presented by natalie scott 2012
DESCRIPTION
Cellulitis Fungal Infection & Venous Eczema. Presented by Natalie Scott 2012. Overview. Skin structure Cellulitis eitiology, pathogens, symptoms Tinea Pedis fungal infection and its potential risk factor for cellulitis Treatment fungal infection Venous Eczema and treatment - PowerPoint PPT PresentationTRANSCRIPT
Cellulitis
Fungal Infection&
Venous Eczema
Presented byPresented by
Natalie Scott 2012Natalie Scott 2012
OverviewOverview
Skin structureSkin structure Cellulitis eitiology, pathogens, Cellulitis eitiology, pathogens,
symptomssymptoms Tinea Pedis fungal infection and its Tinea Pedis fungal infection and its
potential risk factor for cellulitispotential risk factor for cellulitis Treatment fungal infectionTreatment fungal infection Venous Eczema and treatmentVenous Eczema and treatment Summary: Holistic AssessmentSummary: Holistic Assessment
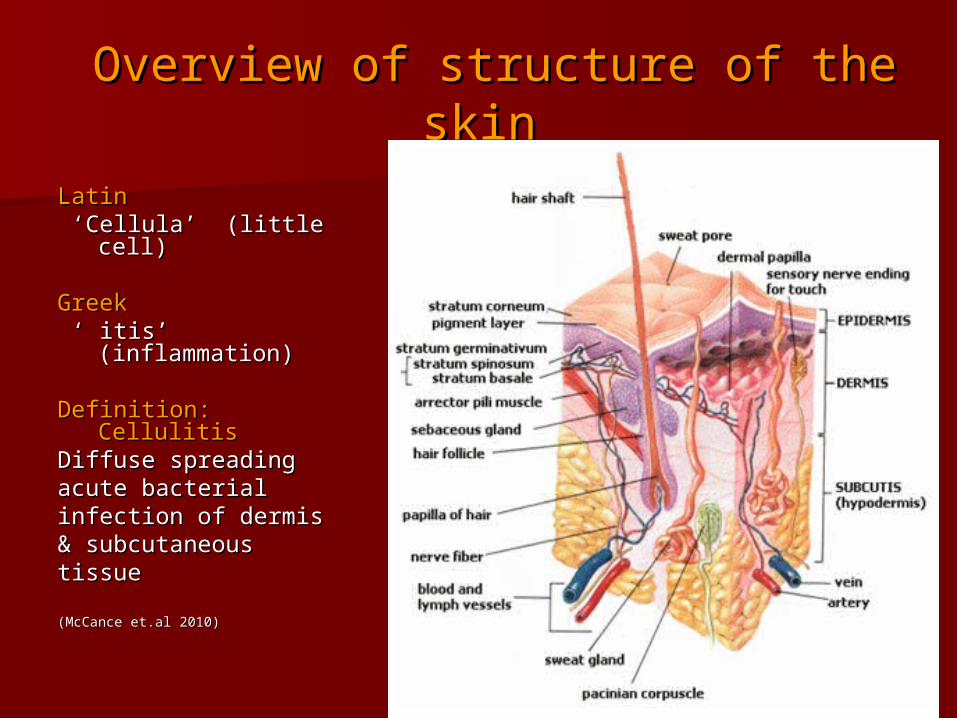
Overview of structure of the skinOverview of structure of the skin
LatinLatin ‘ ‘Cellula’ (little cell)Cellula’ (little cell)
GreekGreek ‘ ‘ itis’ (inflammation)itis’ (inflammation)
Definition:Definition: CellulitisCellulitisDiffuse spreading Diffuse spreading acute bacterialacute bacterialinfection of dermisinfection of dermis& subcutaneous& subcutaneoustissue tissue
(McCance et.al 2010)(McCance et.al 2010)
Cellulitis: Cellulitis: eitiologyeitiologyNormal skin provides effective barrier (1Normal skin provides effective barrier (1stst
line defence) pH 5.5line defence) pH 5.5 Bacteria microbes - opportunistic Bacteria microbes - opportunistic gain entry through breaks in the skingain entry through breaks in the skin e.g. trauma, insect bites, ulcers, burns, e.g. trauma, insect bites, ulcers, burns, surgical incisions, IV catheters (all surgical incisions, IV catheters (all
