prevention of blindness - wpro iris...programmes for trachoma control and prevention of blindness....
TRANSCRIPT

World Health Organization
Prevention of Blindness
Report of the 4th Inter-Country Workshop
Luang Prabang, Lao PDR
February 4-8, 2002
Dept, of Ophthalmology, Juntendo University
WHO Collaborating Centre for PBL, Tokyo

Meeting
Field visit Health care network hospital
1 '

Programme of the 4th Inter-country Workshop on Prevention of Blindness
The First Day (04/02 Mon)
8:30 Registration
"Phu Xi Hotel", Luangprabang
Lao People's Democratic Republic
4 to 7 February 2002
Agenda and Programme
9:00 Opening ceremony
Addressing message
1. Mr. Chansy Phosikham, Gover~or of Luang Prabang
2. Dr. G. Deodata, WHO Representative to Lao, PDR
3. Prof. Atsushi Kanai, WHO Collaborating Centre for PBL
4. Dr. Ponmek Daraly, HE. Ministry of Health
9:30 - 1 0:00 Coffee break
1 0:00 - 11 :30 Selection of Workshop Officers
· Chairperson, Co-chairperson and 2 reporters
· Introducing participants
Keynote lecture (30 min for each)
1) Global situation of PBL and Vision 2020 Dr. S. Resnikoff, WHO/Geneva
2) Healthy City Project Dr. Ogawa, WHO/Manila
11.30- 12:30 Country presentation (20 min. for each)
'The present situation of blindness prevention, emphasising on ocular infection
Cambodia
Laos
VietNam
12:30- 13:30 Lunch
- 1-

13:30- 14:30 Country presentation (cont.)
Myanmar
Thailand
Discussion
14:30- 15:30 Panel discussion (1)
The Perspective of blindness prevention in the sub-region, new challenges,
"Strength "and "Weakness" of the national activities
Panelist: Representative from Cambodia, Laos, Thailand, Myanmar and
VietNam
Coordinator: Dr. K. Konyama (Japan)
Reporter Dr. Patpong G (Thailand)
15:30- 16:00 Coffee break
16:00- 17:00 Panel discussion continues and conclusions and recommendations
The Second Day (05/02 Tue)
8:30- 9:30 Special lecture (1) "Ocular management system development"
Prof. S. Ohno, Hokkaido University.
9:30 - 1 0:00 Special lecture (2) "Recent advance in University management"
Prof. S. Ohno, Hokkaido University
10:00 - 1 0:30 Coffee break
1 0:30- 12:00 Group discussion: Topic one: Ocular infection management in PEC network
· Group A Community and the first level of referral
· Group B Second and tertiary level of referral
· Group C Research and development
12:00- 13:00 Lunch
13:00 - 14:00 Group discussion continues
-2-

11:00- 15:00 Presentation of group discussion topic one, "Conclusions and recommendations"
15:00- 15:30 Coffee break
15:30 - 17:00 Panel discussion 2
Quality assessment of cataract service (60 min)
Panelist: One representative from Cambodia, Laos, and VietNam, Myanmar and
Thailand are also invited.
Dr. R. Pararajasegaram, Dr. K. Konyama
Coordinator: Prof. Ton Thi Kim Thanh (Viet Nam)
Reporter Dr Nguyen Xuan Tinh (Viet Nam)
The Third Day (06/02 Wed)
Morning Field visit
All participants visit the health care network in Luangprabang province.
Afternoon Free afternoon for "Discover Luangprabang".
The Fourth Day (07 /02 Thu)
Morning
(8:30 - 12:00)
Afternoon
All national delegates will meet NGO representative
Programme will be prepared by Mr. Peter Renew (CBM):
All NGOs delegates are welcomed and meet the workshop participants
Each NGO working in the sub-region presents own ongoing activities in the
sub-region.
13:30 - 14:30 Preparation of conclusions and recommendations
14:30 - 15:00 Conclusions and recommendations of the workshop
15:00- 15:30 Coffee break
15:30 - 16:00 Closing ceremony
-3-

IAPB Meeting
International Agency for the Prevention of Blindness (IAPB) Meeting is scheduled for the three countries
in the sub-region of Indochina, Cambodia, Laos and Viet Nam)
Venue: Phu Xi Hotel, Luangprabang, Lao PDR
Date: 8 February 2002
IABP Officers in the sub-region will prepare agenda. All national and NGO delegates of the 41h
Inter-country Workshop are welcome to join the meeting.
Agenda for the IAPB meeting on Friday 8th February in Luangprabang
8:30- 12:00
Welcome address by the IAPB/WPR chairperson and selection of the session officers.
1) Agenda 1: Ocular Infection management
Presentation: Cambodia, Laos, and VietNam
2) Agenda 2: A glance on the trachoma situation
Presentation: Cambodia, Laos, and Viet Nam
12:00- 13:00 Lunch
13:00- 16:30
1) Agenda 3: Cataract situation and intervention
Lecture by Dr. Pararajasegaram
Presentation: Cambodia, Laos, and Vietnam.
2) Subject 2: Situation of refractive errors and service
Presentation: Cambodia, Laos, and VietNam
16:45- 17:30 Conclusions and recommendations
17:30 Closing address and words of appreciation by the IAPB/WPR chairperson
-4-

Acknowledgement
The Organizers of the 41h Inter-country workshop in Luang Prabang Lao PDR wishes to
express our deep gratitude to the Ministry of Health Ophthalmology Centre, the Government
of Luang Prabang and the National sub-committee for Prevention of Blindness of their
supports in hosting the Workshop. Especially, we much appreciate Dr. Vithoune
Visonnavong, Director of Ophthalmology Centre and his staffs for the remarkably work they
did in organizing and making the Work-shop a success.
To WHO Head quarter in Geneva, Collaborating Centre Juntendo University Tokyo, Japan,
the WHO Western Pacific Regional Office and WHO Lao PDR office for supporting the
Workshop.
Unfortunately, this Workshop was Last for Prof. Kanai as you may know he would be retired
in March 2002.
To all participants and representatives of non-governmental organizations, for their
contributions in making the Workshop a success.
Thank you.
-5-

The 4th Inter-Country Work Shop on Prevention of Blindness
In Luang Prabang
Table of Contents
Contents
Acknowledgement ····································· ··································································· ··· 5
List of Annexes ········································ ······································································ ··· 7
The Report of the Fourth Inter-Country Workshop of Prevention of Blindness ............. 10
-Exclusive Summary
-Objectives
-Organizers and Administration
-Participants
-Expected outcome
Conclusions and recommendations ·············································································· ··· 12
-Refraction system development
-Ocular infection management
-Cataract Programme
-Importance of Mid-Level-Personnel in eye care
-Workshop and the support from collaborating centre
-World Health Organization/WHO Collaborating Centres
-International Non-governmental Organization
-6-

List of Annexes
1. Workshop Programme/ Agenda 1
2. List of Participants/Observer/ NGO's ................................................................ 15
3. Welcome message at the opening ceremony ................................................... 19
1) Mr. Chansy Phosikham, Governor Luangprabang province, Lao, PDR ....... 19
2) Dr. Giovanni Deodato, WHO Representative to Lao, PDR ........................... 21
3) Prof. Atsushi Kanai, Director, WHO Collaborating Centre for PBL, Tokyo ... 25
4) Dr. Ponmek Daraloy, HE. Ministry of Health, Lao, PDR ............................... 27
4. Key-note Speech (1st day) ................................................................................. 29
1) Dr. Serge Resnikoff, Representative of WHO Geneva HQ
"Global situation of PBL and Vision 2020 " .................................................... 29
2) Dr. Hisashi Ogawa, Representative of WHO WPRO, Manila
"Healthy City Project" ...................................................................................... 35
5. Country Report (1st day) ..................................................................................... 37
1) Cambodia ....................................................................................................... 37
2) Laos ................................................................................................................ 46
3) Viet Nam ......................................................................................................... 51
4) Myanmar ......................................................................................................... 58
5) Thailand ·········································································································· 61
-7-

6. Panel discussion (1st day) "Ocular Infection" .................................................... 66
Quality Assessment of Ocular Infection (Sample) ............................................. 71
1) Cambodia ............................................................... ................. ... ... .............. ... 7 4
2} Laos ................................................................................................................ 78
3) Viet Nam ..... ............. .... ... ........................................ ............. ........................... 82
4) Myanmar ......................................................................................................... 85
5) Thailand .......................................................................................................... 89
7. Group Presentation (2nd day) .............. ................. ............. ...... .............. ... ... ....... 93
Topic 1: Ocular Infection management in PEC
-Group A "Community Level" .............................................................................. 93
-Group B "Provincial Regional Level" ................................................................. 94
-Group C "Central Level" .................................................................................... 95
Topic 2: Quality Assessment of Cataract Service ............................................. 96
1) Cambodia ....................................................................................................... 96
2) Laos ................................................................................................................ 98
3) Viet Nam ......................................................................................................... 102
4) Myanmar ......................................................................................................... 1 07
5) Thailand .......................................................................................................... 1 08
8. NGOs Session (41h day) ...................................................................................... 115
-8-

9. Conclusions and Recommendations (4th day) ···················································116
1) Cambodia ....................................................................................................... 116
2) Laos ................................................................................................................ 117
3) Viet Nam .......................................................................................................... 118
4) Myanmar ......................................................................................................... 119
5) Thailand .......................................................................................................... 120
10. The Report of IAPB Assembly for the Sub-Region of Indochina (4th day) ........ 121
-9-

The Report of the Forth Inter-country Workshop on Prevention of Blindness Luangprabang, Lao PDR, from 4 to 7 February 2002
Exclusive Summary
Tokyo centre initiated the three countries in Indochina subregion to meet at a two-year interval since 1995. The first meting conducted at Vientiane 1995. Then the second went to Phnom Penh in 1998, and Hanoi 2000. The first of the second round the venue returned to Lao PDR again. The meeting took place in Luangprabang, its old capital, Luangprabang from 4 to 7 February 2002. The Tokyo centre supported all travels and local costs. The very purpose of the meeting is that providing those who are working at operational level of these countries to expose each other. That might facilitate closer friendship personally. Also it provides exchanging and sharing their experiences in blindness prevention. Usually this level is hardly to go out of country even the neighbouring countries. This time Myanmar was first time invited as observers. There were two ophthalmologists attended the workshop from the National Programmes for Trachoma Control and Prevention of blindness.
As a traditional, the last day of the workshop it programmed a special session that all international NGOs working in the subregion are invited and to meet with the national delegates.
The workshop also provided an opportunity that a subregional assembly of IAPB to follow immediately after the workshop. Its report is also attached.
Objectives of the workshop were:
General objectives:
To assess the past and the present activities of the National Programmes for the Prevention of Blindness in Cambodia, Laos and Viet Nam in order to accelerate farther progress in the future with special attention to Vision 2020 initiative. The delegates will exchange their new experiences and strengthen further co-operation among them.
Special review and discussions were centred on the following areas:
1) Review the present situation of ocular infection (trachoma is excluded) and discuss development of its control at various levels of eye care facilities.
2) Manpower development covering ophthalmologists and mid-level personnel in eye care. 3) Cataract services, its costs and the sustainable future 4) Sub-regional mutual collaboration in other areas.
In completing the report of this workshop, Tokyo centre would like express deep appreciation to the Ministry of health, Government of Lao People's Democratic Republic and the entire national who devoted for the success of the workshop and their ward hospital to all delegates.
At the end of the workshop all participants concluded to request generosity from Tokyo centre that the workshop would continue as a means of promoting blindness prevention in the subregion.
-10-

Organiser and Administration:
Chief organiser: WHO Regional Office for the Western Pacific Ministry of Health, Lao PDR WHO Collaboration Centre for Prevention of Blindness, Tokyo Ophthalmic Care Centre, Vientiane
Secretariat: Tokyo Collaborating Centre for Prevention of Blindness Institute of Ophthalmology, Hanoi Institute of Public Health Ophthalmology, Nakhon Ratchasima
Venue: To be announced.
Time: 4 - 8 February 2002 (8 February will have special sessions for "IAPB WPR subregional meeting for Cambodia, Laos, and VietNam).
Participants:
National delegates are invited from Cambodia, Laos, and Viet Nam each five ophthalmologists and from Ministry of Health or health administrators, Ophthalmic Nurses. All must be those who now involve in prevention of blindness activities. In total 15 participants.
Five observers are invited from Myanmar and Thailand comprise of ophthalmologists and health administrators, and Ophthalmic Nurses.
Additional participants are encouraged from Laos at own expenses but not more that ten selected by Ophthalmic Care Centre, Vientiane.
Expected outcome:
It is expected that the workshop will come out with a concrete subregional scheme enhancing the developing, collaborating in the following areas of blindness prevention and eye health prevention and promotion. Especially this will have Myanmar for the first time to join the workshop.
1. Enforced sub-regional moves on prevention of blindness. 2. Strengthening TCDC in the sub-region, regarding
Manpower development Refraction service development
3. Ocular infections control system development Plan of co-operations from NGOs.
-11-

Conclusions and Recommendations:
The Fourth Inter-country Workshop on Prevention of Blindness was conducted at Luang Prabang, Lao PDR from 4 to 7 February 2002. Participants included national delegates from three countries in the Indochina sub-region of the WHO Region of the Western Pacific. In addition Thailand and Myanmar were invited and participated as observers. In total 25 ophthalmologists, five from each country were at
the meetinQ.
The workshop also invited international NGOs working in the sub-region and thus provided an opportunity for INGO representatives to meet with their counterparts at the national operational level. The key themes selected for the meeting were:
G The present situation of ocular infections and strengthening or development of control systems in the national programmes for the prevention of blindness
• The cataract programmes with particular emphasis on quality of surgical outcome.
Since the outset these workshops had been aimed at the programme managers, who are ophthalmologists and actively involved in blindness prevention and providing eye care at servicing level, to come together. Such past workshops which facilitated exchanging experiences have proved a highly beneficial for mutual understanding and friendship, which is a starting point for TCDC to be built at the operational level. Through such meetings the areas of cooperation could be first identified. The results of contact made and views exchanged result in conclusions and recommendations that could be taken to their respective national policy/strategy making level. It is also provided useful information to the group of international NGOs working in the sub-region. 1. Refraction system development
The third inter-country workshop which met at Hanoi in 1999, recommended the development of refraction systems as a joint efforts between Institutions in the Region. Reports presented at this workshop showed that there was substantial progress in this regards in all countries.
The Hanoi Institute of Ophthalmology and Karat Regional Hospital both had refraction clinics. These plan to start their training roles soon. It also includes TCDC for the neighbouring countries. To that end the sub-regional cooperation and national efforts should continue. The development should be hastened and widened to initiate new action elements. Such components such as eye care for children, especially amblyopia and strabismus services can follow provided there was a strong refraction service base.
2. Ocular infection management Ocular infections have remained a common ocular condition causing various problems. It may lead to a serious outcome like corneal blindness and destruction of the whole eyeball. Its current management in participating countries, in general, needs updated knowledge and technology, not only in ophthalmology, but also in microbiology, immunology and pharmacology.
However, all participants recognized that primary prevention is the best strategy and must be initiated at community level. Hence, PEG must be reviewed and strengthened to meet this goal.
All countries also concluded that their laboratory facilities must be upgraded to cope with wide spectrum of causative agents.
-12-

The participants worked out together a plan of action for an updated system of ocular infection management that could be incorporated at the various levels of eye facilities. These are shown in detail in the attached matrices.
For such a new development the need to develop and or revise surveillance systems was emphasized. This could cope to study trends over time. Existing eye care information system must be revised if necessary to include new indicators concerning ocular infection.
Secondary prevention will require laboratory support of varying complexity at all levels. That will ensure better treatment and outcomes. However, appropriate technology must be at the core of the new scheme. Availability of minimum set of relevant anti-microbiological drugs must be assured after reviewing the current situation.
To facilitate all the above it would need the presence of the suitably trained mid-level eye care personnel
Re Training would be necessary for all non-ophthalmic medical and non-medical health personnel. Public education must also be planned and implemented.
3. Cataract programme In most countries cataract intervention programmes seem to have made substantial progress in term of surgical volume. However, further efforts must be made so that output can meet annual requirements In addition the quality aspect needs a standardized assessment method for the sub-region.
Programme sustainability is a remaining issue and cost sharing should be given more attention in all countries. Cataract service therefore, must be made to be self-supporting, yet the best possible quality is assured within available resources. Regional and national efforts should give more awareness to this point.
4. Importance of MLP in eye care All countries accepted that MLP in eye care is essential for the success of blindness prevention. This time it was reiterated that laboratory strengthening for eye infection management need their presence in laboratory work.
Therefore, the development of these personnel in sufficient numbers is a high priority area in blindness prevention. TCDC in this area must be initiated.
5. Workshop and the support from collaborating centre The participants appreciated the role and support given by the WHO Collaborating Centre to this Workshop.
The organizers and participants felt justified that these workshops were really action oriented as evidenced by the follow up actions and achievements following the last workshop in Hanoi which recommended that Hanoi and Korat institutes would start refraction services.
-13-

It was reported this time that now both have implemented this recommendation and the training programmes will start soon. In Lao PDR as well training at the provincial eye units had been completed.
It is expected that the recommendation made at this meeting in relation to the prevention and management of ocular infections will be implemented in individual countries and reports will come in the next workshop. This would be the justification for requesting the Tokyo centre for the support to the next workshop.
+World Health Organization/WHO Collaborating Centres WHOs initiative in the past had made individual countries to systematically begin the national programmes.
The participants noted with appreciation the technical assistance provided by WHO (Global, Regional and National levels), and by the WHO Collaborating Centres to the participating countries in programme development for prevention of blindness.
It was urged that this be further enhanced through providing technical guidelines, training material, assessment and monitoring outlines and assistance with relevant research studies.
+International Non-Governmental Organization The INGOs play an important complementary role in programme activities in the participating countries, assisting governmental efforts. All participants appreciate the continuing support of NGOs for the progress of the national programmes. Moreover, it seems that the workshop provides a useful opportunity for NGOs to access the real situation in individual countries concerning relevant action plans based on the country needs. Collaboration of NGOs must be made to meet the real need. For this reason their presence in the workshop is mutually beneficial.
The participants stressed the need for closer cooperation and better coordination at the national level, among the various INGOs, on the one hand, and with the National authorities and with WHO on the other, to ensure the optimal utilization of resources, through need based planning and implementation.
-14-

No Name
Cambodia
List of participants, The 4th Inter-Country Workshop for PBL Organization/Mailing Address TEUFAX
4-8 Feburary ,2002 Luangpranbang
E-mail Address
} __ .Q~~I~-g~-~~-~-~~Qg_______________________ g_~9l~~?-~,.!:~~~~!:l!i~~-~~.§~!:l-~!:l-~~:>_g9_f!l_~~t.!~~~~!:l_9Q.~~-~!:1_9_t_i_~~P..i!?L _____ .:T..: _ _?_~?_::]_~~-~!?..~? ____________ Q!~~~-~!_g?~~9-~~t~l~~~~:~~-----? __ .Q~:__l:?::>_§~J~-~------------------------------ ~~-g-~~-<?!}..9_ti_~~P..i!?J~_!?~f?.§.i!~~!:l!_<?!_9..e~-~~9!~~l9_9¥ __________________________ .f..:_.?_~?::J_~.?-~9Z~§. ____________ Q!?_~~-~?_g?.@.~~-~~~~~~s:~:~~-----~- .Q~:I~-~-~-~~~!:lJ(J~~~i~?l_~-~~!9!)________ !:I~-~~.§9!_~-~~9~<?~-~~~?-~<?~-~-t!~~.P..~?l ________________________________________ .!..~.?-~?_:~~::~-~~~~~----------- --------------------------------------
:l __ .Q~:_-~.9.>.:_~-~!}..g_____________________________ _IS.§.~9-~~!:~~~!1-~~-!:i9.?.Ei~~~-Q.~p-~~~~!}_~9!_9.E~!~-~~f!1_<?!<?.9.>.: ____________________ :T._:_?_~?::J_??..~!-~?~------------ !}_ID'_f!1_~!:l_q@_~9!!!!~il:~9_f!l __________ _
5 Dr. Touk Barang Head of BMC Eye Unit, No. A30 behind post office, F: 855-12923346
Samaki St. Sisophan. Banteay, Meanchey, Cambodia
Laos
6 Dr. Soukhanthamaly Eye Hospital Savannaknet Province T: 856-41-212216
--- -------------------~-~9-~~~~~-~~~~~~----- ------------------------------------------------------------------------------------- .!:~?-~~-=-~!:?_!~~~~----------- ll~~!~)(~~~~~~!~J:~9-~--------------7 Dr. Siphetthavong Srisaleumsack Deputy Director, Ophthalmology Center, Ministry of Health T: 856-21-612000
...... Lao P.D.R F: 856-21-612079 laoooh@>laotel.com ~ --- --------------------------------------------- ------------------------------------------------------------------------------------- ·-------------------------------- --------------------------------------
8 Dr. Khamkhoune Holanouphab Ophthalmology Center, Ministry of Health T: 856-21-612000
Lao P.D.R F: 856-21-612079 [email protected] --- --------------------------------------------- ------------------------------------------------------------------------------------- ·-------------------------------- -- ---------------- ------------------9 Dr. Gomoua Kaoleng Xieng Khouang Provincial Hospital T: 856-61-312166
Lao P.D.R F: 856-61-211375 --- --------------------------------------------- ------------------------------------------------------------------------------------- ·-------------------------------- --------------------------------------1 0 Dr. Vithoune Visonnavong
Vietnam
Director, Ophthalmology Center, Ministry of Health
Lao P.D.R
T: 856-21-612000
F: 856-21-612079 [email protected]
}_! .Q~:I~9n._!?_~y_fS!~n.________________________ _t_i_~~~J~!:l-~_<;?l!Y_~y~_Q~!:l!~! ______________________________________________________ !..:_?_--~~§.~~~? _________________ -~i~~~~?Jg_~~-~~!:~!:1 ______________ __
12 Dr. Nguyen Chi Dung National Institute of Ophthalmology (N.I.O) 85 Batricu St. T/F: 84-4-8225527
Hanoi, Vietnam. [email protected] --- --------------------------------------------- ------------------------------------------------------------------------------------- ·-------------------------------- --------------------------------------]_~ .Q~:-~.9..~Y~~-g~~~-Q.9! ____________________ _l?_~!:l.§.~g_,Ey~_lj~~Pl!9!·_.?Z~!§._~~i!~-~!:l.!!._~!!__l:?.§.~?-~g_g~tY.;~~~!~?-~------------- :T._:_?_~:?-~!§.1?..~?~------------ ~~~-~o!..~?!~¥9-~9~:_~9!!:1 ___________ _
14 Dr. Ha HuyTai National Institute of Ophthalmology (N.I.O) 85 Batricu St. T /F: 84-4-8225527
___ --------------------------------------------- _lj_~~~~-~J~!~-~~~------------------------------------------------------------------ ·-------------------------------- S:~i~?-~~Y_f!l_~.!!_QlY!l~:~!:l ___________ _ 15 Dr. Nguyen Xuan Tinh National Institute of Ophthalmology (N.I.O) 85 Batricu St. T /F: 84-4-9438004
L-.L._ ____________ __~..H:_:.=:an:..:.:o::.:;i,'-V:..:i.::..et:.:..:n.::.am:.:.:.:.... ___________________ .~.,_ ________ __J~t9_~!~i·_~i~!.b.~!:l-~@-~!:l.:Y~!:l;Y_~------

