pressure ulcer prevention/management policy
TRANSCRIPT

Page 1 of 56
Pressure Ulcer Prevention/Management Policy
Document Summary
The aim of this policy is to equip staff with the knowledge and skills to provide evident based care, which should be implemented to reduce the incidence of pressure ulcers and treat existing pressure ulcers.
DOCUMENT NUMBER POL/001/069
DATE RATIFIED Sept 2017
DATE IMPLEMENTED Sept 2017
NEXT REVIEW DATE July 2020
POLICY AUTHOR Tissue Viability Team, Cumbria
Important Note: The Intranet version of this document is the only version that is maintained.
Any printed copies should therefore be viewed as “uncontrolled” and, as such, may not necessarily contain the latest updates and amendments.

Pressure Ulcer Policy Version 5
Page 2 of 56
TABLE OF CONTENTS
1 SCOPE ............................................................................................................... 4
2 INTRODUCTION ................................................................................................. 4
3 STATEMENT OF INTENT ...................................................................................... 4
4 DEFINITIONS ..................................................................................................... 5
5 DUTIES ............................................................................................................... 7
5.1 NETWORK MANAGER, QUALITY AND SAFETY MANAGERS ARE RESPONSIBLE FOR.............................………………………………………..7
5.2 TISSUE VIABILITY SERVICE IS RESPONSIBLE FOR………………………8 5.3 ALL CLINICAL STAFF, INCLUDING TEMPORARY AND AGENCY STAFF,
ARE RESPONSIBLE FOR……………………………………………………….8
6 DETAILS OF THE POLICY .................................................................................. 9
6.1 RISK ASSESSMENT ................................................................................... 9 6.2 SKIN ASSESSMENT …………………………………………………………...10 6.3 PREVENTING DAMAGE TO THE SKIN………………………………………12 6.4 EQUIPMENT……………………………………………………………………..13 6.5 SAFE USE OF EQUIPMENT…………………………………………………...15 6.6 POSITIONING……………………………………………………………………16 6.7 SEATING…………………………………………………………………………17 6.8 HEEL PROTECTION…..………………………………………………………..18 6.9 NUTRITION………………………………………………………………………19 6.10 INCONTINENCE……………………………………………………………….19 6.11 GRADING PRESSURE ULCERS…………………………………………….20 6.12 REPORTING INCIDENCES OF PRESSURE ULCERS……………………21 6.13 PRESSURE ULCER WOUND ASSESSMENT AND TREATMENT………21 6.14 MONITORING OF PRESSURE ULCERS…………………………………...22 6.15 PATIENT / CARER EDUCATION……………………………………………..23 6.16 SAFEGUARDING………………………………………………………………23
7 TRAINING ........................................................................................................ 23
8 MONITORING COMPLIANCE WITH THIS POLICY ........................................ 23
9 REFERENCES/ BIBLIOGRAPHY .................................................................... 24
10 RELATED TRUST POLICY/PROCEDURES .................................................... 25
11 APPENDICES……………………………………………………………………..26-52
APPENDIX 1 - Scale Abstract ........................................................................... 26
APPENDIX 2 – Waterlow .................................................................................. 27
APPENDIX 3 – SSKIN ................................................................................. 28-29
APPENDIX 4 – 30 Degree Tilt Diagram ............................................................ 30
APPENDIX 5 - Repositioning Chart .................................................................. 31
APPENDIX 6 - Red Bottom Chart ..................................................................... 33
APPENDIX 7 - Moisture Lesions Vs. Pressure Damage ................................... 34

Pressure Ulcer Policy Version 5
Page 3 of 56
APPENDIX 8 - EUPAP Grading……………………………………………………..35
APPENDIX 9 - Black Heel Policy……………………………………………………36
APPENDIX 10 - Patient Comes Into Our Care With Pressure Ulcer…....…..….39
APPENDIX 11- Standard Operating Procedure for Ungradeable Ulcers……...43
APPENDIX 12 - Waterlow Flow Chart for Dementia Assessment Units…….....44
APPENDIX 13 – Discharging patients on DN caseload with Equipment ........... 45
APPENDIX 14 - Risk Assessment Form- Air Loss Mattress……………………..48
APPENDIX 15 – Skeleton with anatomical labels………………………………....53

Pressure Ulcer Policy Version 5
Page 4 of 56
1 SCOPE This is a clinical policy document which is intended for use by all health care staff employed by Cumbria Partnership Foundation Trust who work in a clinical or health improvement capacity with patients and the public, or who lead the delivery of clinical services. This includes locum, bank and agency staffs that are working on behalf of the Trust and are involved in providing any aspect of pressure ulcer care and assessment for patients relevant to their role. This also includes any member of staff undergoing training, for example medical students, health and social care trainees, student nurses, radiographers and physiotherapists, podiatrists, OTs and continence nurses.
2 INTRODUCTION
Pressure ulcers are an economic burden on the National Health Service (NHS) equating to 4% of the NHS budget (Bennett, Dealey & Posnett, 2004), with an estimated cost of £2.3 billion - £3.1 billion per year and rising (Posnett & Franks 2008). More importantly, pressure ulcers are detrimental to patients in terms of their physical, physiological and social wellbeing, resulting in a reduced quality of life and increased morbidity.
This policy aims to promote evidence based care to help prevent the development of pressure ulcers. This applies to all vulnerable individuals of all age groups.
The policy is based on guidelines published by NICE (2005, 2014) EPUAP (2009) and International Guidelines (2009), DH (2010).
Early detection of skin damage and implementation of adequate preventative strategies can prevent tissue damage altogether or reduce the seriousness of the ulceration.
3 STATEMENT OF INTENT
The aim of this policy is to equip staff with the knowledge and skills to provide evident based care, which should be implemented to reduce the incidence of pressure ulcers and treat existing pressure ulcers.
This policy covers all services and settings within the Trust including inpatient settings, clinic settings and the patient’s home. With respect to the home setting it is recognised that patient care in this environment will be provided by different organisations.
In respect to the community nurses role within the home, they will provide assessment; care planning, treatment and education; however care will also be provided by other health and social professionals who will work to their own policies and procedures. The community nurse should agree robust plans with the patient, family and carers, and these should be monitored at each visit and support given where there are difficulties. Care planning should be based on the principles set out in this policy.

Pressure Ulcer Policy Version 5
Page 5 of 56
4 DEFINITIONS What is a pressure ulcer?
Pressure ulcers are caused when an area of skin and the tissues below are damaged
as a result of being placed under pressure sufficient to impair its blood supply.
Typically they occur in a person confined to bed or a chair by an illness and as a result
they are sometimes referred to as 'bedsores', or 'pressure sores'. (NICE 2014)
Because muscle and subcutaneous tissue are more susceptible to pressure induced injury than skin, pressure ulcers are often worse than their initial appearance.
The most common sites include the buttocks, hips and heels, but pressure damage can
occur over any bony prominence (Stephen –Haynes 2006).
Tissue Viability Society.

Pressure Ulcer Policy Version 5
Page 6 of 56
Unavoidable Pressure Ulcer “Unavoidable” means that the person receiving care, developed a pressure ulcer even
though the provider of care had:
• Evaluated the person’s clinical condition and risk factors
• Planned and implemented interventions that are consistent with the person’s
needs, goals and recognised standards of practice
• Monitored and evaluated impact of the interventions and revised actions and
approaches as appropriate
• The individual refused to adhere to prevention strategies in spite of education of
the consequences of non-adherence Avoidable Pressure Ulcer.
“Avoidable” means that the person receiving care developed a pressure ulcer and the
provider of care did not do one of the following:
• Evaluate the person’s clinical condition and pressure ulcer risk factors
• Plan and implement interventions that are consistent with the person’s needs,
goals, and recognised standards of practice
• Monitor and evaluate the impact of interventions or revise the interventions as
appropriate 5 DUTIES
5.1 NETWORK MANAGER AND QUALITY AND SAFETY MANAGER:
• Ensuring this policy is compliant with any statutory legislation and that it is
implemented into practice
• Providing relevant training including record of attendance
• Development of clinical standards of practice and competency frameworks
• Ensuring systems are in place that facilitates workplace assessments of staff
competencies as part of Continuous Professional Development (CPD),
Knowledge and Skills Framework (KSF) review and appraisal
• Providing access to specialist advice for staff, patients and carers.
• Providing a means of recording care in all settings
• The provision of support to conduct audit and collation of information from across
the organisation
• Undertaking investigations, compiling reports and taking appropriate actions to
improve patient care
• Ensuring this policy is implemented and monitored within their area of
responsibility and remain responsible for the support and supervision of their staff
• Supporting a blame free culture in regard to incident reporting so that lessons can
be learnt
Pressure Ulcer Policy Version 5
Page 7 of 56
• Ensure all Grade 3 & 4 pressure ulcers that develop within their area have a 72
Hour Report undertaken and that action plans are put into place to improve
patient care 5.2 TISSUE VIABILITY SERVICE, NETWORK MANAGER AND QUALITY AND
SAFETYMANAGER IS RESPONSIBLE FOR:
• Updating the policy in light of new evidence/ guidance being published
• Lead on the audit of clinical practice
• Providing support and expertise in their specialist area.
• Keeping abreast of new developments in practice
• Involvement in appropriate 72 Hour Reports 5.3 ALL CLINICAL STAFF, INCLUDING TEMPORARY AND AGENCY STAFF, ARE
RESPONSIBLE FOR:
• An understanding of this policy and the recommendations for good practice
• Ensuring all relevant staff attend training in pressure ulcer assessment, and care
planning in line with agreed time frames. Staff are requested to attend face to
face updates a minimum of every three years
• Recording the pressure ulcer grade using the European Pressure Ulcer Advisory
Panel Classification System
• Ensuring that all patients receive an initial and ongoing risk assessment within
the first episode of care, (within the first 2 visits for Community Staff) which must
include an in-depth assessment of intrinsic and extrinsic factors related to
pressure ulcer care as outlined within this policy
• Continually reviewing wound progress to detect either improvement or
deterioration in the pressure ulcer and respond appropriately
• Recognising that all Grade 1 – 4 and ungradeable pressure ulcers are to be
reported as a local clinical incident and Grade 3 and 4 acquired in our services
care requires the completion of a 72 hour report.
• Obtaining clinical photography of the wound. Photographs should be obtained
with patient’s consent, at the initial development of the wound, when any
deterioration is noted, or when the duration of healing rate is expected to be
greater than four weeks. When photographing a wound, it is essential to include
the wound location and wound dimensions, using the measuring guide in the
sterile dressing packs.
• Recognising the importance of and acting upon the outcome of risk assessment
in preventative care
• Understanding the roles of the multidisciplinary team in the prevention and
treatment of pressure ulcers

Pressure Ulcer Policy Version 5
Page 8 of 56
• Recognising and supporting carers and relatives who play vital roles in the
prevention and management of pressure ulcers
• Sharing knowledge and delivering education at all levels about preventative care
and treatment
• Understanding the involvement of clinical experts such as the Tissue Viability
Service within community hospital and community services as and when
appropriate and be able to initiate referral when clinically indicated
• Maintaining accurate records 6 DETAILS OF THE POLICY
6.1 RISK ASSESSMENT
Risk assessment is a fundamental part of preventing pressure ulcers and prescribing
care. Many pressure ulcer risk assessment scales have been developed but these
represent only one part of the process. Risk assessment tools encourage a structured approach to assessment, complement
experienced nurse’s judgment and act as an aide memoir for less experienced
clinicians, but should not be used to prescribe equipment or treatment. Where patients are being cared for in their own homes, Community Services should
ensure that they make every contact count, and regardless of the reason for visit, take
the opportunity to check with the patient if they have any concerns or issues they would
like to discuss in relation to pressure prevention or their pressure care. The Trust’s standardised risk assessments tools and template care plans should be
used when assessing risk and planning care. There are many external factors which predispose a patient to develop a pressure ulcer.
The critical determinants of pressure ulcer formation are the intensity and duration of
pressure, the tolerance of the skin and its supporting structure for pressure, shear and
friction. This includes when patients have received rapid tranquilisation in mental
health. The factors that contribute to pressure ulcer development are divided into two groups:
Extrinsic - external influences that cause skin distortion - pressure, shearing, friction,
continence and moisture.

