principles and practice of cancer...
TRANSCRIPT
PRINCIPLES AND PRACTICE OF
CANCER REHABILITATION
Michael D Stubblefield, MD Director of Cancer Rehabilitation Kessler Institute for Rehabilitation Professor, Physical Medicine and Rehabilitation Rutgers New Jersey Medical School American Board of Physical Medicine & Rehabilitation American Board of Electrodiagnostic Medicine American Board of Internal Medicine

2
Disclosures: None
3
Cancer Rehabilitation Job Description
A specialist in the identification, evaluation, and rehabilitation of neuromuscular, musculoskeletal, pain, and functional disorders associated with cancer and it’s treatment emphasizing the restoration and maintenance of function and quality of life.
4
Cancer Rehabilitation Contemporary Perspective: United States
• 14 million cancer survivors in 20141
• 18.1 million cancer survivors by 20202
• 273,000 spinal cord injury survivors in 20133
• Approximately 68% of persons diagnosed with cancer today can expect to live at least 5 years after diagnosis compared with only 49% in the 1970’s and 35% in the 1950’s.4
1American Cancer Society. Cancer Facts & Figures 2014. Atlanta, GA: American Cancer Society; 2014. 2Mariotto AB, Yabroff KR, Shao Y, Feuer EJ, Brown ML. Projections of the cost of cancer care in the United States: 2010-2020. J Natl Cancer Inst 2011;103(2):117-128. 3 J Spinal Cord Med. 2013 Jan;36(1):1-2 4Ries LAG, Melbert D, Krapcho M, Stinchcomb DG, Howlader N, Horner MJ, Mariotto A, Miller BA, Feuer EJ, Altekruse SF, Lewis DR, Clegg L, Eisner MP, Reichman M, Edwards BK (eds). SEER Cancer Statistics Review, 1975-2005, National Cancer Institute. Bethesda, MD, http://seer.cancer.gov/csr/1975_2005/, based on November 2007 SEER data submission, posted to the SEER web site, 2008.
5
Cancer Statistics
Survivors
New Cancers
Cancer Deaths
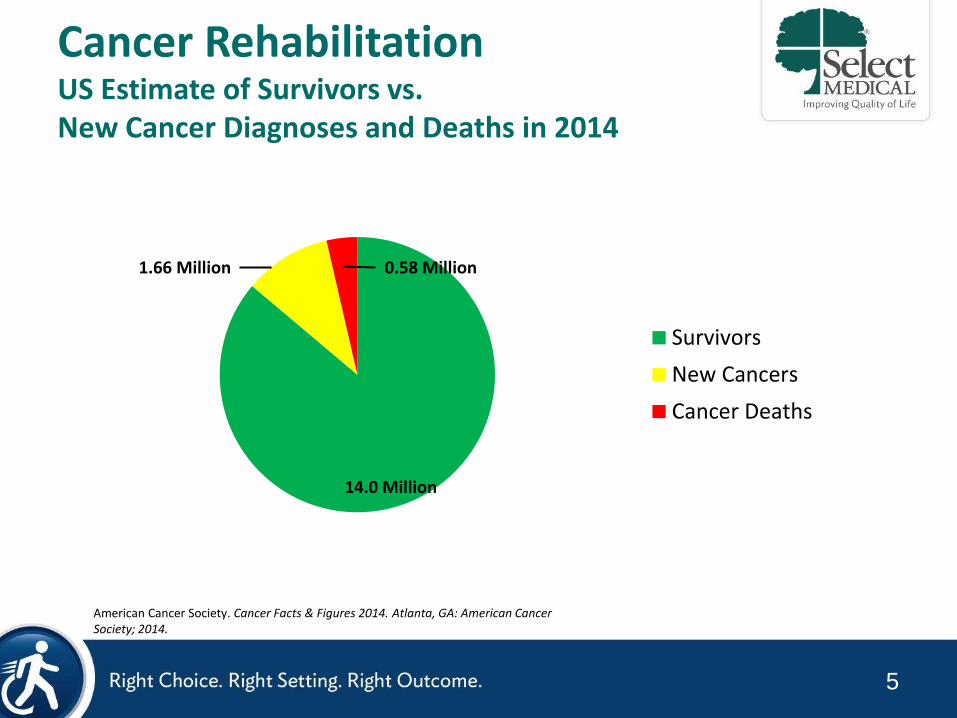
Cancer Rehabilitation US Estimate of Survivors vs. New Cancer Diagnoses and Deaths in 2014
0.58 Million 1.66 Million
14.0 Million
American Cancer Society. Cancer Facts & Figures 2014. Atlanta, GA: American Cancer Society; 2014.
6
Practice of Cancer Rehabilitation
7
• Cancer
• Cancer treatment – Surgery
– Chemotherapy
– Radiation Therapy
• Pre-existing disorders
• The interrelationship between all of the above
Cancer Rehabilitation Success Requires and Understanding of:
8
Cancer Rehabilitation “The Dirty Little Secret”
The principles and practice of cancer rehabilitation are generally similar to those of general rehabilitation…
9
• Neuromuscular – Cerebropathy
– Myelopathy
– Radiculopathy
– Plexopathy
– Neuropathy • Polyneuropathy
• Mononeuropathy
• Mononeuropathy Multiplex
• Ganglionopathy
• Small Fiber
– Myopathy
– Disorders of Neuromuscular Transmission
• Musculoskeletal – Rotator Cuff Tendonitis – Adhesive Capsulitis – Epicondylitis – De Quervain's Tenosynovitis – Neuroforaminal/Central Stenosis – Spinal Instability – Fracture/Impending Fracture – Arthritis – Enthesopathy – Osteoporosis – GVHD – Scoliosis – Bony Metastases
Cancer Rehabilitation Neuromuscular, Musculoskeletal, and Pain Disorders Commonly Seen in Cancer Survivors
10
Cancer Rehabilitation Functional Disorders Commonly Seen in Cancer Survivors
• Lymphedema
• Fatigue
• Myalgia
• Fibromyalgia
• Autonomic dysfunction
• Cardiac dysfunction
• Pulmonary dysfunction
• Endocrine dysfunction
• Gastrointestinal dysfunction
• Genitourinary dysfunction
• Cognitive dysfunction
• Psychiatric dysfunction
• Psychosocial dysfunction
11
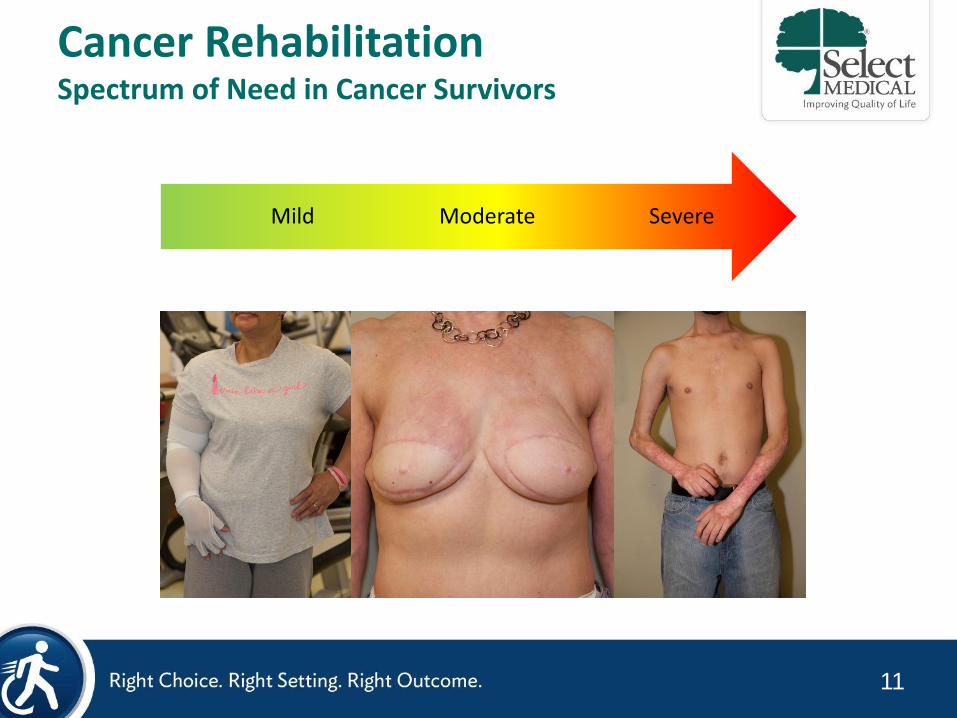
Cancer Rehabilitation Spectrum of Need in Cancer Survivors
Severe Moderate Mild

12
Impending Fracture
13
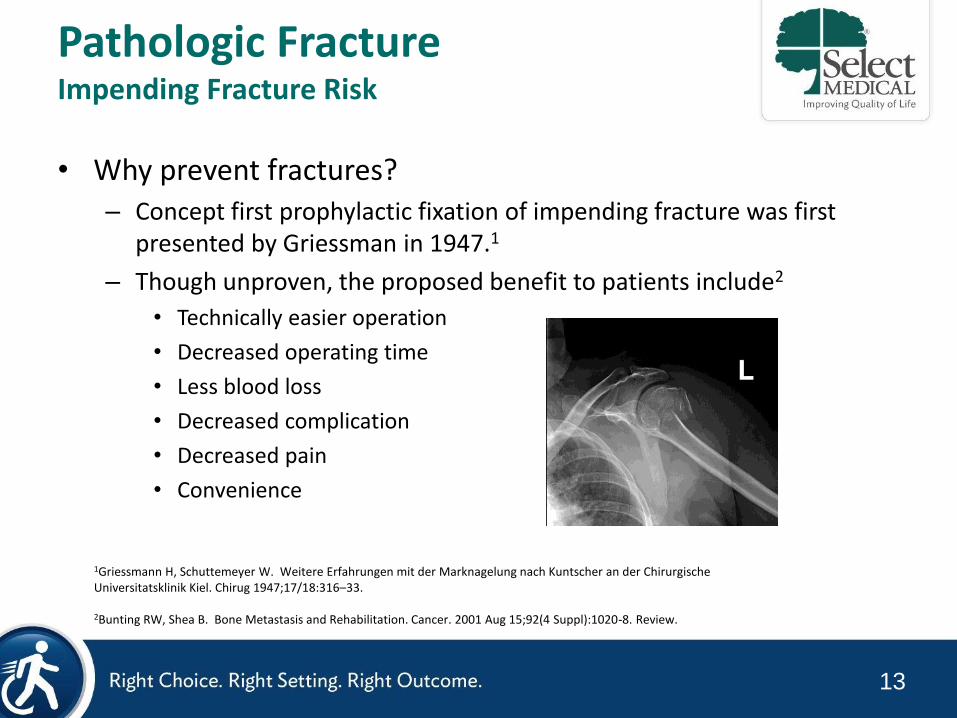
Pathologic Fracture Impending Fracture Risk
• Why prevent fractures? – Concept first prophylactic fixation of impending fracture was first
presented by Griessman in 1947.1
– Though unproven, the proposed benefit to patients include2
• Technically easier operation
• Decreased operating time
• Less blood loss
• Decreased complication
• Decreased pain
• Convenience
1Griessmann H, Schuttemeyer W. Weitere Erfahrungen mit der Marknagelung nach Kuntscher an der Chirurgische Universitatsklinik Kiel. Chirug 1947;17/18:316–33. 2Bunting RW, Shea B. Bone Metastasis and Rehabilitation. Cancer. 2001 Aug 15;92(4 Suppl):1020-8. Review.
