procedure for record keeping for unplanned · pdf fileprocedure for record keeping for...
TRANSCRIPT
PROCEDURE FOR RECORD KEEPING FOR UNPLANNED CARE
First Issued
Issue Version
Purpose of Issue/Description of Change Planned Review Date
One
To promote safe and effective record keeping for all staff working in Unplanned care
2012
Named Responsible Officer:- Approved by:- Date
Nurse Consultant Unplanned Care
Clinical and Policy Procedure Group
September 2010
Unplanned Care Clinical Procedure/
Information Governance IG05
(formerly CP31)
Impact Assessment Screening Complete
Date: 07/09/2010
Full Impact Assessment Required No
UNLESS THIS VERSION HAS BEEN TAKEN DIRECTLY FROM THE TRUST WEB SITE THERE IS NO ASSURANCE THIS IS THE CORRECT VERSION
IG05 Procedure for Record Keeping – Unplanned Care
Page 1 of 12
CONTENTS PAGE
CONTENTS
PAGE
Introduction
2
Policy Aim
2
Target Group
2
Responsibilities of the staff
2
Document Control
2
Record Keeping Training
2
Examples of relevant documentation
3
Related Policies and Guidelines
3
Caldicott Principles
3
Consent Guidelines
3
Best Interest
4
Confidentiality
5
Patient Access and Request for Records
5
Copying letters to patients
5
Safe Storage of Records
6
Long Term Storage of Records
6
Supervision of Record Keeping Standards
6
A-Z of Additional Information
7-9
References and Acknowledgements
9
Appendix 1
Core documentation – Paper Records Template W alk In Centre
10
IG05 Procedure for Record Keeping – Unplanned Care
Page 2 of 12
PROCEDURE FOR RECORD KEEPING FOR UNPLANNED CARE INTRODUCTION Wirral Community NHS Trust is committed to high standards of record keeping, to ensure safe, effective high quality nursing care for its service users. The Nursing and Midwifery Council (2007) states that:
“Record keeping is an integral part of nursing, midwifery and specialist public health nursing; it is a tool of professional practice and one that should help the care process. It is not separate from this process and it is not an optional extra to be fitted in if circumstances allow.”
A IM
• To outline the policies and procedures of record keeping for all staff working in
Unplanned care.
• To provide specific guidance relating to Unplanned Care, this builds on existing
Trust Health Records Policy and the Trust‟s Code of Conduct for handling personal and identifiable information.
• To provide existing and new staff with detailed information regarding record keeping
standards relevant to Unplanned care. TARGET GROUP
All staff working in Unplanned Care including bank staff, students on placement and Medical Practitioners will comply with this procedure. Record keeping standards will be audited yearly.
RESPONSIBILITIES OF STAFF
All individuals who work for Unplanned Care are responsible for any records which they create or use in the performance of their duties.
As an employee, any records you create are public records and the principles of record keeping apply to all documentation. A full copy of the Trust‟s Health Records Policy and the Trust‟s Code of Conduct for Handling Personal Information are both available on the Trust‟s intranet site.
DO C U ME NT C O NT R O L Team leaders/ Lead Nurses are responsible for ensuring their teams are using the most current versions of paper based documentation and referral forms. It is imperative that old versions of forms referring to previous names of organisations are destroyed.
RECORD KEEPING TRAINING
Every new member of staff will attend an induction programme and be provided with an overview of W irral Community NHS Trust Policies.
All new starters must attend Essential Learning which includes record keeping training within four weeks of commencing employment with the organisation. All Unplanned Care Clinical staff must attend Essential Learning every two years.
IG05 Procedure for Record Keeping – Unplanned Care
Page 3 of 12
EXAMPLES OF RELEVANT DOCUMENTATION
These may consist of:
Patient Health Records (electronic or paper based, including specialties and GP
medical records)
Administrative records (e.g. personnel, estates, financial and
accounting records; notes associated with complaint-
handling)
Scanned records
Computerised records
Diaries
Telephone message records
Referral forms
Faxes
Clinic attendance sheets
Accident / incident forms
Communication books
Audio / video tapes
Wound maps / photographs
Memos
Prescription sheets
E-mails
Photographs, slides, and other images
X-ray and imaging reports, output and images
Audio and video tapes, cassettes, CD-ROM etc
Wirral Remote Ordering and Communication System (W
ROCS)
Text messages (outgoing from Wirral Community NHS Trust
and incoming responses from the patient)
Blood Glucose Monitoring Meter Documentation
RELATED POLICIES Please refer to related Trust policies and procedures CALDICOTT PRINCIPLES– refer to the Trust‟s Code of Conduct for issues relating to safeguarding personal and identifiable information.
