prevention and health promotion division compendium 2020
TRANSCRIPT

Prevention and Health Promotion Division Compendium 2020
Page 1
PREVENTION AND HEALTH PROMOTION DIVISION COMPENDIUM 2020
1/23/2020 Prevention and Health Promotion Division

Prevention and Health Promotion Division Compendium 2020
Page 2
PREVENTION AND HEALTH PROMOTION DIVISION STAFF
Carol P. Meredith, Director 860-418-6826
Statewide and Community Based Prevention Initiatives
Andrea Iger Duarte 860-418-6801
Program Manager
Dawn Grodzki 860-418-6772
Program Manager
Robin Cox 860-418-6955
Prevention Services Coordinator
Stephanie L. Moran 860-418-6880
Prevention Services Coordinator
State Tobacco Prevention and Enforcement Program
Gregory F. Carver 860-418-6702
Supervising Special Investigator
Michael Harnois 860-418-6871
Special Investigator
FDA Tobacco Prevention and Enforcement Program
Holly White 860 418-6837
Supervising Special Investigator
Bryan Champagne 860-418-6781
Lead Special Investigator
Albert Harrison 860-418-6821
Special Investigator
Daniela Montes -Hawley 860-418-6757
Special Investigator
Mario Bernardo 860-418-6888
Special Investigator

Prevention and Health Promotion Division Compendium 2020
Page 3
TABLE OF CONTENT
Prevention and Health Promotion Division 4
What is Prevention & Health Promotion?
Prevention Framework
Comprehensive Prevention & Health Promotion System
Management and Organization 7
Structure and Organization
Sub-State Organization
State Advisory Councils
Strategic Action Plan
Infrastructure and Programs 10
Introduction to Infrastructure & Programs
Statewide Resource Links and the Regional Action Councils
Connecticut Strategic Prevention Framework Coalitions Initiative
Local Prevention Councils
Connecticut Networks of Care for Suicide Prevention
State Tobacco Prevention & Enforcement Program
Food and Drug Administration Tobacco Prevention & Enforcement Program
CT Safe Schools Healthy Students (SSHS) Diffusion Project
Partnerships for Success 2015
Now is the Time – Healthy Transitions – CT STRONG
Statewide Healthy Campus Initiative
Specialized CIT for Young Adults
Courage to Speak Foundation
Needs Assessment, Planning, Resource Allocation, Data Collection 25
Needs Assessment
Resource Allocation
Data Collection
Interagency Coordination 31
Introduction to Interagency Coordination
Interagency Boards, Committees, Coalitions,
Collaboratives, Partnerships and Workgroups
Quality Assurance, Monitoring, Workforce Development 39
System Oversight and Program Reporting
Monitoring, Corrective Action and Technical Assistance
Staff Credentialing and Operating Standards
Workforce Development
Connecticut Intermediate Outcomes
Research-Based Best Practice Strategies, Practices and Programs

Prevention and Health Promotion Division Compendium 2020
Prevention and Health Promotion Division
Page 4
PREVENTION & HEALTH PROMOTION DIVISION WHAT IS PREVENTION & HEALTH PROMOTION?
PREVENTION FRAMEWORK
COMPREHENSIVE PREVENTION & HEALTH PROMOTION SYSTEM
WHAT IS PREVENTION & HEALTH PROMOTION?
Prevention means creating conditions that promote good health. It is achieved by reducing those
factors that are known to cause illness and problem behaviors and encouraging those factors that
buffer individuals and promote good health. Prevention promises a reduction in the incidence of new
cases of illness and problem behavior. When properly done, a good preventive intervention is long
lasting and focused on reducing vulnerability and enhancing wellness.
The Institute of Medicine’s Continuum of Care
A classification system that presents the scope of behavioral health services: promotion of
health, prevention of illness/disorder, treatment, and maintenance/recovery.i
Prevention and promotion are the first two steps in the substance abuse and mental health continuum
of care and promotion is encouraged across the spectrum. Interaction with the prevention system often
serves as a catalyst for individuals to seek intervention and treatment services. Prevention
practitioners are trained to identify and refer individuals with problems to appropriate intervention
and treatment services.
Prevention can help decrease hospital stays, long-term residential treatment, suicide, violence and
aggression. It provides for long-term cost savings and can create better quality of life for individuals
and safe and resilient communities.
In the field of mental health, promotion includes efforts to enhance individuals’ ability to achieve
developmentally appropriate tasks (developmental competence) and a positive sense of self-esteem,
mastery, well-being, and social inclusion and to strengthen their ability to cope with adversity.

Prevention and Health Promotion Division Compendium 2020
Prevention and Health Promotion Division
Page 5
PREVENTION FRAMEWORK
Prevention programs fall into three categories based on the Institute of Medicine’s (IOM) Spectrum of
Behavioral Health Disorders: universal, selected and indicated. Universal prevention programs focused
the general public or a whole population that has no known risk factors. Selective prevention
interventions are focused on individuals or a segment of the population whose risk for developing
substance abuse or a mental health disorder is significantly higher than average. Indicated prevention
programs focus on high-risk individuals who have started exhibiting problems. There is an array of
best practice universal, selective and indicated prevention interventions directed at individuals and
families in their schools, neighborhoods, places of worship and workplaces which have proliferated
across the country in the last twenty years. These interventions have evolved from several generations
of programs, theoretical models and approaches that address individuals across the lifespan. Over
the years, these approaches have been researched across focused populations and fields of practice,
with consideration given to developmental appropriateness, gender and sexual orientation factors.
This has resulted in new knowledge and lessons learned about the impact and effectiveness of
prevention, which has assisted developers in creating extremely promissing prevention systems.
There are several state and local agencies within Connecticut with prevention systems that use a
variety of theoretical models. The Connecticut Department of Mental Health and Addiction Services
(DMHAS) is the single state agency for mental health and substance abuse services. The DMHAS’
Prevention and Health Promotion Division is strategically aligned with the Substance Abuse Mental
Health Services Administration’s (SAMHSA) Strategic Prevention Framework (SPF). The Division’s work
is guided by the SPF five steps which comprise of conducting needs assessments, capacity building,
planning, implementing evidenced based strategies, monitoring and evaluation. The division is
organized to provide accountability-based, developmentally appropriate and culturally sensitive
behavioral health services based on best practices, through a comprehensive system that matches
services to the needs of the individuals and communities.
As depicted in the Connecticut Tree of Prevention below, this comprehensive system includes the
following areas aligned with the federal SAMHSA Center for Substance Abuse Prevention’s (CSAP)
concepts of performance management:
COMPREHENSIVE PREVENTION & HEALTH PROMOTION SYSTEM
DMHAS System SAMHSA/CSAP concepts
Management and Organization of DMHAS’
Prevention System Organizational /system performance outcomes are established
Resources are allocated based on established goals
Program Infrastructure including concepts,
strategies and activities, program functions, and
targets.
Cultural issues are approached systemically
Workforce development needs are assessed and capacity is increased
Outcomes, plans and strategies are monitored and evaluated
Planning, Needs Assessment, Resource
Allocation and Data Collection. Data informs adjustments in policy and strategy direction
Data informs decisions that improve public health quality
Coordination with Other Agencies. Data frames to report successful outcomes
Practices, resources and partnerships to sustain long term outcomes
Quality Assurance and Improvement. Budget decisions are based on results
Sub recipients are accountable for outcomes