14
Pathologic Fracture Impending Fracture Risk
• Osteolytic – Characterized by lysis or bone
destruction
– Secretion of proteases directly stimulate bone resorption or the release of osteoclast-stimulating factors
• Osteoblastic – Characterized by new bone
growth
– Appear dense on X-ray and CT
– Bone produced is not good quality
– Thought to be less prone to fracture
• A combination of osteolytic and osteoblastic lesions can occur in the same patient
15
Pathologic Fracture Impending Fracture Risk
• Radiographic Detection of Bone Tumors – X-Ray
– Bone Scan
– CT
– PET - CT
– MRI
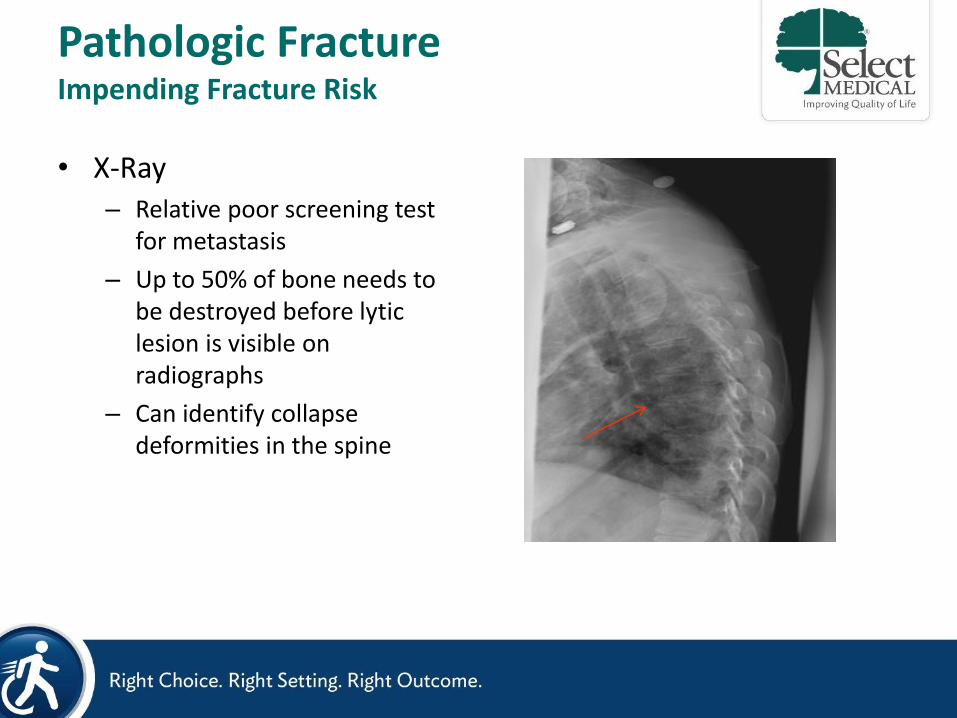
• X-Ray – Relative poor screening test
for metastasis
– Up to 50% of bone needs to be destroyed before lytic lesion is visible on radiographs
– Can identify collapse deformities in the spine
Pathologic Fracture Impending Fracture Risk
17
Pathologic Fracture Impending Fracture Risk
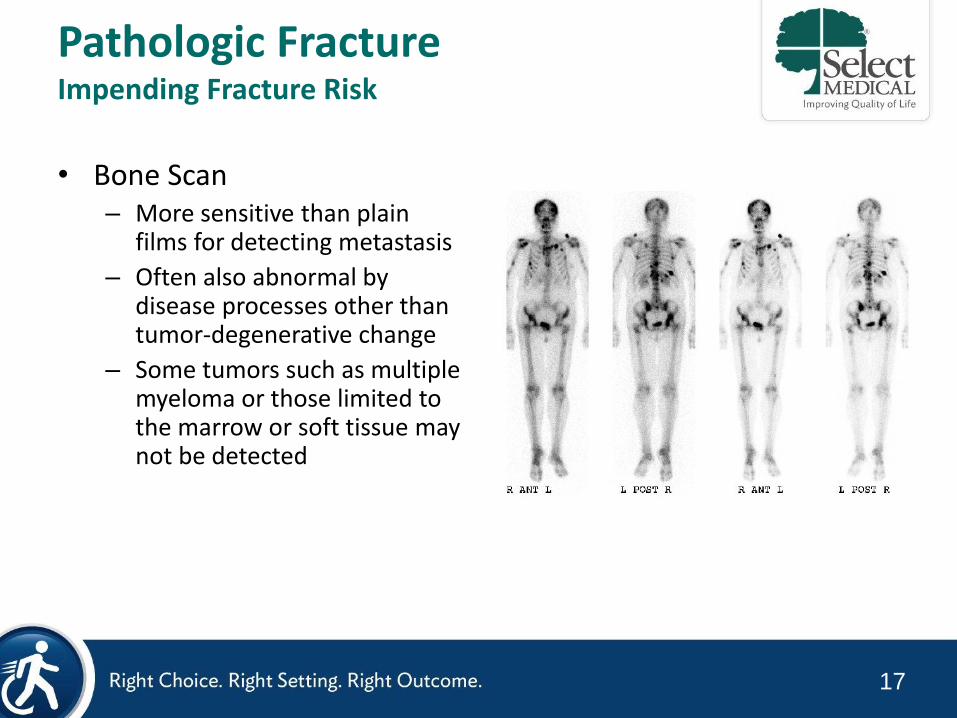
• Bone Scan – More sensitive than plain
films for detecting metastasis
– Often also abnormal by disease processes other than tumor-degenerative change
– Some tumors such as multiple myeloma or those limited to the marrow or soft tissue may not be detected
18
Pathologic Fracture Impending Fracture Risk
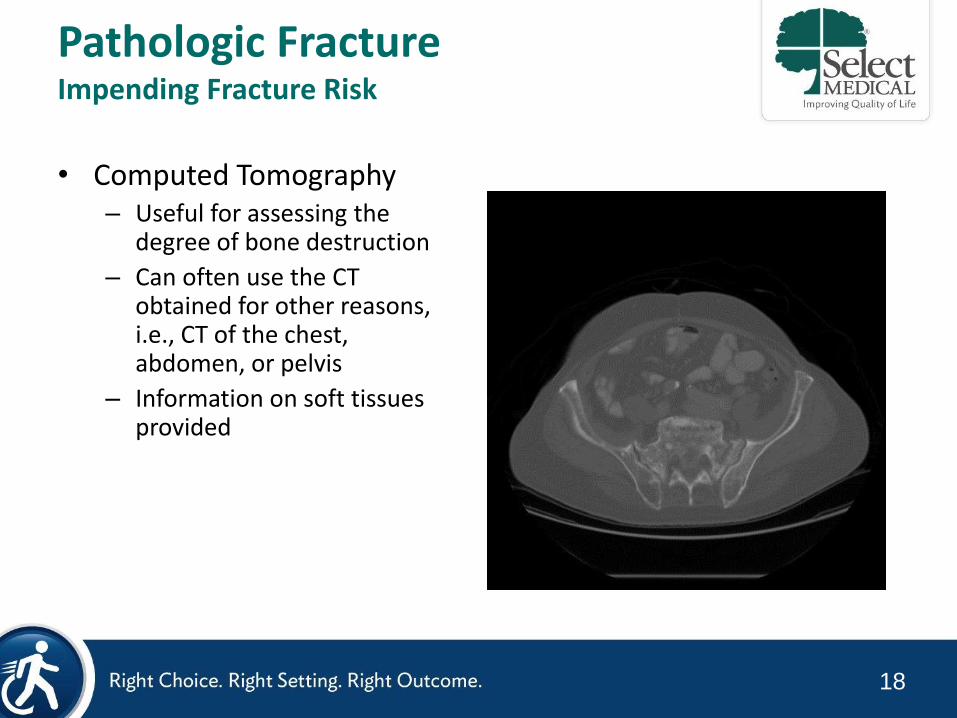
• Computed Tomography – Useful for assessing the
degree of bone destruction
– Can often use the CT obtained for other reasons, i.e., CT of the chest, abdomen, or pelvis
– Information on soft tissues provided
19
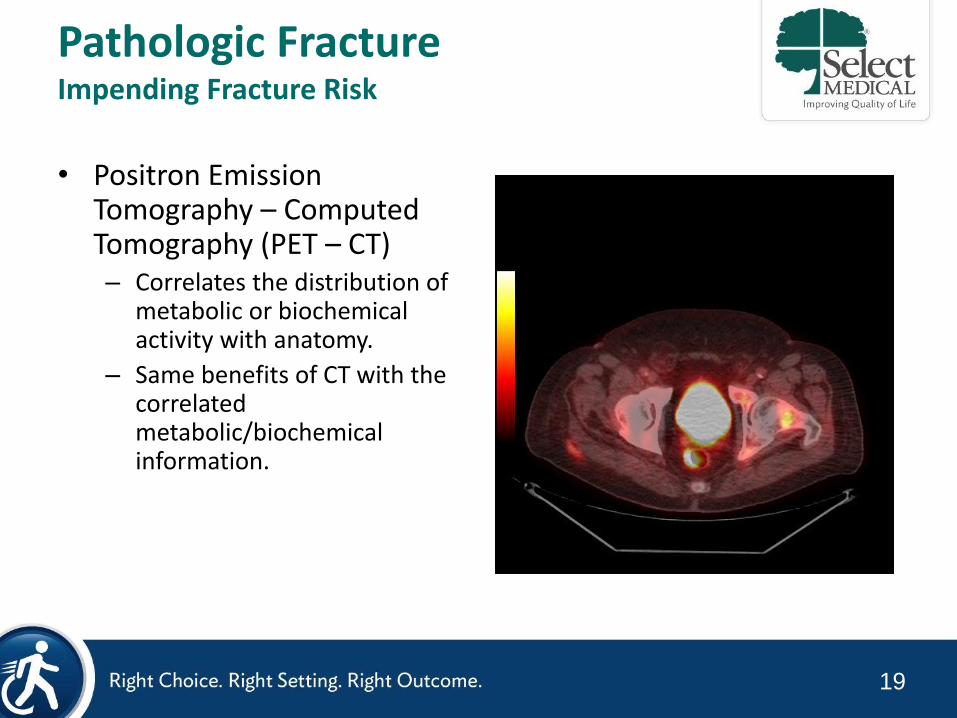
Pathologic Fracture Impending Fracture Risk
• Positron Emission Tomography – Computed Tomography (PET – CT) – Correlates the distribution of
metabolic or biochemical activity with anatomy.