potential pathways) potential pathways)
Cellulitis associated inflammation occursCellulitis associated inflammation occurs potentially dangerous affecting the skin potentially dangerous affecting the skin
layers, epidermis, dermis, subcutaneous layers, epidermis, dermis, subcutaneous tissue and spreading to the lymph and tissue and spreading to the lymph and bloodstreambloodstream
Cellulitis - PathogensCellulitis - PathogensStaphylococcus AureusStaphylococcus Aureus can start from can start from
centralcentral
localised infection & spread e.g. abscesslocalised infection & spread e.g. abscess
Streptococci pyrogenes (Group A) Gram +Streptococci pyrogenes (Group A) Gram + (haemolytic)(haemolytic)
Spreads up the leg rapidly & diffuselySpreads up the leg rapidly & diffusely FeverFever > necrotising fasciitis (flesh eating > necrotising fasciitis (flesh eating
bacterium)bacterium)
Pseudomonas spp. Pseudomonas spp.
Bacteriodes spp.Bacteriodes spp.
Hemophyllis sppHemophyllis spp
Cellulitis symptoms
Local heatLocal heat - hot/warm. Swelling in the tissues - hot/warm. Swelling in the tissues surrounding woundsurrounding wound
Redness Redness – red streaking or broad areas of redness– red streaking or broad areas of redness PainPain or tenderness or tenderness SwellingSwelling – rapid spreading ascent up lower leg. – rapid spreading ascent up lower leg.
Tight glossy stretched appearance of the skinTight glossy stretched appearance of the skin DrainageDrainage or leakage of yellow clear fluid or pus or leakage of yellow clear fluid or pus
from the skinfrom the skin Flu likeFlu like symptoms symptoms