All NHS organisations have a designated Caldicott Guardian to oversee access to patient information. The Trust‟s Caldicott Guardian is Lisa Cooper. [email protected]
CONSENT – see the Trust‟s consent policy for full details
Department of Health consent principles are fully outlined in Trust Consent Policy. All registered nurses must promote a care environment that promotes informed and valid consent, privacy and dignity and actively involve the patient in their care planning.
„Valid Consent‟ is a patient's agreement for a health professional to provide care. To demonstrate capacity individuals should be able to;-
1. understand information about the decision to be made 2. retain that information in their mind 3. use or weigh that information as part of the decision making process 4. Communicate their decision
IG05 Procedure for Record Keeping – Unplanned Care
Page 4 of 12
For consent to be valid, the patient must be able to:-
• Make a free choice
• Free from pressure
• Given voluntarily
Evidence of valid consent must always be documented within the patient‟s records and should be noted each time care is provided. However, for ongoing, routine interventions e.g. administration of daily insulin, valid consent should be obtained and documented in the care plan prior to the initial intervention and care plan reviewed at least 6 monthly or if the patient‟s circumstances or treatment changes. Valid consent should be reviewed at least monthly as a minimum and when care plans are updated.
Reference guide to consent for examination or treatment provides a comprehensive summary of the current law on consent and 12 key points on consent. This document summarises aspects of the law on consent, which arise on a daily basis. To download a copy, access:- http://www.dh.gov.uk/en/AdvanceSearchResult/index.htm?searchTerms=consent
PATIENTS WITHOUT CAPACITY TO CONSENT It should be noted that if an adult does not have the capacity to provide valid consent (either temporarily or permanently) then no other person can consent on their behalf – this includes the patient‟s General Practitioner (GP). Please refer to the Trust‟s Mental Capacity Act Toolkit for further information http://nww.wirral.nhs.uk/about_services/services_that_the_pct_provides/community_nursin g/MCA/
BEST INTERESTS – CONSENT FORM FOUR Health care can be given in the patients best interests. To establish best interests it is essential that the views of all persons involved in that patient‟s care are sought, this would include carers and relatives, GP and other relevant professionals or agencies.
It may be necessary to seek advice from your Service Manager on a case by case basis or the Safeguarding Team.
In some cases the Service Manager may need to consult with Trust solicitors for specific legal advice.
WRITTEN CONSENT FORMS Photographic and video recordings made for clinical purposes form part of a patient‟s health record and Consent form 5 must be signed. It is rarely a legal requirement to obtain written consent, however it is essential if a procedure has significant risks which the patient needs to be aware of e.g. types of surgery. Please refer to Trust Consent Policy for further information.
INFORMATION GOVERNANCE – refer to Trust Health Records Policy
IG05 Procedure for Record Keeping – Unplanned Care
Page 5 of 12
CO-ORDINATING CARE WITH SOCIAL SERVICES AND OTHER AGENCIES
There are times when it is appropriate to pass on information regarding patients to someone else (see Trust Health Records Policy). Information must be able to pass between the NHS, local authority Social Services and other services contributing to a planned programme of care. If patients decline to give permission to share information, and this has an impact on the ability of staff to provide safe packages of care, contact your Service Manager for advice on a case by case basis. Adapted from ‘Confidentiality: NHS Code of Practice’ (Department of Health 2003) (Available from www.dh.gov.uk)
CONFIDENTIALITY
In general, any personal information given or received in confidence for one purpose may not be used for a different purpose or passed on to anyone else without the consent of the provider of that information. This duty of confidence is long established in common law. However, in the NHS or related services this principle cannot be applied so rigidly that it would constitute a risk of disadvantaging the patient or would be detrimental to the public in general. A number of inquiry reports have shown that the flow of accurate information on a 'need to know' basis, in sensitive areas such as mental health and childcare, can be justified for the benefit and safety of all concerned.
Who has a duty of confidence?
