primary koch's infection 2
TRANSCRIPT

I. INTRODUCTION
The joke is that you are not a Filipino if you do not have a TB. It might sound
amusing but it gives you a glimpse of how prevalent this disease is. In the late 1990’s,
the Philippines was fourth in the world for the number of cases of tuberculosis, and had
the highest number of cases per head in South East Asia. Today, there has been some
improvement but a lot still need to be done. Among the 22 countries in the world
accounting for 80 percent of TB worldwide, the Philippine is now ranked no. 9. Almost 75
of Filipinos die everyday because of TB. Almost everyone gets vaccinated with BCG as
a child, and yet, this does not ensure that you will develop TB later. Is the Direct
Observe Treatment Strategy (DOTS) working? To a certain extent yes, and only if those
with symptoms consult immediately. The problem is that most Filipinos ignore their
symptoms, continue to roam around and spread the infection, and consult only when
there is blood coming out when they cough. Also, over the years, no one has developed
a better vaccine and a better class of drugs against this infection. Meanwhile, the multi
drug resistance capability of the organism due to mutation continues to progress.
Primary Koch’s infection or primary tuberculosis is defined as infection of an
individual lacking previous contact with or immune responsiveness to tubercle bacilli. In
primary lung infection, a single lesion (known as Ghon’s focus) is usually found
immediately subjacent to the pleura in the lower part of the upper lobes or upper part of
the lower lobes of one lung, rarely elsewhere. These localizations reflect the areas
receiving the greatest volume flow of inspired air.
Although tuberculosis is now both treatable and to some degree preventable,
still, it is one of the bacterial infection affecting worldwide. Its true incidence cannot be
precisely determined because (1) only a fraction of persons with M. Tuberculosis
manifest clinical disease at anyone time; (2) all infected persons remain indefinitely at
risk of developing active disease; and (3) case reporting, even in developed countries, is
always incomplete.
According to the World Health Organization, the Philippines rank fourth in the
world for the number of cases of tuberculosis and have the highest number of cases per
head in Southeast Asia. The Philippines is among the 22-burdened countries in the
1

world according to WHO. TB is the 6th leading cause of illness and the 6th leading cause
of deaths among Filipinos. Most TB patients belong to the economically productive age
(15-54 years old) according to the 2nd National Prevalence Survey in 1997).
In 1996, WHO introduced the Directly Observed Treatment Short Course (DOTS)
to ensure completion of treatment. The DOTS strategy depends on five elements for its
success: Microscope, Medicine, Monitoring, Directly Observed Treatment, and Political
Commitment. If any of these elements are missing, our ability to consistently cure TB
patients slips through our fingers.
MORTALITY
Ten Leading Causes of Mortality by Sex
Number, Rate/100,000 Population & Percentage
Philippines, 2003
Cause Male FemaleBoth Sexes
Number Rate Percent*
1. Heart Diseases 38,677 29,019 67,696 83.5 17.1
2. Vascular System Diseases 29,054 22,814 51,868 64.0 13.1
3. Malignant Neoplasm 20,634 18,664 39,298 48.5 9.9
4. Accidents 27,720 6,246 33,966 41.9 8.6
5. Pneumonia 15,831 16,224 32,055 39.5 8.1
6. Tuberculosis, all forms 18,367 8,404 26,771 33.0 6.8
2

7. Symptoms, signs and abnormal
clinical, laboratory findings, NEC10,740 10,623 21,363 26.3 5.4
8.Chronic lower respiratory diseases 12,998 5,907 18,905 23.3 4.8
9. Diabetes Mellitus 6,823 7,373 14,196 17.5 3.6
10. Certain conditions originating in the
perinatal period 8,397 5,725 14,122 17.4 3.6
Source: The2003 Philippine Health Statistics
*percent share from total deaths, all causes, Philippines
Last Update: January 11, 2007
MORBIDITY
TEN LEADING CAUSES OF MORBIDITY
No. & Rate/100,000 Population
PHILIPPINES, 2003
CAUSEMALE FEMALE BOTH SEXES
Rate** Rate** Number Rate*
1. Acute Lower RTI and Pneumonia 770.9 748.2 674,386 861.2
2. Diarrheas 695.0 655.0 615,692 786.2
3. Bronchitis/Bronchiolitis 639.6 677.0 604,107 771.4
3

4. Influenza 455.4 503.1 431,216 550.6
5. Hypertension 325.4 420.7 325,390415.5
6. TB Respiratory 126.4 84.0 92,079 117.9
7. Heart Diseases 28.8 29.2 30,398 38.8
8. Malaria 41.1 30.4 28,549 36.5
9. Chickenpox 30.3 30.4 26,137 33.4
10. Measles 30.2 30.4 25,535 32.6
Source: 2003 FHSIS Annual Report
** rate/100,000 of sex-specific pop.
* Total population of regions with reports only
Last Update: January 11, 2007
4

CURRENT TREND: A More Reliable Test For Latent TB
Two new interferon-gamma blood test assays to detect latent tuberculosis
infection (LTBI) showed customers were exposed to a supermarket employee in Holland
who had smear-positive tuberculosis, while traditional tuberculin skin tests (TST) did not,
according to a large contact study.
Ailko Bossink, M.D., Ph.D., of the Department of Pulmonology at
Diakonessenhuis Utrecht in The Netherlands, and eight associates recruited 785
supermarket customers who had not received BCG vaccine against tuberculosis, the
immunizing agent prepared from Calmette-Guéren bacillus. TST results are not accurate
in those vaccinated with BCG.
All individuals in the study cohort were recruited from over 20,000 customers who
had shopped at the supermarket for more than 10 months. Many had numerous contacts
with the infected employee, who had been contagious since February 2004. The large-
scale contact investigation began in January 2005.
For the study, researchers selected 469 customers randomly on the day that
their TST was administered and 316 with a TST result of more than 0 mm.
TSTs are based on a skin reaction to injection, scratching or puncturing the skin with a
purified protein derivative of tuberculosis bacterium. Swelling and redness indicate a
positive result.
"Among the 785 study participants, TST results were associated with age,
whereas positive interferon-gamma blood test assay results were significantly
associated with cumulative shopping time," said Dr. Bossink. "TST results were not
associated with any measure of exposure to the index case in the supermarket."
The researchers noted that positive TST responses largely reflected delayed
type hypersensitivity due to remote infection with M. tuberculosis acquired before the
source case at the supermarket became infectious.Among the 759 shoppers who had
valid results from both interferon-gamma blood assay, slightly over 80 percent (608)
were concordant negative with both blood tests, while 72 were concordant positive and
79 were discordant. Overall agreement between the two tests was 89.6 percent.
5

"Notably, positive interferon-gamma blood assays were observed in a significant
proportion of recently exposed contacts with a negative TST result," he added. "The
clinical significance of this finding merits further study if the blood tests are to replace the
TST and be used for therapeutic decisions."
"The key question is whether the two new IGRAs are better than the TST in
predicting the development of TB disease, and thus identifying persons who will benefit
most from latent TB infection (LTBI) therapy. There is abundant evidence, from
numerous large-scale cohorts and randomized trials, regarding the prognosis of
untreated persons with positive TST results; this remains the greatest advantage of the
TST."
"What is urgently needed is similar longitudinal studies of cohorts who have been
tested with IGRA (ideally both IGRAs) and the TST," they continued. "However, in
almost all low-incidence, high-income countries, it would be ethically impossible not to
treat persons with evidence of LTBI. Moreover, in high-incidence countries, where
treatment of LTBI is not the current standard of care, it would seem unethical to test for a
condition without plans to offer appropriate treatment."
"However, this should not be a problem. Almost everyone would agree that
individuals with concordant positive TST and IGRA are likely to have LTBI and they will
never inform the question as to which test predicts active TB better. Thus, such patients
can and should be managed appropriately. However, individuals with discordant results
(TST+/IGRA- or vice versa) will be informative regarding the risk of development of
active disease without treatment. In addition, because the clinical interpretation, and
therefore management is unclear for persons with such discordant results, equipoise
exists. Therefore, close observation without treatment is reasonable and ethical."
Reference: ScienceDaily (Mar. 15, 2007) — Second issue for March 2007 of the
American Journal of Respiratory and Critical Care Medicine, published by the American
Thoracic Society. Adapted from materials provided by American Thoracic Society.
6

Summary:
These new interferon gamma blood test assays used to detect latent tuberculosis
infection are still under studies and it has not yet been approved except for one, known
as Quantiferon-TB Gold. Although the interferon-gamma blood tests are now considered
more specific and show a better correlation with exposure than tuberculin skin testing, it
has not been demonstrated whether they provide a valid basis for therapeutic decisions
regarding treatment. If studies conclude the efficacy and efficiency of these interferon
gamma blood tests, we would be able to avoid false-negative results given by tuberculin
skin testing thus making it easier for health care workers to do case finding measures
and tracing of those who are exposed to the disease. But problems may also arise with
these new discoveries in terms of its availability and affordability especially here in our
country. We just hope that these new tests would be able to detect latent tuberculosis
without completely phasing out the traditional tuberculin skin testing in order for patients
to have an option in which test would be more convenient for them since these new test
would surely be expensive.
Reason for choosing study
I decided to choose this case, because I wanted to acquire more knowledge
about Koch’s Infection and to use the knowledge I have acquired in promoting
awareness to the people especially to the poor that they should seek for medical care in
order to prevent the development and progression of the disease. I also wanted to focus
on preventive measures. This can cause Tuberculosis Meningitis, a very rare and fatal
disease and I would not want that to happen, so I will focus more on information
campaign as part of primary prevention of health, presently our country has so many
cases in Koch’s Infection. This study will help the nursing profession by providing
information about the proper management and care for patient. It will also educate the
people and vulnerable individuals to seek medical care in order to prevent TBM. It will
increase awareness about the importance of having a healthy life style and clean
environment
7

OBJECTIVES
1. NURSE-CENTERED
After the completion of the study, the nurse researcher shall be able to:
Perform a comprehensive assessment of the patient
Enumerate the signs and symptoms of Koch’s Infection
Identify and list diagnostic procedures that would help in the diagnosis of Koch’s
Infection
Identify nursing problems utilizing the subjective and objective cues based on the
patient’s response
Perform appropriate therapeutic interventions for each of the formulated nursing
diagnosis
Have a background of the disease condition
Known the current trends about the disease
Know the incidence, prevalence and mortality rate of the disease
Identify factors present to the patient that predisposed him to the said disease
Explain briefly the anatomy and physiology of the disease
Gain proper knowledge and understanding about the existing disease condition,
it’s pathophysiology, sociology and etiology involved in its acquisition and
progression
Identify the difference modifiable and non-modifiable factors for the occurrence of
the disease
Identify the different early clinical manifestations of the disease condition
Analyze the different laboratory and diagnostic procedures, their indications to
the disease and identify the nursing interventions before, during and after the
performance of the said procedures
Identify the different signs and symptoms manifested by the client who have had
Koch’s Infection and explain how these signs and symptoms occur
Identify the common complications of Koch’s Infection and the appropriate
preventive measures
Explain the different treatments or medical modalities and their importance, and
different nursing interventions during the performance of the said procedure
8

Identify common medications used as a treatment for the diseases, their
mechanism of action, adverse affects and nursing interventions before, during
and after the administration of the medications, appropriate nursing diagnoses
and their corresponding effects for the disease conditions
Render appropriate nursing interventions to prevent complications of the disease.
2. CLIENT-CENTERED
Have a background of the disease condition ( Koch’s Infection )
Know the reasons why such diagnostic procedures and treatments are
performed
Know the progress of the disease
Cooperate in the necessary medical and nursing interventions
Know the reasons why the patient experiences the signs and symptoms of the
diseases
Know preventive measures in response to the disease so as to prevent
deterioration of the patient’s condition
Participate willingly in the care of his conditions such as adhering to health
teachings provided
Have the necessary awareness for the condition’s familial tendency and thus
perform appropriate activities that may prevent eventual progress of the disease
(for the client’s significant others).
II. NURSING ASSESSMENT
9

A. PERSONAL HISTORY
1. Demographic data
Baby M is 1 year old at the time of assessment, male Filipino, who was born on
November 31, 2008 via Normal Spontaneous Home delivery in district hospital of
Pampanga. He’s the only child of Papa PJ and Mama KC and devout members of the
Roman Catholic. They’ve been married for three years now. Papa PJ is a tricycle driver
and Mama KC is a plain housewife. Papa PJ loves to play “Tong-its” and bets to
cockfights when he has extra money. They prefer to sit and watch TV during the night.
Baby M was admitted at the hospital in Pampanga last December 19, 2009; with a chief
complain of difficulty in breathing and an impression and admitting diagnosis of T/C
Pneumonia. He was discharged last December 26, 2009 with a final diagnosis of Koch’s
Infection.
2. Socio-Economic & Cultural Factors
Papa PJ finished grade VI at a public school in Pampanga, being a tricycle
driver, he earns P250/day. Papa PJ provides the needs of Baby M. Baby M’s
grandparents on his father side also give financial support for their needs. Mama KC is
the one who does the shopping and cooking. Baby M usually eats “lugaw” for his
breakfast. For lunch and dinner, he prefers eating rice with soup broth. In between
meals, Baby M is being milk fed. He was just breast fed for about two months. On usual
day he has crackers, biscuits for his snack. Baby M prefers crackers, biscuits, fruits like
apple and orange and for his main meals; he prefers rice with soup broth. Baby M is still
on milk feeding, he also drinks fruit juices. Since Baby M is just 1 year old, mother and
other SO’s take care of him and assist him in his activities of daily living like eating,
bathing, dressing and grooming. He passes stool twice a day and around 4 diaper
changes a day. Usually he sleeps at 9 pm and wakes up at 6 am in the morning. He
usually sleeps 8-9 hours their source of water came from water district and pitcher
pump. They believe in herbolaryo and manghihilot, used herbal medicines such as
Lagundi for cough and colds.
3. Environmental Factors
10

