presented by: kristi metzger, cnp sanford cardiovascular institute april 7 th, 2015
TRANSCRIPT
Atrial ArrhythmiasPresented by: Kristi Metzger, CNP
Sanford Cardiovascular InstituteApril 7th, 2015

- Review of Atrial arrthymias
Overview
The heart has a conduction system separate from any other system
The conduction system makes up to PQRST complex
An arrhythmia is a disruption in this system
Understanding how the heart conducts normally is essential to understanding arrhythmias
Conduction System
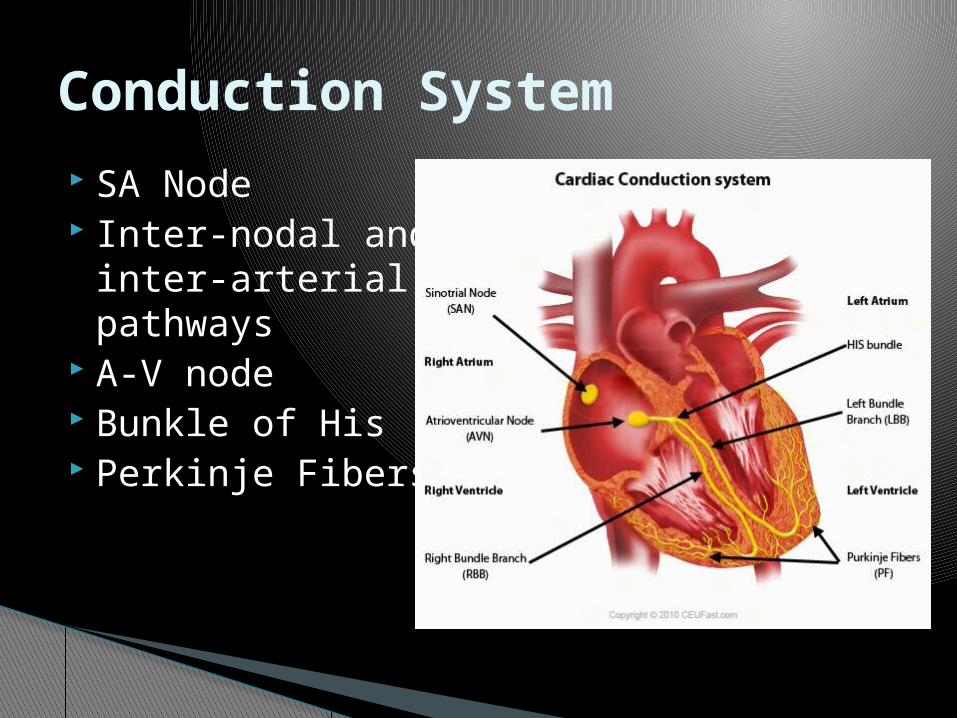
SA Node Inter-nodal and
inter-arterial pathways
A-V node Bunkle of His Perkinje Fibers
Conduction System
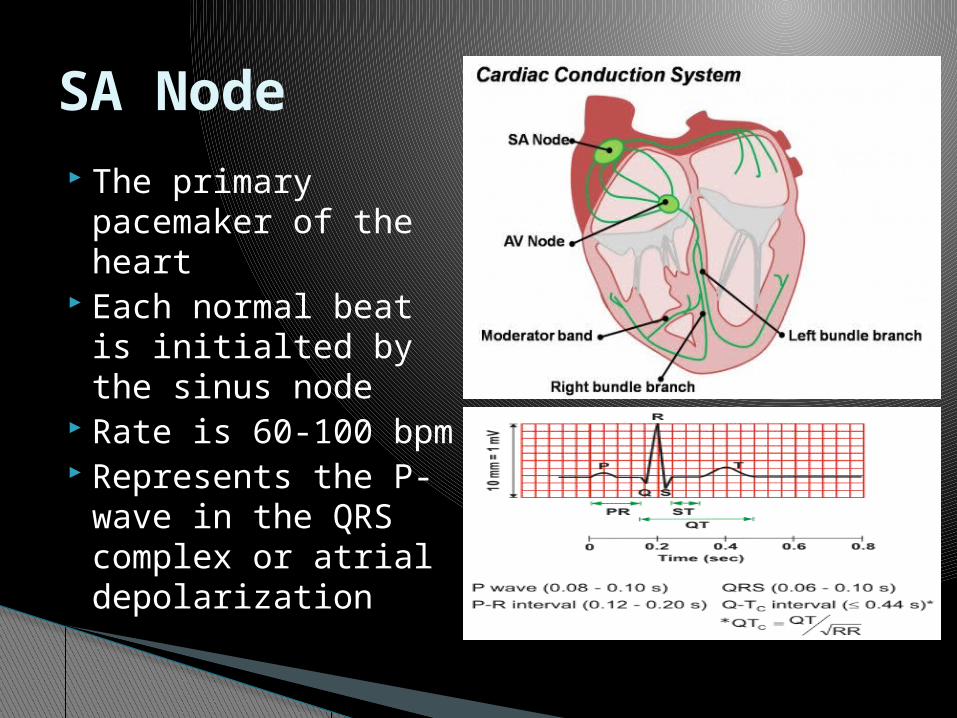
The primary pacemaker of the heart
Each normal beat is initialted by the sinus node
Rate is 60-100 bpm Represents the P-
wave in the QRS complex or atrial depolarization
SA Node
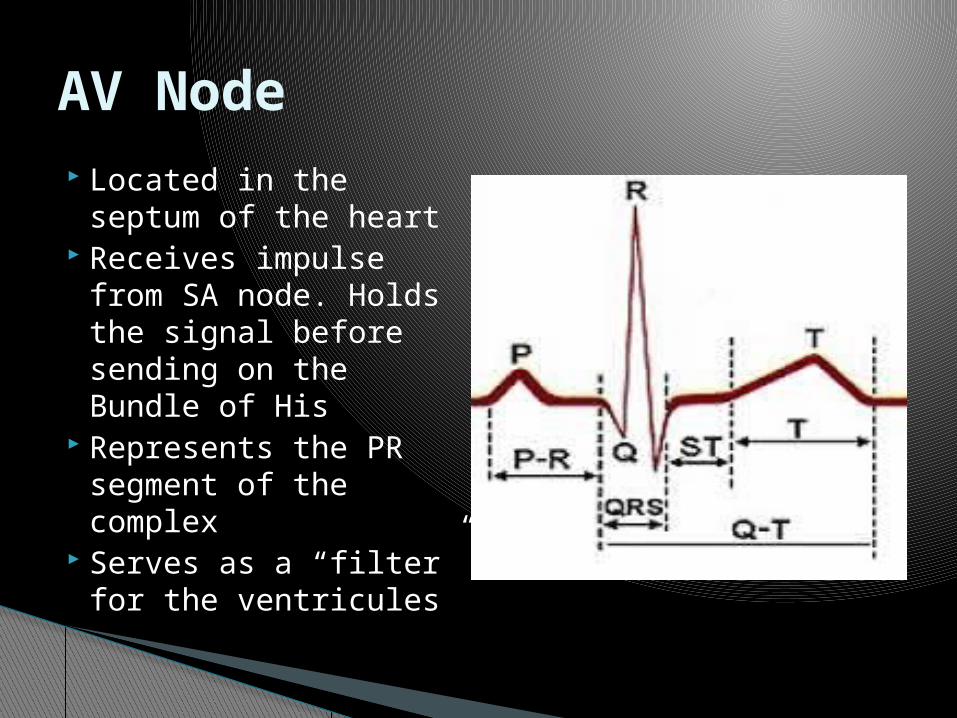
Located in the septum of the heart
Receives impulse from SA node. Holds the signal before sending on the Bundle of His
Represents the PR segment of the complex
Serves as a “filter” for the ventricules
AV Node
Rate is 40-60 bpm Acts as a back up if
the SA node fails Where all