• All NHS bodies
• All NHS employees
• Health professionals - who also have an ethical duty of confidence through their
respective professional bodies • Other individuals and agencies to whom information is passed legitimately
PATIENT INFORMATION
In this procedure the term 'patient information' applies to all personal identifiable information regarding members of the public held in whatever form by, or for, NHS bodies or staff. Information about patients and clients must be treated as confidential and only be used for the relevant purposes for which it was given.
As it is impracticable to obtain consent every time information is shared, it is essential that patients understand that some information may be made available to other members of the team involved in the delivery of their care. These discussions should be an integral part of the care planning process.
The public expects the NHS to respond effectively to its needs. Therefore, an essential feature of the relationship between patients and the NHS is the need for patients / clients to be fully informed what their personal information may be used for.
PATIENT ACCESS AND REQUEST FOR RECORDS
Refer to Trust Health Records Policy
COPYING LETTERS TO PATIENTS
From 1 April 2004, patients have an automatic right to receive copies of letters written about their care. See Trust: Copying Letters to Patients Policy, for specific guidance.
IG05 Procedure for Record Keeping – Unplanned Care
Page 6 of 12
SAFE STORAGE OF RECORDS
Staff must take all reasonable efforts to safeguard confidential client records and personal identifiable information, including the following measures:
• Patient identifiable information, including patient records, patient prescriptions,
electronic sources of information and diaries should not be left unattended.
• Each member of staff must use their own personal log in and password to access the electronic record system.
• Staff should ensure that personal login details are not shared with other members of
staff or members of the public. • All staff must ensure security of patients‟ records by logging off the electronic record
system on every occasion when leaving the computer unattended.
• Patient identifiable information should not be left anywhere where it could be viewed
by a member of the public. • Records must be stored in a secure room and filed appropriately when not in use.
• Personal identifiable information should not be visible to the general public in
reception areas. • No Information Technology equipment can be used to store patient information
unless it has been supplied and approved for safety by W irral Health Information Systems (W HIS) and your Service Manager.
All employees with access to personal identifiable information have a duty to safeguard that information under the confidentiality code of conduct. Administration of patient related information must only be delegated to another team member if they are aware of their responsibilities under this code.
LONG-TERM STORAGE OF RECORDS
Records selected for archival preservation and no longer in regular use should be transferred as soon as possible to a locally agreed archival institution that has adequate storage and public access facilities.
SUPERVISION OF RECORD KEEPING STANDARDS It is the responsibility of every registered nurse who delegates care to non registered staff, to have a system in place to supervise the standards of record keeping within the team. Evidence that this has occurred must be documented e.g. following one to one meetings, peer review, management supervision or Personal Developmental Reviews.
It is mandatory for all Clinical Nursing staff to attend Information Governance and Professional Record Keeping training every two years as part of the Essential Learning Programme.
The Trust can provide support through training, policies and professional guidance from Nurse Management / Service Improvement Unit in relation to record keeping. It is no defence, if held accountable, to your professional body or internal inquiry to say you are unaware of record keeping guidelines and legislation.
IG05 Procedure for Record Keeping – Unplanned Care
Page 7 of 12
A-Z OF ADDITIONAL INFORMATION
Bank nurse work sheets Any work delegated to bank nurses must be documented on the designated bank nurse work sheet. They should complete the comments section for each patient if appropriate and „sign off duty‟ in the space provided. These sheets should then be stored alphabetically at base in line with the Trust Retention and Disposal Schedule.
Blood Glucose Monitoring Meter Documentation Ensure that each book has the serial number of the meter written inside the quality control book. The books need to be stored at base. Under the Consumer Protection Act, these records must be kept for 11 years.
Communication Books
Must be stored at base in a secure room and kept for a period of three years. After this time they must be shredded as they may contain patient identifiable information. Each member of the team, including bank staff and relief team staff must understand the importance of using this form of communication and where it is kept.
Patient Medicines Administration Chart (PMAC)
Patient Medicines Administration Charts are to be completed by the prescriber for all medications to be administered by an authorised healthcare professional. PMAC‟s are valid for 6 months and require updating after that date. A new PMAC is required for each new episode of care. PMAC‟s for controlled drugs have a shorter expiry date, and should be updated every 28 days. Ref: Standard Operating Procedure for Medicine Administration in Community Nursing. Trust Safe Handling and Administration of Medicines Policy (2008)
Immunisations – comply with the relevant Patient Group Directive A record of administration must be communicated to the patients General Practitioner, either by electronic data transfer methods or fax in order to prevent the vaccine being given twice or not at all.