Prevention and Health Promotion Division Compendium 2020
Prevention and Health Promotion Division
Page 6
Prevention and Health Promotion Division Compendium 2020
Management and Organization
Page 7
MANAGEMENT AND ORGANIZATION STRUCTURE AND ORGANIZATION
SUB-STATE ORGANIZATION
STATE ADVISORY COUNCILS
STRATEGIC ACTION PLAN
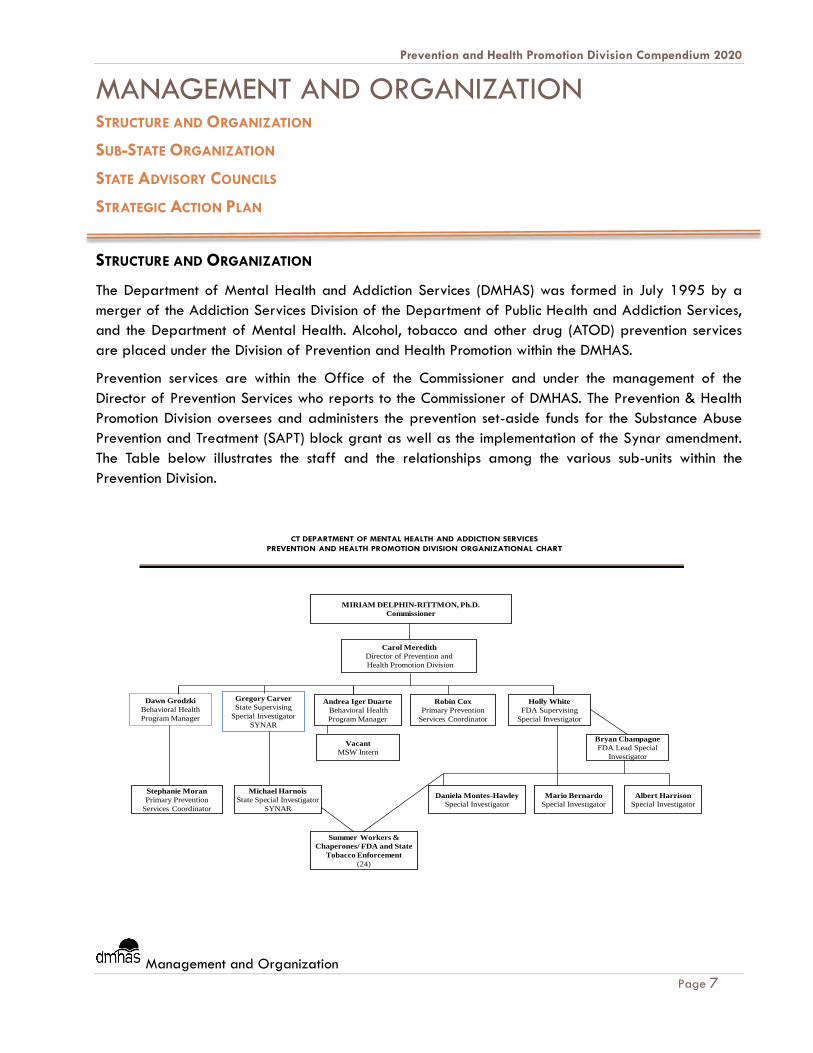
STRUCTURE AND ORGANIZATION
The Department of Mental Health and Addiction Services (DMHAS) was formed in July 1995 by a
merger of the Addiction Services Division of the Department of Public Health and Addiction Services,
and the Department of Mental Health. Alcohol, tobacco and other drug (ATOD) prevention services
are placed under the Division of Prevention and Health Promotion within the DMHAS.
Prevention services are within the Office of the Commissioner and under the management of the
Director of Prevention Services who reports to the Commissioner of DMHAS. The Prevention & Health
Promotion Division oversees and administers the prevention set-aside funds for the Substance Abuse
Prevention and Treatment (SAPT) block grant as well as the implementation of the Synar amendment.
The Table below illustrates the staff and the relationships among the various sub-units within the
Prevention Division.
CT DEPARTMENT OF MENTAL HEALTH AND ADDICTION SERVICES
PREVENTION AND HEALTH PROMOTION DIVISION ORGANIZATIONAL CHART
Summer Workers &
Chaperones/ FDA and State
Tobacco Enforcement
(24)
Carol Meredith
Director of Prevention and
Health Promotion Division
Andrea Iger Duarte
Behavioral Health
Program Manager
Robin Cox
Primary Prevention
Services Coordinator
Michael Harnois
State Special Investigator
SYNAR
Albert Harrison
Special Investigator
Gregory Carver
State Supervising
Special Investigator
SYNAR
Stephanie Moran
Primary Prevention
Services Coordinator
MIRIAM DELPHIN-RITTMON, Ph.D.
Commissioner
Holly White
FDA Supervising
Special Investigator
Bryan Champagne
FDA Lead Special
Investigator
Daniela Montes-Hawley
Special Investigator
Mario Bernardo
Special Investigator
Dawn Grodzki
Behavioral Health
Program Manager
Vacant
MSW Intern

Prevention and Health Promotion Division Compendium 2020
Management and Organization
Page 8
SUB-STATE ORGANIZATION
The Connecticut legislature has established 5 human service regions for the purpose of providing state
health and human services. DMHAS uses 13 subdivisions of these regions as the geographic basis for
prevention services. The prevention services within these regions are comprised of 6 major
components: (1) four Statewide Resource Links that support prevention programs statewide, known as
the Prevention Infrastructure; (2) Connecticut Strategic Prevention Framework Coalition Initiative
aimed at applying the 5-step Strategic Prevention Framework (SPF) to address state and local needs
in twelve communities across the state; (3) 156 Local Prevention Councils providing primary prevention
strategies; (4) Tobacco Prevention and Enforcement Initiatives aimed at reducing underage access and
use of tobacco products; (5) thirteen Regional Action Councils that build capacity of individuals and
communities to deliver prevention services; (6) the Partnerships for Success 2015 Initiative addressing
underage drinking at the state and community levels; (7) the CT Youth Suicide Prevention Initiative
comprised of seventeen high schools, four CT State Universities, a hospital, a middle school, two
training entities; a statewide awareness campaign; (8) the Safe Schools Healthy Students initiative
intended to expand and enhance improvements in school climate, access to behavioral health and
other supports, reduce substance use and exposure to violence in students Pre-K through 12th grade in
3 school districts across the state; and (9) the Now is the Time Healthy Transitions: CT STRONG
program to engage youth ages 16-25 who are at risk for behavioral disorders and connect them to
care.
STATE ADVISORY COUNCILS
The Connecticut Alcohol and Drug Policy Council (ADPC) was established by the Governor through
executive order in 1996 to address substance abuse issues within the state and to implement the
recommendations of its predecessor Blue Ribbon Task Force on Substance Abuse. The ADPC and its
Prevention, Treatment and Criminal Justice committees developed a multi-year, interagency statewide
plan for substance abuse that has been annually updated and evaluated and which provides for
policy and budgetary direction for substance abuse prevention and treatment annually.
The Connecticut Suicide Advisory Board was established January 2012 through the merger of the CT
Youth Suicide Advisory Board and the Interagency Suicide Prevention Network to create one state-
level Suicide Advisory Board to address suicide across the lifespan. The 1989 legislation requires the
existence of an advisory body to inform the Commissioner of DCF on strategies for the coordination
of youth suicide prevention throughout Connecticut. The goals are: 1) Increase public awareness of the
existence of youth suicide and means of prevention; 2) Make recommendations for statewide training
in youth suicide prevention; 3) Develop a strategic youth suicide prevention plan; 4) Recommend
interagency policies and procedures for coordination of services; 5) Implement suicide prevention
procedures in schools and communities; 6) Establish a coordinated system for data collection and
utilization; 7) Make recommendations concerning the integration of youth suicide prevention and
intervention strategies into youth prevention and intervention programs.

Prevention and Health Promotion Division Compendium 2020
Management and Organization
Page 9
Connecticut Healthy Campus Initiative- This statewide initiative, funded through the CSAP Partnership
for Success 2015 is composed of 46 member universities and colleges of higher education, and is
committed to substance abuse prevention in the focused 18 to 25 year old college student population.
The Initiative provides leadership on substance abuse prevention through engagement of senior
college administrators and implementation of evidence based policies, practices and strategies.
STRATEGIC ACTION PLAN
The Prevention & Health Promotion Division has used state policy plans and recommendations, agency
strategic plans and SAMHSA goals to guide the prevention direction. The table below identifies the
Prevention Division’s role in implementing DMHAS’ current operational plan.

Prevention and Health Promotion Division Compendium 2020
Infrastructure and Programs
Page 10
INFRASTRUCTURE AND PROGRAMS INTRODUCTION TO INFRASTRUCTURE & PROGRAMS
STATEWIDE RESOURCE LINKS AND THE REGIONAL ACTION COUNCILS
CONNECTICUT STRATEGIC PREVENTION FRAMEWORK COALITIONS INITIATIVE
LOCAL PREVENTION COUNCILS
CONNECTICUT NETWORKS OF CARE FOR SUICIDE PREVENTION
STATE TOBACCO PREVENTION & ENFORCEMENT PROGRAM
FOOD AND DRUG ADMINISTRATION TOBACCO PREVENTION & ENFORCEMENT PROGRAM
CT SAFE SCHOOLS HEALTHY STUDENTS DIFFUSION PROJECT
PARTNERSHIPS FOR SUCCESS 2015
NOW IS THE TIME – HEALTHY TRANSITIONS – CT STRONG
STATEWIDE HEALTHY CAMPUS INITIATIVE
SPECIALIZED CIT FOR YOUNG ADULTS
COURAGE TO SPEAK FOUNDATION
INTRODUCTION TO INFRASTRUCTURE & PROGRAMS
Prevention activities within DMHAS have historically been based on the public health model.
Programs have also used the empowerment model as promulgated by the SAMHSA/CSAP, and the
creation of conditions to promote general well-being as described in the research of William Lofquist
and David Hawkins. Capacity building at the community level is an important element of the state’s
prevention activities. In recent years, DMHAS has also employed environmental strategies, especially
in the area of reducing underage drinking. Prevention services have been organized to promote local
capacity building and provider agencies are directing their efforts to achieve capacity building for
communities.
Among the state agencies with prevention resources, the mission for prevention is to build a systems
approach to strengthen local capacity and to support local empowerment in meeting the needs and
implementing prevention programs. DMHAS fosters the development of comprehensive culturally
appropriate programs based on scientifically defensible principles and focuses on both individuals
and the environments within which they live. DMHAS has taken deliberate efforts to shift the
prevention paradigm in Connecticut towards the SPF. Utilizing the SPF model at both the state and
community level DMHAS has implemented a statewide data driven needs assessment process,
spearheaded by the State Epidemiological Workgroup, across the prevention continuum of care
related to substance abuse, suicide and gambling. The paradigm shift to the SPF has resulted in
strategic planning including logic model development based on needs assessment, increased capacity
to address needs identified through data analysis and identification and implementation of evidence-
based programs, strategies and policies. Evaluation of these efforts is ongoing and will result in mid-
course corrections as needed.
Prevention and Health Promotion Division Compendium 2020
Infrastructure and Programs
Page 11
DMHAS’ prevention concepts and direction are communicated to provider agencies through the
Request for Proposals process and the DMHAS prevention web-site. Prevention staffs also sponsor
learning communities and information dissemination exchanges for provider agencies.
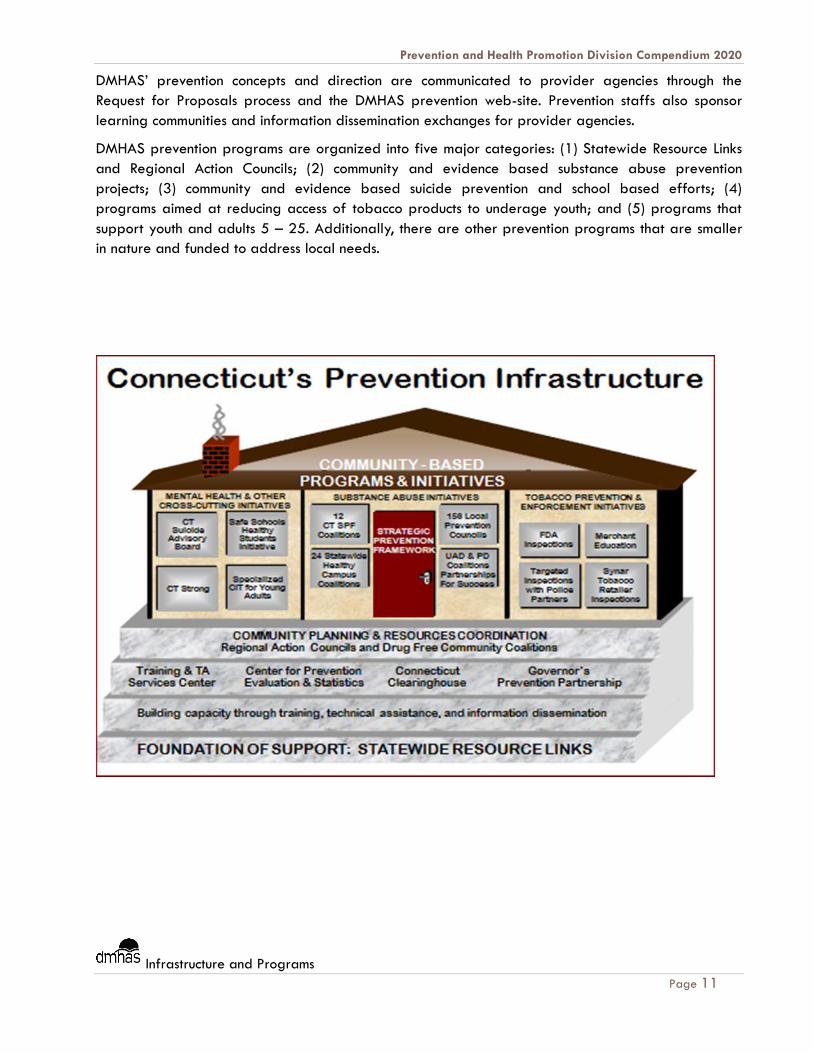
DMHAS prevention programs are organized into five major categories: (1) Statewide Resource Links
and Regional Action Councils; (2) community and evidence based substance abuse prevention
projects; (3) community and evidence based suicide prevention and school based efforts; (4)
programs aimed at reducing access of tobacco products to underage youth; and (5) programs that
support youth and adults 5 – 25. Additionally, there are other prevention programs that are smaller
in nature and funded to address local needs.

