prevalence and risk factors for allergic rhinitis in primary school children
TRANSCRIPT

International Journal of Pediatric Otorhinolaryngology (2007) 71, 463—471
www.elsevier.com/locate/ijporl
Prevalence and risk factors for allergic rhinitis inprimary school children
Zeynep Tamay a,*, Ahmet Akcay b, Ulker Ones a, Nermin Guler a,Gurkan Kilic a, Mehmet Zencir c
aDepartment of Pediatrics, Division of Allergy and Chest Diseases, Istanbul School of Medicine, IstanbulUniversity, Istanbul, TurkeybDepartment of Pediatrics, Pamukkale School of Medicine, Pamukkale University, Pamukkale, TurkeycDepartment of Public Health, Pamukkale School of Medicine, Pamukkale University,Pamukkale, Turkey
Received 13 June 2006; received in revised form 15 November 2006; accepted 17 November 2006
KEYWORDSAllergic rhinitis;ISAAC;Risk factors;Children
Summary
Objective: Allergic rhinitis is a common chronic illness of childhood. The aim of thestudy was to evaluate the prevalence and risk factors of allergic rhinitis in 6—12-year-old schoolchildren in Istanbul.Methods: A total of 2500 children aged between 6 and 12 years in randomly selectedsix primary schools of Istanbul were surveyed by using the International Study ofAsthma and Allergies in Childhood (ISAAC) questionnaire between April and May 2004.Results: Of them 2387 (1185 M/1202 F) questionnaires were appropriately completedby the parents with an overall response of 95.4%. The prevalence of physician-diagnosed allergic rhinitis was 7.9% (n = 189). A family history of atopy(aOR = 1.30, 95% CI = 1.00—1.68), frequent respiratory tract infection (aOR = 1.36,95% CI = 1.08—1.70) and sinusitis (aOR = 2.29, 95% CI = 1.64—3.19), antibiotic use inthe first year of life (aOR = 1.26, 95% CI = 1.01—1.57), cat at home in the first year oflife (aOR = 2.21, 95% CI = 1.36—3.61), dampness at home (aOR = 1.31, 95% CI = 1.04—1.65) and perianal redness (aOR = 1.26, 95% CI = 1.01—1.57) were significant forincreased risk for allergic rhinitis. Frequent consumption of fruits and vegetableswere inversely, and frequent consumption of lollipops and candies were positivelyassociated with allergic rhinitis symptoms.Conclusion: Our study reconfirmed that family history of atopy, frequent respiratorytract infections, antibiotics given in the first year of life, cat at home in the first yearof life, dampness at home, perianal redness and dietary habits are important
* Corresponding author at: Department of Pediatrics, Istanbul Medical Faculty, Capa 34390, Istanbul, Turkey.Tel.: +90 212 4142000/32349; fax: +90 212 6319301.
E-mail address: [email protected] (Z. Tamay).
0165-5876/$ — see front matter # 2006 Elsevier Ireland Ltd. All rights reserved.doi:10.1016/j.ijporl.2006.11.013

464 Z. Tamay et al.
independent risk factors for AR. Researchers worldwide should be focused to thesefactors and try to develop policies for early intervention, primary and secondarypreventions for allergic diseases.# 2006 Elsevier Ireland Ltd. All rights reserved.
1. Introduction
Allergic rhinitis (AR) is a very common disease inchildhood as well as in adults and impairs the qualityof life if left untreated [1]. AR is characterized bynasal itching, sneezing, watery rhinorrhoea andnasal obstruction [1]. The prevalence of childhoodAR shows wide variation throughout the world, ran-ging from 0.8% to 39.7% [2].
The prevalence of allergic diseases has increasedpredominantly in developed countries, which indi-cates that environmental risk factors and life stylerather than genetic predisposition seem to be themajor determinants of allergic diseases [2—4]. Var-ious risk factors have been described for AR accord-ing to different stages during life. Family history ofatopy, month of birth, parental smoking, male sex,early exposure to allergens or pollutions were con-sidered to be potential risk factors by epidemiolo-gical surveys [1,4—6]. But major determinantscontributing development of AR is still not clear.
The aim of the study was to evaluate the pre-valence and risk factors of allergic rhinitis in 6—12-year-old schoolchildren in Istanbul.
2. Methods
This survey was held in children aged between 6 and12 years in randomly selected six primary schools inIstanbul. A total of 2500 questionnaires were dis-tributed to the children to be completed by theirparents at home. The return visit to the school wasdone within a 2-week period to try to collect datafrom children formerly absent. The standardizedISAAC Phase I written core questionnaire was trans-lated into Turkish and used. There have been quite afew studies carried out in Turkey using the ISAACquestionnaire [7—10], therefore it is well known andvalidated in Turkish studies. An additional question-naire was prepared to identify demographic fea-tures and potential risk factors, including: sex,family history of atopy, the presence of physician-diagnosed eczema or food allergy, frequent upperairway infections and sinusitis, history of tonsillect-omy or adenoidectomy, antibiotic or paracetamoluse in the first year of life, exposure to tobaccosmoke at home, maternal and paternal smoking, cator dog ownership in the first year of life, home
dampness, heating system, born in and living periodin Istanbul, exposure to diesel trucks, perianal red-ness and diet.
Dietary intake was estimated by using addition-ally a semi-quantitative food frequency question-naire. Consumption of protective foods includingstarch such as potatoes, rice, cereals, pasta, vege-tables, fish, other sea foods, fruits, nuts, olive oil,fish oil, and some traditional foods made fromgrapes and mulberries, fermented drinks made frommillets and various seeds; aggravating foods includ-ing fast-food, potato chips, crackers, chocolates,lollipops, candies, cookies, muffins, margarine;other foods including eggs, animal fats, milk anddairy products, meat, polyunsaturated fatty acids(butter), sun-flower oil, corn oil, tea, olive and wereasked [11]. Analysis of diet variables were deter-mined by frequency of consumption of foods in threegroups including: ‘‘never or occasionally’’, ‘‘once ortwice per week’’ and ‘‘three or more times a week’’.