Baby M with his parents and grandparents on his father side live in a two-storey
house made of concrete and wood. There are about 12 steps to reach the upper portion
of the house. He and his mother usually spend their time in their bedroom located at the
second floor. Mother sees to it that the door in their bedroom is always close for safety.
They have pail flush toilet located at the back of their house. Their drainage is open and
flowing, unsanitary because of the presence of debris. Use plastic bag for garbage
disposal and throw their garbage in their compost pit located at their backyard, use
mosquito net when they sleep, use physical force t kill rodents.
B. GROWTH AND DEVELOPMENT
STAGE
Infancy and childhood
DEVELOPMENTAL CRISIS
Trust vs. Mistrust
1 year
Motor
: Walks with one hand held
: Stands alone and with support
: Grasps bottle in one hand
Language
: Uses “mama” with specific meaning
: Has vocabulary of two words besides mama and dada
Cognitive
: Obeys simple requests such as “kiss mama”
Personal social adaptive
: Points with index finger
: Releases toy into your hand
11

: Holds cup to drink
: Gives affection
C. FAMILIAL-HEALTH ILLNESS HISTORY
Based on the diagram, parents of Mama KC are both healthy. They do not
manifest any disease condition. Father of Papa PJ has history of PTB, asthma and is a
smoker. Mother of Papa PJ is said to be healthy. Baby M currently has Primary Koch’s
infection.
LEGEND:
- healthy
12
Lolo Diego54 y/o
Lolo Popoy57 y/o
Lola Babes45 y/o
Mama KC20 y/o
Lola Basha53 y/o
Papa PJ22 y/o
Baby M1 y/o

- w/ asthma, history of PTB, Smoker
- w/ asthma, smoker
- w/ Primary Koch’s infection
D. HISTORY OF PAST ILLNESS
Baby M had received vaccinations for BCG, Hepatitis B, DPT, OPV, and Measles.
Vaccines for Varicella, Anti-flu, and Hepatitis A are not yet given. The most common
illnesses Baby M had experienced were colds, cough, and fever. During these
conditions, parents resorted to over the counter medications sometimes they used
herbal medicines such as Lagundi for cough and colds. Baby M’s first hospitalization
was when he was 3 months old because of convulsion due to high fever. SO cannot
remember what medications were given during Baby M’s first hospitalization. Present
hospitalization is Baby M’s second. Baby M has no allergy to any medications or food.
Current medications were Salbutamol nebule given in a pediatrician’s clinic.
E. HISTORY OF PRESENT ILLNESS
Two days prior to admission, Baby M experienced cough and colds. One day
prior to admission, Baby M with SO consulted a pediatrician due to persistent cough and
colds. Nebulization with Salbutamol 1 nebule was provided in the pediatrician’s clinic.
But there was no relief of cough and colds, so few hours prior to admission, Baby M with
SO consulted again the pediatrician. Nebulization with Salbutamol 2 nebules was given
30 minutes apart. Baby M experienced difficulty of breathing and therefore was brought
to the emergency room of a public secondary hospital. Upon assessment, Baby M had
(+) Crackles on bilateral lung fields and attending physician ordered for the admission of
Baby M.
13

F. PHYSICAL EXAMINATION
Upon Admission (December 19, 2009)
(Lifted from the chart)
Vital Signs: T= 36.2, CR= 132 bpm, RR= 30 bpm
Weight: 9 kg
General Appearance:
HEENT: pale palpebral conjunctiva, anicteric sclerae, moist buccal mucosa
Chest: symmetrical chest expansion, (-) retraction, with effort respiration and use of
accessory muscles when breathing
Cardio: adynamic precordium, tachycardia, (-) murmur
Abdominal: flat, soft, non-tender, no organomegally
Chief complaint: DOB
Nurse-Patient Interaction
Sunday, December 20, 2009
VITAL SIGNS:
Temperature -36.6°C, Respiratory Rate- 29 bpm
Heart Rate- 128 bpm
GENERAL SURVEY
The patient is conscious and coherent. The patient lies comfortably on the bed in
a semi-Fowlers position. There was full mobility of the body and movements are
coordinated. He was wearing a blue shirt with white print and pajamas. Patient was
generally clean and well-groomed. Patient’s nails were short and clean. No body odor
was noted. He was able to maintain eye contact and was cooperative to the nurse.
Skin
14

The color of the skin is light brown with no lesions; the temperature of the skin is
uniform. Epidermis appears uniformly thin over most of the body with equal distribution
of hair, the skin had a poor skin turgor with none tenderness.
Hair
The hair is evenly distributed to the body. Scalp hair is also evenly distributed and there
were no patches of hair loss noted. Hair color was black .There were no lice, sores and
dandruff noted.
Nails
The nail surfaces were convex and show no abnormalities. The nails showed pale nail
beds and have a capillary refill time of 2 seconds.
Head
Skull and Face
The skull was normocephalic and there were no tenderness, nodules or masses noted
upon palpation. Has symmetric facial features, no abnormalities noted such as
periorbital edema.
Eyes
The hair in eyebrows are distributed evenly and eyebrows are symmetrically aligned,
and have no scaling or lesions; the skin of the eyelids was intact without redness,
swelling, discharge or lesion and eyelashes were equally distributed along the lid
margins and curve outward. No protrusion or sunken appearance. The conjunctiva was
smooth and moist. Visual Acuity, Extra Ocular movement and Visual field are not
applicable due to his age.
Ears
The ears are equal in size with no swelling or thickening; skin color of the auricles is
consistent with the patient’s facial skin color. The skin is intact with no lumps or lesions;
there was no pain claimed by the patient when the pinna was palpated. Both pinnas
15

recoiled immediately when tested for elasticity. The patient was able to hear whispered
words to both ears.
Nose
The nose is in the midline, and in proportion to other facial features; No deformity,
asymmetry, inflammation, or skin lesions noted. There was no swelling, discharge or
bleeding noted upon inspection.
Mouth
The lips are pinkish in color. No cracking or lesions noted. Gums are pinkish in color,
teeth are white and 8 teeth were intact. No swelling or bleeding was noted. The tongue
is pink and even. Located at the midline, no ulceration found, symmetrical and moves
freely there were no inflammed tonsils noted.
Neck
The head is positioned at the midline, the accessory muscles are symmetrical and the
head was held erect and still.The trachea is in the midline position, no inflammation of
cervical lymph nodes and thyroid glands. There was no pain and limitation during the
active motion. There was no bruit upon auscultation.
Breast
The skin is smooth and even in color. No redness, bulging, edema, dimpling, or
discoloration was noted on the area of both breasts and the axillary areas. The nipples
are symmetrical, everted, and brown in color. No ulceration, bleeding or discharge and
there are no palpable nodes noted in the entire region of the breasts and the axilla.
Chest
The chest is symmetrical, no lesions found, no shallow breathing, no sign of deformities,
no presence of mass, no sign of abnormalities, no resonant sound. Positive rales or
crackles upon auscultation.
Heart
Patient has adynamic precordium and normal rate and regular rhythm of the heart. No
bruit and murmurs heard upon auscultation.
16

Abdomen
The skin is unblemished and uniform in color; there are no rashes or striaes noted. Flat
abdomen and is symmetric in contour; Umbilicus is at the midline, inverted, with no sign
of discoloration, inflammation or herniation. Bowel sound are normal which range from 5
to 10, high pitched and gurgling. Tympany over the stomach and gas-filled bowels.
Dullness is heard over liver and spleen.
Examination of extremities
Upper Extremities
Symmetrical in shape with no signs of deformities.
Lower Extremities
Symmetrical in shape with no presence of edema, lesions, and tenderness, can walk
with one hand held.
Nurse-Patient Interaction
Monday, December 21, 2009
VITAL SIGNS:
Temperature -36.5°C, Respiratory Rate- 27 bpm
Heart Rate- 125 bpm
GENERAL SURVEY
The patient is conscious and coherent. He was able to smile and respond
actively. The patient lies comfortably on the bed in a supine position. There was full
mobility of the body and movements are coordinated. He was wearing a blue shirt with
white print and pajamas. Patient was generally clean and well-groomed. Nails were short
and clean. With a slight odor of sweat was noted. He was able to maintain eye contact
and was cooperative to the nurse.
Skin
17

The color of the skin is light brown with no lesions; the temperature of the skin is
uniform. Epidermis appears uniformly thin over most of the body with equal distribution
of hair, the skin had a poor skin turgor with none tenderness.
Hair
The growth of hair is straight evenly distributed. Hair color was black .There were no
sores and dandruff and no infestations of lice noted.
Nails
The nail surfaces were convex and show no abnormalities. The nails are short and dirty
with no clubbing upon assessment and have a capillary refill time of 2-3 seconds.
Head
Skull and Face
The skull was normocephalic and there were no tenderness, nodules or masses noted
upon palpation. Has symmetric facial features, no abnormalities noted such as
periorbital edema.
Eyes
Eyebrows and eyelashes are equally distributed, eyebrows are black, the skin of the
eyelids was intact without redness, swelling, discharge or lesion and eyelashes were
equally distributed along the lid margins and curve outward. No protrusion or sunken
appearance. The conjunctiva was smooth and moist. Visual Acuity, Extra Ocular
movement and Visual field are not applicable due to his age.
Ears
The ears are equal in size with no swelling or thickening.The auricles are symmetrical
and have the same color as facial skin. Presence of minimal cerumen noted at the
external ear canal. Parallel to the inner canthus of the eye upon inspection. Pinna recoils
after it is folded
Nose
18

With symmetric nares, has no discharge and uniform in color. He breathes through both
nares. Nasal septum intact and at the midline. No tenderness and lesions noted upon
inspection and palpation. No nasal discharge.
Mouth
The lips are pinkish in color. No cracking or lesions noted. Gums are pinkish in color,
teeth are white and 8 teeth were intact. No swelling or bleeding was noted. The tongue
is pink and even. Located at the midline, no ulceration found, symmetrical and moves
freely there were no inflamed tonsils noted.
Neck
Neck is straight, head centered. He is able to move it without difficulty or discomfort. No
masses or lumps noted.
Breast
The skin is smooth and even in color. No redness, bulging, edema, dimpling, or
discoloration was noted on the area of both breasts and the axillary areas. The nipples
are symmetrical, everted, and brown in color. No ulceration, bleeding or discharge and
there are no palpable nodes noted in the entire region of the breasts and the axilla.
Chest
The chest is symmetrical, no lesions found, no shallow breathing, no sign of deformities,
no presence of mass, no sign of abnormalities, no resonant sound. Positive rales or
crackles upon auscultation.
Heart
Patient has adynamic precordium and normal rate and regular rhythm of the heart. No
bruit and murmurs heard upon auscultation.
Abdomen
Patient’s skin in the abdomen is uniform in color. There are no lesions and tenderness
noted when palpated. With audible bowel sounds.
19

Examination of extremities
Upper Extremities
Symmetrical in shape with no signs of deformities.
Lower Extremities
Symmetrical in shape with no presence of edema, lesions, and tenderness, can walk
with one hand held.
Nurse-Patient Interaction
Tuesday, December 22, 2009
VITAL SIGNS:
Temperature -36.4°C, Respiratory Rate- 28 bpm
Heart Rate- 124 bpm
GENERAL SURVEY
The patient is conscious and coherent. He was able to smile and respond
actively. The patient lies comfortably on the bed in a supine position. There was full
mobility of the body and movements are coordinated. He was wearing a red shirt with
black print and shorts. Patient was generally clean and well-groomed. Nails were short
and clean. No body odor was noted. He was able to maintain eye contact and was
cooperative to the nurse.
Skin
The color of the skin is light brown with no lesions, the temperature of the skin is
uniform. Epidermis appears uniformly thin over most of the body with equal distribution
of hair, the skin had a poor skin turgor with none tenderness.
Hair
20

The hair is evenly distributed to the body. Scalp hair is also evenly distributed and there
were no patches of hair loss noted. Hair color was black .There were no lice, sores and
dandruff noted.
Nails
The nail surfaces were convex and show no abnormalities. The nails showed pale nail
beds and have a capillary refill time of 2 seconds.
Head
Skull and Face
The skull was normocephalic and there were no tenderness, nodules or masses noted
upon palpation. Has symmetric facial features, no abnormalities noted such as
periorbital edema.
Eyes
The hair in eyebrows are distributed evenly and eyebrows are symmetrically aligned,
and have no scaling or lesions; the skin of the eyelids was intact without redness,
swelling, discharge or lesion and eyelashes were equally distributed along the lid
margins and curve outward. No protrusion or sunken appearance. The conjunctiva was
smooth and moist. Visual Acuity, Extra Ocular movement and Visual field are not
applicable due to his age.
Ears
The ears are equal in size with no swelling or thickening; skin color of the auricles is
consistent with the patient’s facial skin color. The skin is intact with no lumps or lesions;
there was no pain claimed by the patient when the pinna was palpated. Both pinnas
recoiled immediately when tested for elasticity. The patient was able to hear whispered
words to both ears.
Nose
21