Prevention and Health Promotion Division Compendium 2020
Infrastructure and Programs
Page 12
STATEWIDE RESOURCE LINKS AND THE REGIONAL ACTION COUNCILS
Purpose:
The Statewide Resource Links (SRL) and the Regional Action Councils (RAC) are statewide and regional
entities funded by DMHAS to support prevention efforts within the state by building the capacity of
individuals and communities to deliver prevention services. Since 2006, these entities have provided
distinct services to move Connecticut’s prevention system to align with the Strategic Prevention
Framework (SPF) five steps.
Funded Programs & Services:
Connecticut Clearinghouse (SRL) – is a statewide library and resource center for information on
substance use and mental health disorders, prevention and health promotion, treatment and
recovery, wellness and other related topics.
Training and Technical Assistance Service Center (SRL) – provides training needed to obtain
and maintain certification status; provides training workshops that focus on prevention skills
development and the application of these skills, provides training on mental health promotion, and
violence and substance abuse prevention; supports to individuals looking to increase their
knowledge and skills in the prevention area.
Governor’s Prevention Partnership (SRL) – is a statewide organization comprising of
public/private partnerships designed to change the attitudes and behaviors of Connecticut youths
and adults toward substance through its School, Campus, Workplace and Media Partnerships.
Center for Prevention Evaluation and Statistics (SRL) – The CPES is responsible for designing
and implementing data collection and management; disseminating and utilizing epidemiological
data for decision-making; and providing technical assistance and training on evaluation-related
tasks and topics.
Regional Action Councils (SRL) –13 public/private sub-regional planning and action councils
that have responsibility for the planning, development and coordination of behavioral health
services in their respective region.
Focus Population(s):
Local communities, individuals, and agencies providing prevention programming; regional and
statewide service agencies; societal organizations and institutions, e.g. corporate, medical, religious
and recreational entities
Strategy Type:
The State-wide Service Delivery Agents utilizes multiple strategies to promote the health and well-
being of all Connecticut’s residents throughout their life span. They include, but are not limited to,
information & public awareness, education, community development, capacity building and
institutional change, and social policy.
Program Management Statewide Resource Links Program Management Regional Action Councils
Dawn Grodzki Andrea Iger Duarte
Program Manager Program Manager
860-418-6772 860-418-6801

Prevention and Health Promotion Division Compendium 2020
Infrastructure and Programs
Page 13
CONNECTICUT STRATEGIC PREVENTION FRAMEWORK COALITIONS (CSC) INITIATIVE
Purpose:
The CSC Initiative is a 1.2 million program funded annually through the SAMHSA Substance Abuse
Prevention and Treatment Block Grant. The initiative is comprised of 12 agencies working with
coalitions that are implementing SAMHSA five-step Strategic Prevention Framework (SPF) to address
substance abuse and promote positive mental health at the community level. The CSC Initiative
objectives are to: develop strong linkages between communities and State agencies; implement and
sustain culturally competent, evidence-based prevention services; and achieve measurable outcomes
in reducing substance abuse while also promoting positive mental health.
Focus Population(s):
The CSC Initiative agencies are implementing the SPF in the following 12 communities: Clinton,
Danbury, Darien, Fairfield, Groton, Haddam/Killingworth, Harwinton-Burlington, Lyme/Old Lyme,
Middletown, New Haven, Newtown, and Windsor Locks. Informed by their community coalition,
grantees will focus on populations identified through their Community Needs Assessments and
prioritization process.
Strategy Type:
Each community will use the SPF five-step public health model which includes needs assessment,
capacity building, strategic planning, implementation, and evaluation while incorporating cultural
competency and sustainability throughout the process. The grantees will use epidemiological data to
identify needs, and gaps for implementing evidence-based programs, policies, and practices within
their respective geographical areas.
Program Management
Robin Cox
Prevention Services Coordinator
860-418-6955
Prevention and Health Promotion Division Compendium 2020
Infrastructure and Programs
Page 14
LOCAL PREVENTION COUNCILS
Purpose:
This initiative supports 130 plus local, municipal-based Local Prevention Councils (LPCs) that facilitate
the development of culturally competent ATOD abuse prevention and joint behavioral health
promotion initiatives of Local Prevention Councils (LPCs) within communities directed at citizens across
the lifespan with the support of chief elected officials. The overall goal is to increase public
awareness of the prevention of ATOD abuse and joint behavioral health promotion in the context of
overall health and wellness. This program differs from others in that the eligible grantees are
required to demonstrate the support and involvement of the municipality’s chief elected official, i.e.,
mayor and/or first selectman. The specific goals of Local Prevention Councils (LPCs) are to increase
public awareness of ATOD prevention and joint behavioral health promotion initiatives and stimulate
the development and implementation of local prevention activities.
Funded Programs:
130 plus Local municipalities and town councils throughout the state
Target Populations:
Universal targets in selected communities in the 169 cities and towns throughout Connecticut.
Program Strategy:
LPC programs utilize at least two of the six CSAP identified prevention strategies (information
dissemination, education, community-based processes, alternative programming, environmental, and
program identification and referral) in their community programs.
Program Management
Andrea Iger Duarte
Program Manager
860-418-6801

Prevention and Health Promotion Division Compendium 2020
Infrastructure and Programs
Page 15
CONNECTICUT NETWORKS OF CARE FOR SUICIDE PREVENTION (NCSP)
Purpose:
The Connecticut Networks of Care for Suicide Prevention (NCSP) is a $3.68 million dollar, 5 year
grant from the federal Substance Abuse and Mental Health Services Administration (SAMHSA), and
has a special focus on at risk youth, ages 10 to 24. The grant seeks to establish a statewide network
of care for suicide prevention, intervention and response. It will also facilitate the implementation of
intensive community-based efforts to reduce non-fatal suicide attempts and suicide deaths.
The Network of Care for Suicide Prevention embeds suicide prevention as a core priority across
Connecticut. It utilizes culturally competent interventions that have been researched and shown to be
effective at preventing suicide.
The NCSP will serve diverse youth and young adults age 10-24 and supportive adults representative
of the CT population with emphasis on young people identified at increased risk of suicide and who
have attempted suicide.
The Connecticut Departments of Mental Health and Addiction Services, Children and Families, and
Public Health, with the guidance of the CT Suicide Advisory Board co-direct the grant implementation
and activities.
Priority Populations:
Youth and young adults 10-24 years old, and communities at large and their citizens
Strategy Types:
Three primary evidence-based practices (EBP) drive the NCSP: 1) the SAMHSA’s Strategic Prevention
Framework; 2) the Jed Foundation (TJF)/Suicide Prevention Resource Center Model for
Comprehensive Suicide Prevention and Mental Health Promotion (Suicide Prevention Resource Center,
2011); and 3) the National Action Alliance for Suicide Prevention’s Zero Suicide in Health and
Behavioral Healthcare. A combination of EBPs, strategies, guidance documents and tools will be
applied to address universal, selective, and indicated populations to have the greatest impact at the
state and community levels.
Program Management
Andrea Iger Duarte
Program Manager
860-418-6801