Having a problem with sneezing or a runny, orblocked nose in the absence of a cold or a flu in thepast 12 months was assessed as ‘‘current allergicrhinitis’’ [2,12]. Positive response to the questionabout having had allergic rhinitis diagnosed by aphysician was considered to be ‘‘ever doctor-diag-nosed allergic rhinitis’’. Severity of allergic rhinitiswas assessed among children with current rhinitisfrom the responses the questions on the presence ofaccompanying itchy-watery eyes and about inter-ference with daily activities because of nose pro-blem.
2.1. Ethical consideration
The study was approved by the Ethics Committee ofIstanbul University, Istanbul School of Medicine.
2.2. Statistical analysis
Statistical analysis included percentages, oddsratios (OR), 95% confidence interval (95% CI), chi-squared test and backward logistic regression. Pre-valence estimates were calculated by dividing posi-tive responses to the given question by the totalnumber of completed questionnaires. The 95% CI ofthese prevalence rates was also calculated. Accord-ing to ISAAC policy, missing and inconsistentresponses were included in the denominator for

Prevalence and risk factors for allergic rhinitis 465
the prevalence calculations, but excluded from sub-sequent bivariate analysis [13—17]. The relationbetween risk factors and current AR prevalencewas performed by univariate analysis using chi-squared tests and univariate odds ratio (uOR) andits 95% CI. A p value less than 0.05 was consideredsignificant. Risk factors significantly affecting cur-rent AR prevalence were family history of atopy, thepresence of physician-diagnosed eczema or foodallergy, frequent upper airway infections and sinu-sitis, history of adenoidectomy, antibiotic or para-cetamol use in the first year of life, cat or dogownership in the first year of life, home dampness,exposure to diesel trucks, perianal redness. Theserisk factors were tested in a backward logisticregression analysis with adjusted odds ratio (aOR)and its 95% CI. Consumption of foods were analysedby the same method, separately. The SPSS softwarepackage Version 12 was used for all statistical ana-lyses.
3. Results
Of the 2500 questionnaires distributed, 2387 ques-tionnaires were appropriately completed by theparents with an overall response of 95.4%. Therewere 1185 (49.6%) boys and 1202 (50.4%) girls with aM/F ratio of 0.99.
The prevalence for lifetime rhinitis, rhinitis inlast 12 months, rhinoconjunctivitis in last 12 monthsand physician-diagnosed rhinitis were 44.3%, 28.9%,7.8% and 7.9%, respectively (Table 1).
No significant relation was observed between sexand prevalence of AR (p = 0.34, uOR = 0.92, 95%CI = 0.77—1.10).
A family history of atopy ( p < 0.001, uOR = 1.78,95% CI = 1.44—2.19), physician-diagnosed foodallergy ( p = 0.005, uOR = 1.51, 95% CI = 1.13—2.03), physician-diagnosed eczema ( p = 0.016,uOR = 1.77, 95% CI = 1.11—2.83) were significantfor increased risk for AR. Of the children with AR,62 (34.6%) had family history of atopy, 87 (48.1%)had asthma, 19 (10.6%) had eczema, and 37 (20.8%)had food allergy.
Table 1 Summary of parental-completed allergic rhi-nitis questionnaire data
Questionnaire Prevalence (%)
Lifetime rhinitis 44.3
12-Month prevalenceRhinitis 28.9Associated itchy eye 7.8
Physician-diagnosed allergic rhinitis 7.9
Frequent upper airway infection and sinusitiswere significant risk factors for AR (p < 0.001,aOR = 1.36, 95% CI = 1.08—1.70 and aOR = 2.29,95% CI = 1.64—3.19, respectively). Of children withAR, 62.1% had frequent upper respiratory infectionsand 21.7% had frequent sinusitis.
History of tonsillectomy was not correlated withAR. Although history of adenoidectomy was signifi-cant by univariate analysis, it lost its significancewhen evaluated by multivariate analysis.
Antibiotic and paracetamol use in the first year oflife increased the risk for development of AR byunivariate analysis ( p < 0.001); antibiotic use in thefirst year was a significant risk factor by multivariateanalysis (aOR = 1.26, 95% CI = 1.01—1.57).
