principles of hormone testing
TRANSCRIPT

Principles of Hormone Testing
All I really needed to know I learned
in LU 3 Physiology :)
Iris Thiele Isip Tan MD, MSc Professor, UP College of Medicine Chief, UP Medical Informatics Unit
Baby steps by Kristina Alexanderson, https://flic.kr/p/att5j5

Pathologic Mechanisms of Endocrine Disease
By Herbert L. Fred, MD & Hendrik A. van Dijk, http://commons.wikimedia.org/wiki/File%3AMyxedema_face.png
By Jonathan Trobe, M.D. http://commons.wikimedia.org/wiki/File%3AProptosis_and_lid_retraction_from_Graves'_Disease.jpg
Hormone Excess
DeficiencyResistance

Spring 2012 hackNY student hackathon presentations by hackNY,org https://flic.kr/p/bv1dUj
I don’t want to lecture!

Explain the principle illustrated
Ask a question (that hopefully
you can answer)
Remind you of something you (should
have) learned in LU 3
Don’t forget by juliaf, http://www.freeimages.com/photo/729159
Question mark by 7rains, http://www.freeimages.com/photo/1323680
Black and white by plusverde, http://www.freeimages.com/photo/516694

http://blp6.atw.hu/BLP6/HTML/C0409780323045827.htm

A woman in her 8th week of gestation has palpitations. Her doctor ordered TSH and T4. T4 180 (NV 58-161 nmol)TSH 0.2 (NV 0.5-4.7 mIU/L)
Which of the following is true? A. The woman is hyperthyroid.B. Her thyroid function tests need to be
repeated.C. Both A & B are true.D. Neither A nor B are true.
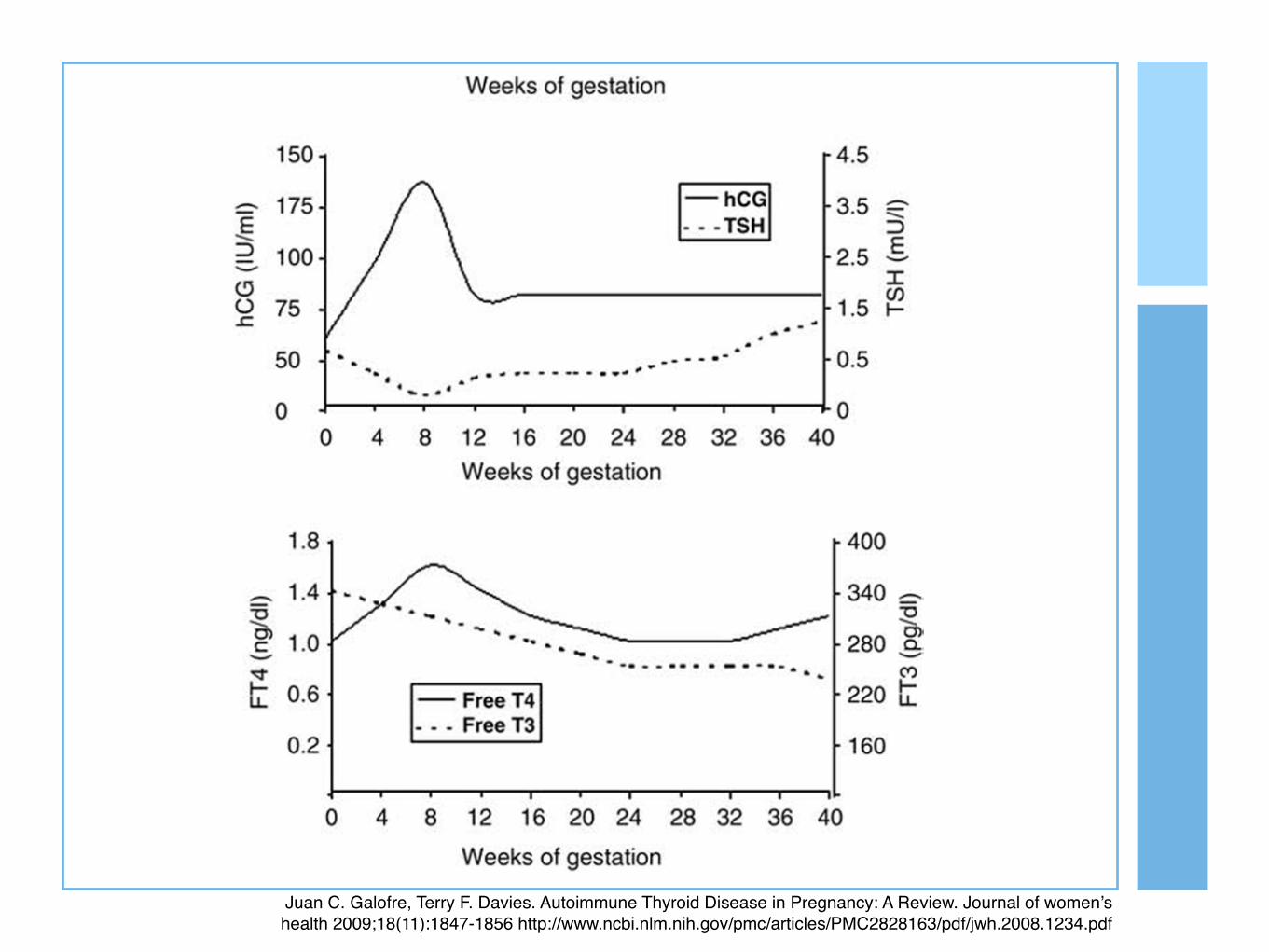
Juan C. Galofre, Terry F. Davies. Autoimmune Thyroid Disease in Pregnancy: A Review. Journal of women’s health 2009;18(11):1847-1856 http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2828163/pdf/jwh.2008.1234.pdf