The nose is in the midline, and in proportion to other facial features; No deformity,
asymmetry, inflammation, or skin lesions noted. There was no swelling, discharge or
bleeding noted upon inspection.
Mouth
The lips are pinkish in color. No cracking or lesions noted. Gums are pinkish in color,
teeth are white and 8 teeth were intact. No swelling or bleeding was noted. The tongue
is pink and even. Located at the midline, no ulceration found, symmetrical and moves
freely there were no inflamed tonsils noted.
Neck
The head is positioned at the midline, the accessory muscles are symmetrical and the
head was held erect and still. The trachea is in the midline position, no inflammation of
cervical lymph nodes and thyroid glands. There was no pain and limitation during the
active motion. There was no bruit upon auscultation.
Breast
The skin is smooth and even in color. No redness, bulging, edema, dimpling, or
discoloration was noted on the area of both breasts and the axillary areas. The nipples
are symmetrical, everted, and brown in color. No ulceration, bleeding or discharge and
there are no palpable nodes noted in the entire region of the breasts and the axilla.
Chest
The chest is symmetrical, no lesions found, no shallow breathing, no sign of deformities,
no presence of mass, no sign of abnormalities, no resonant sound. Positive rales or
crackles upon auscultation.
Heart
Patient has adynamic precordium and normal rate and regular rhythm of the heart. No
bruit and murmurs heard upon auscultation.
Abdomen
22

The skin is unblemished and uniform in color; there are no rashes or striaes noted. Flat
abdomen and is symmetric in contour; Umbilicus is at the midline, inverted, with no sign
of discoloration, inflammation or herniation. Bowel sounds are normal which range from
5 to 10, high pitched and gurgling. Tympany over the stomach and gas-filled bowels.
Dullness is heard over liver and spleen.
Examination of extremities
Upper Extremities
Symmetrical in shape with no signs of deformities.
Lower Extremities
Symmetrical in shape with no presence of edema, lesions, and tenderness, can walk
with one hand held.
Nurse-Patient Interaction
Wednesday, December 23, 2009
VITAL SIGNS:
Temperature -36.2°C, Respiratory Rate- 24 bpm
Heart Rate- 120 bpm
GENERAL SURVEY
The patient is asleep .Upon awake, was unable to smile but responsive to stimuli
and cry actively. The patient carries by his mother. There was full mobility of the body
and movements are coordinated. He was wearing a pink shirt and shorts. Patient was
generally clean and well-groomed. Nails were short and clean. No body odor was noted.
He was able to maintain eye contact.
23

Skin
The color of the skin is light brown with no lesions; the temperature of the skin is
uniform. Epidermis appears uniformly thin over most of the body with equal distribution
of hair. Skin turgor is good, when pinched it springs back to its previous state.
Hair
The hair is evenly distributed to the body. Scalp hair is also evenly distributed and there
were no patches of hair loss noted. Hair color was black .There were no lice, sores and
dandruff noted.
Nails
The nail surfaces were convex and show no abnormalities. The nails showed pale nail
beds and have a capillary refill time of 2 seconds.
Head
Skull and Face
The skull was normocephalic and there were no tenderness, nodules or masses noted
upon palpation. Has symmetric facial features, no abnormalities noted such as
periorbital edema.
Eyes
The hair in eyebrows are distributed evenly and eyebrows are symmetrically aligned,
and have no scaling or lesions; the skin of the eyelids was intact without redness,
swelling, discharge or lesion and eyelashes were equally distributed along the lid
margins and curve outward. No protrusion or sunken appearance. The conjunctiva was
smooth and moist. Visual Acuity, Extra Ocular movement and Visual field are not
applicable due to his age.
Ears
The ears are equal in size with no swelling or thickening; skin color of the auricles is
consistent with the patient’s facial skin color. The skin is intact with no lumps or lesions;
there was no pain claimed by the patient when the pinna was palpated. Both pinnas
24

recoiled immediately when tested for elasticity. The patient was able to hear whispered
words to both ears.
Nose
The nose is in the midline, and in proportion to other facial features; No deformity,
asymmetry, inflammation, or skin lesions noted. There was no swelling, discharge or
bleeding noted upon inspection.
Mouth
The lips are pinkish in color. No cracking or lesions noted. Gums are pinkish in color,
teeth are white and 8 teeth were intact. No swelling or bleeding was noted. The tongue
is pink and even. Located at the midline, no ulceration found, symmetrical and moves
freely there were no inflamed tonsils noted.
Neck
The head is positioned at the midline, the accessory muscles are symmetrical and the
head was held erect and still.The trachea is in the midline position, no inflammation of
cervical lymph nodes and thyroid glands. There was no pain and limitation during the
active motion. There was no bruit upon auscultation.
Breast
The skin is smooth and even in color. No redness, bulging, edema, dimpling, or
discoloration was noted on the area of both breasts and the axillary areas. The nipples
are symmetrical, everted, and brown in color. No ulceration, bleeding or discharge and
there are no palpable nodes noted in the entire region of the breasts and the axilla.
Chest
The chest is symmetrical, no lesions found, no shallow breathing, no sign of deformities,
no presence of mass, no sign of abnormalities, no resonant sound. Positive rales or
crackles upon auscultation.
25

Heart
Patient has adynamic precordium and normal rate and regular rhythm of the heart. No
bruit and murmurs heard upon auscultation.
Abdomen
The skin is unblemished and uniform in color; there are no rashes or striaes noted. Flat
abdomen and is symmetric in contour; Umbilicus is at the midline, inverted, with no sign
of discoloration, inflammation or herniation. Bowel sounds are normal which range from
5 to 10, high pitched and gurgling. Tympany over the stomach and gas-filled bowels.
Dullness is heard over liver and spleen.
Examination of extremities
Upper Extremities
Symmetrical in shape with no signs of deformities.
Lower Extremities
Symmetrical in shape with no presence of edema, lesions, and tenderness, can walk
with one hand held.
Nurse-Patient Interaction
Thursday, December 24, 2009
VITAL SIGNS:
Temperature -36.2°C, Respiratory Rate- 22 bpm
Heart Rate- 120 bpm
GENERAL SURVEY
The patient is conscious and coherent. He was able to smile and respond
actively. The patient lies comfortably on the bed in a supine position. There was full
mobility of the body and movements are coordinated. He was wearing a purple shirt and
26

pajamas. Patient was generally clean and well-groomed. Nails were short and clean. No
body odor was noted. He was able to maintain eye contact and was cooperative to the
nurse.
Skin
The color of the skin is light brown with no lesions; the temperature of the skin is
uniform. Epidermis appears uniformly thin over most of the body with equal distribution
of hair. Skin turgor is good, when pinched it springs back to its previous state.
Hair
The hair is evenly distributed to the body. Scalp hair is also evenly distributed and there
were no patches of hair loss noted. Hair color was black .There were no lice, sores and
dandruff noted.
Nails
The nail surfaces were convex and show no abnormalities. The nails showed pale nail
beds and have a capillary refill time of 2 seconds.
Head
Skull and Face
The skull was normocephalic and there were no tenderness, nodules or masses noted
upon palpation. Has symmetric facial features, no abnormalities noted such as
periorbital edema.
Eyes
The hair in eyebrows are distributed evenly and eyebrows are symmetrically aligned,
and have no scaling or lesions; the skin of the eyelids was intact without redness,
swelling, discharge or lesion and eyelashes were equally distributed along the lid
margins and curve outward. No protrusion or sunken appearance. The conjunctiva was
smooth and moist. Visual Acuity, Extra Ocular movement and Visual field are not
applicable due to his age.
27

Ears
The ears are equal in size with no swelling or thickening; skin color of the auricles is
consistent with the patient’s facial skin color. The skin is intact with no lumps or lesions;
there was no pain claimed by the patient when the pinna was palpated. Both pinnas
recoiled immediately when tested for elasticity. The patient was able to hear whispered
words to both ears.
Nose
The nose is in the midline, and in proportion to other facial features; No deformity,
asymmetry, inflammation, or skin lesions noted. There was no swelling, discharge or
bleeding noted upon inspection.
Mouth
The lips are pinkish in color. No cracking or lesions noted. Gums are pinkish in color,
teeth are white and 8 teeth were intact. No swelling or bleeding was noted. The tongue
is pink and even. Located at the midline, no ulceration found, symmetrical and moves
freely there were no inflamed tonsils noted.
Neck
The head is positioned at the midline, the accessory muscles are symmetrical and the
head was held erect and still. The trachea is in the midline position, no inflammation of
cervical lymph nodes and thyroid glands. There was no pain and limitation during the
active motion. There was no bruit upon auscultation.
Breast
The skin is smooth and even in color. No redness, bulging, edema, dimpling, or
discoloration was noted on the area of both breasts and the axillary areas. The nipples
are symmetrical, everted, and brown in color. No ulceration, bleeding or discharge and
there are no palpable nodes noted in the entire region of the breasts and the axilla.
Chest
The chest is symmetrical, no lesions found, no shallow breathing, no sign of deformities,
no presence of mass, no sign of abnormalities, no resonant sound. Positive rales or
crackles upon auscultation.
28

Heart
Patient has adynamic precordium and normal rate and regular rhythm of the heart. No
bruit and murmurs heard upon auscultation.
Abdomen
The skin is unblemished and uniform in color; there are no rashes or striaes noted. Flat
abdomen and is symmetric in contour; Umbilicus is at the midline, inverted, with no sign
of discoloration, There were no tenderness over the abdomen in all quadrants; relaxed
abdomen with smooth and constant tension upon light palpation. and no tenderness was
noted upon deep palpation.
Examination of extremities
Upper Extremities
Symmetrical in shape with no signs of deformities. The skin color in hands is uniform in
color, no redness or discolorations noted.
Lower Extremities
Symmetrical in shape with no presence of edema, lesions, and tenderness, can walk
with one hand held. The skin color in feet is uniform in color, no redness or
discolorations noted.
Nurse-Patient Interaction
Friday, December 25, 2009
VITAL SIGNS:
Temperature -36.2°C, Respiratory Rate- 22 bpm
Heart Rate- 120 bpm
29

GENERAL SURVEY
The patient is conscious and coherent. He was able to smile and respond
actively. The patient carries by his father. There was full mobility of the body and
movements are coordinated. He was wearing a purple shirt and pajamas. Patient was
generally clean and well-groomed. Nails were short and clean. No body odor was noted.
He was able to maintain eye contact and was cooperative to the nurse.
Skin
The color of the skin is light brown with no lesions, the temperature of the skin is
uniform. Epidermis appears uniformly thin over most of the body with equal distribution
of hair. Skin turgor is good, when pinched it springs back to its previous state.
Hair
The hair is evenly distributed to the body. Scalp hair is also evenly distributed and there
were no patches of hair loss noted. Hair color was black .There were no lice, sores and
dandruff noted.
Nails
The nail surfaces were convex and show no abnormalities. The nails showed pale nail
beds and have a capillary refill time of 2 seconds.
Head
The skull was normocephalic and there were no tenderness, nodules or masses noted
upon palpation. Has symmetric facial features, no abnormalities noted such as
periorbital edema.
Eyes
The hair in eyebrows are distributed evenly and eyebrows are symmetrically aligned,
and have no scaling or lesions; the skin of the eyelids was intact without redness,
swelling, discharge or lesion and eyelashes were equally distributed along the lid
margins and curve outward. No protrusion or sunken appearance. The conjunctiva was
30

smooth and moist. Visual Acuity, Extra Ocular movement and Visual field are not
applicable due to his age.
Ears
The ears are equal in size with no swelling or thickening; skin color of the auricles is
consistent with the patient’s facial skin color. The skin is intact with no lumps or lesions;
there was no pain claimed by the patient when the pinna was palpated. Both pinnas
recoiled immediately when tested for elasticity. The patient was able to hear whispered
words to both ears.
Nose
The nose is in the midline, and in proportion to other facial features; No deformity,
asymmetry, inflammation, or skin lesions noted. There was no swelling, discharge or
bleeding noted upon inspection.
Mouth
The lips are pinkish in color. No cracking or lesions noted. Gums are pinkish in color,
teeth are white and 8 teeth were intact. No swelling or bleeding was noted. The tongue
is pink and even. Located at the midline, no ulceration found, symmetrical and moves
freely there were no inflamed tonsils noted.
Neck
The head is positioned at the midline, the accessory muscles are symmetrical and the
head was held erect and still. The trachea is in the midline position, no inflammation of
cervical lymph nodes and thyroid glands. There was no pain and limitation during the
active motion. There was no bruit upon auscultation.
Breast
The skin is smooth and even in color. No redness, bulging, edema, dimpling, or
discoloration was noted on the area of both breasts and the axillary areas. The nipples
are symmetrical, everted, and brown in color. No ulceration, bleeding or discharge and
there are no palpable nodes noted in the entire region of the breasts and the axilla.
31

Chest
The chest is symmetrical, no lesions found, no shallow breathing, no sign of deformities,
no presence of mass, no sign of abnormalities, no resonant sound. Positive rales or
crackles upon auscultation.
Heart
Patient has adynamic precordium and normal rate and regular rhythm of the heart. No
bruit and murmurs heard upon auscultation.
Abdomen
The skin is unblemished and uniform in color; there are no rashes or striaes noted. Flat
abdomen and is symmetric in contour; Umbilicus is at the midline, inverted, with no sign
of discoloration, There were no tenderness over the abdomen in all quadrants; relaxed
abdomen with smooth and constant tension upon light palpation. and no tenderness was
noted upon deep palpation.
Examination of extremities
Upper Extremities
Symmetrical in shape with no signs of deformities. The skin color in hands is uniform in
color, no redness or discolorations noted.
Lower Extremities
Symmetrical in shape with no presence of edema, lesions, and tenderness, can walk
with one hand held. The skin color in feet is uniform in color, no redness or
discolorations noted.
32

