prison drug store. mohsen saadat, d.o., f.a.c.p medical director san joaquin county, correctional...
TRANSCRIPT

Prison Drug Store
Mohsen Saadat, D.O., F.A.C.PMedical Director
San Joaquin County, Correctional Health Care Facility

Financial Disclosures
• None

Three Focus areas
1. Epidemic of Drug Abuse
2. Medication Abuse by Inmates, Psychotropic
Medications
3. Essential Pearls in dealing with Jail Medicine

Michael Boticelli, Deputy Director of the White House Office of National Drug Control Policy, announced that the abuse of prescribed drugs has been classified as an epidemic by the Centers for Disease Control.
Prescription Drug Abuse: Insight Into the Epidemic
• Joseph Rannazzisi, from the Drug Enforcement Agency provided the following information:
• Deaths in 2010 caused by accidental overdose of prescription opiates exceeded the combined rate from all other drug deaths, including heroin and cocaine combined.
• Deaths from accidental drug overdoses exceeded all other causes of accidental deaths, including vehicle accidents.
Prescription Drug Abuse: Insight Into the Epidemic

Prescription Drug Abuse: Insight Into the Epidemic

Prescription Drug Abuse: Insight Into the Epidemic
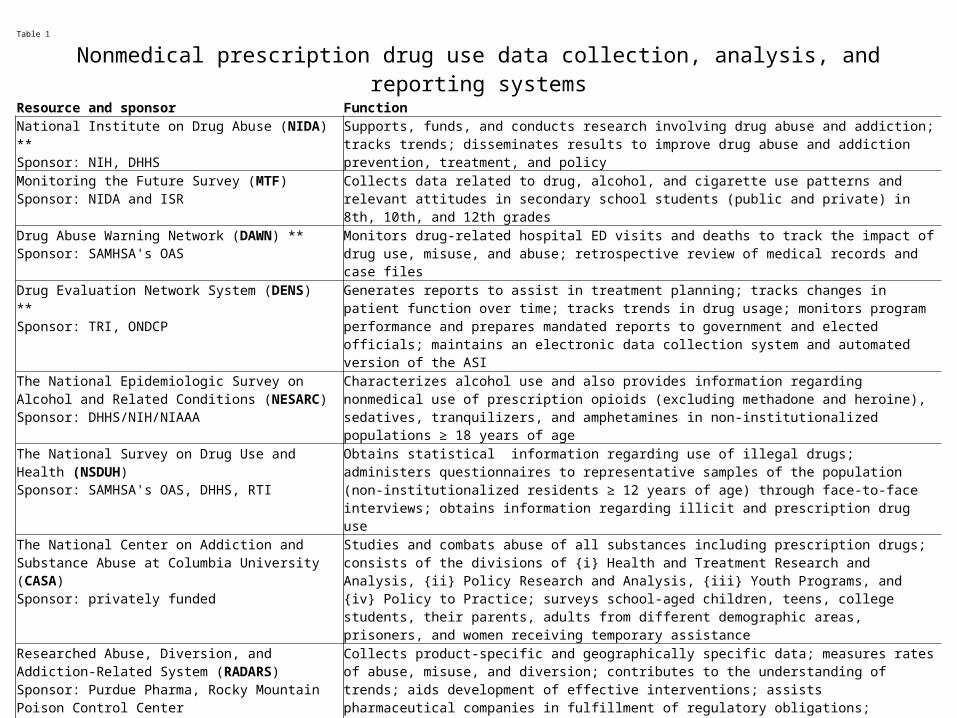
Table 1
Nonmedical prescription drug use data collection, analysis, and reporting systemsResource and sponsor FunctionNational Institute on Drug Abuse (NIDA) **Sponsor: NIH, DHHS
Supports, funds, and conducts research involving drug abuse and addiction; tracks trends; disseminates results to improve drug abuse and addiction prevention, treatment, and policy
Monitoring the Future Survey (MTF)Sponsor: NIDA and ISR
Collects data related to drug, alcohol, and cigarette use patterns and relevant attitudes in secondary school students (public and private) in 8th, 10th, and 12th grades
Drug Abuse Warning Network (DAWN) **Sponsor: SAMHSA's OAS
Monitors drug-related hospital ED visits and deaths to track the impact of drug use, misuse, and abuse; retrospective review of medical records and case files
Drug Evaluation Network System (DENS) **Sponsor: TRI, ONDCP Generates reports to assist in treatment planning; tracks changes in patient function over time; tracks trends in
drug usage; monitors program performance and prepares mandated reports to government and elected officials; maintains an electronic data collection system and automated version of the ASI
The National Epidemiologic Survey on Alcohol and Related Conditions (NESARC)Sponsor: DHHS/NIH/NIAAA
Characterizes alcohol use and also provides information regarding nonmedical use of prescription opioids (excluding methadone and heroine), sedatives, tranquilizers, and amphetamines in non-institutionalized populations ≥ 18 years of age
The National Survey on Drug Use and Health (NSDUH)Sponsor: SAMHSA's OAS, DHHS, RTI Obtains statistical information regarding use of illegal drugs; administers questionnaires to representative
samples of the population (non-institutionalized residents ≥ 12 years of age) through face-to-face interviews; obtains information regarding illicit and prescription drug use
The National Center on Addiction and Substance Abuse at Columbia University (CASA)Sponsor: privately funded
Studies and combats abuse of all substances including prescription drugs; consists of the divisions of {i} Health and Treatment Research and Analysis, {ii} Policy Research and Analysis, {iii} Youth Programs, and {iv} Policy to Practice; surveys school-aged children, teens, college students, their parents, adults from different demographic areas, prisoners, and women receiving temporary assistance
Researched Abuse, Diversion, and Addiction-Related System (RADARS)Sponsor: Purdue Pharma, Rocky Mountain Poison Control Center
