primary open angle glaucoma – surgical management
TRANSCRIPT

POAG – Surgical management
Vinaykumar .S. AppannavarRoll no: 90

Argon laser (ALT) Diode laser (DLT) Selective laser (SLT)
It is done in patients where IOP is uncontrolled despite maximal tolerated medical therapy
Where there is non-compliance to medical therapy it can be used
Laser trabeculoplasty

Technique and role of (ALT) or (DLT) Its hypotensive effect is caused by the producing collagen
shrinkage on inner aspect of trabecular meshwork and opening the inter trabecular spaces
Its been shown to lower IOP by 8-10 mm of hg in patients – on medical therapy IOP by 12-16 mm of hg in patients – not on medical therapy
it consists of 50 spots on the anterior half of trabecular meshwork over
180 deg.
Treatment regime

Transient acute rise of IOP , which can be prevented by pretreatment with apraclonidine and/or acetazolamide
Transient inflammation which can be lessened by use of topical steroids for 3-4 days
Other complications seen less commonly are haemorrahage , uveitis, peripheral anterior synechiae and reduced accommodation
Complications
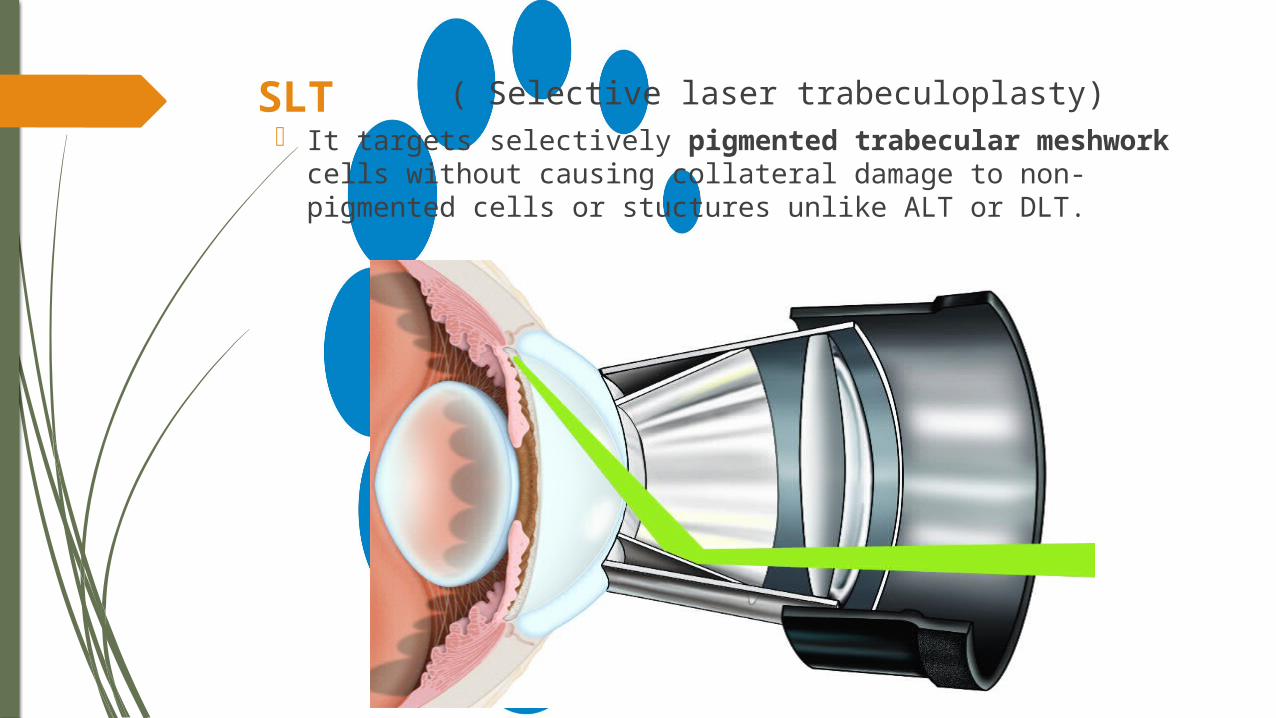
( Selective laser trabeculoplasty) It targets selectively pigmented trabecular
meshwork cells without causing collateral damage to non-pigmented cells or stuctures unlike ALT or DLT.
SLT

