presentation: asia pacific’s health trends-obesity, ncds and adb’s operational plan for...
DESCRIPTION
Presented by ADB's Dr. Susann Roth at the ADB Institute during a consultation meeting last 15 December 2015 in Tokyo.TRANSCRIPT

December 2015
Asia Pacific’s health trends-
Obesity, NCDs
and
ADB’s Operational Plan for Health 2015-2020
Dr. Susann Roth, Senior Social Development Specialist
Disclaimer: The views expressed in this paper/presentation are the views of the author and do not necessarily reflect the views or policies of the Asian Development Bank (ADB), or its Board of Governors, or the governments they represent. ADB does not guarantee the accuracy of the data included in this paper and accepts no responsibility for any consequence of their use. Terminology used may not necessarily be consistent with ADB official terms.
Outline
1.Obesity and NCDs in Asia Pacific
2. Asia Pacific’s health systems
3. ADB’s support to DMCs- The Operational Plan for Health 2015-2020
4. ADB-ADBI collaborations for better evidence based policy making

Outline
1.Obesity and NCDs in Asia Pacific
2. Asia Pacific’s health systems
3. ADB’s support to DMCs- The Operational Plan for Health 2015-2020
4. ADB-ADBI collaborations for better evidence based policy making

1. Obesity and NCDs in Asia Pacific
How do you define overweight and obesity?
Body Mass Index (WHO)
• a BMI greater than or equal to 25 is overweight
• a BMI greater than or equal to 30 is obesity.
What are non-communicable diseases risk associated to overweight and obesity?
• Cardiovascular diseases (mainly heart disease and stroke)
• Diabetes
• Musculoskeletal disorders (especially osteoarthritis)
• Some cancers (endometrial, breast, and colon)

Asia and the Pacific is getting
“fatter” and older
5

Asia Pacific’s population’s diet is
carbohydrate and fat rich
Source: The Blueprint for Chance Program Novo Nordisk. 2013

Expected economic output loss for
Indonesia: $4.47 trillion lost due to NCDs
Source: Background paper for World Economic Forum. Economics of non-communicable
diseases in Indonesia. 2015

Diabetes incidence is increasing faster in
developing countries
Source: The Blueprint for Chance Program Novo Nordisk. 2013

Economic burden from NCDs in increasing

Example: Singapore is investing in
healthy nutrition
Return of
Investment
> 1,1%
Situation High consumption of saturated
fat and sugar
Intervention Training of cooks of foot stalls
and restaurant use health oil
and less sugar
Investment • SGD 8M in saturated fat intake reduction program through grants
• To cover the average costs of price differences between
the healthier and regular ingredient
Result 23%reduction in coronary heart disease incidence
averting 1,860 unhealthy life years in 2020
Economic benefits of SGD 102M2

Epidemiological transition in Viet Nam (hospital cases)
59.2
37.6
24.9 19.8
39
50
62.4
71.6
1.8
12.4 12.7 8.6
0
10
20
30
40
50
60
70
80
1986 1996 2006 2010
Communicable diseases Non-Communicable diseases Injuries, poisoning
National Insurance Agency Viet Nam
NCDs Increase health care costs

12
1,700,000,000,000
170,000,000,000
Cost of
inaction in developing countries globally:
US$ 1.7 trillion (2015)
Cost of
action
in developing countries
US$ 170 billion (2015)
Fighting NCDs: Sooner rather than later
Source: Interim Report of the WHO Working Group of Financing for NCDs

13
Cost of
inaction in developing countries:
US$ 1.7 trillion (2011-2015)
Cost of
action
in developing countries
US$ 170 billion (2011-2015)
Source: Interim Report of the WHO Working Group of Financing for NCDs
Population risk factors
Primary care
• CVD & diabetes
• Cancer
Tobacco use Alcohol use Obesity/
Diet/inactivity
Less than
$0.40 - $1
Prevention annual costs per person
Fighting against NCDs is not expensive