Pressure Ulcer Policy Version 5
Page 9 of 56
Intrinsic - reduced mobility, previous history of pressure damage, sensory impairment,
reduced level of consciousness, acute illness, chronic long term illness, medication
(analgesics, sedation, anti- inflammatory), pain, cognition, nutrition, extremes of age,
posture, weight, incontinence, dehydration, terminal illness (SCALE Skin Changes at
Lifes End document – see Appendix 1)
Those who are seriously ill, neurologically compromised, i.e. individuals with spinal cord
injuries, have impaired mobility or who are immobile (including those wearing a
prosthesis, body brace or plaster cast), or have contracted limbs or who suffer from
impaired nutrition, obesity, poor posture, or use equipment such as seating or beds
which do not provide appropriate pressure relief are particularly at risk. Older people
and pregnant women are also very vulnerable.
• A risk assessment is to be undertaken by qualified nursing staff using the
Waterlow Pressure Ulcer Risk Assessment Tool (See Appendix 2). Using this
assessment with your clinical judgment, assess the risk and plan care
accordingly. Dates and times of each assessment need to be documented.
• All patients admitted to Community hospitals should have a formal risk
assessment documented within 6 hours of their admission. Domiciliary patients
within the community will have a risk assessment documented in their records
on their 1st visit from the team as part of the holistic initial assessment.
• All patients admitted to the Dementia Assessment Units will have a formal
assessment using the Waterlow within 6 hours of admission, this is in line with
their admission-discharge pathway, and will be recorded and filed within the
green notes in Section 3C. Ongoing review will be dependent on the risk score
(see Appendix 12). The Trust policy will be adhered to in relation to monitoring
and reporting of pressure ulcers.
• Adult Mental Health Inpatient Units. All patients should have a Waterlow
assessment undertaken on admission to the unit and reassessed when the
patient’s condition changes.
• Reassessment timescales of patient’s risk using the Waterlow score should be
weekly for inpatients or more frequently if the patient’s condition deteriorates.
Patients in the community should have the frequency of reassessment clearly
identified and this should be based on the patient’s risk of developing pressure
ulcers. This timescale should not exceed 3 months.
• A pressure ulcer risk assessment should be repeated if there is a change in a
person's clinical status. However, changes in clinical status can be difficult to
define. Specific instances where a reassessment should be carried out to ensure
patient and service user safety have been identified as after a surgical or
interventional procedure in hospital, and after a person's care environment
changes following a transfer in any setting. 6.2 SKIN ASSESSMENT
• The patient’s skin condition should be assessed and recorded within four hours of
admission (hospital) or by the 1st visit (community). If this is not achieved, then the

Pressure Ulcer Policy Version 5
Page 10 of 56
reasons must be clearly documented.
When the Waterlow risk assessment is calculated at 10 or above, the SSKIN
bundle will be implemented (Appendix 3). If clinical judgment overrides initiating
the SSKIN bundle at a Waterlow of 10, reasons for not commencing should be
clearly documented. For Adult Mental Health inpatient units and Dementia
Assessment units, the SSKIN principles are documented in person- centred
documentation and when recording rapid tranquilisation. N.B. Clinical judgment
can also indicate SSKIN needs to be commenced with a Waterlow below 10.
• Examination of skin over bony prominences can reveal the first signs of skin
damage. At this early stage ulceration may be prevented. In a patient who is
recognised as ‘at risk’, skin inspection is part of the ongoing risk assessment
process.
• Skin inspection should occur regularly and the frequency determined in response
to changes in the individual’s condition in relation to either deterioration or
recovery. If a patient is considered at any risk following assessment, then skin
should be inspected for signs of pressure damage at regular intervals. Carers
and patients should be encouraged to participate where necessary, following
appropriate information/ training.
• Skin inspection should be recorded and problems acted upon. Skin inspection
can take place during routine care, taking into account patient consent,
preferences, privacy and dignity. This will be completed at least daily in hospital
• The Care and Comfort checks, carried out on each Community Hospital Ward
will further complement the SSKIN bundle, by encouraging and supporting the
patient to change position.
• Skin inspection should be based on an assessment of the most vulnerable areas
of risk for each patient. These are typically heels, sacrum, ischial tuberosities,
and femoral trochanter. Also at risk are parts of the body affected by anti-embolic
stockings, parts of the body where pressure, friction and shear is exerted in the
course of an individual’s daily living activities and parts of the body where there
are external forces exerted by equipment and clothing - elbows, temporal region
of the skull, shoulders, back of the head and toes (See Figure 1). Other areas
should be inspected as necessitated by the patient’s condition.

Pressure Ulcer Policy Version 5
Page 11 of 56
Figure 1
• Individuals, who are willing and able, should be encouraged, following education,
to inspect their own skin. Any informal education and training provided to the
patient/ family or carer should be recorded and backed up with written patient
information leaflets. These are available to print off from the Trust’s intranet site.
The importance of reporting to the health professional any areas of concern should
be stressed.
• For bariatric patients, maintaining skin integrity is vital. The bariatric patient is at
risk and may sustain pressure damage in unusual sites. A comprehensive
assessment of the patient’s risk factors should be completed and the appropriate
support equipment selected.
• Refusal to allow skin inspection should be documented and the risks fully explained
to the patient, family and carers as appropriate.
• Check for:
1. Persistent erythema i.e. redness over a bony prominence that does not fade
within 2 hours
2. Non-blanching erythema, i.e. persistent area of redness over a bony prominence that does not turn white when light finger pressure is applied
3. Blisters
4. Dusky patches or skin over a bony area which looks bruised
5. Localised heat, localised oedema, localised induration (hardness within the
tissue) or localised coolness if tissue death occurs, may be noted in darker
skin tones.
6. Any areas of pain or discomfort that might be attributed to pressure damage,
especially when using plaster casts / splints. Pain over a bony area may be
a precursor to pressure damage
7. Skin damage which may be caused by medical devices e.g. catheters,
oxygen masks
Record ALL SSKIN Assessments, noting details of any painful areas possibly related to
pressure damage.
6.3 PREVENTING DAMAGE TO THE SKIN.
• When handling patients, all health professionals should take care not to damage
the patient’s skin. Neither rings (other than wedding bands) nor watches should be
worn when turning or repositioning patients, and nails should be kept short and nail
varnish removed. (See Dress Code Policy 2016)
• The skin should be kept well hydrated but excessive washing with alkaline soap
should be avoided. Plain water, soap with a pH of 5.5, or the use of a recognised
soap substitute e.g. Zeroderm
• The patient’s skin should be thoroughly dried using a patting motion, particularly
over vulnerable areas. Do not use a rubbing motion or massage when drying
patients as this causes friction forces and is associated with tissue damage.
• Talcum powder should not be used because of its tendency to ‘cake’, thereby

Pressure Ulcer Policy Version 5
Page 12 of 56
increasing friction, clogging the pores and increasing the risk of infection and skin
damage.
• Drugs such as steroids or anti-cancer drugs which affect skin health increase
patient risk and must be taken into consideration, however it is acknowledged the
benefit may outweigh the risk.
• Examination of skin over bony prominences can reveal the first signs of skin
damage. At this early stage ulceration may be prevented. In a patient who is
recognised as “at risk”, skin inspection is part of the ongoing risk assessment
process. 6.4 EQUIPMENT
• Devices (mattresses and cushions) come in two main types; those that reduce
pressure by spreading the weight and increasing the surface area, and those that
relieve pressure by removing the pressure at frequent intervals.
• Pressure relieving equipment does not replace the need for repositioning and
should be used as an adjunct with a repositioning and skin inspection regime that
suits the patient and circumstances.
• Pressure relieving equipment is accessed in the community through the Equipment/
Loan Store.
• Decisions about support surfaces should be made following a holistic assessment
of a person’s risk, comfort and general health state.
• Patient movement in and out of bed should be considered when considering
equipment provision, as air mattresses can impede transferring.
• Environmental assessment should be undertaken particularly when ordering an
electric profiling bed for community use. There needs to be room for the bed and
an electricity supply / availability of sockets. Operational policies within each
equipment service across Cumbria should be followed in relation to health and
safety requirements
• The Medicines and Healthcare products Regulatory Agency (MHRA) is aware of
fatal domestic house fires starting from lit cigarettes being dropped onto non-fire
retardant bedding covering air mattresses and overlays. For patients at risk (i.e.
Smokers), consider using alternative pressure care equipment and fire retardant
bedding. Ensure patients are aware of the dangers of smoking in bed.
• Assessment should be on-going throughout an individual’s episode of care and the
type of pressure relief support changed to suit any alteration in risk.
• Choice of device should be based on:
- Patient choice
- Risk assessment
- Skin assessment
- General health
- Lifestyle and abilities
- Care needs
Pressure Ulcer Policy Version 5
Page 13 of 56
• All surfaces used by the patient should be considered including bed, armchair,
wheelchair, and toilet.
• Changes of device should reflect changes in risk status.
• Equipment for prevention should be reviewed as part of the risk assessment
process taking into account that equipment can be downgraded as well as
upgraded.
• Patients may choose not to use any therapy products because of their personal
circumstances e.g. those that wish to continue sleeping with their partner in the
community. A double mattress (one side alternating) is available from Community
Health Services Equipment Store. Personal choice should be recorded and
respected and full information about the risks should be given and recorded, re-
evaluated and regular re-assessment dates for follow up agreed and documented.
Foam replacement mattresses/cushions- Pressure Re-distribution
• These consist of several layers of different foams and have a pressure reducing
action because they allow the patient to ‘sink-in’ thereby spreading the pressure
over a greater surface area
• They can be used for patients who are at risk but who are still relatively mobile so
that they can move themselves in bed. High specification foam can be used for
high and very high risk patients also
• They should be cared for according to the manufacturer’s instructions and will
require regular checks to ensure their integrity
• They may also require turning at intervals; this is dependent on individual
manufacturer’s guidance
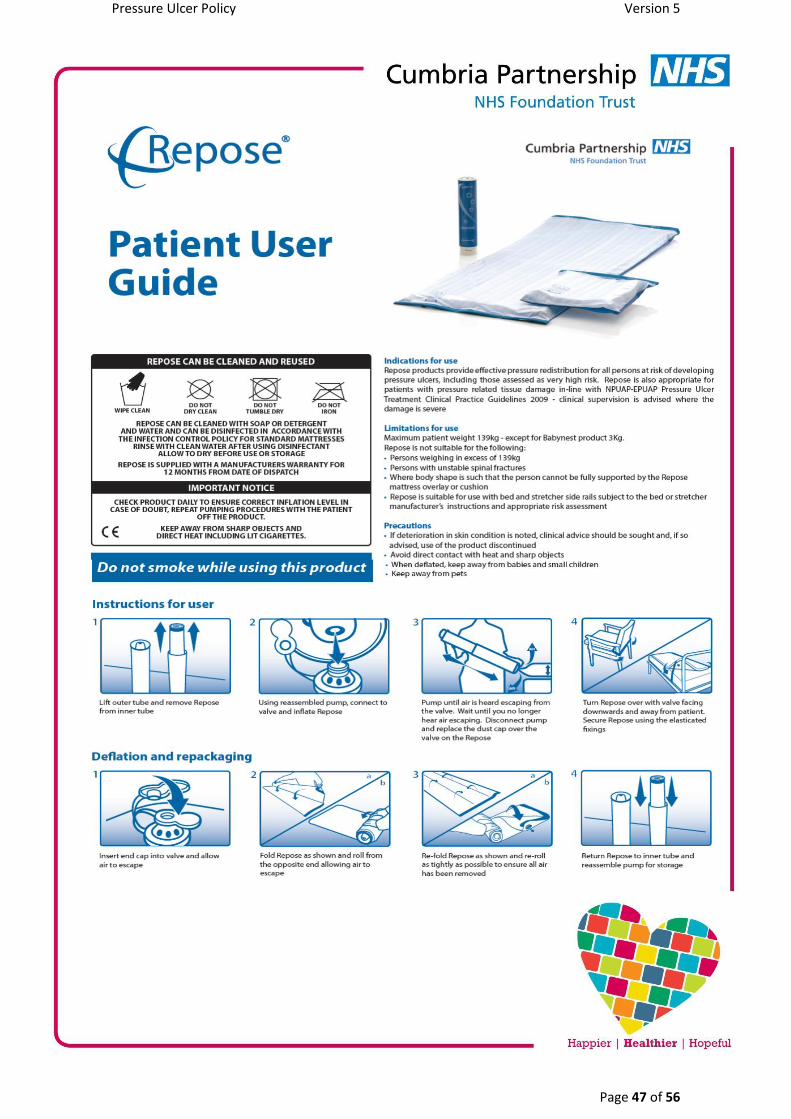
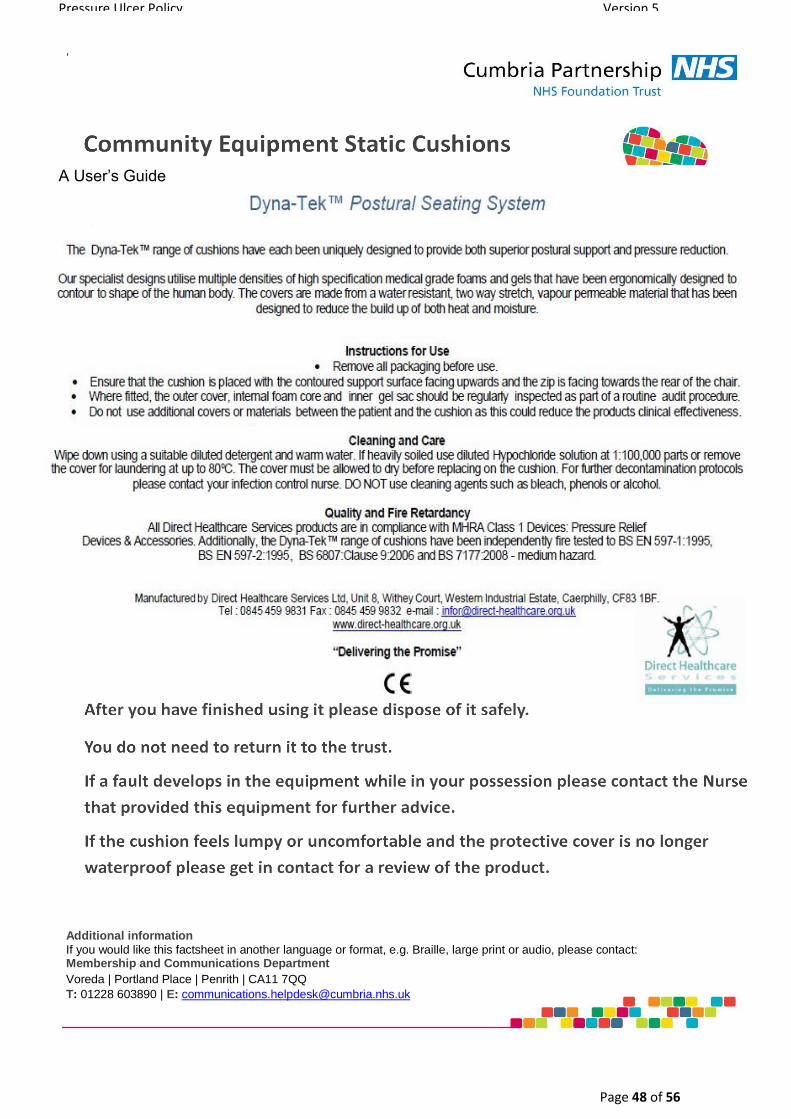
• Please see Standard Operating Procedure and patient user guides in Appendix 13
for discharging patients from caseloads with pressure relieving cushions.
Static air and gel filled mattresses/ cushions
• Air filled devices reduce pressure but may need to be re-inflated at intervals.
• Gel or fluid filled devices also reduce pressure by spreading weight
• Caution should be taken with the use of air filled devices, mattresses, cushions with
patients who cannot maintain or rectify their own posture
Alternating air flow mattresses – Pressure Relieving
• These work on the principle of cyclic inflation and deflation of air cells over a short
period of time. This can be controlled by a dial or by a ‘sensor’ pad which measures
the patient weight and then alternates the amount of pressure to different parts of
the body giving pressure relief
• May lead to an increased risk of falls due to difficulty transferring in and out of bed
for some patients. Raised safety rails are available.
Constant low pressure devices

