pressure injury prevention and management strategies … · pressure injury prevention and...
TRANSCRIPT

Prepared by Rosemary Beenie
Nurse Manager, Clinical Informatics
Liverpool Hospital
March 2014
Pressure Injury Prevention and Management Strategies in
SWSLHD
Background
The Waterlow Pressure Ulcer Risk Assessment scoring
system was introduced at Liverpool in the early 2000’s
A point prevalence audit conducted in 2008 found that only
37% of patients had a Waterlow assessment completed,
and only 54% of patients deemed ‘at risk’ were on
appropriate mattresses
Each ward had their own mattress rental preferences as
there were no hospital wide guidelines

Actions
A hospital wide system for the rental of mattresses was
developed
‘Waterlow Wednesday’ was introduced
On Wednesday of every week a staff member would audit
Waterlow score and mattress for every patient
Results were collated by the Wound CNC and distributed
monthly to NUMs

Mattress Rental Guide
Mattress model Supplier
Phone number
Mattress model Supplier
Phone number
Mattress model Supplier
Phone number

Compliance improved but……
Waterlow Wednesdays were taking 2-3 hours to complete
for ward staff, plus hours for results to be collated for
monthly reports
Large amount of paperwork generated, but audit forms lost
Staff did not remember when Waterlow assessments were
due for each patient
Confusion about the ‘Wednesday’ - Patients admitted on
Thursday could wait almost a week before assessment

The improvements were not
sustainable……
The audits were conducted weekly, but collated monthly –
feedback loop lag
Advice about the preventive measures to be taken was on
the back of the form – staff didn’t always turn it over
Other priorities took precedence

eMR - 2010
The Waterlow assessment tool had already been built in
eMR for community nursing
We worked with the eMR team to make it suitable for the
inpatient setting – adding a preventive measures segment,
and rules to remind staff when to re-assess
eMR was used to reinforce policy – assessment to be done
on admission, on transfer to a new ward, and every 7 days
The computer doesn’t know when the patient’s condition
has changed, this requires nursing judgement to reassess

eMR Waterlow Assessment tool
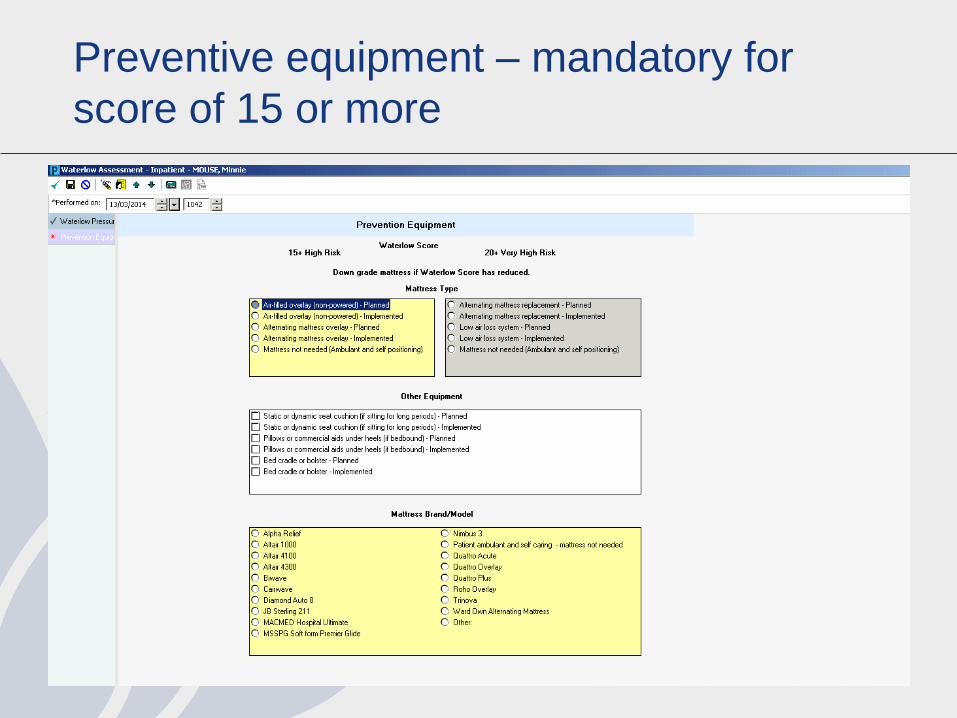
Preventive equipment – mandatory for
score of 15 or more