Low availability of essential NCD medicines
in low & middle income countries
65
57.1
43.1 40.3
45.1
65.6
49.5
34.7 30.1 29.4 27.8
56.1
0
10
20
30
40
50
60
70
Mea
n a
vaila
bili
ty (
%)
Private sector Public sector
From Cameron et al. Bull World Health Organ 2011;89:412–421.
Antidiabetics
Antihypertensives
Antidepressants
Acute medicines
Higher priority still given to acute medicines
65%
57%
45%
67%
50%
35%
28%
56%
Public sector Private sector Mean availability
NCD medicines

Access to Insulin in Indonesia is low Leading to expensive diabetes related complication
Source: The Blueprint for Chance Program Novo Nordisk. 2013

Population impoverished
purchasing essential NCD medicines Country % pop.
below US$ 2 / day
% population below poverty line after generic medicine purchase (1 month supply)
Salbutamol inh.
Glibenclamide
Atenolol Amoxicillin
Pakistan 8 13* 12 12 21
Uzbekistan
38 46 43 41 58
Indonesia
4 20* 6 12 9
Philippines
21 28 29 28 32
Population impoverished by medicine purchase
16 countries
Total pop. 71 m 112 m 133 m
Patient pop.
2 m 5 m 29 m
*Brand purchase; no generic available
From Niens et al. PLOS 2010; 7(8):e1000333
B E F O R E
% of people living on less than $2 a day
A F T E R
8 % Pakistan
4 % Indonesia
Philippines
Uzbekistan
21 %
38 %
12 - 21 %
6 - 20 %
28 - 32 %
41 - 58 %
4% 13% 4%
2% 5% 8%
8% 11% 7%
5% 20% 3%

Preventing overweight and obesity is a
public health best buy

Outline
1.Obesity and NCDs in Asia Pacific
2. Asia Pacific’s health systems
3. ADB’s support to DMCs- The Operational Plan for Health 2015-2020
4. ADB-ADBI collaborations for better evidence based policy making

2. Asia Pacific Health Systems
In-equitable access to
quality health care
Countries commitment to Universal Health
Coverage (SDG 3)
but reform process is slow
Aging
Urbanization
NCDs
Demand Supply
Government commitment

Health spending grows faster than income
Source: HEALTH AT A GLANCE: ASIA/PACIFIC 2012 © OECD 2012 (official WHO data)
.

0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Health expenditure,public (% of totalhealth expenditure)
External resources forhealth (% of totalexpenditure on health)
Out-of-pocket healthexpenditure (% of totalexpenditure on health)
21
Out-of pocket payments remains high

LICs and MICs are aiming for UHC
To do:
• Introduce essential packages for the poor and vulnerable
• Improve quality of essential care
• Improve quality and quantity of health workforce
Low Income
Countries
Financial
Protection and
quality low
To do:
• Purchase of
services from
private sector
• Provide services
for poor and
vulnerable
• Improve quality,
efficiency Coverage and
quality low
Middle Income
Countries

23

To ensure healthy lives and promote wellbeing for all at all ages
Reduce maternal mortality
Reduce child and neonatal mortality End epidemics of HIV, TB, malaria and NTD, and combat hepatitis, water-borne diseases and other
communicable diseases
Reduce mortality due to NCD and improve mental health
Strengthen prevention and treatment of substance abuse (narcotics, alcohol)
Reduce mortality due to road traffic injuries Universal access to sexual and reproductive health-care services
Achieve universal health coverage Reduce deaths and illness due to pollution and contamination
Strengthen implementation FCTC (tobacco)
Access to affordable essential medicines and technologies
Increased health financing and health workforce in developing countries
Enhance capacity for early warning, risk reduction and management of national and global health risks
Targets
3.1
3.2 3.3
3.4
3.5
3.6
3.7
3.8
3.9 3.a
3.b
3.c