Pressure Ulcer Policy Version 5
Page 14 of 56
• Low air loss mattresses float the patient on air filled cells while circulating air across
the skin to reduce moisture and help maintain a constant skin interface pressure.
To achieve this, air escapes through small laser cut holes.
• Lateral turn low air loss mattresses constantly rotate the patient from side, to back,
to side to change pressure points. They can be set at ½ hourly, hourly or 2 hourly
intervals. They improve circulation, provide pressure relief, reduce risk of
pulmonary complications and stimulate the gastro-intestinal tract without disturbing
the patient.
• They can be used on individuals who are at very high risk particularly those who cannot tolerate the movement of an alternating product, for patients who are underweight, or palliative patients for comfort.
• Please note, in the event of a power cut, low air loss mattresses will deflate in a
matter of minutes. See Appendix 14 for the risk assessment which must be
completed for all community patients placed on this type of mattress.
Electric profiling beds Electric profiling beds reduce skin damage by:
• Making patient movement easier for the patient, carers and staff, so reducing
friction and shear.
• Use of the knee break prevents sliding down the bed reducing friction and shear
forces and reduces the pressure and weight exerted on the heel.
• Allowing patients to change their own position. In relation to discharge planning, it is vital that an environmental check is carried out prior
to discharge to ensure space is available, as these beds are larger than a standard divan
and require room to ‘move.’
If the risk to the patient is from shear and friction, then a high risk foam mattress may be
as effective as an alternating mattress.
Other equipment
• Friction and shear can be minimised with the use of a slide sheet.
• Manual handling risk assessment should inform the pressure ulcer prevention care
planning process and any identified needs addressed with relevant equipment
provision e.g. hoist.
• If the patient’s needs are not met by the standard equipment carried by the
Equipment / Loan store, please contact the Tissue Viability Nurse for alternative
options. 6.5 SAFE USE OF EQUIPMENT
• Ensure the mattress does not elevate the patient to an unsafe height in relation
to side rails.
• Ensure the patient is within the recommended weight range for the equipment
(both upper and lower ranges).
• When dynamic equipment is being used, regular checks to ensure the settings
remain correct for the patient, and the system is functioning correctly, must be

Pressure Ulcer Policy Version 5
Page 15 of 56
made. All equipment should be cancelled and returned to the equipment store as soon as it is
finished with for decontamination and maintenance.
If Pressure relieving equipment provided becomes the patient’s property (i.e pressure
relieving cushions), see Appendix 13 - ‘Standard Operating Procedure for Discharging
patients from District Nursing Caseload with pressure relieving equipment’ for guidelines
for safe discharge. REMEMBER: When re-assessing patient’s risk – think ‘does this patient still require
this equipment?’
As some patients can deteriorate very quickly, nurses need to assess, reassess and
access the resources available to support the patient and their condition. When there is
a risk of harm to patients, safeguarding should be considered and clear documentation of
concerns is paramount. If there are any clinical concerns which require medical
reassessment, urgently refer to GP. 6.6 POSITIONING
• Where possible patients should be taught to reposition themselves and redistribute
their weight and carers should be shown how to assist.
• If a person is unable to reposition themselves, health and social care professionals
should help them to change their position, to prevent the development of pressure
ulcers. For some people, repositioning equipment may be needed.
• Patients who are ‘at risk’ of pressure damage or have pressure damage, should be
repositioned and the frequency of repositioning determined by the results of skin
inspection and individual needs, not by a ritualistic schedule (NICE 2014, Moore et
al, 2011).
• Repositioning is recommended at least every 6 hours for adults at risk, and at least
every 4 hours for adults at high risk.
• Repositioning should take into consideration other relevant matters, including the
patient’s medical condition, their comfort, the overall plan of care, the support
surface and attendance of formal and informal carers.
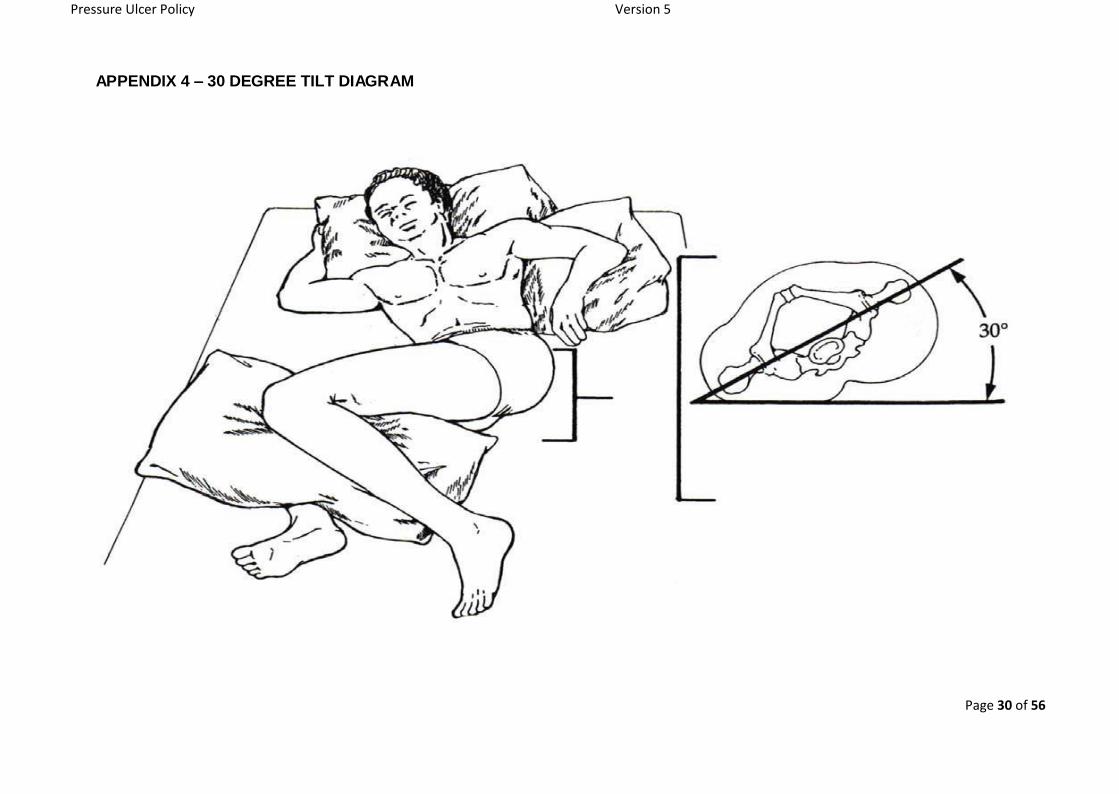
• Patients should be positioned in such a way as to minimise the impact on bony
prominences (e.g. 30° tilt) and any pressure damage (Appendix 4) Tilting the
patient 30º and placing a pillow in the small of the back to relieve pressure on the
sacrum and ischial tuberosities can be effective. Pillows can also be used
lengthways along the calf to raise the heels, protecting them from the surface below.
• Patients should be positioned appropriately to reduce the effect of shear and friction
forces. The use of an electronic profiling bed can assist in repositioning without
turning. Reduce shear factors by maintaining the head position at the lowest
position possible. The use of the knee break will also help to reduce heel pressure.
• A re-positioning schedule should be agreed with the patient and documented. A
repositioning chart (Appendix 5) will be used as deemed necessary for individual
patients.