Assessment due – the Patient Access List
Apples indicate an assessment is due, click on the apple to
open and complete the form
eMR Waterlow Benefits
Quicker than paper – calculations done by the computer
Reminders when assessment or reassessment is due
Recognises when a patient is transferred to a new ward.
Resets the timer if an ad hoc form is completed due to
change in condition
Prompt to record pressure relieving options (planned or
implemented) when the patient is ‘high risk’ i.e. score of 15
or higher
Automated referral to dietician if MST is 3 or more
More eMR Benefits
The PowerChart flowsheet allows comparison of
assessments over time
NUM or delegate can review scores for each patient and
ensure appropriate pressure relieving devices are available
(or removed when no longer required)
Aids but does not override clinical judgement
Waterlow Wednesday audit process automated and
centralised – now takes less than 15 minutes to collate and
distribute weekly compliance reports
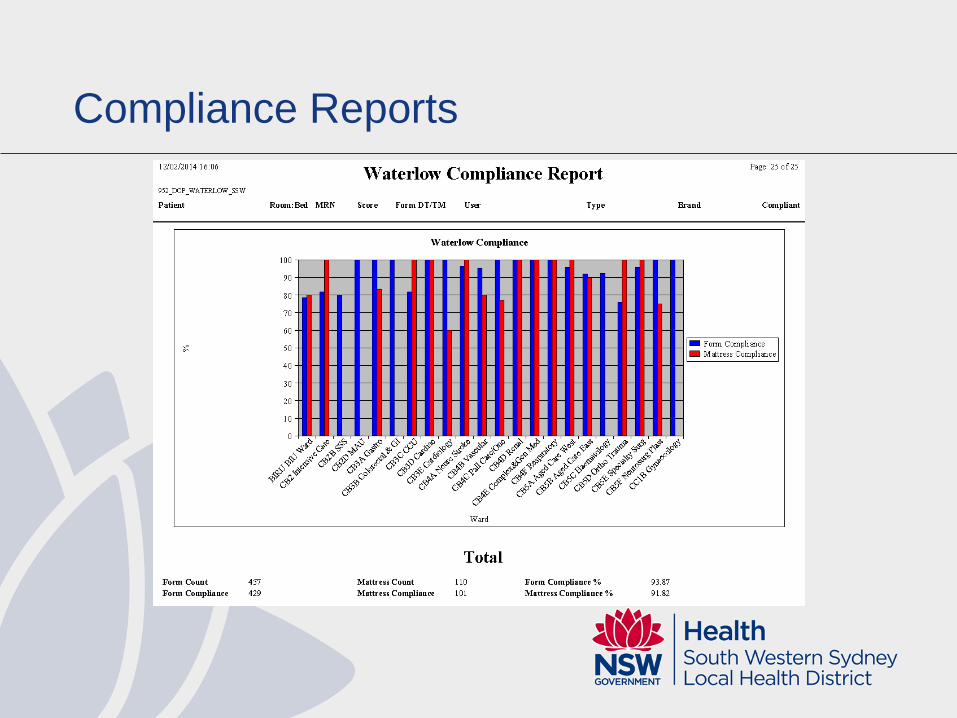
Compliance Reports

Detailed Compliance Reports
Automated reports run weekly for the whole hospital,
but can be run any time at a ward level

What have we achieved?
Compliance with Waterlow assessments improved from
37% in 2008 to 79% in 2009 using paper processes
By 2011, after the eMR implementation, compliance
improved to 91%. Since 2012 it has been sustained
between 80%-95%
Utilisation of appropriate pressure relieving mattresses
increased from 54% in 2008 to over 89% in 2011
An estimated saving of 151 hours per month in manual
auditing

How have our patients benefited?
Point prevalence audits show the incidence of Hospital
Acquired Pressure Injuries has dropped from 13% in 2009
to 8% in 2011 and 5.6% in 2013
Deep ulceration (Grade 3 & 4) dropped from 27% in 2009,
to 3% in 2011 and 1.6% in 2013
An estimated 43 additional patients prevented from
developing a pressure injury over 24 months
Less pain and discomfort, less occasions of extended
length of stay

Where to from here?
New reports to identify whether the Waterlow assessments
are performed within 8 hours of admission or transfer to a
ward
Electronic documentation of pressure injuries when they do
occur

Acknowledgements
Matthew Wilson, former CNC Wound Care Liverpool
Hospital
Cara Bowen, CNC Wound Care, Liverpool Hospital
The eMR team and report writers from the Information and
Technology Division, Sydney & South Western Sydney
LHDs.