Countries are implementing
Social Health Insurance
CHARACTERIZED BY
• Quasi-Independent and
Protected (Pooled) Fund with
Autonomy
• Split between Financing and
Provision
• Funded by payroll taxes and
government revenues
• Entitlements because of your
citizenship and not because of
your job (universality of
population coverage)
DRIVING
• Strategic Health Purchasing for
Results, Outcomes and Outputs
• Leveraging Payments to
ensure:
– Enhanced Efficiency
– Equity and Fairness
– Quality of Care
– Comprehensive Health Services
(primary care, medicines,
referral, hospital)
• Harnessing the private sector
• Empowerment of the insured
– “you do not owe the
provider a favor”
25

• Latest amendment in Health Insurance
law in 2014 now calls for Universal Health
Insurance (UHI)
• Poor (and other populations – war
veterans, soldiers, widows) are subsidized
by the government
• Under-six children ALL covered
• Massive investments in supply side using
“Health Bonds”
• (Explicit) premium subsidies for ALL
informal sector
• Developing NCD insurance packages
Viet Nam
26

• In 2004, decided to have a single health insurance fund
– Survived legal challenges and finally implemented of national health insurance program (JKN) in 2014
– All five health insurance funds pooled into a single fund
• Targets universal health insurance coverage by 2019
– Currently, 63% (151.5 million people) are covered
– Poor (individually determined by provinces) are subsidized by the government
• Government and private providers are
contracted
– ALL required NOT to charge co-payments or to balance bill
Indonesia
27
• National Health Insurance enacted in 1995
• PhilHealth (a government corporation) was established to run the NHI with policies set by its governing board
• In 1997, two health funds were
consolidated into one fund. The third fund (the overseas Filipino health insurance fund) was incorporated in 2005
• Poor are subsidized by the government (increased subsidies by 2012/13 with sin taxes earmarked to increase/sustain the subsidies)
• Government and private providers are contracted
Philippines
28

UHC Coverage is still very low in the region
Outline
1.Obesity and NCDs in Asia Pacific
2. Asia Pacific’s health systems
3. ADB’s support to DMCs- The Operational Plan for Health 2015-2020
4. ADB-ADBI collaborations for better evidence based policy making
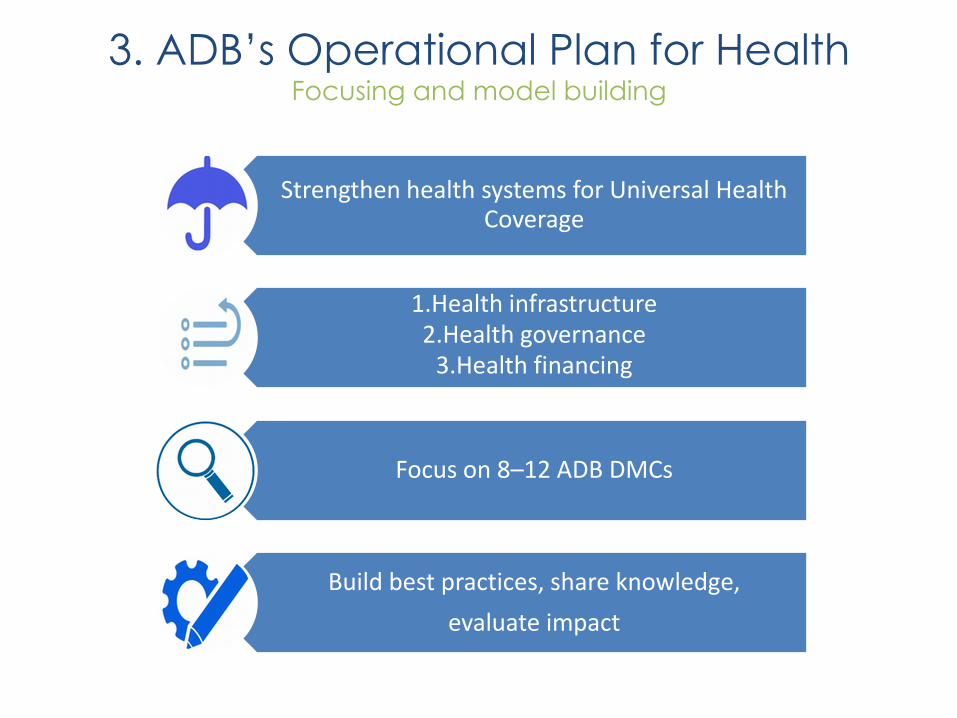
3. ADB’s Operational Plan for Health
Focusing and model building
Strengthen health systems for Universal Health Coverage
1.Health infrastructure 2.Health governance
3.Health financing
Focus on 8–12 ADB DMCs
Build best practices, share knowledge,
evaluate impact

