preop assessment / plan / infection control
TRANSCRIPT

Pre-op AssessmentAnesthetic PlansInfection Control
N Clavel [email protected]
Anesthesia Ottawa HospitalNov 14, 2009

Pre-Op EvaluationWHY?Establish patient-doctor relationshipBecome familiar w surgical illnessBecome familiar with coexisting diseaseDevelop an anesthetic planObtaining informed consent for anesthesiaOffer anesthetic options along w risks/benefitsAlleviate patient anxietyGOALS?Reduction of perioperative mortality & morbidity

HISTORY
HOW?Chart reviewPatient interviewDiscrete discussion with medical/surgical staff

HISTORY
1) Current status of patient2) Coexisting disease3) Medications4) Allergies and Drug Reactions5) Anesthetic history6) Social history7) Review of Systems

Patient Status
• S&Ss of current surgical condition• Relevant diagnostic tests• Review presumptive diagnosis• Initial treatments• Treatment response thus far• Vitals• Fluid balance

Co-existing DiseaseEvaluated using a “systems-based” approach
Emphasis on recent changes in symptoms/signs/treatmentConsults if strange lab results, medications, dramatic
decline in patient condition

MedicationsNamesDoseSchedule
Most important are :antihypertensive antianginalantiarrhythmic anticoagulantanticonvulsant endocrine (insulin, steroids)
Most medications can be continued up to time of surgery

Steroid Replacement?Hypothalamic-pituitary-adrenal
axis suppressionCan’t increase adrenal cortisol
output to match surgical stress
Occurs after >7-10 dys therapyCortisol secretion in adults :
Major surgery :75-150 mg Minor surgery : 50 mg
Controversial replacement strategies

HypoadrenalismCirculatory InstabilityDiscrepancy btw disease state and
presentation of patient :nauseavomitingorthostatic hypotensiondehydrationacute adrenal hemorrhagefatigueweight loss

Incidence of Allergy
Muscle Relaxants (70%) Latex (12%)Colloids (4%) Hypnotics (4%)Antibiotics (8%) Other (2%)Benzos (<2%) Opiods (<2%)

Allergies & Drug Reactions
True allergic reactions are relatively uncommon
TRUE REACTIONDocumented, direct observation, clear pt hxSkin manifestation (hives, pruritis, flushing)Facial/oral edemaSOB/choking/wheezingVascular collapse/arrest

Allergies
1) ANTIBIOTICSsulfonamides, penicillins, cephalosporins
Antibiotic Class Common Use
Cefazolin(ancef)
First GenCephalosporin
Gram + , skin flora
Cipro Fluoroquinolones Gram – rods
Vancomycin Other Gram + , MRSA, pneumococci, enteroccoci
Flagyl Other Anaerobes
Cefotax Third GenCephalosporin
Broad Gram - / + & some anaerobes
Levoquin Third GenFluoroquinolones
Gram –rods, some gram +
Piptazo Extended Spectrum Penicillin
Gram + , Most gram – rods (incl enterobacter, serratia, pseudomonas)
Meropenem Carbapenem Gram +, Gram -, anaerobes (not MRSA, not VRE)

Allergies 2) PROPOFOL
soyabean oil and egg yolk components3) VOLATILES or SUCCINYLCHOLINE
possible malignant hyperthermiahalothane hepatitisplasma cholinesterase abnormality
4) ESTER LOCAL ANESTHETICSr/o intravascular epinephrine procaine, chlorprocaine, tetracaine

Adverse Drug Reactions
Many periopoerative medications can cause unpleasant side effects :
nausea vomitingsedation constipationpruritis tachycardianumbness “locked in”

Anesthetic HistoryResponse to sedation / pain medicationVascular access and invasive monitoringEase of ventilation, Mallampati, ETT/LMA size,
MAC #, Mask sizePerioperative complications
Drug reactions, intra-op awareness, dental trauma, post-op nausea & vomiting, EKG changes, peri-op MI, CHF, admission to ICU, prolonged emergence, reintubation
Past patient experienceTrauma, side effects, post-op pain control, neurologic deficits, regional, hoarseness

Airway history
Prior anesthetic records:(number of intubation attempts, ability to B/M, type of laryngoscope blade, stylet, adjunct, RSI)
Specific symptoms related to airway compromise :( hoarseness, stridor, wheezing, dysphagia, dyspnea, positional airway obstruction )

Family History
“Has anyone in your family experienced unusual or serious reactions to anesthesia?”
MHEnzyme deficienciesCongenitalConnective Tissue d/oMuscular Dystrophies

Malignant Hyperthermia
Triggers :volatile anesthetics, succinylcholine
Hypermetabolic state :Tachycardia, HTN, Hypercarbia, Hypoxemia, Metabolic acidosis, Hyperkalemia, Muscle rigidity, Hyperthermia, Renal failure, DIC, Death
Autosomal dominant - ryanodine receptor Dx : muscle biopsy - halothane/caffeine testTx : Dantrolene 10mg/kg (starting dose)