No Name Organization/Mailing Address
Thailand TEL/FAA
4-8 Feburary .2002 Luangpranbang
E-mail Address
~-~ Q~~I~~~-C:.~.?J_~!-~~P_l:!!?_~~.?..~~------------- Jil_~!i!~!~-~t£:~-~llc h_~§!th Ophthalmology, Korat, Thailand T: 6644-272648 [email protected] --- -------------------------------------~--------------------- ·-------------------------------- --------------------------------------17 Dr. Werasak Anutraungkool Department of Ophthalmology, Khonkaen Hospital, Thailand T: 6643-336789 [email protected] --- -------------------------- ------------------ ------------------------------------------------------------------------------------- ·-------------------------------- ------------------------------- ------_:1_~ !-2£~f?_t.P..~!1_9_CA~!I.?..~?-f!.~~~---------------- _'(.?._l.?.__tj~~PJ!§!._:!::~.?..i!§~~---------------------------------------------------------- ::C:_~-~?-~:.?_:1_~?-~? ______________ R?!R~r:!.9.9.@~9_t_f!l_~~:99_12! _________ _ _:1_~ !2£~-~~.E?l~-~-f3._~iy~~§_____________________ _l?_~!?.?..r:.t_f!l_~~!_9L9..t>!:.t_~§!~9J9_9L!}_q9_r!_t_~§l._r:_i_!::!9~elt_~~-!-~?l~~~~--------------- I:_~-~="-~:.?i~?-~? ______________ .?_l:!R~~~~.@~!::?!!~?.:~~8!1_·.9.~.:!~----20 Dr. Malee Viwathanatepa Faculty of Medicine, Khonkean University, Thailand T: 6643-348383 [email protected]
Myanmar
21 Dr. Ko Ko Tin Yangon Eye Hospital, Yangon, Myanmar T: 951-553955 (Home)
--- --------------------------------------------- ------------------------------------------------------------------------------------- .JC~~~~:~~~~9-~-(~~~l~~~~!V- --------------------------------------22 Dr. Kan Nyunt Yangon Eye Hospital, Yangon, Myanmar T: 951-553955 (Hospital)
--- --------------------------------------------- ------------------------------------------------------------------------------------- .JC~~~~:~~~~9-~-(~-~~l~~~~!V- --------------------------------------~~ !2~~~~~-~?!_!_~~-------------------------- !:~~2-~Yi~ll~?_f!.~~r~~-f!l-~~------------------------------------------------------- .JC~~~~:~~:?_!?_~!_____________ --------------------------------------?_~ !2~~~~-~-~~9_:!::~5:~------------------------ !:~~2-~-~~~9-~~!l_S?)d!_~~?_f!.~?! ________________________________________________ .JC~~-~~:~~=?-~~1:~------------- --------------------------------------25 Dr. Khin Ohn Han Mandalay Eye, Ear, Nose and Throat Hospital, Myanmar T: 951-2-31203 (EENT)
T: 951-2-38286 (Residence)
Japan
26 Dr. Shigeaki Ohno Professor &Director, Dept, of Ophthalmology, Hokkaido University T: 8111-706-5944
Graduate School of Medicine. Sapporo, 7-15Jyo, Nishi, Kita-ku, Sapporo
___ --------------------------------------------- _t:f-~~~~~~92_9~9=?-~?-~------------------------------------------------------------- .£:~?_!~_!:?~-~=9~~~----------- ~~~-~?-~~~~:~~~~-~?l~~~.:ue ______ _ 27 Dr. Schinichirou lmaizumi Director, lmaizumi Eye Hospital, 20-9, Doumae, Kouriyama, T: 8124-922-0665
Fukushima, Japan 963-8877 F: 8124-935-5550 --- --------------------------------------------- ------------------------------------------------------------------------------------- ·-------------------------------- --------------------------------------28 Dr. Takayuki Momose Dept. of Ophthalmology, Juntendo University T: 813-3813-3111
___ --------------------------------------------- -~:!:~ __ t:f?..~R~~-~~-~!.<Y..~:~~_,_I~~1~!-~?P..§!l __ ~!~-:.~~~! ____________________________ f::_?_!9:~~_:1_?:9~~Q ___________ --------------------------------------29 Dr. Keiko Fujiki Department of Ophthalmology, Juntendo University 2-1-1 T: 813-5802-1093
(PhDoctor) Hongo, Bunkyo-Ko. Tokyo, Japan 113-8421 F: 813-3817-0260
Ministry of Public Health
~-Q P-~~£:9_~~~~-1?-~~~~~y______________________ -~i~i_?_~~r:..-~l~l~!~~-~!£~-~~s:_!:!~~~t!:__~?~£:.:~~~---------------------------------- !Jf:._~?~:~~:~!±Q9_~--------- ~~~-r!~5:~.@~~~!~l~~?_f!l _____________ _ ~! Q~~-~9-~~~t~!:IJL__________________________ -~ii1J.:>_t_ry_~~S:!_~!~~~~~-~lr:!l~!~-~!£~~!is:_!:!~~~t_~-~?~£.:~~~--------------------- !!.!::._~?~:~]:~!±99_~--------- [email protected]_~~!~L~9_f!l _____________ _ 32 Dr. Sommone Phounesavath Director, Dept. of Curative Medicine, T/F: 856-21-217848
___ --------------------------------------------- -~i!!i_:>_t!}'_s>!_!:-:!~~~!~2-~-~~-E-_!;?.:f! ___________________________________________________ .~~~l~!::~~~~-:.~9:~!~~?-~------ --------------------------------------33 Dr. Bounepheng Ministry of Health, Lao P.D.R T/F: 856-21-217848