junctional rhythms originate
AV Node
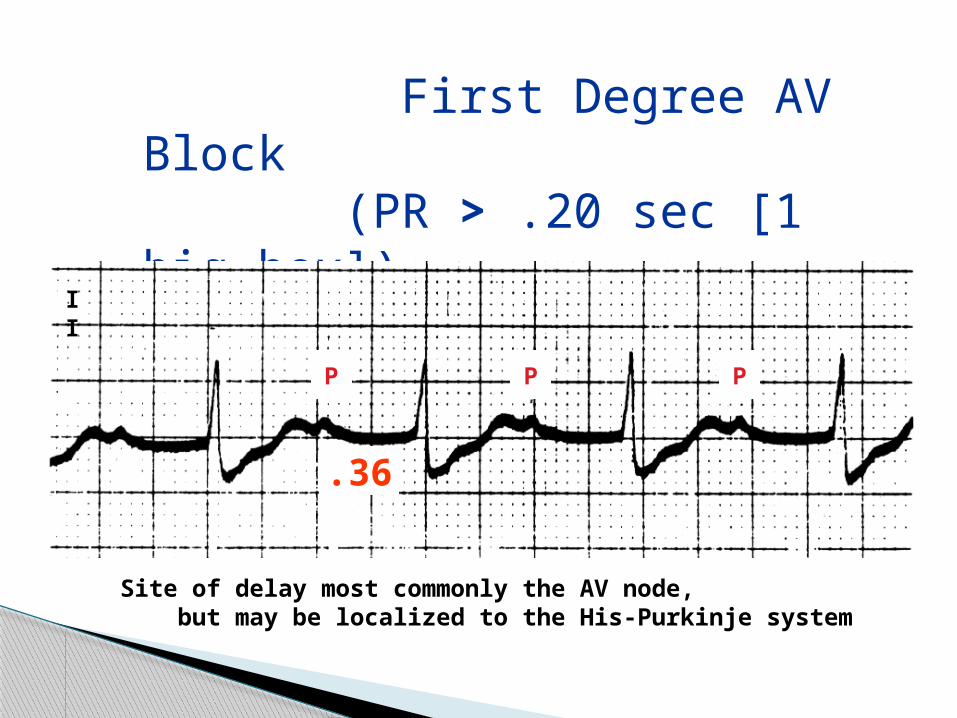
First Degree AV Block (PR > .20 sec [1 big box])
II
P P P
.36
Site of delay most commonly the AV node, but may be localized to the His-Purkinje system

Second Degree AV Block - Type I (Wenkebach or Mobitz I Block)
P P P P
Block
II
• Example of 3:2 conduction ratio; general pattern, n:n-1• Note PR prior to block and post-block• Characteristic of AV nodal site of block

II
Block
P P P PP
• 4:3 conduction ratio• Note first RR longer than second RR
Second Degree AV Block - Type I(Wenkebach or Mobitz I Block)
II
P P P P P P
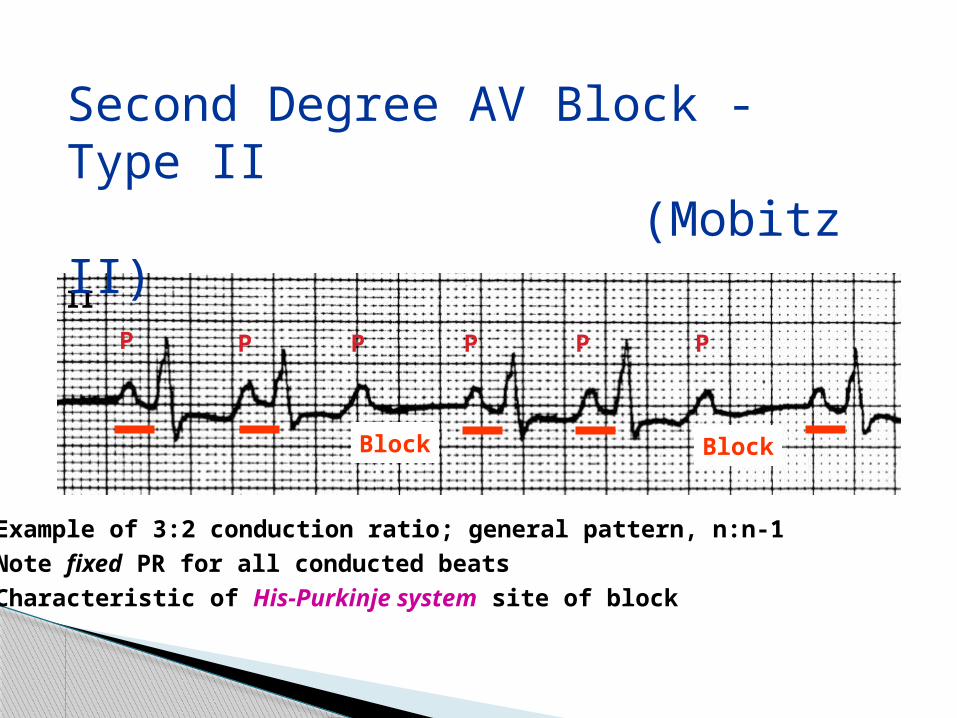
Second Degree AV Block - Type II (Mobitz II)
• Example of 3:2 conduction ratio; general pattern, n:n-1• Note fixed PR for all conducted beats• Characteristic of His-Purkinje system site of block
Block Block

Third Degree AV Block(Complete Heart Block)
V1 P P P PP
• P waves at 50-60 beats/min• QRS complexes (ventricular escape rhythm) at 35 beats/min• Atrial and ventricular activity are completely unrelated• Ventricular escape rhythm suggests His-Purkinje site of block
Represents the ventricles depolarizing (firing) collectively.
