primary pci in anomalous coronary: wire first approach
TRANSCRIPT

Primary PCI in anomalous coronary: Wire first approach

Case Report
Primary PCI in anomalous coronary: Wire firstapproach
Abhijit Kulkarni a,*, B. Ramesh b
a Sr. Consultant, Department of Cardiology, Apollo Hospitals, Bangalore, Indiab Senior Consultant Cardiologist, Apollo Hospital, BG Road, Bangalore, India
a r t i c l e i n f o
Article history:
Received 5 October 2013
Accepted 2 May 2014
Available online xxx
Keywords:
Percutaneous coronary intervention
Acute coronary syndrome
Cardiac catheterization
Ostium
a b s t r a c t
Acute myocardial infarction in an anomalous coronary artery is an uncommon occurrence.
Elective (PCI) percutaneous coronary intervention in anomalous coronary in stable CAD is
challenging. We report a case of Primary PCI in an unstable patient (recurrent VT) with
anomalous coronary. Proximal portion of the occluded artery was delineated using non-
selective injection of dye with inverted left judkins directed towards the ostium. The
coronary guide wire was initially passed into the proximal lumen without guiding support
by skilled manipulation over which the left judkins was engaged. The catheter was
inverted when it engaged the anomalous ostium and the procedure was completed
successfully.
Copyright ª 2014, Indraprastha Medical Corporation Ltd. All rights reserved.
1. Case presentation
A 26-year-old smoker with no co morbidities was admitted to
our hospital with history of retrosternal chest pain with
sweating since 3 h. Electrocardiogram showed ST elevations
in inferior leads. He was administered heparin, nitrates and
antiplatelets and was taken up for cardiac catheterization.
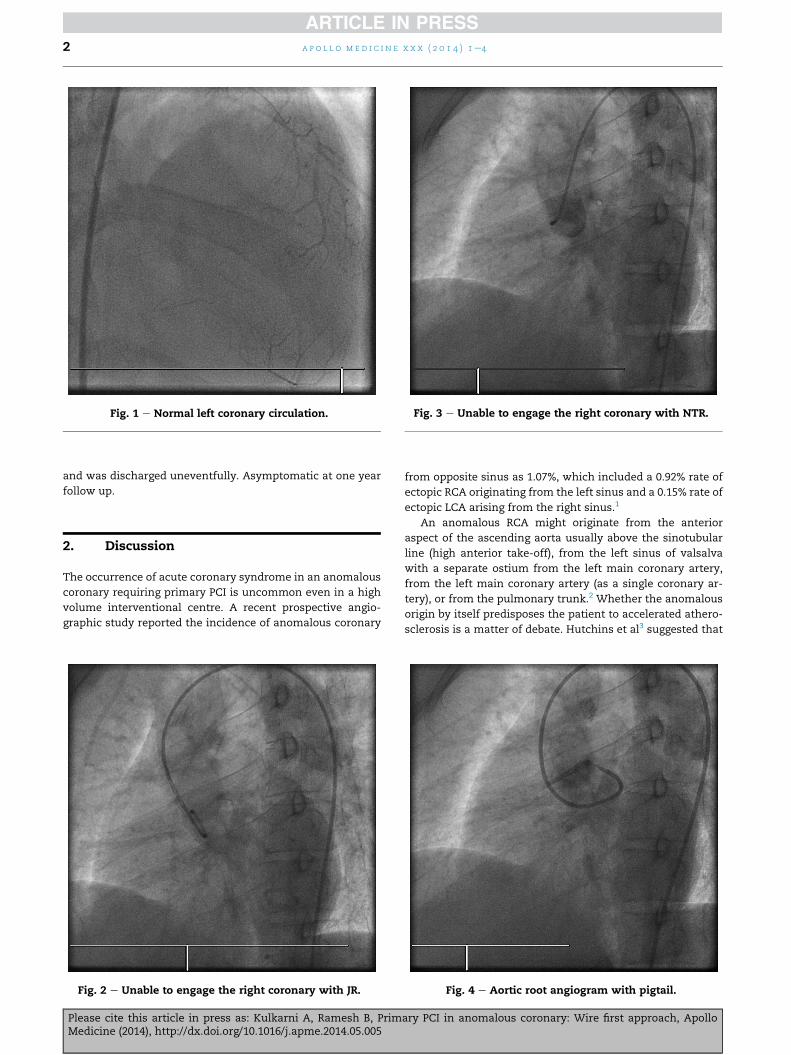
The left anterior descending and left circumflex were
normal (Fig. 1). Right coronary artery was seen filling through
collaterals very faintly from the left side confirming the ECG
findings. Right coronary ostium could not be engaged with
Judkins Right catheter, No Torque Right or amplatz catheters
(Figs. 2 and 3).