(CREST GUIDELINES 2005 ) Management of cellulitis in Adults(CREST GUIDELINES 2005 ) Management of cellulitis in Adults
CellulitisCellulitis
Condition spreadsCondition spreads - Progress to lymph and blood stream - Progress to lymph and blood stream Fever > 38CFever > 38C MalaiseMalaise Chills Chills HeadacheHeadache Elevated white cell count & CRPElevated white cell count & CRP Abscess and tissue destruction (without Abscess and tissue destruction (without
intervention)intervention) Life threatening – e.g. necrotising fasciitis (strep Life threatening – e.g. necrotising fasciitis (strep
spp and anaerobes) spp and anaerobes)

CellulitisCellulitis

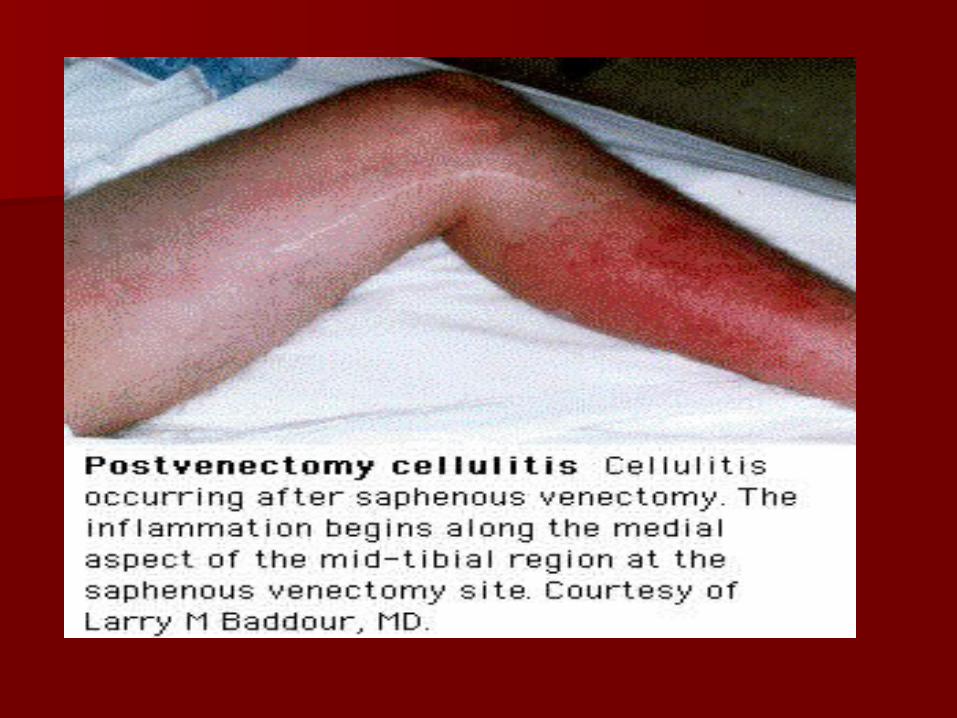
Cellulitis with blisteringCellulitis with blisteringManagement protection /exudatesManagement protection /exudates
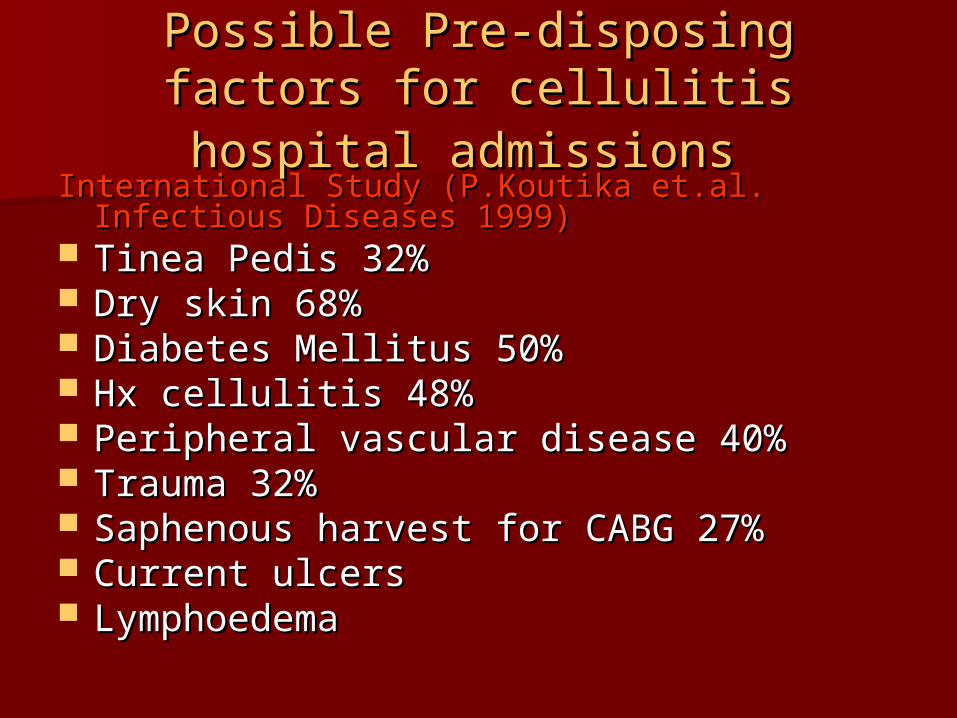
Possible Pre-disposing factors for Possible Pre-disposing factors for cellulitis hospital admissionscellulitis hospital admissions
International Study (P.Koutika et.al. Infectious International Study (P.Koutika et.al. Infectious Diseases 1999)Diseases 1999)
Tinea Pedis 32%Tinea Pedis 32% Dry skin 68%Dry skin 68% Diabetes Mellitus 50%Diabetes Mellitus 50% Hx cellulitis 48%Hx cellulitis 48% Peripheral vascular disease 40%Peripheral vascular disease 40% Trauma 32%Trauma 32% Saphenous harvest for CABG 27%Saphenous harvest for CABG 27% Current ulcersCurrent ulcers LymphoedemaLymphoedema
Management of CellulitisManagement of Cellulitis
Antibiotic regimeAntibiotic regime – –
Cellulitis - Dry skin – – Keep dryKeep dry
Emollient helps re-establish skin integrity Emollient helps re-establish skin integrity 50/50 soft white paraffin50/50 soft white paraffin
Cellulitis Wet skin – – Blistering.Blistering.