DIAGNOSTIC AND LABORATORY PROCEDURES
a. Complete Blood Count
Diagnostic Procedure
Indication(s) or Purpose(s)Date OrderedDate Results
receivedResults
Normal Values
Analysis and Interpretation of results
HemoglobinThis is indicated to the patient to
determine the presence of body fluid
deficit due to elevated Hgb level.
To monitor the iron status and oxygen
carrying capacity of the blood
Date ordered:
12/19/09
Date results
received:
12/19/09
130 g/L 110-150 g/L
The hemoglobin level is normal.
This means that the client has
normal oxygen carrying capacity
of the blood.
33

HematocritThis is indicated to determine the
patient’s hydration status and
presence of anemia.
Date ordered:
12/19/09
Date results
received:
12/19/09
.39 g/L .29-.44g/L The Hematocrit level of the
patient is normal. This means
the patient has normal
hydration status.
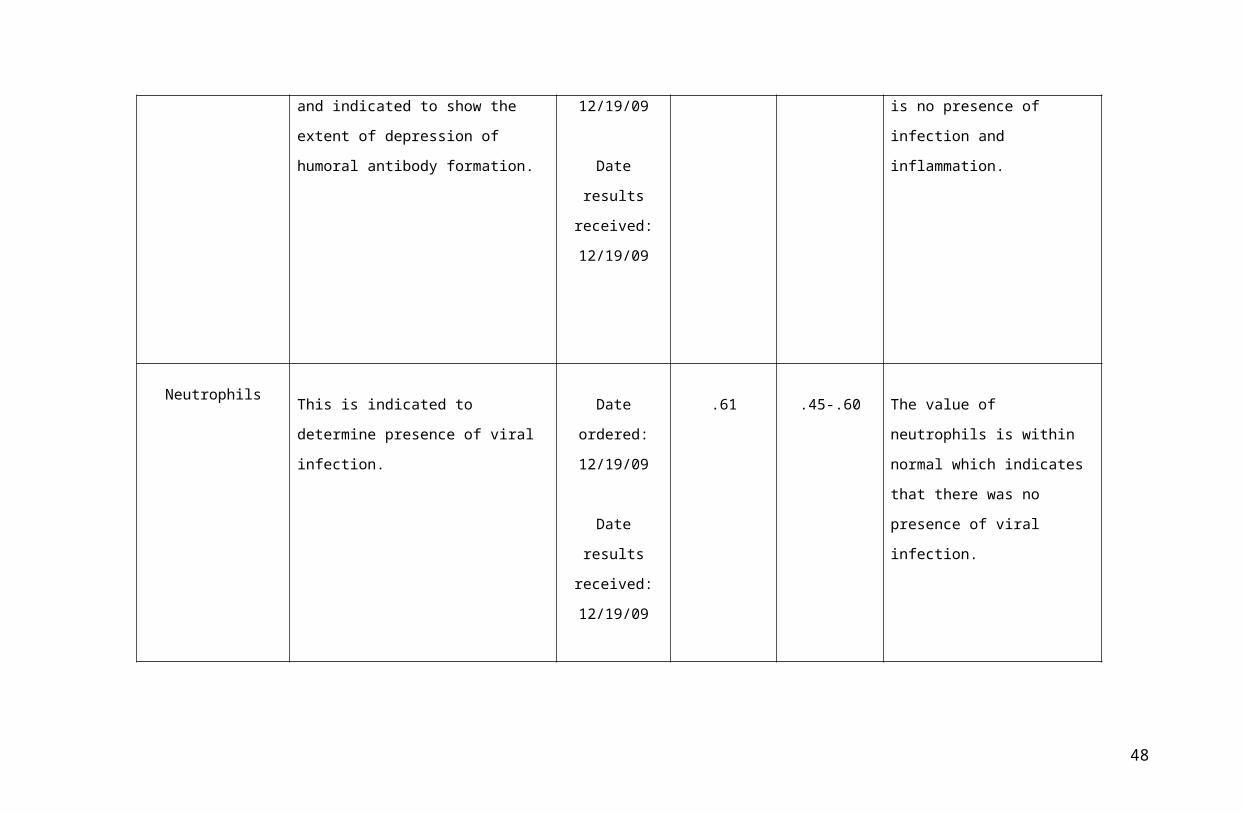
WBCThis is indicated to determine
presence of infection and inflammation
and indicated to show the extent of
depression of humoral antibody
formation.
Date ordered:
12/19/09
Date results
received:
12/19/09
9.0g/L 5-109 /L The WBC of the patient is
within normal value which
means that there is no
presence of infection and
inflammation.
34

NeutrophilsThis is indicated to determine
presence of viral infection.
Date ordered:
12/19/09
Date results
received:
12/19/09
.61 .45-.60 The value of neutrophils is
within normal which indicates
that there was no presence of
viral infection.
Lymphocytes This is indicated to determine presence of infection.
Date ordered:12/19/09
Date results received:12/19/09
.53 .20-40% The lymphocytes level of the patient is high which means that there is a presence of infection or immunodeficiency.
Nursing Responsibilities:
35

Before:
Obtain a history of the patient’s complaints, including a list of known allergens.
Obtain a history of the patient’s gastrointestinal, hematopoietic, immune, and respiratory systems, as well as results of previously performed tests
and procedures.
Obtain a list of medications the patient is taking, including herbs, nutritional supplements, and nutraceuticals. The requesting health care practitioner
and laboratory should be advised if the patient regularly uses these products so that their effects can be taken into consideration when reviewing
results.
Explain the procedure to the patient and its purpose.
Tell the patient that this test requires a blood sample. Explain who will perform the venipuncture and when.
Explain to the patient that patient may experience slight discomfort from the needle puncture and the tourniquet.
Tell the patient that no special diet or fasting is required.
Notify the physician and/or the laboratory of drugs the patient is currently taking that may affect test results; it may be necessary to restrict them.
Inform the patient that specimen collection takes approximately 5 to 10 minutes.
During:
Adhere to standard precaution.
Direct the patient to breathe normally and to avoid unnecessary movement.
If the patient is receiving IV infusion obtain the blood from the opposite arm.
Instructed the patient to avoid opening and closing the hand after a tourniquet is applied.
Perform a venipuncture, and collect the specimen in a 5-mL lavender-top (EDTA) tube. The specimen should be analyzed within 6 hours when
stored at room temperature or within 24 hours if stored at refrigerated temperature. If it is anticipated the specimen will not be analyzed within.
36

4 to 6 hours, two blood smears should be made immediately after the venipuncture and submitted with the blood sample. Smears made from
specimens older than 6 hours will contain an unacceptable number of misleading artifactual abnormalities of the RBCs, such as echinocytes and
spherocytes as well as necrobiotic WBCs.
Label the specimen, and promptly transport it to the laboratory.
After:
Apply pressure to the venipuncture site until bleeding stops.
If large hematoma develops at the venipuncture site, monitor pulses distal to the site.
b. Chest X-ray
37

Diagnostic Procedure
Indication(s) or Purpose(s)
Date OrderedDate Results
receivedResults Normal Values
Analysis and Interpretation of results
Chest X-ray
Chest X-ray is a
procedure used to
evaluate organs and
structures within the
chest for symptoms
of disease.
Date ordered:
12/19/09
Date Results
Received:
12/20/09
There are hazy and patchy infiltrations in
both lung fields. Nodular densities in the
retrocardiac space. The heart is normal in
size by configuration, diaphragms,
costopenic angles and the visualized
bones are intact.
Normal lung
fields, cardiac
size, mediastinal
structures,
thoracic spine,
ribs, and
diaphragm
Impression:
Bronchopneumonia, Primary
Koch’s Infection
Nursing Responsibilities:
Before:
Inform the patient about the purpose of the procedure, various positions to assume, and the need to hold his or her breath. For related tests, refer to
the cardiovascular and respiratory system tables.
Inform the patient that the procedure takes 5 to 10 minutes.
There are no food or fluid restrictions.
Inform the patient that no pain is associated with the study.
During:
Instruct the patient to remove clothing and metallic objects from the waist up.
38

Give the patient a gown and robe to wear.
Remove any wires connected to electrodes, if allowed.
Place patient in a standing, sitting, or recumbent position in front of the x-ray film holder.
For portable examinations, elevate the head of the bed to the high Fowler’s position.
Have the patient place hands on hips, extend neck, and position shoulders forward.
Position the chest with the left side against the film holder for a lateral view.
Instruct the patient to inhale deeply, to hold his or her breath while the x-ray is taken, and then exhale after the film is taken.
After:
Inform the patient of the possible need for additional chest x-rays to evaluate progression of the disease process or to determine the need for a
change in therapy.
Determine if the patient or family members have any further questions or concerns.
A physician sends a written report to the ordering health care provider, who discusses the results with the patient.
Evaluate test results in relation to the patient’s symptoms and other tests performed. Related diagnostic tests include computed tomography and
magnetic resonance imaging of the chest as well as a lung scan.
39

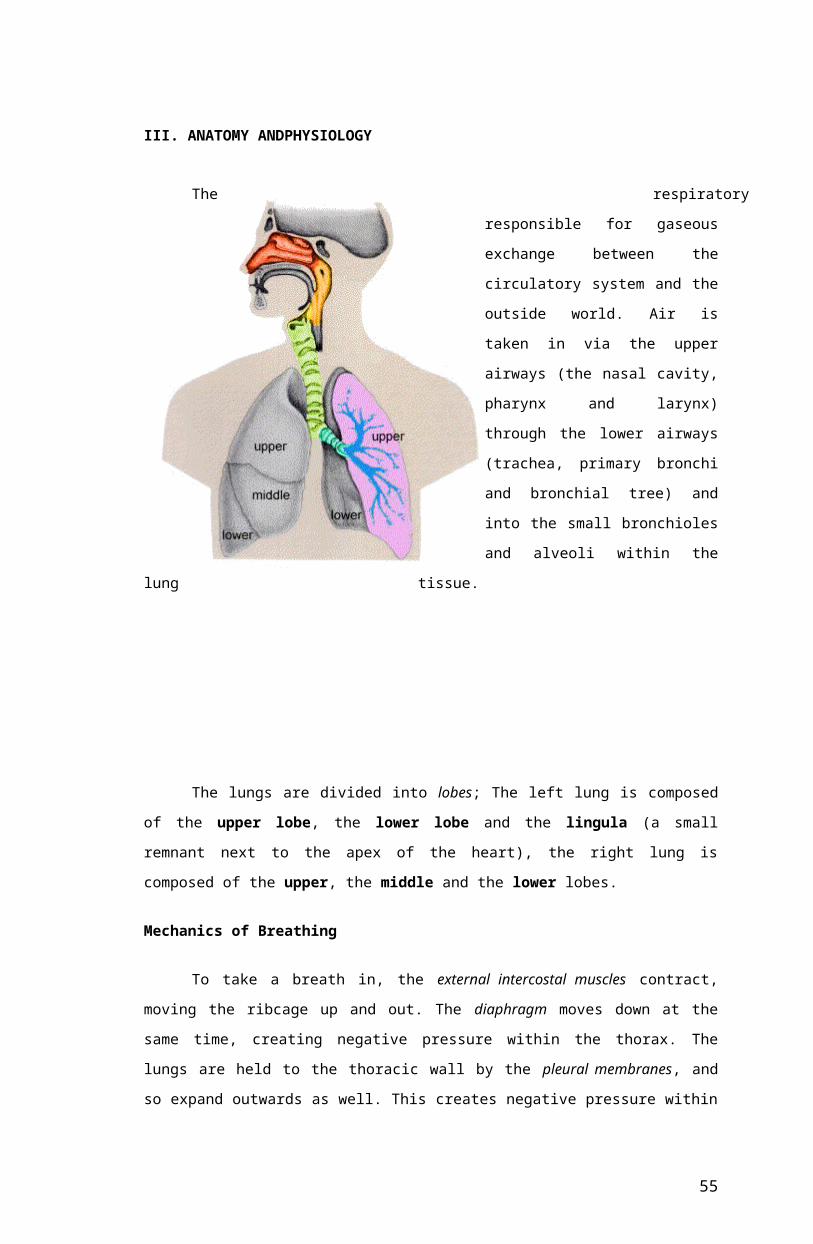
III. ANATOMY ANDPHYSIOLOGY
The respiratory system is situated in the thorax, and is responsible for gaseous
exchange between the circulatory
system and the outside world. Air is
taken in via the upper airways (the
nasal cavity, pharynx and larynx)
through the lower airways (trachea,
primary bronchi and bronchial tree)
and into the small bronchioles and
alveoli within the lung tissue.
The lungs are divided into lobes; The left lung is composed of the upper lobe,
the lower lobe and the lingula (a small remnant next to the apex of the heart), the right
lung is composed of the upper, the middle and the lower lobes.
Mechanics of Breathing
To take a breath in, the external intercostal muscles contract, moving the ribcage
up and out. The diaphragm moves down at the same time, creating negative pressure
within the thorax. The lungs are held to the thoracic wall by the pleural membranes, and
so expand outwards as well. This creates negative pressure within the lungs, and so air
rushes in through the upper and lower airways.
Expiration is mainly due to the natural elasticity of the lungs, which tend to
collapse if they are not held against the thoracic wall. This is the mechanism behind lung
collapse if there is air in the pleural space (pneumothorax).
40