Test results must be interpreted in conjunction with a clear understanding of
the pathophysiology and natural history of suspected disorders.
“Fowler MJ, Pannone AF, Blevins Jr. South Med J 2002;95(5)
1
Laboratory tests only represent a snapshot of endocrine function at the time that the
blood sample was obtained.

A woman in her 8th week of gestation has palpitations. Her doctor ordered TSH and T4. You decide to order FT4 and FT3. Which of the following is true?
A. The FT4 will be normal if euthyroid.
B. In pregnancy, the FT4 and T4 will be the same.

Juan C. Galofre, Terry F. Davies. Autoimmune Thyroid Disease in Pregnancy: A Review. Journal of women’s health 2009;18(11):1847-1856 http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2828163/pdf/jwh.2008.1234.pdf

Remember that many hormones circulate in association
with serum-binding proteins.
2
The normal range for most hormone is relatively broad, varying by a factor of two to tenfold.
The correct normative database is an essential part of interpreting hormone tests.

Harrison’s Principles of Internal Medicine

An obese woman is sent to you for work-up of Cushing’s syndrome. Her doctor already did an 8 am cortisol. Serum cortisol 25 (NV 4.3-22.4 ug/dL)
Which of the following is true? A. An 8 am cortisol is the appropriate test. B. As the 8 am cortisol is elevated, no further tests
are needed.C. Neither A nor B is true.D. Both A and B are true.

http://www.endocrinesurgeon.co.uk/index.php/how-is-cushings-syndrome-diagnosed

Recognition of hormonal rhythms is important for endocrine testing.
3

An obese woman is sent to you for work-up of Cushing’s syndrome. You decide to do a 1-mg dexamethasone suppression test.
A. If the patient has Cushing’s, the 8 am cortisol will not be suppressed.B. If the patient has Cushing’s, the 8 am cortisol will be suppressed.
Harrison’s Principles of Internal Medicine

http://www.endocrinesurgeon.co.uk/index.php/how-is-cushings-syndrome-diagnosed

Diagnostic tests take advantage of negative feedback loops.
4
It is not uncommon for baseline hormone levels associated with pathologic endocrine conditions to
overlap with the normal hormone range.DYNAMIC testing is useful.
An obese woman is sent to you for work-up of Cushing’s syndrome. The patient is afraid of needles. She asks if a urine test can be done. What are the advantages of urine vs serum?
Which of the following is true? A. A urine collection will integrate multiple pulsatile
spikes of hormone secretion.B. A blood sample has both the advantage and
limitation of time dependency.C. Both A and B are true.D. Both A and B are false.