ND:YAG Laser
• Pressure lowering effect of SLT is similar to ALT with the advantage of not causing damage and scarring to TM
• Further, it can be used in patients treated with ALT
SLT is performed using Q- switched frequency doubled 532nm ND:YAG laser with a pulse duration of 3 ms a spot size of 400 microns and 0.8mJ energy

Indications : Uncontrolled glaucoma despite of maximal medical
therapy & laser trabeculoplasty Noncompliance of medical therapy & non availability
of ALT/ SLT Failure of medical therapy & unsuitable for ALT/SLT Eyes with advanced disease , i.e., having very high
IOP, advanced cupping & advanced field lossTypes : It primarly consists of a fistulizing surgery
o Trabeculectomy .o Filtration operations
Surgical therapy
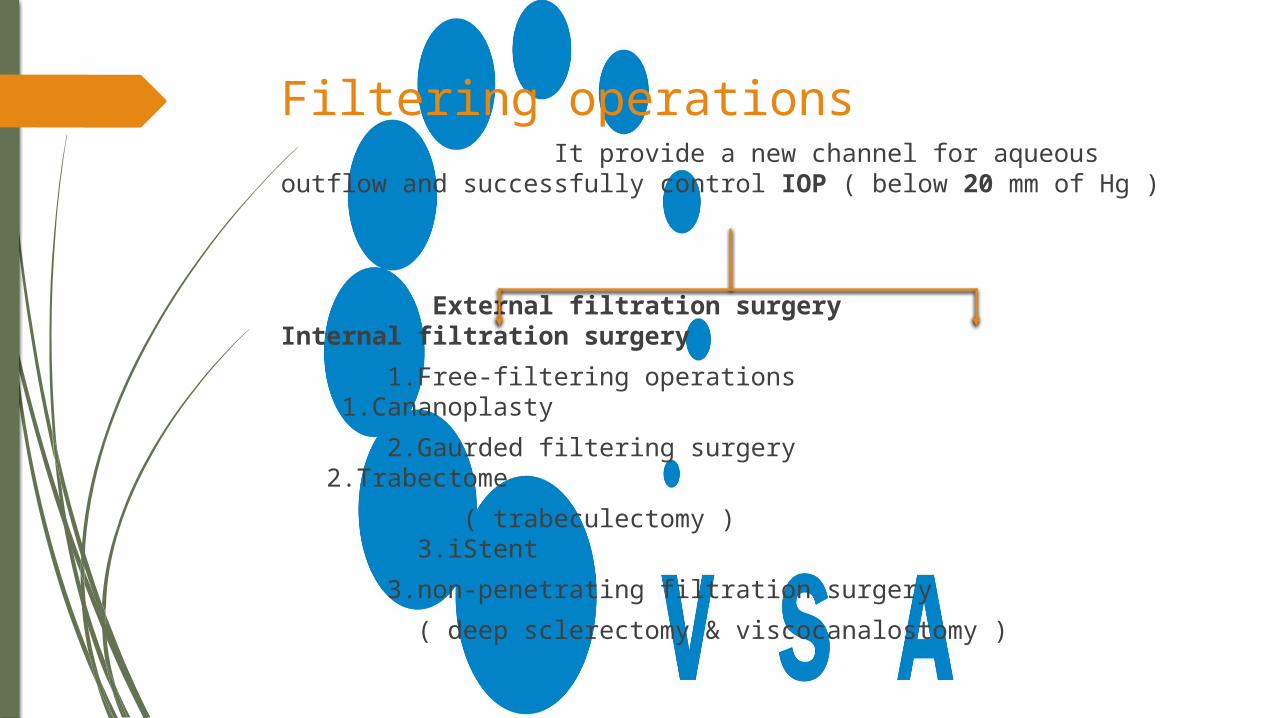
Filtering operations It provide a new channel for aqueous outflow and successfully control IOP ( below 20 mm of Hg )
External filtration surgery Internal filtration surgery 1.Free-filtering operations 1.Cananoplasty 2.Gaurded filtering surgery 2.Trabectome ( trabeculectomy ) 3.iStent 3.non-penetrating filtration surgery ( deep sclerectomy & viscocanalostomy )