Integrated Hospital Care
• Pooling of State and health insurance funds • Improving quality of care for disadvantaged
groups, introducing evidence based care and standards
Project link
Innovative feature
Impact
Partnerships
The next big thing
• MON - Fourth Health Sector Development Project
• Fourth Health Sector Development Project (Additional Financing)
• Fifth Health Sector Development Project
• Infrastructure investment to develop model hospitals backed by strong ICT systems
• Hospital and primary care network with referral system
• Financial autonomy of hospitals
Improved quality of health services
WHO

• Interconnected network of sentinel laboratories for early warning
• Health insurance portability between GMS countries
Project/program link
Innovative feature
Impact
Partnerships
The next big thing
• GMS Communicable Diseases Control Projects 1 + 2 (existing) in CAM, LAO and VIE
• GMS Health Security Loan (in preparation for 2016) (MYA included)
• Regional cooperation on public goods • Infrastructure projects integrate preventive
health activities (HIV) • Neighboring provinces establish cross-border
diseases surveillance, response to epidemics, patients referrals.
Control of communicable diseases with epidemic potential, malaria elimination.
WHO, Global Funds, IOM, International NGOs

• Intersectoral convergence of urban health • Patient centric Health Information System
Management • Service delivery through performance based
PPP models
Project/program link
Innovative feature
Impact
Partnerships
The next big thing
• IND-Support for National Urban Health Mission
• (learning from BAN-Urban Primary Health Care Services Delivery Project)
• Innovation creation for service delivery models and knowledge generation in urban health integrated as Disbursement Linked Indicators
• First Result Based Loan in health
Better health for urban poor

• ICT in health, big data analysis • Benchmarking of prices for services • Harnessing the private sector • Service delivery through performance based
PPP models
Project/program link
Innovative feature
Impact
Partnerships
The next big thing
• PAK- Benazir Income Support Program • MON- Fourth Health Sector Development
Project (Additional Financing)
• Innovation creation for service delivery models and knowledge generation in urban health integrated as Disbursement Linked Indicators
• First Result Based Loan in health
Improved health outcomes, Sustainable financing
University of Seoul

ADB is collaborating with
Centers of Excellence

Outline
1.Obesity and NCDs in Asia Pacific
2. Asia Pacific’s health systems
3. ADB’s support to DMCs- The Operational Plan for Health 2015-2020
4. ADB-ADBI collaborations for better evidence based policy making

38
4. ADB-ADBI collaboration
Urban Health Analyzing the impact of housing on health
NCDs
Economic impact of
NCD risk factors such as
Obesity
NCD prevention
Developing the economic
argument for investing in disease
prevention
?

Dr. Susann Roth – [email protected]
LinkedIn: https://ph.linkedin.com/pub/susann-dr-roth/15/29a/940
Twitter: https://twitter.com/adb_susannr
Blog: http://blogs.adb.org/author/health-team
Health Sector Website: http://www.adb.org/sectors/health/main
For more information

Knowledge Product pipeline Opportunities for knowledge collaboration
ADB’s working paper series 2015-2016 • Pharmaceutical policy/regulatory convergence for better access
to malaria and other communicable diseases treatments
• Unique identifiers for malaria elimination, links to civil registration
and vital statistics and UHC, with reference to in-country landscape analyses
• From malaria surveillance to sustainable e-health architecture
• Interoperability lab for better HMIS
• Malaria surveillance in the GMS • Urban Health in Asia and the Pacific
• Social Health Insurance- From Design to Implementation
• The Business Case of investing in NCD Prevention
• Health Public Private Partnership in Asia and the Pacific • The UHC Dashboard- Why measuring UHC matters