Origin of all ventricular rhythm
Rate of about 20-40 bpm
QRS complex
1. is there a P-wave for every QRS? P-waves are upright and uniform One p-wave preceding each QRS
2. Is the rhythm regular or irregular? Verify by assessing R-R interval Confirm by assessing P-P interval
3. What is the rate? Count the number of beats occuring in one minute Counting the p-wave will give you the atrial rate Counting the QRS will give you the ventricular rate
EKG interpretation
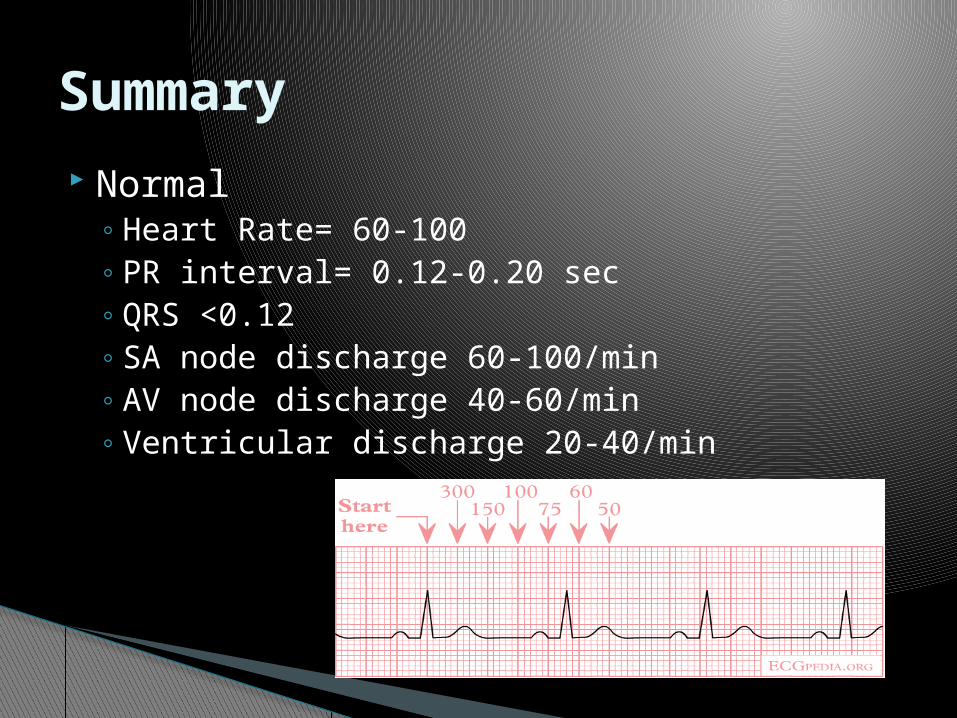
Normal◦ Heart Rate= 60-100◦ PR interval= 0.12-0.20 sec◦ QRS <0.12◦ SA node discharge 60-100/min◦ AV node discharge 40-60/min◦ Ventricular discharge 20-40/min
Summary
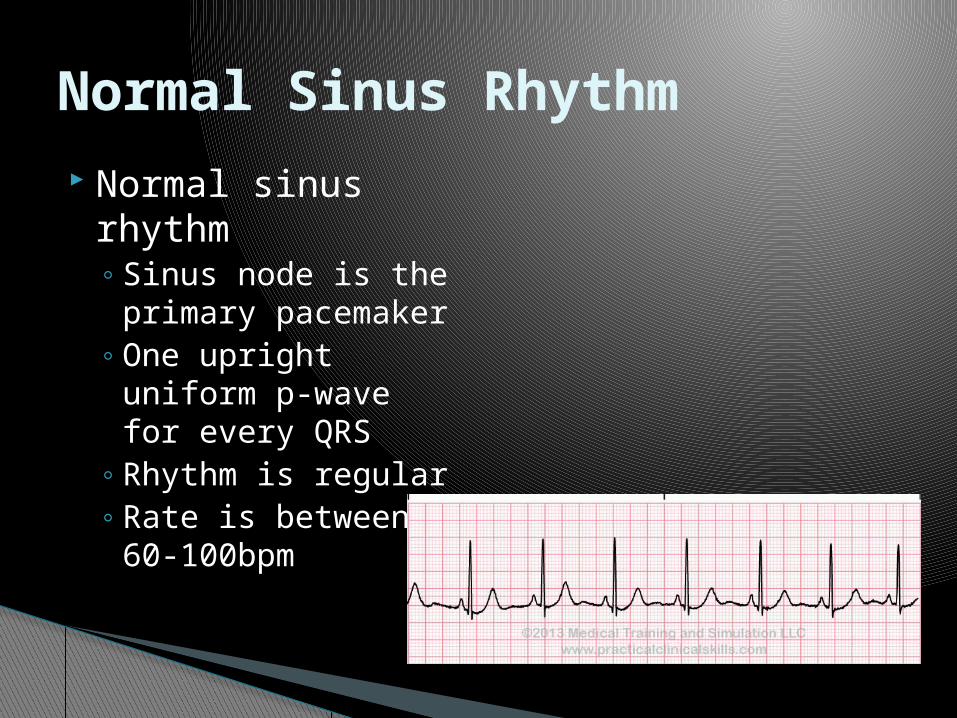
Normal sinus rhythm◦ Sinus node is the
primary pacemaker◦ One upright uniform
p-wave for every QRS
◦ Rhythm is regular◦ Rate is between 60-
100bpm
Normal Sinus Rhythm
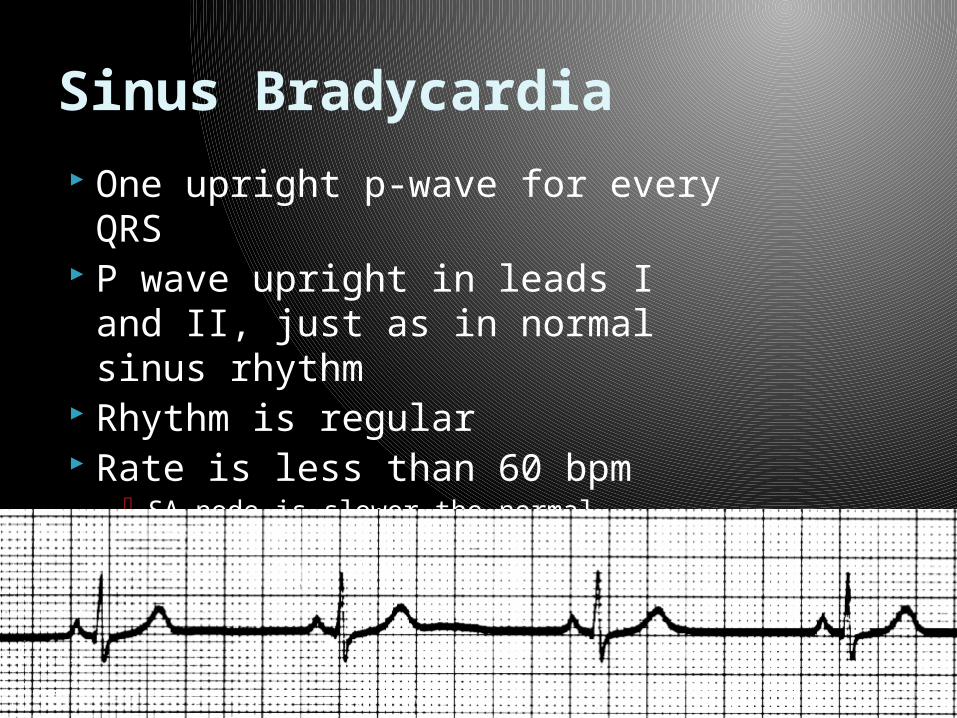
One upright p-wave for every QRS
P wave upright in leads I and II, just as in normal sinus rhythm
Rhythm is regular Rate is less than 60 bpm