Collects product-specific and geographically specific data; measures rates of abuse, misuse, and diversion; contributes to the understanding of trends; aids development of effective interventions; assists pharmaceutical companies in fulfillment of regulatory obligations; prescription drug abuse, misuse, and diversion surveillance system
The Arrestee Drug Abuse Monitoring Program (ADAM)Sponsor: NIJ Collects data related to recently booked arrestees (within 48 h) regarding drug use, drug and alcohol
dependence, treatment, and drug market participation; data help policymakers and practitioners make decisions concerning problems of drugs and crime
The National Poison Data System (NPDS)Sponsor:AAPCC
Real-time comprehensive poisoning surveillance/toxicovigilancew database; a uniform data set from the AAPCC
Office of the Medical Investigator (OMI) **Sponsor: city, county, and state Investigates deaths that come under the jurisdiction of the OMI; includes poisoning and drug-related deaths
AAPCC, American Association of Poison Control Centers; ASI, addiction severity index: DHHS, US Department of Health and Human Services; ED, emergency department; ISR, University of Michigan Institute for Social Research; NIAAA, National Institute on Alcohol Abuse and Alcoholism; NIH, National Institutes of Health; NU, National Institute of Justice; OAS, Office of Applied Studies; ONDCP, White House Office of National Drug Control Policy; RTI, Research Triangle Institute; SAMHSA, Substance Abuse and Mental Health Services Administration; TRI, Treatment Research Institute.
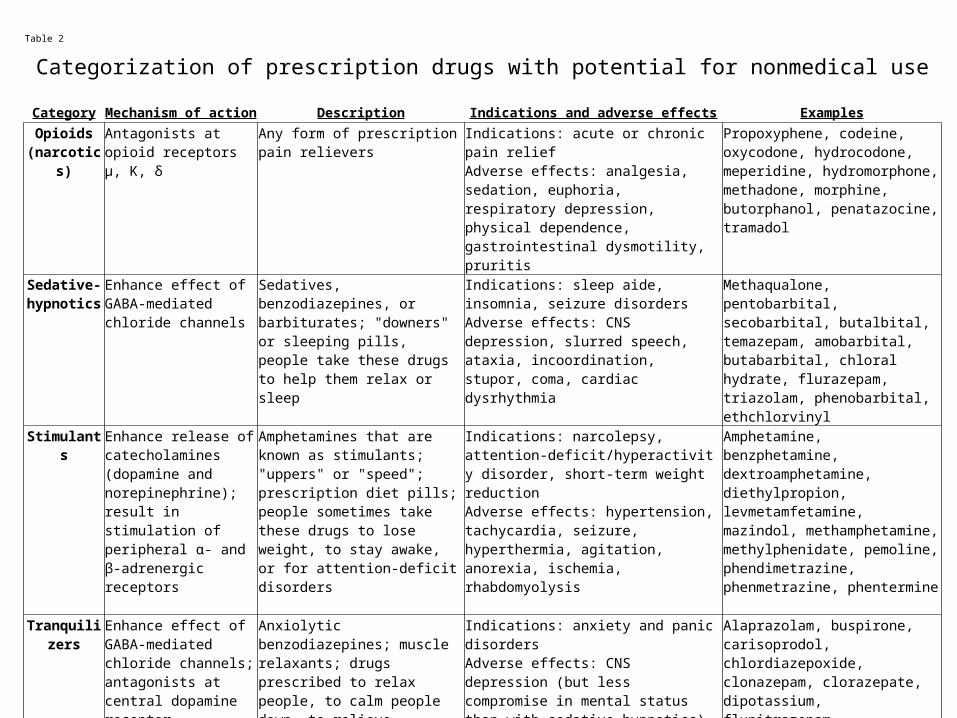
Table 2
Categorization of prescription drugs with potential for nonmedical use
Category Mechanism of action Description Indications and adverse effects ExamplesOpioids
(narcotics)Antagonists at opioid receptors µ, K, δ
Any form of prescription pain relievers
Indications: acute or chronic pain reliefAdverse effects: analgesia, sedation, euphoria, respiratory depression, physical dependence, gastrointestinal dysmotility, pruritis
Propoxyphene, codeine, oxycodone, hydrocodone, meperidine, hydromorphone, methadone, morphine, butorphanol, penatazocine, tramadol
Sedative-hypnotics
Enhance effect of GABA-mediated chloride channels
Sedatives, benzodiazepines, or barbiturates; "downers" or sleeping pills, people take these drugs to help them relax or sleep
Indications: sleep aide, insomnia, seizure disordersAdverse effects: CNS depression, slurred speech, ataxia, incoordination, stupor, coma, cardiac dysrhythmia
Methaqualone, pentobarbital, secobarbital, butalbital, temazepam, amobarbital, butabarbital, chloral hydrate, flurazepam, triazolam, phenobarbital, ethchlorvinyl
Stimulants Enhance release of catecholamines (dopamine and norepinephrine); result in stimulation of peripheral α- and β-adrenergic receptors
Amphetamines that are known as stimulants; "uppers" or "speed"; prescription diet pills; people sometimes take these drugs to lose weight, to stay awake, or for attention-deficit disorders
Indications: narcolepsy, attention-deficit/hyperactivity disorder, short-term weight reductionAdverse effects: hypertension, tachycardia, seizure, hyperthermia, agitation, anorexia, ischemia, rhabdomyolysis
Amphetamine, benzphetamine, dextroamphetamine, diethylpropion, levmetamfetamine, mazindol, methamphetamine, methylphenidate, pemoline, phendimetrazine, phenmetrazine, phentermine
Tranquilizers Enhance effect of GABA-mediated chloride channels; antagonists at central dopamine receptor
Anxiolytic benzodiazepines; muscle relaxants; drugs prescribed to relax people, to calm people down, to relieve anxiety, or to relax muscle spasms
Indications: anxiety and panic disordersAdverse effects: CNS depression (but less compromise in mental status than with sedative-hypnotics), slurred speech, ataxia, incoordination, stupor, coma, cardiac dysrhythmia
Alaprazolam, buspirone, carisoprodol, chlordiazepoxide, clonazepam, clorazepate, dipotassium, flunitrazepam, hydroxyzine, lorazepam, meprobamate, oxazepam