Prevention and Health Promotion Division Compendium 2020
Infrastructure and Programs
Page 16
STATE TOBACCO PREVENTION AND ENFORCEMENT PROGRAM
Synar Tobacco Compliance Initiative
Purpose:
Collaborate with communities to inform retailers and the public about laws prohibiting the sale of
tobacco products to minors, and to support prevention efforts through compliance inspections,
education and awareness.
Focus Population(s):
Tobacco retail owners, managers and front line retail personnel
Strategies:
Annual Synar Tobacco Compliance Inspection Sample– Unannounced tobacco compliance
inspections conducted on a statically drawn sample of establishments to determine
Connecticut’s Retailer Violation Rate as required by the Federal Synar Amendment.
Police Partnership Inspections – Unannounced tobacco compliance inspections conducted in
concert with State and local law enforcement authorities having a Memorandum of Agreement
with DMHAS to enforce the criminal statutes of Connecticut’s tobacco youth access laws.
Eighteen Month Inspections – Unannounced compliance inspections of tobacco retailers that
have not received an inspection in the past eighteen months.
Merchant Education Inspections – Announced inspections to provide tobacco retailers with
education and awareness materials to ensure compliance with state and federal law.
The Electronic Nicotine Delivery System Compliance Inspection Program - Unannounced
electronic cigarette compliance inspections conducted with State and local law enforcement
authorities to prevent the sale of electronic cigarettes to minors.
Tobacco Merchant and Community Education Initiative (TMCEI)
Purpose:
The purpose of the merchant education campaign is to inform tobacco retailers about the provisions
of the state’s youth access laws to encourage voluntary compliance. Through the TMCEI, the Merchant
Education Program produces and distributes educational materials to approximately 4,500
establishments to help merchants and their employees comply with Connecticut’s tobacco youth access
laws. The purpose of community education activities is to increase public awareness of youth tobacco
issues.
Focus Population(s):
Tobacco retail owners, managers, front line retail personnel, youth, and service providers
Strategies:
The Tobacco Merchant Education Campaign provides awareness materials for licensed
tobacco retailers throughout Connecticut. The materials inform retailers about youth access
laws, provide specific strategies for compliance with such laws, and emphasize the health
effects of tobacco use.
Prevention and Health Promotion Division Compendium 2020
Infrastructure and Programs
Page 17
Tobacco Merchant & Community Education Steering Committee is a key component of a
statewide tobacco prevention community services campaign. The Steering Committee guides
and informs the campaign process resulting in the most effective campaign materials and
activities, leading to reductions in sales of tobacco products to youth under 18.
Tobacco Sales: Do the Right Thing is an interactive online training designed to build the skills
and knowledge of tobacco retail owners, managers, and front line retail personnel to prevent
retailer sales of tobacco products to youth under the age of 18. The learning components
feature real-life scenarios, state and federal tobacco laws and the associated legal
requirements.
Urban Tobacco Inspection Program
Purpose:
Historically, urban tobacco non-compliance rates are twice the statewide average and drive the
retailer violation rate reported to SAMHSA in the Annual Synar Report. A grant from the Tobacco
and Health Trust Fund provides funding directly to urban areas to do two separate but equally
important tasks: 1) conduct tobacco compliance inspections to enforce state law at the point of sale
and 2) provide retailers with education and awareness material including information about the new
online training program.
Focus Population(s):
Tobacco retail owners, managers and front line retail personnel in Bridgeport, New Haven, Hartford,
and Stamford
Strategies:
Unannounced compliance inspections conducted independently by the municipal police
agencies in Bridgeport, Hartford, New Haven and Stamford
The distribution of tobacco retailer education and awareness materials
Program Management
Gregory F. Carver
Supervising Special Investigator
860-418-6702

Prevention and Health Promotion Division Compendium 2020
Infrastructure and Programs
Page 18
FOOD AND DRUG ADMINISTRATION (FDA) TOBACCO PREVENTION AND ENFORCEMENT PROGRAM
Purpose:
The Family Smoking Prevention and Tobacco Control Act grants the FDA the authority to regulate
tobacco products in the US and all relevant territories. The Tobacco Control Act places specific
restrictions on the marketing and sales of tobacco products to individuals under 18 years of age.
DMHAS entered into a contract with the FDA to enforce applicable provisions of the Tobacco Control
Act and its implementing regulations in Connecticut.
Focus Population(s):
Tobacco merchants throughout the State: FDA tobacco compliance initiative requires the
implementation of a statewide enforcement program with an emphasis directed toward special
populations located within urban areas.
Strategies:
Undercover Buy Inspections – Unannounced inspections conducted to monitor the sale of
tobacco products to youth under the age of 18, and that photo identification is requested
from individuals appearing younger than 27.
Advertising and Labeling Inspections – Announced inspections conducted to monitor tobacco
labels, store signage, and the sale of non-tobacco products with tobacco band names to
mention a few.
Program Management
Holly White
Program Coordinator
Supervising Special Investigator
860 418-6837
Bryan Champagne
Backup Program Coordinator
Special Investigator
860-418-6781
Prevention and Health Promotion Division Compendium 2020
Infrastructure and Programs
Page 19
CT SAFE SCHOOLS HEALTHY STUDENTS (SSHS) DIFFUSION PROJECT
Purpose:
The Safe Schools/Healthy Students Initiative is a 8.6 million dollar four year grant that takes a
collaborative and comprehensive approach, drawing on the best practices and the latest thinking in
education, justice, social services, and mental health to help communities take action.
SSHS requires the development of statewide management team and local management teams that
serve an advisory role and share in decision making. There are three SSHS local education authorities
including Bridgeport, Middletown and the Consolidated School District of New Britain who serve as
learning laboratories for the project and though the lesson learned to develop, maintain and promote
statewide diffusion and sustainability.
Focus Population(s):
Children and students birth through 12th grade
Strategies:
The guiding principles are one of three components of the SS/HS Framework that links the five
elements with the five strategic approaches to ensure a comprehensive approach to youth violence
prevention and mental health promotion. These principles include: cultural and linguistic competency,
serving vulnerable and at-risk populations, developmentally appropriate, resource leveraging,
sustainability, youth guided and family driven and evidence-based interventions.
The Strategic approach makes up the roadmap that ensures success in planning and implementation
and supports improvement in how education, child, and family-serving agencies work together at the
state and local educational agency (LEA)-community level to address youth violence prevention and
mental health promotion.
Program Management
Carol P. Meredith
Program Manager
860-418-6826
Prevention and Health Promotion Division Compendium 2020
Infrastructure and Programs
Page 20
PARTNERSHIPS FOR SUCCESS 2015
Purpose:
The Partnership for Success 2015 Grant (PFS) is a five year 8.2 million dollar grant awarded through
a competitive bid to Connecticut. It will allow Connecticut to continue successful community-based
approaches that prevent underage drinking and prescription drug abuse/misuse through the use of
the Strategic Prevention Framework. This data-driven public health approach will build on existing
successes of community based coalitions that address underage drinking, including several other state
and federally funded Coalitions and community based programs currently in place covering each
region of the state.
Focus Population(s) and Goals:
Reduction of past month alcohol use rates for individuals aged of 12 - 20.
Reduction of past month prescription drug abuse/misuse rates for individuals aged 12-25
Preventing the onset and reducing the progression of childhood/underage drinking.
Strengthening capacity and infrastructure at the State and community level to implement data
driven evidenced based policies, practices and programs.
Collaborative approach aligning state and community strategies, redirection of existing
services, leveraging human and fiscal resources to sustain efforts.
Strategies:
Community coalitions throughout the state will use a public health approach to decrease alcohol
consumption and prescription drug abuse/misuse; build on existing resources to implement effective
environmental strategies such as curtailing retail and social access, policy change, enforcement, media
advocacy, and parental and merchant education; and measure change utilizing student survey and
other social indicator data.
Program Management
Dawn Grodzki
Program Director
860-418-6772
Stephanie L. Moran
Program Manager
860-418-6880

Prevention and Health Promotion Division Compendium 2020
Infrastructure and Programs
Page 21
NOW IS THE TIME – HEALTHY TRANSITIONS – CT STRONG
Purpose:
The Now is the Time – Healthy Transitions, CT Seamless Transitions & Recovery Opportunities for
Network Growth (STRONG) is a 5 year, 5 million dollar grant awarded to Connecticut through a
competitive process. The program purpose is to identify and engage youth and young adults who
have or are at risk for behavioral health disorders and connect them to high quality care.
Focus Population(s)
CT STRONG will work with youth and young adults ages 16 to 25 who have or are at risk for
behavioral health disorders in the communities of Milford, New London and Middletown.
Strategies and Goals:
Utilize social marketing and public education approaches such as media campaigns to inform
people about mental illness, reduce stigma and discrimination and provide connections to
services.
Identify young people who may have behavioral health disorders and engage them into
treatment, services and supports.
Implement the key principles of the Wraparound approach; a planning process that
incorporates the preferences, strengths and natural supports of the individual to determine
how to best serve them.
Ensure that families, including natural supports beyond traditional families are engaged and
included in recovery planning.
Enhance existing transitional youth behavioral health services to create a strengths based,
family focused, gender responsive and recovery oriented system of care that takes into
consideration the culture of the youth and family.
Program Management
Dawn Grodzki
Program Manager
860-418-6772