No Name
Governor of LuangQrabang Province
34 Mr. Khamdua Yiakuanohervang
WHO
35 Dr. S. Resnikoff
--- ---------------------------------------------36 !2~~-F3~-~~~~-~~i~-~~g-~~?~---------------37 Dr. Hisashi Ogawa
--- ---------------------------------------------38 Dr. Giovanni Deodato
WHO Collaborating Centre1 To~o
39 Prof. Atsushi Kanai
--- ---------------------------------------------40 Dr. Kazuichi Konyama
--- ---------------------------------------------41 Dr. Yoshimune Hiratsuka
Observers ··--· -·
42 Dr. Khamsing Keothongku
--- J~~~J~-~Y~-~~~!9!) ________________________
43 Dr. Sombath Darasouk ---------------------------------------------
44 !2~~52~-~~t~~~-~-~-~~~~~~~9~------------45 Dr. Somchit
Organization/Mailing Address
Vice Governor, Luang Probang Province, Lao PDR
WHO Coordinator, Prevention of Blindness and Deafness
-~-~~~-~]-~-~~~-~Y~-~?l-~-~1~~~!!~~-~-----------------------------------------------~!2~-~-ti:_~?-~!-~~-~~Y-~-~!J_~~J!~~!l?_~g---------------------------------------WHO WPRO Adviser, WHO Regional Office for the Western Pacific
United Nations Ave, P.O. Box 2932,
~9~9-~~~~~-!:~!~P~~~~~---------------------------------------------------------Representative WHO Laos, P.O. Box 343
Vientiane Lao P.D.R
Professor &Director, Department of Ophthalmology, Juntendo University
-~=!~?_!j~~g_q~-E?~-~~)[q:~~:_lC9_~¥9J_~~e~~-!~-~:?~~~----------------------------Course Director, Department of Ophthalmology, Juntendo University
~=1~? __ E?~-~~~q=~~-!j~_~g_q~JC9_~¥92_~9Je9_~_!1_~:~~~1 _____________________________
Course Secretary, Department of Ophthalmology, Juntendo University
3-1-3, Hongo, Bunkyo-Ko. Tokyo, Japan 113-8321
Champasack Province Hospital, Lao P.D.R
-------------------------------------------------------------------------------------_':5~~~~':l!!.9_~!_qY!~~-~-I::f._q~.P.!!?l:._~?~f:g_~'3_ _____________________________________
_i?~ll~~-~~.Y.:~Y_!:~~Yl~.£~-t!~~~~~~l-~9-q_~~Q~~------------------------------------Eye Hospital Saya Boury Province, Lao P.D.R
TEUFAX
T/F: 856-71-212407
Mobile:856-20-570003
T: 41-22-791-2111
F: 41-22-791-4124 ·--------------------------------T: 41-221-7913886 ·--------------------------------T: 632-528-8001
F: 632-521-1036 --------------------------------T: 856-21-413431
F: 856-21-413432
T: 813-5802-1092
F: 813-38170260 ·--------------------------------T: 813-5802-1 092
F: 813-38170260 --------------------------------T: 813-3813-3111
F: 813-5689-0394
T: 856-31-212018
F: 856-31-212018 ·--------------------------------T: 856-51-212084 ·--------------------------------T: 856-54-212154 --------------------------------T: 856-74-211081
4-8 Feburary ,2002 Luangpranbang
E-mail Address
!5:~~1~~~~-~~~-q~~~----------------~~!9!_~~~~~~~---------------------
~~~-~~~~!~!~~e~9~~~~J~) ________
[email protected](2ro.who.int
--------------------------------------
l~L~~~~~g~~1~~9!~·-~~j_t2__ __________
------------------------------------------------------------------------------------------------------------------

...... 00
No Name Organization/Mailing Address
NGOs
46 Prof. Patrick Ho IAPB Regional Co-Chairman, Lions Club International
TEUFAX
T: 752-2501-0919
4-8 Feburary ,2002 Luangpranbang
E-mail Address
Foundation, Sight First Technical Admises, Hong Kong F: 752-2501-0666 [email protected] --- --------------------------------------------- ------------------------------------------------------------------------------------- ·-------------------------------- --------------------------------------47 Dr. Richard Millar Regional Consultant, Orbis, 79/72 Patumwan soi, T/F: 662-6538394 [email protected]
--- --------------------------------------------- !:~~y~~~9l_~-~9-~~-~~~~~?!~~J!-~~~9-~9~--~9~Q9_J[~~~9-~~---------------------- -------------------------------- -~~~?!_~~-~~:~~:~9-~---------------~~ ~~~~~-~~~-~-~~~~~~g______________________ !:!~9:~~~~!~~!-~~~9-~~~~9~~9-~~-~?~~:-~!~-~-~-~-~~~~~J[~~~-~~~!~-------- .JC~?-~9:~~~~?-~? ______________ s!~9-~~-~~~~Y-~:~:g ________________ _ 49 Mr. Stuart Shepherd CBM, P.O. Box:5 Kew vic 3101, Australia T: 613-98174566
--- --------------------------------------------- ------------------------------------------------------------------------------------- ~:-~-~?:~~_:1-~_:1-~?~------------ ~~~-~8~~:9_~~-~~~-£~<.:!:9~---------50 Mr. Peter Renew Regional Representative, CBM Regional Office, 37 lnthamara soi 7, T: 66-2-6169920
___ --------------------------------------------- -~~~~~~!!:l_~~.:"-~-~~.9.~9-~-~9-~!Q._I~.§.i!9!!.~-------------------------------------- ~:-~-~:?:§.~~-~9.?..!__ ___________ £~!.1:£~?!£~~~!.1:~~.:~_<~:.~~---------?_! ~~:.-~~9~~?--~-~~-~~~----------------------- ------------------------------------------------------------------------~------------ ·-------------------------------- --------------------------------------~~ ~~:-~S'J[_~l~~~Q ____________________________ ------------------------------------------------------------------------------------- -------------------------------- --------------------------------------~~ .!2~:£:_~~~~JQp~~~9I~s>J9_9~~~------------ I~~~£-~Y..~_I::I_~~.P..i!9L!::Q:_~9-~~~?.:?.~£:~-~9.!!1E~-~~~.§.r:!:~£~!~------------------ I-~-~?:.:?.?:~-~].:?.?:!. ___________ £~~~~~!~~-@!>J.9J29_~9.:~E.~:~~-----54 Dr. Bal Kumar IRIS(International Resources for the improvement of sight) T 855-23-211412
___ --------------------------------------------- -~~_q_~!:_~!~.J:~-~9_r:!:e~~~2-~9!!:1_~9s!i~:!::~~~9-~~~?-~--------------------------- ·-------------------------------- l~~~?-~-~9-~~~~-~~~-~~;~£~:~~-----49 Dr. Fumio Kogure President , Japan National Society for the Prevention of Blindness. T: 813-5261-1444
Torio Tower North 4F, 261 Yamabuki-cyo,Shinjukuku, i(Ophthalmologist) Tokyo, Japan F: 813-5261-1321
Secretariat
50 Ms. Udomsiri Parnrat Institute of Public Health Ophthalmology T/F: 66-44-272648
___ --------------------------------------------- ~.!!!E~-~~-~-~9-~9-'-~~~-~9~~~!~~-~~i~9J?_QQ_qg2_~-~9l~~~s!~----------------------- ·-------------------------------- ~~~r:!:.~!~~~~~~~~:r:!:.~!L~:9£~~----~! .!2~:_15!:_~~P..~9-~9-~9~-~~~~~!.l:~9!!:..________ g_e~~~-~~r:!:.~!~Q~_<?-~!:l~~!J_Y.!~tl9I!~:.-~?-~£.:Q:.~-~~9~·--------------------------- !J£:._~?~:~~--~!3.Q?_~--------- !9£~!{~.@)~~!~!:~9-~----------------~~ M!:_~_~p~~~-.!:9_~Y?_~~E.___________________ <.?..e!:.!~-~~r:!:.9!~.9.~_g_~!:l~~!J_Y.!~~!i~~~.!-!:-_~9_f..:'?.:~--------------------------------- !!£:._~?~:?~:~!3.Q~_q _________ --------------------------------------~~ Q~:£:~~!~9-~-~!!.~-~~~~~~------------------ _<.?_f-r:~~-!.1]~~~9~!J_Q~~~!.l]~~y-~y~_!j9_~~i!~~-~~~-f..~l?;f! ________________________ JC~~?~:-~9:~~~~?-~------------ -~-~!:1-~~~~_:I_@~~!~?J~_<:~!_l] ________ _ ~~ !2~~-~9-~!:1E~i~-~~~e!:_~~9~.§.~-------------- -~~-~~.9.P!?_~9-~9-~~~-t!9~Je~~~~-~~~-~~!2~f!~!:~9-~_C<.?.e~!~-~~~-~!~9J~~2 ___________ -~~~?~:~~:.:?.!~Q~~------------ --------------------------------------
Dept. of Ophthalmology, Juntendo University, T: 813-5802-1092 55 Ms. Atsuko Nishikawa 2-1-1 Bunkyo-ku Hongo,Tokyo 113-8421, Japan F: 813-3817-0260 [email protected]

Welcome Speech of Excellency Mr. Chanasy Phosikham,
Governor of Luangprabang Province
Distinguish Excellency Mr. Dr Ponemeke DARALOY, Minister of Public Health
Respect to local and foreign guests.
Today, the people of Luangprabang are very pleased and it's a great honor that
Luangprabang was chosen to be the site of the fourth Inter-Country Workshop on
Prevention of Blindness.
In this significance occasion, I am on behalf of local authorities and people in the whole
province would express our worm hospitality welcome to excellency Mr. Dr, Ponemek
DARALOY, Minister of Public Health that on behalf of the government attending this
Workshop and also I would express my welcome to local and foreign participants, ladies and
gentlemen who attend today's Workshop.
Dear guests,
Luangprabang has been established, preserved and developed over 1200 years, it's
abundant of famous ruins that shows to the civilization of culture and nearly fine arts and
handwork of our ancestors, it's the town of beauty scenery on cultural and natural so it was
named the World Heritage Town on its reputation by UNESCO at the beginning of 1998.
Other hand, Luangprabang is the central northern provinces and being the Medical center of
the northern part of Laos, so it's condition that facilitate for the treatment services to rescue
the people's lives in the northern region.
Dear guests,
As you all aware the prevention of blindness is very important because eye is the most
important organ in the human structure, in case of careless of prevention process means the
leading organ is blind it's also means that life is not perfect and in the darkness forever.
I believe that all the participants to the workshop on prevention of blindness take your ability
discover the prevention and treatment process of the eyes of Laotain, specifically and also
the global citizen in general vies.
-19-

On this fine occasion I would like to express my sincere thanks to WHO collaborating Centre,
Juntendo University, Japan for your support this workshop in Luangprabang province.
Last but not lease. I wish Excellency Mr. Dr, Ponemek DARALOY, Public Health Minister
having good health and prosperity.
Wish all local and foreign participants good health and prosperity.
Wish the fourth Inter-Country Workshop on Prevention of Blindness that organized in
Luangprabang Province having fruitful success
Thank you
-20-
WHO Opening remarks Inter-Country Workshop for the Prevention of Blindness and the
"Control of Ocular Infections", Luangprabang, Lao PDR
Your Excellency Dr. Ponemek Dalaloy, Ministry for Health,
Your Excellency, Governor of Luangprabang,
WHO Tokyo Collaborating Centre for the Prevention of Blindness
WHO Colleagues from Geneva and Manila
Representatives from NGOs
Dr. Vithoune, Director of the Ophthalmological Services in Lao PDR,
Ladies and Gentlemen and Friends,
It is a real pleasure for me to attend this very important Inter-Country Workshop on eye care.
First of all I wish to thank the govern or of Luangprabang for hosting the meeting in this
World Heritage beautiful city, and his excellency Dr. Ponemek Dalaloy for his presence with
us, today, which underlines the importance of the meeting itself.
I would like to express the WHO's appreciation to the Tokyo Collaborating Centre for
Prevention of Blindness for organizing and financially supporting the meeting and, of course,
my congratulation also to the MOH for all the local arrangements and for the agreement tot
have the meeting in Laos.
I would also like to welcome all the foreign participants from Cambodia and VietNam, the
observers from Thailand and Myanmar, the representatives from various NGOs and all the
other participants.
During the last seven years there have been already 3 meetings of this nature.
This is therefore the 41h one.
The first meeting took place in1995 in Vientiane.
The second was held in Phnom Penh in 1998,
The third in VietNam, so it is now time to return to Laos once again ....
As you may know, each time the workshop deals with a specific issue related to eyes, to eye
sight and to prevention of blindness.
-21-

The last meeting dealt with refraction problems and provided, to all countries concerned,
indications on how to establish or improve refraction services for the population.
This year the major topic of discussion will be on "how to prevent, control and treat ocular
infections".
Somebody, who is not working in this specific field, might be wondering why so much
attention paid to eyes, when there are so may other killing diseases to deal with.
Are the eyes and their problems really such a priority?
I am sure I am now talking to the converted, but I would just like to respond to those people,
to keep their eyes closed for one day only and try to go around or to do their normal
activities.
In other words we often take our vision for granted and realize the importance of our
eye-sight only when we do not have it anymore or when we start getting blind.
The vision is definitely the most important of our senses. We can easily survive without the
feeling of smell, or the taste of the food we eat, or the feeling of touch, but the life of blind
person is really miserable for many aspects.
Preserving the vision and treating all causes which might lead to blindness or to vision
impairment, are therefore of paramount importance for all people.
We thank the Government of Japan for the assistance in eye care infrastructure
development in strategic provinces and we are also grateful to many NGOs, for the logistic
support they provided.
Eye care in Laos is the result of coordinated efforts from many sides. I n this connection I am
glad to inform the participants that the MOH, with the support of WHO, the financial
assistance of the Government of Korea and the technical support of the Tokyo Collaborating
Centre, established in 1996, a large programme for cataract operations throughout Laos.
In the last 4 years there have been more than 8,000blinding cataract people operated, and
-22-

there is now the capacity to carry out the operation in remote areas, giving back the vision to
more than 3,000people every year.
The recent trainings on refraction, established as a result of the last meeting in Hanoi and
Korat, further improved the quality of eye care and services.
It is now hoped that all the problems related to eye infection will be dealt with the most
appropriate way in each country here represented, as a result of this meeting.
It is very important to look at the practical aspects, required to improve the eye care, and to
analyze the constraints and problems to be solved in order to establish effective and high
quality services.
In this connection it will be very useful to review the operational progress of various national
programmes, to hear from you about the difficulties encountered, and to propose together
practical and feasible solutions for the problems identified.
In future it will be essential to look for alliances and coordinate eye services with other health
programmes.
For instance, in the area of eye infection, it will be necessary to strengthen and improve the
laboratory and microbiology services for better identification of the cause of infection.
Equally important is the coordination with the pharmaceutical departments, in order to obtain
the most appropriate drugs for specific infections.
Other important elements of the programme include:
1. The primary health care services, for the expansion of primary eye care at peripheral
levels,
2. The training required to enable health staff to deal competently with eye problems and
the
3. Close cooperation with the reproductive health services to eliminate ophtalmia
neonatorum, still affecting many newborns, even in urban areas.
The importance of clean water and hygienic practices for the prevention of trachoma and
other infections is well known to everybody and need therefore to cooperate with water
-23-

supply and sanitation programmes aw well.
I hope that each programme manager will be able to establish alliances and closely
cooperate with all different departments and sectors involved for better eye care.
One of the main purposes of inviting to this meeting observers and many NGOs, is exactly
to foster mutual cooperation, to encourage sharing of information and experiences, to
establish coordinated programmes and, especially, to promote Technical Cooperation
among Developing Countries.
We have to learn from each other and put together our knowledge in order to find the bet
solution to prevent all possible cases of blindness or treat on time, and in the most
appropriate way, all eye diseases.
I wish therefore to all participants the very best for a productive discussion for a useful
sharing of experiences and for learning from each other the best way to avoid or treat all eye
infections.
Thank you very much.
-24-

The 4th Inter-Country workshop on Prevention of Blindness
at Opening Ceremony
Atsushi Kanai, M.D.
Professor and Director, WHO Collaborating Centre for PBL, Tokyo
His excellency Dr. Ponmek Daraloy, Ministry of Public Health, Lao PDR
Mr. Chansy Phosikham, Governor, Luangprabang province
Dr. Vongehan Phomsavat, vice governor, Luangprabang province
Dr. Sommonc Phounsavathm Head of Curative department,
Dr. Giovanni Deodato, WHO Representative to Lao PDR
Dr. Serge Resnikoff, WHO Geneva
Dr. Hisashi Ogawa, WHO Western Pacific Region
Distinguished guests, Dear Colleagues, ladies and gentlemen of Blindness in the Western
Pacific Region, I would like to address you at this opening ceremony.
It is my great pleasure to open the 41h Inter-Country Workshop on prevention of blindness
in this Luangprabang, in 4days from today. The participants came from four countries
namely from Cambodia, Lao PDR, Viet Nam and Thailand.
Tokyo Centre initiated this Workshop for the first time in Vientiane, Laos, October 1995,
then we held it every 2years, second time was in Cambodia in 1998, last time was in Hanoi,
VietNam, 2000. We also have generous cooperation from the WHO headquarter, Geneva,
WHO Western Pacific Region office and Ministry of Public Health Thailand, who is making
successes in national blindness prevention programme since first time. In addition, this time
we invited new participant of Myanmar. The purposes of this Workshop are to exchange the
experiences of each national programme for Prevention of Blindness and to plan for the
further mutual cooperation. We had focused on Cataract Intervention in this programme in
the past, now we can see clearly that it is going well and contribution of people's quality of
vision. In the last Workshop in Hanoi, we could the plan of refraction service development.
I do hope that you may be able to discuss the important problems of ocular infections of
each country in the present situation.
On behalf of Tokyo Centre, I appreciate very much to Ophthalmic Care Centre, Ministry of
Public Health, and the Government of Lao PDR for hosting to this workshop and also to
-25-

WHO for generous supports. We wish very success of the Workshop as well as last three
meeting.
Finally, I hope all of you would enjoy beautiful landscape with an old capital Luangprabang,
where is one of the World Heritages.
Thank you
-26-

Opening addressing by his Excellency Minister of Health
Dr. PoneMek Daraloy, Ministry of Helath, Lao. PDR
On this occasion the WHO Inter-country Workshop on Prevention of Blindness taking
place in Luangprabang, on behalf of Ministry of Health, I extend my hearty welcome to all of
you. This is the fourth time that the ophthalmologists and health administrators in prevention
of blindness from Cambodia, Laos, Vietnam, Thailand and Myanmar are together and joined
each other since they were counterpart for a long time.
This Workshop is prepared by WHO Collaborating Centre, Tokyo and Institute of Public
Health Ophthalmology, Nakhorn Ratchasima Regional Hospital, Thailand played very
secretariat role. Funded by Tokyo Centre and WHO Regional Office for the Western
Pacific. The objectives are to exchange experiences in the past in the field of blindness
prevention in five countries and discuss cooperation among all participating countries,
International Non-Governmental Organisation are invited to share part of the Workshop for
presenting the mission.
Blindness especially ocular infection in the community has been and still remains one of
serious health threats in Lao PDR. This is the same issues in our neighboring countries.
National efforts therefore, have to further go for prevention and control. It has been no more
visually impaired but a problem of health system included in general health system of the
country. They should be as follow: every one can enjoy the good and highest status of eye
health.
However, we are proud of all of you for your success in the study progress in the past. The
national program for the prevention of blindness based on primary health care proves good
and effective outcomes. Even ocular infection has been successfully implemented within the
framework of secondary health care.
Taking the opportunity, on behalf of the ministry of Health and the people of Lao PDR, I
would like to express deep thanks to counterparts in the neighboring countries who gave us
energetic and closed cooperation. To all of us, blindness, however, challenges us with the
different dimensions. Also my thanks and best regards to all of the international
organizations. Governmental and non-organizations, which have extended to us various
co-operations. We determine that ourselves must firstly tackle the challenges. The actions
-27-

must be appropriate and self sustained by our own. To that reason the Ministry of Health will
continue to consider as a highest priority of eye health of people. Of anywise, I hope that
you are all ready to discuss on mutual collaboration with the spirit of Technical Cooperation
between Developing Countries (TCDC).
Eye care in this country enjoys high priority in health services. We do believe further
progress by own efforts. However, acceleration could be assured by TCDC among the
neighbors and NGOs supports, we hope this opportunity would provide us more technical
exchange and cooperation plans in the future.
Once again, I welcome you all and expect from every successful workshop. I do hope all
of you will enjoy you stay in Luangprabang, World Heritage city Lao PDR.
-28-

The Global Situation of the Prevention of Blindness
v s o n
Q~~ THE RIGHT TO SIGHT
S. Resnikoff MD, PhD World Health Organization
Geneva
IV'h Intercountry Workshop Luang Prabang, Lao PDR, 4 February 2002
World Prevalence of Blindness (available data and estimates - 1997)
. ..-)· -~~v~~~~-~~~ - [Q;~ t~~"':fJ ..
Prevalence of Blindness
-29-
Present situation
1. Present estimation:
,. 45 million people blind
+ ,. 135 million visually disabled
< 6/18-3/60 <0.3- 0.05
Low Vision
Blind < 3/60 <0.05
ICD-10
Best corrected VA
Prevalence of Blindness
Global Distribution of Blindness by Cause
Oncho. 1%
{WHQ,PBL 1995)
Macular degeneration
Diabetic retinopathy
Aefracf1ve errors (uncorrected)

Present situation
80% of blindness is avoidable
Cataract
Long-term outcome of cataract surgery from selected population-based studies in Asia
%Eyes w1th V1sual Acuity < 6/60 (0 1)
W!lh ~_y_.rujg!;JJ~ GQ_fJ.G<A!911
____ Uncorrected Ref. Err
-30-
Present situation
1. However, good quality eye care is:
, not always available (geographical barriers)
, not always accessible (socio-economic barriers)
Coverage
LDC
Cataract
" F1rst cause of blindness ( ... 50 %)
, backlog: 20 m11lion unoperated cases
" only 1 o million cataract surgeries I year globally
,, major constraints :
" coverage
" access " quality +H
Cataract
CSR
6000
I 5000
4000
3000
2000
1000
USA
t
I • .
I ' :
• i .to ...
EU India Lat.Am A !rita. China
Cataract operations/million population'year
%
Presenting Post Op. Visual Acuity 2: 6/18 (0.3)
7 population-based studies
I liN~ l_g_IOL + ~

Percentage of IOL implantation
Trachoma
;_ Still the main global cause of preventable blindness
;_ Estimates:
" 146 million persons with active disease
" 10 million trichiasis
" 6 million severely visually impaired
; A social disease, linked to poverty
Childhood blindness
-31-
Trachoma
Geographical distribution
Childhood blindness
;, Present situation:
" 1.5 million blind children in the world
-Asia: 1 million
-Africa: 0.3 million
" 5 million visually disabled
i. Causes:
.. vary from place to place change over time according to socio-economic development
Childhood blindness
everywhere: congenital cataract I glaucoma hereditary retinal diseases
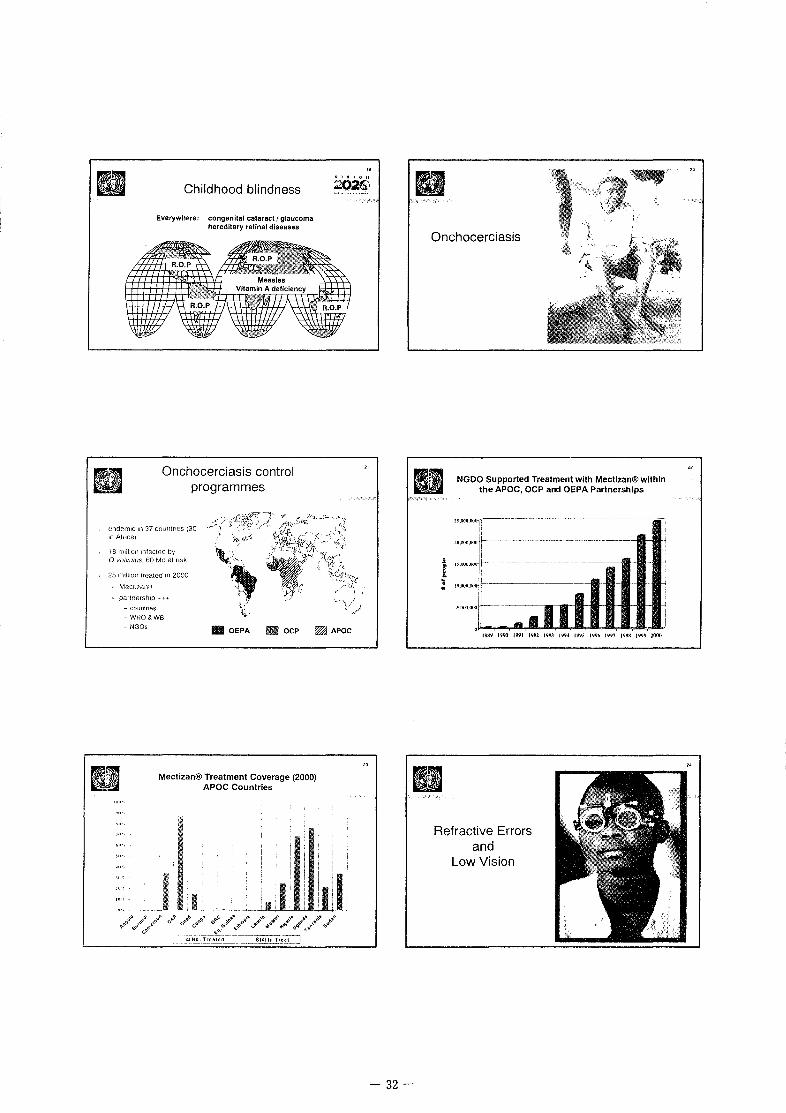
Onchocerciasis control programmes
(~ndem:c 11'1 37 countnes (30 1n AfriCa)
18 million 1nfecwcl !)y 0 volvulus. 60 Mo at nsk
25 1lldl1c>n treated 1n 2000
Mect1zan~u
partnerst1rp ..-T~
~ COU!l1rleS
- WHO&WB
- NGOs lllllllll OEPA i!B OCP WJ APOC
Mectizan® Treatment Coverage (2000) APOC Countries
-32-
Onchocerciasis
t '0 .
NGDO Supported Treatment with Mectlzan® within the APOC, OCP and OEPA Partnerships
1\ll!Y 1990 !!WI 19\11 199.\ IW4 I'W.'> IVYh I'W7 19911
Refractive Errors and
Low Vision

Refractive Errors and Low Vision
'· Globally:
" huge number of uncorrected significant refractive errors - under-estimated for a long time - mainly in developing countnes - but also 1n industrialized countries
, 1/3 of low VISIOn cases due to uncorrected refractive errors
, osk factors: ~. soc1al isolation ..
" low VIsion care services - non-ex1sting 1n most of the countnes
- or fragmented and patchy
What we know
i. Global trends over next 20 years:
1. global population growth
from 6 billion people to 8 billion by 2020
II
Global population ageing
-33-
Million blind
Vision 2020: Where do we stand now?
2000 2010
Future projections
" Global trends over next 20 years:
1. global population growth
2. global population ageing
Trend
2020
from 1 billion aged over 45 to 2 billion by 2020
What we know
1- Global trends over next 20 years:
1. global population growth
2. global population ageing
3. reduction of governmental support for blindness prevention