– Same benefits of CT with the correlated metabolic/biochemical information.
20
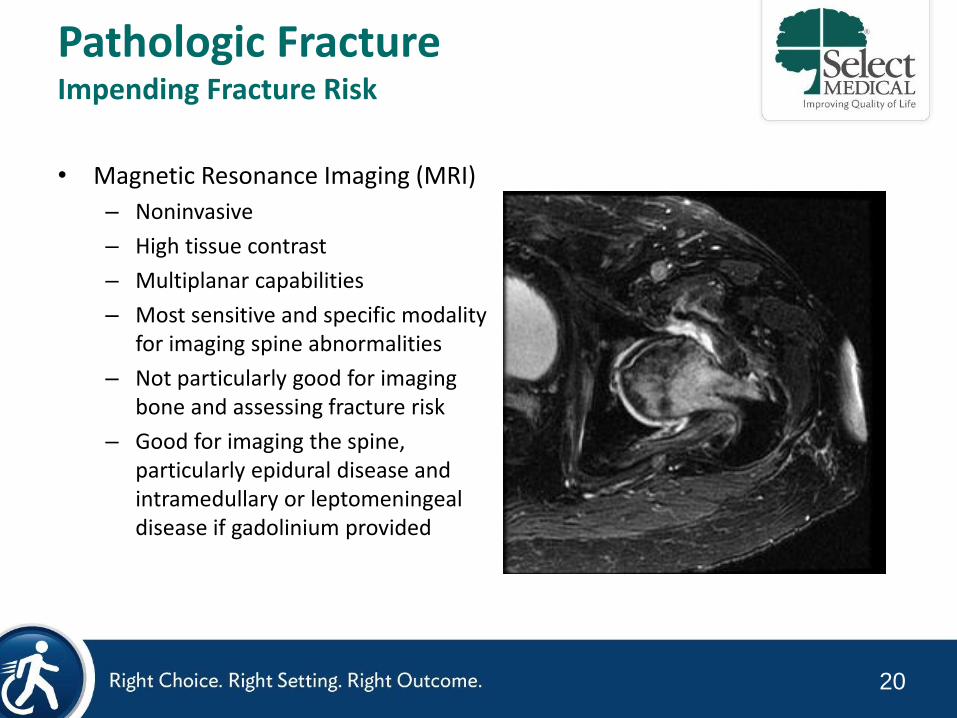
Pathologic Fracture Impending Fracture Risk
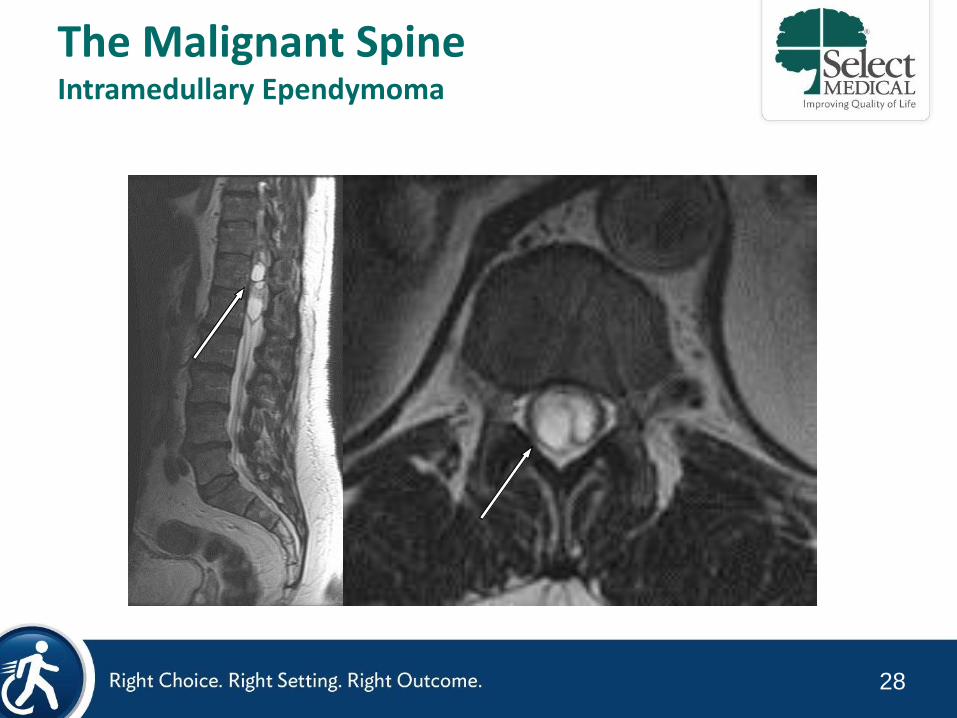
• Magnetic Resonance Imaging (MRI)
– Noninvasive
– High tissue contrast
– Multiplanar capabilities
– Most sensitive and specific modality for imaging spine abnormalities
– Not particularly good for imaging bone and assessing fracture risk
– Good for imaging the spine, particularly epidural disease and intramedullary or leptomeningeal disease if gadolinium provided
21
Pathologic Fracture Impending Fracture Risk
• Risk Factors – Anatomic site
• i.e., long bones
– Pain
• i.e., biologic, functional
– Primary tumor type
• i.e., multiple myeloma
– Amount of bony destruction
i.e., 50% cortical destruction, >2.5 cm diameter
– Lytic vs. blastic
From: Stubblefield MD and O'Dell MW, editors. Cancer Rehabilitation: Principles and Practice. New York, NY: Demos Medical Publishing; 2009.
22
Pathologic Fracture Impending Fracture Risk
• Risk Factor Caveats – Lesions not static and tend to progress
– Degree of bone destruction difficult to measure
– Amount of weight bearing placed on a bone difficult to measure
– A collapsed vertebral body can still support weight
– Chemotherapy has improved
– Steroids and other osteoporosis-inducing drugs common
– Radiation therapy has improved but can cause radio-osteonecrosis
– Bisphosphonates are standard therapy in bone metastases
From: Stubblefield MD and O'Dell MW, editors. Cancer Rehabilitation: Principles and Practice. New York, NY: Demos Medical Publishing; 2009.
23
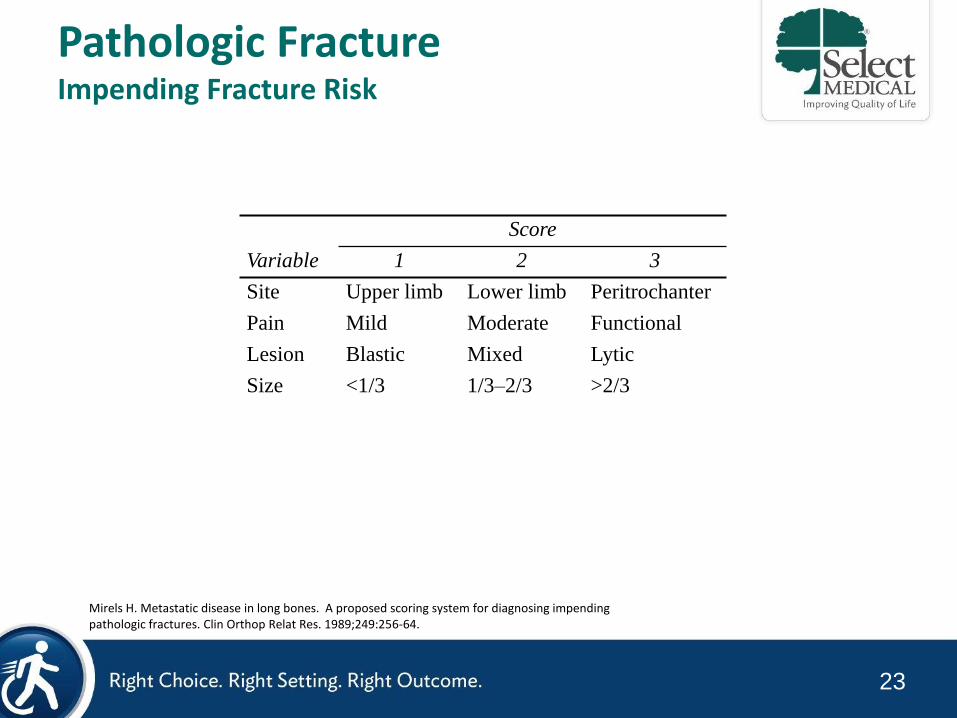
Pathologic Fracture Impending Fracture Risk
Score
Variable 1 2 3
Site Upper limb Lower limb Peritrochanter
Pain Mild Moderate Functional
Lesion Blastic Mixed Lytic
Size <1/3 1/3–2/3 >2/3
Mirels H. Metastatic disease in long bones. A proposed scoring system for diagnosing impending pathologic fractures. Clin Orthop Relat Res. 1989;249:256-64.
Prophylactic fixation prior to XRT recommended for patients with score ≥9

24
The Malignant Spine
25
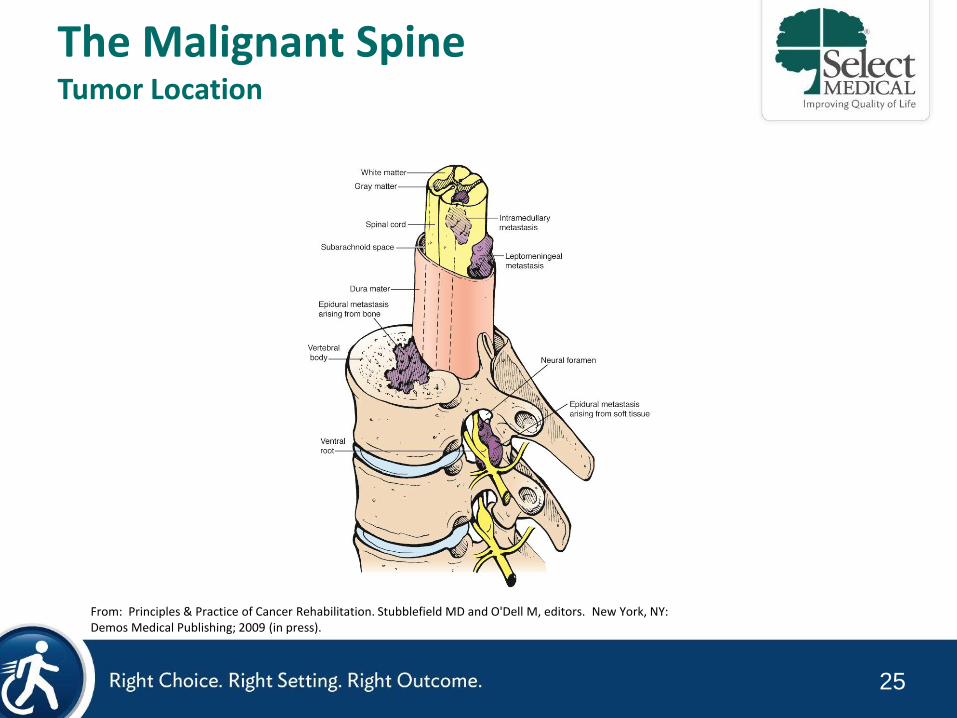
The Malignant Spine Tumor Location
From: Principles & Practice of Cancer Rehabilitation. Stubblefield MD and O'Dell M, editors. New York, NY: Demos Medical Publishing; 2009 (in press).