Patient at this time became unstable with VT and was
electrically cardioverted multiple times before stabilizing.
Aortogram with pigtail performed at this stage showed faint
opacification of an occluded anomalous right coronary artery
arising near left coronary ostium in the late phase (Fig. 4).
A left Judkins was chosen to attempt to engage the ostium,
which was near the left ostium. The ostium and the proximal
portion which was occluded were clearly delineated by the
angiogram with inverted left judkins (Fig. 5). However, we
could not cannulate the ostium and the patient had ongoing
pain with two episodes of VT, which were cardioverted. This
time BMW floppy wire was passed into the occluded artery by
skilled manipulation while the catheter was still in the root
(without guiding catheter support) (Fig. 6) and then over the
wire the guiding catheter was engaged. Export thrombus
aspiration catheter was used to aspirate the thrombus.
2.0� 8mmTREK balloon (Fig. 7) was used and after predilation
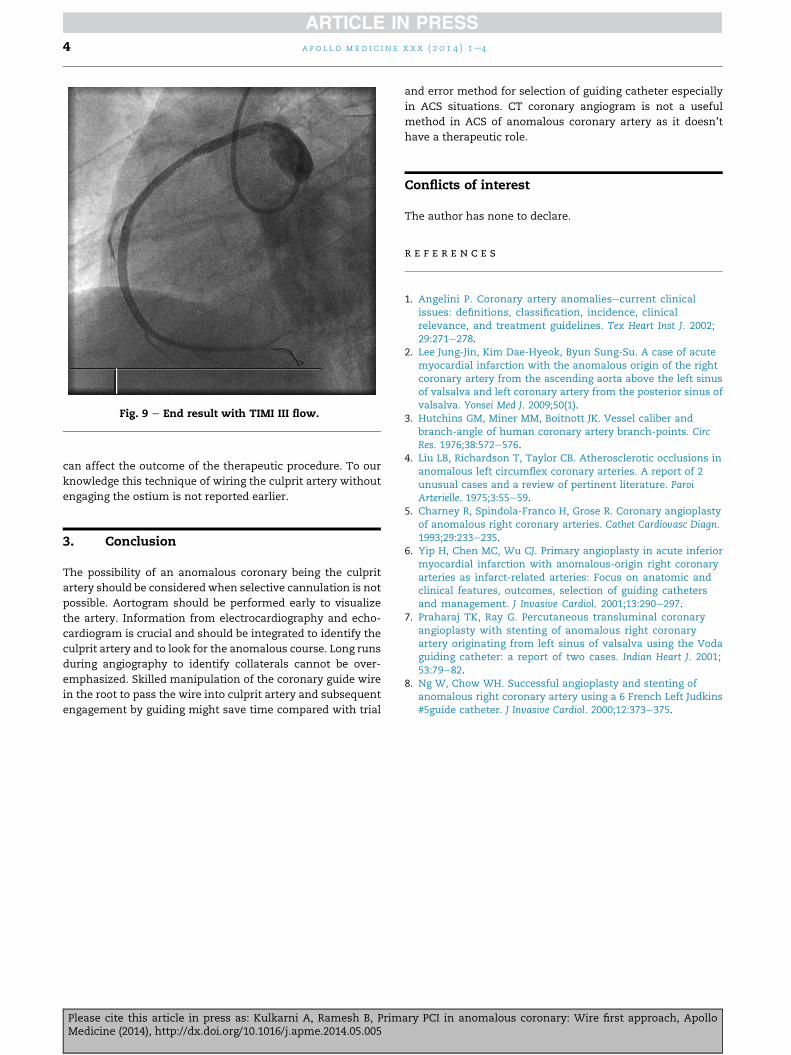
distal artery was visualized (Fig. 8). The thrombotic lesion was
covered with 3 � 24 mm PROMUS ELEMENT stent and TIMI III
flow was achieved (Fig. 9). The patient stabilized electrically
* Tel.: þ91 9008022866 (mobile).E-mail address: [email protected] (A. Kulkarni).