Control exudate with absorbent dressings Control exudate with absorbent dressings (foams, alginates, hydrofibre, zetuvit). (foams, alginates, hydrofibre, zetuvit). Control macerationControl maceration
Management of CellulitisManagement of Cellulitis
Pain - regular analgesia Inflammation - Monitor area (mark with
pen) Rest – plenty of it Exercise - Dorsiflexion and plantar foot
exercises will aid drainage of oedema Oedema – elevate limb Patients with venous insufficiency history –
compression bandage post acute stage
(Hofman, 1998 & Van Onselen, 2001)(Hofman, 1998 & Van Onselen, 2001)
Tinea pedis ‘Athletes foot’Tinea pedis ‘Athletes foot’15-25%15-25% population infected population infected at any one at any one
timetime Caused by Parasitic fungi – Trichophyton
dermaphyte
Webs between toes - warm moist environment plantar of the foot and bullous (blister) form
Inadequate hygiene /drying Infected - public amenities
Tinea pedis spp. (fungal) provides entry point for bacteria to invade the soft tissue through the broken skin, abrasions/wounds leading to infection – potential cellulitis
Tinea Pedis: symptoms
Appears “macerated” between toe webs
(skin peeling) Scales or flaking Cracks or blisters Itching or burning sensation in
localised area Redness & inflammation of the toes Exposure of raw tissue