26
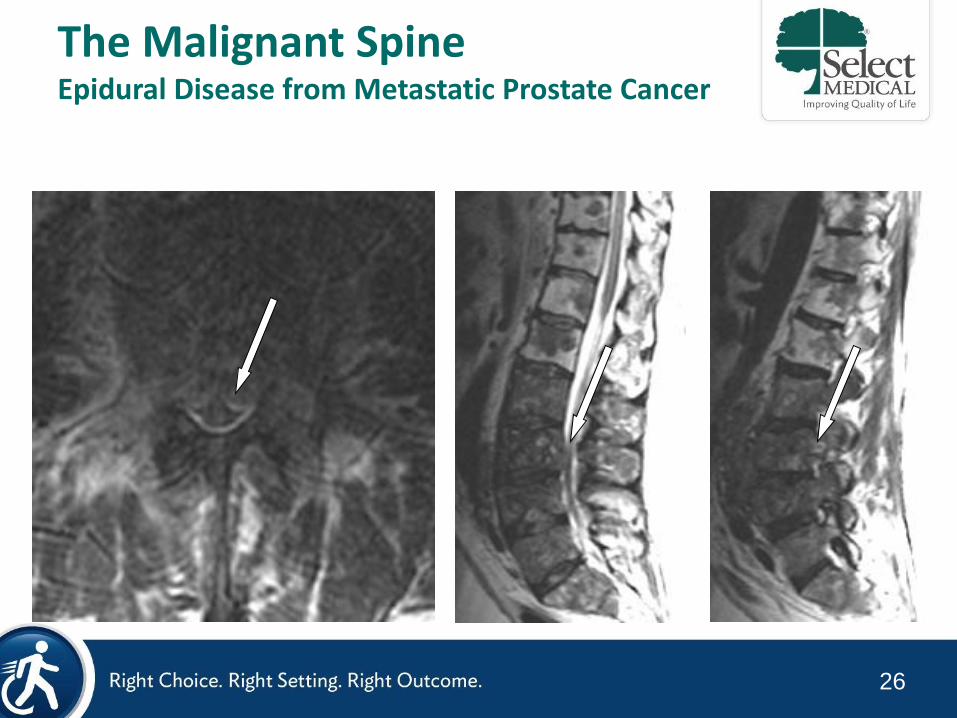
The Malignant Spine Epidural Disease from Metastatic Prostate Cancer
27
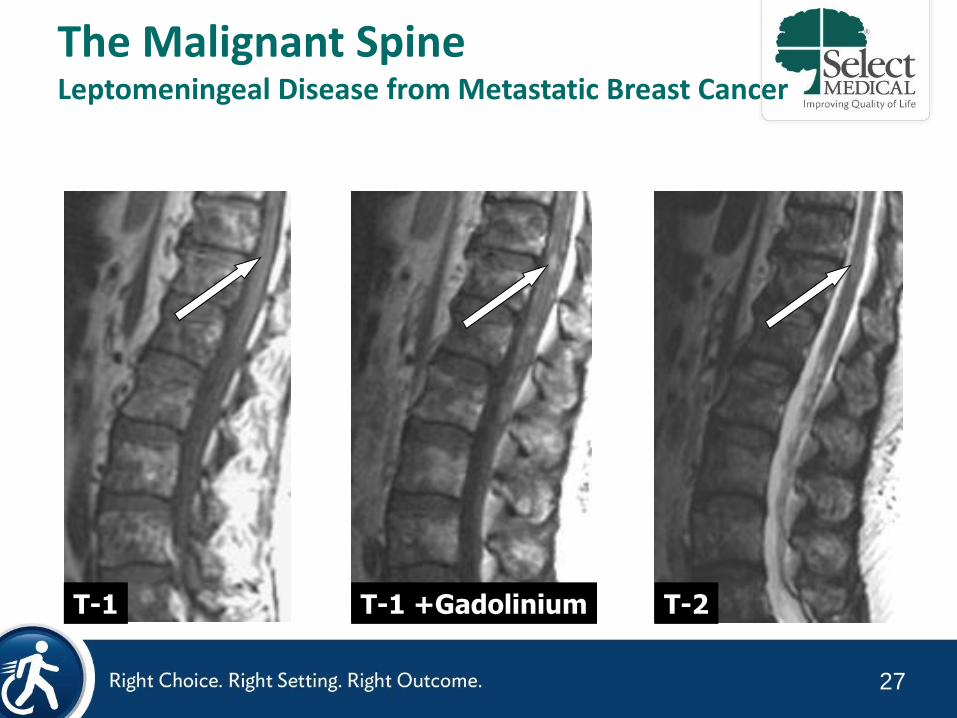
T-1 T-1 +Gadolinium T-2
The Malignant Spine Leptomeningeal Disease from Metastatic Breast Cancer
28
The Malignant Spine Intramedullary Ependymoma
29
0
3
1
4
1
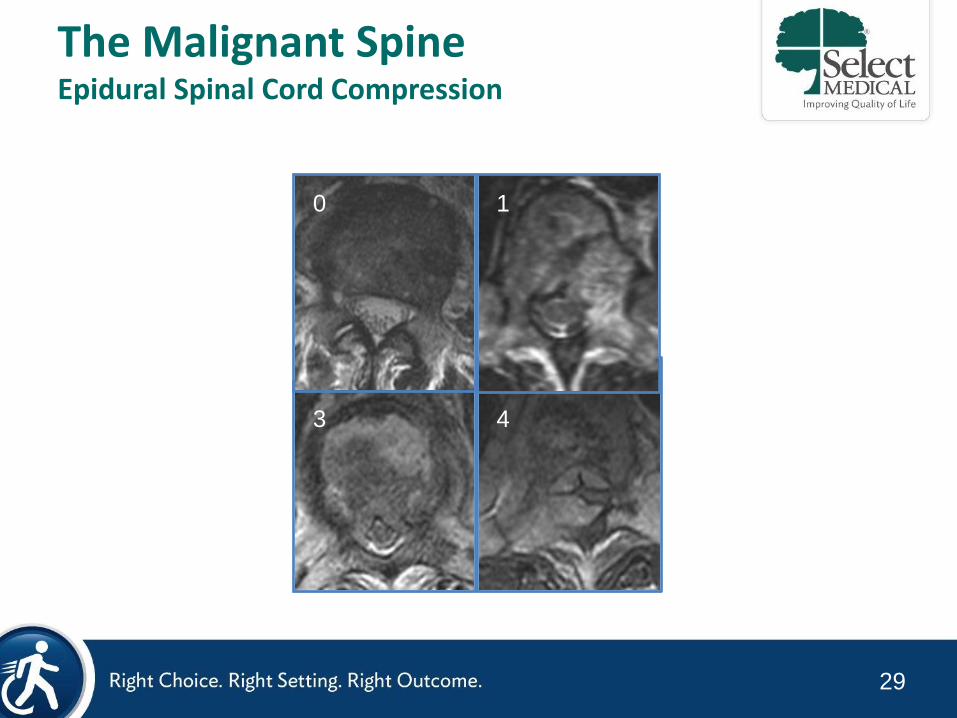
The Malignant Spine Epidural Spinal Cord Compression
30
The Malignant Spine Definition of Spinal Instability
The Spine Oncology Study Group (SOSG) defines spine instability as loss of spinal integrity as a result of a neoplastic process that is associated with movement-related pain, symptomatic or progressive deformity, and/or neural compromise under physiologic loads
Fisher CG, DiPaola CP, Ryken TC, Bilsky MH, Shaffrey CI, Berven SH et al. A novel classification system for spinal instability in neoplastic disease: an evidence-based approach and expert consensus from the Spine Oncology Study Group. Spine (Phila Pa 1976) 2010;35(22):E1221-9.
31
The Malignant Spine Mechanical Instability vs. Biologic Pain
• Involves release of chemical mediators, elevated intraosseous pressure, and stretching or irritation of the periosteum
• Worse at night and when recumbent
• Responds to steroids
• Requires Surgery • Defined by level of tumor
involvement • Involves release of chemical
mediators, elevated intraosseous pressure, and stretching or irritation of the periosteum
• Movement Related • Exacerbated increased axial load
(sitting, standing) • Not helped by steroids
Biologic/Tumor Mechanical
Instability
Bilsky MH. New therapeutics in spine metastases. Expert Rev Neurother 2005;5(6):831-40.
32
SINS
Component
Description Score
Location Junctional (Occ-C2, C7-T2, T11-L1, L5-
S1)
Mobile (C3-6, L2-4)
Semirigid (T3-10)
Rigid (S2-5)
3
2
1
0
Pain Yes*
Occasional non-mechanical pain
No
3
1
0
Bone Lesion Lytic
Mixed
Blastic
2
1
0
Alignment Subluxation / translation
De novo deformity
Normal
4
2
0
Vertebral Body >50% collapse
<50% collapse
No collapse with >50% VB involved
None of above
3
2
1
0
Posterolateral
Involvement of
Spinal Elements†
Bilateral
Unilateral
None
3
1
0
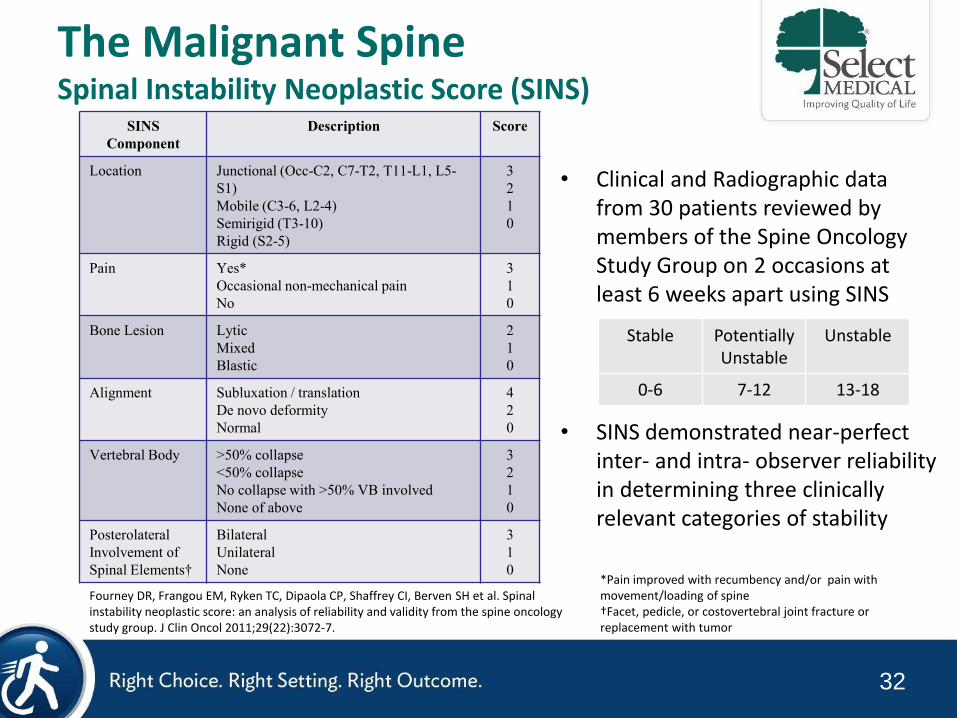
The Malignant Spine Spinal Instability Neoplastic Score (SINS)
• Clinical and Radiographic data from 30 patients reviewed by members of the Spine Oncology Study Group on 2 occasions at least 6 weeks apart using SINS
• SINS demonstrated near-perfect inter- and intra- observer reliability in determining three clinically relevant categories of stability
Stable Potentially Unstable
Unstable
0-6 7-12 13-18
Fourney DR, Frangou EM, Ryken TC, Dipaola CP, Shaffrey CI, Berven SH et al. Spinal instability neoplastic score: an analysis of reliability and validity from the spine oncology study group. J Clin Oncol 2011;29(22):3072-7.