Prevention and Health Promotion Division Compendium 2020
Infrastructure and Programs
Page 22
STATEWIDE HEALTHY CAMPUS INITIATIVE
Purpose:
To develop a comprehensive prevention system that is responsive to the needs of young adults, ages
18-25 attending public universities throughout Connecticut. The Initiative is based on a 3-in-1
Framework recommended by the National Institute on Alcohol Abuse and Alcoholism (NIAAA). The
goal is to change the culture of drinking and other substance use/abuse using broad-based and
comprehensive, integrated programs with multiple complementary components that focus on: (1)
individuals, including at-risk or alcohol-dependent drinkers, (2) the student population as a whole, and
(3) the college and the surrounding community.
Focus Population(s):
The primary focus population is college students ages 18-25. Secondarily, programs may focus on
family members, peers, schools and communities at large.
Strategies:
Address gaps in substance abuse prevention and early intervention services;
Support culturally responsive, age appropriate, and evidence-based approaches for young
adults;
Further develop Connecticut’s prevention data infrastructure and capacity to collect and
analyze outcome data and report on key performance measures.
Program Management
Dawn Grodzki
Program Director
860-418-6772
Stephanie L. Moran
Program Manager
860-418-6880
Prevention and Health Promotion Division Compendium 2020
Infrastructure and Programs
Page 23
SPECIALIZED CIT FOR YOUNG ADULTS
Purpose:
The Specialized CIT for Young Adults is a $966,666 dollar, 3 year grant (9/30/13-9/29/16) from
the federal Substance Abuse and Mental Health Services Administration (SAMHSA) to enhance the
capacity of its Crisis Intervention Teams (CITs) involving law enforcement and mental health mobile
crisis providers to respond to the needs of young adults aged 18-25 who are diverted from arrest to
the most appropriate treatment for their mental health, substance abuse, or co-occurring disorders. At
least 225 young adults (75 per year) are expected to be served.
This initiative builds on close relationships between criminal justice and behavioral health agencies that
followed the creation of CT’s Criminal Justice Policy Advisory Commission (CJPAC), including DMHAS,
corrections and parole, probation, the State’s Attorney, public defender, municipal and state police,
and victims’ advocates. Additional partners include the CT Alliance to Benefit Law Enforcement
(CABLE), the entity which conducts training for current Crisis Intervention Teams (CITs), the National
Alliance on Mental Illness: Connecticut (NAMI CT), Advanced Behavioral Health, and consultants from
Yale and the Institute of Living. to create a strong team with all relevant stakeholders well
represented. The project is being evaluated by the University of CT School of Social Work.
Priority Populations:
Young adults 18-29 years old
Strategy Types:
Train and provide on-going consultation to CITs to employ age-specific techniques for
engaging YAs in treatment and/or support services;
Train and provide on-going consultation to CITs to recognize Early Psychosis and to distinguish
Early Psychosis from other conditions, such as substance-induced psychosis and trauma-related
conditions;
Organize a statewide network of providers with expertise in treatment of YAs, especially
those with the ability to provide Early Psychosis treatment, or to treat co-occurring disorders
(CODs);
Provide 24/7 clinical phone consultation assistance which can be accessed by CITs whenever
there is a problem identifying appropriate providers; and
Offer young adult peer services throughout the regions of the state, including support groups
and networking through social media.
Program Management
Andrea Iger Duarte
Program Manager
860-418-6801

Prevention and Health Promotion Division Compendium 2020
Infrastructure and Programs
Page 24
COURAGE TO SPEAK FOUNDATION
Purpose:
The Courage to Speak Foundation was founded in 1996 after Ginger and Larry Katz lost their son,
Ian to a drug overdose. Since then The Courage to Speak Foundation mission has been to save lives
by empowering youth to be drug free and encouraging parents to communicate effectively with their
children about the dangers of illicit drug use.
Priority Populations:
School age youth, young adults, and parents who have lost a family member to drug addiction
Strategy Types:
Positive Youth Development Prostrations encourages effective communication between children
and parents/trusted adults about the dangers of drugs and other risky behaviors.
Helping Families Heal Parent Support Group is for parents who have lost a family member to
drug addiction.
Helping Families Heal Phone Support Group is for parents who have lost a family member to
drug addiction that may be in crisis and need immediate support.
The Courage to Speak Foundation website is a comprehensive resource for parents, students,
educators, families and others interested in preventing adolescent/teen use of substance
abuse.
Program Management
Robin Cox
Prevention Services Coordinator
860-418-6955

Prevention and Health Promotion Division Compendium 2020
Needs Assessment, Planning, Resource Allocation and Data Collection
Page 25
NEEDS ASSESSMENT, PLANNING, RESOURCE
ALLOCATION AND DATA COLLECTION NEEDS ASSESSMENT
RESOURCE ALLOCATION
DATA COLLECTION
NEEDS ASSESSMENT
Using epidemiological and other relevant data and information, the Prevention and Health Promotion
Unit regularly explores substance use and abuse patterns unique to Connecticut’s communities and use
these data to paint a picture of the nature and burden of the problem throughout the State.
Collectively, the groups and processes described below inform funding decisions by 1) assessing the
prevalence of risk factors based on gender, race, age, socio-economic status and geographic
location; 2) analyzing trends as well as the number of individuals needing services; 3) assessing the
adequacy and appropriateness of prevention services; 4) matching prevention needs to resources;
and 5) predicting where future substance abuse problems are likely to arise.
The State Epidemiological Outcomes Workgroup
The State Epidemiological Outcomes Workgroup (SEOW) is charged with compiling indicators of
substance abuse and related consequences, tracking data trends over time, and promoting the use of
data to continually focus and strengthen ATOD prevention efforts statewide. In addition to DMHAS, it
is comprised of representatives from the Departments of Children and Families, Consumer Protection
Liquor Control Unit, Corrections, Education, Motor Vehicles, Public Health, Public Safety, Social
Services, and Transportation; the Judicial Branch Court Support Services; Multicultural Leadership
Institute; Office of Policy and Management, and researchers from the University of Connecticut Health
Center. It meets quarterly to eamine new sources of prevention and treatment need indicator data.
Regional Action Councils
DMHAS Regional Action Councils (RACs) legislative mandate is to (1) determine the extent of the
substance abuse problems within their sub-regions; (2) determine the status of resources to address
such problems; (3) identify gaps in the substance abuse service continuum; and, (4) identify changes
to the community environment that will reduce substance abuse (Connecticut Statute Sec. 17a-671).
Furthermore, the legislation requires that their membership be comprised of diverse members of the
community, including, chief elected official, the chief of police and the superintendent of schools of
each municipality within the sub-region; one representative designated by the Commissioner of
Mental Health and Addiction Services from each treatment facility operated by the department and
serving such sub-region; business and professional leaders; members of the General Assembly;
service providers; representatives of minority populations; religious organizations; representatives of
private funding organizations; and the media.

Prevention and Health Promotion Division Compendium 2020
Needs Assessment, Planning, Resource Allocation and Data Collection
Page 26
Sub-regional Prevention Priority Reports
Every two years, RACs produce Sub regional Prevention Priority Reports to describe 1) the burden of
substance abuse, problem gambling, and suicide in the subregions, 2) prioritized prevention needs,
and 3) the capacity of the sub-regions’ communities to address those needs. These reports are based
on data-driven analyses of issues in the sub-region, with assistance from key community members.
The reports and accompanying data are used as a building block for state and community-level
processes, including capacity and readiness building, strategic planning, implementation of evidence-
based programs and strategies, and evaluation of efforts to reduce substance abuse and promote
mental health.
Sub regional Priority Setting Process
The sub regional priority setting process conducted by the RACs involves the following tasks:
Compile sub regional socio demographic and indicator data using data provided by the
SEOW and additional community-level data and information, such as student survey focus
group results;
Produce eight one-page sub regional epidemiological profiles describing magnitude, impact,
and response capacity;
Convene their Community Needs Assessment Workgroups to conduct the priority ranking
process.
Community Needs Assessment Workgroups
DMHAS is committed to supporting an inclusive, comprehensive assessment process at the local, sub
regional, regional, and state levels. Accordingly, RACs convene Community Needs Assessment
Workgroups to participate in the development of the Subregional Prevention Priority Report and to
support the work of community prevention coalitions. The role of the workgroup is to 1) contribute
additional data and information; 2) assist in interpreting data and information; and 3) participate in
the priority setting process.
Each RAC Director ensures that the Community Needs Assessment Workgroup comprises diverse
community stakeholders, including youth; parents; school personnel; staff from youth-serving
organizations; researchers; local government officials; healthcare professionals, nonprofit agency
staff; and representatives from the business community, law enforcement, faith community, and
prevention coalitions. Sub-populations (i.e., those of various racial/ethnic, sexual orientation, gender,
language, disability, and culture) and members of historically underrepresented populations are also
represented.
Prevention Training Needs Assessment
The Training and Technical Assistance Service Center will conduct a Needs Assessment to develop
prevention training and technical assistance strategies to enhance Workforce Development efforts in
the State.