SA node is slower the normal Normal for many individuals
Sinus Bradycardia
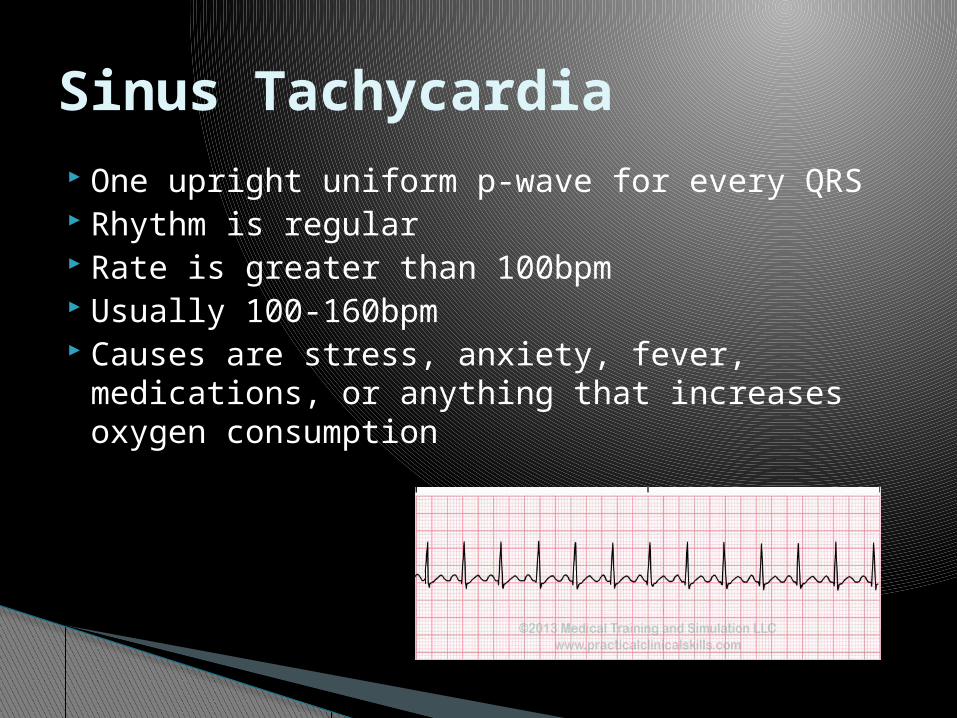
One upright uniform p-wave for every QRS Rhythm is regular Rate is greater than 100bpm Usually 100-160bpm Causes are stress, anxiety, fever,
medications, or anything that increases oxygen consumption
Sinus Tachycardia

One upright uniform p-wave for every QRS
Rhythm is irregular Rate increases are you
breath in Rate decreases as you
breath out
Sinus Arrthymia
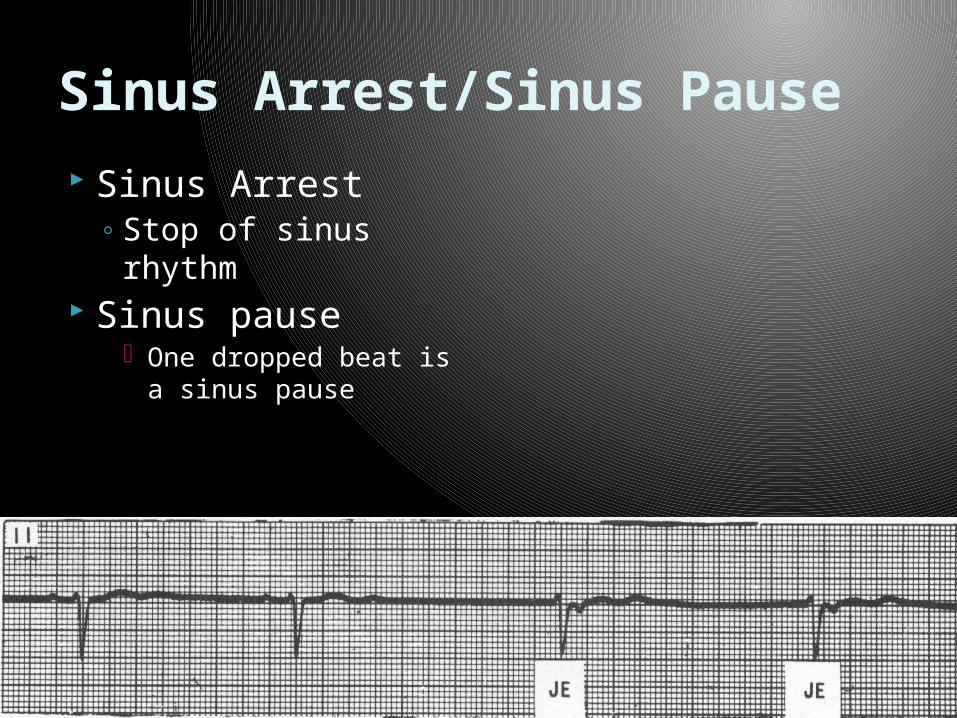
Sinus Arrest◦ Stop of sinus rhythm
Sinus pause One dropped beat is a
sinus pause
Sinus Arrest/Sinus Pause

No discernible p-waves preceding the QRS
Rhythm is grossly irregular
If HR is > 100 it is considered controlled, if HR is greater than 100 it is considered RVR
AV node acts as a “filter” blocking most of the impulses sent by the atria in attempt to control heart rate
Atrial Fibrillation
Background Most common cardiac arrhythmia in adults in
USA 3.1 million patients in 2005; 7.6 million by 2050
Lifetime risk 26% for men, 24% women
10% of all patients over 80 have AF