Available online at www.sciencedirect.com
ScienceDirect
journal homepage: www.elsevier .com/locate/apme
a p o l l o m e d i c i n e x x x ( 2 0 1 4 ) 1e4
Please cite this article in press as: Kulkarni A, Ramesh B, Primary PCI in anomalous coronary: Wire first approach, ApolloMedicine (2014), http://dx.doi.org/10.1016/j.apme.2014.05.005
http://dx.doi.org/10.1016/j.apme.2014.05.0050976-0016/Copyright ª 2014, Indraprastha Medical Corporation Ltd. All rights reserved.
and was discharged uneventfully. Asymptomatic at one year
follow up.
2. Discussion
The occurrence of acute coronary syndrome in an anomalous
coronary requiring primary PCI is uncommon even in a high
volume interventional centre. A recent prospective angio-
graphic study reported the incidence of anomalous coronary
from opposite sinus as 1.07%, which included a 0.92% rate of
ectopic RCA originating from the left sinus and a 0.15% rate of
ectopic LCA arising from the right sinus.1
An anomalous RCA might originate from the anterior
aspect of the ascending aorta usually above the sinotubular
line (high anterior take-off), from the left sinus of valsalva
with a separate ostium from the left main coronary artery,
from the left main coronary artery (as a single coronary ar-
tery), or from the pulmonary trunk.2 Whether the anomalous
origin by itself predisposes the patient to accelerated athero-
sclerosis is a matter of debate. Hutchins et al3 suggested that
Fig. 1 e Normal left coronary circulation.
Fig. 2 e Unable to engage the right coronary with JR.
Fig. 3 e Unable to engage the right coronary with NTR.
Fig. 4 e Aortic root angiogram with pigtail.
a p o l l o m e d i c i n e x x x ( 2 0 1 4 ) 1e42
Please cite this article in press as: Kulkarni A, Ramesh B, Primary PCI in anomalous coronary: Wire first approach, ApolloMedicine (2014), http://dx.doi.org/10.1016/j.apme.2014.05.005

the unusual angle of take-off and the more tortuous course of
the proximal portion of the anomalous coronary artery can
accelerate the rate of atherosclerosis.
Liu et al4 suggested that the junction point of the bound
portion and the free portion of an anomalous artery as it
wraps around the aorta is an area that is susceptible to lipid
accumulation.
Technical aspect of the procedure can be challenging
especially in an unstable patient as in our case. It is important
to identify the culprit artery based on integration of ECG, Echo
and angiogram reports so that search for the anomalous ar-
tery is hastened. It is suggested to do an aortogram early and
then choose catheters depending on position of anomalous
ostium. The catheters suggested in case of anomalous right
ostium are amplatz,5e7 voda6,7 or an undersized left judkins.8
Instead of “trial and error” for selection of catheter it is a
useful strategy to manipulate the wire inside the root with
guiding catheter directed towards the ostium so that wire
enters the culprit artery especially in the setting of primary
PCI. The guiding catheter can be engaged over the coronary
guide wire for the subsequent procedure. This saves time and
Fig. 5 e Occluded RCA delineated with JL catheter.
Fig. 6 e Skilled manipulation resulting in wire in the RCA
without guiding catheter support.