Inter-Agency Referrals
Details of any referral made, including telephone referrals, must be documented in the electronic or paper health records. Telephone referrals should be followed up by completing the appropriate inter-agency referral form.
Non-Medical Prescribing - Record Keeping Refer to the Non-Medical Prescribing Procedure
Record of Patient Care in Clinics / All Day Health Centre
Assessment and treatment records for care provided in All Day Health Centre or clinics are to be recorded onto the relevant computer system or paper records and communicated to the patient‟s own General Practitioners surgery within 24 hours of attendance. Recording health care on a computer should adopt the same standards of practice as hand written records. Therefore, any entry needs to be clearly identifiable and evidence patient consent.
IG05 Procedure for Record Keeping – Unplanned Care
Page 8 of 12
Locking of patient records should only be applied in cases of emergency when the consulting nurse is called away to deal with an emergency, in which case electronic records must be completed as soon as the nurse has returned to the computer base.
Record of Patient Care in Primary Care Assessment Unit
Assessment and treatment records for care provided in Primary Care Assessment Unit are filed into the patients hospital case notes which should be returned to medical records department after patient‟s discharge. Discharge summary letters should be sent to patients GP within 24 hours of discharge.
Telephone Calls
All patient related telephone contact, including health advice, must be evidenced in the patient‟s record. Messages should be documented in a carbonated message book and the top copy of the message filed in the patient‟s health records. Any health related advice or patient related discussion should be documented in the health records / base notes on the communication sheet. The patient-held record should also be updated if any aspect of care is affected as the result of a telephone conversation. Message books need to be kept for three years and then shredded or disposed of in confidential waste bag. If the message was taken by another member of the team, this needs to be signed and dated by the healthcare professional as evidence that the message has been received and reviewed before it is filed.
Work Diaries
Diaries should be stored at your base when completed at the end of the year and kept for a period of two years. After this period the diaries should be shredded or placed in a confidential waste bag as they contain patient identifiable information. Entries must be recorded in black ink.
Do not record any patient clinical information in your diary as it forms part of a patient’s record
Ear Care Documentation The ear care assessment documentation must be completed and filed in the base notes. This is available on the intranet.
Wound Mapping – reassess every 4 weeks as a minimum This must be recorded on the patients‟ electronic records.
Wounds should be measured in order to provide a baseline measurement from which to evaluate wound-healing progress.
GENERAL PRINCIPLES
• Adhere to Trust Health Records Policy.
• Each record must be clearly labelled with the patient‟s full name, date of birth and
National Health Service (NHS) Number.
• Every entry in the patient‟s paper record must have the date (day, month, year) and time (24 hour clock) of the intervention recorded;( this is automatically stored in electronic records)
IG05 Procedure for Record Keeping – Unplanned Care
Page 9 of 12
• All staff involved in the patient/clients care must print, sign their name and record their
designation on every entry made in paper records (this is automatically stored in electronic records)
• If the date and time of an event / intervention differs from when the paper records are
written up, this must be clearly noted in the records. • Any reports / results / letters or other incoming documentation relating to patient care,
must be signed by the reviewing practitioner and their designation, the dated and time recorded before filing.
N.B. All verbal communication relating to a patient‟s care following referral or discharge
must be documented in the patients electronic / paper records.