Pressure Ulcer Policy Version 5
Page 16 of 56
• When repositioning a patient, staff should note any area of redness. Please refer
to the Red Bottom flow chart in Appendix 6.
• Refusal or difficulties to reposition should be recorded; it may not always be
possible to reposition patients because of their medical condition; patients are
within their rights to refuse care, however the reasons for this should be determined
and must be documented. Issues such as pain management should be addressed
to increase the likelihood of concordance. Staff must state what exactly has been
advised, and the potential risks of declining care. A re-assessment date must be
defined and agreed.
• Patient, carers and health staff should be aware of the importance of repositioning
- Is carer support available? Can the carer turn the patient safely? - Where a schedule is used, carers should be encouraged to complete
documentation where necessary. - In the community, carers and patients should be taught about the equipment
that is being used.
6.7 SEATING
• For patients who spend significant periods of time seated, an assessment of their
seating is as important as an assessment of their bed. This includes patients in a
mental health setting who may experience a reduction in their normal mobility.
• Seating and sitting position should be assessed by a trained assessor taking into
account the time a patient will spend seated, their ability to relieve their own
pressure, the height, depth and condition of the chair.
• Advice should be sought from the multidisciplinary team (occupational therapists,
physiotherapists, wheelchair services) if seating is a problem, and referral made to
the relevant local service if appropriate. Patients ‘at risk’ from pressure damage, who cannot relieve their own pressure
independently, should restrict chair sitting to a maximum of 2 hours at any one time. EPUAP 2014 recommends that patients with existing pressure damage to seating area,
sit out for no more than 1 hour three times a day irrespective of category or type of
equipment in use Pressure redistribution cushions should be considered. When patients are sitting out
ensure:
• The patient should be able to sit with their bottom right at the back of the seat and
their feet flat on the floor
• The patient’s thighs should be level and their lower legs at 90°
• The patient should be able to get two fingers between their knees and the front of
the seat.
• The seat should be wide enough to fit the patient, but not so wide that it doesn’t
give them any sideways support. If it has arm rests, the patient should be able to
Pressure Ulcer Policy Version 5
Page 17 of 56
sit between them with enough room to get their hand in on each side.
• Repositioning charts apply to patients sitting out in chairs. Monitor how long
patients are sat out. Patients should be stood, mobilised, transferred out of chair
(or reclined in chair if possible) as per repositioning chart. 6.8 HEEL PROTECTION
The incidence of pressure ulcers on the heels is high and needs careful, consideration
and management as they can lead to prolonged intervention, amputation, infection and
death. The shape of the heel makes it more difficult to reduce pressure as the calcaneus
bone has a pointed shape with very little subcutaneous fat, therefore ‘total off-loading’ is
recommended to lift the heel directly off the bed, footstool etc. This is preferable and more
effective than any dynamic air mattress. Prevention of heel pressure
Patients should be encouraged to mobilise and wear good fitting footwear.
When patients are in bed or elevating the legs, the heels should be ‘free – floating’ (Black
2013).This can be achieved by the use of:
• heel lifts
• heel protectors
• troughs
• pillows placed lengthways The patient should be informed of the need and frequency to remove any compression or
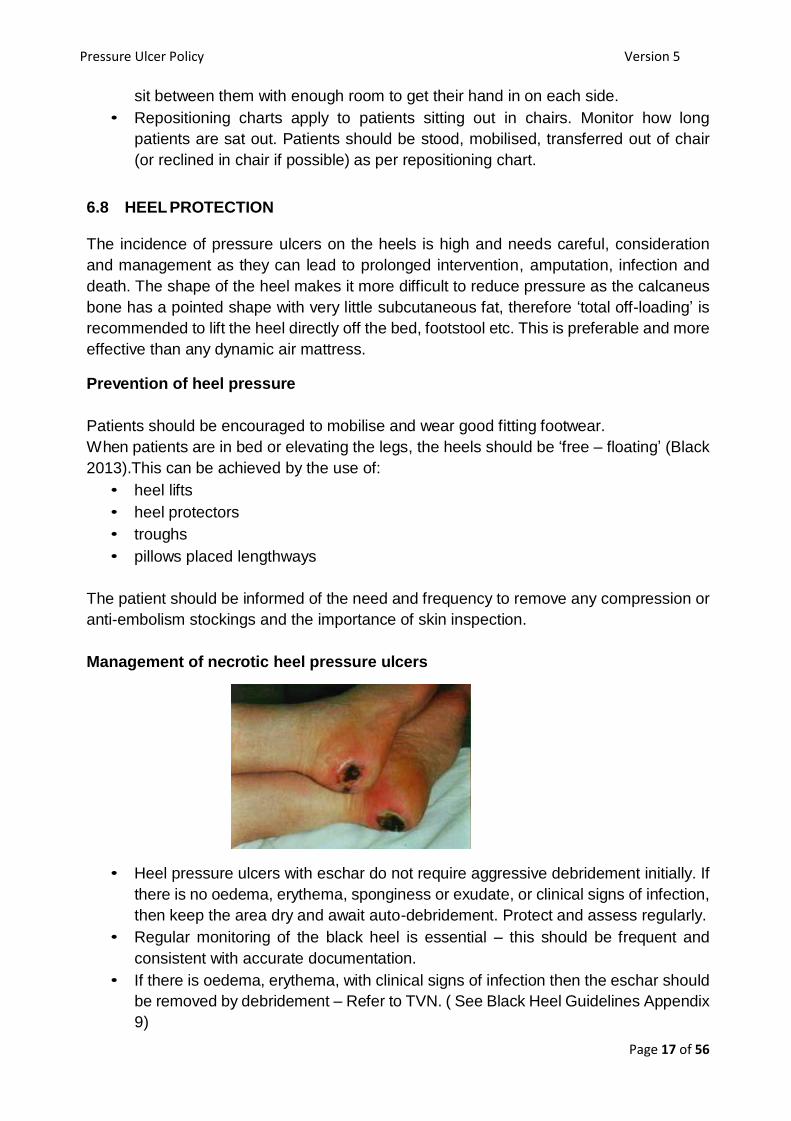
anti-embolism stockings and the importance of skin inspection. Management of necrotic heel pressure ulcers
• Heel pressure ulcers with eschar do not require aggressive debridement initially. If
there is no oedema, erythema, sponginess or exudate, or clinical signs of infection,
then keep the area dry and await auto-debridement. Protect and assess regularly.
• Regular monitoring of the black heel is essential – this should be frequent and
consistent with accurate documentation.
• If there is oedema, erythema, with clinical signs of infection then the eschar should
be removed by debridement – Refer to TVN. ( See Black Heel Guidelines Appendix
9)

Pressure Ulcer Policy Version 5
Page 18 of 56
• An ankle brachial pressure index (ABPI) should be performed on all patients with
black heels to determine if there is any arterial insufficiency.
6.9 NUTRITION
It is widely agreed that impaired nutrition and hydration will influence tissue vulnerability
to pressure and shear.
Individuals at risk of malnutrition:
• Elderly, children, chronic illness, neurological disorders, post-surgery, HIV/AIDS,
psychiatric, physical disabilities, learning difficulties, inflammatory bowel disease,
critical care needs.
To prevent occurrence of pressure ulcers we must:
• Provide nutritional support to patients with an identified deficiency
• Base decisions on nutritional assessment via a recognised tool. MUST assessment is to be completed at initial assessment and reviewed as per guidelines.
6.10 INCONTINENCE
• Wet skin is more prone to damage and requires extra care.
• Assess the patient and develop a plan of care
• Advice can be sought from the Continence Service (acute) or the Bladder and
Bowel Team (community) re management of incontinence.
• Skin barriers should be considered for prevention such as Sorbaderm non- sting
barrier film, silicon based product which covers and protects the skin.
• The diagnosis of the existence of a pressure ulcer is more difficult than one
commonly assumes. There can be confusion between a pressure ulcer and a
moisture lesion caused by the presence of sweat, urine / faeces. The differentiation
between the two is of clinical importance since prevention and treatment
strategies differ (EPUAP 2005). Appendix 7 tables the different characteristics of
pressure ulcers and moisture lesions.
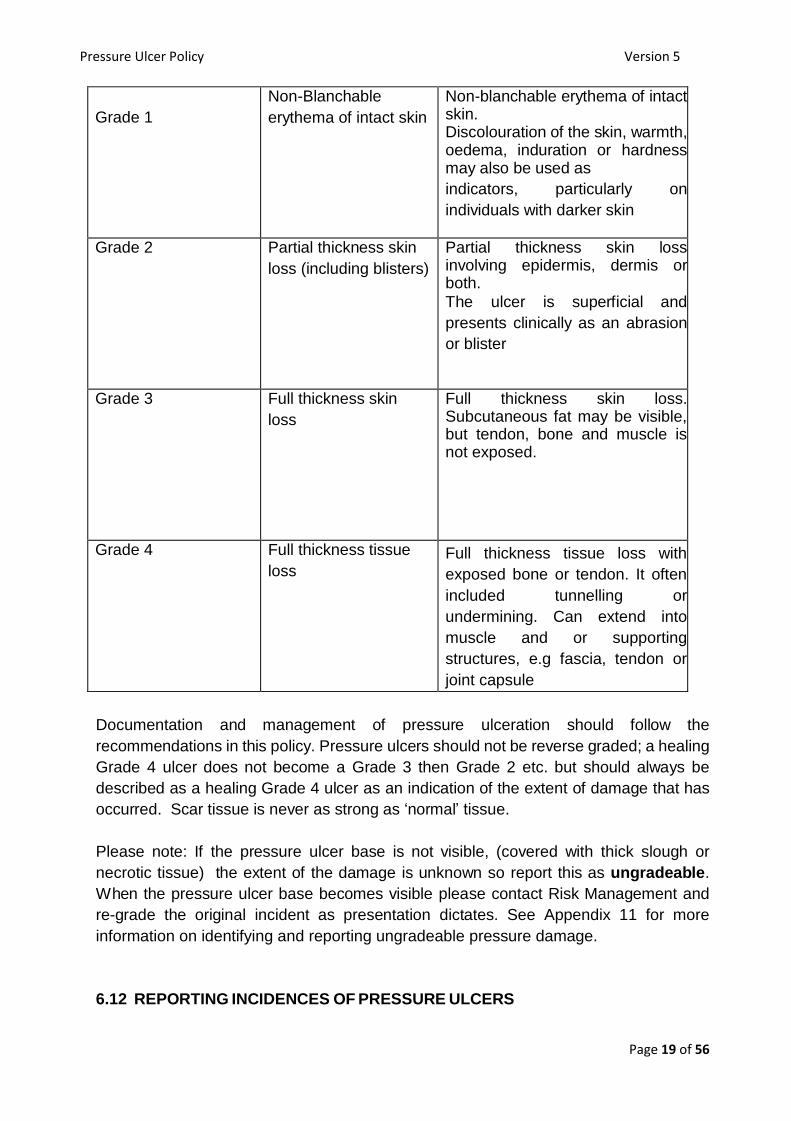
6.11 GRADING PRESSURE ULCERS.
Any area of persistent redness should be recorded including site and size. Pressure
ulcers will be categorised using the following system: See Appendix 8 for EPUAP guide
of pressure ulcer classification.
Grade Short description Definition
Pressure Ulcer Policy Version 5
Page 19 of 56
Grade 1
Non-Blanchable
erythema of intact skin
Non-blanchable erythema of intact skin. Discolouration of the skin, warmth, oedema, induration or hardness may also be used as
indicators, particularly on
individuals with darker skin
Grade 2 Partial thickness skin
loss (including blisters)
Partial thickness skin loss involving epidermis, dermis or both.
The ulcer is superficial and
presents clinically as an abrasion
or blister
Grade 3 Full thickness skin
loss
Full thickness skin loss. Subcutaneous fat may be visible, but tendon, bone and muscle is not exposed.
Grade 4 Full thickness tissue
loss Full thickness tissue loss with
exposed bone or tendon. It often
included tunnelling or
undermining. Can extend into
muscle and or supporting
structures, e.g fascia, tendon or
joint capsule
Documentation and management of pressure ulceration should follow the
recommendations in this policy. Pressure ulcers should not be reverse graded; a healing
Grade 4 ulcer does not become a Grade 3 then Grade 2 etc. but should always be
described as a healing Grade 4 ulcer as an indication of the extent of damage that has
occurred. Scar tissue is never as strong as ‘normal’ tissue.
Please note: If the pressure ulcer base is not visible, (covered with thick slough or
necrotic tissue) the extent of the damage is unknown so report this as ungradeable.
When the pressure ulcer base becomes visible please contact Risk Management and
re-grade the original incident as presentation dictates. See Appendix 11 for more
information on identifying and reporting ungradeable pressure damage.
6.12 REPORTING INCIDENCES OF PRESSURE ULCERS