> 50% of all AF patients are 80 years or older
Lloyd-Jones DM, et. al, Circulation. 2004;110(9):1042Naccarelli GV et. Al, Am J Cardiol. 2009;104(11):1534
Atrial fibrillation
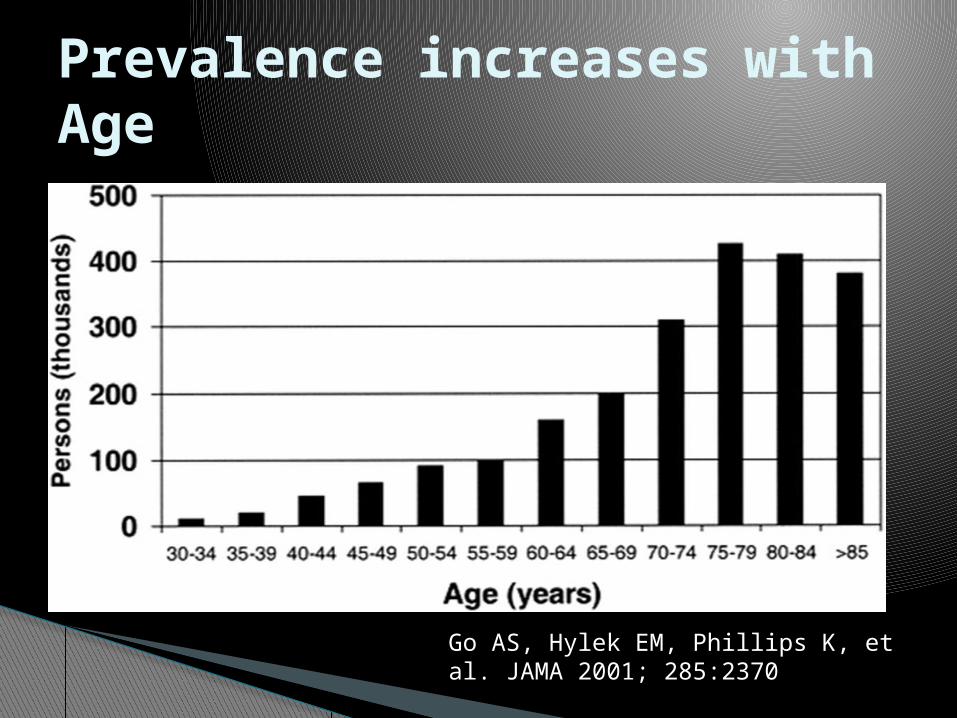
Prevalence increases with Age
Go AS, Hylek EM, Phillips K, et al. JAMA 2001; 285:2370
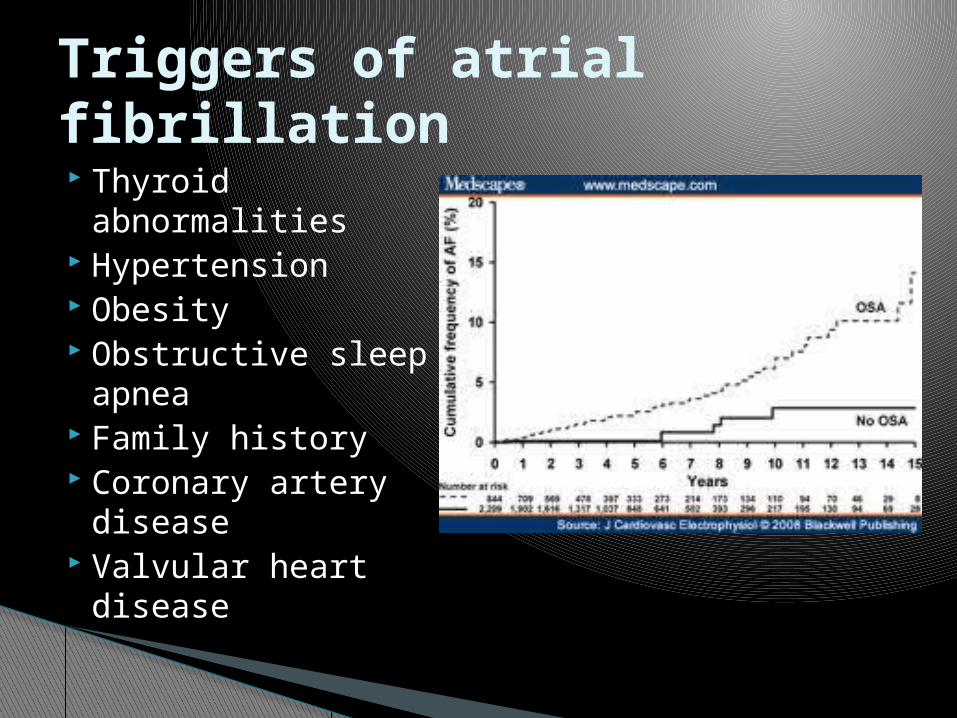
Thyroid abnormalities
Hypertension Obesity Obstructive sleep
apnea Family history Coronary artery
disease Valvular heart
disease
Triggers of atrial fibrillation

Rhythm Control Options
A) cardioversion B) anti-arrthymic
medications C) pulmonary vein
isolation/atrial fibrillation ablation if patient fails AA.
Rate control◦ AV nodal blocking
agents such as beta blockers or calcium channel blockers
◦ Pacemaker/AV node ablation
◦ Anticoagulation◦ Holter monitor to
assess average ventricular rate
Treatment of atrial fibrillation
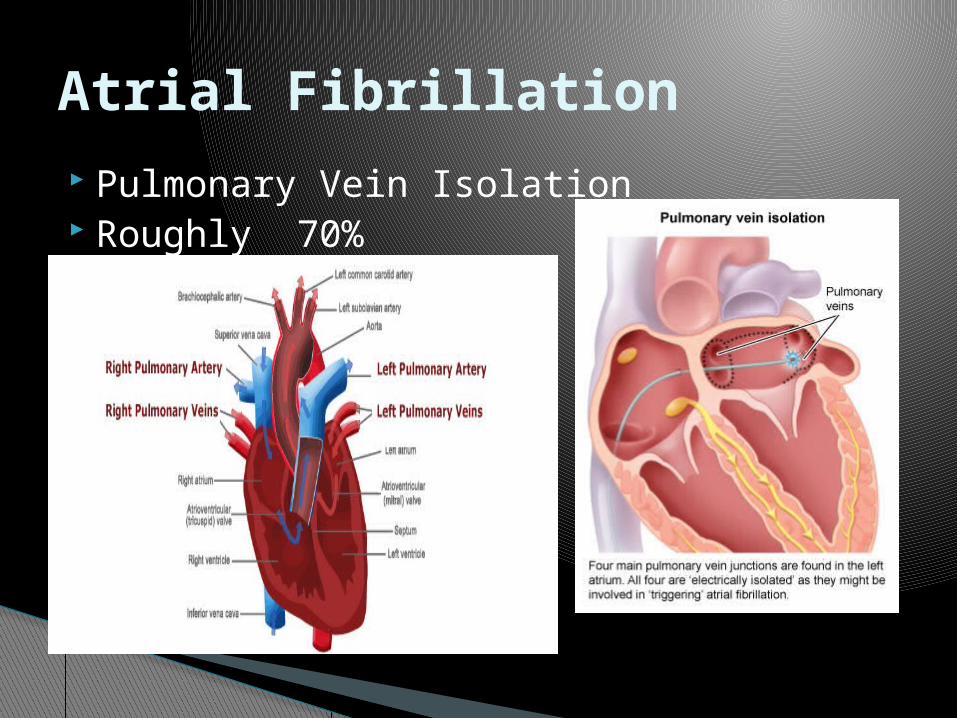
Pulmonary Vein Isolation Roughly 70%
Atrial Fibrillation
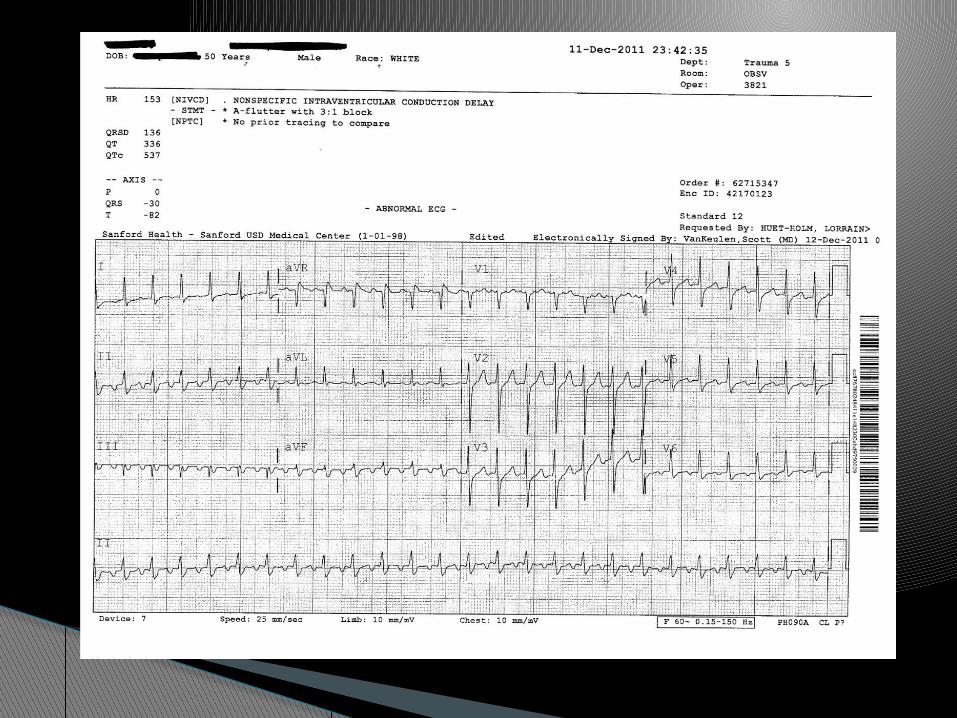
Typical vs atypical atrial flutter. Right sided vs left sided.