References
DH (2003) „Confidentiality: NHS Code of Practice‟ www.doh.gov.uk/ipu/confiden
DH (2004) Choosing health – Making Healthy Choices Easier Data Protection Act 1998
Nursing and Midwifery Council (2007): Guidelines for Record Keeping
DOH (1997) 'Report on the Review of Patient-Identifiable Information‟
NHS Modernisation Agency (2003) Essence of Care - Patient Focused Benchmarks for Clinical Governance
Mental Capacity Act Tool Kit (2007)
Trust Records Policy (2009)
Trust Retention and Disposal Schedule Trust Safe Handling and Administration of Medicines Policy (2008)
Acknowledgments
Record Keeping Training Groups
IG05 Procedure for Record Keeping – Unplanned Care
Page 10 of 12
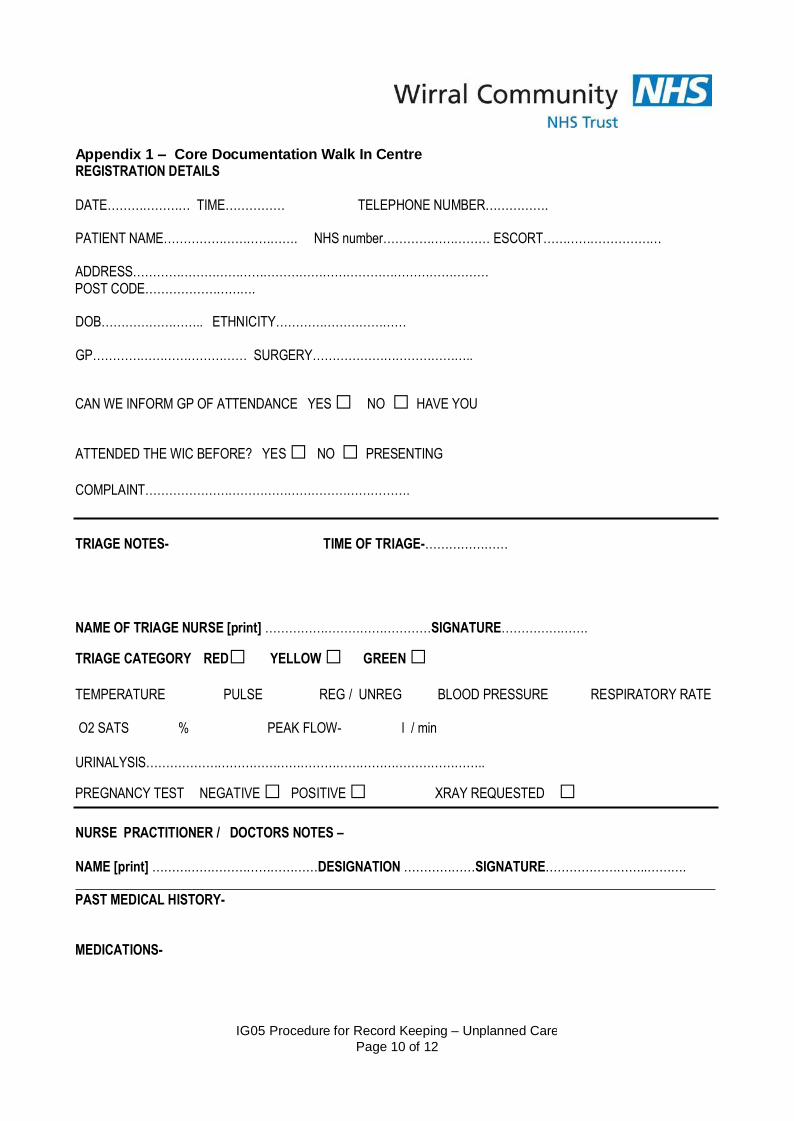
Appendix 1 – Core Documentation Walk In Centre REGISTRATION DETAILS
DATE………………… TIME…………… TELEPHONE NUMBER…………….
PATIENT NAME……………………………. NHS number……………………… ESCORT…………………………
ADDRESS……………………………………………………………………………… POST CODE……………………….
DOB…………………….. ETHNICITY……………………………
GP………………………………… SURGERY…………………………………..
CAN WE INFORM GP OF ATTENDANCE YES □ NO □ HAVE YOU
ATTENDED THE WIC BEFORE? YES □ NO □ PRESENTING
COMPLAINT………………………………………………………….
TRIAGE NOTES- TIME OF TRIAGE-…………………
NAME OF TRIAGE NURSE [print] ……………………………………SIGNATURE………………….
TRIAGE CATEGORY RED□ YELLOW □ GREEN □
TEMPERATURE PULSE REG / UNREG BLOOD PRESSURE RESPIRATORY RATE
O2 SATS % PEAK FLOW- l / min
URINALYSIS…………………………………………………………………………..
PREGNANCY TEST NEGATIVE □ POSITIVE □ XRAY REQUESTED □
NURSE PRACTITIONER / DOCTORS NOTES –
NAME [print] ……………………………………DESIGNATION ………………SIGNATURE……………………..……….
