dysfunction• Monitor thyroid function during treatment with CYRAMZA. In study 4, the incidence of
hypothyroidism reported as an adverse event was 2.6% in the CYRAMZA plus FOLFIRI-treated patients and 0.9% in the placebo plus FOLFIRI-treated patients.
Embryofetal Toxicity• Based on its mechanism of action, CYRAMZA can cause fetal harm when administered to pregnant
women. Animal models link angiogenesis, VEGF, and VEGF Receptor 2 (VEGFR2) to critical aspects of female reproduction, embryofetal development, and postnatal development. Advise pregnant women of the potential risk to a fetus. Advise females of reproductive potential to use effective contraception during treatment with CYRAMZA and for at least 3 months after the last dose of CYRAMZA.
Most Common Adverse Reactions—Single Agent• The most commonly reported adverse reactions (all grades; grade 3/4) occurring in ≥5% of patients
receiving CYRAMZA and ≥2% higher than placebo in study 1 were hypertension (16% vs 8%; 8% vs 3%), diarrhea (14% vs 9%; 1% vs 2%), headache (9% vs 3%; 0% vs 0%), and hyponatremia (6% vs 2%; 3% vs 1%).
• The most common serious adverse events with CYRAMZA in study 1 were anemia (3.8%) and intestinal obstruction (2.1%). Red blood cell transfusions were given to 11% of CYRAMZA-treated patients vs 8.7% of patients who received placebo.
• Clinically relevant adverse reactions reported in ≥1% and <5% of CYRAMZA-treated patients vs placebo in study 1 were: neutropenia (4.7% vs 0.9%), epistaxis (4.7% vs 0.9%), rash (4.2% vs 1.7%), intestinal obstruction (2.1% vs 0%), and arterial thromboembolic events (1.7% vs 0%).
Please see Important Safety Information continued on pages 60-62 and full Prescribing Information for CYRAMZA, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing.

60
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
IMPORTANT SAFETY INFORMATION FOR CYRAMZA, CONTINUEDMost Common Adverse Reactions—Single Agent, Continued • Across clinical trials of CYRAMZA administered as a single agent, clinically relevant adverse
reactions (including grade ≥3) reported in CYRAMZA-treated patients included proteinuria, gastrointestinal perforation, and infusion-related reactions. In study 1, according to laboratory assessment, 8% of CYRAMZA-treated patients developed proteinuria vs 3% of placebo-treated patients. Two patients discontinued CYRAMZA due to proteinuria. The rate of gastrointestinal perforation in study 1 was 0.8% and the rate of infusion-related reactions was 0.4%.
Most Common Adverse Reactions—Combination With Paclitaxel• The most commonly reported adverse reactions (all grades; grade 3/4) occurring in ≥5% of patients
receiving CYRAMZA plus paclitaxel and ≥2% higher than placebo plus paclitaxel in study 2 were fatigue/asthenia (57% vs 44%; 12% vs 6%), neutropenia (54% vs 31%; 41% vs 19%), diarrhea (32% vs 23%; 4% vs 2%), epistaxis (31% vs 7%; 0% vs 0%), hypertension (25% vs 6%; 15% vs 3%), peripheral edema (25% vs 14%; 2% vs 1%), stomatitis (20% vs 7%; 1% vs 1%), proteinuria (17% vs 6%; 1% vs 0%), thrombocytopenia (13% vs 6%; 2% vs 2%), hypoalbuminemia (11% vs 5%; 1% vs 1%), and gastrointestinal hemorrhage events (10% vs 6%; 4% vs 2%).
• The most common serious adverse events with CYRAMZA plus paclitaxel in study 2 were neutropenia (3.7%) and febrile neutropenia (2.4%); 19% of patients treated with CYRAMZA plus paclitaxel received granulocyte colony-stimulating factors.
• Adverse reactions resulting in discontinuation of any component of the CYRAMZA plus paclitaxel combination in 2% or more patients in study 2 were neutropenia (4%) and thrombocytopenia (3%).
• Clinically relevant adverse reactions reported in ≥1% and <5% of the CYRAMZA plus paclitaxel-treated patients in study 2 were sepsis (3.1% for CYRAMZA plus paclitaxel vs 1.8% for placebo plus paclitaxel) and gastrointestinal perforations (1.2% for CYRAMZA plus paclitaxel vs 0.3% for placebo plus paclitaxel).