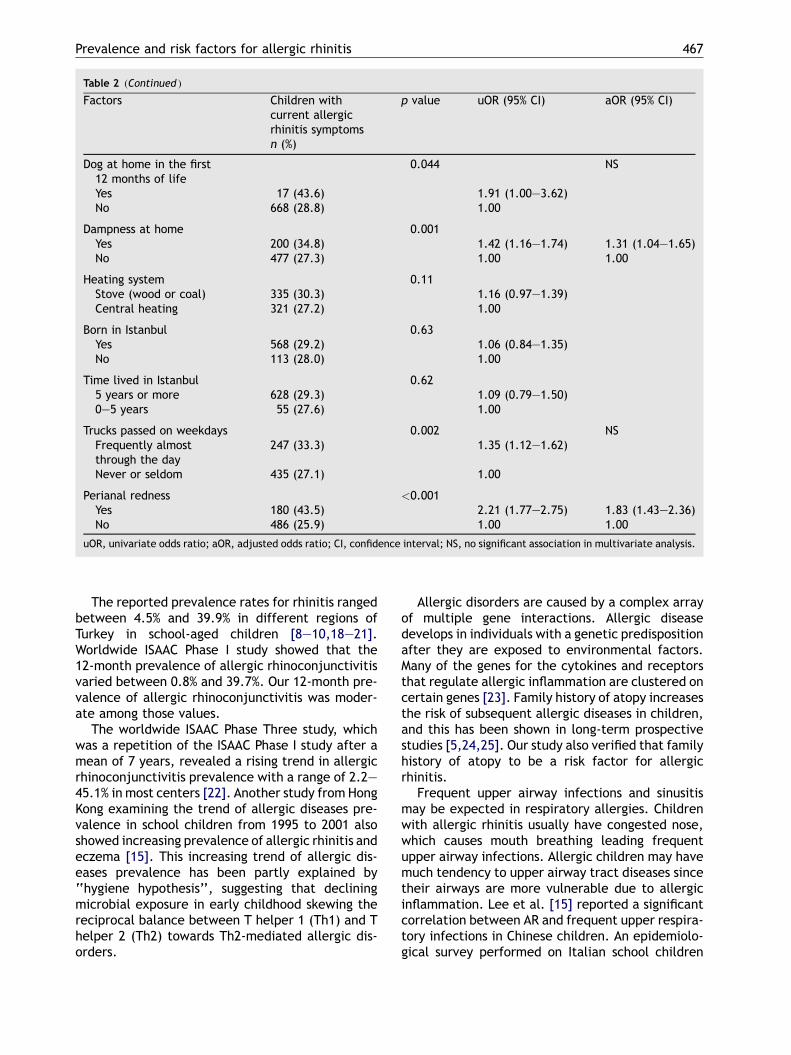
AR prevalence was neither associated with expo-sure to tobacco smoke at home nor with maternaland paternal smoking. Cat or dog ownership duringthe first year of life significantly affected the devel-opment of AR ( p = 0.001, uOR = 2.02, 95% CI = 1.32—3.09 and p = 0.044, uOR = 1.91, 95% CI = 1.00—3.62,respectively). Especially cat at home during the firstyear of life was an independent risk factor for AR(aOR = 2.21, 95% CI = 1.36—3.61). Dampness athome was significantly and independently asso-ciated with AR ( p = 0.001, uOR = 1.42, 95%CI = 1.16—1.74 and aOR = 1.31, 95% CI = 1.04—1.65).
Although exposure to diesel truck was a signifi-cant risk factor for AR (p = 0.002, uOR = 1.35, 95%CI = 1.12—1.62) by univariate analysis, it lost itssignificance when it was evaluated by multivariateanalysis. Heating system, born in Istanbul or timelived in Istanbul did not affect the AR prevalence.
Perianal redness was a significant independentrisk factor for AR ( p < 0.001, uOR = 2.21, 95%CI = 1.77—2.75 and aOR = 1.83, 95% CI = 1.43—2.36). Risk factors for AR were shown in Table 2.
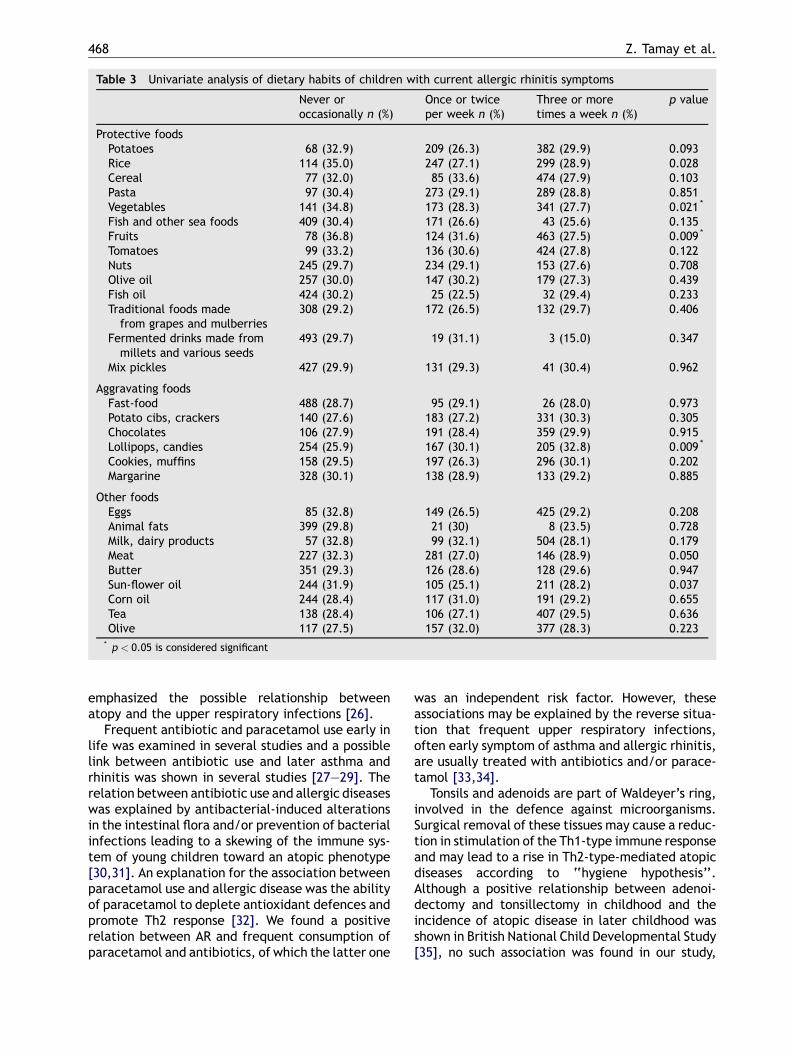
Among the protective foods rice, vegetables andfruits were relatively less consumpted; among theaggravating foods lollipops, candies were relativelymore consumpted and among other foods meat andsun-flower oil were consumpted three or more timesa week by children with allergic rhinitis (Table 3).When these risk factors were tested in a backwardlogistic regression analysis with adjusted odds, onlyfruit, vegetable and lollipop, candy consumptionwere independently and significantly affected ARprevalence (Table 4).