Table 3
Terminology used to describe nonmedical prescription drug use
Resource Terminology and definition
Monitoring the Future Survey (MTF) Misuse: "on your own, that is, without a doctor telling you to take them"
Drug Abuse Warning Network (DAWN) Abuse or misuse: meets criteria for case types classified as overmedication, malicious poisoning, and other
The National Epidemiologic Survey on Alcohol and Related Conditions (NESARC)
Nonmedical use: "without a prescription, in greater amounts, more often, longer than prescribed or for a reason other than a doctor said you should use them"
The National Survey on Drug Use and Health (NSDUH) Abuse: "without a prescription of the individual's own or simply for the experience or feeling the drugs caused"
The National Center on Addiction & Substance Abuse at Columbia University (CASA)
Abuse: "was not prescribed for you or was taken only for the experience or feeling it caused"
Researched Abuse, Diversion, and Addiction-Related System (RADARS)
Abuse: {i} use to get high or {ii} use in combination with other drugs to get high, or {iii} use as a substitute for other drugs of abuse
The National Poison Data System (NPDS) Abuse: "intentional improper or incorrect use of a substance, likely attempting to gain a high, euphoric effect, or some other psychotropic effect"
Office of Chief Medical Examiner (OCME) Death from abuse: "accidental"; death was not the intended outcome of the behavior: "unnatural"; death from complications of chronic abuse: "natural"

• United States has 4.6 percent of the world’s population, but consumes 80 percent of the world’s opiates and 99 percent of the entire world production of hydrocodone.
• For every death by opiate, there are 130 individuals abusing the drug chronically.
• Pain in the rest of the world is managed with far fewer opiates than in U.S. Alternatives include NSAIDs, acetaminophen, physical therapy, herbal remedies and supportive care.
Prescription Drug Abuse: Insight Into the Epidemic
Correlating the General Population Data with the subset of the Population
Residing in the State Hospitals and Prisons

Medication Abuse by Inmates

Medication Abuse by Inmates

Medication Abuse by Inmates

From Deinstitutionalization to Trans-institutionalization

Psychotropic Medication Abuse in Correctional Facilities
• 20% of the 2.1 million Americans in county jails and state prisons are seriously mentally ill.
• Only 80,000 in mental hospitals.
• 72% of inmates with mental illness have substance abuse/dependence.
Psychotropic Medications: Abuse by Inmates

Concerns in Treating the Incarcerated Psychiatric Patient
1) Compromised Care for Those Who Need It
2) The Malingering Patient
3) Inmates Creativity factors

Care Compromise
• These individuals may be bullied, abused, have their medications taken from them by other inmates.
• Paradoxically, there are prisoners who would benefit from psychiatric agents but fear treatment will make them vulnerable to other inmates. “ You can’t make me a zombie.”