economic recession and competing demands

Scenario for the future:
i. Because of :
" p_opulation increase and ageing
" and present weakness of eye care delivery
OlherNGOs & Agencies
blindness will continue to increase
... unless more aggressive intervention is taken ... and despite obvious progresses
Who will implement "Vision 2020 - the Right to Sight" ?
WHO ./Professionals, NGOs /
/'Other NGOS"\ -~ Agencies/'
I Nutrition· .... \
. · _imm;~nit<ltion ' ' Sl!fol]fl'!!ion · ! Civil Society
/--~-~
· Education Poverty
alleviation ' .. __ :..:...:..:'f>.'i~~~: •• __ )
Thank You!
-34-
General objective
1- Building a comprehensive eye care system
" integrated into existing health services
" providing the best technology that can be afforded
;, In order to make high quality eye care
, accessible
, affordable } to all those in need
Conclusion: the Right to Sight
;. Vision 2020:
, a very ambitious, yet realistic venture
" not a new organization or agency
, a unique opportunity to work together, more efficiently, on a common agenda
2o26S ,_ .. : .... , ....... .:.
Vision 2020 is a partnership at the global, regional and particularly at the country level

·.· .....
Healthy Cities programme in the Western Pacific Region
Hisashi Ogawa Regional Adviser in Environmental Health
Western Pacific Region
World Health Organization
Urbanization: The Global Picture (2)
• 1,3 of the curn.:nl urhan popuhttion. ahout 1.6 billion people. arc in developing countries.
• Of these. 600 million, or ahout 37%. live in severe, life~ threatening environments.
Urbanization: The Regional Picture
urbanization and Population Growth Western Pacific, 1950-1995
1950 1970 1995 2020
-35-
Urbanization: The Global Picture (1)
Increasing global pop'n: 1950 2.5 Billion
1970 3. 7 Billion 1995 5.7 Billion 2000 6.0 Billion
&IUI'IHIII
IDRun1l 1950
'"
1995
Urbanization: The Global Picture (3) Mega-cities (in millions)
2015 ----- -~···-----··----- ----
4 MOXICOCI!y(ll 21 ~ 4 SaoPaulu(1761
5 SaoPauloi10.01 ! 5 NewYork(166l
! 6 Lagusp34)
:5 $;1uPauln(20·l•
I 6 Klll<lC1H(1921
i 7 LosAnUHfm;(\3 II 7 M!!~ICOCoty 1192)
i 8 Calculta(129) '1:1 NewYork(174
i ~~-s;~~:~=~a~~::~~~~ 2 61 ~ o J~:~~:~n~ :1 ~1
31 i 11 0hllka(123) II 0e!!u(168l
12. Karacht 11 L8l 12.Metro Manita(t4.8)
13 Delh•0171 13.Stlanghal{14.6)
14.Jakru1a!11 01 14.losAngeteS(14 n 15.0snka{11.0} 15 BuenusAut~s(14 11
16. Metro Manna (10.9) 16 Cauo (13111
17.&1jlng(10.8) !7.1s1anllul(125!
18. Rio de Janc11o (10.6) 18. Beijing (12.3)
19.Cruro(106) 19. Riod(!Janeuo(11.9!
20.0saka(11.0)
21.Tianjin{10.7)
22 Hyd<!fabad!1051
23 B~nglwk no 11
Urban Health Challenges (1) v Inequity in access to
and quality of health services
" Insufficient and inadequate housing and urban infrastructure leading to unhygienic conditions

Urban Health Challenges (2) Unsafe workplaces located within urban cities of developing countries contribute to: - poor f1eaftt1 and unsafe
condrtiOns for workers - enwonmental pollutiOn
" Worsening air quality - arr pollution a major problem
rn many farge cities in the Western Pacrfic
,. Increased traffic contributes to noise and accrdents
Solving Urban Health Problems
Need to address "determinants of health" (i.e. physical and social environments that affect health) Controlling physical and social environments is not in the domain of the health sector
" Need for coordination and collaboration with other sectors (e.g. housing, transport, trade, industry, labour, etc.) to provide "supportive physical and social environments for health"
,. Also. involvement of the communtiy and mobilization of their resources Promotion of healthy lifestyles- Individuals are responsible for own health
The Healthy Cities Initiative (2) ,. Healthy Cities projects
focus on special settings
" 1996 - 5 healthy cities projects in the region
" In 2001, about 100 healthy cities projects on WHO database (www. wpro. who. int)
-36-
Urban Health Challenges (3) " Unhealthy lifestyles
D1et habit: obesity Vs. nutritional deficiencies
- Increasing tobacco and substance use
- Lack of physical exercise
},".....,
The Healthy Cities Initiative (1)
" Healthy Cities is an intersectoral approach with community participation to addressing physical and social determinants of health in the city
v Cities identify their priority health problems and feasible solutions.
v -180 cities in the Western Pacific now implementing Healthy Cities projects
Keys to Success
v Political will/support is needed for sustainable efforts - Strong political leadership
v Citizens' participation essential, leading to a popular movement -Including the private sector businesses
" Local governments and departments coordinate to provide supportive mechanisms and services

Fourth Inter-Country Workshop February 4 - 8, 2002 Luangprabang, Lao People Democratic Republic
Country Report on The Progress of Blindness Prevention and Ocular Infection in
Cambodia (Sub-Committee for the Prevention of Blindness)
Introduction:
Cambodia occupies a territory of 181035 square kilometers. It located in the southwestern part of Indochina, boundary by Thailand, Laos, Vietnam and the gulf of Thailand in the Indochina sea.
Cambodian culture similar to other countries in Indochina and still maintain its culture heritages, 95% are Buddhism and other are Christian and Islamic.
The census conducted in 1998 show 11 .87 millions people and 85% living in rural area. Majority of them are farmers and have agriculture skill.
Health Care system in Cambodia:
National health system based on an equitable geographic access to basic health and referral system for population in order to optimize the allocation of scare of health resource.
A Primary health care strategy, which is base on the development of district health system is being implemented.
At the provincial level will be result in a 2 system of referral hospital that serving about 200,000 people and each health center serving about 9000 to 10,000 population. As the result of this reform policy, in the whole country there are:
929 health centers 67 referral hospitals 73 operational district 7 National hospital
Blindness in Cambodia:
Cambodia is a country where blindness remains one of the major health and social problem, because of long turmoil war and inadequate of eye care personnel. There is no national survey on blindness have been conducted in Cambodia , but the two different survey have been conducted in Kandal province and Battambang province estimated the prevalence of blindness approximate 1.2% and the major cause of blindness are : cataract , uncorrected refractive error , glaucoma and corneal scare and pterygium.
Eye Care System In Cambodia:
All Eye unit in the provinces has supported by government and non government organization and the eye care coverage has been increased, but service delivery in
-37-

Cambodia are still not meet thee basic need of population, because lack of medical infrastructure, qualified personal and material facility. There are 3 level of eye care in Cambodia: tertiary, secondary and primary level. The secondary and primary level are in operational district that coverage about 100,000 population.
-Tertiary level is not yet to developed as in most other developing country Preah Ang Doung hospital one of the national hospital will be developed to national eye center for tertiary level in Cambodia and it also the office of national subcommittee for blindness prevention of Cambodia
- Secondary level has change a lot after general election in Cambodia 1993. the number eye unit has been increased from 4 eye unit in 1993 to 15 eye unit in 2001. The coverage of eye care delivery is almost complete in Cambodia except for the province that infrastructure is difficult to access, but eye camp in these area have been done.
- Primary level: Primary eye care are integrated into primary health care. The training program of primary eye care have been done in province has eye unit to provided the knowledge to the health center staff to perform primary care in their communities.
+The Progress of Blindness Prevention (Five years after the Implementation of the First Year Plan of Action )
The blindness prevention programme in Cambodia has started since 1995 following the development of the Master Plan which aims to provide basic eye care service in each region of Cambodia and to reduce blindness prevalence to less 0.5 % by the year 2005 and First Five Year Plan of Action (1995- 2000). The First Five Year Plan of Action had finished with steadily progress noted, thanks to the well coordinated among the national, international organizations and International NGOs.
The Second Five Year Plan of Action has been developed to support the new global initiatives of the VISION 2020 - The Right to Sight. Top priorities for the second phase implementation are:
Human resource development Disease control Infrastructure and Appropriate technology Sustainability of Eye Care Development
These top priorities have been recommended following the National Workshop VISION 2020 and Partnership for National Eye Care Programme in Cambodia, held in Phnom Penh from 12 to15 December, 2000.
-38-

The Progress of Blindness Prevention
A- Human Resource/ Manpower :
Eye Care Professionals 1995 1998 2001 2005 Ophthalmologist 1 1 3 9 Eye Doctor 30 35 32 34 Basic Eye Doctor 0 6 15 28 Basic Eye Nurse 22 47 42 Optometry Technician 8 14 45 Ophthalmic Assistant 18 132 Primary Eye Care Worker/ province 3pro 9 pro 20 pro
B - Disease Control :
Cataract:
Cataract accounts for 65 % of the main causes of blindness and 75 % of low vision. Current estimates show the backlog cataract is 80,000 with the anuall incidence of over 19,500.
The number of cataract operation performed in Cambodia has been increased
Year 1992 1998 1999 2000 2001 Total Cataract Operation 500 3500 5500 6000 6735 Cataract Surgical Rate 50 350 550 600 670
The above figure shows the current out put has cover only 30 % of the annual incidence i.e. to cover the annual incidence the number of operation needs to increase 3 to 5 times. However, 80 % of all cataract operation were performed in the provinces.
Refractive Errors I Low Vision
Account for 1 0 % of the main causes of blindness. Hospital data shows 6.5 % of out patients has got Refractive Errors.
There are 14 Optometry Technicians trained in the country. There are up to 1 00 optical shops in Phnom Penh and in the provincial towns.
There are mobile refraction service in 5 provinces in 2000 which screened5483 people and distributed 6509 glasses. In 2001 the mobile team screened 1 0,442 and distributed 8471 glasses. These mobile team had been carried out by the local Optometry Association, overseas NGOs and visiting optometrists. There were no more Optometry Technician Trained after 1998.
-39-

Trachoma
The magnitude of Trachoma problem is unknown in Cambodia. The Rapid Assessment in three provinces and examined 16803 ( of which 2637 were children ) revealed:
Trichiasis 0. 7 % Tl!fF 2.9%
The establishment of the National Trachoma Control Committee is under way.
Vitamin A Deficiency
Vitamin A Capsule ( VAG ) distribution started in Cambodia in 1994 and since 1996 the distribution of VAG was integrated with the National Immunization Days ( NIDs) and since 1998 the distribution of VAG has gone through the routine immunization outreaches , the National Program for Immunization ( EPI ). The current National Micronutrient Survey conducted by HKI and MoH in 2000 shows VAC coverage varies widely among and within provinces ( 10 -55 % ). However, there has been a steady decline in the prevalence of Vitamin A deficiency in the last five year.
Childhood Blindness I Congenital Cataract
Data on childhood blindness is limited. Surveys of children of the school for the blind in Cambodia showed that corneal scarring from Vitamin A deficiency, congenital cataract, high refractive errors and degenerative retinal diseases were the common causes of blindness and low vision.
Data on the prevalence of congenital cataract among Cambodians is unknown. Hospital based data showed that congenital cataract of familial origin is common in Cambodia. Operation for congenital cataract accounted for 2% of all ophthalmic operations within the eye units. Late presentation of the children for surgery, the lack of adequately trained personnel and equipment for pediatric surgery are contributory.
C - Infrastructures and Appropriate Technology
Currently, it is estimated that only 40% of Cambodians have access to eye care services in 10 provinces of the country. The estimated coverage of eye care services is about 25% and the utilization of eye care services was less that 1% in 1999. The number of eye units had increased from 4 in 1993 to 10 in 1998, 14 in 2000 and 15 by the end 2001. The total number of eye beds in the country has increased to 200 in 2001.
D - Sustainability of Eye Care Development
As part of an effort in building sustainable national capacities for universal coverage and easy access to eye care, various measures are being taken. The national plan for eye care development envisages a network of eye care service in each of the provinces of Cambodia, with development of 5 regional eye centers, including the national eye center in Phnom Penh for research, training and policy development.
-40-

Various forms of cost recovery systems are being developed within the eye units to ensure self reliance and sustainability of the eye care services, though a lot of work needs to be done to make this more efficient. A national workshop to address the issues of sustainability in the eye care programs was organized in 1999 to identify and address the needs, major constrains and challenges for development of sustainable eye care services in Cambodia. The workshop recommended that cost recovery system in the eye units should be strengthened, as part of an overall provincial hospital system with some form of autonomy. The accessibility of public services to poor patients should be improved through improvement in quality of services, affordable fees, exemption from payment and adequate information to the community.
E - NGOs in Vision 2020 in Cambodia
Various NGOs are supporting the eye care development plans in Cambodia. This includes Helen Keller International, CBM I Caritas, Help Age International and IRIS. Other includes Mekong Eye Doctors, SEVA Foundation, FHF and Asian Eye Care. Voluntary organizations like the Rotary International and Lions Sight First Program have also been involved.
+Situation Ocular Infection In Cambodia:
Cambodia is located in tropical zone, hot climate and hum ides so it favorite to many infection disease including eye infection. On the other hand, the eye care network and integration of primary eye care into primary health care not overall completed. This is a problem that primary eye care activities could not access to many communities. This situation make avoidable blindness could not be prevented. The magnitude of ocular infection is unknown. There is no study on this field since the eye care program started in1994.
Starting to face on this problem, recently, we collected data on ocular infection from 12 eye unit from the provinces and 3 eye hospital in the capital city., data collection based on OPD registration and WARD registration for period 1 year from May 2000 to May 2001. The final VA after treatment when patient discharge from the hospital less than 3/60 after correction have been record, We counted for 1 blind case if the patient has one eye or both eye blind.
Data collection:
During 1 year from May 2000 to May 2001 the number of OPD patient 44890, among that 5351 have found ocular infection and 714 lead to blind by VA less than 3/60 after correction.
The ocular infection rate: 5351 x 100 = 11.92% 44890
Ocular infection lead to blind:___l14 x 100 = 1.59% 44890
-41-

The Major condition of ocular infection :
Conjunctivitis 45.44% ( 2886) Corneal ulcer 14.22% ( 903) Viral Keratoconjunctivitis 24.29% ( 1543} Trachoma 5.43% ( 345} Post injury endophthalmitis 0.64% ( 41) CMVretinitis 0.54% ( 36 ) Herpes simplex Keratitis 0.45% ( 29) Herpes zoster keratitis 0.40% (25) Ophthalmia neonaturum 0.11% (7) Post op endophthalmitis 0.06% (4) Other 8.38% ( 532)
Ocular Infection In percentage
50.00%
45.00~o
40.00'\,
35.00~o
25.00°o
10.00%
5.00%
0.009o
0 Co/1jUflC\IVI!IS
0 V1rai keratoconJunhviiiS
0 Comea1 ulcer
0Trachoma
m Post inJury endophthalmihs
0 CMV RetinitiS
0HSK
0HZK
I ophlhal rn1a neonaterum
0 post op edophthalm1tis
Oother
24.29'lo
14.22%
5.43'},
0.64%
0,54%
0.45%
0.40%
0.06%
8.38%
-42-

The major cause lead to blind:
- Corneal ulcer 71.28 % ( 509) - Trachoma 12.32% (88 ) - Viral Keratoconjunctivitis 5. 75% (41)
Post injury endophthalmitis 5.04% ( 36) - CMV retinitis 3.92% (28)
Herpes zoster Keratitis 0.56 (4) Herpes simplex keratitis 0.56% ( 4)
- Ophthalmia neonaturum 0.42% ( 3 ) Post op endophthalmitis 0.42% ( 3 )
Ocular Infection lead to Blind
80.00%
60.00%
40.00%
20.00%
0.00%
DC orne a I ulcer OTrachoma
OViral Keratoconjunctivitis • Post injury endophthalmitis
.CMV retinitis I.IJHSK
•HZK f.IJOphthalmia neonaturum
• Post op endophthalm itis
-43-

Ocular infection in Cambodia
-----·
-----=-=~~~~ ---------- ---.
Name of disease Province Capital city Overall in Cambodia
I -+--
No Infect No Blind j_ No Infect No Blind No Infect No Blind Conjunctivits 1259 0 -+ 1627 0 2886 0 Ophthalmia neonaturum 6 2 1 1 7 3 Trachoma 224 69 121 19 345 88 Corneal ulcer 795 421 108 88 903 509 Viral Keratoconjunctivitis 859 41 684 0 1543 41 Herpes simplex Keratitis 19 4 10 0 29 4 Herpes zoster keratitis 23 4 2 0 25 4 CMV retinitis 21 15 15 13 36 28 Post injury endophthalmitis 34 30 i 7 4 41 34 Post op endophthalmitis 2 2 2 1 4 3 other 383 0 149 0 532 0
Total Number 3625 588 I 2726 126 6351 714
OPD case Number 28295 16595 44890

Strategies: Strategy to prevent blindness relate to ocular infection and ocular infection by provided
eye care service facility and quality of eye care in the hole country :
1. Increased coverage eye unit from 4 in 1994 to 15 in 2001. 2. Integrate PEG into PHC in some provinces 3. Trachoma control by health education, campaign trichiasis surgery providing
lid rotation surgery skill and collaboration with other sector 4. Training program for midwife to prevent newborn ocular infection 5. Education, promotion program concerning to ocular safety through foster
and TV spot
Constraints: 1. Eye care network not complete the hole country is not reach the community
level. 2. Social economic problem 3. transportation and communication difficulty. 4. Knowledge and behavior of patients 5. Poor quality of care 6. Community participation
Future strategy: 1. Integration PEG into PHC should be complete and extend eye care service
coverage the hole country. 2. Training program for mid level personal 3. Improved quality of eye care by upgrade microbiology laboratory 4. Promotion, Health education program and safety protection 5. Tertiary level referral hospital
Conclusion: Cambodia is the country under developing not adequate eye care facility and have a
lot of communicable disease and lack of CDC, so ocular infection is the one of the eye care problem in Cambodia and about 13.34% of ocular infection lead to blind. But most of blindness relate to ocular infection can be preventable and curable.
So in aim to reduce blindness by ocular infection, Cambodia need to develop the ocular infection control system to avoidable blindness by ocular infection problem.
-45-
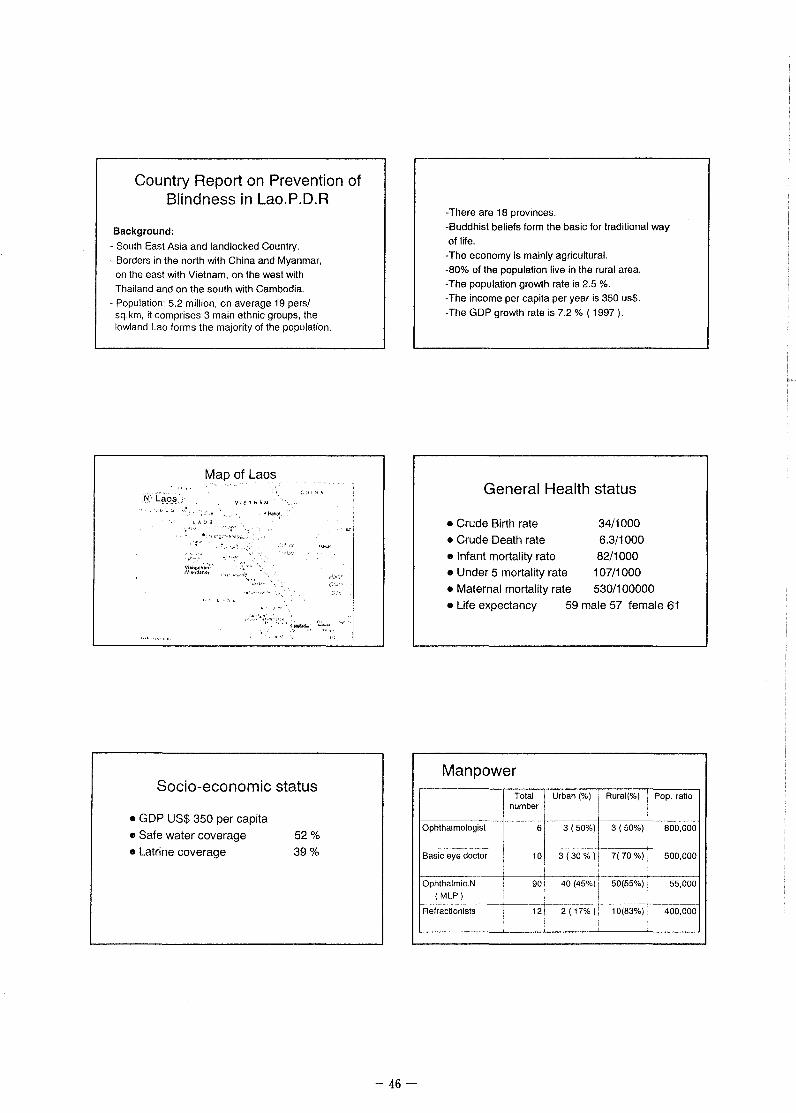
Country Report on Prevention of Blindness in Lao.P.D.R
Background:
- South East Asia and landlocked Country.
- Borders in the north with China and Myanmar,
on the east with Vietnam, on the west with
Thailand and on the south with Cambodia.
- Population: 5.2 million. on average 19 pers/ sq.km, it comprises 3 main ethnic groups, the lowland Lao forms the majority of the population.
Map of Laos ·,
. ·i I •, ~
~i-4; c;os;
l A 0 S
Socio-economic status
• GDP US$ 350 per capita
• Safe water coverage 52 %
• Latrine coverage 39 %
-46-
-There are 18 provinces.
-Buddhist beliefs form the basic for traditional way
of life.
-The economy is mainly agricultural.
-80% of the population live in the rural area.
-The population growth rate is 2.5 %. -The income per capita per year is 350 us$.
-The GOP growth rate is 7.2% ( 1997 ).
General Health status
• Crude Birth rate 34/1000
• Crude Death rate 6.3/1 000
• Infant mortality rate 82/1000 • Under 5 mortality rate 1 07/1 000
• Maternal mortality rate 530/100000 • Life expectancy 59 male 57 female 61
Manpower
I Total -] Urban(%) 1 Rural(%) I
Pop. ratio number . I
! ' i i Ophthalmologist
I 6 3 (50%)1 3 (50%)1 800,000
Basic eye doctor 101 3 (30% )I 7(70%)1 500,000
' I i
f---------- J __ Ophthalmic.N I 90 40 (45%) i 50(55%): 55,000
(MLP) ) I 1------------------j--· --+--------------+-----··········· --Refractionists 12 2 ( 17%): 10(83%): 400,000
' ' i

Magnitude of Blindness problem Assessment of needs:
-The population: 5.2 million. -Estimated that at least 1 % are blind.
-Therefore, the total of blind persons are 50,000 people.
The leading cause of blindness is:
Cataract Information
Year 1996-1997 i 1997-1998 i 1998-1999 1999- 00
P~~p~lati;;;:;-,---4~72- -! '~~-·~-~--+------ --·-~c--::-:----
4.84 4.96 5.00 ' (Million)
.l !----No.cat.ops/su i 112 287 250 128 rgeon/yr
CSR I 190 651 656 256 No.cat.ops/mi i llion/yr I
i
Ocular infection
• Ocular infection is one of the leading causes of blindness ( 13% ).
• Most of it occur with people who live in rural area of the country.
• Problem of public health especially is corneal ulcer.
-47-
The table shows the causes of Blindness in Laos.
CAUSES %of Blind
-:-cataract I 60%
- Ocular infection 13% ( Trachoma. Corneal ulcer, Trauma ..... ) 10% -Glaucoma 7% - Childhood blindness 10% -Others
Total: : 100%
1996-1997 1997·1998 1998·1999 1999·2000
Number Blind
30,000
6.500
5,000 3,500 5,000
i
i 50,000
!'ilECCE with IOL
'•ECCE wlthoutlOL
~.!.~!~L:~~:~pera~l~
Number of cataract operation each year
From 1996-2000 as well as the proportion of IOL implantation
Number of ocular infection

Trachoma control program
• Trachoma control has been conducted in 10 provinces in the year 2000.
• Prevalence of trachoma is considered endemic.
• After one year of program intervention, a remarkable result has achieved:
Existing Manpower
• Inadequate of manpower I refractionist in the country.
• A total of 12 refractionists: 3 work in VT prefacture and 9 in provinces.
• Some provincial eye units do not have refraction service yet.
Refraction Training Course
• Two months training for refractionist.
• Training four refractionists per year.
• We trained 8 refractionists two months, they came from other provinces who ever passed 4 months course for ophthalmic nurse. After finished course they returned to work in their eye units in VT prefacture and six provinces of Lao P.D.R.
-48-
Percentage of trachoma in 1 0 provinces
f-:-~ 0·9y;,-~ TF Tl Male(%) I Female(%) i Total(%)
CH~ 900 I 142 I ' 75(8.3) 67(7.4) I 15.7
XK I 300 : 64 0 I 30(10) ' 34(11.3) --+- 21.3
AT i 450 I 79 1 --1-·33(7.3)--1~(102) I-~--s V ! 750 ! 163 1 1 I 3(0.3) 102(13.6) i 21.7
1--------j--·---------'-------------t-·----·· -----·-!--- ------·-----------------:-------------8 K ~50 i 61 1 0 _ : 60(8) i 30(2.2) i 4.5
r.<M- I sOOT14-t-o--·----t22-(11.5J~t~_~l~1.5-____ __, ___ :-+-----::---t-----___,-------+----+----------t L B i 900 _.j-~--i---~-- , ~0(285~_:s_i_'~.:_9 _ __j _ _______,~
I u X I_ 750~~~-~~~--~~--~-~I-~75(~~-J.---~8(10.4) ~-~-~xe-----t 191 1 53 1 o : 22(11.5)
1 31(16.2)
1 21.2
VT _ _QS-t----;,8 1 o ! 50(28.5) i 68(38.81 I 67.4--
;:;;;;-- I 6666 I 990 I 28 I 475(7.1) I 515(7.7) I 14.8
Current situation of refraction service
• Existing manpower • Refraction training • Existing facilities • Inadequate of manpower I refractionist in the
country. • A total of 12 refractionists: 3 work in vr
prefacture and 9 in provinces. • Some provincial eye units do not have refraction
service yet.
Number of Optical Shop in Laos
Province 1 Government I Private sector ! General I I I I I I
VT Prefecture i 2 l 7 ! >40 i '
----------i--------------+---------___f__------1 Savannakhet I 1 I 1 i >20
I , I 1 1 1
Khammouane I 1 1 0 I >10
I
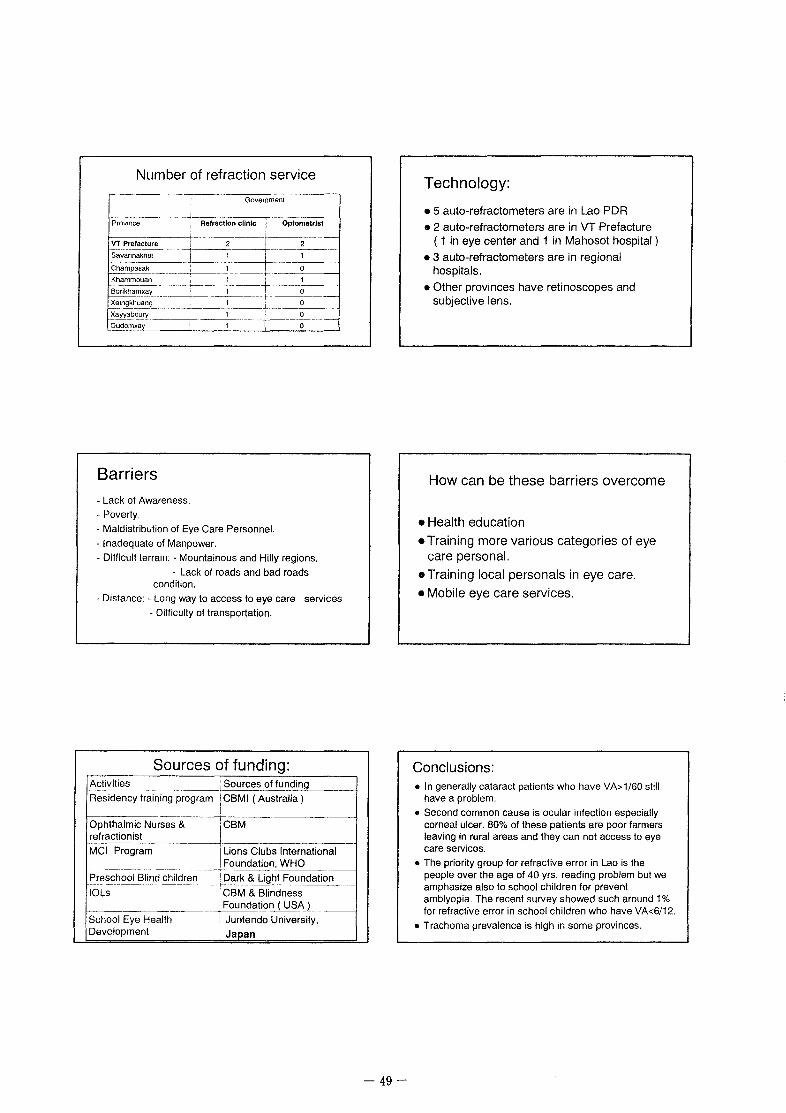
Number of refraction service
Government
~;;;;----~ Refraction clinic Opto;.~
VT Prefacture i- --Sa;~~;;;k~-~---~~T-~
Champasak : 0
Barriers - Lack of Awareness. -Poverty.
- Maldistribution of Eye Care Personnel.
-Inadequate of Manpower.
- Difficult terrain: - Mountainous and Hilly regions.
- Lack of roads and bad roads condition.
- Distance: - Long way to access to eye care services
- Difficulty of transportation.
Sources of funding: ~~~~-------;Sources of funding Residency training program I CBMI (Australia)
l Ophthalmic Nurses & _J CBM refractionist
MCI Program 1 Lions Clubs International , Foundation, WHO
-·------·---------·· Preschool Blind children 1 Dark & Light Foundation ------------- ~----------- --·--1-· ------
IOLs CBM & Blindness
r----------· ! Foundation ( USA )
School Eye Health : Juntendo University, Development ; Japan