Harrison’s Principles of Internal Medicine

There are advantages and limitations in doing urine and blood
measurements of hormones.
5

An obese woman is sent to you for work-up of Cushing’s syndrome. She had read on the internet that she could have a pituitary tumor and would like to have an MRI done immediately.Serum cortisol 25 (NV 4.3-22.4 ug/dL)
What will you do? A. You tell her that further hormonal tests are
needed.B. You agree and order the MRI.

Harrison’s Principles of Internal Medicine

Harrison’s Principles of Internal Medicine

Biochemical confirmation of endocrine disease precedes imaging.
6


A 45/M with nephrolithiasis is referred to you by a urologist for consideration of hyperparathyroidism. Serum calcium 3.5 (NV 2.12-2.57 mmol/L)
What will you do? A. You will order intact PTH assay.B. You will order a paired serum Ca and iPTH assay.


A 25/F is referred for persistent hypokalemia and hypertension. Renin 1.22 ng/mL/h (NV 0.15-3.96 ng/ml/h)Aldosterone 100 ng/dL (NV 1-16 ng/dL)ARR 83 (NV <20)
Which of the following is true? A. She likely has primary hyperaldosteronism.B. Her lab results are consistent with renal artery
stenosis.

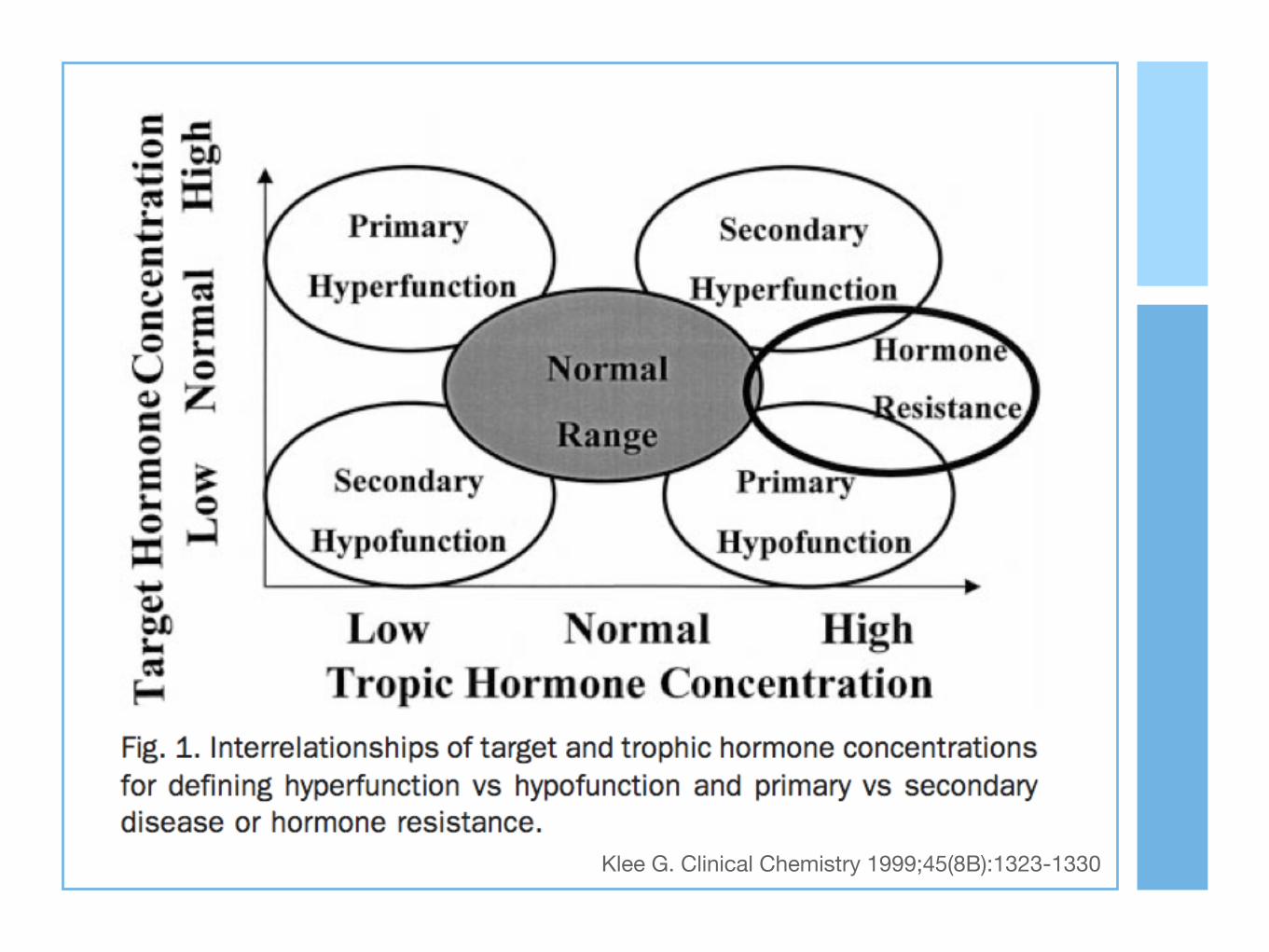
Klee G. Clinical Chemistry 1999;45(8B):1323-1330