Physiology of Gas Exchange
Each branch of the bronchial tree eventually sub-divides to form very narrow
terminal bronchioles, which terminate in the alveoli. There are many millions of alveloi in
each lung, and these are the areas responsible for
gaseous exchange, presenting a massive surface
area for exchange to occur over.
Each alveolus is very closely associated with a
network of capillaries containing deoxygenated
blood from the pulmonary artery. The capillary and
alveolar walls are very thin, allowing rapid
exchange of gases by passive diffusion along
concentration gradients.
CO2 moves into the alveolus as the concentration is
much lower in the alveolus than in the blood, and
O2 moves out of the alveolus as the continuous flow
of blood through the capillaries prevents saturation
of the blood with O2 and allows maximal transfer
across the membrane.
41

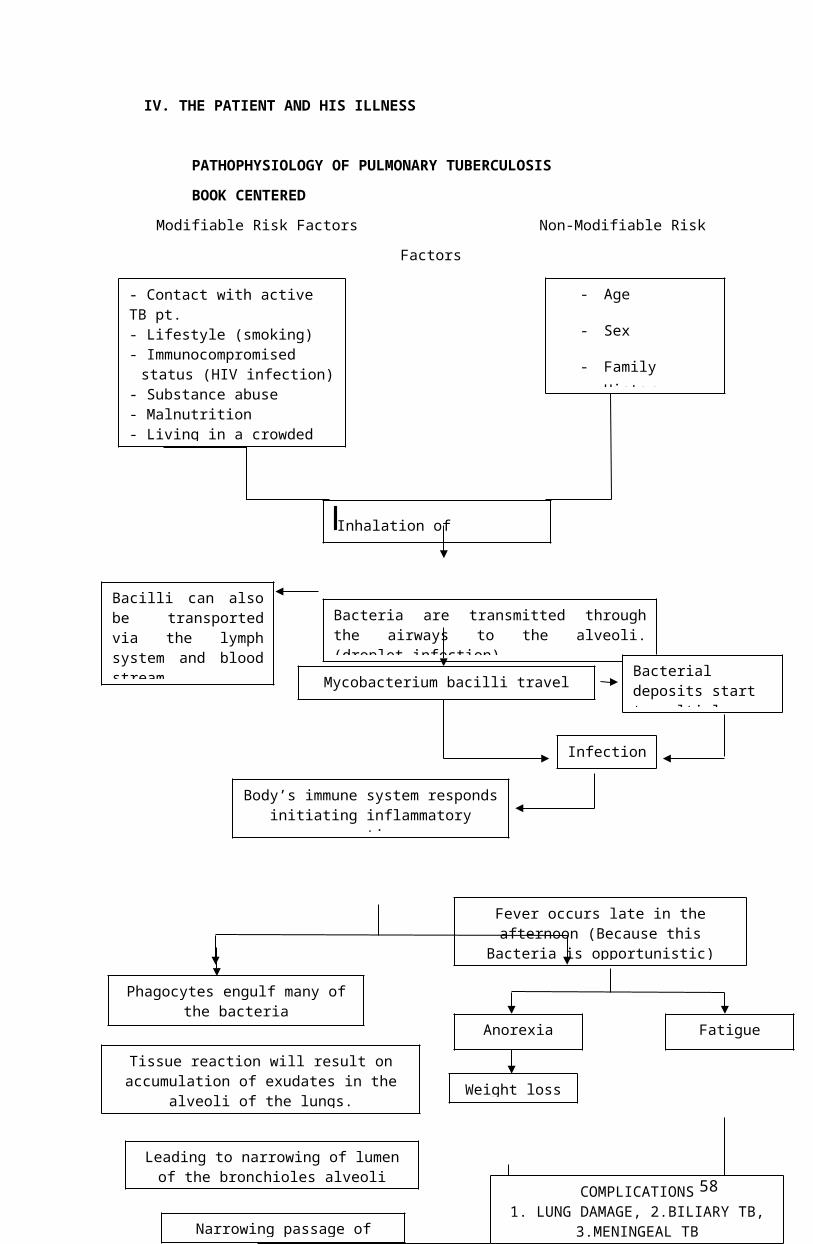
IV. THE PATIENT AND HIS ILLNESS
PATHOPHYSIOLOGY OF PULMONARY TUBERCULOSIS
BOOK CENTERED
Modifiable Risk Factors Non-Modifiable Risk Factors
Tissue reaction will result on accumulation of exudates in the
alveoli of the lungs. Weight lossAnorexia FatigueChest pain
Non-productive
cough
Leading to narrowing of lumen of the bronchioles alveoliNarrowing passage of
airways
Bacilli can also be transported via the lymph system and blood stream.
Bacteria are transmitted through the airways to the alveoli. (droplet infection)
- Contact with active TB pt.- Lifestyle (smoking)- Immunocompromised status
(HIV infection)- Substance abuse - Malnutrition- Living in a crowded place
B BInhalation of Mycobacterium
- Age
- Sex
- Family History
- Environment
Mycobacterium bacilli travel and lodges to the lungs.
Bacterial deposits start to multiply.
Infection
Tissue reaction will result on accumulation of exudates in the alveoli of the lungs.
Weight loss
Anorexia Fatigue
Chest pain Non-productive cough
Body’s immune system responds initiating inflammatory reaction.
Phagocytes engulf many of the bacteria Fever occurs late in the afternoon
(Because this Bacteria is opportunistic)
Leading to narrowing of lumen of the bronchioles alveoli
Narrowing passage of airwaysCOMPLICATIONS
1. LUNG DAMAGE, 2.BILIARY TB, 3.MENINGEAL TB
42

V. PATHOPHYSIOLOGY OF PULMONARY TUBERCULOSIS (client centered)
Modifiable Risk Factors Non-Modifiable Risk Factors
CracklesRales
Bacteria are transmitted through the airways to the alveoli. (Droplet infection)
- Contact with undiagnosed TB pt.- Living in a crowded place
B B BInhalation of Mycobacterium Bacilli
- Age
- Environment
Mycobacterium bacilli travel and lodges to the lungs.
Bacterial deposits start to multiply.
Infection
Tissue reaction will result on accumulation of exudates in the alveoli of the lungs.
Difficulty of breathing Non-productive cough
Body’s immune system responds initiating inflammatory reaction.
Phagocytes engulf many of the bacteria
Leading to narrowing of lumen of the bronchioles alveoli
Narrowing passage of airwaysSigns and Symptoms
43

SYNTHESIS OF THE DISEASE
Koch’s Infection is an infectious disease caused by slow- growing bacteria that
resembles a fungus, Myobacterium tuberculosis, which is usually spread from person to
person by droplet nuclei through the air. The lung is the usual infection site but the
disease can occur elsewhere in the body.
Typically, the bacteria from lesion (tubercle) in the alveoli. The lesion may heal, leaving
scar tissue; may continue as an active granuloma, heal, then reactivate or may progress
to necrosis, liquefaction, sloughing, and cavitation of lung tissue. The initial lesion may
disseminate bacteria directly to adjacent tissue, through the blood stream, the lymphatic
system, or the bronchi.
Most people who become infected do not develop clinical illness because the body’s
immune system brings the infection under control. However, the incidence of
tuberculosis (especially drug resistant varieties) is rising. Alcoholics, the homeless and
patients infected with the human immunodeficiency virus (HIV) are especially at risk.
Complications of tuberculosis include pneumonia, pleural effusion, and extrapulmonary
disease. The Predisposing Factors are malnutrition, overcrowding, alcoholism, ingestion
of infected cattle, virulence, and over fatigue.
The sign and Symptoms are productive cough-yellowish in color, low fever, night sweats,
dyspnea, anorexia, generated body malaise, weight loss, chest back pain and
hemoptysis
TB results from infection by any of the TB complex mycobacteria, including
Mycobacterium tuberculosis, M bovis, M africanum, M microti, and M canetti.
TB can be divided into primary, progressive-primary, and postprimary forms on the basis
of the natural history of the disease. Postprimary TB results from either reactivation of a
latent primary infection or, less commonly, from the repeat infection of a previously
sensitized host. The term “postprimary” is preferred to “reactivation” when referring to
the clinical diagnosis because firmly distinguishing recurrence from an antecedent
infection is impossible in most cases.
Approximately 10% of all infected patients are likely to develop reactivation, and the risk
is highest within the first 2 years or during periods of immunosuppression.
The major determinants of the type and extent of TB disease are the patient’s age and
immune status, the virulence of the organism, and the mycobacterial load. Postprimary
44

TB is typically a disease of adolescence and adulthood that results from reactivation of
an initially contained infection by a TB complex mycobacterium. Pulmonary reactivation
usually occurs in the apical and posterior segments of the upper lobes or in the superior
segments of the lower lobes.This distribution may be related to the higher oxygen
tension or the reduced perfusion and lymphatic clearance in these lung segments.
Sources:
Medscape
News Author: Laurie Barclay, MD
CME Author: Désirée Lie, MD, M
CME Released: 01/10/2005; Valid for credit through 01/10/2006
45

V. THE PATIENT AND HIS CARE
A. Medical Management
a. IVF, Nebulization, Oxygen Therapy
Medical
Management/
Treatment
Date ordered,
performed,
changed/ d/c
General Description Indications or PurposesClient’s response to the
treatment
IVF
D5.3NaCL Date ordered:
12-19-09
Date performed:
12-19-09 to 12-26-09
Date changed/dc:
12-26-09
5% Dextrose, 0.3 Sodium
Chloride is an isotonic solution
-maintenance of fluid in clients
who cannot drink or eat
-replacement fluids when large
amounts are lost
-administration of IV medications
- It reduces the edema, stabilizes
blood pressure and regulates
urine output
The patient exhibited
improved hydration status
as evidenced by good skin
turgor.
The patient received
parenteral medications.
46

Nursing Responsibilities
Pre-Procedure
Verify the doctor’s order.
Identify the patient.
Verify the patient’s name by asking his S.O.Assess the client previous experience with IV therapy and arm placement
preference
Determine if client is to undergo any planned surgeries or procedures
Assess the type and duration of IV therapy as ordered by the physician or license
Assess the laboratory data and client history of allergies
Asses client’s medical history for chronic illnesses
Explain the procedure to the patient/SO and explain the purpose of the procedure.
Medical
Management/
Treatment
Date ordered,
performed, changed/
d/c
General DescriptionIndications or
Purposes
Client’s response to
the treatment
Nebulization Date ordered: 12-19-
09
Date performed: 12-19-
09
to 12-25-09
Date changed/dc: 12-
25-09
Delivers most medications
administered through inhaled
route.
To administer
Salbutamol, necessary
to loosen patients
secretions.
The patient improved
breathing pattern &
airway exchange as
evidenced by absence
of cyanosis.
47
Nursing Responsibilities
Before:
a. Check doctor’s order
b. Prepare the equipment
c.Explain the procedure to the client
d. Place medication into the nebulization kit and turn machine on.
During:
a. Instruct the patient to breathe in the vapor
b. Shake the nebulization equipment from side to side.
c.If necessary, directly place the mouthpiece in the mouth
After:
a. Clean equipment thoroughly
b. Document the procedure.
48

Generic name/Brand
name
Date ordered Route/Dosage/Frequency
of administration
General
action/Classification
Client's response
to the medication
with S/E
Amikacin/Amikin Started: Dec 19,
2009
Date performed: 12-
19-09
to 12-25-09
Date changed/dc:
12-25-09
IV
15 mg
Every 8 hours
Amikacin inhibits protein
synthesis in bacteria by
binding to bacterial rib
Anti-
infective agent.
Aminoglycosides
No report signs of
tinnitus and muscle
weakness to the
patient.
49

NURSING RESPONSIBILITIES:
Prior:
o Check doctor's order.
o Verify the patient.
o Wash hands before handling the medication.
o Assess patient’s vital signs prior to administering the medication.
o Obtain a history of previous use and reactions to amikacin. Persons with a negative history of amikacin sensitivity may
still have an allergic response.
During:
o Administer as indicated (right drug, right dosage, right frequency)
o Give IV dose over 1-2 minutes.
o Clean the IV insertion site for medications with a cotton ball with alcohol.
o Gradually inject the drug into the port.
o Administer cautiously and slowly with aseptic technique.
o Observe patient for signs and symptoms of pruritus, wheezing.
After:
o Monitor patient's vital signs
o Advise patient to report the signs of super infection and allergy
o Wash hands
50

o Observe for client's reaction
o Document
51

Name of
DrugDate Ordered
Route and
Frequency of
Administrati
on
General Action and Mechanism
of Action Indication and
Purposes
Client's response to the
medication with S/E
Ampicillin:
Omnipen
Started: Dec 19,
2009
Date performed:
12-19-09
to 12-21-09
IV route
100mg q 6
hours
General Action: Anti infectives
Mechanism of Action: Bactericidal
action; spectrum is broader than
penicillin
To fight against
infection due to
vaginal bleeding
The patient didn't manifest any
signs and symptoms of
inflammation.
Side Effects: Diarrhea, nausea,
vomiting
NURSING RESPONSIBILITIES:
Prior:
o Check doctor's order.
o Verify the patient.
o Wash hands before handling the medication.
o Assess patient’s vital signs prior to administering the medication.
52

o Obtain a history of previous use and reactions to ampicillin. Persons with a negative history of ampicillin sensitivity
may still have an allergic response.
During:
o Administer as indicated (right drug, right dosage, right frequency)
o Give IV dose over 1-2 minutes.
o Clean the IV insertion site for medications with a cotton ball with alcohol.
o Gradually inject the drug into the port.
o Administer cautiously and slowly with aseptic technique.
o Observe patient for signs and symptoms of pruritus, wheezing.
After:
o Monitor patient's vital signs
o Advise patient to report the signs of super infection and allergy
o Wash hands
o Observe for client's reaction
o Document
53