Most Common Adverse Reactions—Combination With Docetaxel• The most commonly reported adverse reactions (all grades; grade 3/4) occurring in ≥5% of
patients receiving CYRAMZA plus docetaxel and ≥2% higher than placebo plus docetaxel in study 3 were neutropenia (55% vs 46%; 49% vs 40%), fatigue/asthenia (55% vs 50%; 14% vs 11%), stomatitis/mucosal inflammation (37% vs 19%; 7% vs 2%), epistaxis (19% vs 7%; <1% vs <1%), febrile neutropenia (16% vs 10%; 16% vs 10%), peripheral edema (16% vs 9%; 0% vs <1%), thrombocytopenia (13% vs 5%; 3% vs <1%), lacrimation increased (13% vs 5%; <1% vs 0%), and hypertension (11% vs 5%; 6% vs 2%).
• The most common serious adverse events with CYRAMZA plus docetaxel in study 3 were febrile neutropenia (14%), pneumonia (6%), and neutropenia (5%). The use of granulocyte colony-stimulating factors was 42% in CYRAMZA plus docetaxel-treated patients versus 37% in patients who received placebo plus docetaxel.
60
Please see Important Safety Information continued on pages 61-62 and full Prescribing Information for CYRAMZA, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing.

61
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
IMPORTANT SAFETY INFORMATION FOR CYRAMZA, CONTINUEDMost Common Adverse Reactions—Combination With Docetaxel, Continued• In patients ≥65 years of age, there were 18 (8%) deaths on treatment or within 30 days of
discontinuation for CYRAMZA plus docetaxel and 9 (4%) deaths for placebo plus docetaxel. In patients <65 years of age, there were 13 (3%) deaths on treatment or within 30 days of discontinuation for CYRAMZA plus docetaxel and 26 (6%) deaths for placebo plus docetaxel.
• Treatment discontinuation due to adverse reactions occurred more frequently in CYRAMZA plus docetaxel-treated patients (9%) than in placebo plus docetaxel-treated patients (5%). The most common adverse events leading to treatment discontinuation of CYRAMZA in study 3 were infusion-related reaction (0.5%) and epistaxis (0.3%).
• For patients with nonsquamous histology, the overall incidence of pulmonary hemorrhage was 7% and the incidence of grade ≥3 pulmonary hemorrhage was 1% for CYRAMZA plus docetaxel compared to 6% overall incidence and 1% for grade ≥3 pulmonary hemorrhage for placebo plus docetaxel. For patients with squamous histology, the overall incidence of pulmonary hemorrhage was 10% and the incidence of grade ≥3 pulmonary hemorrhage was 2% for CYRAMZA plus docetaxel compared to 12% overall incidence and 2% for grade ≥3 pulmonary hemorrhage for placebo plus docetaxel.
• Clinically relevant adverse reactions reported in ≥1% and <5% of CYRAMZA plus docetaxel-treated patients in study 3 were hyponatremia (4.8% CYRAMZA plus docetaxel versus 2.4% for placebo plus docetaxel) and proteinuria (3.3% CYRAMZA plus docetaxel versus 0.8% placebo plus docetaxel).
Most Common Adverse Reactions—Combination With FOLFIRI• The most commonly reported adverse reactions (all grades; grade 3/4) occurring in ≥5% of patients
receiving CYRAMZA plus FOLFIRI and ≥2% higher than placebo plus FOLFIRI in study 4 were diarrhea (60% vs 51%; 11% vs 10%), neutropenia (59% vs 46%; 38% vs 23%), decreased appetite (37% vs 27%; 2% vs 2%), epistaxis (33% vs 15%; 0% vs 0%), stomatitis (31% vs 21%; 4% vs 2%), thrombocytopenia (28% vs 14%; 3% vs <1%), hypertension (26% vs 9%; 11% vs 3%), peripheral edema (20% vs 9%; <1% vs 0%), proteinuria (17% vs 5%; 3% vs <1%), palmar-plantar erythrodysesthesia syndrome (13% vs 5%; 1% vs <1%), gastrointestinal hemorrhage events (12% vs 7%; 2% vs 1%), hypoalbuminemia (6% vs 2%; 1% vs 0%). Twenty percent of patients treated with CYRAMZA plus FOLFIRI received granulocyte colony-stimulating factors.
• The most common serious adverse events with CYRAMZA plus FOLFIRI were diarrhea (3.6%), intestinal obstruction (3.0%), and febrile neutropenia (2.8%).
• Treatment discontinuation of any study drug due to adverse reactions occurred more frequently in CYRAMZA plus FOLFIRI-treated patients (29%) than in placebo plus FOLFIRI-treated patients (13%). The most common adverse reactions leading to discontinuation of any component of CYRAMZA plus FOLFIRI as compared to placebo plus FOLFIRI were neutropenia (12.5% versus 5.3%) and thrombocytopenia (4.2% versus 0.8%). The most common adverse reactions leading to treatment discontinuation of CYRAMZA were proteinuria (1.5%) and gastrointestinal perforation (1.7%).