Pseudocholinesterase Deficiency
Found predominately in Indian population
Delay in metabolizing :SuccinylcholineEster local anestheticsMivacurium

Social History & HabitsSMOKING
Will talk about it in more detail …DRUGS (dose, timing, route)
Stimulants = palpitations,angina, wt loss, arrhythmias, seizures
Opioids/ Benzos – increased perioperative requirements
ALCOHOLDecreases anesthetic requirementsPredisposition to hypothermia and hypoglycemiaWithdrawl – HTN, seizures, tachycardia, tremors, delerium, increased anesthetic requirements

Laboratory Studies
Hematological studies1) Risk of blood loss2) History of anemia3) Coagulopathy4) Cancer
CBC, Plts, INR/PTT

Laboratory Studies
Serum Chemistry1) Chronic kidney disease2) Cardiovascular / Hepatic / Neuro pts3) Diabetes4) Morbid Obesity5) Diuretics / digoxin / steroids / aminoglycosides

EKG
If risk factors for CAD exist HTN, SMOKING, FAM Hx, DM, prev MI
DysrythmiasMen > 45 yrsWomen > 55 yrs

CXR
Heavy Smoking HistoryElderlyPulmonary S & Ss
Lymphadenopathy - hilar PE – V/Q scan & CXR

CXR - systematic review Tests %Abnormal %Chang
e%Events
Routine (8) 21517.4
(2.5–37)0.5
(0–2.1)1.2
(0–6.8)
Routine + Indicated(28)
18913
20 (1.4–60)
2.4 (0–5.9)
1.2 (0–8.8)
Results reported as median (range)Munro J. Health Technol Assess 1997;1:1-62

PFTs
Pulmonary Function TestsEvaluation of bronchodilator therapyThoracic surgery

Special Studies – Difficult A/W
LARYNGOSCOPYDirect, indirect, fiberopticHypopharynx, laryngeal inlet, vocal cord function
CXRTracheal deviation, bony deformities, cervical spine
(trauma, rheumatoid, trisomy)
CT, PFTs, ABGs

Physical Examination
Vital SignsHeight & weightBlood pressureResting HRRespiratory rate
NEED TO KNOW THE BASELINE

Physical Examination
A/WHeartLungsAbdomenExtremitiesBackNeurological Exam

AW Exam


Head and Neck EXAMNOSE
patency of naresMOUTH
macroglossia, facials scars, contractures, TMJ issues, poor dentition
NECKTMD <6cm, mobility of larynx/tissues, palpate trachea, scars, thyroid goitre, paratracheal masses
C-SPINETouch chin to chest, posterior neck extension, lateral rotation w/o pain/paresthesisa
TRACHEOSTOMY/STOMASuspect subglottic stenosis, prior complications with airway management?, use smaller ETT

TMD
Ideal >6cm (4 fingers)3 Fingers : Difficult but
should be able to visulaize the cords
2 Fingers : May only see arytenoids or epiglotis
1 Finger : May not even see epiglotis

OthersMOUTH OPENING
<2.5 cm
ATLANTO-OCIPITAL EXTENSIONNormal = 35’ , Need extension to attain good sniffing position
JAW THRUSTApproximates anterior jaw motion with laryngoscopy

Mallampati Classification
Class 1: Faucial pillars, soft palate, and uvula are visibleClass 2: Faucial pillars and soft palate may be seen. Uvula masked by base of tongueClass 3: Only soft palate is visible. Intubation is predicted to be difficult.Class 4: Soft palate not visible. Intubation is predicted to be difficult.

Arthritis & Cervical Disk Disease
Rheumatoid ArthritisDIFFICULT AIRWAY
cervical spine instability and limitation of mandibularmotionrisk atlantoaxial subluxation and spinal cord injuryhighest risk patients have severe hand deformities and skin nodules

Infection and TumoursFloor of mouth, salivary glands, tonsils, pharynx, Pain, edema, trismus, DIFFICULT AIRWAY limited mouth opening
Mono
viral
Tonils / strep
schwanoma

Tracheal Deviation

Trauma

Previous surgery/radiation
Scarring, contractures, limited tissue mobility

Morbid Obesity

Congenital / SystemicTrisomy 21Atlanto-occipital instability and macroglossiaSclerodermaSkin tightness, decreased mandibular motion,
limited mouth openingAcromegalyMandibular/ tongue/ epiglottis/ vocal cord
hypertrophyDawrfismAtlanto-axial instability, difficult B/M
(micrognathia)
Acromegaly
Scleroderma
Trisomy 21

Congenital
Severe retrognathia , decreased TMD
Pierre -robin
Treacher-collinsgoldenhar