More than one p-wave for every QRS complex
Demonstrates a “sawtooth” appearance Classified as ratio of p-waves per QRS.
(ex: 3:1 flutter)
Atrial Flutter


3 Main types◦ 1). AVNRT-AV nodal re-entry tachycardia
◦ 2). AVRT- accessory bypass tract
◦ 3). Atrial Tachycardia
SVT


Roughly 10% of the population has dual AV nodal physiology
Most common type of SVT
Comes on “like a light switch”
Can attempt vagel maneuvers to terminate
AVNRT (AV Nodal Re-entry tachycardia)
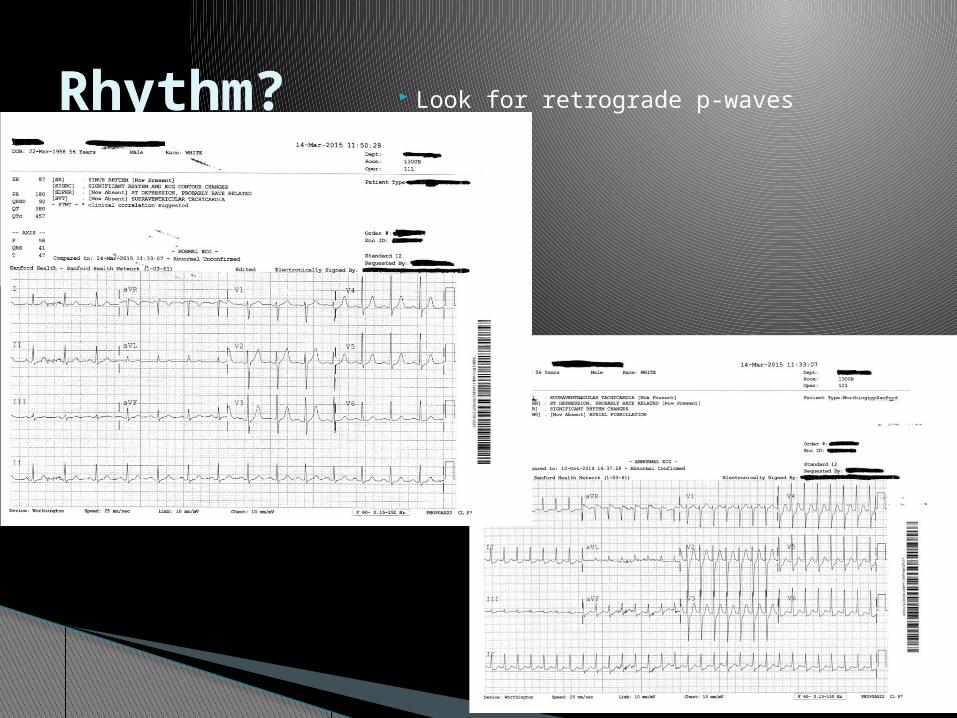
Look for retrograde p-wavesRhythm?
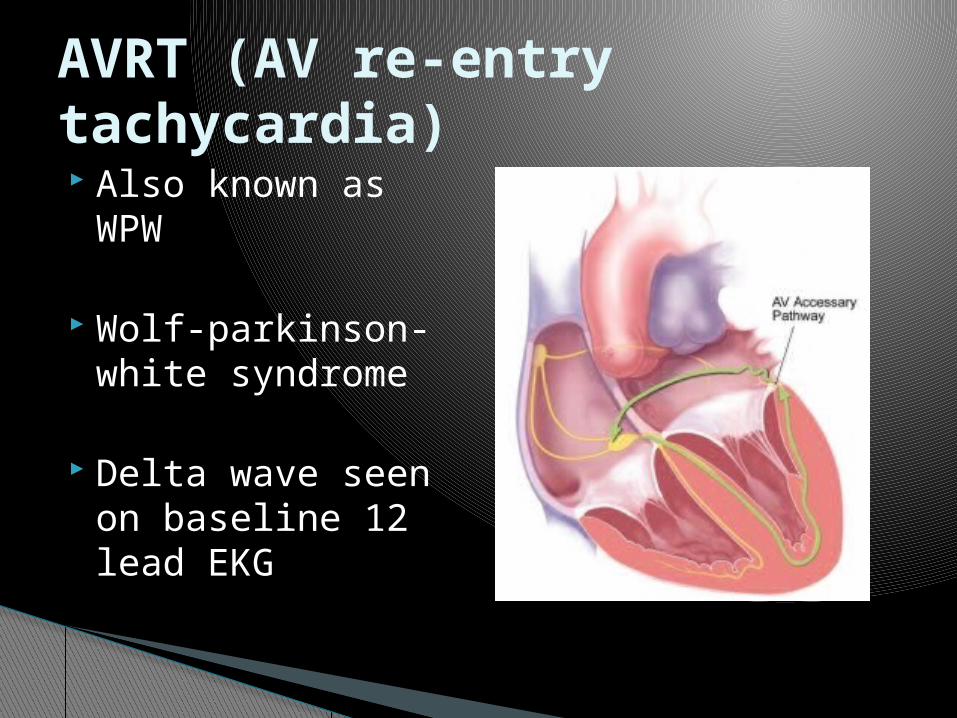
Also known as WPW
Wolf-parkinson-white syndrome
Delta wave seen on baseline 12 lead EKG
AVRT (AV re-entry tachycardia)

Delta wave
Pre-excitation on EKG

Atrial tachycardia is a form of SVT.