Generic name/Brand name
Date ordered/started/discontinued
Route/Dosage/Frequency of administration
General action/ClassificationClients response to the
medication w/ SE
Hydrocortisone
Cortizan
Started: Dec. 21, 2009
Date performed: 12-21-09
to 12-22-09
Changed to Prednisone: Dec.
23, 2009
IV
150 mg
Every 6 hours
Glucocorticoid with Anti-
inflammatory effect because of
its ability to inhibit prostaglandin
synthesis, inhibit migration of
macrophages leukocytes,
fibroblasts at site of
inflammation.
Anti-inflammatory
No repert signs of headche,
increased intarcranial presure
and restlessness.
NURSING RESPONSIBILITIES:
Prior:
o Check doctor's order.
o Verify the patient.
o Wash hands before handling the medication.
54
o Assess patient’s vital signs prior to administering the medication.
o Obtain a history of previous use and reactions to hydrocortisone. Persons with a negative history of hydrocortisone
sensitivity may still have an allergic response.
During:
o Administer as indicated (right drug, right dosage, right frequency)
o Give IV dose over 1-2 minutes.
o Clean the IV insertion site for medications with a cotton ball with alcohol.
o Gradually inject the drug into the port.
o Administer cautiously and slowly with aseptic technique.
o Observe patient for signs and symptoms of pruritus, wheezing.
After:
o Monitor patient's vital signs
o Advise patient to report the signs of super infection and allergy
o Wash hands
o Observe for client's reaction
o Document
Generic
name/Brand
Date Route/Dosage/Frequency General Clients
response to
55

name ordered/started/discontinued of administration action/Classification the medication
w/ SE
Ipratropium
bromide
Combivent
Started:
Dec. 21, 2009 (10am)
Inhalation
½ nebule
Every 8 hours
Anti-cholinergic
(atrophine-like); relaxes
bronchial smooth
muscle.
Bronchodilator
No report signs
of GI irritation
and nausea.
NURSING RESPONSIBILITIES:
Prior:
o Check doctor's order.
o Verify the patient.
o Wash hands before handling the medication.
o Assess patient’s vital signs prior to administering the medication.
During:
o Assess respiratory rate.
o Ausculcate lung sounds.
56

o Assess pulses.
o Warn patient to avoid accidentally spraying drug into eyes. Temporary blurring of vision may result.
After:
o Monitor patient's vital signs
o Advise patient to report the signs of super infection and allergy
o Wash hands
o Observe for client's reaction
o Document
Generic name/Brand
name
Date ordered/started/discontinued
Route/Dosage/Frequency of administration
General Action/Classification
Client’s response to medication
Cefuroxime
Roxicef
Started:
Dec. 21, 2009 (4pm)
Date performed: 12-21-09
to 12-25-09
IV
250 mg
Every 8 hours
Binds to bacterial cell
wall membrane,
causing cell death.
Bactericidal action
against susceptible
bacteria.
Dizziness,
drowsiness,
fatigue,
headache,
vomiting,
change in taste
57
Anti-infective 2nd
generation
Cephalosphorin
NURSING RESPONSIBILITIES:
Prior:
o Check doctor's order.
o Verify the patient.
o Wash hands before handling the medication.
o Assess patient’s vital signs prior to administering the medication.
o Obtain a history of previous use and reactions to cefuroxime. Persons with a negative history of cefuroxime sensitivity
may still have an allergic response.
During:
o Administer as indicated (right drug, right dosage, right frequency)
o Give IV dose over 1-2 minutes.
o Clean the IV insertion site for medications with a cotton ball with alcohol.
o Gradually inject the drug into the port.
o Administer cautiously and slowly with aseptic technique.
58

o Observe patient for signs and symptoms of pruritus, wheezing.
After:
o Monitor patient's vital signs
o Advise patient to report the signs of super infection and allergy
o Wash hands
o Observe for client's reaction
o Document
Generic name/Brand
Date ordered/started/discontinued
Route/Dosage/Frequency of administration
General action/Classification
Clients response to the medication
59

name w/ SE
Albute-rol
Salbutamol
Started:
Dec. 19, 2009 (10pm)
Revised:
Dec. 20, 2009 (2pm)
Inhalation
1 nebule + 1 cc NSS
1 nebule
Every 8 hours
Beta 2-adrenergic
bronchodilator.
Anti-asthmatics,
Sympathomimetic.
The patient
improved
breathing pattern
& airway
exchange as
evidenced by
absence of
cyanosis.
NURSING RESPONSIBILITIES:
Prior:
o Check doctor's order.
o Verify the patient.
o Wash hands before handling the medication.
o Assess patient’s vital signs prior to administering the medication.
60

During:
o Administer as indicated (right drug, right dosage, right frequency)
o Clean the IV insertion site for medications with a cotton ball with alcohol.
o Gradually inject the drug into the port.
o Administer cautiously and slowly with aseptic technique.
o Observe patient for signs and symptoms of nervousness, tremors, and restlessness.
After:
o Advise patient to report the signs of super infection and allergy
o Wash hands
o Observe for client's reaction
o Document
o Advise patient that frequent mouth rinses, good oral hygiene, and sugarless gum or candy may decrease dry mouth.
Generic name/Brand
Date ordered/started/discontinued
Route/Dosage/Frequency of Administration
General action/Classification
Clients response to
61

name the medication w/ SE
Rifampin
Rifampicin
Ordered:
Dec. 22, 2009 (4pm)
Started:
Dec. 23, 2009 (7am)
Revised:
Dec. 23, 2009
Oral
160 mg (Stock dose: 200
mg/5 ml) = 4 ml
110 mg (Stock dose: 200
mg/5 ml) = 2.75 ml
Once a day, pre-breakfast
Inhibits DNA-
dependent RNA
polymerase, which
impairs RNA synthesis;
bactericidal.
Anti-infective, anti-TB
Red
discoloration of
urine noted.
NURSING RESPONSIBILITIES:
Prior:
o Check doctor's order.
o Verify the patient/SO.
o Wash hands before handling the medication.
During:
o Administer as indicated (right drug, right dosage, right frequency)
62

o Caution client to avoid sharing of medication.
After:
o Monitor patient's vital signs
o Wash hands
Generic name/Brand name Date ordered/started/discontinued
Route/Dosage/Frequency of Administration
General action/Classification Clients response to the medication w/ SE
Isoniazid
Isotamine
Ordered:
Dec. 21, 2009 (4pm)
Started:
Dec. 22, 2009 (7am)
Oral
100 mg = 5 ml
Once a day, pre-breakfast
Inhibits synthesis of mycolic
acids, essential metaboilites
for mycobacteria. The action
may be bactericidal.
Anti-infective, anti-TB
No report signs of rashes.
o Observe for client's reaction
o Document
NURSING RESPONSIBILITIES:
Prior:
63

o Check doctor's order.
o Verify the patient/SO.
o Wash hands before handling the medication.
During:
o Administer as indicated (right drug, right dosage, right frequency)
o Caution client to avoid sharing of medication.
After:
o Monitor patient's vital signs
o Wash hands
o Observe for client's reaction
o Document
NURSING RESPONSIBILITIES:
Prior:
o Check doctor's order.
o Verify the patient/SO.
64

o Wash hands before handling the medication.
During:
Generic name/Brand name Date
ordered/started/discontinued
Route/Dosage/Frequency of
administration
General
action/Classification
Clients response to the
medication w/ SE
Pyrazinamide
Tebrazid
Ordered:
Dec. 21, 2009 (4pm)
Started:
Dec. 22, 2009 (7am)
Revised:
Dec. 23, 2009
Oral
125 mg (Stock dose: 250
mg/5 ml) = 2.5 ml
200 mg (stock dose: 250 mg/5
ml) = 4 ml
Bacteriostatic or bactericidal
by unknown mechanisms.
Anti-infective, an-TB
Itching and skin rash noted.
o Administer as indicated (right drug, right dosage, right frequency)
o Caution client to avoid sharing of medication.
After:
o Monitor patient's vital signs
o Wash hands
65

o Observe for client's reaction
o Document
C .Diet
Type of Diet
Date Ordered
Date Started
Date Changed
General
DescriptionIndication(s)
Specific Foods
Taken
Client’s Response
to Diet
Nothing Per Orem
(NPO)
Date Ordered:
12/19/09
Date Performed:
12/19/09
Date Changed:
12/20/09
No food and fluid
is passed through
the alimentary
canal.
Since the pt has
been admitted
and is to be
subjected to a
series of
observation and
prevent irritating
the body until
definitive
diagnosis is
established.
None The patient strictly
complied with the
prescribed diet.
Soft rice and The patient followed
66

DAT Date ordered::
12/20/09
Date Performed:
12/20/09 -
12/26/09
Any foods and
fluids that are
being tolerated by
the patient.
To provide
nutrients needed
by the body.
chicken Tinola.
Milk
the Diet.
67

NURSING RESPONSIBILITIES:
Prior:
o Check doctor's order.
o Verify the patient/SO.
o Explain the importance of complying with the dietary prescription
o Cite foods that are applicable to the indicated diet.
During:
o Be sure that patient is taking or having foods that he can tolerate.
o Explain the importance of complying with the dietary prescription.
After:
o Assess for patient’s response to the diet.
o Take note for any signs of abdominal pain or as client verbalizes so.
o Document relevant data.
d. Exercise/ Activity
68

Type of Exercise
Date Ordered
Date Started
Date Changed
General DescriptionIndication(s
)Client’s Response
Bed Rest Date Ordered:
12/19/2009
Date Started:
12/19/2009
Date changed:
12-23-09
A medical treatment
which refers to staying in
bed day and night as a
treatment for an illness or
medical condition. Patient
should be restricted from
any stressful activities
and be on bed most of
the time to decrease
oxygen demand and
prevent fatigability.
To decrease
oxygen and
energy
demand
Shakespeare was able to comply with
the prescribed activity and reported
that he had enough rest, gained more
energy, and did not experience
further difficulty of breathing starting
November 4, 2008 with the help of
oxygen therapy.
NURSING RESPONSIBILITIES:
Prior:
o Check doctor's order.
69

o Provide comfort and safety of the client at all times
o State the purpose and indications of the activity.
o Explain to the patient and to his significant others the importance of complying with the order
During:
o Encourage the patient the importance of having adequate amounts of rest.
o Always ensure the comfort of the patient while he complies with the exercise or activity.
o Provide safety measures by removing sharp objects or objects that may hinder range of motion on the bed’s surface
o Provide comfort measures by stretching bed linens and puffing pillows
o Ensure safety by raising the side rails of the bed.
o Monitor and assist the patient as necessary
After:
o Continuous monitoring of the client’s exercise should be observed.
o Nurse should make sure that the patient adheres to the ordered exercise.
o Note tolerance to prescribed activity as well as other significant data.
o Monitor and document patients’ reaction to the treatment given
VIII. NURSING MANAGEMENT
70

ACTUAL NURSING CARE PLAN
Cues Nursing diagnosis
Scientific explanation
Objective Nursing Intervention
Rationale Evaluation
S- “may
konting ubo
siya at
nahihirapan
huminga” as
verbalized by
SO.
O- afebrile,
with on and
off cough and
clear nasal
secretions.
Vital signs:
Pr-128bpm
RR-30cpm
T-36.2c
Ineffective
airway
clearance r/t
retained
secre
tions.
Entry of foreign
substance.
Proliferation/
multiplication of
foreign substance
Compensatory
response
Irritation of
bronchioles
Produce secretion
Accumulation and
After 2-3
hours of
nursing
interventions,
patient will be
able to
maintain
airway
patency.
Established
rapport.
Vital signs
taken and
recorded.
Positioned
head
midline with
flexion
appropriate
for age or
condition.
☺ To gain
trust and
cooperation
from the
patient and
SO.
☺ To have a
baseline data
and monitor
changes in
the patient’s
condition.
☺ To open or
maintain
open airway
in at-rest or
After 2-3
hours of
nursing
interventions,
patient was
able to
maintain
airway
patency as
evidenced by
reduced
secretions.
71

blockage
Bronchoconstrictio
n
Ineffectve airway
clearance
Elevated
head of the
bed/change
position
every 2
hours and
prn.
Kept
environment
allergen/
pollutant
free.
Administere
d
bronchodilat
ors as
ordered.
compromised
individual.
☺ To take
advantage of
gravity
decreasing
pressure on
the
diaphragm
and
enhancing
drainage of/
ventilation to
different lung
segments.
To reduce
irritant effect
on airways.
72