The Malingering Patient
• Those desperate to escape the larger prison community out of fear: “Just to get some sleep”, “Just to get away from the noise”, “I want a little peace”, “ A little Privacy”.
• Those who want to trick the system into providing psychotropic drugs.

The Creativity Factor
• Sliding the white pill into the empty socket of a missing tooth.
• Using denture adhesive on the roof of the mouth to hide the pills.
• For crushed meds and powders, pretend to swallow but would leave the powder on the back of the tongue. Then scrape the powder off the tongue and mix it with saliva to make a paste, then dry the paste and sell it to the other inmates.
Lessons to be learned
• Apart from the initial “Ewww”, it shows how desperate some inmates are for the drugs and how far they go to get anything that alter consciousness.
• Also, the effort we put into preventing checking is not always successful, inmates are just too creative.
• Control is an important motivating factor for the inmates to give them a sense of independence and respect by other inmates.

Bridging Medications
• A lesser known phenomenon to use other prescription medications to minimize physiological withdrawal until individuals can obtain their next “chemical high” with their drug of choice.

Inappropriate Drugs in Jails and Prisons
A List of Pearls
The definition of a ‘pearl” is a bit of pithy and insightful information that can be communicated in a few sentences.

A List of Pearls• Seroquel; “Quell”, “susie Q”, “or “Baby Heroin”, “Q-
ball” - when combination with cocaine. Crushed and snorted, injected, or inserted rectally. Hypnotic effects and Amnesia.
• Risperdal; “ Orange Monster” 2-3 pills for sleep.
• Zyprexa; used orally or intravenously, causing a “buzz”.
• Gabapentin; “Nana”, if a meth addict can produce a high, if heroin addict can produce drowsiness, hallucination. Snorted with Wellbutrin to decrease the nasal irritation.

A List of Pearls
• Artane; “ A’s”, take (3) 5 mg pills with a cup of coffee, or directly snort, effects similar to meth.
• Wellbutrin; “ Welbys”, mix in coffee provides a high similar to meth. Can be snorted or injected. 3-4 pills are crushed and placed in a spoon with a drop of water, mix well and let the water evaporate.

A List of Pearls
• Benadryl; 5-6 of 50 mg does can cause high similar to speed in some individuals.
• Albuterol; can be used in rapid succession to promote one hour high. Can express into a plastic bag and huffed, 2-3 hour high. Can keep cap on and deployed until canister empty, then scrape residue off cap and sniff, ingest, or shoot.

A List of Pearls
• Nasal Decongestants; 20-40 drops heat in a spoon and inhale the vapor. Effects appear in a few seconds and last for 2-4 hours. Feeling of “stimulation”, “excitation”, “strength”.
• Dextromethorphan, common in OTC cough suppressant, used at much higher doses for its dissociative effects. “ robo-tripping” or “Triple Cs”.
A List of Pearls
• Bupropion SR; reported as being crushed and snorted, most often as an adjuvant to gabapentin.
• TCAs; multiple reports of hoarding and used to commit suicide.
• Tramadol; synthetic codeine with weak mu receptor activity as an anxiolytic. Lowers threshold for seizure.
A List of Pearls
• Pruno; Jail house wine, fruits such as oranges, soup noodles or potato flakes and 3-4 packages of sugar. Let ferment for 7-10 days. Many different recipes.
• Wheat bread mashed with orange peels, place in a warm place for the mold to grow. Extract brown mold and inhale, causes hallucinations similar to LSD.
• Metamucil; reports of it being dissolved after given to an inmate and solidified into a shank.

National Strategy of Quality Improvement in Health Care (National Quality Strategy) “Three Part Aim”
Better Health for the population
Better Care for
Individuals
Lower Cost Through
Improvement The Medicare Quality Improvement of California


Medical Board Recommendations
• Document appropriate H&P.
• Establish a Diagnosis and an objective measure of pain.
• Obtain an opiate contract.
• Perform periodic review of patient condition and effectiveness of therapy.

Medical Board Recommendations
• Obtain further consultation from other specialties if pain is difficult to control.
• Maintain accurate records.
• Perform periodic review of the records.
• Provide adequate and appropriate documentation of the NP/PA supervision.

Three Reasonable Criteria
• The risk of abuse the medication has in this correctional setting.
• The potential benefit the medication offers.
• Whether a less problematic substitute is available for this setting.