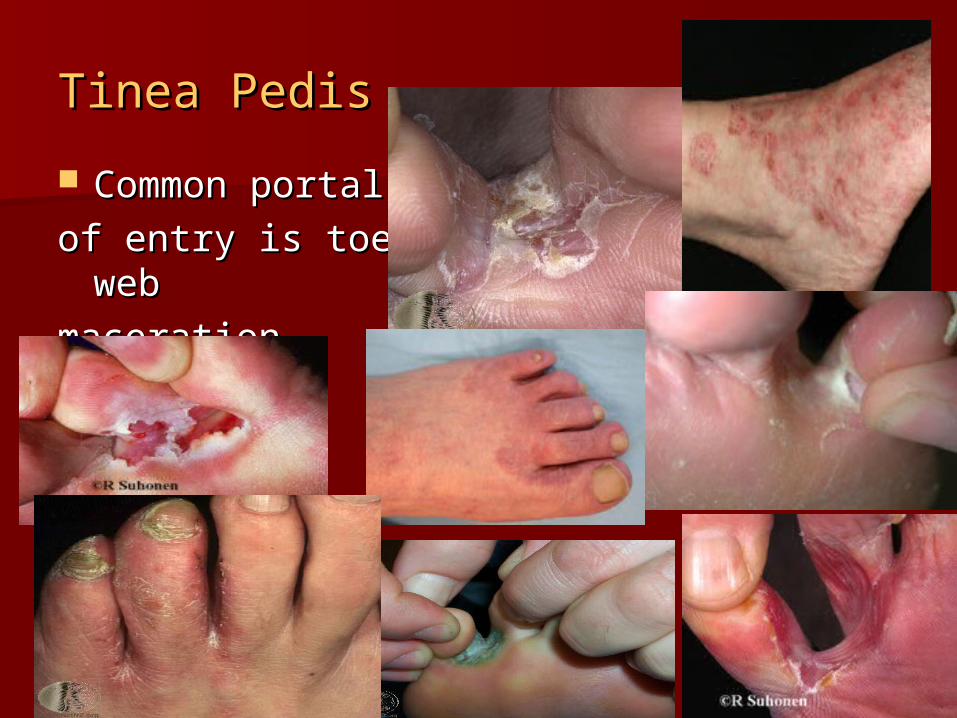
Tinea PedisTinea Pedis
Common portal Common portal
of entry is toe webof entry is toe web
maceration maceration
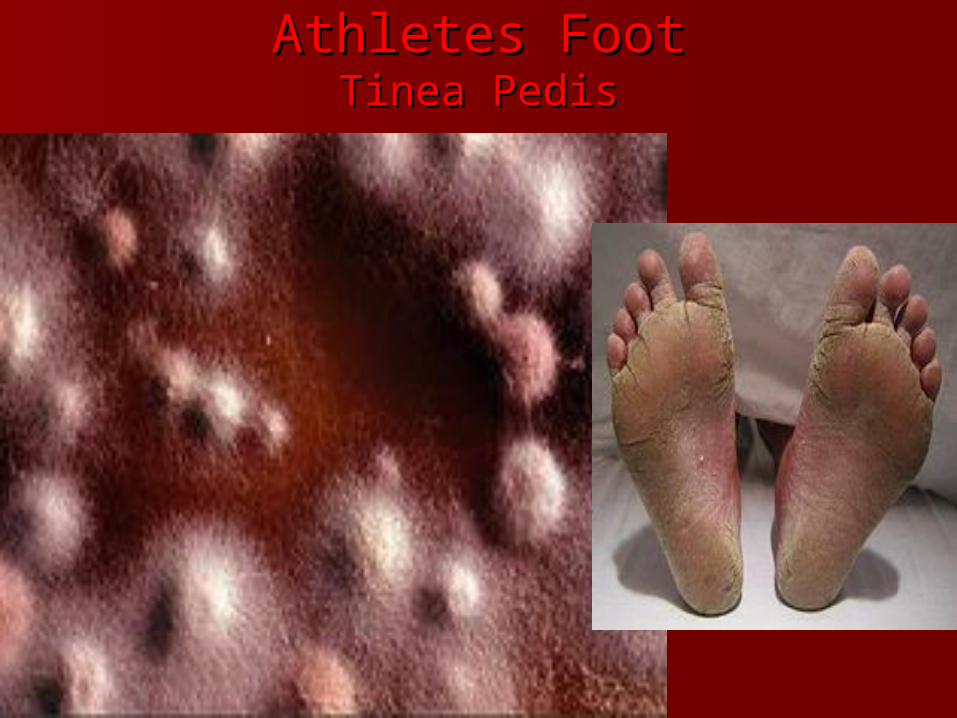
Athletes FootAthletes FootTinea PedisTinea Pedis
Tinea PedisTinea PedisTreatment (anti-fungal creams/tabs)Treatment (anti-fungal creams/tabs)
Lamisil (Terbinafine) (86% cure rate at 6 wks)Lamisil (Terbinafine) (86% cure rate at 6 wks) Azoles: Miconazole & Clotrimazole (53% cure) Apply to dried skin (weave gauze around toes)
Oral tabs
Fluconazole & Terbinafine
Antibiotics for co-existing bacterial infection Continue tx till 1 – 2 weeks after fungal infection resolved
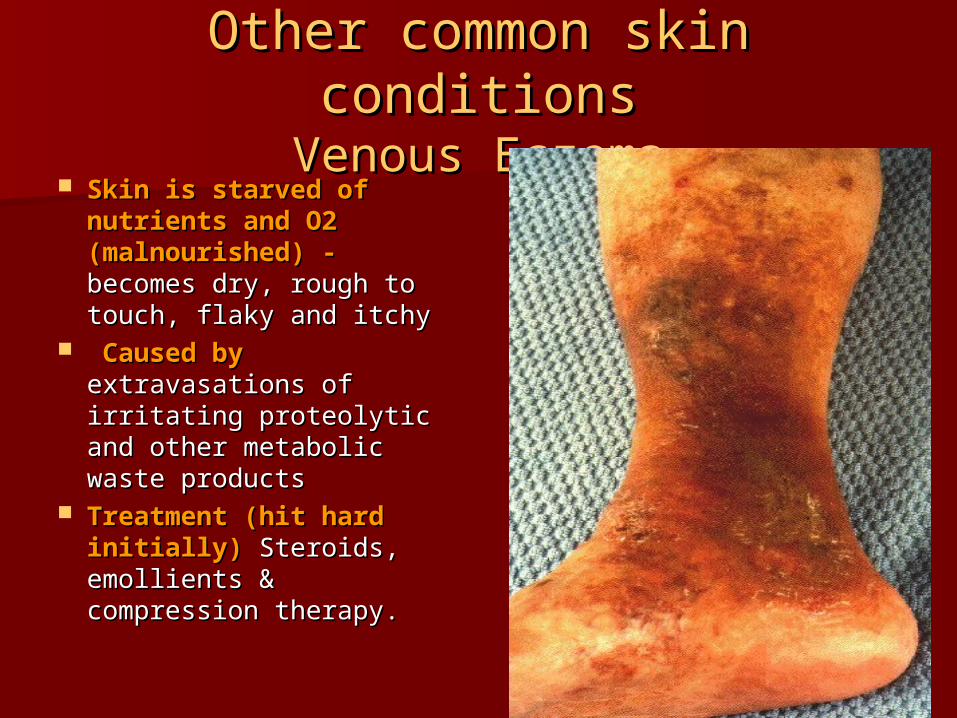
Other common skin conditionsOther common skin conditionsVenous EczemaVenous Eczema
Skin is starved of Skin is starved of nutrients and O2 nutrients and O2 (malnourished) -(malnourished) - becomes dry, rough to becomes dry, rough to touch, flaky and itchytouch, flaky and itchy
Caused byCaused by extravasations of irritating extravasations of irritating proteolytic and other proteolytic and other metabolic waste productsmetabolic waste products
Treatment (hit hard Treatment (hit hard initially)initially) Steroids, Steroids, emollients & compression emollients & compression therapy.therapy.