Simultaneous measurement of trophic and target hormones may help to determine the
location of the abnormality.
7
“Klee G. Clinical Chemistry 1999;45(8B):1323-1330

http://www.slideshare.net/VNyuntWai/blood-pressure-regulation-2013

A 38/F is referred for an adrenal incidentaloma. She is taking Metoprolol 50 mg od for palpitations. You plan to rule out pheochromocytoma.
What will you do? A. Discontinue and wash out metoprolol before
proceeding with tests.B. Request a 24-h urine collection for
metanephrine.

Always ask what drugs can interfere with the results of hormone tests.
8
How should the patient prepare for the hormone tests?
One swallow does not a summer make, but one tophus makes gout and one crescent, malaria.
Sir William Osler
“

A 26/M seafarer is referred for pre-employment clearance. On examination, you do not find any signs of hyperthyroidism.T3 ECLIA 3.2 (NV 0.9-2.8 nmol/L)T4 ECLIA 180 (NV 58-161 nmol/L)TSH ECLIA 2.0 (NV 0.3-5.0 U/mL)
What will you do? A. Start Methimazole 5 mg bid.B. Request a repeat TSH IRMA

A 35/F is referred by an ophthalmologist. She has been amenorrheic for one year. Perimetry showed bitemporal hemianopsia. The MRI showed a 1.5 x 2.2 cm sellar-suprasellar mass.Prolactin 25 (NV 2.8-29.2 ng/mL)
What will you do? A. Refer to a neurosurgeon; this is a non-
functioning pituitary adenoma.B. Request a repeat prolactin assay with dilution.
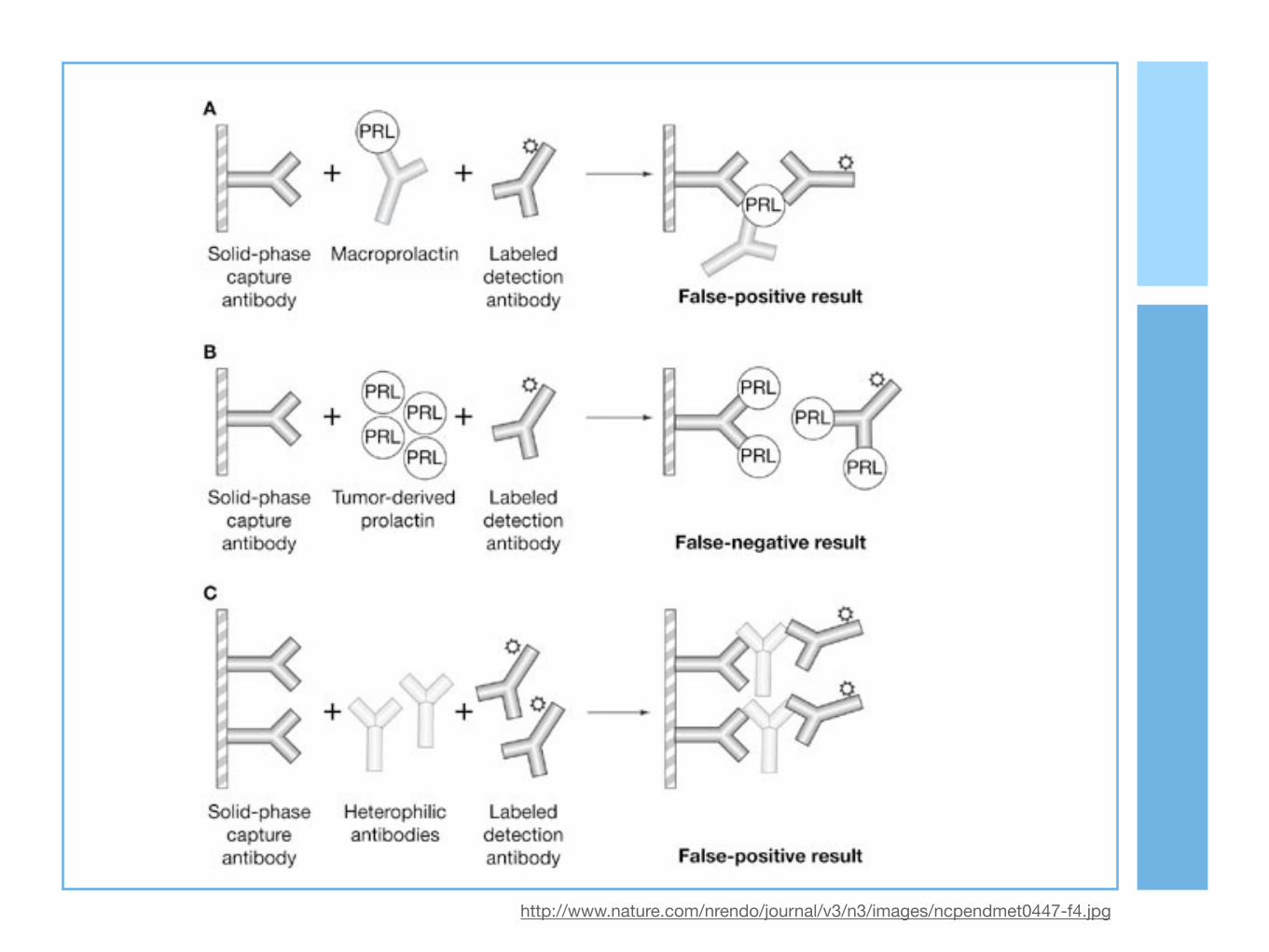