Impulse originating within the atria but outside the sinus node
Can be multifocal or unifocal
Known to cause cardiomyopathy if untreated especially in asymptomatic patients
Atrial Tachycardia
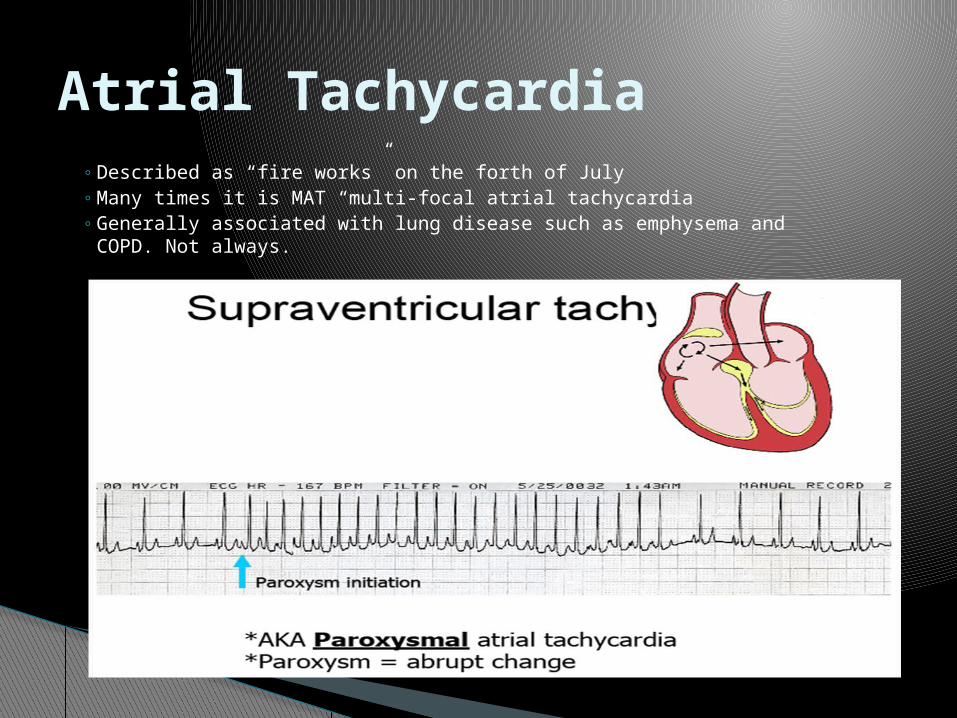
◦ Described as “fire works” on the forth of July◦ Many times it is MAT “multi-focal atrial tachycardia◦ Generally associated with lung disease such as emphysema and COPD.
Not always.
Atrial Tachycardia
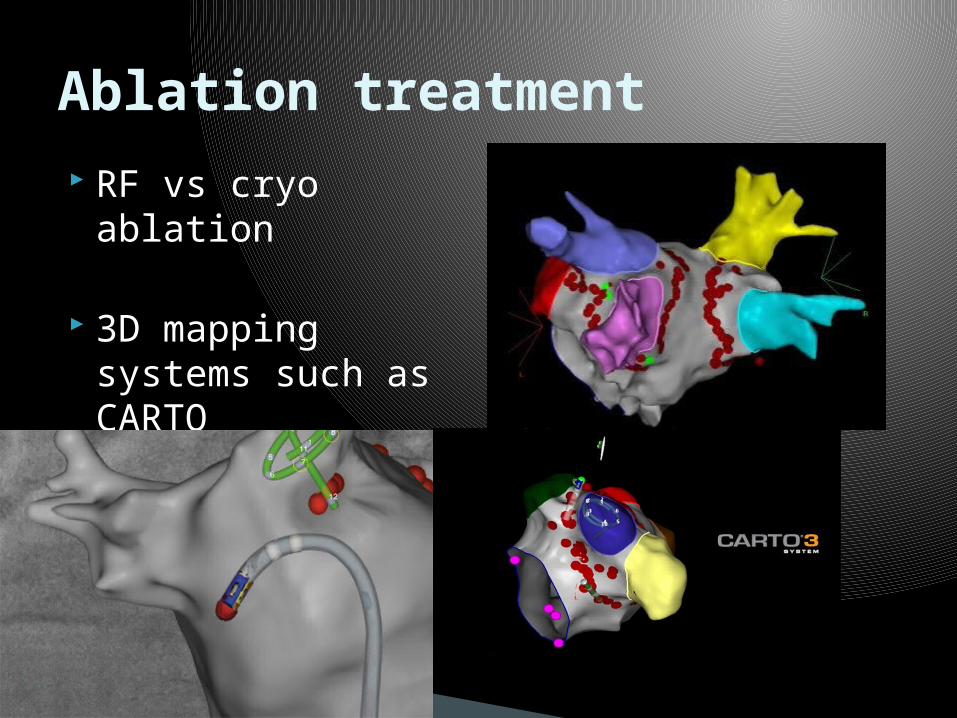
RF vs cryo ablation
3D mapping systems such as CARTO
Ablation treatment
48 year old male: chief complaint palpitations- couple times a week
Large anterior MI 8 months ago, LAD was stented
EF 38%, mild MR NYHA 2 Meds- asa, plavix, lisinopril 20mg daily,
Metoprolol succinate 75mg bid
Case Studies
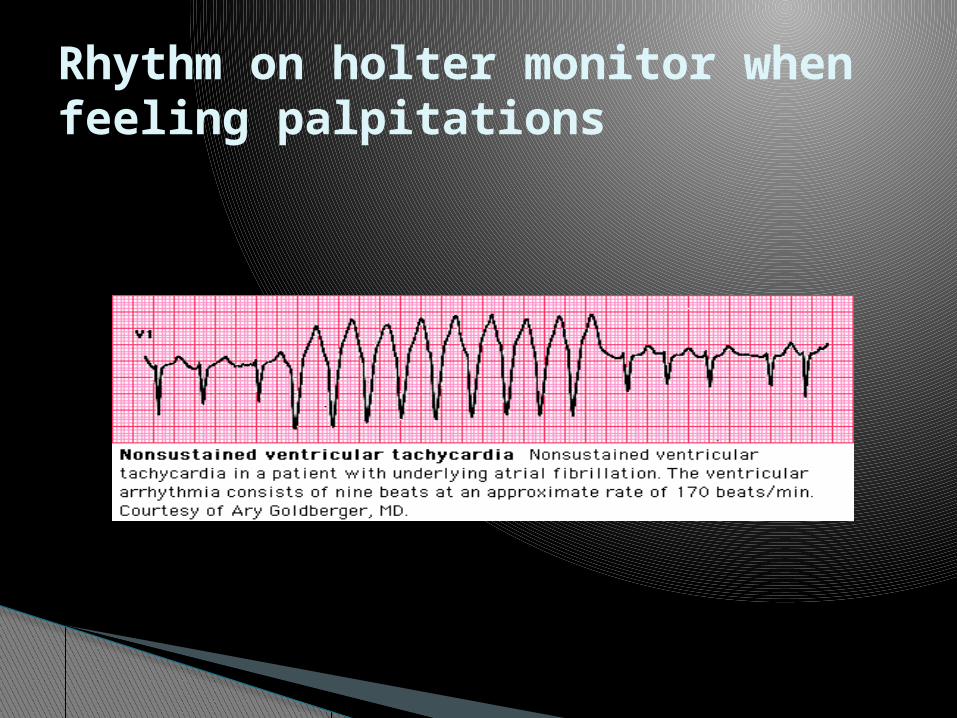
Rhythm on holter monitor when feeling palpitations
Add sotalol?
Add amiodarone?
ICD implant?
EP Study?