Venous eczema:Venous eczema: requiresrequires urgent Doppler))
Treat with steroid cream/zinc/emollients Treat with steroid cream/zinc/emollients and compressionand compression
Steroid ClassificationSteroid ClassificationNZ DermNetNZ DermNet
Class 1:Class 1: DermolDermol 600 x more potent than hydrocortisone (very potent)600 x more potent than hydrocortisone (very potent)
Class 2:Class 2: Betnovate/Locoid/EleconBetnovate/Locoid/Elecon 100 -150 x more potent than 100 -150 x more potent than
hydrocortisone (potent)hydrocortisone (potent)
Class 3:Class 3: Eunovate cream, kenacomb cream/ungEunovate cream, kenacomb cream/ung 25 x more 25 x more
potent than hydrocortisone (mod potent)potent than hydrocortisone (mod potent)
Class 4Class 4: Hydrocortisone 0.5-2.5%: Hydrocortisone 0.5-2.5% found in Lemnis fatty cream, pimafucort, DP lotion found in Lemnis fatty cream, pimafucort, DP lotion
HC1% mildly potentHC1% mildly potent
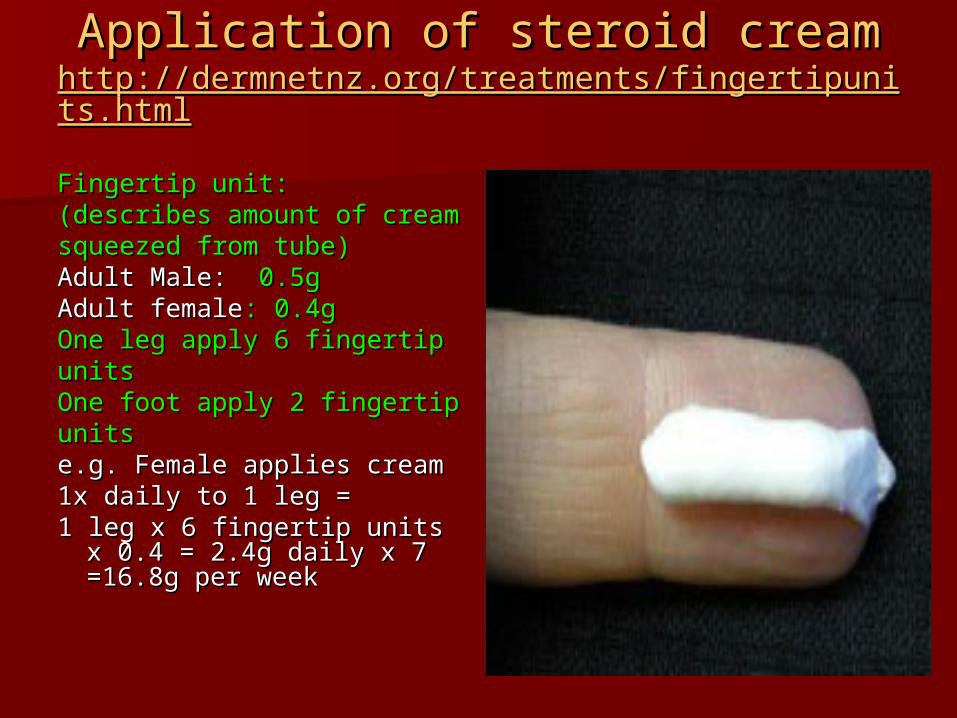
Application of steroid creamApplication of steroid creamhttp://dermnetnz.org/treatments/fingertipunits.htmlhttp://dermnetnz.org/treatments/fingertipunits.html
Fingertip unit:Fingertip unit:(describes amount of cream(describes amount of creamsqueezed from tube)squeezed from tube)Adult Male:Adult Male: 0.5g 0.5gAdult femaleAdult female: 0.4g: 0.4gOne leg apply 