Fig. 7 e 2 3 8 mm TREK balloon dilatation.
Fig. 8 e Result of post balloon dilatation.
a p o l l o m e d i c i n e x x x ( 2 0 1 4 ) 1e4 3
Please cite this article in press as: Kulkarni A, Ramesh B, Primary PCI in anomalous coronary: Wire first approach, ApolloMedicine (2014), http://dx.doi.org/10.1016/j.apme.2014.05.005
can affect the outcome of the therapeutic procedure. To our
knowledge this technique of wiring the culprit artery without
engaging the ostium is not reported earlier.
3. Conclusion
The possibility of an anomalous coronary being the culprit
artery should be considered when selective cannulation is not
possible. Aortogram should be performed early to visualize
the artery. Information from electrocardiography and echo-
cardiogram is crucial and should be integrated to identify the
culprit artery and to look for the anomalous course. Long runs
during angiography to identify collaterals cannot be over-
emphasized. Skilled manipulation of the coronary guide wire
in the root to pass the wire into culprit artery and subsequent
engagement by guiding might save time compared with trial
and error method for selection of guiding catheter especially
in ACS situations. CT coronary angiogram is not a useful
method in ACS of anomalous coronary artery as it doesn’t
have a therapeutic role.
Conflicts of interest
The author has none to declare.
r e f e r e n c e s
1. Angelini P. Coronary artery anomaliesecurrent clinicalissues: definitions, classification, incidence, clinicalrelevance, and treatment guidelines. Tex Heart Inst J. 2002;29:271e278.
2. Lee Jung-Jin, Kim Dae-Hyeok, Byun Sung-Su. A case of acutemyocardial infarction with the anomalous origin of the rightcoronary artery from the ascending aorta above the left sinusof valsalva and left coronary artery from the posterior sinus ofvalsalva. Yonsei Med J. 2009;50(1).
3. Hutchins GM, Miner MM, Boitnott JK. Vessel caliber andbranch-angle of human coronary artery branch-points. CircRes. 1976;38:572e576.
4. Liu LB, Richardson T, Taylor CB. Atherosclerotic occlusions inanomalous left circumflex coronary arteries. A report of 2unusual cases and a review of pertinent literature. ParoiArterielle. 1975;3:55e59.
5. Charney R, Spindola-Franco H, Grose R. Coronary angioplastyof anomalous right coronary arteries. Cathet Cardiovasc Diagn.1993;29:233e235.
6. Yip H, Chen MC, Wu CJ. Primary angioplasty in acute inferiormyocardial infarction with anomalous-origin right coronaryarteries as infarct-related arteries: Focus on anatomic andclinical features, outcomes, selection of guiding cathetersand management. J Invasive Cardiol. 2001;13:290e297.
7. Praharaj TK, Ray G. Percutaneous transluminal coronaryangioplasty with stenting of anomalous right coronaryartery originating from left sinus of valsalva using the Vodaguiding catheter: a report of two cases. Indian Heart J. 2001;53:79e82.
8. Ng W, Chow WH. Successful angioplasty and stenting ofanomalous right coronary artery using a 6 French Left Judkins#5guide catheter. J Invasive Cardiol. 2000;12:373e375.
Fig. 9 e End result with TIMI III flow.
a p o l l o m e d i c i n e x x x ( 2 0 1 4 ) 1e44
Please cite this article in press as: Kulkarni A, Ramesh B, Primary PCI in anomalous coronary: Wire first approach, ApolloMedicine (2014), http://dx.doi.org/10.1016/j.apme.2014.05.005

Apollo hospitals: http://www.apollohospitals.com/Twitter: https://twitter.com/HospitalsApolloYoutube: http://www.youtube.com/apollohospitalsindiaFacebook: http://www.facebook.com/TheApolloHospitalsSlideshare: http://www.slideshare.net/Apollo_HospitalsLinkedin: http://www.linkedin.com/company/apollo-hospitalsBlog:Blog: http://www.letstalkhealth.in/