PAST MEDICAL HISTORY-
MEDICATIONS-

IG05 Procedure for Record Keeping – Unplanned Care
Page 11 of 12
ALLERGIES-
IMMUNISATION HISTORY-
IG05 Procedure for Record Keeping – Unplanned Care
Page 12 of 12
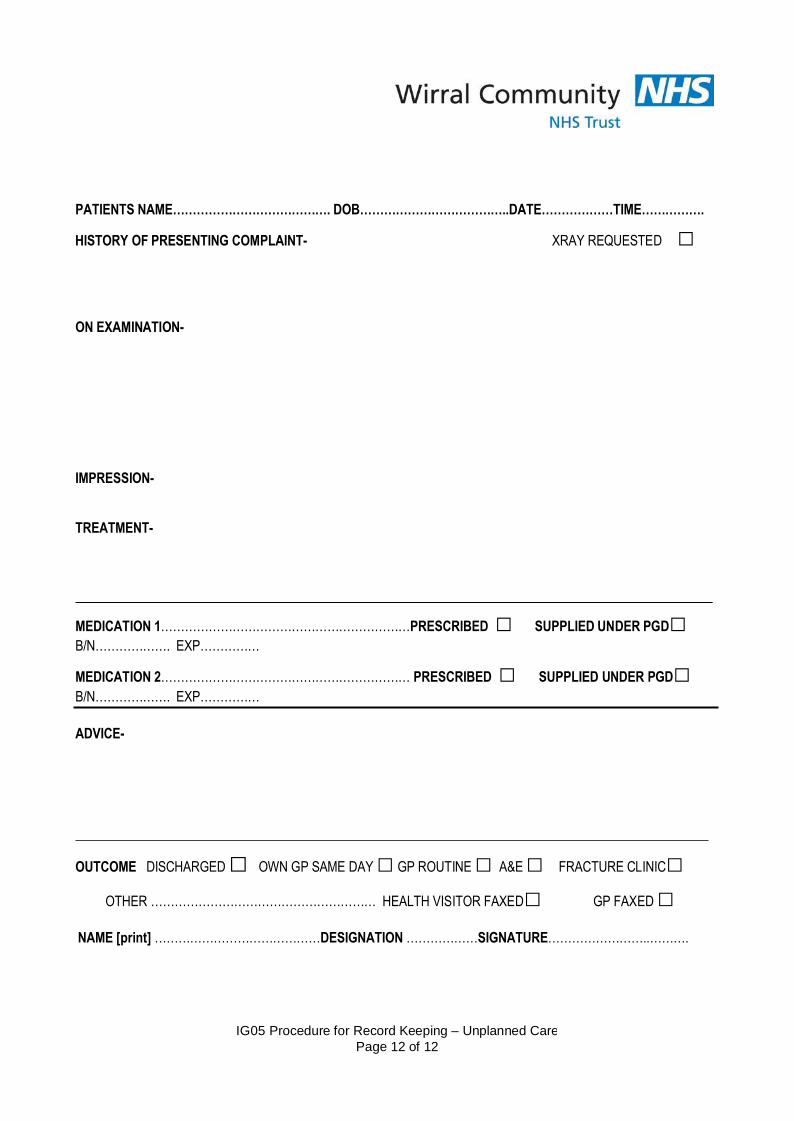
PATIENTS NAME…………………………………. DOB………………………………..DATE………………TIME…………….
HISTORY OF PRESENTING COMPLAINT- XRAY REQUESTED □
ON EXAMINATION-
IMPRESSION-
TREATMENT-
MEDICATION 1………………………………………………………PRESCRIBED □ SUPPLIED UNDER PGD□ B/N………………. EXP……………
MEDICATION 2……………………………………………………… PRESCRIBED □ SUPPLIED UNDER PGD□ B/N………………. EXP……………
ADVICE-
OUTCOME DISCHARGED □ OWN GP SAME DAY □ GP ROUTINE □ A&E □ FRACTURE CLINIC□
OTHER ………………………………………………… HEALTH VISITOR FAXED□ GP FAXED □
NAME [print] ……………………………………DESIGNATION ………………SIGNATURE……………………..……….

IG05 Procedure for Record Keeping – Unplanned Care
Page 13 of 12
[CONTINUATION SHEET]
PATIENTS NAME…………………………………. DOB………………………………..DATE………………TIME…………….
DATE OF CONSULTATION-…………………… TIME OF CONSULTATION-……………
NAME [print] ……………………………………DESIGNATION ………………SIGNATURE……………………..……….

Procedure for Record Keeping – Unplanned Care
Page 14 of 12