Prevention and Health Promotion Division Compendium 2020
Needs Assessment, Planning, Resource Allocation and Data Collection
Page 27
Other Studies/Surveys
DMHAS also utilizes results of other local, state and national studies and surveys in its program
decisions. Some of these studies and surveys are the DMHAS Ecstasy Prevention Initiative (2003),
DMHAS CT Youth Suicide Prevention Initiative (2010), CT Department of Public Health’s Connecticut
School Health Survey, American College Health Association National College Health Assessment, Penn
State Center for the Study of Collegiate Mental Health Pilot Study, University of Michigan’s
Monitoring the Future Study; SAMHSA National Survey on Drug Use and Health; Centers for Disease
Control and Prevention’s Behavioral Risk Factor Surveillance System Survey, core survey of alcohol
and drug use on campus and a host of other studies conducted statewide.

Prevention and Health Promotion Division Compendium 2020
Needs Assessment, Planning, Resource Allocation and Data Collection
Page 28
RESOURCE ALLOCATION
The majority of DMHAS’ prevention funding is obtained from the Substance Abuse, Mental Health
Services Administration (SAMHSA) Center for Substance Abuse Prevention (CSAP). Funds comprise of
the stipulated 20% of the Substance Abuse Prevention & Treatment Block Grant set aside for
prevention services and competitive grants. A smaller portion of funds comes from the State’s
General and Drug Asset Forfeiture Funds. Allocation of these funds is based on funding mandates,
priority setting reports, State Epidemiological/Outcomes Workgroup and other advisory groups’
recommendations, and is made through competitive requests for proposals (RFPs). The allocation
approach used in the CT ensures that all funded policies, practices, and programs support community-
level ATOD consumption and consequences.
PREVENTION RESOURCE ALLOCATION SFY 2015
Funding Streams Amount Programs Supported
SAMHSA Center for Mental
Health Services $400,000 Connecticut Suicide Prevention Initiative
SAMHSA Center for Substance
Abuse Prevention $1,658188 Partnerships for Success 2015
SAMHSA Center for Mental
Health Services 1,000,000 Now is the Time – Healthy Transitions
State Drug Assets Forfeiture
Revolving Account $246,350 Regional Action Councils
State Pretrial Alcohol Education
Services $499,996 Regional Action Councils
Federal Substance Abuse
Prevention & Treatment Block
Grant
$4,772,719
Connecticut SPF Coalitions Initiative, Local Prevention Councils,
CT Clearinghouse, Regional Action Councils, Statewide
Resource Links, Tobacco Prevention & Enforcement Program,
Courage to Speak Foundation.
Social Services Block Grant $17,272 CT Clearinghouse
Federal Food & Drug
Administration $1,150,000 FDA Tobacco Prevention and Enforcement Program
State Tobacco & Health Trust Fund $287,000 Urban Tobacco Inspection Program
Other State Funds $1,664,496 Regional Action Councils, Governor’s Prevention Partnership,
CT Clearinghouse, Tobacco Prevention & Enforcement Program
Total Prevention Funding $11,696,021

Prevention and Health Promotion Division Compendium 2020
Needs Assessment, Planning, Resource Allocation and Data Collection
Page 29
DATA COLLECTION
Interagency Data Workgroup
Standing legislation requires DMHAS to establish uniform policies and procedures for collecting,
standardizing, managing and evaluating data related to substance use, abuse and addiction
programs administered by state agencies, state-funded community-based programs and the Judicial
Branch. The Interagency Operational Data Collection Workgroup was created in response to this
legislation. At the core of this legislation is the desire to have a comprehensive understanding of those
individuals receiving substance abuse education, prevention, intervention and treatment services, as
they move through an array of state-sponsored services. This initiative is meant to create a fully
integrated substance abuse services data system. A system which can not only provide client
demographic data across state agencies, and reveal trends in those receiving services, but also
indicate the full breadth of whether the services resulted in positive client outcomes, and determine
the cost benefit to the state. Having this policy-relevant and program development information at
hand will lead to better approaches to preventing, delaying or treating substance use or abuse.
There are several agencies serving on this workgroup that have resources in prevention. They include
Departments of Children and Families, Motor Vehicles, Transportation, Social Services, Education, the
Judicial Branch, and the Office of Policy and Management as well as DMHAS’ prevention staff.
The State Epidemiological Outcomes Workgroup
The State Epidemiological Outcomes Workgroup (SEOW) is charged with compiling indicators of
substance abuse and related consequences, tracking data trends over time, and promoting the use of
data to continually focus and strengthen ATOD prevention efforts statewide. In addition to DMHAS, it
comprises representatives from the Departments of Children and Families, Consumer Protection Liquor
Control Unit, Corrections, Education, Motor Vehicles, Public Health, Public Safety, Social Services, and
Transportation; the Judicial Branch Court Support Services; Multicultural Leadership Institute; Office of
Policy and Management, and researchers from the University of Connecticut Health Center. It meets
quarterly to explore new sources of prevention and treatment need indicator data.
Prevention Data Infrastructure (PDI)
In response to the SAPT Block Grant requirement to collect and report National Outcome Measures
(NOMS) for prevention, which comprise eight domains (abstinence, employment/ education, crime and
criminal justice, stability in housing, access/capacity, retention, social connectedness, perception of
care cost effectiveness, and use of evidence-based practices), DMHAS has enhanced its Prevention
Data Infrastructure. With technical assistance from SAMHSA, all States will:
Standardize operational definitions and outcome measures, and link records to support pre-
and post-service comparisons.
Develop benchmarking strategies to determine acceptable levels of outcomes.
Produce routine management reports to direct technical assistance and science-to-services
program to implement interventions designed to result in improved outcomes.
Achieve full State reporting by the end of fiscal year (FY) 2007. In the interim, each year
more States will report with standard definitions until all States are on board.
Prevention and Health Promotion Division Compendium 2020
Needs Assessment, Planning, Resource Allocation and Data Collection
Page 30
The PDI uses the following data management systems for reporting on prevention program activities:
CT IMPACT – collecting process and qualitative data on program monitoring and provider
reports for Substance Abuse Prevention and Treatment Block Grant reporting
Tobacco Compliance System – collecting State tobacco compliance inspection data and field
merchant education activities for the Annual Synar Report
Tobacco Inspection Management System – collecting federal Food & Drug Administration
(FDA) tobacco compliance inspection data and advertising & labeling for the Annual Synar
Report FDA contract reporting
Tobacco Sales: Do the Right Thing – collecting retailer training data for reporting to the
Department of Revenue Services and the Annual Synar Report

Prevention and Health Promotion Division Compendium 2020
Interagency Coordination
Page 31
INTERAGENCY COORDINATION INTRODUCTION TO INTERAGENCY COORDINATION
INTERAGENCY BOARDS, COMMITTEES, COALITIONS, COLLABORATIVE, PARTNERSHIPS AND
WORKGROUPS
INTERAGENCY COORDINATION INTRODUCTION
There is a growing understanding in Connecticut of the importance of a coordinated approach to
both substance abuse prevention service delivery and fiscal policy. Government leaders have
recognized the limited capacity that one agency has on its own in reducing substance abuse and have
worked hard to foster relationships that could support and enhance the state’s substance abuse
prevention system. The chart below shows the participants in the state’s efforts to implement a plan to
improve cost-efficiency, interagency coordination, and the effectiveness of the prevention and
intervention system. The interagency committees described on the following pages are those in which
staff from the DMHAS Prevention Unit is involved.

Prevention and Health Promotion Division Compendium 2020
Interagency Coordination
Page 32
NATIONAL PREVENTION NETWORK
Partners:
Prevention Leaders from the Single State Authorities for Alcohol and Other Drug Abuse representing
each of the 50 states, the District of Columbia and 8 U.S. Territories
Purpose:
As a component of the National Association of State Alcohol and Drug Abuse Directors (NASADAD)
the National Prevention Network provides culturally appropriate guidance and leadership to
national, state and local prevention efforts to reduce the incidence and prevalence of alcohol,
tobacco and other drug problems.
ACADEMIC PARTNERSHIP
Partners:
University of Connecticut School of Social Work, University of Connecticut Health Center, The
Consultation Center at Yale University
Purpose:
This partnership was created to provide consultation and evaluation support to several federally
funded prevention initiatives: the Connecticut Youth Suicide Prevention Initiative, Governor’s
Prevention Initiative for Connecticut State Universities, and Tobacco Prevention & Enforcement
Program, Interagency Boards, Committees, Coalitions, Collaborative, Partnerships and Workgroups.
CONNECTICUT ALCOHOL & DRUG POLICY COUNCIL
Partners:
Office of Policy and Management Department of Education Department of Children and Families Department of Transportation Department of Social Services Department of Public Health Judicial Branch Department of Corrections Department of Public Safety Department of Motor Vehicles Department of Consumer Protection Department of Insurance Board of Parole Office of the Chief Public Defender Legislators Chief State’s Attorney UCONN Health Center Department of Higher Education Private Sector Representatives
Purpose:
The Connecticut Alcohol and Drug Policy Council was created by legislation charging it with
examining and improving the statewide substance abuse system and developing a plan and action
strategies to reduce the harmful effects of this complex and challenging problem.