4. Discussion
The present study showed that nearly one third of6—12-year-old Turkish children had rhinitis, definedas sneezing, runny or blocked nose in the absence ofa cold or the flue.

466 Z. Tamay et al.
Table 2 Potential risk factors for allergic rhinitis
Factors Children withcurrent allergicrhinitis symptomsn (%)
p value uOR (95% CI) aOR (95% CI)
Sex 0.34M 332 (28.0) 0.92 (0.77—1.10)F 358 (29.8) 1.00
Family history for atopy <0.001Yes 192 (39.2) 1.78 (1.44—2.19) 1.30 (1.00—1.68)No 485 (26.6) 1.00 1.00
Physician-diagnosedfood allergy
0.005 NS
Yes 80 (37.2) 1.51 (1.13—2.03)No 584 (28.1) 1.00
Physician-diagnosed eczema 0.016 NSYes 31 (41.3) 1.77 (1.11—2.83)No 636 (28.5) 1.00
Frequent respiratorytract infection
<0.001
Yes 370 (36.3) 1.85 (1.54—2.22) 1.36 (1.08—1.70)No 302 (23.6) 1.00 1.00
Frequent sinusitis <0.001Yes 109 (53.2) 3.09 (2.31—4.13) 2.29 (1.64—3.19)No 563 (26.9) 1.00 1.00
Tonsillectomy 0.26Yes 45 (33.1) 1.23 (0.85—1.79)No 637 (28.8) 1.00
Adenoidectomy 0.037 NSYes 61 (36.3) 1.42 (1.02—1.96)No 624 (28.7) 1.00
Antibiotics given in thefirst year of life
<0.001
Yes 430 (33.2) 1.57 (1.30—1.89) 1.26 (1.01—1.57)No 241 (24.1) 1.00 1.00
Paracetamol given in thefirst 12 months of life
<0.001 NS
Yes 503 (31.4) 1.45 (1.18—1.78)No 171 (23.9) 1.00
Smoking at home 0.08Yes 407 (30.4) 1.18 (0.98—1.41)No 272 (27.1) 1.00
Smoking of child’s mother 0.41Yes 183 (30.4) 1.09 (0.89—1.33)No 496 (28.6) 1.00
Smoking of child’s father 0.17Yes 408 (30.1) 1.14 (0.95—1.37)No 267 (27.5) 1.00
Cat at home in the first12 months of life
0.001
Yes 40 (44.4) 2.02 (1.32—3.09) 2.21 (1.36—3.61)No 640 (28.4) 1.00 1.00
Prevalence and risk factors for allergic rhinitis 467
Table 2 (Continued )
Factors Children withcurrent allergicrhinitis symptomsn (%)
p value uOR (95% CI) aOR (95% CI)
Dog at home in the first12 months of life
0.044 NS
Yes 17 (43.6) 1.91 (1.00—3.62)No 668 (28.8) 1.00
Dampness at home 0.001Yes 200 (34.8) 1.42 (1.16—1.74) 1.31 (1.04—1.65)No 477 (27.3) 1.00 1.00
Heating system 0.11Stove (wood or coal) 335 (30.3) 1.16 (0.97—1.39)Central heating 321 (27.2) 1.00
Born in Istanbul 0.63Yes 568 (29.2) 1.06 (0.84—1.35)No 113 (28.0) 1.00
Time lived in Istanbul 0.625 years or more 628 (29.3) 1.09 (0.79—1.50)0—5 years 55 (27.6) 1.00
Trucks passed on weekdays 0.002 NSFrequently almostthrough the day
247 (33.3) 1.35 (1.12—1.62)
Never or seldom 435 (27.1) 1.00
Perianal redness <0.001Yes 180 (43.5) 2.21 (1.77—2.75) 1.83 (1.43—2.36)No 486 (25.9) 1.00 1.00
uOR, univariate odds ratio; aOR, adjusted odds ratio; CI, confidence interval; NS, no significant association in multivariate analysis.
The reported prevalence rates for rhinitis rangedbetween 4.5% and 39.9% in different regions ofTurkey in school-aged children [8—10,18—21].Worldwide ISAAC Phase I study showed that the12-month prevalence of allergic rhinoconjunctivitisvaried between 0.8% and 39.7%. Our 12-month pre-valence of allergic rhinoconjunctivitis was moder-ate among those values.
The worldwide ISAAC Phase Three study, whichwas a repetition of the ISAAC Phase I study after amean of 7 years, revealed a rising trend in allergicrhinoconjunctivitis prevalence with a range of 2.2—45.1% in most centers [22]. Another study from HongKong examining the trend of allergic diseases pre-valence in school children from 1995 to 2001 alsoshowed increasing prevalence of allergic rhinitis andeczema [15]. This increasing trend of allergic dis-eases prevalence has been partly explained by‘‘hygiene hypothesis’’, suggesting that decliningmicrobial exposure in early childhood skewing thereciprocal balance between T helper 1 (Th1) and Thelper 2 (Th2) towards Th2-mediated allergic dis-orders.
Allergic disorders are caused by a complex arrayof multiple gene interactions. Allergic diseasedevelops in individuals with a genetic predispositionafter they are exposed to environmental factors.Many of the genes for the cytokines and receptorsthat regulate allergic inflammation are clustered oncertain genes [23]. Family history of atopy increasesthe risk of subsequent allergic diseases in children,and this has been shown in long-term prospectivestudies [5,24,25]. Our study also verified that familyhistory of atopy to be a risk factor for allergicrhinitis.