*Pain improved with recumbency and/or pain with movement/loading of spine †Facet, pedicle, or costovertebral joint fracture or replacement with tumor
33
Radiation Fibrosis Syndrome

34
Radiation Fibrosis Syndrome Common Clinical Sequelae
• Myelo-radiculo-plexo-neuro-myopathy
• Cervical dystonia
• Neck extensor weakness (“dropped head syndrome”)
• Trigeminal neuralgia
• Cervical plexopathy
• Trismus (oropharyngeal dystonia)
• Mononeuropathies
• RTC tendonitis/adhesive capsulitis
• Lymphedema
Stubblefield MD. Radiation Fibrosis Syndrome: Neuromuscular and Musculoskeletal Complications in Cancer Survivors. PM&R. 2011;3:1041-54.
35
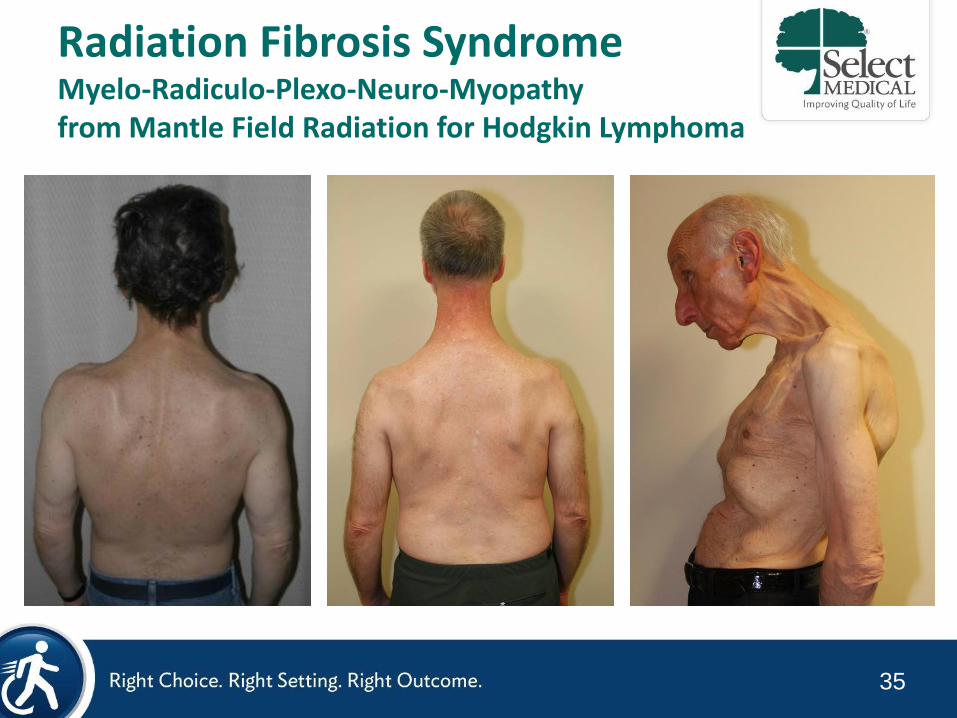
Radiation Fibrosis Syndrome Myelo-Radiculo-Plexo-Neuro-Myopathy from Mantle Field Radiation for Hodgkin Lymphoma
36
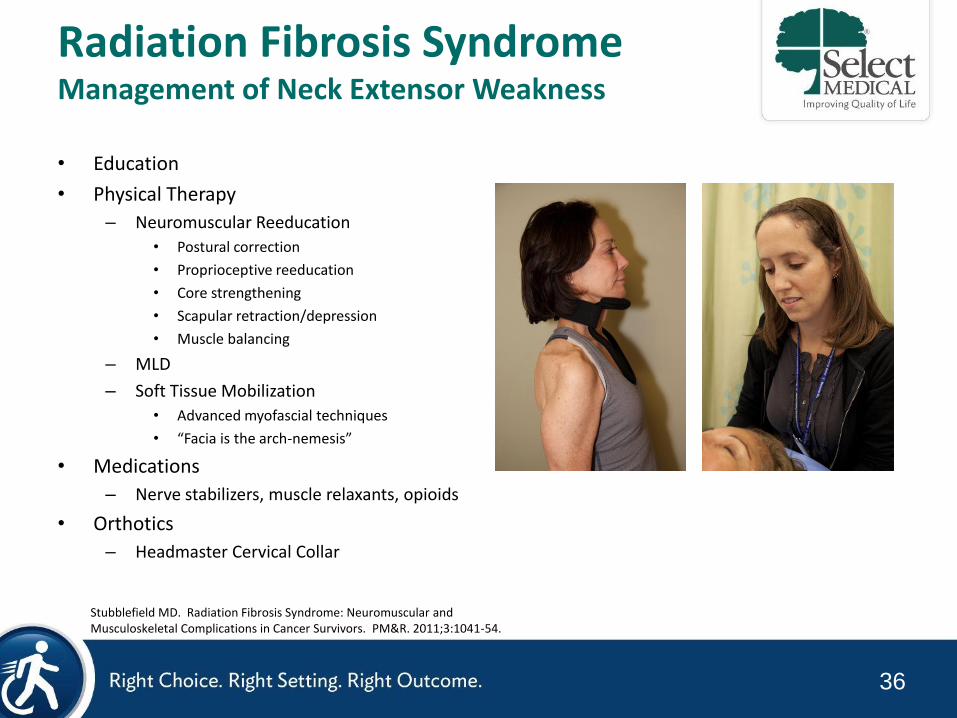
Radiation Fibrosis Syndrome Management of Neck Extensor Weakness
• Education
• Physical Therapy
– Neuromuscular Reeducation
• Postural correction
• Proprioceptive reeducation
• Core strengthening
• Scapular retraction/depression
• Muscle balancing
– MLD
– Soft Tissue Mobilization
• Advanced myofascial techniques
• “Facia is the arch-nemesis”
• Medications
– Nerve stabilizers, muscle relaxants, opioids
• Orthotics
– Headmaster Cervical Collar
Stubblefield MD. Radiation Fibrosis Syndrome: Neuromuscular and Musculoskeletal Complications in Cancer Survivors. PM&R. 2011;3:1041-54.
37
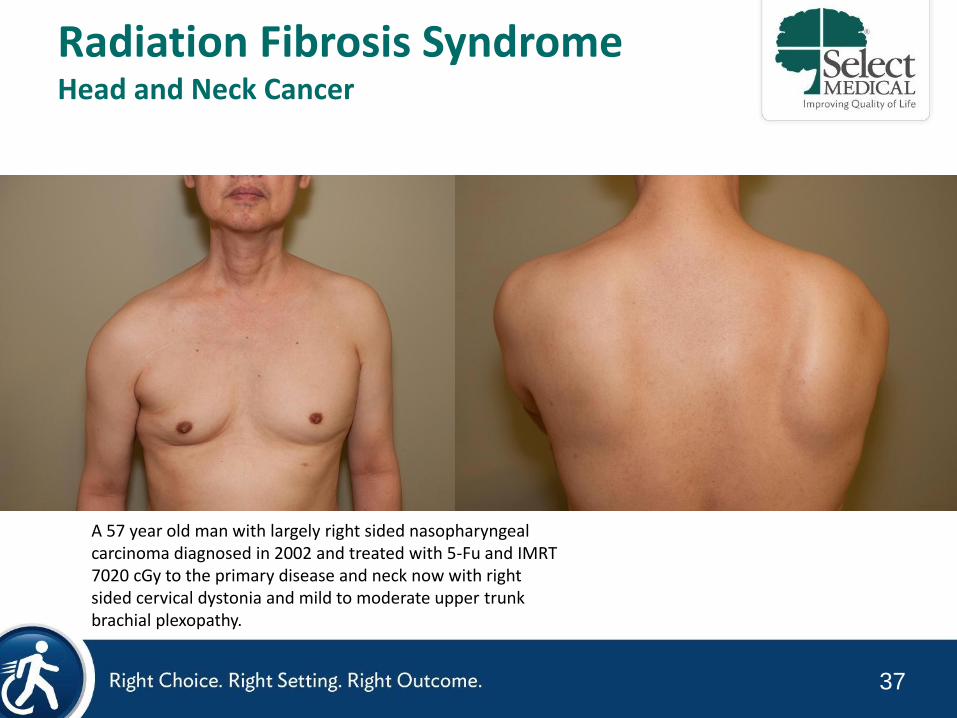
Radiation Fibrosis Syndrome Head and Neck Cancer
A 57 year old man with largely right sided nasopharyngeal carcinoma diagnosed in 2002 and treated with 5-Fu and IMRT 7020 cGy to the primary disease and neck now with right sided cervical dystonia and mild to moderate upper trunk brachial plexopathy.