-49-
Technology:
• 5 auto-refractometers are in Lao PDR
• 2 auto-refractometers are in VT Prefacture ( 1 in eye center and 1 in Mahosot hospital )
• 3 auto-refractometers are in regional hospitals.
• Other provinces have retinoscopes and subjective lens.
How can be these barriers overcome
• Health education • Training more various categories of eye
care personal.
• Training local personals in eye care.
• Mobile eye care services.
Conclusions: • In generally cataract patients who have VA>1/60 still
have a problem.
• Second common cause is ocular infection especially corneal ulcer. 80% of these patients are poor farmers leaving in rural areas and they can not access to eye care services.
• The priority group for refractive error in Lao is the people over the age of 40 yrs, reading problem but we amphasize also to school children for prevent amblyopia. The recent survey showed such around 1% for refractive error in school children who have VA<6/12.
• Trachoma prevalence is high in some provinces.

Recommendation:
• Sharing cost for cataract surgery.
• Dev~lop eye care net work integrate PEC into PHC.
• Provide low cost reading spectacles to community.
• Subsidy cost for ocular infection, especially corneal ulcer.
-50-
THANKS FOR YOUR KIND ATTENTION
,{~~\. ~ ~~ Welcome to Laos t?/1 .. ]1 ~~
~rt:J~~

THE OCULAR INFECTION IN VIETNAM
• 1. Introduction • One of the most common eye diseases in VN
due to tropical climate with high temperature and humidity, poor condition of hygiene.
• 1995 national survey on blindness and eye diseases in VN:
- Corneal opacities was the second cause of blindness,7.8% of blind people. more than half of them are due to entropion.
II. Some data on ocular infection in VNIO (Inpatients during 5 years)
Year Corneal ulcers Uveitis -----483 _____ _,505(107 e~oPhthJ
- ·--,---·- ·-- --------~·
511 495(151)
457 586 (196)
2000 401 547 (176)
646 (274)
2779 (904)
1. Infectious keratitis and corneal ulcer
Type of Bacte. Fungal Bac. & Acantha ! Bac. Total kera kera fungal moeba i endop ..
---- -------· ------- --~~--·------·-----+·--··-·-~--t---~---+----~-4----------No of 134 146 : 6 I 4 1 60 1 350
patients (38.2% 1 (41.7%) l (1.7%) : (1.14%) I (17.0%) I (100%)
f----M;;;-;,---,------+---r-- I. ,. I i9i-' I · (56.2%) ' I I
--Fe;;;ale·-~------~-- ---i---j--·--j-- ! 153
i I (43.8)
-51-
• I. Introduction
- The uveitis (including anterior uveitis, posterior uveitis, total uveitis, endophthalmitis and panophthalmitis) was the fourth cause of blindness, 4.2% of blind people
(The first cause is senile cataract, 70.7% the cause of blindness).
1. Infectious keratitis and corneal ulcer
• According to one research conducted in conjunctiva-corneal department of VNIO from June 1998 to April 1999 (1 0 months) on the 1200 inpatients, there are 350 patients suffering from infectious keratitis:
*Remarks:
• Proportion of fungal keratitis was highest: 41. 7%, then bacterial keratitis: 38.2%
• Majority of patients lived in rural areas: 82%, with the poor condition. The incidence of male was higher than female
• Argricultural trauma was the main risk factor (35% of corneal ulcer)
• 200/350 (57%) patients received medical treatment by themselves or by local physicians before hospitalization. 101 patients (28.8%) used antibiotics. Particularly 44 patients (12.6%) have been treated with topical corticosteroids. 55 patients (15.7%) used unknown medication.
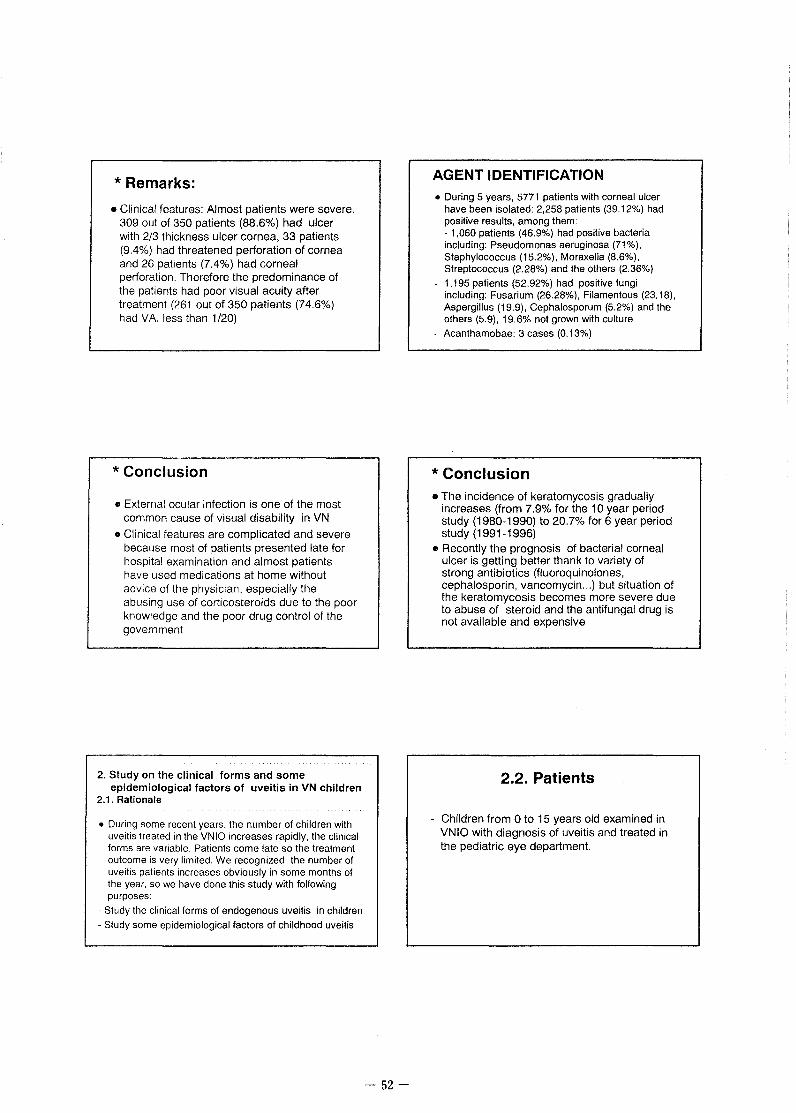
*Remarks:
• Clinical features: Almost patients were severe. 309 out of 350 patients (88.6%) had ulcer with 2/3 thickness ulcer cornea, 33 patients (9.4%) had threatened perforation of cornea and 26 patients (7.4%) had corneal perforation. Therefore the predominance of the patients had poor visual acuity after treatment (261 out of 350 patients (74.6%) had VA less than 1 /20)
* Conclusion
• External ocular infection is one of the most common cause of visual disability in VN
• Clinical features are complicated and severe because most of patients presented late for hospital examination and almost patients have used medications at home without advice of the physician, especially the abusing use of corticosteroids due to the poor knowledge and the poor drug control of the government
2. Study on the clinical forms and some epidemiological factors of uveitis in VN children
2.1. Rationale
• During some recent years, the number of children with uveitis treated in the VNIO increases rapidly, the clinical forms are variable. Patients come late so the treatment outcome is very limited. We recognized the number of uveitis patients increases obviously in some months of the year, so we have done this study with following purposes:
- Study the clinical forms of endogenous uveitis in children
- Study some epidemiological factors of childhood uveitis
-52-
AGENT IDENTIFICATION • During 5 years, 5771 patients with corneal ulcer
have been isolated: 2,258 patients (39.12%) had positive results, among them: - 1,060 patients (46.9%) had positive bacteria including: Pseudomonas aeruginosa (71 %), Staphylococcus (15.2%), Moraxella (8.6%), Streptococcus (2.28%) and the others (2.36%)
1,195 patients (52.92%) had positive fungi including: Fusarium (26.28%), Filamentous (23.18), Aspergillus (19.9), Cephalosporum (5.2%) and the others (5.9), 19.6% not grown with culture
Acanthamobae: 3 cases (0.13%)
* Conclusion • The incidence of keratomycosis gradually
increases (from 7.9% tor the 10 year period study (1980-1990) to 20.7% tor 6 year period study (1991-1996)
• Recently the prognosis of bacterial corneal ulcer is getting better thank to variety of strong antibiotics (fluoroquinolones, cephalosporin, vancomycin ... ) but situation of the keratomycosis becomes more severe due to abuse of steroid and the antifungal drug is not available and expensive
2.2. Patients
- Children from 0 to 15 years old examined in VNIO with diagnosis of uveitis and treated in the pediatric eye department.

2.3. Study methodology
• * Prospective study: children with uveitis treated from September 2000 to September 2001 (group 1) * Retrospective study: children with endogenous uveitis or endophthalmitis treated in 5 years from January 1996 to December 2000 (excluding the uveitis or endophthalmitis due to trauma, surgery, corneal ulcer ... ) (group 2)
a) age and sex
Male
<= 2 years 4
Female
7
Total
11
23
21
30
85
Remarks: - Youngest patient is 2 months -A big number of patients belongs to age group less than 5 year old, accounting for 39%.
b) Clinical forms and age:
vo <=2y .. 3-5y .. 6-10y. 11-15y., Total Forms j
Total 13 21 21
4
85
- Antenor uvellfs is often encountered tn the age group of 11-15 year old {67%}
- Endophtha!mitis is often encountered 1n the age group less than 5 year old (47%)
-53-
2.4. Study result
• 2.4.1. For group 1 (Prospective study): 85 patients (50 females, 35 males) with endogenous uveitis, aged from 0 to 15 year old, treated in pediatric dep. from September 2000 to September 2001.
a) Clinical forms:
Clinical ' Ant. Post. Total Uve.
Endo. · Panop. Total form . Uveitis Uveitis
Remark:
-Endophthalmitis are most common (69.4%)
2.4.2. For group 2 (Retrospective study):
• 831 patients (440 males (52.9%) and 391 females (47.1%) with uveitis or endophthalmitis treated in the pediatric eye department from 1/1996 to 12/2000.

a) Number of patients distributed by the months of the year during 5 years:
10 , 11 12 ' Total
y '
96 14 10 11 6 20 26 23 65 26 13 226
Remark: The patients were most crowded in 3 months: September, October and November (Autumn)
b) Clinical forms:
701 out of 803 medical records having the classification of clear clinical forms: - Antenor uveitis: 119 cases, 17%
- Posterior uveitis: 12 cases, 1. 7% - Pan uveitis: 66 cases, 8.6%
- Endophthalmitis: 492 cases, 70.2%
- Panophthalmitis: 18 cases, 2.5%
2.5.2. Clinical forms of uveitis Ant Post Pan- Endo. , Panopth
uve1tis uvettis uveitis almitis No. of cases
Pedtat. 14.1% 1.2% 10.6% 69.4% :4.7% 85 Depart ·children 2000· 2001
Retina 17.1% 25.1% 50.3% '7.5% Depart 1992· 1996
-54-
180 'T-----------------------------------~~----------
160 140 120 -f--------------------------------------'-L"'-
1 00 ,_ . ' '-----~ ~---~---------<
::ri~;R~,3}l1i1[~~~i .• 20 -- -- --- --1 !---1 - J 1--~ r---ll--1 ~-- -1 f---! '---4 o -- _.)J __ JL_JL__Jl_Jl_,lL_.)LJL_,
~· :<)' ,. ,. ~ ~· ~· ¢)' "' "'' ~· c.· '),"> «e ~"' ~~ ~"' '),"' '),'> ~"' <?e"' o"' ~0 Qe
of Uveitis 0 liD
2.5. Discussion
2.5.1. Age of patients relating to uveitis *In the group 1 (prospective study):
- 39% patients belongs to age group under 5 year old (34/85 cases)
- About 50 % of endophthalmitis and panophthalmitis were met in children under 5 years old (31/63 cases)
- Explanation: Inflammation reaction in young children is stronger than that in older children and adult, childhood eye tissue is softer and the eye defense barrier is easier to be break up, so it is more sensible to the toxin.
• There is a remarkable difference between children and adult: in children the endophthalmitis and the panophthalmitis represent a large proportion (74%), while in adult: it accounts for a low percentage (7.5%) but pan-uveitis represents 50.3%
• The result depends much on the clinical forms of uveitis in children: for the anterior uveitis, the result is very optimistic whereas pan uveitis, endophthalmitis result is very poor.

2.5.3. Causative Agents
93 vitrectomies were done for endophthalmitis (among 831 cases of uveitis), specimen are cultured. Identification is as follows: - Pseudomonas aeruginosa: 43% -Streptococcus: 5.3% - Moraxella: 8.6% - Fungus: 4.3% - Others: 38.8%
2.6. Conclusion
With the prospective study on 85 patients and the retrospective study on 831 patients in the pediatric eye department of VNIO, we can conclude that:
Uveitis in children is one severe disease with variety of forms, its cause is complicated, difficult to identify the agents, difficult to prognosis its evolution, the treating result is limited.
-The endophthalmitis represents a high proportion in the total number of children with endogenous uveitis. This is contrary to the adult.
Anterior uveitis: posterior synechia of the iris
-55-
2.5.4. Uveitis relating to weather
• Uveitis happen all year round, with highest frequency in September, October and November (Autumn). Other study in Ho Chi Minh city (South Vietnam). showed no remarkable difference between the months of the year. We think that in the North of Vietnam, there are 4 seasons with different climate. whereas in the South there are only the rainy and dry seasons.
• Uveitis related to weather ?
• - The endophthalmitis is often encountered in children under 5 year old. The younger is the children. the more severe is the endophthalmitis. Although the treatment is very intensive but the result is very poor. A lots of children in this age group must be enucleated.
• - Anterior uveitis, posterior uveitis and total uveitis is often met in older children (11-15 year old). its treatment is easier and the result is more optimistic.
• - Childhood endogenous uveitis apears with highest frequence in the 3 months of the Autumn, so it has a close relationship to the weather. It is different between the regions due to the climate. The clearest different between 2 regions: the North and the South of Vietnam.
Precipitates behind of the cornea

Total uveitis: precipitates behind the cornea Endophthalmitis: hypopion and exudate
Endophthalmitis: vitreous opacity Endophthalmltls In late stage: vlrtreous organization
Panophthalmitis: pus fill the A.C and vitreous cavity
-56-

6 months after lensectomy and vitrectomy Cataract: sequalla of the total uveitis
-57-

~.~. . .
Administrative Structure of Trachoma Control and Prevention of Blindness Programme
~-~·· --"···---.-~-·--~---~~~-~
Oeparmentof Health
. Trachoma Control and Prevention otl
-~-~~~-~~-~~--~~~~~J REGIO\' 2 REG;QN' ;---~ :-·-;EQ~ON4~-~ r~~ON'S'l rmTeRN~TiONAi.l \'EiKHT!lA VO~YWA ': BAGO i ~ KYAUKSE i i""EYEBANK :
--~-~----.. -- ·---··-·~----~ L __ ~_, _____ j L~~~~~-~-~--;
INFRASTRUCTURE
Facilities
Government
NGO (Sanga Hospital, Muslim Free, Thidagu)
Private
CBR PEC
Number of eye beds
500
100
50
Eye care teams exist in private and public sectors:
Average no. of surgery/week Refractivn services
- 25000/52 = 480 - State and Divisional
level Regular school screening programme - present
-58-
Location
Population
COUNTRY REPORT UNION OF MYANMAR
- Between North Latitude 9• 30' and 28• 30' South East Asia Total Area- 676,552 Sq.km (261 ,218Sq.ml) North to South - 2085 km East to West- 930 km
-(2000 Estimate) is 50 million. Majority in Rural Areas. The overall population density is 69 persons per sq.km, one of the lowest in East Asia.
National Health Plan General Objectives "To make primary eye care available all and eliminate avoidable blindness with special emphasis on cataract". "Reduction and ultimate elimination of blindness due to trachoma, cataract, glaucoma, ocular trauma, corneal blindness blinding malnutrition etc., by promotion of eye health, prevention, curative, sight restoration and sight saving surgical intervention".
National Objectives To prevent disability due to blindness an to reduce the blindness rate to less than 0.5% in all States and Divisions of Myanmar.
• Eye care facilities are available in the country at all level: schools, government, polyclinics, university and public hospitals, private sector.
• There are adequate number of beds for all ophthalmic patients, although the majority of surgeries are day cases.
• There is no waiting list and surgeries can be performed on demand in the private sector. or within the week in the public sector.
• In some N.G.O. Eye center (M.F.H.) waiting list 1-2 weeks because patients outnumbered eye surgeon.

HUMAN RESOURCES (Manpower) Existing Human Resources For Eye Care Deliveries in the whole nation
Category Number Health Workers:
Population Population ratio
Ophthalmologist 168 1:298,000
Ophthalmic Assistant 391 1:130,000
(PBL Field Staff)
Optician/Optometrist 30 1:1.7 million
Orthoptists 2 1:25 million
Ophthalmic Nurses 250 1:200,000
Equipment Technical 5
Eye Care Manager 25
PHC Workers trained 5,000 1:10,000 eye care
CORNEAL BLINDNESS CORNEAL ULCERS (Bacteria, Fungal, Viral, Nutritional (Childhood)
• One of the commonest causes of blindness in Myanmar.
• Common occurrence in the Ophthalmological practice common among farmers, agriculture workers, industrial workers 7 occupational hazard.
• Most corneal ulcers are resistant to treatment. • Perforation and Blindness common.
Comparison of Isolated Organisms causing Corneal Ulcers
Mya Han Ko Ko Tin No 100 cases 80 cases % %
1 Commensals 28 34 28 42.5
2 Coliforms 12 14 37.5 38.8
3 Pseudomonas Aeruglnosa 7 13 21.8 36.1
4 Staph: Aureus 6 1 17.5 2.8
5 Step: Pyogenes 1 2.8
6 Pneumococcus 1 3.12
7 Moraxella Lacunata 1 3.12
8 Proteus Mirabilis 1 3.12
9 Haemophifus lnfluenzae 1 3.12
10 , Fungus 4 7 12.5 19.4
11 No Organ1sms 40 10 40 12.5
Major Causes of Blindness in Myanmar 1998 (Total population- 50 million)
Causes of Blindness No. of Blind Proportion (%) of
person blindness
Cataract 190.000 63
Glaucoma 48,000 16
Posterior segment 21,000 7 disease
Trachoma 12,000 4
Corneal opacity 9,000 3
Ocular trauma 3,000 1
Others 18,000 6
Total 300,000 100
MAIN CAUSES
• MISMANAGEMENT
• POOR HEALTH EDUCATION
• LACK OF KNOWLEDGE OF ETIOLOGICAL AGENTS
• INAPROPLATE USE OF ANTIBIOTICS AND STEROIDS
• NON A VAILIBILITY OF ANTIFUNGAL DRUGS
1997 Dr. Aye Win Kyi Bacterial Flora of External Eye Infections
Eye Hospital Yangon
No. Bacterial Normal Eye Ext: Eye lnfe: (160) Cases (150) Cases
1 Coag: (neg) staph: 68% 32%
2 Diptheroids 30% 32%
3 Staph: aureus 26% -4 Moraxella 4% 13%
5 Bacillus species 2% 6.7%
6 Haemophillus species 2%
7 Streptococci 2% 6.7%
8 Pseudomonas - 6.7%
9 Coliforms - 2.7%
-59-

FUNGAL INFECTIONS KO KO TIN (80 CASES)
No. I Organism Remarks
1 I Candida Parapsilosis With Staph Albus
2 I C~ndida Parasilosis With Diptheroids
3 i Candida Guilliermondi With Staph Albus
4 f Aspesgillaus Flavus (3) With Diptheroids
5 ! Aspesgillaus Flavus i
With Non Haemo: Strep
HERPETIC OCULAR INFECTION . Less common than bacterial and fungal infections . . Common among patients with Tuberculosis Malignant disease H.I.V. patients. . Laboratory tests not available yet. . Each and every case of keratitis and corneal ulcer-possibility of viral etiology should be considered. . Antiviral drugs as eye drops and tables are available but they are very much expensive.
Prevalence of Herpetic ocular infection (K.K.K. 1998)
HSV I HSV HZO HZO --··-
NO I % NO %
36 I 60% 24 40%
-60-
KHIN MG AYE (1995) CULTURE RESULTS OF 32 PATIENTS WITH
FUNGAL INFECTION (CORNEA)
22 %
• A'pergillus fumigatu. !.ll Candida Albican
Hl Negative Culture
Refraction service system in Myanmar • Ordinary refraction and post operative refraction
mainly done by Ophthalmologists. • Because of very few refractionists and optometrists . • Refraction mainly done by Retinoscopy. • In the Hospitals and in some eye care centres
refraction is done free of charge by the refractionists. • Autorefractometer is rarely used, but they are widely
used in private eye clinics. • Field visits by ophthalmologists and refractionists are
frequent to villages and remote areas - eye examination and refraction are done free of charge and reading spectacles are given free.

Sources of data
• Year 2000 • 17 Eye clinics from 17 general hospitals
North 2 Northeast 5 Central 3 East 1 South 6
• Total of 242,674 OPD patient visits • 20,891 eye patient admissions
- Infection-related diagnosis in OPD
1. Conjunctivitis 5.11 % 2. Viral conjunctivitis,EKC,AHC 4.82% 3. Hordeolum 3.91 % 4. Keratitis s. Uveitis,iridocyclitis,iritis s. Corneal ulcer 7. Blepharitis 8. Dacryoadenitis 9. Keratoconjunctivitis 10. Chorioretinal inflammation
1.68% 1.27% 1.25% 1.18% 0.66% 0.64% 0.30%
-61-
Causes of Monocular Blind 1994
% prevalence per 1000
• Cataract 51 4.54
• Phthisiscal/disorganised/ 13.5 1.20
absent globe • Corneal opacity 6.2 0.55
• Optic atrophy 6.2 0.55
• Glaucoma 5.1 0.45
Size classification of hospitals in the study
• small 4000-7000 OPD visits/year • medium 10,000-15,000 OPD visits/year • large 18,000-35,000 OPD visits/year
-3 small -9 medium -5 large
Infection-related diagnosis inOPD
11. Herpes ocular disease 0.22% 12. Endophthalmitis 0.19% 13. Zoster ocular disease o. 16 %
14. Trachoma 0.15% 15. Neonatal conjunctivitis 0.12% 16 Inflammatory of orbit 0.12 %
17. HIV disease o. 11 %
18. 4.Fl21 B ,::O)JiljO)A.71'F*'Z'@iE

700°o
600°o
500'o
400",
300',
200°:
1 ooc~
000°:
Serious ocular infections in OPD
Corneal ulcer
o keratitis
c corneal ulcer
• llerpes ocular disease
o zoster ocular dtsease
• orbttaltnflammatton
Keratitis
Uveitis
rmuveitis
0 chonoretimtis
o purulent and other endophthalmitis
oTrachoma
a HIV disease
OPOocular tnfect!Ons m hosprtals of different sizes
osmali m medrum olarge
11~ II
~ I oiJ 00 00 <ILm lk ~ Sb .c:B.b.~ . ......€L . j " . " 1'! t i Jii j Q
~ H jj ~ ~ j E i ~ ~ " ~~ ~ " i f ~ " 1! : ~ ~ ~
Distribution of IPD ocular infections in different regions
oNorth
oNE
12.00~'0
10.00%
8.00%
6.00%
4.00%
2.00%
ocentral
oEast
"' "' "' E "' "' c " "' :::: "" "" 0 u
-~ " "' > ':; "' .,; > E 0 t; !1 ~ .. 'C ::1 .. <I> :e E
" 'C c " .c 0 "' ~ <I> 0 :E c 0 c
~ Q. .c ~ 0 0 0
u " 'C u
•South
oTotal
'C c <I>
-62-
7.00% 6.00% 5.00% 4.00% 3.00% 2.00% 1.00% 0.00%
1.
2.
3.
4,
5.
6.
7.
8.
9.
10.
Distribution of OPD ocular infection in diferent regions
Ocular infection in IPD Keratitis 1.68% Uveitis, iridocyclitis, iritis 1.27% Corneal ulcer 1.25%
Chorioretinitis 0.30% Herpes ocular disease 0.22% Endophthalmitis 0.19% Zoster ocular disease 0.16%
Trachoma 0.15% Inflammatory of orbit 0.12%
HIV disease 0.11%
Distribution of IPD ocular infections in hospitals of different sizes
5 00°-o o small m medium 0 large
4 00"'-o
3.00'lo

Common Predisposing Factors
1. Organic materials trauma during agricultural work
2 Foreign bodies: dust, earth,stone,iron
3. Insects
4. Contact lens (Siriraj and Ramathibodi Hospital)
Patients treated before reaching hospital
%treated
Ramathibodi U Hospital i 70
---Siriraj U Hospital i
92
······
Chiang Mai Hospital 72.2
Buriram hospital 50.6 i
Corneal Ulcer Thai literatures review
authors 1 study center : year , cases
s;:;lapaha s .. et al i Chia~g-Mai u H;;;p;~~----1-·19n-i9iiiT·-·186 ~paiboon Y. ---tKonkaen·U-Hospiia;--~ 1986 • 183 ----------~- -------------~·---------~-~---···--·
Kunavisrut S .. et al i Ramathibodi U Hospital ' 1987-1988 : 60 -------~----------~-------+----Kosirakwong P .. et al i Siriraj U Hospital 1989-1990 105 ---------~----i------------~-------,----,----------+··------Kanokkanpong S. 1 Songklanagarind U Hosp1tal : 1990-1993 ' 81
Asayak~n S.,et ;;r·ichi;;~-g-Mai Hospit;;;------;--,984-19Bil"' _____ 224 1------~---··~~-t-----~~-·~-------.-.<~--~----·-1-~-----·-Chinangrong T. I Buriram hospital · 1994-1995 : 235
1---------------+-------------------+-- --------+-------Kiorwuthinun M. 1 Sawanpracharuk Hospital , 19~ __ .) ___ 1_~
Fi-ai;.;s~---·--tu;:;;;~;;;;;;:;~i-H~;;;----:- 2001 2oo
-63-
Self~management
• average onset: 4-7 days before seeing doctor (Burirum Hospital)
• most of the patients see the health staff at the health offices as the first point of contact (Vajamun P.:A study of self-care behavior of the corneal ulcer patients at Maharat Nakhon Ratchasima Hospital .1994)
Laboratory investigation
• 18% (Udornthani Hospital)
• 22.4% (Data from 17 MOPH hospitals)
of cases' scraping sample were sent for smear/culture

Yields of smear and culture % of positive yield
smear culture --·~------~~
Ramathibodi U Hospital I 34.4 56.3
Siriraj U Hospital ! 58 51
Songklanagarind U Hospital i 38.2 34.5
Sawanpracharuk Hospital 48.8 : 9. ------~--------
Udornthani Hospital !
47.2
Causative Bacteria
Hosp1tal 1 2 ; 3 -----------+----------__j ______ _
pseudomonas . strep.pneumoniae :1
klebsiella
(52.6%) : (31.6%) '(5.3%) ............ -----------~------------;-----------
Konkaen U
Rarnalh!bOdt U pseudomonas streptococcus ' ___________________ ___, ________ +-------1---------------l
--~~r~!~.-- ___ ... !-~:~~~ona~----~ micrococcus ] Songklanagannd U pneumococcus 1 pseudomonas J
---------------- ----------~---------;-----+--------Chiang Mai pneumococcus i pseudomonas
Sawanpracharuk
Udorntt1an1
Hospital I·-Konf\acn l.'
Ram;tthihmli l;
~iriraj t:
!-><!\\<llljli<Ll'hil!U~
l.d,lrnthanl
(26.9%) (15.4%)
. ----···-···---~---~~----------4~------gm + cocc1 pseudomonas
pseudomonas staphylococcus
Causative Fungi
2 4 -- ------------------+------+------------1
lu-.arium , aspergillus I - )~~~~21__. ___ -~~~--J--------!--~
---~t'ip...:rgilltl'i~~m __ ___j______ __ ---+-------l '"'po..:rgillu!> : dmJnspnrium 1
Ju.,arium
ru..;arillnl
lu-.;Jrium
. ·-~~:")(~ .. ~~~ !. -~m + lungu-.
Ju-.anum i I
-64-
Causative organisms ~ %
~u~~~~ri~Ttungus I virus j,;,i~lu--~k~~;:;-~K_o_n_k_a_en __ u_H_o_s_p_lta_l+-__ 3_9 ___ 1~--2~_27 ___ ~ __ 1_1+1------~ Ramathlbodl U 70 6 I 10 1 13 3 i 6.1 Hospital ' 1 i . i !
~S~Ir~lr~~~U~H---o-s-p-lta_I __ I __ 5_3_.3 __ ~!--2--4-.B-~!----~-1-0.-5+;-----11-.4~ ~----------~------~-----1------L---~----~ Songklanagarlnd U 1 65.4 I 25.9 1 3.7 2.41 Hospital I i l ~~~-------~--t--~----~--~---------~ Chiang Mal I 46.4 i,· 41.5 ,
1· 8.5 ,
Hospital :
Results of treatment cases(%)
(2.6%)
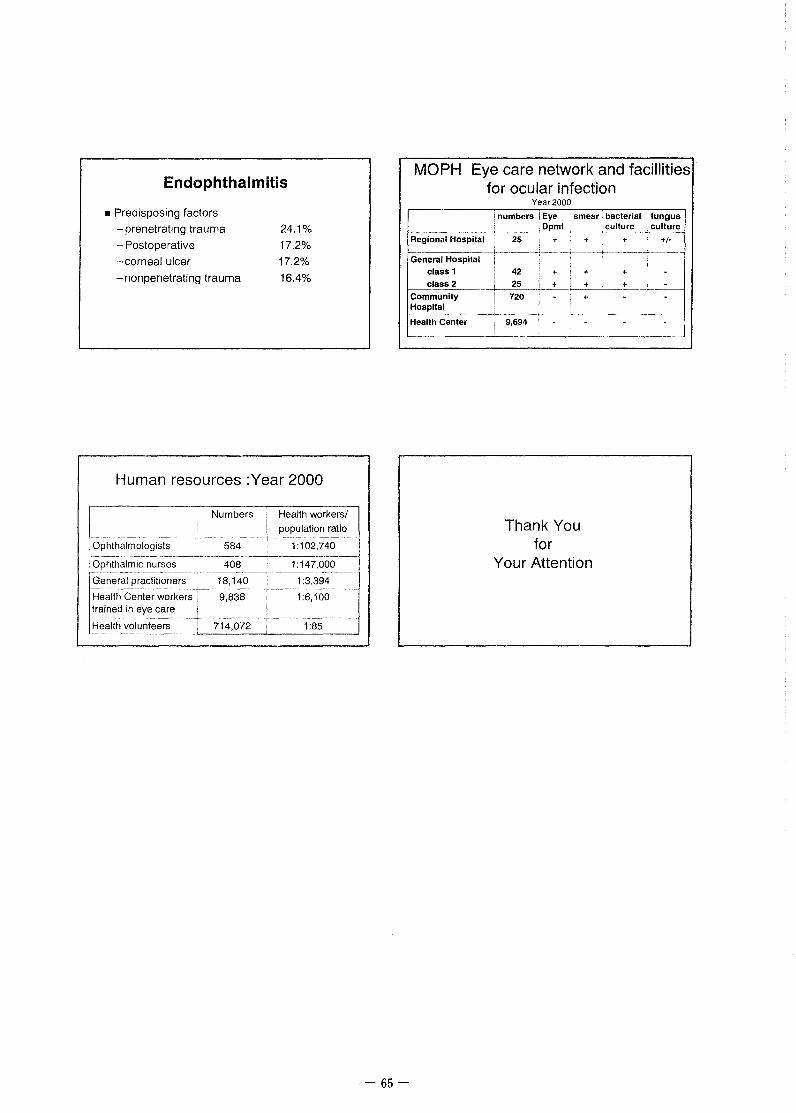
Endophthalmitis
• Predisposing factors - prenetrating trauma -Postoperative -corneal ulcer
-nonpenetrating trauma
24.1%
17.2%
17.2%
16.4%
Human resources :Year 2000
I : -- ---.Ophthalmologists
Numbers i Health workers/
!. population ratio
584 1:102,740
~t:)p_~~~~rl1~_n_::r~_e~-~---- -~~!3__~_,_---~~_o_o~----General practitioners . 18,140 i 1 :3,394 ---~-------~~----j---------------1~------~---
Health Center workers i 9,838 I 1:6,100 rained in eye care i i -~-------------"--------1----------
Health volunteers 1 714,072 I 1 :85 --~-·-----~·---
-65-
MOPH Eye care network and facillities for ocular infection
Year2000
! numbers i Eye smear . bacterial culture ------.--·--------- -- ·-··-··---~----
;!ll'rn'-_. "'- ·-- ----·---·-- ----------Regional Hospital
General Hospital class 1 class 2
Community Hospital
Health Center
:
i [
i
25 +
i
42 _j : i 25
720
! i
9,694 i i
Thank You for
+
+ + +
Your Attention
+
)
+ +
I -
fungus culture
+I-
---

Panelists:
Panel discussion 1 Ocular Infection
Panel Discussion on Weakness and Strength
1- Dr. Ngy Meng 2- Dr. Siphetthavong 3- Dr. Patpong 4- Dr. Ko Ko Tin 5- Dr. Tran Duy Kien
(Cambodia) (Lao) (Thailand) (Myanmar) (VietNam)
Cambodia : Weakness
At all levels of eye care network
1 . Poor Knowledge 2. Consult or treated by traditional heater 3. Misuse of medicine (steroid) 4. Presentation to eye hospital late 5. Referral system not well functioning 6. Lack of medicine, anti fungus, viral 7. Lack of microbiological laboratory in second and third level of eye
care system.
What Needs?
1. Community level :
Train volunteer health worker and PEC worker Health education Provide teaching material and transportation facility
2. Provincial level:
Special training eye doctor, MLP and laboratory technicians on microbiology Update on ocular infection treatment and surgical skill PKP Need laboratory equipment for smear, culture and sensitive test Need eye drug supplies as: anti fungus, anti viral Develop monitoring and supervision system
3. National and regional level Special training of microbiology Establishment of eye bank facilities and eye bank management
-66-

Special training on surveillance system for all eye care professionals Continuing to Upgrade knowledge for ophthalmologist Establishment of Subspecialty training Doing scientifically Research Need microbiology lab equipment and supplies Need eye bank facility and instruments
Lao P.D.R :Weakness
~ A reason: Poverty. People respect spiritual. Treat with medicine traditional. Low income. Low education. Lack of essential drug. Eye care network not strongly enough yet into community. Difficulties of terrain. Bad road Difficult to access to eye care services. No have essential drug. Low understanding the knowledge about eye problem.
- Almost staff at the health center do not get training in eye care
~ How can these barriers be overcome : 8 Primary level of eye care :
Health education for individual & families, booklet, Poster etc .... Sanitation & water supply. Training volunteer for community eye health workers. Provide essential drug for CEHWs to give the first aid and safe the eye. Every staff at the health center should be trained in PEC and they should know how to integrated into PHC Severe cases immediately referral.
8 Secondary level of care service : Health education. Training of staff of health centers. Special training course of ocular infection. Provide essential drug and some anti fungal drug for District Hospital. Immediate referral cornea ulcer cases to tertiary level.
-67-

Thailand
e Tertiary level of eye care : Adequate proper management preventing in serious of complication therapeutic. Refresh course of Keratoplasty. Training for sub special cornea clinic. Eye bank. Laboratory ( Smear, Gram stain , Culture ) Provide anti fungal & anti bacterial drug for provincial & regional hospital.
Thai's weak points in ocular infection
1.Surveillance and information system Although our information recording and reporting system have been established which require every hospital to record and report monthly to the central statistical department at the central level and publish their annual report at the provincial level and these data were made uniform by adopting ICD10,1CD9CM., we still lack a central responsible agency to analyses and make use of these data for eye care management.
2.0ur eye care network and facilities are now strongly setup and sufficient. Bacterial culture laboratories are existed in every general hospital in every province. Fungus culture laboratories are available in some regional hospitals. But these facilities are under utilized as only around 20% of corneal ulcer cases are scraped and sent for smear or culture before treatment despite our general practice guidelines issued by Thai Royal Society of Ophthalmology recommend that every suspected corneal ulcer cases should do so. Without these evidence-based practice ,ophthalmologists tend to give broad spectrum antibiotics as first choice. And they are usually under affluence by commercial drug company or rely on newly developed drug. This will risk drug resistance and increase the cost of treatment.
3. Our eye bank system is still weak. A strong eye bank system is required to support the successful combat of serious corneal infection. We still lack public motivation and eye bank management skills to adequately supply corneal tissue for PKP
Additional comments: Support Prof. Para that we should have socio-cultural knowledge of the people who often come late to seek medical help in corneal ulcer. For the patients who get corneal injury in the farm during their harvest season before developing ulcer. They need to wait until finish harvesting before they can go to see a doctor. The ophthalmologists should be flexible and delegate their authority to
-68-

the community doctor or health officer to give initial simple antibiotics treatment and give daily follow up close to their home while they still can continue their work.
Myanmar
I. Weakness.
1. Lack of health education in the community. 2. Mismanagement of eye infection. 3. Lack of medicine (eg. Anti bacterial, antifungal, and antiviral drugs). 4. Lack of laboratory facilities. 5. Late arrival to the health centers. 6. Indiscriminate use of steroids by the patients.
II. What needs?
1. Community level • Health education to the public and PEC workers, village elders,
teachers, red cross volunteers, etc ... • Training of PEC workers.
2. District level • Training of health assistants, field workers and dressers. • Need laboratory tests for identification of organisms • Need adequate drug supply. • Monitoring supervision and referral. • Surveillance by district PBL Ophthalmologist and its team
should be done effectively and regularly.
3. Tertiary level. • Upgrading of eye bank facilities and eye bank management. • Need pathologist, microbiologist, immunologist. • Training of ophthalmologists for PKP. • Law enforcement concerning with cornea bank act should be
implemented by Government.
4. National level. • Research work. • Proper statistical recording and monitoring.
-69-

VietNam:
• Strength: Existing an eye care network from central to community PEG has been integrated into PHG GHWs have been trained Some center can do smear test and culture test
• Weakness Patients are not aware about eye problem Eye drops were abused by the patients themselves Late referral from lower level to higher level Some special eye drops (anti fungal) are not available Laboratory is not set up in every province In tertiary level laboratory technique is not developed and function not very well Lack of instrument for corneal transplant Lack of eye bank Research on microbiology is limited
• Solutions: Health education on eye care Better control antibiotic and steroid eye drop (new law for example) Training more GHW on PEG Develop microlab in the tertiary and secondary levels Establish eye bank Equip specific equipment for corneal transplant in tertiary level
-70-

The Matrix on Ocular Infection Management
1 . Problem identification
Level of eye facility Quality of eye care Present situation Problem identified Solution (*)
1.
Community Self eye care (by 2. people themselves) 3.
4.
Auxiliary eye care (by 1.
Health centre 2. non-medical)
3.
Community Medical eye care (by (**)
ophthalmic medical .hospital
officer)
Provincial hospital Specialized eye care
by ophthalmologist
Specialized eye care (***)
Regional Hospital by ophthalmologist
Sample
(*) In general people are not much aware of living style and cleanness poor personal hygiene. Community environment is also poor. Slow action when anything happens with the eye, e.g. minute corneal injury. PH workers lack proper training in eye care.
(**) Eye care quality is rather poor because of staff lack proper training. No adequate drug.
(***) No drug available for fungal infection. Therapeutic keratoplasty is not available. Therapeutic contact lens is not available. Very poor laboratory facility without culture

2. Eye care network
-- ------- ,---------------- - ··- -----·-- ···--- --
Minimum service Minimum facility Supplies and
Level of eye facility Quality of eye care Present situation equipment necessary Training need Activity needed developed
for support
Self eye care (by To know this is infection
Eye drop and ointment To strengthen health
Community people themselves)
and seek for immediate (specify the drugs)
education, booklet, help poster
To recognize this is an Eye drop and
infection.
Health centre Auxiliary eye care
To give first aid and refer antibiotics Additional hours to
(by non-medical) preparations (specify PEC refresher course to the higher level after
the drugs) adequate management
To recognize this is a
Medical eye care serious infection. Smear
Antibiotics eye drop, Additional hours to
Community hospital (by ophthalmic To give first aid and refer Sensitivity test
ointment, oral/injection PEC refresher course
medical officer) to the higher levels after (specify the drugs)
adequate management
Identify causative agent. Smear 1. Antibacterial drug
Specialized eye care Adequate management
Sensitivity test 2. Antifungal drugs Special training
Provincial hospital for preventing serious course on ocular by ophthalmologist Culture 3. Microscope
complications ?? 4. ??
infection (one week?)
Therapeutic keratoplasty
Identify causative agent.
Specialized eye care Adequate management
Regional Hospital for preventing serious by ophthalmologist
complications Therapeutic keratoplasty

3. Surveillance and recording and reporting system
Responsible body Level Who collect R/R system Surveillance system The use of information
Where to be sent
I Information
Item:
What
The provincial/regional Where Sentinel
When Item: Report: coordination committee are
Provincial and responsible for data collection Magnitude Frequency Weekly
Management Weekly Monthly regional level and report to the central level.
Outcome Monthly Quarterly Technical interpretation must be
Frequency: Quarterly Annual added.
Weekly Annual
Monthly
Quarterly
Annual
Provincial/regional coordinating To be presented in academic
committee are responsible to meeting regularly
report to the central coordinating
National level committee. The report is then
submitted to the PBL national
committee with data
interpretation and
conclusions/recommendation.

1. Problem identification
Level of eye facility Quality of eye care
Self eye care
(by people
Community themselves) and
Health volunteer
worker
Health center staff
Health center .and auxiliary eye
care
Specialized eye care Provincial hospital
by BED or or referral hospital
ophthalmologist
Regional Hospital Specialized eye care
or National hospital by ophthalmologist
The Matrix on Ocular Infection Management Cambodia
Present situation Problem identified
- Poor hygiene - Poor knowledge and
socio economic - Not aware of serious problem
- Transportation and - Behavior, traditional medicine
communication difficulty treatment
- Self treatment - No trust in health care
- Farmer and children at high risk of and eye care
- No protection to mini ocular infection during in harvest
accident trauma
- Minimal training no
- Not sufficient knowledge budget for refreshment course
- Not functioning - No drug
- No drug available - Low salary, no intensive
support
- No drug anti fungus, anti viral - Eye health care low
available priority
- No laboratory, microbiology - Funding support
- Limitation knowledge of BED - Available drug
- Lack of drug
- No anti fungus, anti viral drug - Microbiology not available
- No microbiology technician and and lab technician
- Nursing by patient - Limit of ophthalmologist
- No keratoplasty and subspecialty eye care
- No eye bank
Solution
- Early protection to mini
accident injury and infection
- Early simple treatment
especially in harvest season - Restore trust in health care
system
- Training health center staff
to manage and referral case and refreshment course
' - Community share by
payment for treatment
- Improved funding support
from government and
patient charity
- Provide supplies for
microbiology laboratory
- Build the reliable support
system by using resources
of general hospital
- Subspecialty eye care
- Funding support

2. Eye care network
Level of eye 1 Minimum service I Minimum
Supplies and equipment facility
Quality of eye care Present situation Activity needed
facility necessaryforsupport
Training need developed
- Poor hygiene - To know ocular - Not aware of infection and - Health education
serious problem emergency - Health center to people
- Behavior, traditional treatment and close to - Antibiotic: - Training village
Self eye care (by medicine treatment know the place people live gentamicin, chloram,
volunteer to know Community people ocular infection
themselves) - Self treatment for immediate - Health tetracycline ointment
- TV advertisement - Farmer and children help volunteer - Teaching material at high risk of ocular - Self care team worker
and poster
- Inform to public by infection during in - Private drug field worker harvest store
- Training PEC and
Referral Antibiotic eye drop: refreshment - Not sufficient -.Health center - -
knowledge Many private I system Genta, chloram, tetra 1%, - Course express on -
Health centre Health center staff ocular infection - Not functioning dispensaries - Intensive Povidone Iodin 5% - Training private
- No drug available - Staff motivation support - Training material dispensary and pharmacies staff
- Carry on by Smear - Antibacterial drug: -
- No drug anti one BED and 2
sensitive Genta, ciproflox ... - Upgrade Special
nurses training course on fungus, anti viral test, Gram - Antifungal drugs: - Use laboratory ocular infection Specialized eye available stain Natamicin, Provincial in general - Training for care by BED and - No laboratory, - Culture Amphoterecin B hospital I hospital keratoplasty ophthalmologist microbiology - Donation - Antiviral: Zovirax, - Therapeutic - Microbiology - Limitation cornea, eye - Microscope for
knowledge of BED keratoplasty
bank from laboratory microbiology training course for
- Microbiology lab technician central level - Material for keratoplasty lab technician
·-·

-----· --------- ---- ··--- ~---~· ··-- . ----------~-·----I
I
- Research I - Report and
I surveillance
I system ----+---·-···-f--
- Use laboratory
in general - Upgrade Special hospital -Smear
Antibacterial drug: training course on -- No anti fungus, anti - Therapeutic sensitive test,
Genta, ciproflox ... ocular infection viral drug Keratoplasty Gram stain
Antifungal drugs: - Training for -- No microbiology - Microbiology lab - Culture
Natamicin, keratoplasty Specialized eye technician and technician - Eye bank
Amphoterecin B ... - Microbiology Regional
care by - Nursing by patient - Research - Pathology
Antiviral: Zovirax, training course for -Hospital
ophthalmologist - No keratoplasty - Report and service
Microscope for lab technician No Subspecialty clinic --surveillance - Subspecialty
laboratory microbiology - Cornea system cornea
Material for keratoplasty subspecialty --More service
ophthalmologist training
responsible

3. Surveillance and recording and reporting system
--·
Responsible body ---
Level Who collect R/R system Surveillance system The use of information Where to be sent
- Information
Item: -Develop data collection
-Number ocular infection The provincial/regional
-Cornea ulcer (Keratitis) sheet:
coordination committee head of - Sentinel eye unit are responsible for data
From every heath center and Item:
province: Report: Provincial and collection and report to the - No cornea ulcer regional level central level subcommittee for
-Every month from HC Referral
- Every 3 Monthly -the PBL.
-Management treatment Treatment
-To central -
Collect the data from health and referral
Cause -
center every month and analysis Result Outcome:
Frequency: -No blind
- Monthly Frequency:
- Every month
- Information Develop data collection Item: sheet
-Number ocular - Sentinel infection Cornea Item:
- To be presented in Provincial/regional coordinating -Ulcer (Keratitis) - No cornea ulcer academic meeting committee are responsible to From every heath center and - Referral
report to the central coordinating province: Treatment regularly every 4
-National level month subcommittee PBL for data -Every month from HC - Cause from trauma - Find out the interpretation and -Management treatment - Germ identify
conclusions/recommendation. and referral Frequency: weakness
and strong Result Outcome: - 3 Monthly -No blind Analysis data and set the
I Frequency: priority sold the problem
- Every 3 month - --~- ·----
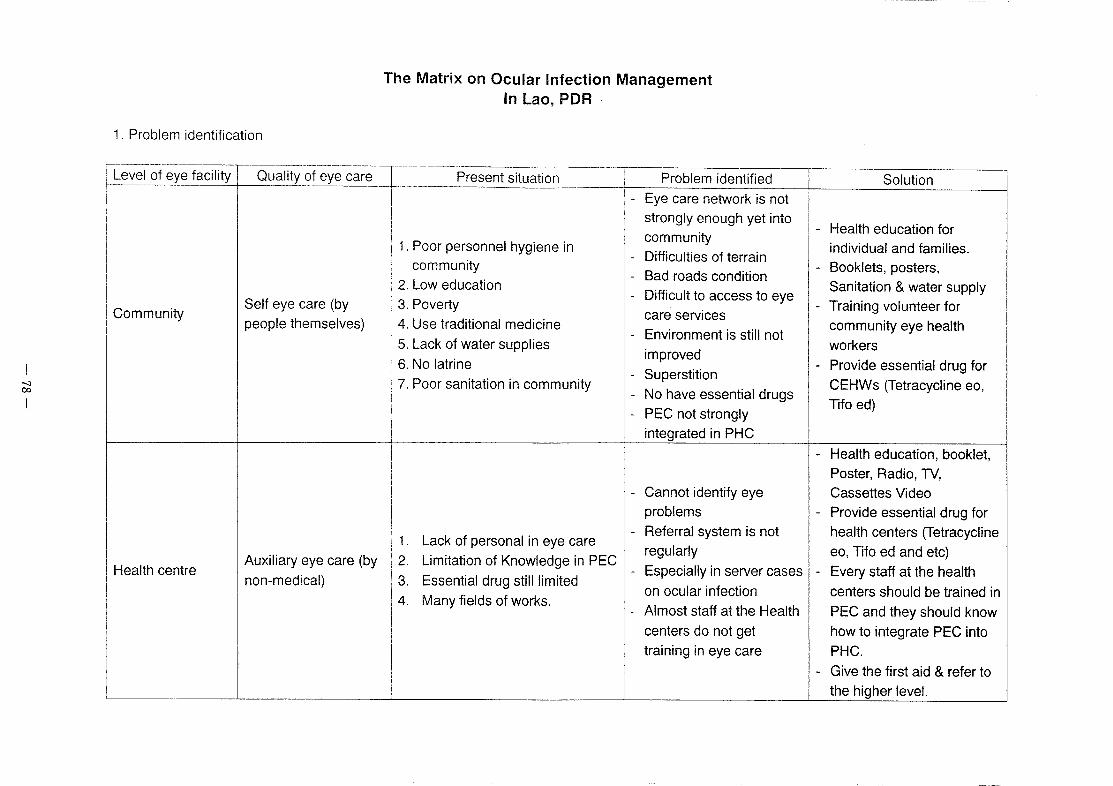
1 . Problem identification
The Matrix on Ocular Infection Management In Lao, PDR
r-------·---------
oualityQfe;;e-ca,._=-r =-= P;ese~iSituOt,;,n ==-1 _ ~~;~~~;i:e~~~~~~~~~~ Level of eye facility 1--------
1. Poor personnel hygiene in community
- Difficulties of terrain community
- Bad roads condition 2. Low education
Difficult to access to eye -
Community Self eye care (by 3. Poverty
care services people themselves) 4. Use traditional medicine
- Environment is still not 5. Lack of water supplies
improved 6. No latrine
- Superstition 7. Poor sanitation in community
No have essential drugs -- PEC not strongly
integrated in PHC
- Cannot identify eye
problems
- Referral system is not 1. Lack of personal in eye care
regularly Auxiliary eye care (by 2. Limitation of Knowledge in PEC
Health centre - Especially in server cases non-medical) 3. Essential drug still limited
on ocular infection 4. Many fields of works.
- Almost staff at the Health
centers do not get
training in eye care
Solution l
- Health education for individual and families.
- Booklets, posters,
Sanitation & water supply
- Training volunteer for
community eye health
workers - Provide essential drug for
CEHWs (Tetracycline eo,
Tifo ed)
- Health education, booklet, Poster, Radio, TV,
Cassettes Video - Provide essential drug for
health centers (Tetracycline
eo, Tifo ed and etc) - Every staff at the health
centers should be trained in
PEC and they should know
how to integrate PEC into PHC.
- Give the first aid & refer to
the higher level.

- Health education 1. Ophthalm·lc nurse cannot identify - Training of staff of health
the causes of ocular infection - Poor laboratory
centers 2. Many field of works - Special training course on
Community Medical eye care (by 3. Limitation of essential drugs - Referral system is not so
ocular infection good where do not have
hospital ophthalmic medical 4. Some district don not have - Immediate referral corneal (district hospital) officer) ophthalmic nurses
MLP in eye care ulcer cases to secondary
- Can not affordable/anti 5. The patients who have ocular
fungal drugs levels
infection/cornea ulcer come late - Surveillance, recording &
to see the ophthalmic nurse reporting system to
provincial level.
- Special training course on
- Some provinces where do not ocular infection
- Continue Health education have ophthalmologist can not
to public & community identify the causes of ocular - Poor laboratory (smear,
infection Gram stain culture) - Training trainer
Specialized eye care - Provide anti fungal & - . Very few ophthalmologists at - Expensive cost of anti
Provincial hospital by provincial levels treatment fungal & antibacterial
antibacterial drugs for
(Secondary level) ophthalmologists/basic - Basic eye doctor can not clinically drugs
provincial hospital
eye doctor - Needs laboratory to identify identify the causes of ocular - The cost of Anti fungal
infection drugs is very expensive the organism (Gram stain,
smear & sensitive test) - Lack of specify eye drop for
- Surveillance, recognizing & fungal
reporting to the Center or
Regional Hospital
- Ophthalmologist can identify the - Poor laboratory (smear, - Continue health education
causes of ocular infection Gram stain culture) - Training for sub special
Regional Hospital/ - Do not have sub special cornea - Expensive cost of anti cornea clinic & upgrade on
Ophthalmology Specialized eye care
clinic fungal & antibacterial ocular infection treatment &
Centre level by ophthalmologist
- Do not have eye bank yet drugs surgical skill PKP
- No have anti fungal drug - We received very few - Setting up laboratory facility
(Amphoteracine B, Natamycine donors from abroad - Provide ant- fungal &

00 0
L_-___ :~:---~-r e-k-_.) ----··:_-_:_···-_--_:-_-_-:::: l ________ ~[ ~~~"f~:~~~~~:: ~~:nter 2. Surveillance and recording and reporting system
Responsible body Level Who collect R/R system Surveillance system The use of information
Where to be sent
Information
Item:
1. What ocular infection
(recording & reporting) - Trachoma
- Endophthalimits - Viral infection - Uveitis Sentinel (Provincial level)
The provincial/regional Suppurative keratatis Item: -
Report: coordination committee are Etc Frequency: -
-Monthly Provincial and responsible for data collection 2. Where: Provincial hospital -Monthly 1
regional level and report to the central level. level -Quarterly
-Quarterly Technical interpretation must be -Annual
3. When: every month, every -Annual added.
4 month, every year
4. Magnitude:
- No OPD cases of ocular
infection
- No IPD admission 5. Management:
- No of patient treat fungal
- No of patient treat

00 .....
National level
Provincial/regional coordinating
committee are responsible to
report to the central coordinating
committee. The report is then
submitted to the PBL national
committee with data
interpretation and
conclusions/recommendation.
bacteria - No of patient treat anti
viral - Etc.
6.0utcome - How many cases had a
good treatment - How many cases failed
post treatment
- How many cases PKP
- How many cases
enucleations or eviscerations
- Etc 7. Frequency:
- Every 1 month time - Every 4 month time - Every year 1 time
-One time I year
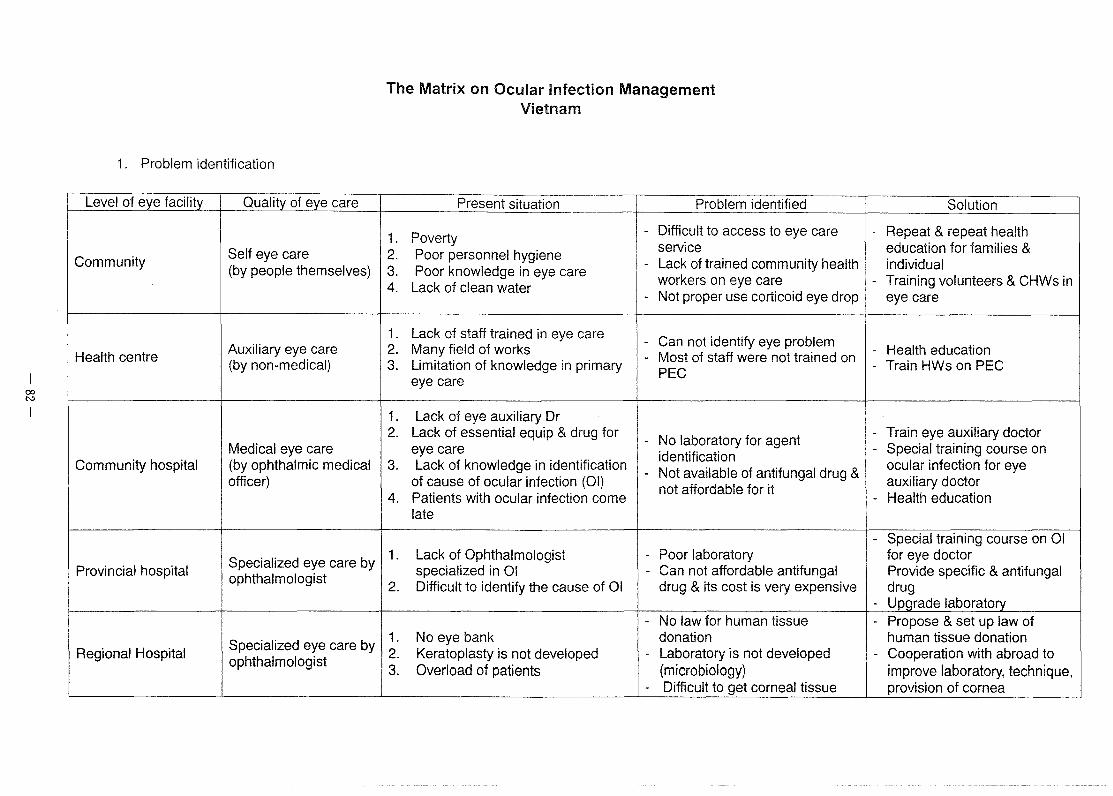
00 N
1 . Problem identification
Level of eye facility Quality of eye care
Self eye care Community
(by people themselves)
Health centre Auxiliary eye care (by non-medical)
Medical eye care Community hospital (by ophthalmic medical
officer)
Specialized eye care by Provincial hospital
ophthalmologist
Specialized eye care by Regional Hospital
ophthalmologist
The Matrix on Ocular Infection Management Vietnam
----
Present situation Problem identified
1. Poverty - Difficult to access to eye care
2. Poor personnel hygiene service
3. Poor knowledge in eye care - Lack of trained community health
4. Lack of clean water workers on eye care
- Not proper use corticoid eye drop
1. Lack of staff trained in eye care - Can not identify eye problem 2. Many field of works - Most of staff were not trained on 3. Limitation of knowledge in primary
PEG eye care
1. Lack of eye auxiliary Dr 2. Lack of essential equip & drug for
- No laboratory for agent eye care
identification 3. Lack of knowledge in identification
- Not available of antifungal drug & of cause of ocular infection (01)
not affordable for it 4. Patients with ocular infection come
late
1. Lack of Ophthalmologist - Poor laboratory specialized in 01 - Can not affordable antifungal
2. Difficult to identify the cause of 01 drug & its cost is very expensive
- No law for human tissue 1. No eye bank donation 2. Keratoplasty is not developed - Laboratory is not developed 3. Overload of patients (microbiology)
- Difficult to get corneal tissue
Solution
- Repeat & repeat health education for families & individual
- Training volunteers & CHWs in eye care
- Health education - Train HWs on PEG
- Train eye auxiliary doctor - Special training course on
ocular infection for eye auxiliary doctor
- Health education
- Special training course on 01 for eye doctor Provide specific & antifungal drug
- Upgrade laboratory - Propose & set up law of
human tissue donation - Cooperation with abroad to
improve laboratory, technique, provision of cornea

00 w
2. Eye care network
Level of eye Quality of eye facility care
Self eye care Community (by people
themselves)
Auxiliary eye care Health centre
(by non-medical)
Medical eye care Community
(by ophthalmi.c hospital
medical officer)
Specialized eye Provincial hospital care by
ophthalmologist
Specialized eye Regional Hospital care by
ophthalmologist
Minimum service Present situation Activity needed
- Village health - To know this is infection
volunteers with very poor knowledge in and seek for immediate
PEC help
- To recognize this is an - No staff responsible infection.
for eye care -To give first aid and refer to professionally the higher level after
adequate management
- A small proportion - To recognize this is a
of district hospital serious infection.
have eye doctor - To give first aid and refer to
- Most of district hospitals have eye
the higher levels after
auxiliary doctor adequate management
- Identify causative agent.
- Very few eye doctor - Adequate management for specialized in ocular preventing serious infection complications
- Therapeutic keratoplasty
- Have a Department - Identify causative agent.
responsive for - Adequate management for
ocular infection preventing serious
disease complications - Therapeutic keratoplasty
Minimum facility Supplies and
developed equipment necessary Training need for support
- Eye drop and - To strengthen health ointment education, booklet,
(specify the drugs) poster
- Lack of essential - Eye drop and drug & equipment antibiotics - Additional hours to
for eye care preparations PEC refresher
No gram stain (specify the drugs) course -
- Anti-biotics eye - Additional hours to No smear sensitivity drop, ointment,
PEC refresher test oral/injection (specify the drugs) course
- Almost Provincial
- Low cost - Special training
Anti-bacterial & hospital can do
Anti-fungal drugs course on ocular
gram stain & infection (one week) culture
- Microscope
- Specific - Special training - Can do gram
Anti-bacterial & course on corneal stain & culture