Frequent upper airway infections and sinusitismay be expected in respiratory allergies. Childrenwith allergic rhinitis usually have congested nose,which causes mouth breathing leading frequentupper airway infections. Allergic children may havemuch tendency to upper airway tract diseases sincetheir airways are more vulnerable due to allergicinflammation. Lee et al. [15] reported a significantcorrelation between AR and frequent upper respira-tory infections in Chinese children. An epidemiolo-gical survey performed on Italian school children
468 Z. Tamay et al.
Table 3 Univariate analysis of dietary habits of children with current allergic rhinitis symptoms
Never oroccasionally n (%)
Once or twiceper week n (%)
Three or moretimes a week n (%)
p value
Protective foodsPotatoes 68 (32.9) 209 (26.3) 382 (29.9) 0.093Rice 114 (35.0) 247 (27.1) 299 (28.9) 0.028Cereal 77 (32.0) 85 (33.6) 474 (27.9) 0.103Pasta 97 (30.4) 273 (29.1) 289 (28.8) 0.851Vegetables 141 (34.8) 173 (28.3) 341 (27.7) 0.021 *
Fish and other sea foods 409 (30.4) 171 (26.6) 43 (25.6) 0.135Fruits 78 (36.8) 124 (31.6) 463 (27.5) 0.009 *
Tomatoes 99 (33.2) 136 (30.6) 424 (27.8) 0.122Nuts 245 (29.7) 234 (29.1) 153 (27.6) 0.708Olive oil 257 (30.0) 147 (30.2) 179 (27.3) 0.439Fish oil 424 (30.2) 25 (22.5) 32 (29.4) 0.233Traditional foods madefrom grapes and mulberries
308 (29.2) 172 (26.5) 132 (29.7) 0.406
Fermented drinks made frommillets and various seeds
493 (29.7) 19 (31.1) 3 (15.0) 0.347
Mix pickles 427 (29.9) 131 (29.3) 41 (30.4) 0.962
Aggravating foodsFast-food 488 (28.7) 95 (29.1) 26 (28.0) 0.973Potato cibs, crackers 140 (27.6) 183 (27.2) 331 (30.3) 0.305Chocolates 106 (27.9) 191 (28.4) 359 (29.9) 0.915Lollipops, candies 254 (25.9) 167 (30.1) 205 (32.8) 0.009 *
Cookies, muffins 158 (29.5) 197 (26.3) 296 (30.1) 0.202Margarine 328 (30.1) 138 (28.9) 133 (29.2) 0.885
Other foodsEggs 85 (32.8) 149 (26.5) 425 (29.2) 0.208Animal fats 399 (29.8) 21 (30) 8 (23.5) 0.728Milk, dairy products 57 (32.8) 99 (32.1) 504 (28.1) 0.179Meat 227 (32.3) 281 (27.0) 146 (28.9) 0.050Butter 351 (29.3) 126 (28.6) 128 (29.6) 0.947Sun-flower oil 244 (31.9) 105 (25.1) 211 (28.2) 0.037Corn oil 244 (28.4) 117 (31.0) 191 (29.2) 0.655Tea 138 (28.4) 106 (27.1) 407 (29.5) 0.636Olive 117 (27.5) 157 (32.0) 377 (28.3) 0.223
* p < 0.05 is considered significant
emphasized the possible relationship betweenatopy and the upper respiratory infections [26].
Frequent antibiotic and paracetamol use early inlife was examined in several studies and a possiblelink between antibiotic use and later asthma andrhinitis was shown in several studies [27—29]. Therelation between antibiotic use and allergic diseaseswas explained by antibacterial-induced alterationsin the intestinal flora and/or prevention of bacterialinfections leading to a skewing of the immune sys-tem of young children toward an atopic phenotype[30,31]. An explanation for the association betweenparacetamol use and allergic disease was the abilityof paracetamol to deplete antioxidant defences andpromote Th2 response [32]. We found a positiverelation between AR and frequent consumption ofparacetamol and antibiotics, of which the latter one
was an independent risk factor. However, theseassociations may be explained by the reverse situa-tion that frequent upper respiratory infections,often early symptom of asthma and allergic rhinitis,are usually treated with antibiotics and/or parace-tamol [33,34].
Tonsils and adenoids are part of Waldeyer’s ring,involved in the defence against microorganisms.Surgical removal of these tissues may cause a reduc-tion in stimulation of the Th1-type immune responseand may lead to a rise in Th2-type-mediated atopicdiseases according to ‘‘hygiene hypothesis’’.Although a positive relationship between adenoi-dectomy and tonsillectomy in childhood and theincidence of atopic disease in later childhood wasshown in British National Child Developmental Study[35], no such association was found in our study,

Prevalence and risk factors for allergic rhinitis 469
Table 4 Multivariate analysis of dietary habits of children with current allergic rhinitis symptoms
Children with current allergicrhinitis symptoms n (%)
Multivariant aOR (95% CI)
FruitsNever or rarely 78 (36.8) 1.00Once or twice/a week 124 (31.6) 0.79 (0.53—1.53)Three or more/a week 463 (27.5) 0.64 (0.45—0.91)
Vegetables NSNever or rarely 141 (34.8)Once or twice/a week 173 (28.3)Three or more/a week 341 (27.7)
Lollipops, candiesNever or rarely 254 (25.9) 1.00Once or twice/a week 167 (30.1) 1.26 (0.99—1.59)Three or more/a week 205 (32.8) 1.44 (1.15—1.81)
aOR, adjusted odds ratio; CI, confidence interval; NS, no significant association in multivariate analysis.
which was in agreement with Dutch longitudinalbirth cohort study [36].
The presence of a cat home has been found to bea significant risk factor for AR in Turkish children,although the rate of pet ownership is extremely lowin our population. The association between petownership in childhood and subsequent allergic dis-eases and sensitization is very controversial. Intri-guing, but contradictory, reports have causedconsiderable uncertainty [37—39]. Keeping a catin the home provides high-dose exposure to catallergens and increases the risk of sensitization tocat in susceptible children. On the other hand,endotoxin may be abundant in house dust particu-larly in houses with cats and dogs, and protectagainst allergen sensitization by enhancing Th1immunity. Contradictory results may be due to het-erogeneity of the population, different immuneresponse to antigens in susceptible individuals.