38
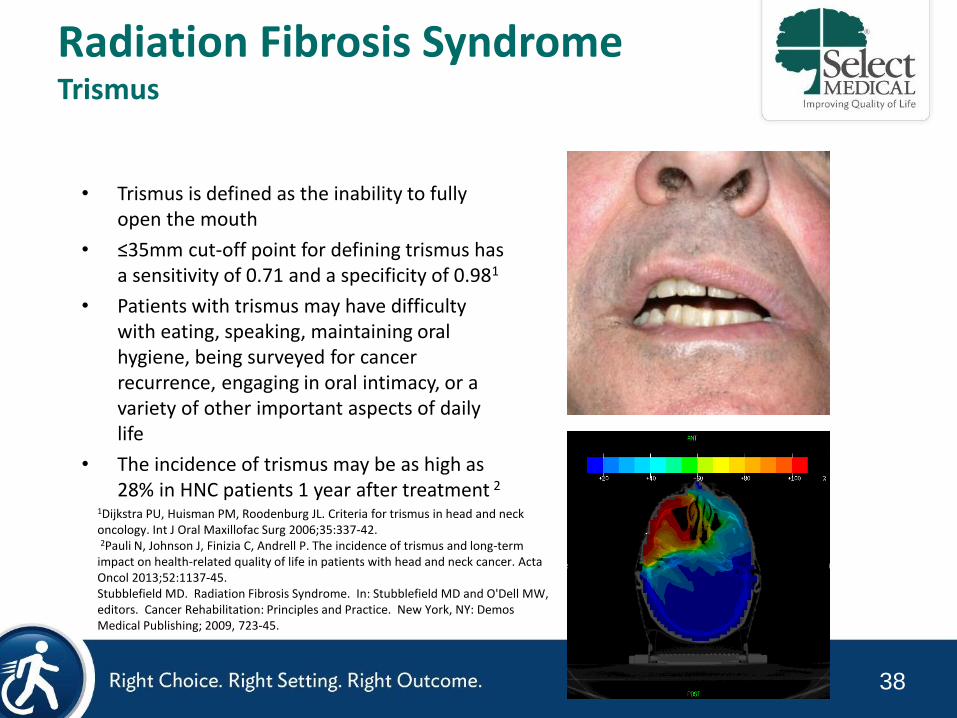
Radiation Fibrosis Syndrome Trismus
• Trismus is defined as the inability to fully open the mouth
• ≤35mm cut-off point for defining trismus has a sensitivity of 0.71 and a specificity of 0.981
• Patients with trismus may have difficulty with eating, speaking, maintaining oral hygiene, being surveyed for cancer recurrence, engaging in oral intimacy, or a variety of other important aspects of daily life
• The incidence of trismus may be as high as 28% in HNC patients 1 year after treatment 2
1Dijkstra PU, Huisman PM, Roodenburg JL. Criteria for trismus in head and neck oncology. Int J Oral Maxillofac Surg 2006;35:337-42. 2Pauli N, Johnson J, Finizia C, Andrell P. The incidence of trismus and long-term impact on health-related quality of life in patients with head and neck cancer. Acta Oncol 2013;52:1137-45. Stubblefield MD. Radiation Fibrosis Syndrome. In: Stubblefield MD and O'Dell MW, editors. Cancer Rehabilitation: Principles and Practice. New York, NY: Demos Medical Publishing; 2009, 723-45.
39
Radiation Fibrosis Syndrome Management of Radiation-induced Trismus
• Education
• Physical Therapy
– Soft Tissue Mobilization
• Advanced myofascial techniques
– Neuromuscular Reeducation
• Postural correction
• Proprioceptive reeducation
• Muscle balancing
– MLD
• Medications
– pregabalin, gabapentin, duloxetine
• Orthotics
– Dynasplint, Therabite
• Injections
– Botulinum Toxin Injection
Stubblefield MD, Levine A, Custodio CM, Fitzpatrick T. The role of botulinum toxin type A in the radiation fibrosis syndrome: a preliminary report. Arch Phys Med Rehabil 2008;89(3):417-21. Stubblefield MD, Manfield L, Riedel ER. A Preliminary Report on the Efficacy of a Dynamic Jaw Opening Device (Dynasplint Trismus System) as part of the Multimodal Treatment of Trismus in Patients with Head and Neck Cancer. Arch Phys Med Rehabil. 2010;91:1278-82 Stubblefield MD. Radiation fibrosis syndrome: neuromuscular and musculoskeletal complications in cancer survivors. PM R 2011;3(11):1041-54.
40
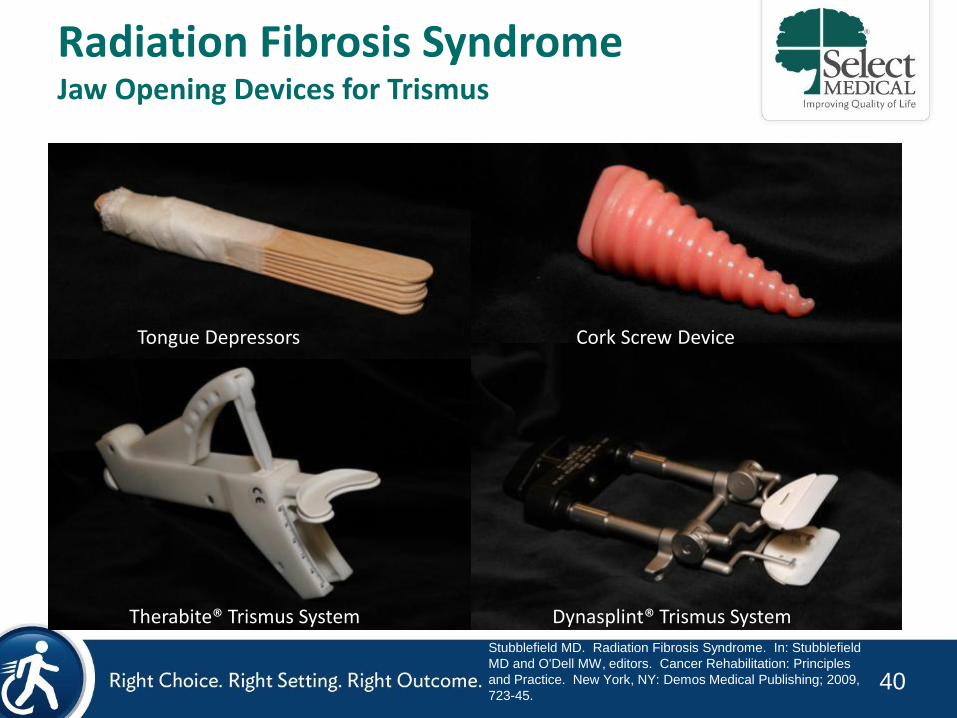
Radiation Fibrosis Syndrome Jaw Opening Devices for Trismus
Tongue Depressors
Dynasplint® Trismus System
Therabite® Trismus System
Cork Screw Device
Stubblefield MD. Radiation Fibrosis Syndrome. In: Stubblefield
MD and O'Dell MW, editors. Cancer Rehabilitation: Principles
and Practice. New York, NY: Demos Medical Publishing; 2009,
723-45.
41
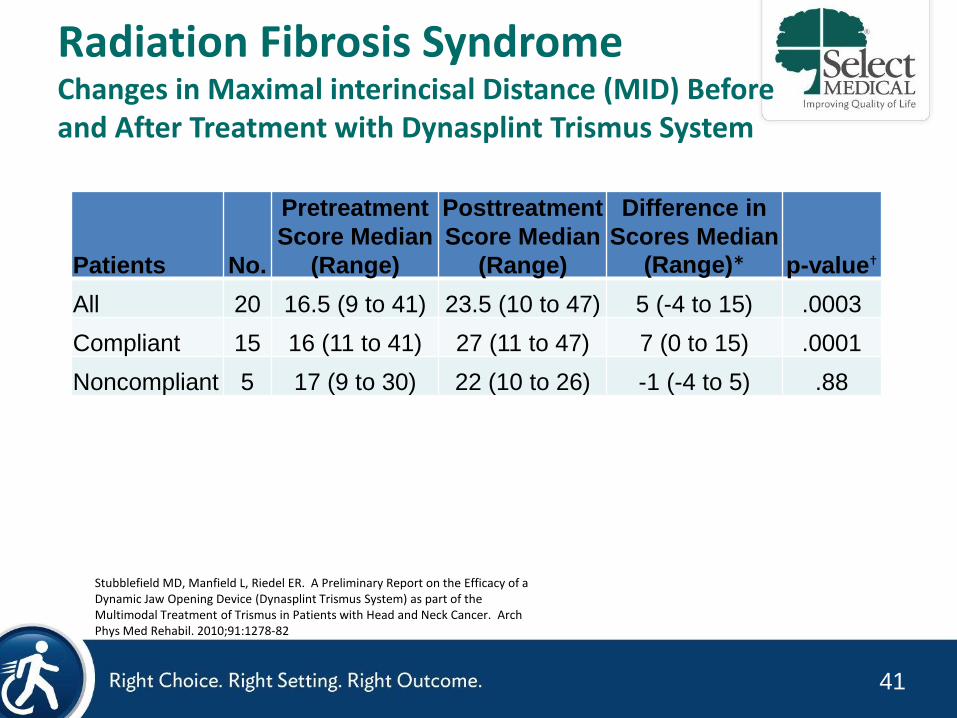
Radiation Fibrosis Syndrome Changes in Maximal interincisal Distance (MID) Before and After Treatment with Dynasplint Trismus System
Patients No.
Pretreatment
Score Median
(Range)
Posttreatment
Score Median
(Range)
Difference in
Scores Median
(Range)* p-value†
All 20 16.5 (9 to 41) 23.5 (10 to 47) 5 (-4 to 15) .0003
Compliant 15 16 (11 to 41) 27 (11 to 47) 7 (0 to 15) .0001
Noncompliant 5 17 (9 to 30) 22 (10 to 26) -1 (-4 to 5) .88
*Based on the difference of the preintervention and postintervention values for each individual patient. †P values were calculated for differences in the pretreatment and posttreatment scores using the Wilcox sign-rank test.
Stubblefield MD, Manfield L, Riedel ER. A Preliminary Report on the Efficacy of a Dynamic Jaw Opening Device (Dynasplint Trismus System) as part of the Multimodal Treatment of Trismus in Patients with Head and Neck Cancer. Arch Phys Med Rehabil. 2010;91:1278-82
42
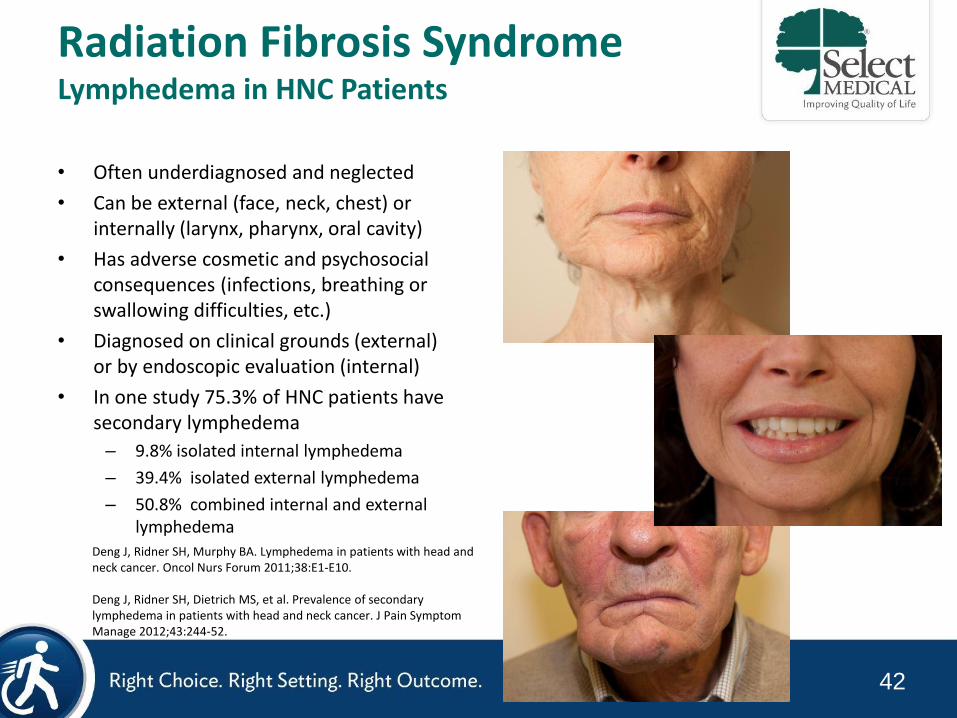
Radiation Fibrosis Syndrome Lymphedema in HNC Patients
• Often underdiagnosed and neglected
• Can be external (face, neck, chest) or internally (larynx, pharynx, oral cavity)
• Has adverse cosmetic and psychosocial consequences (infections, breathing or swallowing difficulties, etc.)