What would you do? Next Step
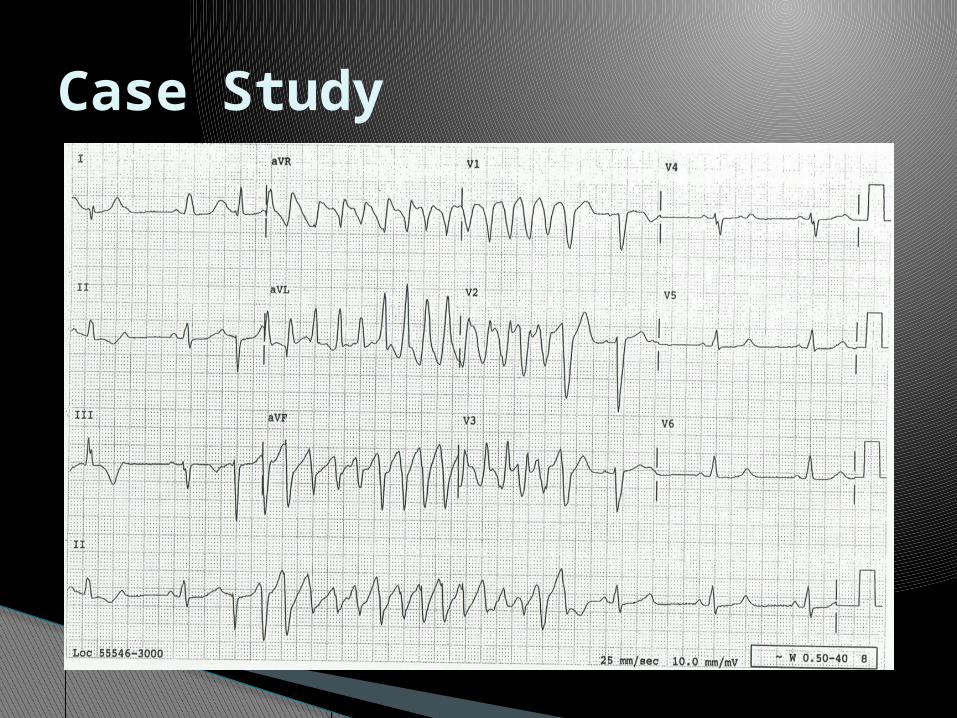
67 year old female admitted for syncope
EP consult to evaluate rhythm
Case Study
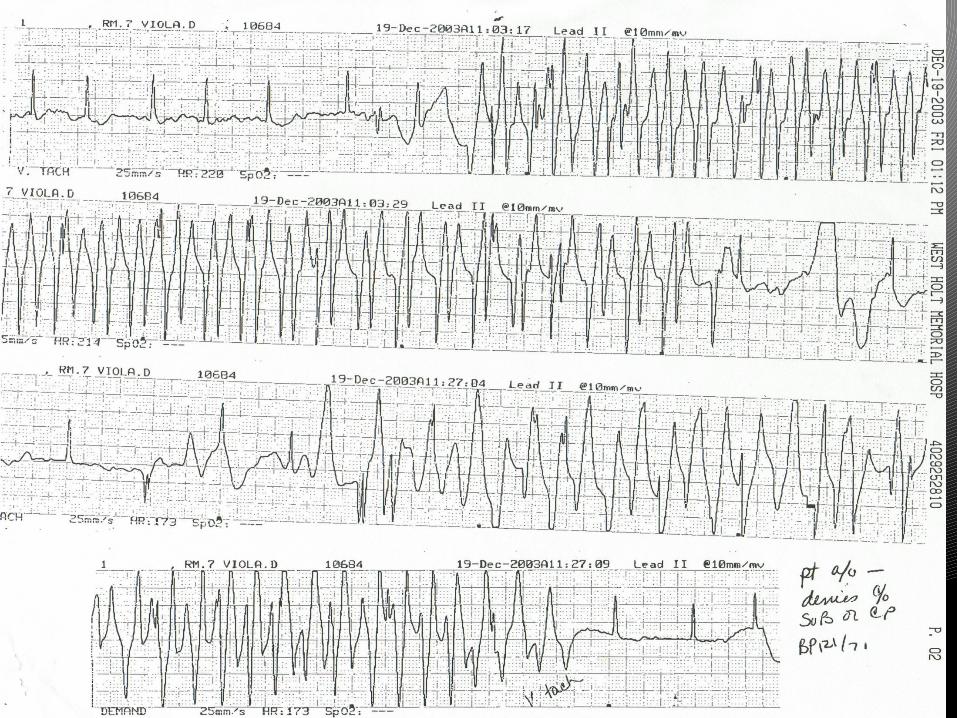
A) SVT
VT
Torsades
??
What is your diagnosis?

24 year old female referred to cardiology for palpitations by her PCP
Previously healthy Meds: BCP, levaquin for bronchitis, MVI Smoke 1 ppd x 5 years
Case Study
Case Study
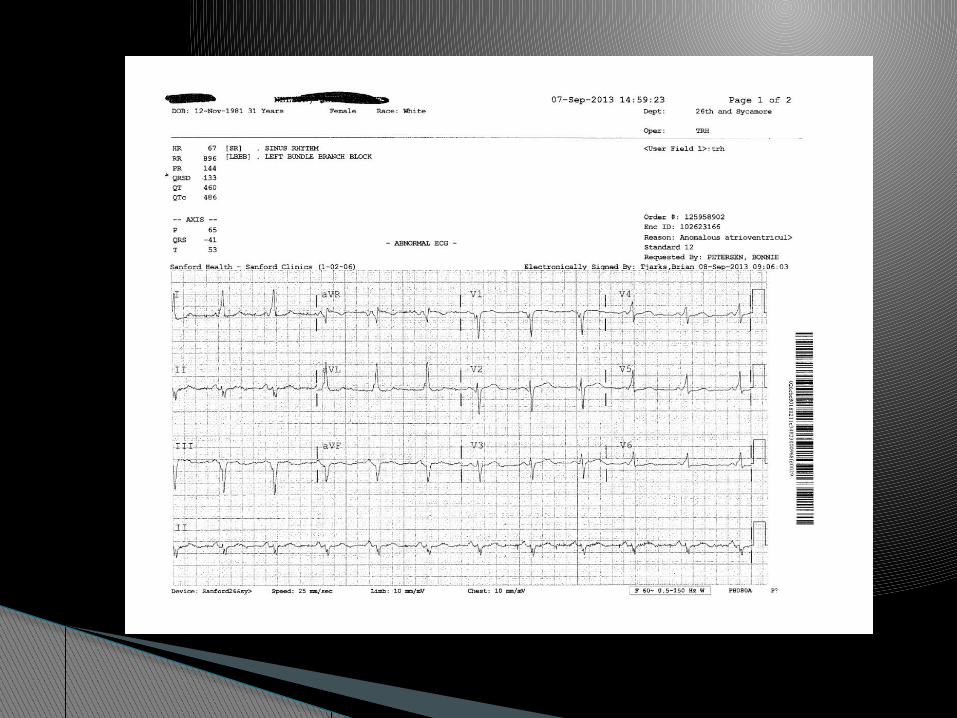
33 year old female who was referred by her PCP.
Had a baseline EKG done for life insurance puposes
Case Study

Refused EP Study when offered. She was placed on BB and flecainide.
Was admitted on with palpitations.
Case Study