http://www.nature.com/nrendo/journal/v3/n3/images/ncpendmet0447-f4.jpg

Test abnormalities do not always reflect endocrine dysfunction.
9
Some tests may be normal in the setting of real endocrine
dysfunction.

http://labtestsonline.org/understanding/features/reliability/start/1

http://www.med.uottawa.ca/sim/data/Images/Sen_spec.gif

You are working up a 40/F for Cushing’s syndrome. Urine free cortisol 450 (NV 55-248 nmol/day)
Repeat Urine free cortisol 200 (NV 55-248 nmol/day)
What will you do? A. Repeat urine free cortisol a third time.B. Request for a cranial MRI.

Harrison’s Principles of Internal Medicine

Keep in mind the four indicators of reliability of laboratory testing:
accuracy, precision, sensitivity, specificity
1 0

Questions to Ask What are the key clinical issues?What sequence of tests would be optimal?What drugs should be discontinued before testing?What stabilizing, provocative or inhibitory procedures should the patient undergo before the specimen collection?
Klee G. Clinical Chemistry 1999;45(8B):1323-1330

Efficacy of endocrine tests depends on
Choice of testsPreparation of the patientsIntegrity of the specimensQuality of the measurementsValidity of reference data
Klee G. Clinical Chemistry 1999;45(8B):1323-1330

Principles of Hormone Testing
All I really needed to know I learned
in LU 3 Physiology :)
Iris Thiele Isip Tan MD, MSc Professor, UP College of Medicine Chief, UP Medical Informatics Unit
Baby steps by Kristina Alexanderson, https://flic.kr/p/att5j5