Prevention and Health Promotion Division Compendium 2020
Interagency Coordination
Page 33
CONNECTICUT INHALANT PREVENTION TASK FORCE
Partners:
Youth Service Agencies Police Departments Regional Substance Abuse Action Councils Connecticut Poison Control Center Governor’s Prevention Partnership State Agencies & Other Community Organizations
Purpose:
The Taskforce has two primary goals: 1) Increase awareness of inhalant abuse statewide and 2)
Research, recommend and implement effective prevention strategies.
These goals will be carried out through activities that include: the collection of data on inhalant use,
related injuries, and deaths, training of trainers for the purpose of expanding the knowledge base in
Connecticut, and dissemination of print materials to parents, educators, and youth serving agencies.
CONNECTICUT PRESCRIPTION DRUG ABUSE TASK FORCE
Partners:
Youth Service Agencies Police Departments State Agencies Connecticut Poison Control Center Governor’s Prevention Partnership Connecticut Clearinghouse Regional Substance Abuse Action Councils Other Community Organizations
Purpose:
The Taskforce has two primary goals: 1) Increase awareness of prescription drug abuse statewide
and 2) Research, recommend and implement effective prevention strategies.
DMHAS POLICE PARTNERSHIP PROGRAM
Partners:
Municipal Police Agencies Connecticut State Police
Purpose:
This program is a partnership between Connecticut police agencies and DMHAS to facilitate the
enforcement of criminal laws that prohibit the sell of tobacco products to individuals less than 18
years of age. DMHAS investigators work in concert with law enforcement and infractions are issued
to non-compliant vendors, merchant education materials are distributed, and press releases are
publicized. There are approximates 100 Connecticut cities and towns that have Memorandum of
Agreement with DMHAS. The Connecticut State Police work with DMHAS in town that do not have
municipal police department.

Prevention and Health Promotion Division Compendium 2020
Interagency Coordination
Page 34
INTERAGENCY DATA SHARING INITIATIVE
Partners:
Office of Policy and Management Department of Education Department of Children and Families Department of Social Services Department of Transportation Department of Public Health Department of Motor Vehicles Judicial Branch
Purpose:
This workgroup was created in response to legislation requiring DMHAS to establish uniform policies
and procedures across the state for collecting, standardizing, managing, and evaluating data. Data
will include: 1) the use of prevention, education, treatment and criminal justice services related to
substance use, abuse and addiction; 2) client demographics and substance use, abuse and addiction
information; and 3) the quality and cost effectiveness of substance use, abuse and addiction services.
CONNECTICUT SUICIDE ADVISORY BOARD
Partners:
Jordan Matthew Porco Memorial Foundation True Colors United Way of CT& National CT State University System Wellness & Recovery & National CT National Guard Suicide Prevention Lifeline Crisis Center Office of the Child Advocate Children and Families CT Community College System Veterans Administration CT University of CT Health Center Healthcare System-Suicide Prevention Program Multicultural Leadership Institute University of CT School of Social Work Wheeler Clinic Center for Prevention Veterans Affairs Graduate students, and parents
Purpose:
The Connecticut Suicide Advisory Board (CTSAB) was established January 2012 through the merger
of the CT Youth Suicide Advisory Board and the Interagency Suicide Prevention Network to create
one state-level Suicide Advisory Board to address suicide across the lifespan. The 1989 legislation
requires the existence of an advisory body to inform the Commissioner of DCF on strategies for the
coordination of youth suicide prevention throughout Connecticut. The CTSAB is co-chaired by the CT
Department of Mental Health and Addiction Services and the Department of Children and Families,
and is a diverse, collaborative network of over 250 people and 100 agencies representing
advocates, educators, leaders, and survivors concerned with advancing and sustaining efforts to
eliminate suicide across the life span. The CTSAB developed the State of CT Suicide Prevention Plan
2020 (PLAN 2020) that establishes five goals and 22 objectives for the state to initiate state
prevention activities, and is aligned with the National Strategy for Suicide Prevention and Healthy
People 2020. PLAN 2020 is designed to be accessible to everyone to be utilized as a working
template to guide their efforts small and large to prevent suicide attempts and deaths and ultimately
save lives in Connecticut.

Prevention and Health Promotion Division Compendium 2020
Interagency Coordination
Page 35
JUVENILE JUSTICE ADVISORY COMMITTEE – SUBCOMMITTEE ON COMBATING UNDERAGE DRINKING
Partners:
Office of Policy and Management Local Law Enforcement Agencies Department of Children and Families Court Support Services Division Judicial Branch Department of Transportation Department of
Public Safety Purpose:
The purpose of the Juvenile Justice Advisory Committee (JJAC) is to prevent delinquency and improve
Connecticut's juvenile justice system. It was established in accordance with the Juvenile Justice and
Delinquency Prevention Act (JJDPA) of 1974 as amended, and it is responsible for overseeing the
distribution and use of federal juvenile justice funds to support youth development programs and
improvements to Connecticut's juvenile justice system.
CONNECTICUT POVERTY AND PREVENTION COUNCIL
Partners:
Governor’s Office of Policy and Management Department of Children and Families State Department of Education Department of Public Health Judicial Branch-Court Support Services Division Department of Mental Retardation
Purpose:
The SPPC was created in 2001 through prevention legislation (PA 01-121) and is charged with
evaluating and promoting prevention work in the state of CT. SPPC goals are to: increase the
awareness of the value of prevention; strengthen state and local networks’ involvement in prevention;
improve data collection on prevention programs to enhance system measurement capabilities; and
share & implement best practices through effective prevention programs.
TOBACCO MERCHANT & COMMUNITY EDUCATION STEERING COMMITTEE
Partners:
Wheeler Clinic's Connecticut Clearinghouse State Agencies New England Convenience Store Association Regional Action Councils Convenience Stores and Large Chain Stores Ledge Light Health District Independent Connecticut Petroleum Association J. Polep Distribution Services
Purpose:
A key component of a statewide tobacco prevention community services campaign, to guide and
inform the campaign process resulting in the most effective campaign materials and activities, leading
to reductions in sales of tobacco products to youth under 18 years of age

Prevention and Health Promotion Division Compendium 2020
Interagency Coordination
Page 36
CONNECTICUT CANCER PARTNERSHIP – PREVENTION SUBCOMMITTEE
Partners:
Over 200 groups and individuals that are key stakeholders in cancer prevention and control in
Connecticut
Purpose:
To coordinate a statewide comprehensive approach to cancer prevention and control, through the
development, implementation, and evaluation of a statewide Comprehensive Cancer Control Plan.
MOBILIZE AGAINST TOBACCO FOR CONNECTICUT’S HEALTH (MATCH COALITION INC.)
Partners:
American Cancer Society American Lung Association American Heart Association Connecticut Association of Directors of Health American Academy of Pediatrics State Agencies Parents and Youth Non-profit organizations/agencies
Purpose:
MATCH advocates for resources for public health policies to reduce the use of tobacco among
children and adults, and collaborates with programs furthering those goals.
CT STRONG STATE LEVEL; TRANSITION TEAM
Partners:
DMHAS FAVOR Family Advocacy Organization Department of Public Health Department of Children Families Bureau of Rehab Services (BRS) Southwest Regional Mental Health Board Judicial Court Support Services Division (CSSD) Office of the Health Care Advocate (OHCA) Department of Social Services State Department of Education Department of Labor Office of the Child Advocate Department of Corrections (DOC) Advanced Behavioral Health Department of Higher Education Join, Be, Rise
Purpose:
Is to review progress on state and local level initiatives to improve seamless transition for youth ages
16 to 25.

Prevention and Health Promotion Division Compendium 2020
Interagency Coordination
Page 37
SPE/PFS ADVISORY COUNCIL
Partners:
DMHAS Department of Consumer Protection Department of Public Health Department of Children Families Department of Transportation Veterans Affairs Judicial Court Support Services Division Board of Pardons & Parole Department of Social Services State Department of Education Office of Policy & Management UConn Health Center Department of Corrections Department of Emergency Services & Public
Protection
Purpose:
To improve the statewide alcohol, tobacco and other drug (ATOD) prevention infrastructure and in
turn help families and communities to prevent or delay the use of alcohol, tobacco, and other drugs.
Also to provide advice and guidance on the implementation of the PFS 2015 which will expand the
use of the Strategic Prevention Framework (SPF) to urban communities that demonstrate a high need
for prevention programs that address a reduction in: 1) alcohol use in youth age 12 to 20 or 2)
prescription drug misuse or abuse among persons age 12 to 25.
AMERICAN FOUNDATION FOR SUICIDE PREVENTION –NORTHERN CT CHAPTER
Partners:
Survivors of suicide, individuals with mental disorders and their families, mental health professionals,
community and business leaders, state agencies, hospitals
Purpose:
In CT there are two chapters of the American Foundation for Suicide Prevention. These Chapters are
two of 75 local chapters nationwide. Chapter volunteers deliver innovative prevention programs to
schools and businesses, reach out to survivors of suicide loss, organize fundraising events, and act as a
go-to resource for their entire community. They are at the forefront of increasing the public’s
awareness of suicide as a public health issue that is preventable and are able to advocate for policy
change. Out of the Darkness Walks hosted in communities statewide serve as the primary fundraising
effort, and 50% of funds raised go to the chapter and support CT suicide prevention.
SCHOOL BASED HEALTH CENTERS ADVISORY COMMITTEE
Partners
Family Advocate or Parent Department of Public Health (FLIS) School Nurse, Hartford Public Schools State Department of Education Cornell Scott Hill Health Center Department of Mental Health and Addiction Services Integrated Health Services, Inc. Department of Social Services Branford Public Schools Department of Children and Families SBHC not receiving state funds Connecticut Association of School Based Health Centers American Academy of Pediatrics Quinnipiac Valley Health District Griffin Hospital Commission on Children