Some investigators found a negative significantassociation between the prevalence of allergic rhi-nitis and exposure to tobacco and parental smoking[40,41]. This inverse relation was also explained by‘‘hygiene hypothesis’’. Passive smoking might leadto high infection rates in infancy, resulting with thedominance of Th1-type immune response and lessallergic diseases. On the contrary, a positive asso-ciation between tobacco smoke and rhinitis wasreported in a number of studies [6,40,42]. Accord-ing to a meta-analysis data, no consistent associa-tion emerged between parental smoking andallergic rhinitis, which was compatible with ourresults [41].
Moisture at home may increase sensitization tomould in susceptible children by stimulating Th2-immune response. Moisture-related problems inbuildings were found to be a risk factor for asthmaand allergic symptoms among preschool children
[43]. In our study, home dampness was significantlyassociated with symptoms of AR.
Istanbul is the biggest city of Turkey, with morethan 10 million inhabitants. Western lifestyle ispredominant in this city and adaptation of immi-grants to this lifestyle can quickly occur. In ourstudy, born in or living in Istanbul was not signifi-cantly increased the risk for AR. Not classifying thepatients according to urban and rural parts of thecity might affect our results.
Motor vehicle exhaust from freeways could havean inverse effect on respiratory health of children.van Vliet et al. reported that cough, wheeze, runnynose and asthma were more frequent in childrenliving within 100 m from the freeway, where expo-sure to diesel truck too much [44]. Exposure todiesel truck may have irritant effect on airwaysfacilitating penetrating allergens to airways. Inour study, frequent exposure to diesel truck wasmore frequently reported by parents of childrenwith symptoms of AR, but it was not an independentsignificant risk factor.
Perianal redness has not been evaluated as a riskfactor for allergic diseases before. Iacono et al.found that chronic constipation with perianal fis-sures or perianal erythema can be amanifestation ofcow’s milk intolerance [45]. We think that perianalerythema can be a clue of mucosal inflammation dueto food allergy in infants and young children accord-ing to our clinical observations. In our study, peri-anal redness was a significant risk factor for AR.Although there are other factors such as fungalinfections, thread worms that cause perianal red-ness, it may be also a sign of mucosal inflammationdue to concomitant subclinic food allergy in childrenwith AR.
Several studies have suggested that the increas-ing prevalence of symptoms of allergic diseases

470 Z. Tamay et al.
could be associated with changes in the diet [46—48]. Changes in the diet may mediate an effect,through changes in gut flora. Intestinal flora ofallergic children differs from healthy children[49]; different intestinal flora may induce Th2-typeimmune response against antigens and preservationof intestinal mucosal integrity by ‘‘healthy’’ gutflora may be a protective factor against atopy andatopic diseases [50]. Besides this effect, nutrientslike antioxidants, polyunsaturated fatty acids maybe needed for healthy immune system develop-ment. In our study, a significant inverse relationshipwas found between symptoms of AR and the intakeof fruits and vegetables. Our results were in agree-ment with the previous studies [47,48]. Frequentconsumption of fruits and vegetables may be pro-tective against allergic diseases due to their anti-oxidant effects [47,48]. We also found a dose-dependent association between frequent consump-tion lollipops, candies and symptoms of AR.Although allergies to food additives are rarely seenin children, food additives existing in lollipops andcandies may act as non-specific adjuvant factors inthe development of allergic diseases.
There are several strengths of this study. First,ISAAC questionnaire has been validated in a numberof Turkish studies. Second, the data is large enoughto reflect Istanbul population. Since potential riskfactors are influenced by the same social and envir-onmental conditions and can also interact with eachother, they may affect the situation only when theyexist together. This may be the reason of the dif-ference between the results of the univariate andthe multivariate analyses, whichmay be a limitationof the study.
In conclusion our study reconfirmed that familyhistory of atopy, frequent respiratory tract infec-tions, antibiotics given in the first year of life, cat athome in the first year of life, dampness at home,perianal redness and dietary habits are importantindependent risk factors for AR. Researchers world-wide should be focused to these factors and try todevelop policies for early intervention, primary andsecondary preventions for allergic diseases.
References
[1] International Conference on Allergic Rhinitis in Childhood,in: D. Passali, R. Mosges (Eds.), Allergy 54 (S55) (1999) 7—34.
[2] D. Strachan, B. Sibbald, S. Weiland, N. Ait-Khaled, G. Ana-bwani, H.R. Anderson, et al., Worldwide variations in pre-valence of symptoms of allergic rhinoconjunctivitis inchildren: the International Study of Asthma and Allergiesin Childhood (ISAAC), Pediatr. Allergy Immunol. 8 (1997) 61—176.
[3] The International Study of Asthma and Allergies in Childhood(ISAAC) Steering Committee: worldwide variations in the
prevalence of asthma symptoms: the International Study ofAsthma and Allergies in Childhood (ISAAC), Eur. Respir. J. 12(1998) 315—335.
[4] R.M. Sly, Changing prevalence of allergic rhinitis andasthma, Ann. Allergy Asthma Immunol. 82 (1999) 233—248.
[5] S.M. Tariq, S.M. Matthews, E.A. Hakim, M. Stevens, S.H.Arshad, D.W. Hide, The prevalence of and risk factors foratopy in early childhood: a whole population birth cohortstudy, J. Allergy Clin. Immunol. 101 (1998) 587—593.
[6] M.A. Monteil, G. Joseph, C. Chang Kit, G. Wheeler, R.M.Antonie, Smoking at home is strongly associated with symp-toms of asthma and rhinitis in children of primary school agein Trinidad and Tobago, Rev. Panam. Salud Publica 16 (2004)193—198.