• Clinically relevant adverse reactions reported in ≥1% and <5% of CYRAMZA plus FOLFIRI-treated patients in study 4 consisted of gastrointestinal perforation (1.7% CYRAMZA plus FOLFIRI versus 0.6% for placebo plus FOLFIRI).
• Thyroid-stimulating hormone (TSH) was evaluated in 224 patients (115 CYRAMZA plus FOLFIRI-treated patients and 109 placebo plus FOLFIRI-treated patients) with normal baseline TSH levels. Patients received periodic TSH assessments until 30 days after the last dose of study treatment. Increased TSH was observed in 53 (46%) patients treated with CYRAMZA plus FOLFIRI compared with 4 (4%) patients treated with placebo plus FOLFIRI.
Please see Important Safety Information continued on page 62 and full Prescribing Information for CYRAMZA, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing.

62
mCRC
Important Safety Information
Lilly Resources
Dosing and Administration
CYRAMZA Overview
Advanced Gastric and
Gastroesophageal Junction
Adenocarcinoma
mNSCLC
Drug Interactions• No pharmacokinetic interactions were observed between ramucirumab and paclitaxel, between
ramucirumab and docetaxel, or between ramucirumab and irinotecan or its active metabolite, SN-38.
Use in Specific Populations• Pregnancy: Based on its mechanism of action, CYRAMZA can cause fetal harm. Animal models
link angiogenesis, VEGF, and VEGF Receptor 2 (VEGFR2) to critical aspects of female reproduction, embryofetal development, and postnatal development. There are no available data on CYRAMZA use in pregnant women to inform any drug-associated risks. No animal studies have been conducted to evaluate the effect of ramucirumab on reproduction and fetal development. Advise females of reproductive potential of the potential risk for maintaining pregnancy, risk to the fetus, and risk to newborn and pediatric development, and to use effective contraception during CYRAMZA therapy and for at least 3 months following the last dose of CYRAMZA.
• Lactation: Because of the potential risk for serious adverse reactions in nursing infants from ramucirumab, advise women that breastfeeding is not recommended during treatment with CYRAMZA.
• Females of Reproductive Potential: Advise females of reproductive potential that based on animal data CYRAMZA may impair fertility.
Please see full Prescribing Information for CYRAMZA, including Boxed Warnings for hemorrhage, gastrointestinal perforation, and impaired wound healing.
RB-P HCP ISI 17SEP2015
IMPORTANT SAFETY INFORMATION FOR CYRAMZA, CONTINUED

63
REFERENCES1. CYRAMZA (ramucirumab) [package insert]. Indianapolis, IN: Eli Lilly and Company; 2015. 2. Data on file, Eli Lilly and Company. ONC20141016a. 3. Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Gastric Cancer V.3.2016. © National Comprehensive Cancer Network, Inc 2016. All rights reserved. Accessed October 14, 2016. To view the most recent and complete version of the guidelines, go online to http://www.nccn.org. NATIONAL COMPREHENSIVE CANCER NETWORK®, NCCN®, NCCN GUIDELINES®, and all other NCCN content are trademarks owned by the National Comprehensive Cancer Network, Inc. 4. Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Esophageal and Esophagogastric Junction Cancers V.2.2016. © National Comprehensive Cancer Network, Inc 2016. All rights reserved. Accessed October 14, 2016. To view the most recent and complete version of the guidelines, go online to http://www.nccn.org. NATIONAL COMPREHENSIVE CANCER NETWORK®, NCCN®, NCCN GUIDELINES®, and all other NCCN content are trademarks owned by the National Comprehensive Cancer Network, Inc. 5. Data on file, Eli Lilly and Company. ONC20150415e. 6. Data on file, Eli Lilly and Company. ONC20150415g. 7. Data on file, Eli Lilly and Company. ONC20150415i. 8. Data on file, Eli Lilly and Company, ONC20150415a. 9. Data on file, Eli Lilly and Company, ONC20150415c. 10. Data on file, Eli Lilly and Company, ONC20150415b. 11. Fuchs CS, Tomasek J, Yong CJ, et al; REGARD Trial Investigators. Ramucirumab monotherapy for previously treated advanced gastric or gastro-oesophageal junction adenocarcinoma (REGARD): an international, randomised, multicentre, placebo-controlled, phase 3 trial. Lancet. 2014;383:31-39. 12. Supplement to: Fuchs CS, Tomasek J, Yong CJ, et al; REGARD Trial Investigators. Ramucirumab monotherapy for previously treated advanced gastric or gastro-oesophageal junction adenocarcinoma (REGARD): an international, randomised, multicentre, placebo-controlled, phase 3 trial. Lancet. 