Trabeculectomy Indications : Primary open-angle glaucoma Primary angle-closure glaucoma with anterior
synechial involving more than 270 deg. angle or where PI and medical treatment fail
Congenital and developmental glaucomas Secondary glaucomasMechanisms of filtration : A new channel is created around the margin of scleral
flap through which aqueous flow from anterior chamber subconjuctival space
If the tissue is dissected posterior to scleral spur, a cyclodialysis may be produced leading to increased uveoscleral outflow
Aqueous flows through the cut ends of Schlemm’s canal, now it is established that this mechanism has negligible role

Surgical technique
Initial steps of anaesthesia, cleansing, draping ,exposure of eyeball and fixation with superior rectus suture Conjunctival flap , a fornix based conjunctival flap is fashioned and the underlying sclera is exposed. Scleral flap , a partial thickness limbal based scleral flap of 5mm*5mm size is reflected down towards the cornea Excision of trabecular tissue, a narrow strip of the exposed
deeper sclera near the cornea containing the Schlemmn canal and trabecular meshwork
Peripheral iridectomy

Closure, the scleral flap is replaced and 10-0 nylon sutures are applied then the conjunctival flap is reposited with or continuous suture
Subconjunctival injections of dexmethasone and gentamycin are given
Patching

Complications Postoperative shallow anterior chamber, hyphaema, iritis,
cataract due to accidental injury to the lens and endopthalmitis
Use of antimetabolites Any of the following risk factors for the failure of conventional trabeculectomy are present Previous failed filtration surgery Glaucoma in aphakia Secondary glaucomas Patients treated with topical antiglaucoma medications Chronic cicatrizing conjunctival inflammation

Antimetabolite agents Either 5- fluorouracil or mitomycin -C can be used A sponge soaked in 0.02% solution of mitomycin –C is
placed at the site of filtration b/w the scleral and Tenon’s capsule of two minutes, followed by a thorough irrigation with balanced salt solution
Use of collagen implant with glaucoma filtration surgery
Technique: Usually a 6mm diameter and 1mm thick implant is sutured over the scleral flap.