6 fingertipOne leg apply 6 fingertipunitsunitsOne foot apply 2 fingertipOne foot apply 2 fingertipunitsunitse.g. Female applies creame.g. Female applies cream 1x daily to 1 leg =1x daily to 1 leg =1 leg x 6 fingertip units x 1 leg x 6 fingertip units x
0.4 = 2.4g daily x 7 0.4 = 2.4g daily x 7 =16.8g per week=16.8g per week
AssessmentAssessment Differential diagnosis: cellulitis or Differential diagnosis: cellulitis or
inflammationinflammation
ThisThis is common source of diagnostic is common source of diagnostic confusion with redness alone – spreading confusion with redness alone – spreading erythema more accurate indicator of erythema more accurate indicator of infection when accompanied with raised infection when accompanied with raised temp or increased pain levelstemp or increased pain levels))
Elderly, obese or chronic oedematous legs Elderly, obese or chronic oedematous legs can have significant erythema (usually not can have significant erythema (usually not hot to touch & is symmetrical)hot to touch & is symmetrical)
ConclusionConclusionThorough Wound/Skin AssessmentThorough Wound/Skin Assessment
Need a good assessment toolNeed a good assessment tool
History taking-History taking- medical status looking for the medical status looking for the underlying cause e.g. underlying cause e.g.