Relaxes
bronchial
smooth
muscles.
Cues Nursing
diagnosis
Scientific
explanation
Objectives Nursing
Intervention
Rationale Evaluation
S> “nahihirapan
syang huminga”
as verbalized by
SO
O>cold clammy
skin
restlessness
RR=50bpm
Impaired
gas
exchange
r/t
ventilation
perfusion
imbalance.
Presence of
bacteria in the lower
respiratory tract
Goes to the alveoli
for proliferation
Immune system will
recognize foreign
After 1-2
hours of
nursing
intervention,
patient will
demonstrate
improved
ventilation
and
Established
rapport
Taken and
recorded vital
signs
☺ To gain
trust and
cooperation
from the
patient and
SO.
☺ To have
After 4 hours
of nursing
intervention,
patient
demonstrated
improved
ventilation and
adequate
oxygenation of
73

substance and
facilitates
inflammatory
response
Macrophages
engulfs the bacteria
Accumulation of
dead cells in the
alveoli
Retention of
secretions and
bronchoconstriction
Leading to
ventilation perfusion
imbalance in the
alveoli and capillary
membrane
Impaired gas
adequate
oxygenation
of tissues.
Elevated head
of bed/position
client
appropriately
Encouraged
frequent
position
changes and
deep
breathing/cough
ing exercises.
Kept
environment
allergen or
pollutant free
Encourage rest
baseline
data and
monitor
changes in
the patient’s
condition.
☺ To
maintain
airway.
☺ To
promote
optimal
chest
expansion.
To
reduce
irritant
effect on
tissues.
74

exchange periods or limit
activities.
airways.
To
prevent
fatigue.
75

Cues Nursing diagnosis Scientific
explanation
Goal Nursing
Intervention
Rationale Expected Outcome
76

S>”la syang ganang
kumain” as
verbalized by the SO
O> Body Weakness
Projectile
vomiting
irritability
loss of appetite
wt: 9.0 kg
DBW=15 kgs
Imbalance nutrition:
less than body
requirements r/t
inability to ingest
adequate nutrients.
Presence of bacteria
in the body
Inflammatory
response occur
Systemic
vasodilation in the
circulation of the
body
Increase peristalsis
Causing pressure in
the intestine
Nausea and vomiting
After 2 months of
nursing intervention,
patient will be able
gain weight from 9.0
kgs to 15 kgs.
Established
rapport
Taken and
recorded vital
signs
Discussed eating
habits including
food preferences
such as giving
colorful food
Noted total daily
intake. As
maintained diary
of calorie intake,
patterns, and
times of eating
☺ To gain trust and
cooperation from the
patient and SO.
☺ To have a
baseline data and
monitor changes in
the patient’s
condition.
☺ To encourage
patient to eat.
☺ To reveal
changes that should
be made in client’s
dietary intake.
After 1 month of
nursing intervention,
patient was able to
gain weight from 9
kgs to 15 kgs.
77

Loss of appetite
Inability to ingest
adequate nutrients
Imbalance nutrition
Encourage
proper oral
hygiene
Prevent or
minimize
unpleasant odors
Weigh weekly
and document
results
Give
supplemental
vitamins as
ordered
To increase
appetite.
To avoid or
prevent negative
effect on appetite on
eating.
To monitor
effectiveness of
dietary plan.
To induce patient’s
appetite.
78

Cues Nursing diagnosis Scientific
explanation
Objectives Nursing Intervention Rationale
S>” Di naming
alam kung ano
ang gagawin” as
verbalized by SO
O>Inaccurate
follow through of
instructions
Knowledge deficit
regarding condition,
treatment, prevention,
self care, and
discharge needs
related to lack of
exposure to or
misinterpretation of
information as
evidenced by request
for information.
Absence or
deficiency of
cognitive information
about Primary Koch’s
Infection
After 2-3 hours of
nursing intervention,
pt. will initiate
behavior/ lifestyle
changes to improve
general well-being
and reduced risk of
reactivation of TB
Established
rapport.
Vital signs taken
and recorded.
Determined client’s
most urgent need
from both client’s
and nurse’s
viewpoint.
Stated objectives
clearly in learner’s
terms.
Determined client’s
method of
☺ To gain trust and
cooperation from the
patient and SO.
☺ To have baseline
data and monitor
changes in the
patient’s condition.
☺ To identify starting
point.
☺ To meet learner’s
needs.
☺To facilitate
learning.
79

accessing
information and
include in teaching
plan.
Provided written
information/guideli
nes for client to
refer to as
necessary
☺To Reinforces
learning.
Cues Nursing
diagnosis
Scientific
explanation
Objectives Nursing
Intervention
Rationale Expected
outcome
S>
O> (+) dyspnea
(+)
tachypnea
Irritability
Poor skin
turgor
Impaired
gas
exchange
r/t
ventilation
perfusion
imbalance.
Presence of
bacteria in the
lower respiratory
tract
Goes to the alveoli
for proliferation
Immune system will
recognize foreign
substance and
After 1-2
hours of
nursing
intervention,
patient will
demonstrate
improved
ventilation
and
adequate
oxygenation
Established
rapport
Vital signs taken
and recorded
Elevated head
of bed/position
☺ To gain
trust and
cooperation
from the
patient and
SO.
☺ To monitor
changes in the
patient’s
condition.
Patient
demonstrated
improved
ventilation
and adequate
oxygenation
of tissues.
80

Restlessness
Diaphoresis
Cyanosis
Rr= 45bpm
facilitates
inflammatory
response
Macrophages
engulfs the bacteria
Accumulation of
dead cells in the
alveoli
Retention of
secretions and
bronchoconstriction
Leading to
ventilation
perfusion
imbalance in the
alveoli and capillary
membrane
Impaired gas
of tissues. client
appropriately
Encouraged
frequent position
changes and
deep
breathing/coughi
ng exercises.
Assess for
dyspnea,
tachypnea,
abnormal or
diminished
breath sounds,
increase
respiratory
effect, limited
chest wall
expansion and
fatigue
Note cyanosis/
☺ To maintain
airway
☺ To promote
optimal chest
expansion.
Helps clarify
degree of
difficulty and
changes in
condition
Accumulation
of secretions
or airway
compromise
81

exchange change in skin
color, including
mucus
membranes and
nail beds
Promote bed
rest or limit
activity and
assist with self
care activities as
necessary
Monitor serial
ABG’s or pulse
oximetry
can impair
oxygenation of
vital organs
and tissues
Reducing
Oxygen
consumption
or demand
during periods
of respiratory
compromise
may reduce
severity of
symptoms
Decreased
oxygen
content
(PaO2) or
saturation/
increased
PaCO2
indicate need
82

Provide
supplemental
Oxygen as
appropriate
for intervention
or change in
therapeutic
regimen
Aids in
correcting
hypoxemia
that may occur
secondary to
decreased
ventilation or
diminished
alveolar lung
surface
83

2. Actual SOAPIERs
12/20/09
S1 > “may konting ubo siya at nahihirapan huminga” as verbalized by SO.
S2> “nahihirapan syang huminga” as verbalized by SO
S3> ”la syang ganang kumain” as verbalized by the SO
S4> Di naming alam kung ano ang gagawin” as verbalized by SO
O> Received patient on bed, conscious and coherent with on going IVF of D5 0.3
NaCl 500ml regulated at 56 cc/hr at 250 cc level infusing well on the left hand,
the skin of the eyelids was intact without redness, swelling, discharge or lesion
and eyelashes were equally distributed along the lid margins and curve outward.
No protrusion or sunken appearance. The conjunctiva was smooth and moist.
The chest is symmetrical, no lesions found, no shallow breathing, no sign of
deformities, no presence of mass, no sign of abnormalities, no resonant sound.
Positive rales or crackles upon auscultation. , the skin had a poor skin turgor with
none tenderness, with vital signs taken as follows: Temperature=36.6°C Heart
Rate=128 bpm Respiratory Rate=29 bpm.
A1> Ineffective airway clearance r/t retained secretions.
A2> Impaired gas exchange r/t ventilation perfusion imbalance.
A3> Imbalance nutrition: less than body requirements r/t inability to ingest adequate
nutrients
A4> Knowledge deficit regarding condition, treatment, prevention, self care, and
discharge needs related to lack of exposure to or misinterpretation of information
as evidenced by request for information.
P1> After 2-3 hours of nursing interventions, patient will be able to maintain airway
patency as evidence by reduced secretions.
P2> After 2 hours of nursing interventions the patient will verbalize awareness of
causative factors and initiate necessary interventions.
P3> After 1 month of nursing intervention, patient will be able to gain weight from 9
kgs to 15 kgs.
P4> After 2-3 hours of nursing intervention, patient will be able to initiate lifestyle
changes and participate in treatment regimen to improve general well-being and
reduced risk of reactivation of TB.
84
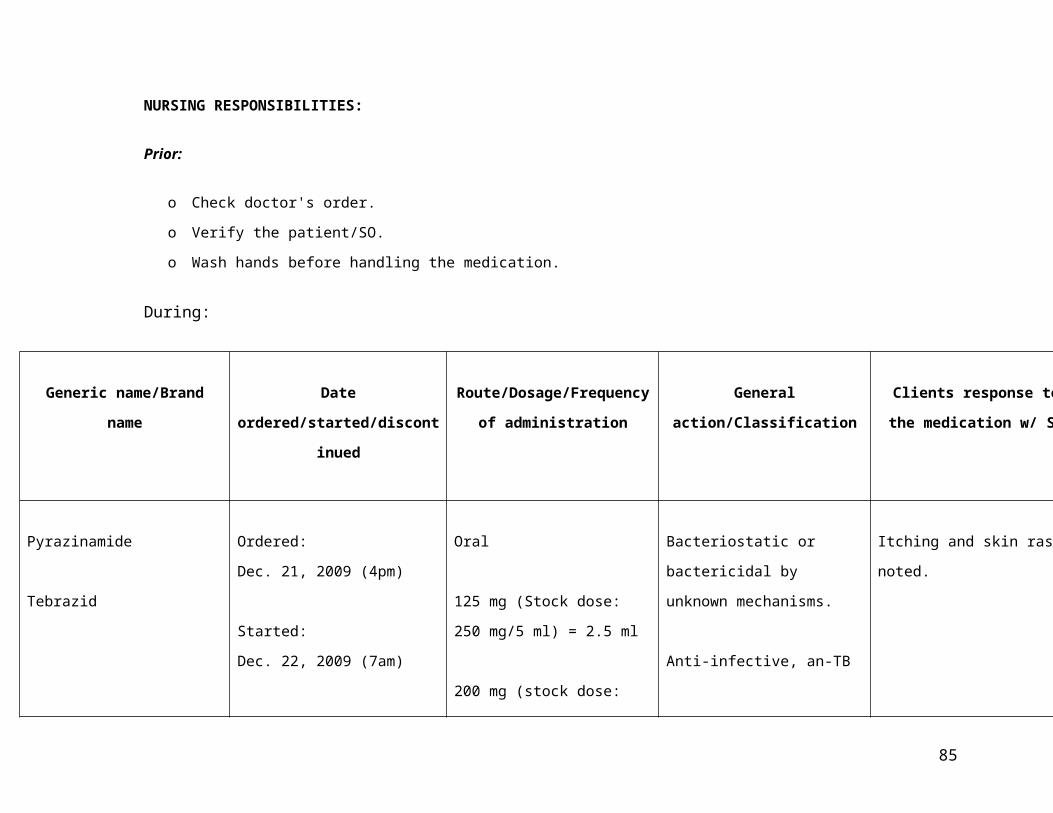
I1> Established rapport.
Vital signs taken and recorded.
Positioned head midline with flexion appropriate for age or condition.
I2> Established rapport.
Vital signs taken and recorded.
Elevated head of bed/position client appropriately
Encouraged frequent position changes and deep breathing/coughing exercises.
I3> Established rapport.
Vital signs taken and recorded.
Discussed eating habits including food preferences such as giving colorful food
Noted total daily intake. As maintained diary of calorie intake, patterns, and
times of eating.
Encourage proper oral hygiene.
Prevent or minimize unpleasant odors.
Weigh weekly and document results.
Give supplemental vitamins as ordered.
I4> Established rapport.
Vital signs taken and recorded.
Determined client’s most urgent need from both client’s and nurse’s viewpoint.
Stated objectives clearly in learner’s terms.
Determined client’s method of accessing information and include in teaching
plan.
Provided written information/guidelines for client to refer to as necessary.
E1> Goal partially met, the patient maintained airway patency but secretions are still
present.
R1> Reinforce above-mentioned interventions.
E2> Goal met, patient verbalized awareness of causative factors and initiated
necessary interventions.
E3> Goal partially met, the patient was able to eat a little.
R3> Reinforce above-mentioned interventions.
E4> Goal met, patient verbalized understanding of causative factors and necessary
interventions.
85

12/21/09
S> 0
O> The patient is asleep .Upon awake, was unable to smile but responsive to stimuli
and cry actively. The patient carries by his mother, with on going IVF of D5 0.3
NaCl 500ml regulated at 56 cc/hr at 400 cc level infusing well on the left hand,
the skin of the eyelids was intact without redness, swelling, discharge or lesion
and eyelashes were equally distributed along the lid margins and curve outward.
No protrusion or sunken appearance. The conjunctiva was smooth and moist.
The chest is symmetrical, no lesions found, no shallow breathing, no sign of
deformities, no presence of mass, no sign of abnormalities, no resonant sound.
Positive rales or crackles upon auscultation. , the skin had a poor skin turgor with
none tenderness, with vital signs taken as follows: Temperature=36.5°C Heart
Rate=125 bpm Respiratory Rate=27 bpm.
A1> Ineffective airway clearance r/t retained secretions.
A2> Impaired gas exchange r/t ventilation perfusion imbalance.
A3> Imbalance nutrition: less than body requirements r/t inability to ingest adequate
nutrients
P1> After 2-3 hours of nursing interventions, patient will be able to maintain airway
patency as evidence by reduced secretions.
P2> After 2 hours of nursing interventions the patient will verbalize awareness of
causative factors and initiate necessary interventions.
P3> After 1 month of nursing intervention, patient will be able to gain weight from 9
kgs to 15 kgs.
I2> Established rapport.
Vital signs taken and recorded.
Elevated head of bed/position client appropriately
Encouraged frequent position changes and deep breathing/coughing exercises.
I3> Established rapport.
Vital signs taken and recorded.
Discussed eating habits including food preferences such as giving colorful food
Noted total daily intake. As maintained diary of calorie intake, patterns, and
times of eating.
Encourage proper oral hygiene.
Prevent or minimize unpleasant odors.
86