Anti-fungal drug graft and new
(No microscope) - Microscope technique of
microscope

3. Surveillance and recording and reporting system
-- .,. Responsible body
Level Who collect Where to be sent
R/R system Surveillance system The use of information
-Information Item:
The provincial/regional What coordination committee are Where
Report: Provincial and responsible for data collection When Quarterly Quarterly regional level and report to the central level. Magnitude: Annual Annual Technical interpretation must be Management
added. Outcome: Quarterly Annual
-Information
Provincial/regional coordinating Item:
What committee are responsible to
Where report to the central coordinating
When To be presented in academic
National level committee. The report is then
Who (do) Annual submitted to the PBL national meeting regularly committee with data
Magnitude:
interpretation and Management Outcome:
conclusions/recommendation. Quarterly Annual

00 c.n
1 . Problem identification
Level of eye facility Quality of eye care
Community Self eye care (by
people themselves)
Auxiliary eye care Health centre
(by non-medical)
The Matrix on Ocular Infection Management Myanmar
Present situation Problem identified
1. Poor personnel hygiene - Eye care network not
2. Inadequate knowledge on eye enough
disease - Lack of health knowledge
3. Use of traditional medicine - Improved enough to
4. Inadequate water supply in promote health
central Myanmar
5. Poor sanitation in community
1. Inadequate knowledge of
common eye infection
2. Limited essential drugs
3. Less interest in eye care
because of inadequate
knowledge, drugs and many
field works
Solution
- Health education through
media, school teacher,
volunteers - Primary eye care training to
volunteers and those who
actively take part in welfare
of the community and
VGO's
- Improving sanitation and
environment - Essential drugs to the
volunteer workers
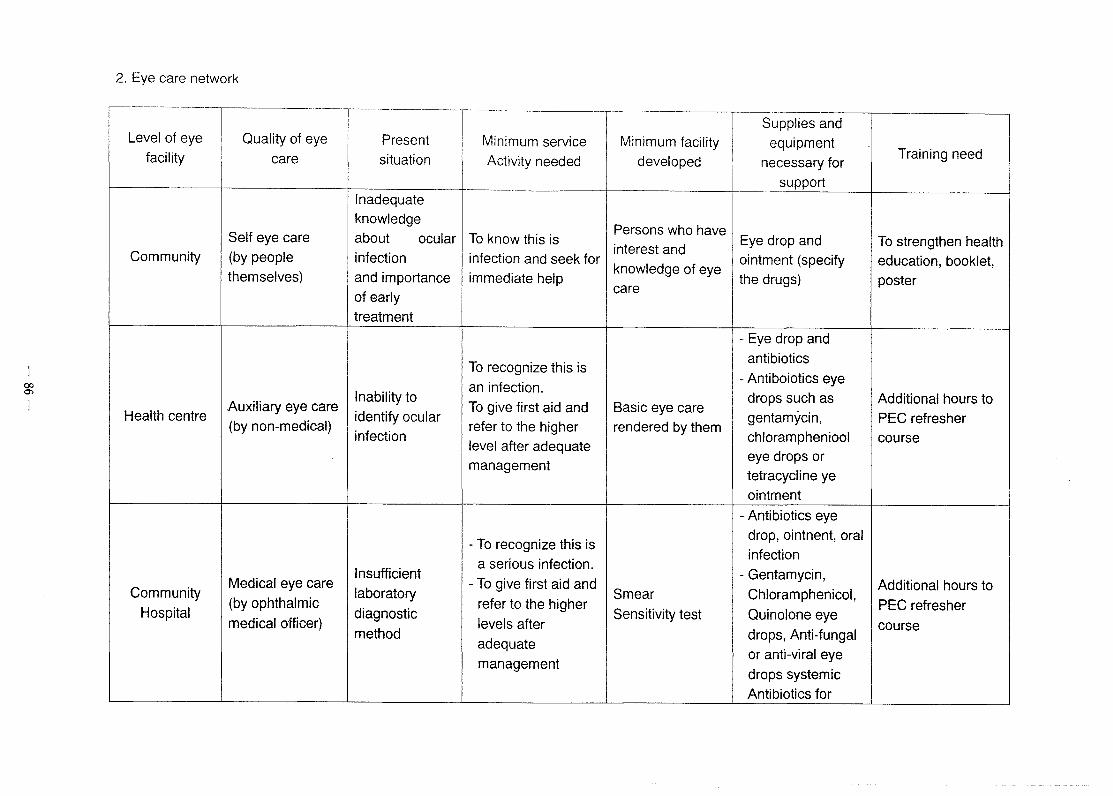
00 0>
2. Eye care network
---- -------·· -·--·---
Level of eye Quality of eye facility care
1------ --
Self eye care Community (by people
themselves)
.Auxiliary eye care Health centre
(by non-medical)
Medical eye care Community
Hospital (by ophthalmic
medical officer)
-----·-
Present
situation
!---- --Inadequate
knowledge about ocular infection
and importance
of early
treatment
Inability to
identify ocular infection
Insufficient
laboratory
diagnostic
method
Supplies and Minimum service Minimum facility equipment Activity needed developed necessary for
Training need
----···---· support
Persons who have To know this is
interest and Eye drop and To strengthen health
infection and seek for knowledge of eye
ointment (specify education, booklet, immediate help the drugs) poster
care
- Eye drop and
To recognize this is antibiotics
- Antiboiotics eye an infection.
To give. first aid and Basic eye care drops such as Additional hours to gentamycin, PEC refresher
refer to the higher rendered by them chloramphenicol course
level after adequate eye drops or
management tetracycline ye
ointment
- Antibiotics eye
-To recognize this is drop, ointnent, oral
infection a serious infection.
- Gentamycin, -To give first aid and Additional hours to
Smear Chloramphenicol, refer to the higher
Sensitivity test Ouinolone eye PEC refresher
levels after drops, Anti-fungal
course adequate
or anti-viral eye management
drops systemic
Antibiotics for

I I severe infection
cases _Identify causative
1 . Anti bacterial agent. _Smear sensitivity
1 2. Anti-fungal
Special training Insufficient -Adequate
culture 3. Anti-viral
course on ocular
Specialized eye laboratory management for
_ Surgical unit for 4. Microscope
infection
Provincial care by
diagnostic preventing serious corneal
5. Surgical
Hospital ophthalmologist
method complications transplantation
Instruments _ Therapeutic
Keratoplasty
_ Special training _ Identify causative
course on ocular 1 . Microscope
infection. agent
_ Smear sensitivity 2. Surgical
_ Hand on training
Inadequate -Adequate
culture Instruments New
for corneal
Specialized eye facility and man management for
_ Surgical unit for Eye Bank
transplantation
Regional care by poser for
preventing serious corneal
3. Essential eye and modern
Hospital ophthalmologists corneal
complications transplantation
drops and drugs management of
transplantation _ Therapeutic
corneal infections keratoplasty I I

00 00
3. Surveillance and recording and reporting system
,...-------·--·-
Responsible body Level Who collect
Where to be sent
The provincial/regional
coordination committee
(Regional and District
Provincial and Prevention of Blindness Teams)
regional level are responsible for data
collection and report to the
central level. Technical
interpretation must be added.
Provincial/regional coordinating committee are responsible to
report to the central coordinating
National level committee. The report is then
submitted to the PBL national
committee with data
interpretation and
conclusions/recommendation.
------~··-·-- --- ---
R/R system Surveillance system The use of information
·-
Information
Item
What
Where -Sentinel
When -Item -Report
Magnitude -Frequency -Weekly
Management -Weekly -Monthly
Outcome -Monthly -Quarterly
Frequency -Quarterly -Annual
Weekly -Annual
Monthly Quarterly Annual
Quarterly Annually To be presented in academic
meeting regularly

00 <.0
1 . Problem identification
Level of eye facility Quality of eye care
Self eye care (by Community
people themselves)
Health centre Auxiliary eye care (by
non-medical)
Community Medical eye care (by
ophthalmic medical hospital
officer)
Provincial hospital Specialized eye care
The Matrix on Ocular Infection Management Thailand
Present situation Problem identified
1. Lack of knowledge,
1. Misbelief, negligence, 2. Modern eye care is
inapropriate self-care unavailable or hard to
access 2. Quack
3. Availability of 3. Self bought drugs
4. Unable to help one's self (old uncontrolled dangerous
drug people)
4. Lack of family or social 5. No eye protection during work
support 5. Lack of concern, attitude
1. Inappropriate management of 1. Lack of knowledge,
cases training
2. No firs aid equipment and drug 2. Lack of supply
1 . Inappropriate management, too 1. Lack of knowledge,
much dependent on provincial training
hospital 2. Essential drugs and
2. Treatment capacity is limited equipments are
3. Delayed treatment and referral unavailable
Limited capacities and facilities
Solution
1. Training
2. Consultation system with
specialist
3. Development of guidelines
4. Supervision and
monitoring by community
hospital
1. Training
2. Consultation system with
specialist
3. Development of guidelines
4. Supervision and
monitoring by
provincial/regional hospital

-------- I by ophthalmol;gist_r________________________ --- f · -------
--- I 1. Limited--~hoices of antifungal ______ --
drugs
2. Fungal culture facility is 1. Weak: 1. Stimulate local eye bank
Specialized eye care unavailable in some hospitals eye bank management and seek supplies from
Regional Hospital by ophthalmologist
3. Donor cornea is unavailable for 2. Too much workload to outside country's eye bank keratoplasty follow standard practice 2. Clinical audit and increase
4. Trial and error treatment rather guidelines role of MLP than evidence-based (in corneal
ulcer)
2. Eye care network
Level of eye Quality of eye Present situation
Minimum service Minimum facility Supplies and equipment Training need
facility care Activity needed developed necessary for support
1. Common corneal ulcers
develop after 1. How to
minor injury manage F.B. Chloramphenicol eye drop and To strengthen
Self eye care during To know this is First aid for ointment health
Community (by people agriculture infection and seek corneal Education poster education,
themselves) and factory for immediate help abrasion Eye protection devices booklet, poster
works 2. Hygienic eye
2. Hordeolum care
and
blepharitis
People coming To recognize this Eye irrigation set Eye drop and antibiotics Additional hours
Health Auxiliary eye for first aid and is an infection. Fluorescein strip preparations Chloramphenicol
to PEC care(by initial treatment To give first aid and cobalt blue eye drop and ointment,
centre refresher non-medical) Unrecognition of and refer to the penlight terramycin ointment
serious cases higher level after Communication Education poster, spot course

I adequate ! line for diagnosis pictures management I consultation poster, booklet
Lack of To give initial
confidence in treatment and
Fluorescein strip treating or
close follow up and cobalt blue
Antibiotics eye drop, ointment,
Medical eye managing simple To recognize when
penlight oral/injection
Additional hours there is a serious Chloramphenicol eye drop and Community care (by cases Magnifier to PEC infection. ointment, terramycin ointment, hospital ophthalmic Mismanagement Smear refresher To give first aid polymycinB+gramicidine+neom
medical officer) of the serious and refer to the
± ycin eyedrop
course cases Culture/Sensitivity Don't know how
higher levels after test for bacteria
Proparacaine eyedrop
to follow up adequate
management
• Under Identify causative 1. Antibacterial drug: full utilization of agent. Adequate
Slitlamp range
Special training Specialized eye laboratory management for 2. Antifungal drugs:
Provincial care by facilities preventing serious
Smear AmphotericinB,
course on hospital Culture /Sensitivity ocular infection
ophthalmologist · low yields of complications test for bacteria
ketoconazole (one week?)
culture/ Therapeutic 3. Microscope sensitivity test keratoplasty
Under utilization
of laboratory Identify causative 1 0 Antibacterial drug: full
facilities
Low yields of agent. Adequate Slitlamp range Keratoplasty
Regional Specialized eye
culture/sensitivity management for Smear 2. Antifungal drugs: course
Hospital care by
test preventing serious Culture /Sensitivity AmphotericinB, Lab quality
ophthalmologist High percentage
complications test for bacteria ketoconazole, assurance for Therapeutic ±for fungus 3. Microscope lab technician
of resistant cases keratoplasty 4. Eye bank
Lack of good eye
bank support
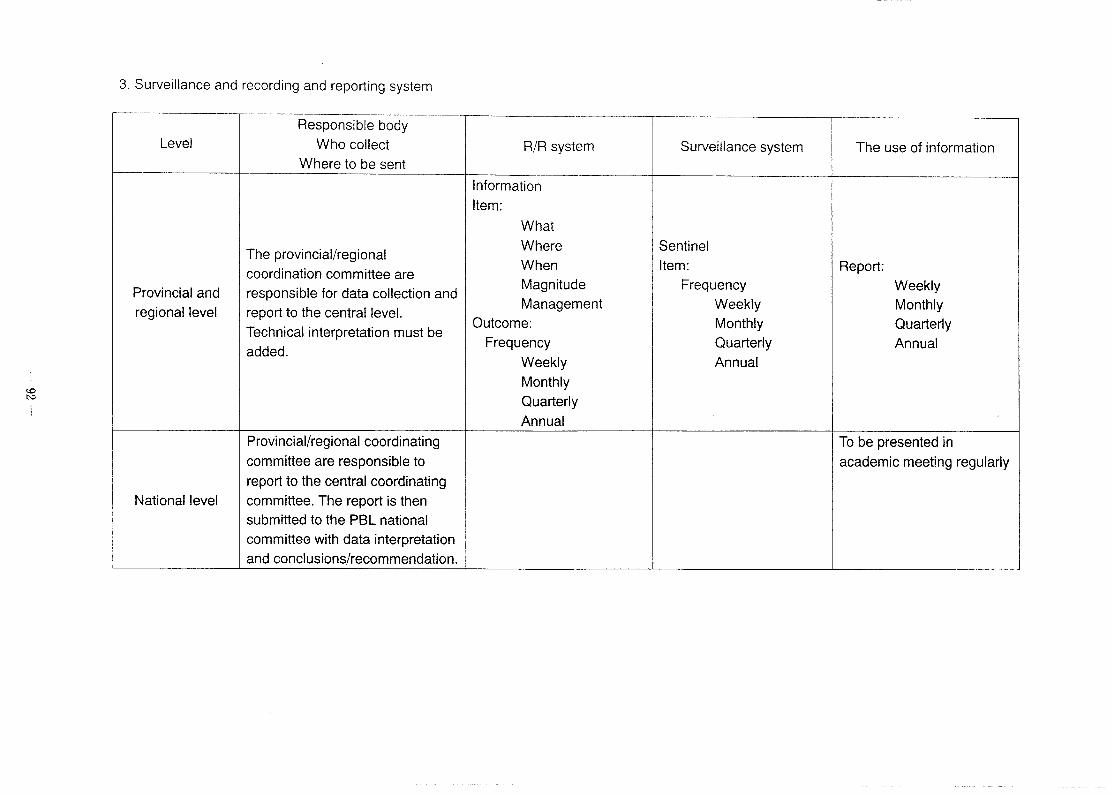
3. Surveillance and recording and reporting system
-- ··-~--- . -- -·---~-- --------------·-·-------- r---·----------------~---------··-·· -·- --Responsible body
Level Who collect R/R system Surveillance system The use of information
f---. Where to be sent
Information
Item:
What
The provincial/regional Where Sentinel
When Item: Report: coordination committee are Provincial and responsible for data collection and
Magnitude Frequency Weekly
regional level report to the central level. Management Weekly Monthly
Technical interpretation must be Outcome: Monthly Quarterly
added. Frequency Quarterly Annual
Weekly Annual
Monthly
Quarterly
Annual
Provincial/regional coordinating To be presented in committee are responsible to academic meeting regularly report to the central coordinating
National level committee. The report is then submitted to the PBL national committee with data interpretation
and conclusions/recommendation.

Group A Community level eye care network development
Quality eye care Present situation Minimum service Minimum facility Supplies, equipment Training need activity need develo_Q_ed necess~forsu~port
Self eye care Lack of eye health Eye health . Media: Poster TV Poster Training for knowledge education by Radio, school . Leaflets health volunteer . Self treatment appropriate media: lesson . Speaker, amplifier . Not awareness TV, radio, poster concern serious eye condition
. Supplies of . Seasonal Protection device . HC close to their goggle/Sunglasses agriculture injury home . Delayed Increased PEC presentation for capacity treatment
. Bicycle, . Motorcycle . Unable help oneself Home visit by PHC . Information (elderly or disabled /PEC system and call people) center
1st level of referral . Limitation of eye . Increased PEC . Essential drug: antibiotic Training PEC or health center care knowledge PHC
PEC .Health education . Education manual . Lack of for PEC and hand book drug/equipment . Poor transportation of referring Limit accessibility

Group B: Second and tertiary level of referral
Level of Eye Facility of Eye Care Present Minimum Service Minimum Facility Supplied and Training Needed Facility Situation Activity Needed Developed Equipment
necessary for support
Provincial Specialized eye care -In adequate -Proper -Smear, culture -Proper lab: -Special training Hospital (by ophthalmologists ophthalmologist. management for and sensitivity equipments, (S.L.E to eye doctors, (Secondary level) and basic eye doctor) -No Lab. severe ocular test. and Microscope, nurses, and
-In adequate infection cases chemical) technicians. drugs and -Should able to -Adequate instruments. identify the antibacterial, anti-
organism. fungal, antiviral drugs.
Regional Specialized eye care -In adequate -Same as above+ -Same as above+ -Equipments for -Special training Hospitai/Ophthal (by ophthalmologists) ophthalmologist PKP -Eye bank eye bank to mology Center s -Can identify the ophthalmologists
-No proper lab. causative and eye bank organism. staff for P.K.P.
-Pathologists. -Microbiologists.

Group C : Eye Care Network Ophthalmology Centre The Matrix on Ocular Infection Management
Supplied and Level of eye Quality of eye
Present situation Minimum service Minimum facility equipment Training need facility care Activity needed developed necessary for
support -No micro. lab - Identify - Smear Test - Micro lab - Special
causative equipment training of agent - Sensitive test and supplies. Microbiology.
- No eye bank, - Inadequate - Adequate - Immunology - Eye bank
equipment for management /serological test facilities, - - Eye bank eye bank for preventing Instrument management.
serious - Establishment and - limited anti complication. of eye bank equipment of - Special
fungus I viral PKP. training on drugs - Information - Eye drops (anti surveillance
Data bank fungal , viral) - Government - information special Center for
Ophthalmology Sub Specialized system - Doing some provision. drug supplies.
Center eye care (by inadequate researches.
ophthalmologists) - Standardized - Infrastructure - No regulation - therapeutic information for tertiary
of drug keratoplasty I system and training control PRK. surveillance Center
system. - No law on
tissue - Proposal to - Special donation. government to training
issue regulation like PKP. No sub specialty of drug control unit-cornea.
-· ---- ------·-

cataract program
Cataract
Situation of cataract and intervention in Cambodia
National subcommittee for PBL
Situation of Cataract
1992 1995.
output/year 500
Cataract
surg1cal rate 50 110 350 I 550 1 600 . 670 ------- -'---------------j-------4---- --j----
i i IOL 0 6.2% 59% !79.7%/83.9% I 85%
Situation of Cataract
• Current cataract program - Eye care seNice - outreach seNice
• Applied standard procedure - ECCE and ECCE with IOL
-96-
Situation of Cataract
+Cambodia population: 11.7 M + Blindness prevalence: 1.2% +Blinding cataract : 65% main cause of
blindness +Cataract backlog : 80,000 +Annual incidence : 19,500
Cataract output from 1992 to 2001
8000
7000 735
6000
5000
4000 3500
3000
2000
1000
0 1992 1995 1998 1999 2000 2001
Situation of Cataract
+Constraints - Limited network
- Lack of equipment and fund - Patient : fear of surgery, can not afford
operation, transportation - Lack of staff motivation

Situation of Cataract
What will we do for next step? * Increase output I year: 10000 to 15000 by year 2005
*To achieve this target by: - Increase manpower
-Increase PEC network
- Maximum utilization the remaining resources -Increase outreach activity
- Seek fund from donor
-Education
Quality assessment of cataract service
+Apply procedure: - ECCE + IOL : 85% -No phaco
* Complication rate : 5%
-97-
Quality assessment of cataract service
Assessment at regional hospital at Takeo eye hospital:
- VA pre operation < 3/60 - 5 day after operation
VA post operation: . 6/18 to 6/6: 20% . 6/60 to 6/18: 55% . 3/60to 6/60 ; 20% . < 3/60: 5%
Quality assessment of cataract service
Patient satification: 95%:
. 53% recommend for other to operate
. 65% could perform activity

Quality assessment of cataract service in Lao PDR
Background: The major of blindness in Lao P.D.R. is cataract which represents a massive public health and socioeconomic problem in developing countries. Cataract is by far the most common cause of blindness and visual impairment among people all over the world including Lao P.D.R. Delivery of cataract surgery is often difficult because of shortage of manpower and other facilities including poor utilization of existing services. This situation has led to the accumulation of un operated case of cataract in Lao P.D.R.
During 1996CE1999, the cataract intervention program was implemented in 7 selected provinces in Lao P.D.R. Total of cataract operated were nearly 7,000 cases. The evaluation of cataract intervention program was required to assess the surgical results and quality of life outcome in cataract operated in first phase which was conducted in seven provinces: Savannakhet, Champassack, Louangprabang, Vientiane prefecture, Vientiane, Khammouane, Xaiyaboury.
Purpose: To evaluation the surgical results and quality of life outcome in cataract operated who were performed in cataract intervention program during 1996CE1999.
Sample population: The patients who had been performed cataract operated during 1996CE1999 And lived in Savannakhet, Champassack, Louangprabang, Vientiane prefecture, Vientiane, Khammouane, Xayyaboury provinces. It was nearly 7,000 cases. Sample size requirements were based on estimating prevalence of complications of cataract surgery. The total of required sample size was 490' cases in 7 provinces.
Method: A cross sectional population based study was performed in Savannakhet, Champasack, Louangprabang, Vientiane prefecture, Vientiane, Khammouane, Xayyaboury. Visual acuity and eye examination including retinoscopy were performed in a cluster sample of these provinces. The survey was preceded by a pilot study in which operational methods
-98-
were refinded and assurance measures were performed. The preCEoperation of readiness of 17 Lao ophthalmic nurses involved in this program was started at ophthalmological center Vientiane during 24CE27 April 2000. They were properly trained in health interview principle in community, principle of refractive errors and subjective method including usage of autoCErefractometer. The training course was organized and evaluated by 4 Thai ophthalmic nurses.
The survey field work was conducted by three team during 27 April CE 5 May 2000. Each team consisted of Local ophthalmologist, ophthalmic nurses, health staff and Thai ophthalmic nurse who was responsible as a supervisor. All of three teams visited the villages to identify cataract operated cases.Visual acuity screening, qualityCE ofCE life (QOL) interviewing and eye examination took place at the village examination sites in three provinces: Savannakhet, Champasack and Louanprabang. A basic eye examination was performed by local ophthalmologist and the Lao ophthalmic nurse, who was a interview, was responsible for post operative refractive status measured by autorefractometer and qualityCE ofCE live ( QOL) interviewing. For 4 provinces we started survey evaluation on December 2000 CE February 2001. The Lao ophthalmologist and ophthalmic nurses took survey this time. We took the same method in each province.
Result The total examined population who were perfomed in Savannakhet, Champasack, Louangprabang, Vientiane prefrecture, Vientiane, Khammouane, Xayyaboury during 1 996CE 1 999.
-99-

Table 1 Number of cataract operated who were performed d . 1 996 1999 b unng - 1y area
Province Target population Examined population (%)
Savannakhet 70 70 (1 00.00) Champasak 70 58 ( 82.85)
I Louangprabang 70 70 (1 00.00) Xayyaboury 70 68 (97.14) Vientiane Prefecture 70 69 ( 98.57) Vientiane 70 70 (1 00.00) Khammouane 70 70 (1 00.00)
Total 490 475 ( 96.93)
Table 2 Analysis of visual acuity postCEop cataract peration in 7 provinces on 1996 .. (E 1999
[ Vision grad Pre-operative I (N=475) ~-------
6/6CE6/18= Good vision <6/18CE6/60= Borderline <6/60CE3/60= Poor <3/60CENOPL= Poor
Total=
# Success Rate = >90%
475 475
Post -operative (N=475) (%) 205 43.15 234 49.26
10 2.10 26 5.47
475 100
Table 3 Complication of cataract surgery in the operated eye following cataract surgery at 3CEyears followCEup in community based studies in 7 provinces:
1 Complication of cataract I surgery f After cataract ! Retinal detachment i • [ Vitreous loss LQther I Total:
Number
32 6
13 15 66
-100-
Percentage
6.73 1.26 2.73 3.15
13.87

Recommendation: The preparation of readiness for local team who was
responsible in Savannakhet, Champasack, Louangprabang, Vientiane prefecture, Vientiane, Khammouane, Xayyaboury should be more trained especially in refractive errors measuring by subjective method. Because of time imited in schedule training. Some part of the interview format weren ut clear and difficult to fill out. It took time approximately 45 minute per case for quality of life interviewing. Most of problem occurred during survey field work were lacked of planning between central team and local teams and affected to the effective of the evaluation of the cataract intervention program. Some of local team should be informed in advance about the details of the program to prepair the readiness to work together. The rainy season, most of local people work in their field and it was difficult to fine the target population.
-101-
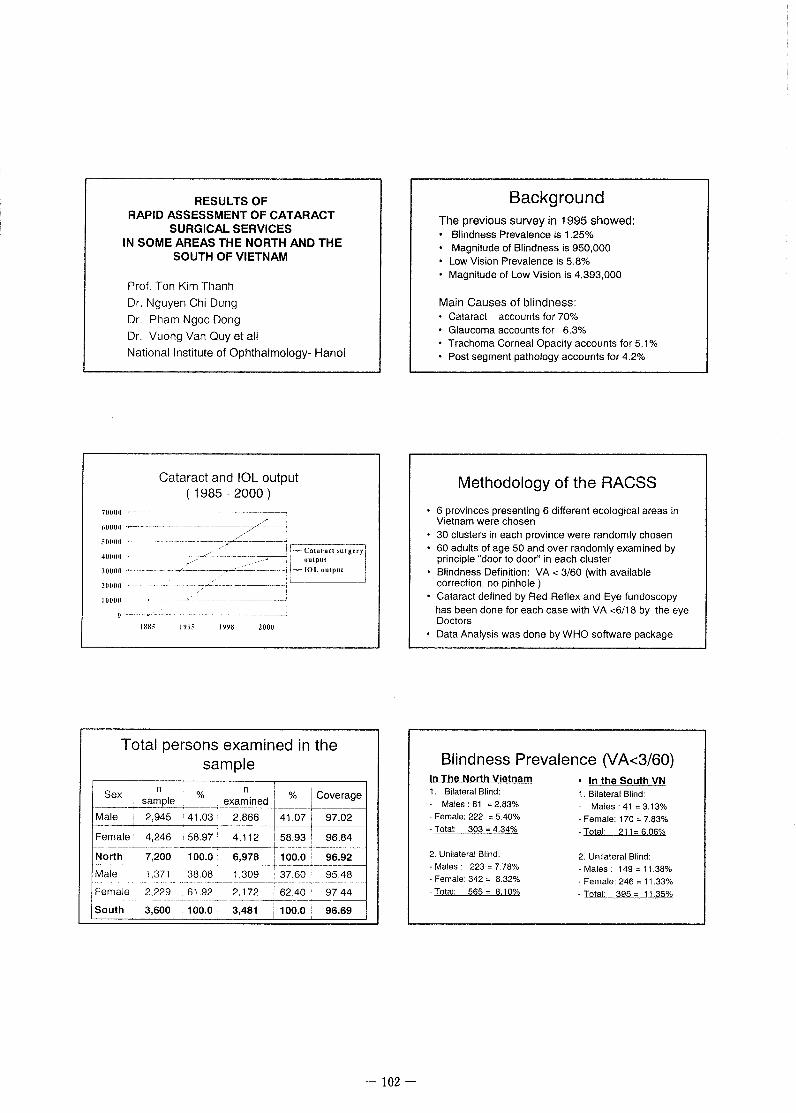
700011
40000
.100110
20000
RESULTS OF RAPID ASSESSMENT OF CATARACT
SURGICAL SERVICES IN SOME AREAS THE NORTH AND THE
SOUTH OF VIETNAM
Prof. Ton Kim Thanh
Dr. Nguyen Chi Dung
Dr. Pham Ngoc Dong
Dr. Vuong Van Quy et all
National Institute of Ophthalmology- Hanoi
Cataract and IOL output ( 1985 - 2000 )
2000
Total persons examined in the sample
n n ' % Jcoverage Sex sample
% examined 1
~----+ _,
Male ! 2,945 . 41.03 i 2,866 41.07J 97.02
Female· 4,246 ' 58.97 I 4,112 58.93 I 96.84 1-·· ----'~------·--
.. 10o.o~- 6,978 ·11oo-:ot" 96.92 North 7,200 ---···-··· ...... ·--·-······----+~·--·----l---------·----
Male 1,371 38.08 1,309 I 37.60 95.48
Female 2,229 61.92 2,172 62.40 . 97.44 ····- -·--···--- -- --~----
South 3,600 100.0 3,481 100.0 : 96.69
-102-
Background The previous survey in 1995 showed: • Blindness Prevalence is 1.25% • Magnitude of Blindness is 950,000 • Low Vision Prevalence is 5.8% • Magnitude of Low Vision is 4,393,000
Main Causes of blindness: Cataract accounts for 70% Glaucoma accounts for 6.3%
• Trachoma Corneal Opacity accounts for 5.1% • Post segment pathology accounts for 4.2%
Methodology of the RACSS
• 6 provinces presenting 6 different ecological areas in Vietnam were chosen 30 clusters in each province were randomly chosen 60 adults of age 50 and over randomly examined by principle "door to door" in each cluster Blindness Definition: VA< 3/60 (with available correction, no pinhole ) Cataract defined by Red Reflex and Eye fundoscopy has been done for each case with VA <6/18 by the eye Doctors
• Data Analysis was done by WHO software package
Blindness Prevalence (VA<3/60) In The North Vietnam 1. Bilateral Blind:
- Males: 81 = 2.83%
• Female: 222 = 5.40%
. Total: 303 - 4.34%
2. Unilateral Blind:
. Males· 223 = 7.78%
. Female: 342 = 8.32%
-Total: 565- 8.10%
In the South VN 1. Bilateral Blind:
- Males: 41 = 3.13%
· Female: 170 = 7.83%
. Total: 211 = 6.06%
2. Unilateral Blind: - Males · 149 = 11.38%
. Female: 246 = 11.33%
. Total: 395 = 11.35%

Main causes of Blindness (persons)
The North of VN 1. Cataract = 66.0%
2.Post Segment = 13.9% 3.Giaucoma = 5.3% 4.Trachoma C.O.= 4.6% 5. Corneal opac. = 2.3% 6.Uncorr aphakia= 2.6% ?.Surgical campi= 2.0% 8. Other = 3.3%
• The South of VN 1. Cataract = 75.4 %
2.Post Segment = 9.0% 3.Giaucoma = 7.1 % 4.Trachoma C.O.= 0.0% 5. Corneal opac. = 2.4% 6. Uncorr aphakia = 1 .4 % ?.Surgical campi= 1.9% 8. Other = 2.8%
Main Causes of Low Vision
The North of VN 1. Cataract = 63.0% 2.Refractive err.= 15.8%
3. Post Segment = 9.6 % 4. Glaucoma = 2.4% 5.Trachoma CO= 2.1% 6. Corneal Op. = 2.0% 7. Uncorr aphakia = 1 . 7% 8.Surgical campi= 1.3%
9. Other = 2.1 o/o
• The South of VN 1. Cataract =71.5%
2.Refractive err.= 13.0% 3. Post Segment = 6.9% 4. Glaucoma = 2.4% 5.Uncorr aphakia= 1.8%
6.Surgical campi = 1. 7% 7. Trachoma CO = 0. 0%
8. Corneal Op. = 0. 9% 9. Other = 1. 8%
COMPARISON OF THE C.S.C. IN THE SOUTH & NORTH
C.S.C. C.S.C. (PERSONS) (EYES)
-103-
Low Vision Prevalence (VA<6/18) * In The North Vietnam
1. Bilateral Low Vision : Males: = 14.38% Female: = 21.98 %
Total: - 18.86%
2. Unilateral Low Vision Males:
Female: Total:
= 14.55% = 14.18% - 14.33%
In the South VN 1. Bilateral Low Vision:
Males: = 21.39% Female: = 31.63%
Total: = 27.78%
2. Unilateral Low Vision Males : = 18.26 %
Female: = 14.92 % Total: = 16.17%
Cataract Surgical Coverage
In The North VIetnam 1.C.S.C. (per eyes):
Males = 36 .5 % - Female = 28 .9 %