• Diagnosed on clinical grounds (external) or by endoscopic evaluation (internal)
• In one study 75.3% of HNC patients have secondary lymphedema
– 9.8% isolated internal lymphedema
– 39.4% isolated external lymphedema
– 50.8% combined internal and external lymphedema
Deng J, Ridner SH, Murphy BA. Lymphedema in patients with head and neck cancer. Oncol Nurs Forum 2011;38:E1-E10. Deng J, Ridner SH, Dietrich MS, et al. Prevalence of secondary lymphedema in patients with head and neck cancer. J Pain Symptom Manage 2012;43:244-52.
43
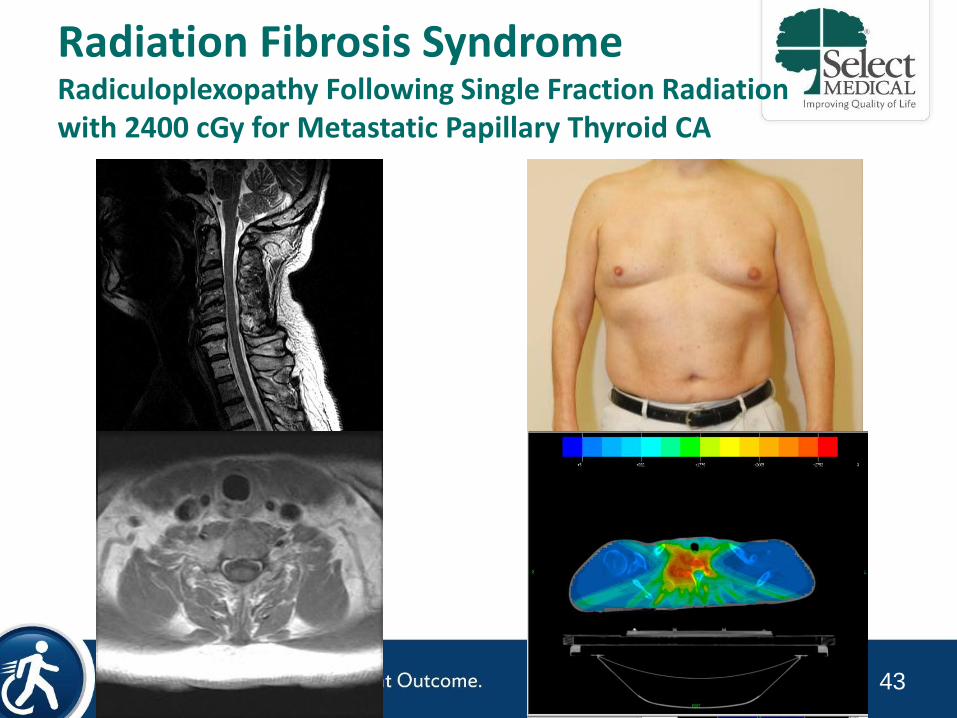
Radiation Fibrosis Syndrome Radiculoplexopathy Following Single Fraction Radiation with 2400 cGy for Metastatic Papillary Thyroid CA
2011-5-11 2011-6-7

44
Neuropathy
45
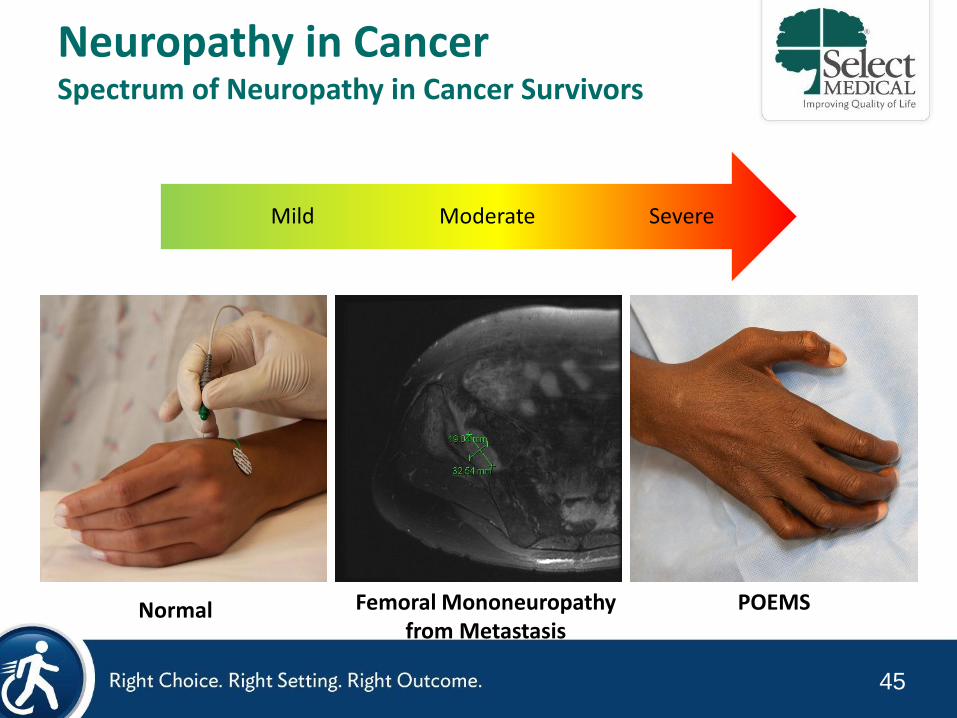
Neuropathy in Cancer Spectrum of Neuropathy in Cancer Survivors
Severe Moderate Mild
Normal Femoral Mononeuropathy from Metastasis
POEMS
46
Neuropathy in Cancer Common Neurotoxic Chemotherapeutics
• Platinum Analogues – Cisplatin
– Carboplatin
– Oxaliplatin
• Vinca Alkaloids – Vincristine
– Vinblastine
– Vinorelbine
– Vindesine
• Taxanes – Paclitaxel
– Abraxane
– Docetaxel
• Others – Bortezomib
– Ixabepilone
– Thalidomide
– Lenalidomide
Stubblefield MD, Burstein HJ, Burton AW, Custodio CM, Deng GE, Ho M et al. NCCN task force report: management of neuropathy in cancer. J Natl Compr Canc Netw 2009;7 Suppl 5:S1-S26; quiz S7-8.
47
Neuropathy in Cancer Incidence of Neuropathy by Agent
• Taxanes
– Paclitaxel: 57%-83% overall; 2%-33% severe
– Docetaxel: 11%-66% overall; 3%-14% severe
• Vinca alkaloids
– 30%-47%
• Platinum Analogues
– Cisplatin: 28%-100%
• Capecitabine (unknown)
• Capecitabine + Ixabepilone (microtubulin-targeting agent)
– 67% overall; 21% severe
• Paclitaxel + Carboplatin
– 67%
Stubblefield MD, McNeely ML, Alfano CM, Mayer DK. A prospective surveillance model for physical rehabilitation of women with breast cancer: Chemotherapy-induced peripheral neuropathy. Cancer 2012;118(8 Suppl):2250-60.

48
Neuropathy in Cancer Vinca Alkaloids (vincristine, vinblastine, vinorelbine)
• Indications:
– Solid tumors, lymphoma, leukemia
• Mechanism of action:
– Binds tubulin and blocks its polymerization into microtubules
– Arrests mitosis in metaphase
• Clinical Features:
– Distal symmetric sensorimotor axonal PN
– Affects large and small fibers
49
Neuropathy in Cancer Taxanes (paclitaxel, docetaxel)
• From Pacific Yew Tree (Taxus brevifolia)
• Indications:
– Solid tumors (i.e., ovarian and breast cancer)
• Mechanism of action:
– Binds tubulin and blocks its polymerization into microtubules
– Arrests mitosis in metaphase
• Clinical Features:
– Distal symmetric sensorimotor axonal PN
– Affects large fiber > small fiber functions
50
Neuropathy in Cancer Platinum Analogues (cisplatin, carboplatin, oxaliplatin)
• Indications: – Solid tumors (ie, ovarian, testicular, & bladder cancer)
• Mechanism of action: – Binds and cross-links DNA, inhibits protein synthesis, and impairs axonal
transport
• Clinical Features: – Preferential damage to dorsal root ganglion
– Distal symmetric predominately sensory axonal PN
– Affects large fiber > small & sensory > motor fibers
– Sensory ataxia
– Symptoms can appear after treatment and progress for months following treatment
51
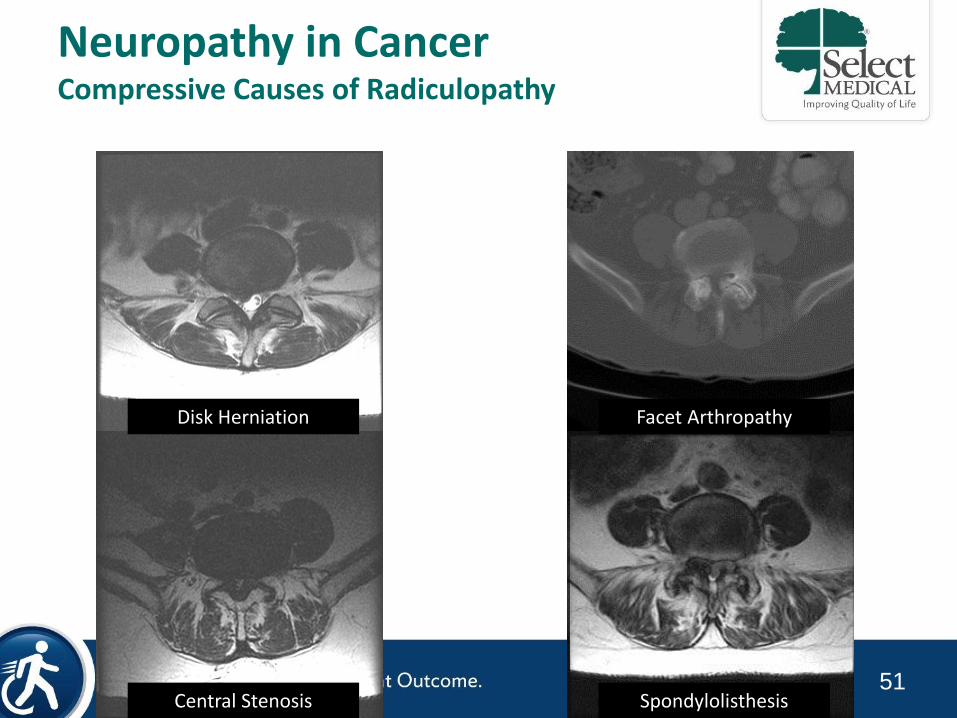
Neuropathy in Cancer Compressive Causes of Radiculopathy
Central Stenosis Spondylolisthesis
Facet Arthropathy Disk Herniation
52
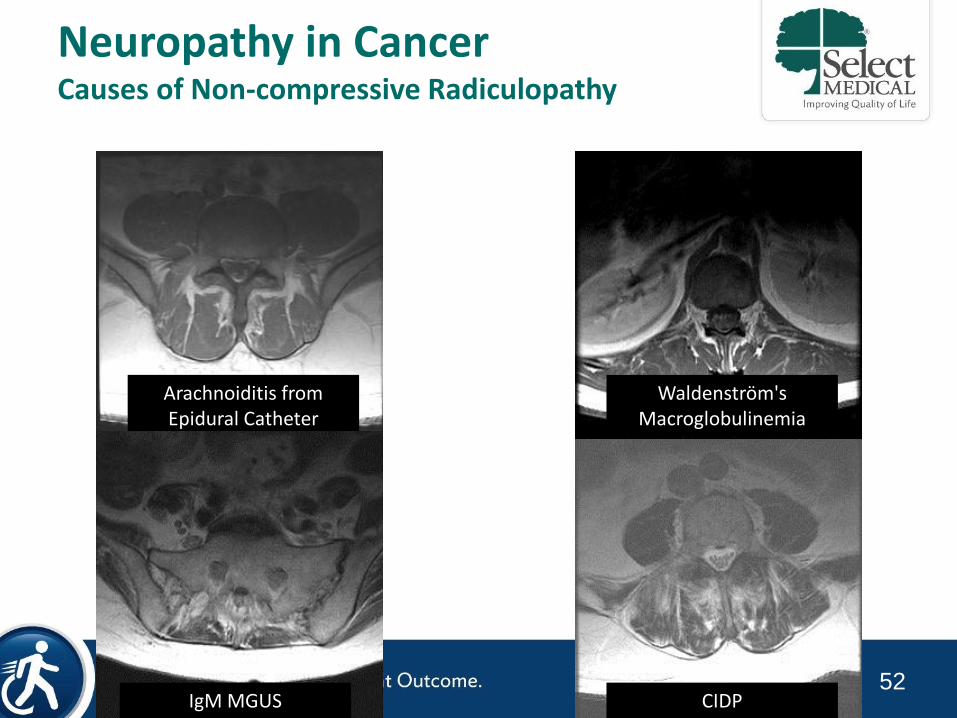
Neuropathy in Cancer Causes of Non-compressive Radiculopathy
Arachnoiditis from Epidural Catheter
Waldenström's Macroglobulinemia
IgM MGUS CIDP
53
Upper Body Pain Disorders Common Diagnoses
• Neuromuscular
– Cervical Radiculopathy
– Brachial Plexopathy
– Polyneuropathy
– Mononeuropathy
– Post-mastectomy pain syndrome
– Complex regional pain syndrome
• Lymphovascular
– Lymphedema
– Axillary web syndrome
– Post-thrombotic syndrome
• Musculoskeletal
– Post-surgical pain
– Rotator cuff disease
– Bicipital tendonitis
– Adhesive capsulitis
– Bony metastases
– Epicondylitis
– DeQuervain’s tenosynovitis
– Arthralgias
– Arthritis
• Integumentary
– Cellulitis
– Radiation dermatitis
Stubblefield MD, Keole, N. Upper Body Pain and Functional Disorders in Breast Cancer Patients. PMR. 2014;6(2):170-83.
54
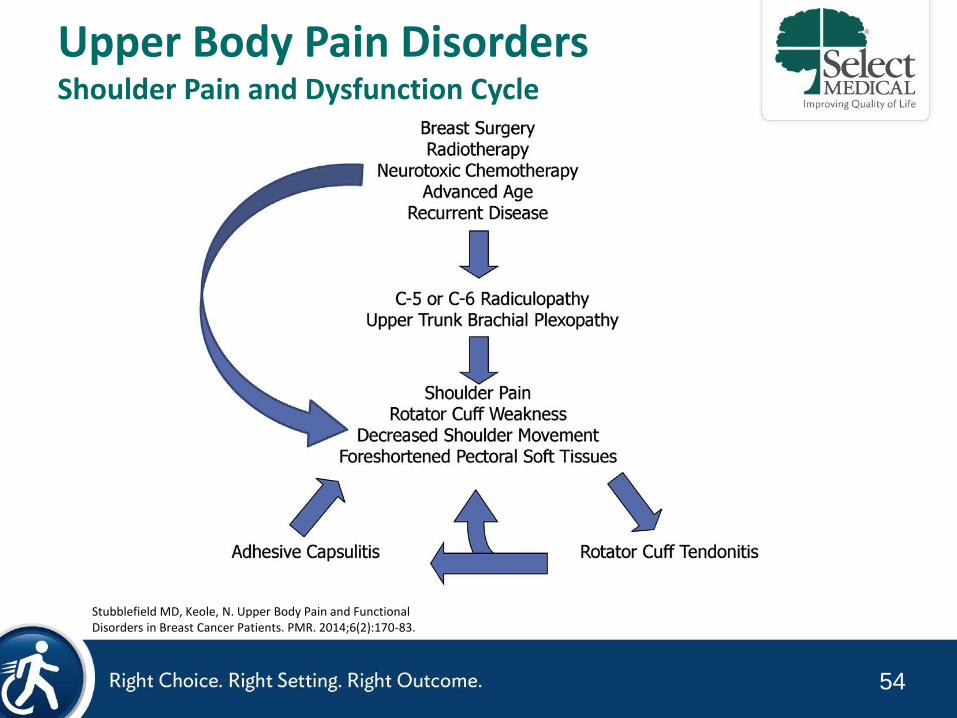
Upper Body Pain Disorders Shoulder Pain and Dysfunction Cycle
Stubblefield MD, Keole, N. Upper Body Pain and Functional Disorders in Breast Cancer Patients. PMR. 2014;6(2):170-83.
55