Prevention and Health Promotion Division Compendium 2020
Interagency Coordination
Page 38
Purpose:
The School Based Health Centers Advisory Committee is a legislatively mandated committee. Its
purpose is to advise the Commissioner of Public Health on matters relating to (1) statutory and
regulatory changes to improve health care through access to school-based health centers, and (2)
minimum standards for the provision of services in school-based health centers to ensure that high
quality health care services are provided in school-based health centers.
Prevention and Health Promotion Division Compendium 2020
Quality Assurance, Monitoring, and Workforce Development
Page 39
QUALITY ASSURANCE, MONITORING, AND WORKFORCE DEVELOPMENT SYSTEM OVERSIGHT AND PROGRAM REPORTING
MONITORING, CORRECTIVE ACTION AND TECHNICAL ASSISTANCE
STAFF CREDENTIALING AND OPERATING STANDARDS
WORKFORCE DEVELOPMENT
CONNECTICUT INTERMEDIATE OUTCOMES
RESEARCH-BASED BEST PRACTICE STRATEGIES, PRACTICES AND PROGRAMS
SYSTEM OVERSIGHT AND PROGRAM REPORTING
Each DMHAS Prevention provider is required to submit a quarterly report that provides information
on program activities and progress in addition to reports on the numbers of populations served by
strategies. These reports provide information that assists DMHAS in assessing program effectiveness,
planning, program development, resource allocation and ensuring access to services.
MONITORING, CORRECTIVE ACTION AND TECHNICAL ASSISTANCE
Prevention staffs in conjunction with DMHAS Regional Teams visit all funded prevention programs
annually to review compliance with DMHAS operating standards, contract language and program
mandates. Major problems found during monitoring visits are brought to the provider’s attention and
programs are given the opportunity to implement corrective action. Prevention staffs provide technical
assistance. Technical assistance is also available through the statewide service delivery agents or
Resource Links. The purpose of the site visit is to ensure compliance with Prevention Standards, DMHAS
contract and federal requirements enhance accountability and ensure that prevention programs are
implemented consistently throughout the state. Site visits include an administrative review
(administration), a program review (set up & operation), and records/document review. Our
feedback loop to the Agency includes an entrance conference to explain focus of visit, an exit
conference to discuss findings, a written report with recommendations or corrective action plan, and
additional feedback to agencies through management meetings and independent evaluations. Our
follow up entails Prevention staff monitoring for completeness of corrective action plan and overall
progress.
STAFF CREDENTIALING AND OPERATING STANDARDS
DMHAS, in conjunction with Connecticut prevention provider agencies and organizations, developed
the Cultivating Programs That Work: Operating Standards for Prevention and Health Promotion
Programs for prevention programs funded by DMHAS. The standards, guidelines, and supporting
documents link state-of-the-art prevention theory to effective, comprehensive, and accountable

Prevention and Health Promotion Division Compendium 2020
Quality Assurance, Monitoring, and Workforce Development
Page 40
prevention practice and implementation of the standards should result in positive outcomes for
programs, staff and participants.
The purpose of these standards is to provide assurances to the public that alcohol and drug abuse
prevention and early intervention programs are regulated under a set of minimum standards
established by DMHAS. These standards establish a minimum level of program operation intended to
reflect quality substance abuse prevention programs. The operating standards articulate a service
philosophy that promotes the concept of health promotion as a means of building on the strengths and
positive resources of individuals, families, schools, and communities throughout the State of Connecticut
to prevent the use, misuse, or abuse of legal or illegal substances. To support prevention staff training
and certification, the Prevention Training Collaborative provides a wide range of prevention training
across the state. There are three levels of prevention certification for paraprofessionals, and
volunteers and prevention program staffs with and without four-year degrees.
WORKFORCE DEVELOPMENT
Towards the prevention goal of promoting the overall health and wellness of individuals within
communities through effective practices, the Prevention Unit facilitates the provision of a broad
spectrum of workforce development and capacity building trainings to social service agencies,
community members, prevention professionals and volunteers.
Training courses offered by the Prevention Unit are consistent with the SAPT Block Grant, which
requires that continuing education be provided for employees who deliver prevention services to
individuals and communities. DMHAS is committed to developing its workforce at the state, regional
and local levels including grant funded programs.
Utilizing the Training and Technical Assistance Service Center, (TTASC), the DMHAS Prevention unit will
increase prevention workforce competencies and improve access by prevention workers to the most
relevant, responsive, and culturally appropriate prevention education and training resources by
utilizing the Strategic Prevention Framework (SPF) process to:
Maximize and target training and technical assistance resources by coordinating efforts across
multiple sectors to recruit, retain, educate and train the prevention workforce
Increase the use of evidence-based programs and strategies that address the national
outcome measures (NOMs) and lead to measureable outcomes, and
Increase the reach of prevention training through the application of technology.
The TTASC will conduct a training, technical assistance and staff development Needs Assessment of
the Prevention Workforce. A Training and Technical Assistance Workgroup will advise in the
development and implementation of the Needs Assessment and the Workforce Development and
Training Plan. The workgroup will consist of representatives from Prevention service providers, the
DMHAS Prevention and Health Promotion Unit and other associated stakeholders. A comprehensive
Workforce Development and Training Plan will be created and training and technical assistance
opportunities will be created, publicized and implemented.

Prevention and Health Promotion Division Compendium 2020
Quality Assurance, Monitoring, and Workforce Development
Page 41
Intensive cutting edge training are provided statewide by leaders, practitioners and experts in the
field including the Northeast Center for the Application of Prevention Technologies (NECAPT).
Trainings cover all core areas of prevention as required by the International Certification and
Reciprocity Consortium (ICRC) for alcohol and other drug abuse prevention certification and focus on
substance abuse, mental health and other related problems.
DMHAS employees and providers alike have opportunities to develop professionally through
participation in annual national prevention conferences and regional prevention schools.
Another source of training is the New England School of Addiction Studies. The school was formed in
1970 to provide training opportunities in support of substance abuse service system development
and workforce development across New England. Each year the NEIAS offers an intensive weeklong
experience for participants to further their knowledge, skills and experience in the field of substance
abuse prevention. The school has a comprehensive curriculum of best practice courses for all skill
levels, taught by regional and national experts.
In addition to the ongoing statewide prevention workforce development, the Director of Prevention at
DMHAS serve as members of the National Prevention Network’s (NPN) Workforce Development
Committee. In this capacity, the leadership at DMHAS has worked with CSAP staff and other state
NPNs in the development of a framework that aims to enable NPN members, SSA/state staff to
develop skills necessary for planned change. Core components and priorities of the NPN/CSAP have
served as a blueprint for workforce development within Connecticut’s SSA to include: organization
and infrastructure development, substance abuse prevention data systems/ NOMS, program
standards, the SPF five steps, planning and managing for outcomes, leadership and resource
development, and other core competencies in supervision, fellowship/mentoring, and cultural
competence.
CONNECTICUT INTERMEDIATE OUTCOMES
The vision for Connecticut is the quantifiable reduction of substance use and promotion of mental
health through a statewide prevention system that allows its citizens to live healthy, productive and
rewarding lives. An Intermediate Outcomes document was developed by the State Agency
Workgroup for use by the providers to drive the goals and objectives of their prevention programs.
Intermediate outcomes are short-term indicators to measure progress toward a long-term goal. These
outcomes are based on research about what factors increase or decrease the likelihood of substance
use and are referred to as risk or protective factors. To take it one step further, state agency
prevention partners are in the process of developing an outcome monitoring system for mental health,
violence and substance abuse across state agencies.
RESEARCH-BASED BEST PRACTICE STRATEGIES, PRACTICES AND PROGRAMS
Over the past few years there has been increased emphasis in the field of prevention to implement
programs that have been evaluated and proven effective. Congress wants to demonstrate to
taxpayers that the money going into prevention is addressing societal concerns by funding programs
Prevention and Health Promotion Division Compendium 2020
Quality Assurance, Monitoring, and Workforce Development
Page 42
that are known to show positive results. Therefore all federal agencies that currently fund prevention
efforts have included a requirement that programs must be researched and shown to produce positive
outcomes.
As a result, DMHAS has been involved with a variety of science-based initiatives over the past years
that have been evaluated by our academic partners at the University of Connecticut (UConn) Health
Center Department of Community Medicine, UConn Center for Public Health and Health Policy-
Institute for Public Health Research, UConn School of Social Work, and Yale University:
1999-2003 CSAP State Incentive Grant: Governor’s Prevention Initiative for Youth
1999-2003 CSAP Family Strengthening Program Series
2000-2003 CMHS Partnership Resource Infrastructure- Violence Prevention Initiative
2001-2005 CSAP Achievement Through Mentoring
2002-2006 CSAP Ecstasy and Other Club Drug Prevention Intervention
2004-2008 CSAP State Incentive Grant Enhancement Initiative: Governor’s Prevention Initiative for
Connecticut State Universities
2004-2010 CSAP Strategic Prevention Framework State Incentive Grant
2006-2010 CMHS CT Youth Suicide Prevention Initiative
2009-2014 CSAP Underage Drinking/Partnerships for Success
2009-2015 CSAP Partnership for Success
2010-2012 DOE Grants for Coalitions
2011-2012 CSAP Strategic Prevention Enhancement Grant
2011-2014 HHS/FDA Tobacco Compliance Initiative
2011-2015 CMHS CT Campus Suicide Prevention Initiative
i National Research Council and Institute of Medicine. (2009). Preventing mental, emotional, and behavioral disorders among young people: Progress and possibilities (O’Connell, M. E., Boat, T., & Warner, K. E., Eds.) Washington, DC: National Academies Press.