Total- 31 .1%
2. C.S.C.(persons) Males = 55 .2 %
Female= 41 .8% Total = 45 .5 %
In the South VN 1 C. S.C. (per eyes):
Males = 42 .0% Female = 33 .6 % Total= 35 .7%
2. C.S.C.(persons)
Males = 67 .7% Female= 51 .5%
Total= 55_.1%
Types of Cataract Surgery
I North South Vietnam Types I
% % %
Non IOL 51.4 64.9 58.16
Surgery 1--------·
IOL
Surgery 48.6 35.1 41.84
Couching i 0.0 0.0 0.0

Post-operative V.A.of the operated eyes with available correction or pinhole
V.A. North South I Vietnam
Non IOL Non IOL , IOL s IOLs s : Both
s eyes . eyes ,
:~~1~ -;:~~~---7~-.~~: 3:~~+-;~~~~-r~~~ %-
Poor 1 ,_ I
62.0% 10.9% i 41.4% 13.3% 33.6% < 6/60
Major Causes of Poor Visual outcome (V.A.< 6 /60)
Causes
Uncorrected
Ap~~kia
North South ' Total % % %
29.3 29.4 29.37 ~-. ····~- ··-·~--- - -r-~-------------~~-;--------~~---
Surgery ; 28 3 Complications ' · 32.4 30.00
·-·--·--------·-·-~----+------+--Concurrent
causes of BL 42.4 38.2 40.62
Reasons for not Using Glasses after Cataract surgery
North South Vietnam Causes
% % % : Glasses never
26. 7 22.2 24.9 provided -·-- . -- ·----·-··--·---------~--------------r-------
Glasses Lost 2.0 4.2 2.9 and Damaged : -- ---
; No need (IOL
68.3 l
69.4 68.8 implanted) !
-104-
Post-operative V.A.of the operated eyes
I -It!------' jo Good I 1!+---------i [.9 POQ.L]
VIETNAM
Use of Spectacles after Cataract surgery
North South i Vietnam Causes
% % % i i
Using glasses ! !
30.8 : 51.4 41.15
Not using 69.2 48.6 58.85
glasses
Total 100.0 100.0 100.0
Place of Cataract Surgery !
I Vietnam North I South Places
% i
% : % I I ---
I
Community I 10.3 I 1.4 I 5.8 Health Centre : I i
--
Govt. Hospitals I I
I 88.4 : 92.6 90.5
Private Practice 1.4 : 6. 1 !
3.7 i
Traditional ! 0.0 I 0.0 I 0.0

Costs of Cataract surgery Provided
Costs North / South ! Vietnam % % %
Totally Free 21.2 17.6 19.4 ---
' Partially Free 33.6 12.2 22.8
--· -·-···-·· ·-· ---·------------··· --·---· ------------
Fully Paid 45.2 70.3 57.8
Barriers to Cataract surgery
Barriers i North South (continues) ; %
; %
Contra-indication :
6.3 i
9.3
Fear of operations & 4.6 7.5
l~()~i':JfJ __ SJfJI!! ___ ___, ____ ·----~---~---r-- -------------~-~
Wait for maturity 2.2 L 0.4 --------
No services, no 2.1 0.7 information : I
Conclusion Blindness Prevalence in the adults of age 50 and over in Vietnam today is 4. 91% Cataract is still most important cause of Blindness
in Vietnam today, it accounts for 66 -75% of all blind C.S.C.per eyes is about 31-35% and per persons is 45-55% in Vietnam today
• 51.9% of cataract surgery had a good Vision outcome, but 33.6% still had a poor Vision outcome due to many reasons: concurrent blindness, complications, uncorrected aphakia
-105-
Barriers to Cataract surgery
Barriers North South
% % ·- .
Unaware 36.7 34.9 --~---~-------------· ---
Can not afford 20.0 24.6
Old age: no need 19.2 11.0
No company 6.3 10.3
Barriers to cataract surgery
No service
Conclusion (continues) • Mainly cataract surgeries ( 90. 5%) done in the Govt.
Hospitals, about 42.2% of them is totally or partially free of charge Main Barriers to Cataract surgery are unawareness of curable blinding cataract and not affording of surgery, so that promotion of multi-channel Health education and Mobilization of all social resources should take more important role.
• Within VISION 2020, emphasis need to be placed on solving cataract blindness, increasing access to cataract surgery and improving visual outcomes of cataract surgical service in Vietnam!

Proposed solutions
Promoting social mobilization of all resources for easier access of the poor to cataract surgery . Improving health education through many channels in the community.
Strengthening the existing PEC network.
Improving surgical quality through the development of surgical skills of eye surgeons and equipment.
Developing International and Inter-country cooperation in the BLP Programme.
-106-
We sincerely thank
WHO and Dr. S. Resnikoff for their kindest financial and technical supports to carry out this RACSS in Vietnam All other NGO's for their valuable assistances in our Blindness Prevention Programme for many years.
Sight First Committee and Dr. K. Konyama for the opportunity to attend this workshop.
Thank You for attention!

No. of Cataract Surgeries performed in Myanmar, 2001 Trachoma Control and Prevention of Blindness Programme Department of Health, Ministry of Health, Union of Myanmar
I No. of Surgeries IOL% I I Prevention of Blindness programme I
I (12 team) 9,069 60%
I I Hospitals c -· Yangon Eye Hospital 4,094 90% I
I States and Divisional 4,780 40% I Hospital (24 eye units) I
~ '
I Private Eye Centres 15,000 80% [ I I
! (Yangon and Mandalay) I I I I
r-~--~
32,943 67o/o I 1 Total
-107-

Quality assessment of cataract service
Cataract services in Thailand is managed mainly by governmental eye care facilities. We have about 114 health care facilities allocated in every provinces and big cities, every which has an eye clinic as shown in the table. This figures do not included private sectors.
E f ·rt . Th "I d ~ye care ac1 1 ry 1n a1an . . Health care facility urban rural total
MOPH 9 94 102
MILITARY 3 + 3+
UNIVERSITY 8+ - 8+
Ministry of interior 1 - 1+
Private some some total 114+
E ~ye care personne In
By the year 2001 number governmental service( data
from 88 of 114) Ophthalmologists 625 256
Eye nurses 307 302
Beside eye care facilities and eye care personnel, there is another important thing that contributes to the success of eye care service is net working and referring system. As many of you have known that primary health care has rooted in Thailand for more than twenty years ago and we have already integrated primary eye care in the system.
Health care structure in each provinces are drafted as follow:
-108-

Provincial hospitals, about 93 with eye clinics (and I or regional hospital)
~ 820 community hospitals in every district
(take care by general physicians who have basic knowledge of eye diseases)
~
7,800 health centers in every tambon (run by health personnel)
~
11 ,000 village health centers (located in every villages and run by village health volunteers)
To day this system is strengthen by the last constitution that determine village health centers have to be supported yearly by tax that come through local administrative body at the level of tambon. This highly facilitate the continuous development. This budget can be used in three ways; first for emergency health problems, second continuous human resources development and third for development of village health centers.
These village health centers and village health volunteers are the grass roots of primary health care (together with primary eye care) and the strength of referring system.
These are the prime sites of cases finding. Cataract cases are referred to be operated in eye clinics and the cost of operation is covered by 30 baht scheme of the government policy. Every Thai people should have the basic health insurance by this way.
-109-

Quality assessment of cataract service
Indicators : 1.Assess of referring system, effectiveness= number of patients under go surgery I number of patients registered or referred.
2. Time of waiting list for surgery.
3.Quantitative assess of cataract surgery out come ; cataract surgical rate , cataract surgical coverage Surgical rate (year 2000) 75991/60 million = 1266 I million Surgical coverage 75991 /backlog* 100% (number of backlog in the year 1996 = 180,000 ) = 42%
T bl 2 E a e :ye surg1ca t t . Th "I d ou tpu 1n a1an Surgery 1998 1999 2000
(95 from 115)
Cataract 71,354 71,051 75,991
Glaucoma 3,993 3,993 4,136
Vitreoretina 5,571 5,571 3,581
Stabismus 1,376 1,376 1,347
Keratoplasty 292 292 542
Surgical rate: quantitative assets of out put I year= member of cataract operation performed (eyes) or number of patients having a cataract operation( persons )/ 1 ,000,000 inhabitants
Cataract surgical coverage is number of persons or eyes that have received surgery I total number of persons or eyes of estimate backlog in a certain area at a certain period in term of proportion.
-110-

4.Qualitative assess of cataract service; sight restoration rate,surgical success rate.
Sight restoration rate is proportion of cataract operation done in a population over a certain period of time that change a blind person to a sighted person ;
Success rate ; the proportion of cataract operations done in a population over a certain period of time that change a blind eye into a sighted eye.
By this time I have only figure from Udornthani hospital :
Quality of visual out come of cataract surgery I
Report of cataract surgery in Udonthani hospital in the year 2001
Age range (year) Males Females
0-4 0 0
5'-14 9 4
15-29 17 4
30-44 37 19
45-59 139 178
60-69 228 299
70-79 172 191
Over 80 29 25
TOTAL 631 720
1351
- lll-

Cataract grading of male patients undergone surgery . Ud th . h "t I . 2001 tn on an• osp1 a 1n
Blinding Cataract GRADE no. of blinding no. of
Male Grade1 Grade2 3 Grade4 patients eyes
0-4 0 0 0 0 0 0
5 1-14 0 1 2 5 1 1
15-29 1 1 5 11 0 0
130-:44_-l 9 3 8 17 6 6
145-59 '
1 1 9 42 77 10 10
60-69 7 10 58 143 30 37
70-79 12 10 60 90 20 24
Over80 3 2 5 19 6 6
~otal 43 36 180 362 ' ~------~
Blinding Cataract f I no. of blinding no. Of IFemalesl Grade1 Grade2 Grade3 Grade4 patients eyes
lo-4- I o 0 0 0 0 0 r-----r- --
15 1-14 I 1 0 1 2 0 0
rs-29 1 o 0 0 4 0 0 I I -
130-44 l 2 3 4 10 0 0
~5-59 I 13 15 56 94 27 31 I
/60-69 ~ 18 19 83 173 44 54
/70-79 I 14 12 64 99 41 53 I
i 10ver 80 0 1 7 17 5 5
~a tal 48 50 215 399
Total blind people by cataract grade 4 117 + 73 = 190
-112-

p t OS f opera 1on v1sua "t · brnding patients aCUIty In I Grading number
Gr1 113
Gr2 54
Gr3 27
Gr4
Gr5
total 227
sight restoration rate ( 73 + 117 ) - ( 32 + 1 ) I 1351 = 12 %
surgical success rate( 362 + 399 ) - ( 59 =41 )11351 * % = 761-1 oo = (661 I 1351 ) * % = 50%
p t f "t OS opera IOn VISUa aCUIty Grading Males Females Total percent
Gr1 403 447 850 62.92%
Gr2 86 135 221 16.36%
Gr3 83 97 180 13.32°/o
7.40%
total 631 720 1351 100.00%
-113-

C t t t t . Th "I d 2001 a arac ou pu 1n a1an Hospital Yea[ 2001
Regional & provincial hospitals 55,768
(Data 76 of 93)
Hospitals in Bangkok 6430
(data from 8 of 12)
University hospital 5614
I (data from 4 of 8)
Total 67812
Eye surgery out put in Thailand (data 87 of 114 eye care facilities)
I Type of surgery Year 2001 Cataract with IOL I
Cataract 67,812 66460= 98%
Glaucoma 2,283
Vitreoretinal surgery 2,131
/ Strabismus 848 I
1 Keratoplasty 161
Oculoplasty No data
1
Trauma No data
Laser treatment in Thailand Hospital Year 2001 Year2002
University hospitals 3,180
Regional & 20,518
i provincial hospitals
j Bangkok hospital 5,178
- 114-

The Fourth Day 07/02/2002 Thursday
NGO session Moderator: Mr. Peter Renew (CBM)
Each NGO working in the sub-region presents own ongoing activities in the subregion.
1. Seva foundation Ms. Dechen Tsering; Program director, Seva Foundation
2. Orbis Dr. Richard Millar; Regional consultant, Orbis
3. Iris Dr. Bal Kumar K.C.; Iris, Cambodia
4. CBM Mr. Peter Renew; Regional representative, CBM
Discussion in country-groups, and in one or two NGO groups. In order to foster good understanding about the realities of programme implementation and output, between NGOs and National programmes, they had group discussions.
-115-

Conclusions and recommendations on ocular infection in Cambodia
The Cambodia National Subcommittee for Prevention of blindness:
Conclusions: Prevention blindness in Cambodia have set up the top priority for new strategies
for the vision 2020 on the manpower development and diseases control program. Ocular infection is main cause of blindness, that we could preventable and
avoidable, So our priority is focus on community level of eye care system development.
Recommendations: 1. Community level :
The ocular infection is the main problem for ocular blindness that we could avoid by prevention .So we need:
Train volunteer health worker and PEG worker Health education Provide teaching material and transportation facility
2. Provinciallevel: Special training eye doctor, MLP and laboratory technicians on microbiology Update on ocular infection treatment and surgical skill PKP Need laboratory equipment for smear, culture and sensitive test Need eye drug supplies as: anti fungus, anti viral Develop monitoring and supervision system Surveillance and information system should develop Heath education program
3. National and regional level Special training of microbiology Heath education and eye care management for student Establishment of eye bank facilities and eye bank management Special training on surveillance system for all eye care professionals Continuing to Upgrade knowledge for ophthalmologist Establishment of Subspecialty training Doing scientifically Research Need microbiology lab equipment and supplies Need eye bank facility and instruments
-116-

Conclusions and recommendations for Laos in management of ocular infection (lao PDR)
Primary level eye care service • Health education for individual and families are very important, should
be done through repetitive health education to community, school students, health school (poster)
• Sanitation and water supply • Training volunteer for community eye. • Provide essential drug for CEHWs to give the first aid and safe the eye. • Every staff at the health center should be trained in PEC and they
should know how to integrated into PHC.
Secondary level eye care service • Continue health education to public, community etc ... • Training of staff of health center. • Special training course of ocular infection. • Provide essential drug in some anti fungal drug for District hospital. • Immediate referral ocular infection in severest cases to tertiary level. • Surveillance, recording and reporting system with a responsible body at
the provincial level should be set up to collect data, analyse and distribute to the eye care management team both at the local and central level.
Tertiary level of eye care • Setting up laboratory facility. • Training for sub special cornea clinic • Provide anti fungal and anti bacterial drug for provincial and regional
hospital. • Health education
-117-
Workshop Recommendations and Conclusions of Vietnamese delegation
1. Ocular infection. Especially keratitis and uveitis are common eye problem in Vietnam. It
may lead to serious consequences such as corneal blindness and destruction of the eyeball. It needs urgent action to develop an adequate system of comprehensive eye care covering all levels of eye care network. Its management needs updated knowledge and technology not only in ophthalmology but also in microbiology, immunology and pharmacology. The laboratory facilities at the secondary level and tertiary level must be upgraded to cope with wide spectrum of causing agents. Its management also needs some special training on eye bank management and technology of penetrating keratoplasty (PKP) and supply necessary instrumentation for this purpose. Besides that, prevention of ocular infections and their blinding complications plays a very important role. It is necessary to strengthen and develop more PEC network to meet this goal. Eye care information system also must be revised to include new items of ocular infections. At the same time, the proposal to Ministry of Health and government for eye drug control and tissue donation law should be prepared and submitted. Availability of minimum sets of anti-microbiological drug must be assured after the reviewing the current situation.
2. Cataract program. The national effort must still be made so that the output can meet the
annual requirement. At the same time the cataract surgical outcome should be standardized and improved, for this purpose training of eye surgeons and upgrading cataract instrument and technology should be maintained and developed Program sustainability is an issue on which cost recovering should be paid more attention. Social mobilization of all resources and international cooperation play a very important role to improving the access of the poor to the cataract surgical service.
3. Refraction system development. As discussed in the Hanoi workshop, refraction service should be
emphasized in new situation. Refraction service must be established in tertiary and secondary levels. Training on refraction should be promoted, but it is very necessary to have technical and financial assistance from WHO and Tokyo collaborating Center for PBL and others NGOs.
*Conclusion: To achieve the goal "Vision 2020" the national effort should be
strengthen and emphasized on the main causes of blindness, including cataract, refractive error and ocular infections. The continuing support from WHO, NGOs and inter-country collaboration for the progress of the national program are very important and should be maintained and developed.
-118-

Ocular Infection in Myanmar Conclusions and recommendations
I. Weakness. 1. Lack of health education in the community. 2. Mismanagement of eye infection. 3. Lack of medicine (eg. Anti bacterial, antifungal, and antiviral drugs). 4. Lack of laboratory facilities. 5. Late arrival to the health centers. 6. Indiscriminate use of steroids by the patients.
II. What needs? 1. Community level
• Health education to the public and PEC workers, village elders, teachers, red cross volunteers, etc ...
• Training of PEC workers. 2. District level
• Training of health assistants, field workers and dressers. • Need laboratory tests for identification of organisms • Need adequate drug supply. • Monitoring supervision and referral. • Surveillance by district PBL Ophthalmologist and its team should
be done effectively and regularly. 3. Tertiary level.
• Upgrading of eye bank facilities and eye bank management. • Need pathologist, microbiologist, immunologist. • Training of ophthalmologists for PKP. • Law enforcement concerning with cornea bank act should be
implemented by Government. 4. National level.
• Research work. • Proper statistical recording and monitoring.
Conclusion "The success of eye infection"
1. Cooperation of the persons of the various levels. 2. Proper eye care and treatment including follow up treatment by
trained eye care personels. 3. C.M.E and further research works.
-119-

Conclusions and recommendations for Thailand in management of ocular infection
1. Primary prevention is the utmost importance and this should be done through repetitive health education to the public, specific target groups as well as the school students.
2. The nation's newly set up primary care units should be strengthened in primary eye care through training and refresher courses for the various levels of personnel.
3. Delegate more authority to the community hospital level in managing eye cases especially corneal infection which should go together with technology transfer and close monitoring and supervision by the provincial level.
4. Surveillance, recording and reporting system with a responsible body at the provincial level should be set up to collect data, analyse and distribute to the eye care management team both at the local and central level.
5. Upgrading laboratory facilities for scientific microbiology study at all provincial hospitals with quality audition is needed. Utilization of these facilities should be regularly reviewed and feed back.
6. Encouraging more research and development regarding ocular infection especially at the tertiary centers and university hospitals. The sociocultural behaviors factors that affect the happening of corneal infection should be clearly understood for planning of primary prevention actions.
7. Eye bank is still weak and do not adequately serve the demand. A more combined effort is needed to push and make Eye bank better functioning.
-120-

The Report of IAPB Assembly for the Sub-Region of Indochina,
The Region of the Western Pacific
Luangprabang, 8 February 2002.
Introduction
Reported by: K. Konyama, M.D., Ph.D., M.P.H.
Department of Ophthalmology Juntendo University School of Medicine
WHO Collaborating Centre for PBL Co-Chairman, lAPS Region of the Western Pacific
International Agency for Prevention of Blindness (lAPS) had a sub-regional meeting for three member countries, Cambodia, Lao PDR and Viet Nam on 8 February 2002, at Phusi Hotel, Luangprabang, and Lao PDR. The meeting was a special session in the last day of the 41
h Inter-country Workshop on Prevention of Blindness where those three countries and two observer countries, Myanmar and Thailand had participated. A group of the international NGOs, working in this sub-region attended the workshop also joined this lAPS meeting.
Dr. Nguyen Chi Dung from Institute of Ophthalmology, Hanoi, was selected to chair the meeting together with Dr. Vithoune Visonnavong, Vientiane Ophthalmic Centre the co-chairperson. Dr Dung expressed his appreciation for selecting him and apology, on absence of Dr. Ton Thi Kim Thanh. She is the co-chairperson of the IAPB/WPR, supposed to chair the meeting this meeting. Dr. Do Seiha, Cambodia and Dr. Nguyen Xuan Tinh, Viet Nam were selected as reporters.
Dr. Dung made an opening remark and conveyed the messages from Dr. Hugh Taylor, the regional chairperson and Dr. Ton Thi Kim Thanh to welcome all participants and their regret for absence this time.
-121-

Agenda for the IAPB meeting 8:30 Registration
Opening remark Introducing Chairperson and Co-chair person
Select reporters Introducing participants from three member countries and the delegates
international NGOs
Subject 1: 8: 45-9:00
Ocular Infection management
Cambodia Dr. Do Sheiha
9: 00- 9:15 Viet Nam Dr. Nguyen Xuan Tinh
9:15- 9: 30 Laos Presentation Dr. Siphetthavong Srisaleumsack
9:30- 10:00 Coffee break
Subject 2: A glance on trachoma situation 1 0: 00 - 1 0:15 Cambodia Dr. Ngy Meng
10:15- 10:30 VietNam 1 0: 30 - 1 0:45 Laos
10:45- 12:00 Discussion
Dr. Ha Huy Tai Dr. Khamkhoune Holanouphab
Ocular infections control has many significant points in blindness prevention and eye care. The session discussed on present weakness and the needs to be urgently strengthened
in each country. Firstly, corneal ulcer is a common problem to aiL Importance of early management was recognised. Action must be started at community. Secondly, in general drugs, such antibiotic preparations are in short at all levels, especially anti-fungal
preparations. Thirdly, all levels lack laboratory support and urgent need for a supporting system from the high-level. Routine investigation like, smear, culture and sensitivity tests are not yet practised in some countries. Lastly, it needs strong information system support.
All countries lack a working surveillance system. In conclusion, many countries require
urgent action upgrading scientific foundation and updated management.
Ophthalmia neonatorum is now rather prevalent in Laos. In general, in most countries no
such recording/reporting system is working in general. It therefore, resulted in the overall situation is unclear. Ocular infections must be regarded as a sort of eye injuries and emergency. Management must start at where people are living and working. The
management system must be reviewed and give more weight to prevention in the context of Primary Health Care. Attention must be also given to upgrading level of ophthalmic
sciences.
-122-

Viet Nam has shown its great efforts for long, which had led to the decline of trachoma. It resulted in school eye health no longer requires trachoma programme and replaced by such check-up refractive errors. Moreover, in the sub-region may consider a multi-institute linked study soon in the area of molecular epidemiology of chlamydia, where Chlamydia came from and where it goes? While the condition needs continuous efforts against
trachoma complications, like trichiasis correction.
12:00- 13:00 Lunch
Subject 3: Cataract situation and intervention 13:00- 13:20 Assessment of quality of cataract programme: Lectured by Dr.
Pararajasegaram 13:20 - 13:30 Cambodia 13:30 - 13:40 Vietnam 13:40- 13:50 Laos
13: 50 - 14:00 Discussion
Dr. Touk Barang Dr. Nguyen Chi Dung Dr. Siphetthavong Srisaleumsack
Dr. Pararajasegaram gave a lecture that assessing cataract surgery and its outcome. These are similar to process control in manufacturing sector. Input/output assessment
needs careful consideration of the production line. He was reminding such a concept of quality control in industrial sector should be introduced. Laos and Viet Nam gave their outcomes of cataract surgery.
Cataract services in these countries participated the meeting aim at establishing a local system to cope with the local needs occurring in individual territory. Therefore, it requires working Primary Eye Care incorporated within Primary Health Care scheme. This strategy
seemed to be well retained in three countries. Laotian programmes supported by the South Korean fund channelled by WHO/WPRO had taught local surgeons self-confidence through operation. However, it might need further external financial input for some more
time. Thus, creating a local recurrent financial system seems to be the current concern.
14:00 - 14:30 Coffee break
-123-