Pressure Ulcer Policy Version 5
Page 20 of 56
• Identify pressure ulcer in clinical setting and complete electronic incident report
(IR1).
• If a patient is admitted into our service with a documented pressure ulcer on
handover, an incident form does not need to be completed, unless other concerns
are identified. If the pressure ulcer is not documented upon handover to our service,
an incident form should be completed (see Appendix 10).
• If a pressure ulcer increases in Grade (from a Grade 1 to a Grade 2, or Grade 2 to
Grade 3 etc.) another Incident form is to be completed, reporting the highest grade
of pressure damage.
• Grade 1 or 2 completed correctly, are signed off by Team Leader.
• For all Grade 3 or 4 acquired in our care, a 72 hour report is initiated within the
team, with the TVN or Professional Lead. Those which develop into a SIRI (Serious
Incident Requiring Investigation) are reported to STEIS by the investigations team.
• The 72 hour report is completed along with an action plan and is presented at the
Quality and Safety / TVN Group.
• Team Leaders are responsible for local actions resulting from the 72 hour report to
be implemented.
• Themes and lessons learned from completed 72 hour reports are communicated
quarterly (see Appendix 10.4).
6.13 PRESSURE ULCER WOUND ASSESSMENT AND TREATMENT.
• Assessment of the patient with a pressure ulcer should include an examination of
the intrinsic and extrinsic factors, plus an assessment of the wound.
• Factors that may affect wound healing should be recorded
• Possible reasons for occurrence can be recorded
• Removal of any recognised cause should form part of the care plan
• Dressing selection should follow a comprehensive assessment as presented in the
Wound Dressings Formulary
• Specialist advice can be sought from the Tissue Viability Services. Please refer ALL patients with multiple Grade 2 pressure ulcers, or Grade 3 or 4 ulcers to the Tissue Viability Nurses.
• On discharge from the hospital, the patient should be given a 7 day supply of
primary and secondary dressings, tapes and bandages (where applicable) to
ensure continuity of pressure ulcer management. If specialist dressings are being
used e.g. topical negative pressure therapy, then discussion with the appropriate
District Nurse team will be required prior to the patients discharge. 48 hours’ notice
is required and a spare canister and wound sealing kits must be supplied upon
discharge.
• If the patient has received ongoing care for a pressure ulcer in the community and
is being admitted into hospital, every effort should be made by the Named Nurse
and District Nurse to discuss previous treatment and care of the pressure ulcer to
ensure continuity of care, where appropriate.
• If a pressure ulcer is non-healing, osteomyelitis should be considered.
Radiography (X-ray / MRI scan) should be considered in discussion with other

Pressure Ulcer Policy Version 5
Page 21 of 56
health professionals (GP, Consultant).
• Treatment for pressure ulcers to heels should be treated as outlined in the
Guidance for Management of Black Heels in Appendix 9. 6.14 MONITORING OF PRESSURE ULCERS
The presence or absence of pressure ulcers is often seen as an indicator of quality of
care. Incidence and prevalence are the two ways to measure pressure ulcer frequency. Prevalence
• Is the proportion of people in a given population with a pressure ulcer, or who have
had an ulcer in a defined period of time
• Prevalence is affected by people admitted to caseloads who have existing ulcers,
patient healing rates, rates of successful treatment and availability of preventative
equipment Incidence
• Is the proportion of people in a given population who develop a pressure ulcer in a
given time period
• Incidence is affected by the risk status of the given population and the availability
of equipment and staff to provide preventative care Local monitoring
Pressure ulcers should be documented as a local clinical incident
• Overall prevalence and incidence rates will be monitored
• Grade 1 and above pressure ulcers are to be reported.
• Information will be used to improve patient care i.e. through future training sessions
etc. 6.15 PATIENT / CARER EDUCATION
• Education for the prevention of pressure damage should be made available to
patients and family or caregivers. The education for prevention of pressure damage
should include information on risk factors, principles of pressure reduction,
positioning and use of prescribed equipment.
• Patients and caregivers should be involved in all aspects of pressure ulcer
prevention and management, to assist then in making informed choices regarding
care.
• All patients and carers should be given the information leaflet ‘Preventing Pressure
Ulcers’ produced by the Tissue Viability Team and available on the Trust intranet
site.
6.16 SAFEGUARDING
Skin damage has a number of causes, some relating to the individual patient, such as
poor medical condition and others relating to external factors such as poor nursing care,

Pressure Ulcer Policy Version 5
Page 22 of 56
lack of resources, e.g. equipment, staffing. It is recognised that not all skin damage can
be prevented and therefore the risk factors in each case should be reviewed on an
individual basis before a safeguarding referral is considered. Not all pressure ulcers in
vulnerable adults are the result of neglect but this factor must be considered. If there are
concerns that observed pressure damage may be the result of neglect or omissions of
care, please refer to Safeguarding team / Adult Social Care. (See Local Authority
published ‘Safeguarding Adults at Risk. A Cumbria Partnership Guidance Paper 5,
Pressure Ulcers, December 2015’).
7 TRAINING
• All members of the health care team should receive training on the principles of
pressure ulcer prevention targeted to their role. Locally this will be provided by the
Tissue Viability Nurse and the Learning and Development Team.
• Formal training should be cascaded between teams.
• This will also be included in PMVA training and rapid tranquilisation training.
8 MONITORING COMPLIANCE WITH THIS DOCUMENT
The table below outlines the Trusts’ monitoring arrangements for this policy/document. The Trust reserves the right to commission additional work or change the monitoring arrangements to meet organisational needs.
Aspect of compliance or effectiveness being monitored
Monitoring method
Individual responsible for the monitoring
Frequency of the monitoring activity
Group / committee which will receive the findings / monitoring report
Group / committee / individual responsible for ensuring that the actions are completed Reporting of
Pressure Ulcers
Ulysses Safety Thermometer
Quality and Safety Manager
Monthly Corporate Clinical Governance Group - Quarterly
Corporate Clinical Governance Group - Quarterly
72 hour reports are completed for all Grade 3 and 4 pressure ulcers acquired within our care.
72 hour report Data Base
Quality and Safety Managers
Monthly Care Group Clinical Governance Group
Care Group Clinical Governance Group
Pressure Ulcer Policy Version 5
Page 23 of 56
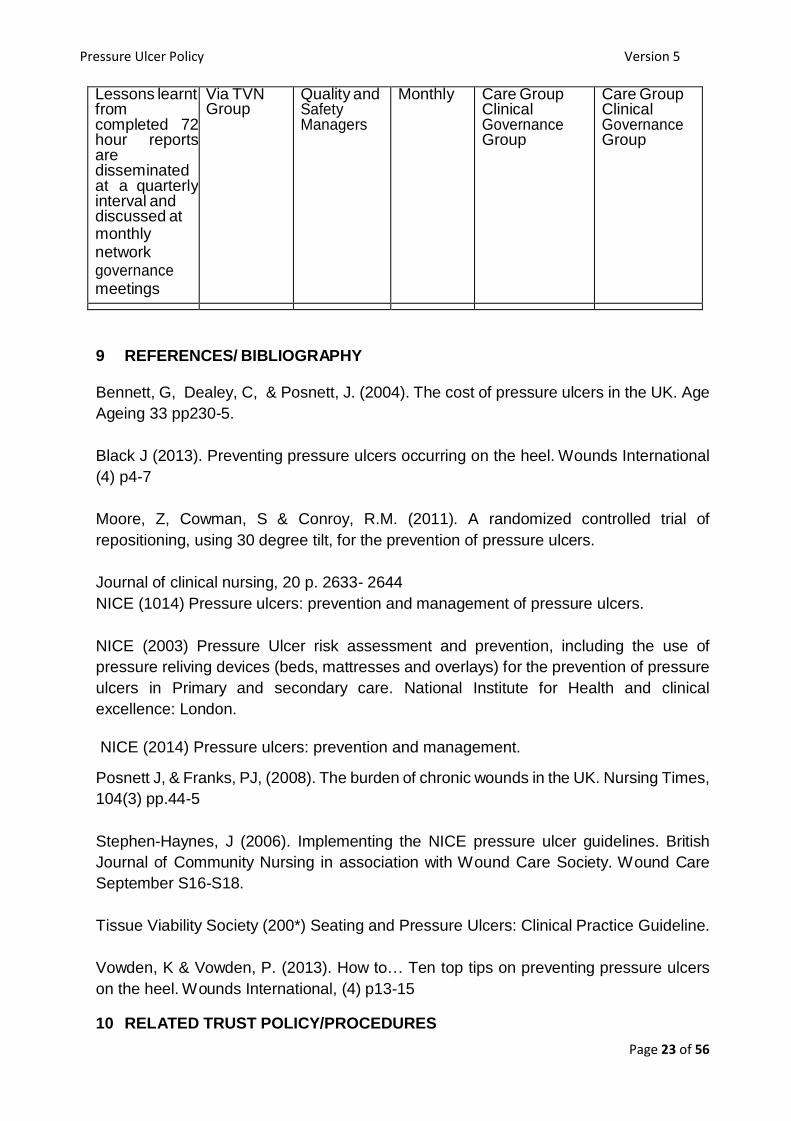
Lessons learnt from completed 72 hour reports are disseminated at a quarterly interval and discussed at monthly network governance meetings
Via TVN Group
Quality and Safety Managers
Monthly Care Group Clinical Governance Group
Care Group Clinical Governance Group
9 REFERENCES/ BIBLIOGRAPHY
Bennett, G, Dealey, C, & Posnett, J. (2004). The cost of pressure ulcers in the UK. Age
Ageing 33 pp230-5.
Black J (2013). Preventing pressure ulcers occurring on the heel. Wounds International
(4) p4-7
Moore, Z, Cowman, S & Conroy, R.M. (2011). A randomized controlled trial of
repositioning, using 30 degree tilt, for the prevention of pressure ulcers.
Journal of clinical nursing, 20 p. 2633- 2644
NICE (1014) Pressure ulcers: prevention and management of pressure ulcers.
NICE (2003) Pressure Ulcer risk assessment and prevention, including the use of
pressure reliving devices (beds, mattresses and overlays) for the prevention of pressure
ulcers in Primary and secondary care. National Institute for Health and clinical
excellence: London.
NICE (2014) Pressure ulcers: prevention and management.
Posnett J, & Franks, PJ, (2008). The burden of chronic wounds in the UK. Nursing Times,
104(3) pp.44-5
Stephen-Haynes, J (2006). Implementing the NICE pressure ulcer guidelines. British
Journal of Community Nursing in association with Wound Care Society. Wound Care
September S16-S18.
Tissue Viability Society (200*) Seating and Pressure Ulcers: Clinical Practice Guideline.
Vowden, K & Vowden, P. (2013). How to… Ten top tips on preventing pressure ulcers
on the heel. Wounds International, (4) p13-15
10 RELATED TRUST POLICY/PROCEDURES

Pressure Ulcer Policy Version 5
Page 24 of 56
Dress Code Policy 2013
Safeguarding Adults at Risk.
A Cumbria Partnership Guidance Paper 5 Pressure Ulcers, December 2015 Policy. Rapid Tranquilisation Policy

NHS Confidential please file within patient held record along with your current location tracer
25
APPENDIX 1 – SCALE ABSTRACT
SCALEAbstractStatements2009.pdf