Deep sclerectomy
Viscocanalostomy
Non-penetrating filtration surgeries
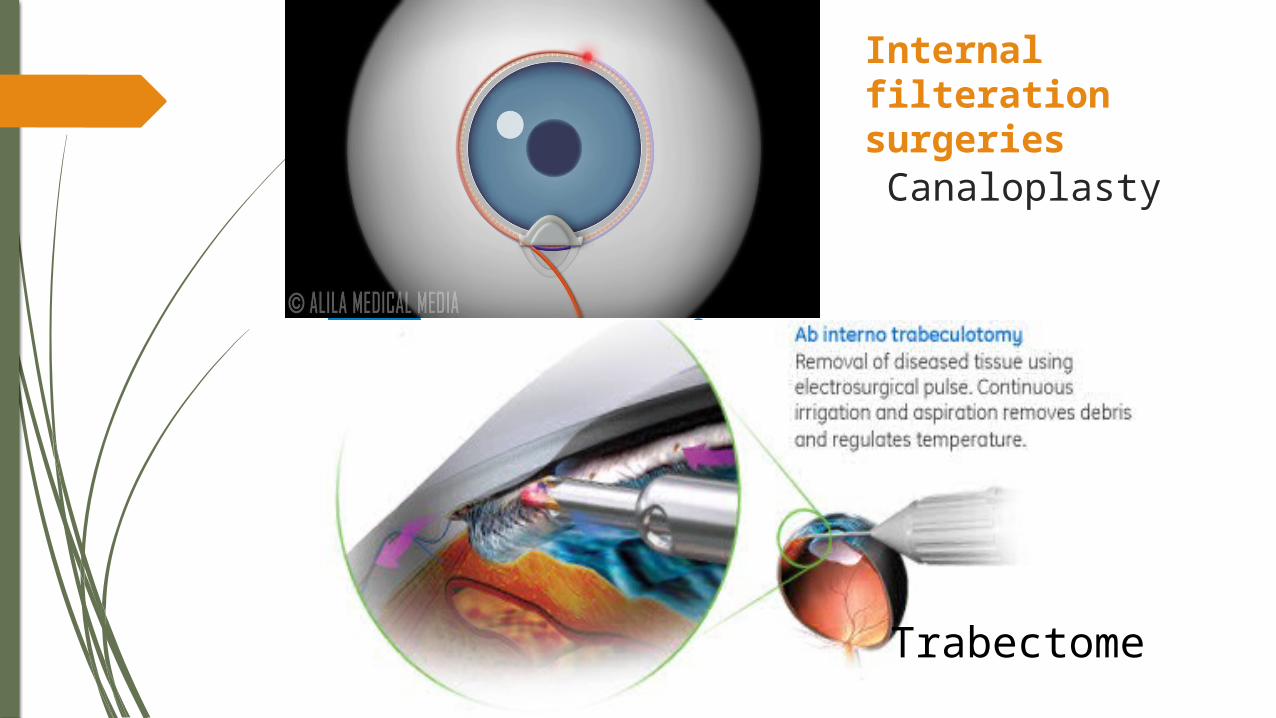
Canaloplasty
Trabectome
Internal filteration surgeries
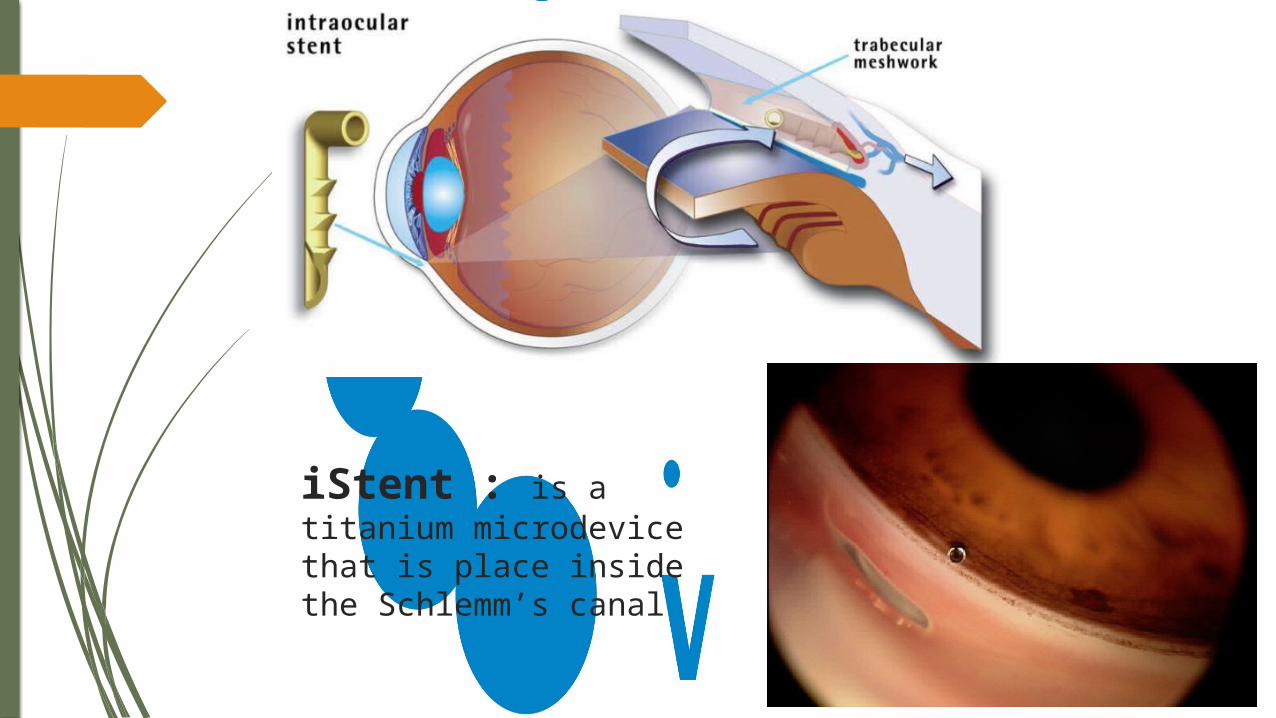
iStent : is a titanium microdevice that is place inside the Schlemm’s canal