[7] U. Ones, N. Sapan, A. Somer, R. Disci, N. Salman, N. Guler,et al., Prevalence of childhood asthma in Istanbul, Turkey,Allergy 52 (1997) 570—575.
[8] A. Ece, A. Ceylan, Y. Saraclar, G. Saka, F. Gurkan, K. Has-polat, Prevalence of asthma and other allergic disordersamong schoolchildren in Diyarbakir, Turkey, Turk. J. Pediatr.43 (2001) 286—292.
[9] I. Bayram, S. Guneser-Kendirli, M. Yilmaz, D.U. Altintas, N.Alparslan, G. Bingol-Karakoc, The prevalence of asthma andallergic diseases in children of school age in Adana in south-ern Turkey, Turk. J. Pediatr. 46 (2004) 221—225.
[10] N. Tomac, F. Demirel, F. Acun, F. Ayoglu, Prevalence and riskfactors for childhood asthma in Zonguldak, Turkey, AllergyAsthma Proc. 26 (2005) 397—402.
[11] ISAAC Phase Three. Environmental Questionnaire Instruc-tions and Hypotheses, 6—7 yr Instructions for Completingthe Environmental Questionnaire (EQ) 6—7 years, 2006http://isaac.auckland.ac.nz/Phasethr/EnvrQuest/EQFra-me.html.
[12] H. Duhme, S.K. Weiland, P. Rudolph, A. Wienke, A. Kramer,U. Keil, Asthma and allergies among children in West andEast Germany: a comparison between Munster and Greifs-wald using the ISAAC phase I protocol, Eur. Respir. J. 11(1998) 840—847.
[13] S.H. Downs, G.B. Marks, R. Sporik, E.G. Belosouva, N.G. Car,J.K. Peat, Continued increase in the prevalence of asthmaand atopy, Arch. Dis. Child. 84 (2001) 20—23.
[14] T. Annus, M.A. Riikjarv, K. Rahu, B. Bjorksten, Modestincrease in seasonal allergic rhinitis and eczema over 8 yearsamong Estonian schoolchildren, Pediatr. Allergy Immunol. 16(2005) 315—320.
[15] S.L. Lee,W.Wong, Y.L. Lau, Increasing prevalence of allergicrhinitis but not asthma among children in Hong Kong from1995 to 2001 (Phase 3 International Study of Asthma andAllergies in Childhood), Pediatr. Allergy Immunol. 15 (2004)72—78.
[16] B. Kaur, H.R. Anderson, J. Austin, M. Burr, L.S. Harkins, D.P.Strachan, et al., Prevalence of asthma symptoms, diagnosis,and treatment in 12—14 year old children across GreatBritain (International Study of Asthma and Allergies in Child-hood, ISAAC UK), BMJ 316 (1998) 118—124.
[17] ISAAC Phase One. Section 6.1 Data Quality and Handling,2006 http://isaac.auckland.ac.nz/PhaseOne/Manual/Man-Frame.html.
[18] E. Demir, R. Tanac, D. Can, F. Gulen, A. Yenigun, K. Aksakal,Is there an increase in the prevalence of allergic diseasesamong schoolchildren from the Aegean region of Turkey?Allergy Asthma Proc. 26 (2005) 410—414.
[19] N. Akcakaya, K. Kulak, A. Hassanzadeh, Y. Camcioglu, H.Cokugras, Prevalence of bronchial asthma and allergic rhi-nitis in Istanbul school children, Eur. J. Epidemiol. 16 (2000)693—699.

Prevalence and risk factors for allergic rhinitis 471
[20] Z.T. Selcuk, T. Caglar, T. Enunlu, T. Topal, The prevalence ofallergic diseases in primary school children in Edirne, Turkey,Clin. Exp. Allergy 27 (1997) 262—269.
[21] S. Kuyucu, Y. Saraclar, A. Tuncer, P.O. Geyik, G. Adalioglu, A.Akpinarli, et al., Epidemiologic characteristics of rhinitis inTurkish children: The International Study of Asthma andAllergies in Childhood (ISAAC) phase 2, Pediatr. AllergyImmunol. 17 (2006) 269—277.
[22] M.I. Asher, et al., Worldwide time trends in the prevalenceof symptoms of asthma, allergic rhinoconjunctivitis, andeczema in childhood: ISAAC Phases One and Three repeatmulticountry cross-sectional surveys, Lancet 368 (2006)733—743.
[23] J.E. Gern, R.F. Lemanske, Pediatric allergy: can it be pre-vented? Immunol. Allergy Clin. North Am. 19 (1999) 233—252.
[24] L.G. Hansen, S. Halken, A. Host, K. Moller, O. Osterballe,Prediction of allergy from family history and cord blood IgElevels. A follow-up at the age of 5 years. Cord blood IgE. IV,Pediatr. Allergy Immunol. 4 (1993) 34—40.
[25] R.S. Zeiger, S. Heller, The development and prediction ofatopy in high-risk children: follow-up at age seven years in aprospective randomized study of combined maternal andinfant food allergen avoidance, J. Allergy Clin. Immunol. 95(6) (1995) 1179—1190.
[26] E. Porro, P. Calamita, I. Rana, L. Montini, S. Criscione, Atopyand environmental factors in upper respiratory infections:an epidemiological survey on 2304 school children, Int. J.Pediatr. Otorhinolaryngol. 24 (1992) 111—120.
[27] R.B. Newson, S.O. Shaheen, S. Chinn, P.G.J. Burney, Para-cetamol sales and atopic disease in children and adults: anecological analysis, Eur. Respir. J. 16 (2000) 817—823.
[28] G. Davey, Y. Berhane, P. Duncan, G. Aref-Adib, J. Britton, A.Venn, Use of acetaminophen and the risk of self-reportedallergic symptoms and skin sensitization in Butajira, Ethio-pia, J. Allergy Clin. Immunol. 116 (2005) 863—868.