Pressure Ulcer Policy Version 5
Page 26 of 56
APPENDIX 2 – WATERLOW PRESSURE ULCER PREVENTION/TREATMENT TOOL
N.B. Several scores per category can be used
Forenames: Surnames
Address:
NHS Number:
CHI Number: DOB:
Date
Date
Date
Date
Date
Date
Build/weight for height Average BMI 20-24.9 0 0 0 0 0 0
Above Average BMI 25-29.9 1 1 1 1 1 1
Obese BMI > 30 2 2 2 2 2 2
Below Average BMI < 20 3 3 3 3 3 3
Continence Complete/catheterised 0 0 0 0 0 0
Urine Incontinence 1 1 1 1 1 1
Faecal incontinence 2 2 2 2 2 2
Urinary and faecal incontinence 3 3 3 3 3 3
Skin Type Healthy 0 0 0 0 0 0
Tissue Paper 1 1 1 1 1 1
Dry 1 1 1 1 1 1
Oedematous 1 1 1 1 1 1
Clammy, pyrexia 1 1 1 1 1 1
Discoloured Grade 1 2 2 2 2 2 2
Broken/spots Grade 2 - 4 3 3 3 3 3 3
Mobility Fully 0 0 0 0 0 0
Restless/Fidgety 1 1 1 1 1 1
Apathetic 2 2 2 2 2 2
Restricted 3 3 3 3 3 3
Bedbound e.g. traction 4 4 4 4 4 4
Chair bound e.g. Wheelchair 5 5 5 5 5 5
Sex/Age Male 1 1 1 1 1 1
Female 2 2 2 2 2 2
14 – 49 1 1 1 1 1 1
50 – 64 2 2 2 2 2 2
65 – 74 3 3 3 3 3 3
75 – 80 4 4 4 4 4 4
81 + 5 5 5 5 5 5
Appetite Appetite Average 0 0 0 0 0 0
Appetite Poor 1 1 1 1 1 1
Weight loss 0.5-5kg 1 1 1 1 1 1
Weight loss 5-10kg 2 2 2 2 2 2
Weight loss 10-15kg 3 3 3 3 3 3
Tissue Malnutrition Terminal Cachexia 8 8 8 8 8 8
Multiple organ failure 8 8 8 8 8 8
Single organ failure (respiratory, renal, cardiac) 5 5 5 5 5 5
Peripheral Vascular Disease 5 5 5 5 5 5
Anaemia 2 2 2 2 2 2
Smoking 1 1 1 1 1 1
Neurological Deficit Diabetes, Multiple Sclerosis, CVA, 4-6 4-6 4-6 4-6 4-6 4-6
Motor/Sensory 4-6 4-6 4-6 4-6 4-6 4-6
Paraplegia (Max of 6) 4-6 4-6 4-6 4-6 4-6 4-6
Major Surgery/Trauma Orthopaedic – Below waist/spinal 5 5 5 5 5 5
On table > 2 hrs (score discounted 48hr post op if patient recovering normally) 5 5 5 5 5 5
On table >6 hrs (score discounted 48h post op if patient recovering normally 8 8 8 8 8 8
Medication Cytotoxics/High dose or long term Steroids/Anti-Inflammatory Max 4
Max 4
Max 4
Max 4
Max 4
Max 4
Assessment Tool No

Pressure Ulcer Policy Version 5
Page 27 of 56
Score 10 + At Risk; 15 + High Risk; 20+Very High Risk
Score
Pressure Ulcer Policy Version 5
Pressure Ulcer Pag 27 of 4 3 P OL/ 0 1/06 9
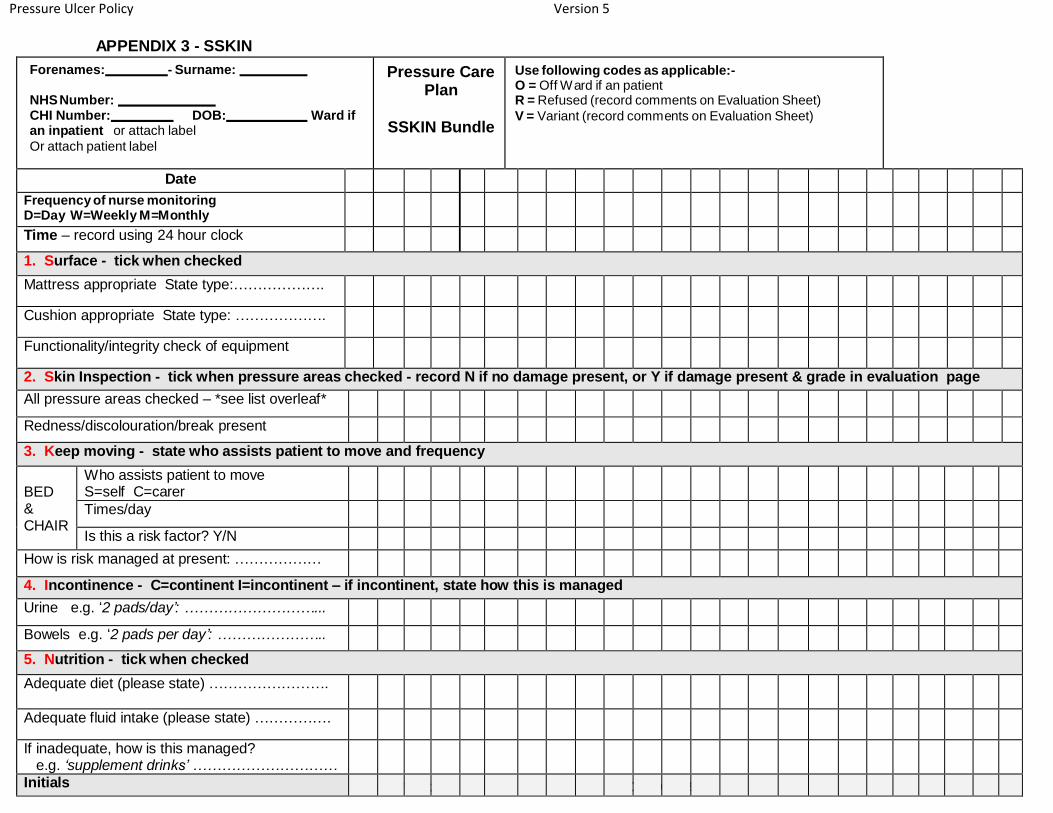
APPENDIX 3 - SSKIN
Forenames: - Surname:
NHS Number: CHI Number: DOB: Ward if an inpatient or attach label
Or attach patient label
Pressure Care Plan
SSKIN Bundle
Use following codes as applicable:- O = Off Ward if an patient R = Refused (record comments on Evaluation Sheet)
V = Variant (record comments on Evaluation Sheet)
Date
Frequency of nurse monitoring D=Day W=Weekly M=Monthly
Time – record using 24 hour clock
1. Surface - tick when checked
Mattress appropriate State type:……………….
Cushion appropriate State type: ……………….
Functionality/integrity check of equipment
2. Skin Inspection - tick when pressure areas checked - record N if no damage present, or Y if damage present & grade in evaluation page
All pressure areas checked – *see list overleaf*
Redness/discolouration/break present
3. Keep moving - state who assists patient to move and frequency
BED & CHAIR
Who assists patient to move S=self C=carer
Times/day
Is this a risk factor? Y/N
How is risk managed at present: ………………
4. Incontinence - C=continent I=incontinent – if incontinent, state how this is managed
Urine e.g. ‘2 pads/day’: ………………………...
Bowels e.g. ‘2 pads per day’: …………………..
5. Nutrition - tick when checked
Adequate diet (please state) …………………….
Adequate fluid intake (please state) …………….
If inadequate, how is this managed? e.g. ‘supplement drinks’ …………………………
Initials
Pressure Ulcer Policy Version 5
Page 29 of 56
For example, if you are bed bound, you are at risk of developing pressure ulcers on:
your shoulders, or shoulder blades,
your elbows,
the back of your head,
the rims of your ears,
your knees, ankles, heels, or toes,
your lower back, or hipbone,
the genitals (in men), and
the breasts (in women).
If you are a wheelchair user, you are at risk of developing pressure ulcers on:
your buttocks,
your tailbone (the small bone at the bottom of your spine),
your spine,
your shoulder blades, and
the back of your arms and legs.
Pressure Ulcer Policy Version 5
Page 30 of 56
APPENDIX 4 – 30 DEGREE TILT DIAGRAM

Pressure Ulcer Policy Version 5
Page 31 of 56
APPENDIX 5 – REPOSITIONING CHART
Frequency of repositioning………….. Date Advised. ……….By…………………………………
Daily Repositioning & Skin Inspection Chart
Date: / /
• Inspect skin for evidence of change
• Reassess at every positional change and document below
• Reposition the patient/ client to reduce the risk of further damage, e.g. using the 30 degree tilt
• Use manual handling aids to minimise risk of friction and shear
• Patients/ clients on any form of pressure redistribution equipment still require skin inspection and regular repositioning
• Provide suitable seating including pressure redistribution cushions, if required, encourage repositioning/mobilisation where possible
• Acutely ill patients/ clients are seated out for no longer than 2 hours and returned to bed for no less than 1 hour
Time Repositioning
(Using Codes) From To
Skin Inspection Comments
Action Taken Signature
E.g.: 08.00
L U Left Hip Non- Blanching Reassess at next positional change
Code: L = left, R = right, B = back, P = prone (front), M = mobilised, U = up to sit

Pressure Ulcer Policy Version 5
Page 32 of 56
Time Repositioning
(Using Codes) From To
Skin Inspection Comments
Action Taken Signature
Code: L = left, R = right, B = back, P = prone (front), M = mobilised, U = up to sit

Pressure Ulcer Policy Version 5
Page 33 of 56
APPENDIX 6 – RED BOTTOM CHART

Pressure Ulcer Policy Version 5
Page 34 of 56
APPENDIX 7 – MOISURE LESIONS V PRESSURE DAMAGE

Pressure Ulcer Policy Version 5
Page 35 of 56
.
APPENDIX 8 – EUPAP GRADING
European Pressure Ulcer Advisory Panel (EPUAP) Grading Tool Grade 1 Non-blanchable erythema of intact skin. Discolouration of the skin, warmth, oedema, induration or hardness may also be used as indicators, particularly on individuals with darker skin.
Grade 2 Partial thickness skin loss involving epidermis, dermis, or both. The ulcer is superficial and presents clinically as an abrasion or blister.
Grade 3 Full thickness skin loss involving damage necrosis of subcutaneous tissue that may extend down to, but not through, underlying fascia.
Grade 4 Extensive destruction, tissue necrosis, or damage to muscle, bone, or supporting structures with or without full thickness skin loss.
Moisture Lesions
A lesion limited to the
anal cleft only and has Kissing Ulcer is most a linear shape is most likely a moisture lesion likely to be a moisture lesion.
Pressure Ulcer Page 35 of 43 POL/001/069

Pressure Ulcer Policy Version 5
Page 36 of 56
APPENDIX 9 – BLACK HEEL POLICY
Guidelines for the Management of Black Heels
This guideline should be read in conjunction with the Trust Guidelines for the Prevention and management of Pressure Ulcers. Black heels should, where possible, be managed using a multidisciplinary approach and by the development of an agreed plan which can be formulated, implemented and reviewed accordingly Definition: An area of ‘black’ necrotic eschar or ‘shell’ on the heel Assessment Black heels should be uniformly described to facilitate communication amongst staff and to accurately monitor progress or deterioration of the lesion. To ensure this the clinician should describe the location and history of the wound, which should be accurately measures and the type/s of tissue present observed. All information should be recorded on the Wound Assessment sheet.
Management
1. Relief of pressure and/or shear: correct moving and handling is essential:
glide sheets should be used and must be long enough to incorporates the
heels in the manoeuvre
2. Debridement: Heel wounds which have dry eschar and no oedema, on
erythema or fluctulance (sponginess), DO NOT require aggressive
intervention (i.e. any dressings) but continuous assessment is essential as
the management plan may change.
If there is oedema, fluctulance or drainage, then the eschar should be removed, as this necrotic tissue will provide an optimal environment for bacterial growth. There are several methods of wound debridement available and the wound may appear larger after debridement. The clinician should select the method which is most suitable to the patient’s needs and their own scope of professional practice.
3. Sharp Debridement: Sharp debridement is the method of removing thick
adherent, devitalised tissue. Where there are signs of advancing cellulitis of
sepsis, rapid debridement is imperative and should only be carried out by an
experienced practitioner. Those who perform sharp debridement should
have the necessary clinical skills, underpinned by the successful completion
of Sharp Debridement training, and these skills must be within the
practitioner’s scope of practice
4. Other debridement methods: These methods include hydrogels, honey
and/or larvae dependent on the needs of the patient