Exercise and Lymphedema
56
Exercise in Cancer 2010 American College of Sports Medicine Guidelines
“Some of the psychological and physiological challenges faced by cancer survivors can be prevented, attenuated, treated or rehabilitated through exercise”
• Exercise is Safe
– During and after cancer treatments*
– Results in improvements in
• Physical functioning
– Aerobic fitness
– Muscular strength
– Flexibility
• Quality of life
• Cancer-related fatigue
• Body image & composition
• Anxiety
*Only select groups studied
Schmitz KH, Courneya KS, Matthews C, Demark-Wahnefried W, Galvao DA, Pinto BM et al. American College of Sports Medicine roundtable on exercise guidelines for cancer survivors. Med Sci Sports Exerc 2010;42(7):1409-26.
57
Lymphedema Upper Extremity Exercise for Breast Cancer Survivors
Upper body exercise has historically been discouraged in breast cancer survivors following axillary lymph node dissection and/or radiation for fear of precipitating or exacerbating lymphedema.
Cheema B, Gaul CA, Lane K, Fiatarone Singh MA. Progressive resistance training in breast cancer: a systematic review of clinical trials. Breast Cancer Res Treat 2008;109(1):9-26.
58
Lymphedema Dragon Boat Racing
McKenzie DC. Abreast in a boat--a race against breast cancer. CMAJ 1998;159(4):376-8
59
Lymphedema Weight Lifting in Women with Breast Cancer-Related Lymphedema
•141 Breast Cancer survivors with lymphedema –71 twice weekly weight lifting
•No upper limit on progression
•Instructed to wear compression garment
–70 controls
•Instructed not to change their exercise during the study
Schmitz KH, Ahmed RL, Troxel A, Cheville A, Smith R, Lewis-Grant L et al. Weight lifting in women with breast-cancer-related lymphedema. N Engl J Med 2009;361(7):664-73.
60
Lymphedema Weight Lifting in Women with Breast Cancer-Related Lymphedema
•Primary Outcome –5% change in hand/arm swelling at 1 year
•Secondary Outcomes –Exacerbations of lymphedema
–Amount and severity of lymphedema symptoms
–Muscle strength
Schmitz KH, Ahmed RL, Troxel A, Cheville A, Smith R, Lewis-Grant L et al. Weight lifting in women with breast-cancer-related lymphedema. N Engl J Med 2009;361(7):664-73.
61
Lymphedema Weight Lifting in Women with Breast Cancer-Related Lymphedema
•Results: Primary Outcome –Compared with Controls, weight lifters did not have worsening of their lymphedema (11% vs. 12%)
•Results: Secondary Outcomes –Exacerbations of lymphedema decreased (14% vs. 29% in controls)
–Amount and severity of lymphedema symptoms decreased (p=0.03)
–Upper- and lower-body strength increased (p<0.001)
Schmitz KH, Ahmed RL, Troxel A, Cheville A, Smith R, Lewis-Grant L et al. Weight lifting in women with breast-cancer-related lymphedema. N Engl J Med 2009;361(7):664-73.
62
Lymphedema Weight Lifting in Women at risk for Breast Cancer-Related Lymphedema
Schmitz KH, Ahmed RL, Troxel AB, Cheville A, Lewis-Grant L, Smith R et al. Weight lifting for women at risk for breast cancer-related lymphedema: a randomized trial. JAMA 2010;304(24):2699-705.
•154 Breast Cancer survivors 1-5 years post-breast cancer surgery (including lymph node removal) with no clinical signs of lymphedema
–72 randomized to weightlifting in a community fitness center (usually a YMCA) with 13 weeks supervised instruction and 9 months unsupervised
–75 controls
63
•Primary Outcome –5% change in hand/arm swelling at 1 year
•Results –No increase incidence of lymphedema
–11% (8/72) in the weight lifting group vs. 17% (13/75) in the control group developed lymphedema (p=0.04)
–In women with ≥5 lymph nodes removed 7% (3/45) in the weight lifting group vs. 22% 11/49 in the control group developed lymphedema (p=0.003)
Schmitz KH, Ahmed RL, Troxel AB, Cheville A, Lewis-Grant L, Smith R et al. Weight lifting for women at risk for breast cancer-related lymphedema: a randomized trial. JAMA 2010;304(24):2699-705.
Lymphedema Weight Lifting in Women at risk for Breast Cancer-Related Lymphedema
64
Lymphedema Compression Garments and Exercise
•The National Lymphedema Network position paper on exercise states “current understanding of the underlying physiology provides strong support for the use of compression garments”
•The systematic review by Kwan et al. states that “a clear evidence-based recommendation for use of compression garments cannot be made based on this current review”
Kwan ML, Cohn JC, Armer JM, Stewart BR, Cormier JN. Exercise in patients with lymphedema: a systematic review of the contemporary literature. J Cancer Surviv 2011;5(4):320-36.

65
Thank You