2014;383:31-39. 13. Wilke H, Muro K, Van Cutsem E, et al; for the RAINBOW Study Group. Ramucirumab plus paclitaxel versus placebo plus paclitaxel in patients with previously treated advanced gastric or gastro-oesophageal junction adenocarcinoma (RAINBOW): a double-blind, randomised phase 3 trial. Lancet Oncol. 2014;15(11):1224-1235. 14. Data on file, Eli Lilly and Company. ONC20150415f. 15. Data on file, Eli Lilly and Company. ONC20150415h. 16. Data on file, Eli Lilly and Company. ONC20150415j. 17. Data on file. Eli Lilly and Company. ONC20141014a. 18. Data on file, Eli Lilly and Company. ONC09302014b. 19. Data on file, Eli Lilly and Company. ONC09302014c. 20. Data on file, Eli Lilly and Company. ONC09302014d. 21. Supplement to: Wilke H, Muro K, Van Cutsem E, et al; for the RAINBOW Study Group. Ramucirumab plus paclitaxel versus placebo plus paclitaxel in patients with previously treated advanced gastric or gastro-oesophageal junction adenocarcinoma (RAINBOW): a double-blind, randomised phase 3 trial. Lancet Oncol. 2014;15(11):1224-1235. 22. Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Non-Small Cell Lung Cancer V.1.2017. © National Comprehensive Cancer Network, Inc 2016. All rights reserved. Accessed October 14, 2016. To view the most recent and complete version of the guidelines, go online to http://www.nccn.org. NATIONAL COMPREHENSIVE CANCER NETWORK®, NCCN®, NCCN GUIDELINES®, and all other NCCN content are trademarks owned by the National Comprehensive Cancer Network, Inc. 23. Garon EB, Ciuleanu T-E, Arrieta O, et al. Ramucirumab plus docetaxel versus placebo plus docetaxel for second-line treatment of stage IV non-small-cell lung cancer after disease progression on platinum-based therapy (REVEL): a multicentre, double-blind, randomised phase 3 trial. Lancet. 2014;384(9944):665-673. 24. Supplement to: Garon EB, Ciuleanu T-E, Arrieta O, et al. Ramucirumab plus docetaxel versus placebo plus docetaxel for second-line treatment of stage IV non-small-cell lung cancer after disease progression on platinum-based therapy (REVEL): a multicentre, double-blind, randomised phase 3 trial. Lancet. 2014;384(9944):665-673. 25. Data on file, Eli Lilly and Company. ONC20150415k. 26. Data on file, Eli Lilly and Company. ONC20150415l. 27. Data on file, Eli Lilly and Company. ONC20150415m. 28. Data on file. Eli Lilly and Company. ONC20141217a. 29. Data on file, Eli Lilly and Company. ONC20141217c. 30. Data on file. Eli Lilly and Company. ONC20150107a. 31. Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Colon Cancer V.2.2016. © National Comprehensive Cancer Network, Inc 2016. All rights reserved. Accessed October 14, 2016. To view the most recent and complete version of the guidelines, go online to http://www.nccn.org. NATIONAL COMPREHENSIVE CANCER NETWORK®, NCCN®, NCCN GUIDELINES®, and all other NCCN content are trademarks owned by the National Comprehensive Cancer Network, Inc. 32. Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Rectal Cancer V.2.2016. © National Comprehensive Cancer Network, Inc 2016. All rights reserved. Accessed October 14, 2016. To view the most recent and complete version of the guidelines, go online to http://www.nccn.org. NATIONAL COMPREHENSIVE CANCER NETWORK®, NCCN®, NCCN GUIDELINES®, and all other NCCN content are trademarks owned by the National Comprehensive Cancer Network, Inc. 33. Tabernero J, Yoshino T, Cohn AL, et al. Ramucirumab versus placebo in combination with second-line FOLFIRI in patients with metastatic colorectal carcinoma that progressed during or after first-line therapy with bevacizumab, oxaliplatin, and a fluoropyrimidine (RAISE): a randomised, double-blind, multicentre, phase 3 study. Lancet Oncol. 2015;16:499-508. 34. Data on file, Eli Lilly and Company. ONC20151015a. 35. Data on file, Eli Lilly and Company. ONC20151110a. 36. Data on file, Eli Lilly and Company. ONC20150418a. 37. Data on file, Eli Lilly and Company. ONC20150629a. 38. Data on file, Eli Lilly and Company. ONC20150624a. 39. Data on file, Eli Lilly and Company. ONC20150418b. 40. Data on file, Eli Lilly and Company. ONC20150419a. 41. National Institutes of Health. A Study in Second Line Colorectal Cancer. https://clinicaltrials.gov/ct2/show/NCT01183780?term=ramucirumab+folfiri&rank=2. Accessed October 14, 2016.
PP-RB-US-0671 11/2016 © Lilly USA, LLC 2016. All rights reserved.CYRAMZA® is a registered trademark owned by or licensed to Eli Lilly and Company, its subsidiaries. or affiliates.