Pressure Ulcer Policy Version 5
Page 37 of 56
5. Infection: All black heels will be colonised with bacteria but are not
necessarily clinically infected. If bone is exposed or can be probed, an x-ray
should be performed where possible to rule out osteomyelitis
6. Dressing selection: Dressing choice will depend upon
The type and condition of the underlying tissues
The level of exudate Odour Condition of the surrounding skin Depth of wound
Reassessment Regular monitoring of the black heel is essential- this should be a frequent and consistent process, with accurate documentation. Deterioration in the patient’s physical condition will also be influential. A black heel with adequate sensation and vascular supply should show evidence of improvement within 2-4 weeks. Whilst healing is the preferred goal, there are cases, for example in the terminally ill, where the maintenance of comfort is the more realistic or appropriate goal.
Acknowledgement This guideline has been developed by Fania Pagnamenta, Nurse Consultant In Tissue Viability at Newcastle upon Tyne Acute Hospitals NHS Foundation Trust and is used with her kind permission. These guidelines have been reviewed by Cumbria Tissue Viability Team 2017.
References Blaszczky J, Majewski M, Sato F (1998) Make a difference: standardise your health care practice. Ostomy/wound management 44(5), 32-40
Burdette-Taylor SR, Kass J, (2002) Heel ulcers in Critical Care Units: a major pressure problem. Critical Care Nursing Quarterly 25(2), 41-53 Cock KA (2006) Anti-embolism stockings: are they used effectively and correctly? British Journal of Nursing (suppl.) 15(6) - s12. Donnelly J (2001) Hospital-acquired heel ulcers: a common but neglected problem. Journal of Wound Care 10(4), 131-136 Nixon J, Thorpe H, Barrow H, Phillips A, Nelson EA, Mason SA, Cullum N (2005) Reliability of Pressure ulcer classification and diagnosis. Journal of Advanced Nursing 50(6), 613-623 Vanderwee K, Grypdonck MHF, De Bacquer D, Defloor T (2006) The reliability of two observation methods of non-blanchable erythema, Grade 1 pressure ulcer. Advanced Nursing research 19, 156-162 Whitney JA, Phillips L. Aslam R, Barbul A, Gottrup F, Gould L, Robson MC, Rodeheaver G, Thomas D, Stotts N (2006) Guidelines for the treatment of pressure ulcers. Wound Repair and Regeneration, 14, 663-679 Wong VK, Stotts NA (2003) Physiology and Prevention of heel Pressure Ulcers: the state of science. Journal of Wound Care, 30(4), 191-198

Pressure Ulcer Policy Version 5
Page 38 of 56
BLACK HEEL
All patients with diabetes and/or Peripheral Vascular Disease should be seen by an ‘expert in the field’ i.e. Podiatry, Diabetologist, Vascular Nurse, Tissue Viability Nurse
Pressure relief is of paramount importance at all stages in the management of pressure ulcers. Please note that therapy mattresses do not offer much pressure relief to the heels
Management decision
Dry eschar/shell Eschar autolysis (I.e. wound is open and exuding) with
surrounding
Leave exposed
If arterial disease is suspected, absent pulses) a full
vascular assessment should be performed
ABPI <0.7 or >1.3 refer to
vascular surgeon
erythema
DO NOT DEBRIDE: Keep dry and inspect daily
If osteomyelitis, liaise with microbiologist for antibiotic advice
X-Ray ?osteomyelitis
If and when healing is accomplished, measures should be taken to prevent recurrence
Apply dressing Contact TVN for sharp debridement

Pressure Ulcer Policy Version 5
Page 39 of 56
Wound management

Pressure Ulcer Policy Version 5
Page 40 of 56
Appendix 10 - Patient comes into our care with Pressure Ulcer
Patient comes into our services with a Pressure Ulcer
Pressure Ulcer is documented on handover Pressure Ulcer is not documented or shared on handover or grading is not what has been handed over
RECORD IN CLINICAL RECORDS: Nurse to complete CPFT pressure documentation as per CPFT policy:
Grade the pressure damage
Obtain a photograph/ consent
Describe the skin damage.
Inform patient and carers of damage, provide education.
Complete all the following tools:
o Wound assessment chart including body map. o Waterlow o SSKIN CARE BUNDLE o Care and comfort checks for inpatients o MUST o Commence a wound care plan with clear
evaluation documented.
OTHER ACTIONS:
Ensure any equipment needed is ordered and delivered in timely manner and its use is documented within the care plan.
Assess CONTINENCE and ensure care plan in place
Consider urgent MDT.
Refer to safeguarding if any concerns
REVIEW PLAN AND ACTIONS DOCUMENT ALL AND SCHEDULE REVIEW
.
Complete Incident Form RECORD IN CLINICAL RECORDS:
Nurse to complete CPFT pressure documentation as per CPFT policy:
Grade the pressure damage
Obtain a photograph/ consent
Describe the skin damage.
Inform patient and carers of damage, provide education.
Complete all the following tools:
o Wound assessment chart including body map.
o Waterlow o SSKIN CARE BUNDLE o Care and comfort checks for inpatients o MUST o Commence a wound care plan with clear
evaluation documented.
OTHER ACTIONS:
Ensure any equipment needed is ordered and delivered in timely manner and its use is documented within the care plan.
Assess CONTINENCE and ensure care plan in place
Consider urgent MDT.
Refer to safeguarding if any concerns
REVIEW PLAN AND ACTIONS DOCUMENT ALL AND SCHEDULED REVIEW
.
Team to Feedback to e.g. ward /Acute Trust and record in the clinical records the content of communication. TS RECORDS
Quality and Safety leads will link CPFT Governance to approach other Trust GP Acute for feedback of the harm care and incident
Incident form not required unless other concerns identified by the clinician

Pressure Ulcer Policy Version 5
Page 41 of 56
Appendix 10.2 ( Team Guide)
Community and inpatient
Grade 3 or 4 Pressure Ulcer has occurred or deteriorated within Community services whilst
under care of CPFT Services
2. Incident Report is completed the same day as identified
Clinical team always :
1. RECORD IN CLINICAL RECORDS:
Nurse to complete CPFT pressure documentation as per CPFT policy:
Grade the pressure damage
Obtain a photograph/ consent
Describe the skin damage.
Inform patient and carers of damage, provide education.
Complete all the following tools:
o Wound assessment chart including measurement body map/ Photo.
o Waterlow o SSKIN CARE BUNDLE o Care and comfort checks for inpatients o MUST o Commence a wound care plan with clear evaluation
documented. OTHER ACTIONS:
Ensure any equipment needed is ordered and delivered in timely manner and its use is documented within the care plan.
Assess CONTINENCE and ensure care plan in place
Consider urgent MDT.
Refer to safeguarding if any concerns
Consider mental capacity assessment in non-compliance
Apply positive motivational interviewing techniques
REVIEW PLAN AND ACTIONS DOCUMENT ALL AND SCHEDULE REVIEW
.
3. Team complete a written 72 hour investigation and submit to their Quality and Safety lead .
4. Apply Duty of candour – refer to Policy

Pressure Ulcer Policy Version 5
Page 42 of 56
Apendix 10.3 (Assurance investigation process)
Grade 3/4 pressure ulcer (aquired in our service) reported on
Ulysses
Quality & Safety Lead to ensure72hr report is completed & Duty
Of Candour is applied
72 hr report sent to Senior Quality and Safety Lead for sign
off
Senior Quality & Safety Lead to close incident with decision to proceed to clinical review or as needed declare SIRI(serious Incident Requiring Investigation) (following usual process)
documented on sign off and on 72 hr report.
Clinical Review to be returned to Senior Quality and Safety Lead within 10 working
days
SIRI report to be submitted to Assistant Director OfNursing - timescale as Per Policy
Clinical review scrutinised at next Tissue Viability Nurse group then sent to Assitant
Director Of Nursing for final sign off. Sent to Care group governance for information.
All Completed SIRI reports to be presented at Care Group governance by Author supported by Qualiy & Safety lead, Signed off by Assitant Director Of
Nursing.
LESSONS LEARNT SHARED VIA NETWORKS.
DUTY OF CANDOUR COMPLETED.

Pressure Ulcer Policy Version 5
Page 43 of 56
Appendix 10.4
Community
Thematic Review of Pressure Ulcers
All Guidelines, Policies in place and followed. Patient choice and carer issues. No Capacity concerns No Safeguarding concerns Omissions in care.
Provide list incidents including paragraph of individual: clinical condition, Background Diagnosis, mental health issues, outcome, lesson learnt
STEIS No when appropriate Incident Number
Sign off by Associate Director of Nursing / Medical Director Care Group Governance Meeting. May also be shared with CCG and Trust Governance
Investigation is required if : Failure or suspected failure in adherence to guidelines Failure to treat Missed process/missed visits Staff error Death/hospitalisation Sepsis Safeguarding
Usually a clinical review but there may be occasions that a SIRI is declared and an investigation is required
Sign off by the Associate Director of Nursing/ Associate Medical Director/ Care Group
Copy report to CCG as SIRI requirement

Pressure Ulcer Policy Version 5
Page 44 of 56
Appendix 11
Ungradable/ Unstageable pressure ulcers
Standard Operating Practice(SOP)
Definition : Unstageable/ Ungradable Class of Pressure damage : Full thickness skin or tissue loss – depth unknown If the pressure ulcer base is not visible,(covered with thick slough or necrotic tissue) the extent of the damage is unknown so report this as ungradeable. Further description: Until enough slough and/or eschar are removed to expose the base of the wound, the true depth cannot be determined; (dry, adherent, intact without erythema or fluctuance) eschar on the heels serves as “the body’s natural (biological) cover” and should not be removed ( EPUAP(1998)/ POL 001/069(https://www.cumbriapartnership.nhs.uk/assets/uploads/policy-documents/Pressure_Ulcer_Prevention_Management_Policy_POL001069.pdf)

Pressure Ulcer Policy Version 5
Page 45 of 56
Appendix 12 Waterlow Flow Chart for Dementia Assessment Units.
Be aware that all patients are potentially at risk of developing a pressure ulcer
Risk Factors Present Yes No
An individual may develop pressure ulcers if they have the following risk factors:
Extremes of Age (Consider
Patients over 75)
Vascular disease
Previous history of pressure damage
Malnutrition (e.g. Anorexia) and dehydration
Chronic or terminal illness
Reduced mobility or immobility
Sensory impairment
Acute illness (Physical)
Reduced level of consciousness
Severe depressive illness where patients are sitting for long periods
Reassess pressure ulcer risk weekly OR if change in clinical status
Complete Waterlow Risk Assessment Document Risk and identify pressure ulcer
prevention strategies as per Pressure Ulcer
Prevention/Management Policy.
Pressure ulcer risk identified
Reassess and update Waterlow Weekly
Adapted from NICE CG179 (2014)

Pressure Ulcer Policy Version 5
Page 46 of 56
Appendix 13
Standard Operating Procedure (SOP)
Discharging patients from District Nursing case load with pressure equipment
Patients who have been on a CPFT caseload and no longer require input from the service but have been provided with equipment that becomes the patients property and does not need sending back to ICES such as static
pressure relieving cushions.
The following must take place:
• The patient must have capacity to understand the
implications of pressure damage.
• The patient and family/ carers should have the education
around pressure damage and be provided with the leaflet.
• Be assessed as low or medium risk. • Be provided with the nice guideline on pressure ulcers.
• Clearly documented how to re ref to the service if necessary.
• Patient given product information leaflets.
Pressure Ulcer Policy Version 5
Page 47 of 56
Pressure Ulcer Policy Version 5
Page 48 of 56
,
A User’s Guide
Additional information
If you would like this factsheet in another language or format, e.g. Braille, large print or audio, please contact: Membership and Communications Department
Voreda | Portland Place | Penrith | CA11 7QQ
T: 01228 603890 | E: [email protected]