[29] C. Cohet, S. Cheng, C. MacDonald, M. Baker, S. Foliaki, N.Huntington, et al., Infections, medication use, and the pre-valence of symptoms of asthma, rhinitis, and eczema in child-hood, J. Epidemiol. Community Health 58 (2004) 852—857.
[30] J.H. Droste, M.H. Wieringa, J.J. Weyler, V.J. Nelen, P.A.Vermeire, H.P. Van Bever, Does the use of antibiotics in earlychildhood increase the risk of asthma and allergic disease?Clin. Exp. Allergy 30 (2000) 1547—1553.
[31] C.C. Johnson, D.R. Ownby, S.H. Alford, S.L. Havstad, L.K.Williams, E.M. Zoratti, et al., Antibiotic exposure in earlyinfancy and risk for childhood atopy, J. Allergy Clin. Immu-nol. 115 (2005) 1218—1224.
[32] S.O. Shaheen, J.A. Sterne, C.E. Songhurst, B.M. Margetts,P.G. Burney, Frequent paracetamol use and asthma inadults, Thorax 55 (2000) 266—270.
[33] J.C. Celedon, S.T. Weiss, Use of antibacterials in infancy:clinical implications for childhood asthma and allergies,Treat. Respir. Med. 3 (2004) 291—294.
[34] P. Cullinan, J. Harris, P. Mills, S. Moffat, C. White, J. Figg,et al., Early prescriptions of antibiotics and the risk ofallergic disease in adults: a cohort study, Thorax 59(2004) 11—15.
[35] H.R. Anderson, J.M. Bland, C.S. Peckham, Risk factors forasthma up to 16 years of age. Evidence from a nationalcohort study, Chest 91 (Suppl. 6) (1987) 127S—130S.
[36] E.S. van Hattum,W.A. Balemans, M.M. Rovers, G.A. Zielhuis,A.G. Schilder, C.K. van der Ent, Adenoidectomy and/ortonsillectomy in childhood is not associated with atopicdisease later in life, Clin. Exp. Allergy 36 (2006)40—43.
[37] F. Kurosaka, Y. Nakatani, T. Terada, A. Tanaka, H. Ikeuchi, A.Hayakawa, et al., Current cat ownership may be associatedwith the lower prevalence of atopic dermatitis, allergicrhinitis, and Japanese cedar pollinosis in schoolchildren inHimeji, Japan, Pediatr. Allergy Immunol. 17 (2006)22—28.
[38] A. Simpson, A. Custovic, Pets and the development of allergicsensitization, Curr. Allergy Asthma Rep. 5 (2005) 212—220.
[39] C. Almqvist, High allergen exposure as a risk factor forasthma and allergic disease, Clin. Rev. Allergy Immunol.28 (2005) 25—41.
[40] E.A. Mitchell, A.W. Stewart, ISAAC Phase One Study Group.International Study of Asthma and Allergy in Childhood, Theecological relationship of tobacco smoking to the prevalenceof symptoms of asthma and other atopic diseases in children:the International Study of Asthma and Allergies in Childhood(ISAAC), Eur. J. Epidemiol. 17 (2001) 667—673.
[41] D.P. Strachan, D.G. Cook, Health effects of passive smoking.5. Parental smoking and allergic sensitisation in children,Thorax 53 (1998) 117—123.
[42] H.J. Wittig, E.T. Mclaughlin, K.L. Leifer, J.D. Belloit, Riskfactors for the development of allergic disease: analysis of2190 patient records, Ann. Allergy 41 (1978) 84—88.
[43] C.G. Bornehag, J. Sundell, L. Hagerhed-Engman, T. Sigsg-gard, S. Janson, Aberg N, D.B.H. Study Group, ‘‘Dampness’’at home and its association with airway, nose, and skinsymptoms among 10,851 preschool children in Sweden: across-sectional study, Indoor Air 15 (2005) 48—55.
[44] P. van Vliet, M. Knape, J. de Hartog, N. Janssen, H. Hars-sema, B. Brunekreef, Motor vehicle exhaust and chronicrespiratory symptoms in children living near freeways,Environ. Res. 74 (1997) 122—132.
[45] G. Iacono, F. Cavataio, G. Montalto, A. Florena, M. Tummi-nello, M. Soresi, et al., Intolerance of cow’s milk and chronicconstipation in children, N. Engl. J. Med. 339 (1998) 1100—1104.
[46] A. Seaton, D.J. Codden, K. Brown, Increase in asthma: amore toxic environment or a more susceptible population?Thorax 49 (1994) 171—174.
[47] P. Ellwood, M.I. Asher, B. Bjorksten, M. Burr, N. Pearce, C.F.Robertson, Diet and asthma, allergic rhinoconjunctivitis andatopic eczema symptom prevalence: an ecological analysisof the International Study of Asthma and Allergies in Child-hood (ISAAC) data. ISAAC Phase One Study Group, Eur. Respir.J. 17 (2001) 436—443.
[48] Y. Miyake, S. Sasaki, Y. Ohya, S. Miyamoto, I. Matsunaga, T.Yoshida, et al., Soy, isoflavones, and prevalence of allergicrhinitis in Japanese women: the Osaka Maternal and ChildHealth Study, J.AllergyClin. Immunol. 115 (2005)1176—1183.
[49] B. Bjorksten, P. Naaber, E. Sepp, M. Mikelsaar, The intestinalmicroflora of Estonian and Swedish 2-year-old children, Clin.Exp. Allergy 29 (1999) 342—346.
[50] S.F. Bloomfield, R. Stanwell-Smith, R.W.R. Crevel, J. Pickup,Too clean, or not too clean: the Hygiene Hypothesis andhome hygiene, Clin. Exp. Allergy 36 (2006) 402—425.