Weigh weekly and document results.
Give supplemental vitamins as ordered
E1> Goal partially met, the patient maintained airway patency but secretions are still
present.
R1> Reinforce above-mentioned interventions.
E2> Goal met, patient verbalized awareness of causative factors and initiated
necessary interventions.
E3> Goal met, as evidenced by the patient was able to eat and drink milk regularly.
12/22/09
S1> “medyo hirap pa syang huminga” as verbalized by SO
O> Patient was received on bed, sleeping with an IVF of D5 .3 Nacl 1L at 750cc
level, regulated at 56 gtts/min. monitored and recorded vital signs, fixed bed
linen, changed clothing, kept back dry, assisted in nebulization. Health teachings
were imparted such as proper positioning of thee patient while feeding to prevent
aspiration. Advised significant others of patient to increase patient’s fluid intake.
Positive rales or crackles upon auscultation. Skin turgor is good, when pinched it
springs back to its previous state, with vital signs taken as follows:
Temperature=36.4°C Heart Rate=124 bpm Respiratory Rate=28 bpm.
A1> Ineffective airway clearance r/t retained secretions.
P1 > After 3 hours of nursing intervention, the S.O will identify ways to maintain
patients patent airway.
I1> established rapport
assessed patients condition
monitored and recorded vs
monitored IVF patency and regulation
instructed S.O to put patient in high back rest
provide adequate rest period
kept back dry
changed position every 2 hours
encouraged S.O to perform frequent hand washing
due meds given
E1 > Goal met as evidence by patient was able to maintain a patent airway.
87

12/23/09
S1> “tamang pagaalaga ba ang ginagawa namin” as verbalized by SO
O1> Patient was received sitting on bed, awake, IV out, afebrile with on and off cough
and clear nasal secretions. Vital signs as follows: temperature: 36.2°, HR: 120
bpm, RR: 24brpm. IVF of D5 .3 Nacl 1L inserted at 6:45pm using vasocan g.24
at right hand and regulated at 56ml/hr, hence IV medications was continued. The
skin of the eyelids was intact without redness, swelling, discharge or lesion and
eyelashes were equally distributed along the lid margins and curve outward. No
protrusion or sunken appearance. The conjunctiva was smooth and moist. The
chest is symmetrical, no lesions found, no shallow breathing, no sign of
deformities, no presence of mass, no sign of abnormalities, no resonant sound.
Positive rales or crackles upon auscultation
A1> Knowledge deficit regarding condition, treatment, prevention, self care, and
discharge needs related to lack of exposure to or misinterpretation of information
as evidenced by request for information.
P1> After 2-3 hours of nursing intervention, patient will be able to initiate lifestyle
changes and participate in treatment regimen to improve general well-being and
reduced risk of reactivation of TB.
E1> Goal met, patient verbalized understanding of causative factors and necessary
interventions.
88

VI. CLIENT’S DAILY PROGRESS IN THE HOSPITAL
1. Client’s Daily Progress Chart
DAYS Admission
12-19-09
Day 2
12-20-09
Day 3
12-21-09
Day 4
12-22-09
Day 5
12-23-09
Day 6
12-24-09
Day 7
12-25-09
Discharge
12-26-09
Nursing Problems
1. Ineffective airway
clearance r/t retained
secretions.
2. Impaired gas
exchange r/t ventilation
perfusion imbalance.
3. Imbalance nutrition:
less than body
requirements r/t
inability to ingest
adequate nutrients.
4. Knowledge deficit
regarding condition,
treatment, prevention,
self care, and
89

discharge needs
related to lack of
exposure to or
misinterpretation of
information as
evidenced by request
for information.
5. Impaired gas
exchange r/t ventilation
perfusion imbalance.
Vital Signs
Temperature 36.8°C 36.6C 36.5°C 36.4°C 36.2°C 36.2C 36.4C 36.2C
Cardiac Rate 132 bpm, 128 bpm 125 bpm 124 bpm 120bpm 128 bpm 120bpm 120 bpm
Respiratory Rate 30 cpm 29 cpm 27 cpm 28 cpm 22 cpm 22 cpm 22 cpm 22 cpm
Dx/Lab Procedures
Complete Blood Count #1:
Hgb: 130
Hct: .39
WBC: 9.0
Neutro:0.6
1
Lympho:
0.53
90

Chest X-ray There are
hazy and
patchy
infiltrations
in both
lung fields.
Nodular
densities
in the
retrocardia
c space.
The heart
is normal
in size by
configurati
on,
diaphragm
s,
costopenic
angles
and the
visualized
bones are
intact.
91

Medical Management
IVF: D5 .3NaCl
Nebulization
Drugs
Cefuroxime 250mg/IV
q 8
Amikacin 15mg/ IV q 8
Hydrocortisone
150mg/IV q6
Ampicillin 100 mg/IV
q6
Rifampicin110 mg
(Stock dose: 200 mg/5
ml) = 2.75 ml OD
Pyrazinamide Oral
200 mg (stock dose:
250 mg/5 ml) = 4 ml
Isoniazid Oral
100 mg = 5 ml OD
92

VII. Discharge Planning
The patient was discharged on December 26, 2009. The doctor gave the MGH order at
9:00 am and after settling the bill, the patient was able to go home at 4:00 pm. The
patient was wearing a clean white shirt and brown shorts. His hair was combed but there
was dirt under his fingernails. His vital signs were: T- 36.2°C, HR- 120 bpm, RR- 22
bpm. He was afebrile, with no complaints of pain, with no presence of jaundice.
M > Rifampicin 200/5 syrup 2.75ml OD Pre breakfast x 6 mos.
> Isoniazid 100/5 syrup 5 ml OD Pre breakfast x 6 mos.
> Pyrazinamide 250/5 syrup 4 ml OD pre breakfast x 2 mos.
> Bronchorex ½ tsp TID
> CTAX P ½ tsp BID
>Prednisone 10 mg/5 ml ½ tsp BID
Health teachings:
Instructed patient to take medication with full glass of water. To
enhance absorption.
Instructed patient no to take the medication with milk.
Instructed patient to report blurring of vision, severe gastrointestinal
symptoms, headache, muscle pain, weakness.
Instructed patient to store the medication in a cool environment in tight
container protected from light.
E > Complete bed rest
> Limit activities
Encouraged patient to do deep breathing exercise to promote proper
lung expansion and facilitate proper carbon dioxide elimination.
Instructed patient to avoid strenous activities to avoid fatigue and
instructed patient to resume usual ADLs gradually and as tolerated
93

T > Instructed to follow medical regimen
Instructed patient about the improtance of complying to treatment
regimen.
Instructed patient to do proper handwashing
H > Instructed SO to increase fluid intake
> Advised SO in proper positioning of patient while feeding to prevent
aspiration
> Instructed SO about the strict compliance of therapeutic regimen
O > Advised to have a follow up check-up after 2 weeks
D > Bottle feeding aspiration precaution
> Increase intake of foods high in protein
VII. SUMMARY OF FINDINGS
The nurse researcher was able to know the background of the disease condition
(Koch’s Infection), Know the reasons why such diagnostic procedures and treatments
are performed, Know the progress of the disease, Cooperate in the necessary medical
and nursing interventions, Know the reasons why the patient experiences the signs and
symptoms of the diseases, Know preventive measures in response to the disease so as
to prevent deterioration of the patient’s condition and Participate willingly in the care of
his conditions such as adhering to health teachings provided, Have the necessary
awareness for the condition’s familial tendency and thus perform appropriate activities
that may prevent eventual progress of the disease (for the client’s significant others).
The nurse researcher was able perform a comprehensive assessment of the
patient, enumerate the signs and symptoms of Koch’s Infection, identify and list
diagnostic procedures that would help in the diagnosis of Koch’s Infection, Identify
nursing problems utilizing the subjective and objective cues based on the patient’s
response, Perform appropriate therapeutic interventions for each of the formulated
nursing diagnosis, Have a background of the disease condition, Known the current
94

trends about the disease, Know the incidence, prevalence and mortality rate of the
disease, Identify factors present to the patient that predisposed him to the said disease,
Explain briefly the anatomy and physiology of the disease, Gain proper knowledge and
understanding about the existing disease condition, it’s pathophysiology, sociology and
etiology involved in its acquisition and progression, Identify the difference modifiable and
non-modifiable factors for the occurrence of the disease, Identify the different early
clinical manifestations of the disease condition, Analyze the different laboratory and
diagnostic procedures, their indications to the disease and identify the nursing
interventions before, during and after the performance of the said procedures, Identify
the different signs and symptoms manifested by the client who have had Koch’s
Infection and explain how these signs and symptoms occur, Identify the common
complications of Koch’s Infection and the appropriate preventive measures, Explain the
different treatments or medical modalities and their importance, and different nursing
interventions during the performance of the said procedure, Identify common
medications used as a treatment for the diseases, their mechanism of action, adverse
affects and nursing interventions before, during and after the administration of the
medications, appropriate nursing diagnoses and their corresponding effects for the
disease conditions, Render appropriate nursing interventions to prevent complications of
the disease.
IX. CONCLUSION
Prognosis depends largely on the extent of the disease. Primary, dormant or
limited secondary tuberculosis responds very well to chemotherapy. As with this case of
Primary tuberculosis or Primary Koch’s infection in a one year old child, prognosis is
good as long as the entire course of medication is taken by the patient. There is also a
need to trace and screen contacts or anyone who is in close contact with the patient.
Patient with tuberculosis needs to be isolated while infectious but in this case the patient
can not infect other people especially adults. Since adults have stronger immune
system than children do. But the patient can infect children of his same age because
they have weak immune system. We also have to stress out to the patient or significant
other the importance of having plenty of rest and eating a balanced meal. Once the
patient has completed the entire course of treatment, he should maintain or keep his
95

immune system as healthy as possible. The patient had improved breathing patterns
and lesser secretions when he was discharged.
Primary tuberculosis used to be one of the greatest killers – attacking anyone
who is at risk. Treatment with medications for a period of 6 months has made it possible
to save countless lives.
In this case study, the nurse researcher learned about the disease process, the
microorganism that causes tuberculosis. Also the anatomy and pathophysiology of the
disease as well as the proper management of the disease. The client’s family also was
able to demonstrate behaviors, understanding on how to prevent the recurrence of the
disease and compliance to health teachings given.
Lastly, the nurse researcher concluded that prevention is better than cure,
because it is easier to prevent a disease than to cure it.
X. RECOMMENDATION
Diagnosis of childhood tuberculosis still presents a problem because of paucity of
specific sign and symptoms clinical evidence and difficulty in sputum collection.
Tubercullin Testing seems to be an important diagnostic tool. Since a majority of our
population. Whether used in hospital, health centers, the test needs careful training of
medical health providerl and adaption of precise and sophisticated technique.
The findings suggest that the researchers offer these recommendations:
1. Physicians, nurses, other health care providers and the people should have an
orientation on the signs and symptoms and the different factors that contribute in
the disease condition.
2. To those who are at risk of acquiring the disease, that they may be able to know
the signs, symptoms, factors that aggravate and alleviate the disease condition
and different treatment options that they may account into.
96

3. To the patient’s significant others, they must give support and help the patient in
achieving optimum nutrition as well as to provide support and effective coping
mechanisms to reduce stress and depression.
4. Student Nurses, caring for patients, must provide holistic care to help the patient
achieve optimum well being and maintain health.
XI LEARNING DERIVED
As a professional nurse, this study showed me the importance of early detection
of diseases that may lead to more serious conditions if it is not properly managed or
treated. Giving care to a patient whether pediatric, geriatric, a medical case or surgical
case makes no difference. Rendering care to everyone who needs it is a real sense of
responsibility. In making this case study, I was able to work well because I know for
myself that I did my best for my patient. We can say that nursing is significant
therapeutic and dynamic process. It is therefore significant for the nurse caring for the
patient to wholeheartedly understand what he is doing like in carrying out some basic
skills in relation to identified goals, comfort and care, interventions and prevention of
illness.
Bibliography
Smeltzer, Suzane, et al.2000.Brunner and Suddrath’s text book of Medical Surgical
Nursing. 11th Edition.
Diseases 3rd Edition spring house .2000.
Seeley, Tate, Stephen.2004.Essentials of Anatomy and Physiology 5th ed.
Nowak, Thomas., Gordon handford.Pathophysiology Concepts and applications for
health care professionals.3rd ed.
2007.Mims.11th ed.
Luxner,karla.2005. Delmar Maternal and infants care plans.2nd ed.
Elkin,perry,potter.2004.Nursing Intervensions and clinical skills.3rd edition
97

Schnell, Leeuwen, Kranprits. Davis’ Comprehensive Handbook of Laboratory and
Diagnostic Tests with Nursing Implications.2003
www.wikipedia.com
www.yahoohealth.com
www.google.com
98

99