Pressure Ulcer Policy Version 5
Page 49 of 56
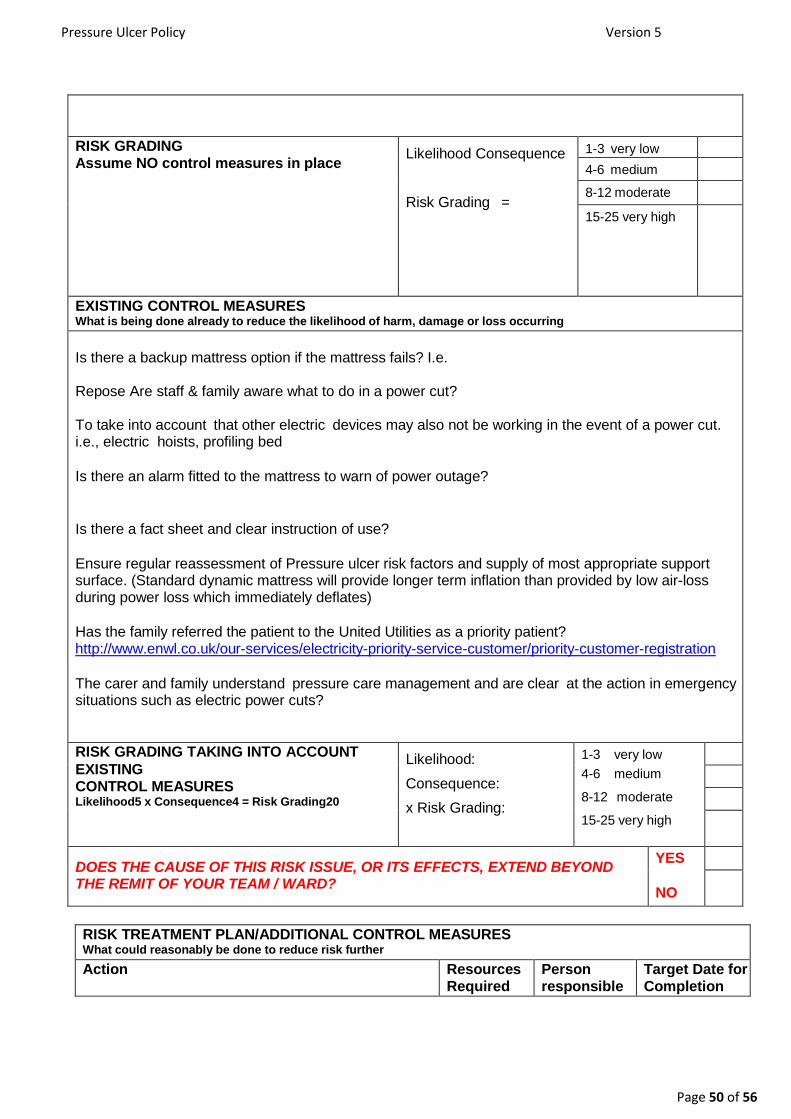
Appendix 14
RISK ASSESSMENT FORM FOR INDIVIDUAL PATIENT AIR LOSS MATTRESSES USED IN THE COMMUNITY SETTING
PATIENT NAME PATIENT DETAILS
COMMUNIYY TEAM INVOLVED RISK ASSESSMENT COMPLETED BY:
HAZARD, WORK TASK, ACTIVITY task, object, product, work environment, or situation with the potential to cause harm, damage or loss to people, property or service delivery
Patient . Is at very high risk of developing pressure ulcers and has been assessed as needing a low air- loss mattress, with or without lateral turn facility.
In the patient . own home there is/is not a carers who would be aware of a power outage and could take steps to minimise further risk?
RISK potential outcome or effect of hazard
During a power outage the mattress will deflate and the patient will be laying on the bed frame alone leading to further risk of pressure damage
Patient and/or carers may be unaware of power loss
Patient and / or carers may not fully understand the high risk implications of the mattress deflating and the patient laying on a hard frame for even a short amount of time.
If the patient lives alone a low air loss mattress should be carefully considered and discussed with Tissue Viability Team.
Pressure Ulcer Policy Version 5
Page 50 of 56
RISK GRADING Assume NO control measures in place
Likelihood Consequence
Risk Grading =
1-3 very low
4-6 medium
8-12 moderate
15-25 very high
EXISTING CONTROL MEASURES What is being done already to reduce the likelihood of harm, damage or loss occurring
Is there a backup mattress option if the mattress fails? I.e.
Repose Are staff & family aware what to do in a power cut?
To take into account that other electric devices may also not be working in the event of a power cut. i.e., electric hoists, profiling bed
Is there an alarm fitted to the mattress to warn of power outage?
Is there a fact sheet and clear instruction of use?
Ensure regular reassessment of Pressure ulcer risk factors and supply of most appropriate support surface. (Standard dynamic mattress will provide longer term inflation than provided by low air-loss during power loss which immediately deflates)
Has the family referred the patient to the United Utilities as a priority patient? http://www.enwl.co.uk/our-services/electricity-priority-service-customer/priority-customer-registration
The carer and family understand pressure care management and are clear at the action in emergency situations such as electric power cuts?
RISK GRADING TAKING INTO ACCOUNT
EXISTING CONTROL MEASURES Likelihood5 x Consequence4 = Risk Grading20
Likelihood:
Consequence:
x Risk Grading:
=
1-3 very low
4-6 medium
8-12 moderate
15-25 very high
DOES THE CAUSE OF THIS RISK ISSUE, OR ITS EFFECTS, EXTEND BEYOND THE REMIT OF YOUR TEAM / WARD?
YES
NO
RISK TREATMENT PLAN/ADDITIONAL CONTROL MEASURES What could reasonably be done to reduce risk further
Action Resources Required
Person responsible
Target Date for Completion
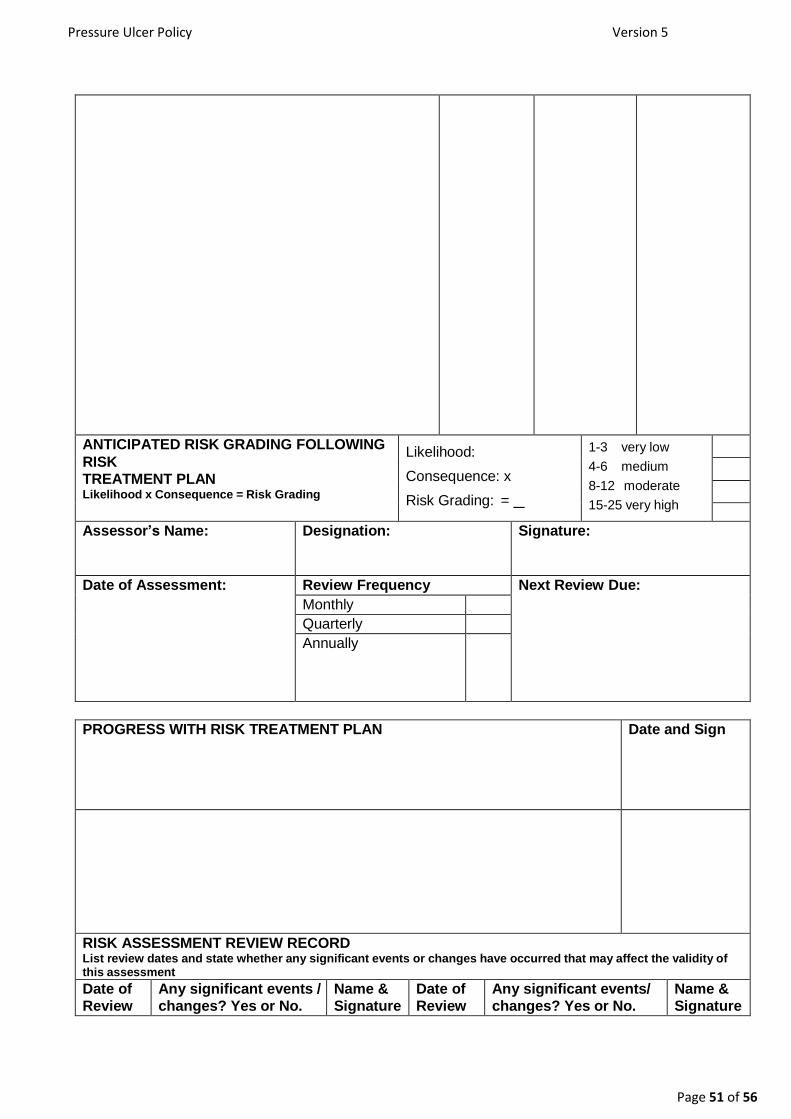
Pressure Ulcer Policy Version 5
Page 51 of 56
ANTICIPATED RISK GRADING FOLLOWING
RISK TREATMENT PLAN Likelihood x Consequence = Risk Grading
Likelihood:
Consequence: x
Risk Grading: =
1-3 very low
4-6 medium
8-12 moderate
15-25 very high
Assessor’s Name: Designation: Signature:
Date of Assessment: Review Frequency Next Review Due:
Monthly
Quarterly
Annually
PROGRESS WITH RISK TREATMENT PLAN Date and Sign
RISK ASSESSMENT REVIEW RECORD List review dates and state whether any significant events or changes have occurred that may affect the validity of this assessment
Date of Review
Any significant events / changes? Yes or No.
Name & Signature
Date of Review
Any significant events/ changes? Yes or No.
Name & Signature

Pressure Ulcer Policy Version 5
Page 52 of 56
If YES do new
assessment
If YES do new
assessment
Pressure Ulcer Policy Version 5
Page 53 of 56
FOR RISK MANAGEMENT DEPARTMENT USE ONLY
Include on Corporate Register for consideration by Board? Yes No
Accepted by Director? Name Yes No
If not accepted by Director, state reasons and further action
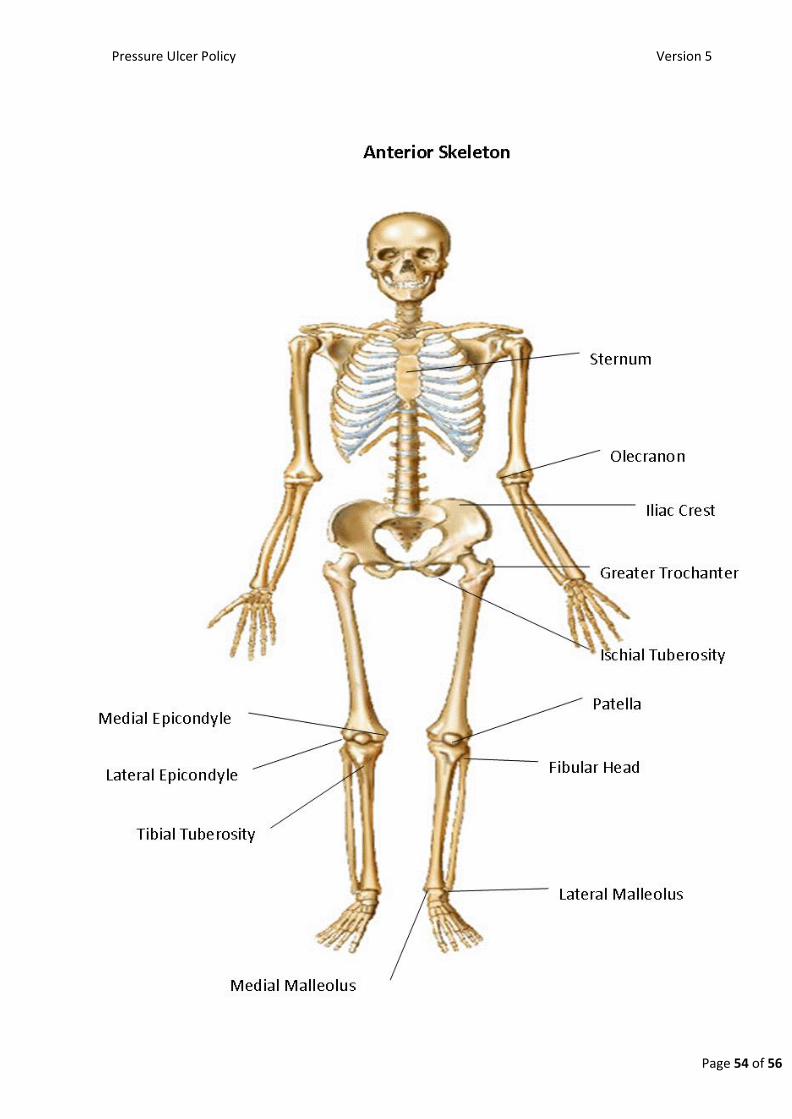
Pressure Ulcer Policy Version 5
Page 54 of 56

Pressure Ulcer Policy Version 5
Page 55 of 56
Occipital
Acromion
Centrally Spinous Process
Greater Tubercle Scapular
Olecranon
Iliac Crest
Sacrum
Coccyx
Greater Trochanter
Ischial Tuberosity
Medial Epicondyle
Lateral Epicondyle
Calcaneum
Medial Malleolus
Lateral Malleolus
Posterior Skeleton

Pressure Ulcer Policy Version 5
Page 56 of 56