Physical assessmentPhysical assessment – thorough examination – thorough examination of the limb, foot examinationof the limb, foot examination
Plan –Plan – manage infection, pain, manage manage infection, pain, manage venous insufficiency, wound management, venous insufficiency, wound management, wound measurementwound measurement
(Note: 30% reduction in wound size at 4 (Note: 30% reduction in wound size at 4 weeks the wound will be healed at 12 weeks the wound will be healed at 12 weeks)weeks)
Referral?Referral? To specialist To specialist

QuestionsQuestions
ReferencesReferences
Eagle M (2007). Understanding Cellulitis of the lower limb. Eagle M (2007). Understanding Cellulitis of the lower limb. Wound Essentials Wound Essentials 2 Dermnet NZ Fingertip unit 2 Dermnet NZ Fingertip unit
http://dermnetnz.org/treatments/fingertip units.htmlhttp://dermnetnz.org/treatments/fingertip units.html
Semel JD, Goldin H, (1996) Association of athletes foot with Semel JD, Goldin H, (1996) Association of athletes foot with cellulitis of the lower extremities: diagnostic value of cellulitis of the lower extremities: diagnostic value of bacterial cultures of ipsilateral interdigital space samples.bacterial cultures of ipsilateral interdigital space samples. Clinical Infectious Diseases 23 Clinical Infectious Diseases 23 pp1162-1164pp1162-1164
http://dermatology.jwatch.org/egi/content/full/1997/301/1http://dermatology.jwatch.org/egi/content/full/1997/301/1
Wiley On Line Library (2009) Diabetic Medicine Vol 26 Issue 5Wiley On Line Library (2009) Diabetic Medicine Vol 26 Issue 5
http://onlinelibrary.wiley.com/doi/10.1111/j.1464-5491.2009http://onlinelibrary.wiley.com/doi/10.1111/j.1464-5491.2009.02722.x/pdf.02722.x/pdf
ReferencesReferences
Roujeau, J., Sigurgeirsson, B., Korting, H., Helmut, K., & Paul, C. Roujeau, J., Sigurgeirsson, B., Korting, H., Helmut, K., & Paul, C. (2004). Chronic Dermatomycoses of the Foot as Risk Factors for (2004). Chronic Dermatomycoses of the Foot as Risk Factors for Acute Bacterial Cellulitis of the Leg: A Case-controlled Study.Acute Bacterial Cellulitis of the Leg: A Case-controlled Study. DermatologyDermatology,, 209, 301-307. Retrieved from, 209, 301-307. Retrieved from, http://content.karger.com/produktedb/produkte.asp?DO1=10.1159http://content.karger.com/produktedb/produkte.asp?DO1=10.1159/000080853/000080853
Vanhooteghem, O., Szepetiuk, G., Paurobally, D., & Heureux, F. Vanhooteghem, O., Szepetiuk, G., Paurobally, D., & Heureux, F. (2011). Chronic interdigital dermatophyic infection: a common (2011). Chronic interdigital dermatophyic infection: a common lesion associated with potentially severe consequences. lesion associated with potentially severe consequences. Diabetes Diabetes Research Clinical Practice, Research Clinical Practice, 91(1), 23-5. Retrieved from 91(1), 23-5. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/21035887http://www.ncbi.nlm.nih.gov/pubmed/21035887 Al Hasan, M., Al Hasan, M., Fitzgerald, S.M., Saoudian,Fitzgerald, S.M., Saoudian,
M., & Krishnasamy, G. (2004).Dermatology for the practicing allergist:M., & Krishnasamy, G. (2004).Dermatology for the practicing allergist:Tinea pedis and its complications.Tinea pedis and its complications.Clinical and Molecular AllergyClinical and Molecular Allergy,, 2(5). 2(5).
Retrieved from, Retrieved from, http://www.ncbi.nlm.nih.gov/pmc/articles/PMC419368/http://www.ncbi.nlm.nih.gov/pmc/articles/PMC419368/