Difficult Intubation
Inability to open mouthPoor c-spine mobilityReceding chin (micrognathia)Large tongue (macroglossia)Prominent IncisorsShort muscular neckMorbid Obesity

Difficult B/M
ObeseEdentulousBeardsCervical arthritis

1965 – Skinner & PearceMortality Risk
1) Intraperitoneal /thoracic sx2) Old MI = 14% & Acute MI = 40% 3) Shock (SBP<100 or diastolic<50) 4) Aortic Valve Dx5) COPD and abdo/thoracic sx. = 37%6) Mild CHF 4% & severe CHF 67%7) AbN EKG8) Emergency sx

Perioperative Risk

Causes of Death at POD #3System implicated % of casesCardiovascular 59 Respiratory 25Renal 22Sepsis 21Hematological 12GI 11Metabolic 10Surgical condition 9CNS 8Hepatic 6
NCEPOD 2002 www.ncepod.org. uk

ASA Physical Status
Gives an overall impression of the complexity of a patient’s medical condition
Class Description I Healthy II Systemic disease no functional limitation III Systemic disease with functional limitation IV Systemic disease with functional limitation
constant threat to life V Moribund unlikely to survive 24 hrs
with or without surgery E Emergency procedure
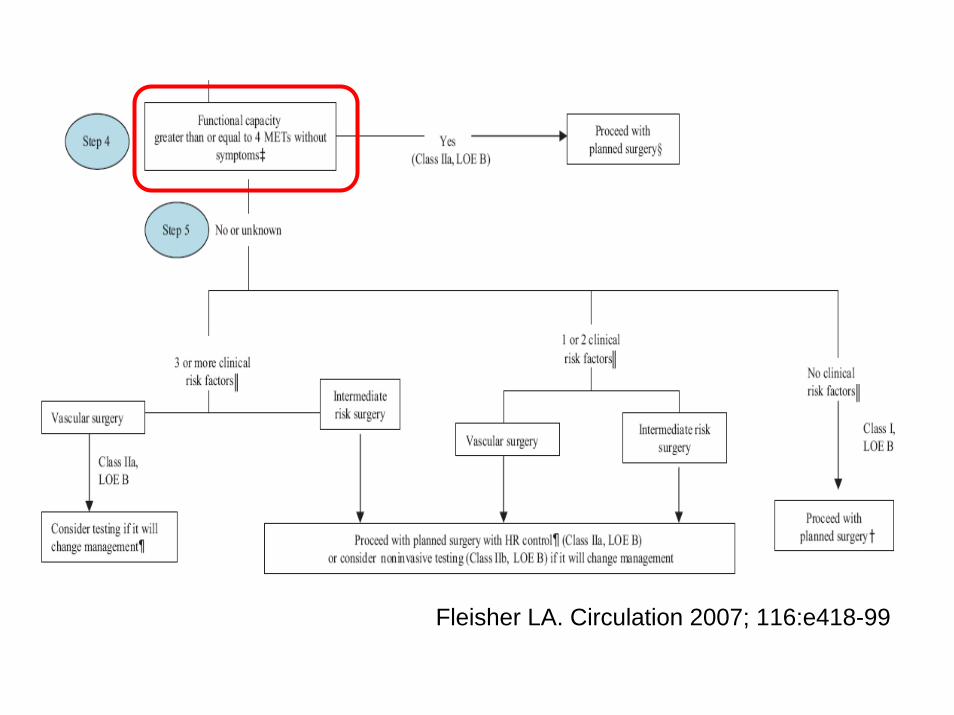
Fleisher LA. Circulation 2007; 116:e418-99

What’s a MET?

Focused Physical ExamCoexisting conditions will increase the risk of
perioperative morbidity and mortality 1) URTI2) ASTHMA3) CAD4) DIABETES5) HTN6) GERD/ HIATUS HERNIA7) PREGNANCY

URTI
Upper Respiratory Tract Infectionchildren bronchspasmlaryngospasminduction and emergencegeneral anesthesia
* 4 week recovery time *


Asthma
Airway mucous plugging
Acute bronchospamsInductionETT placementAirway manipulation

Smoking Cessation12-24 hrs
elimination of carbon monoxide and systemic nicotine improved oxygen supply and reduction of oxygen demand
>48 hrs – 2 wksslow improvement in airway hyperactivity and sensitivitypossible increase in pulmonary complications due to increased secretions (need 4+ wks to improve mucous clearing)
>4 wksdecreased risk of post-op pulmonary complications
>10 wkssame post-op pulmonary complication rate as non-smokers

Incidence of PPCs in patients who underwent pulmonary surgery
Nakagawa M et al. Chest 2001;120:705-710
©2001 by American College of Chest Physicians

Decrease postop pulmonary complications
PreoperativeInstruction in respiratory manouvresSmoking cessationBronchodilatorsAntibiotics for active dxChest physio
PostoperativeLung expansion manouvresChest physioEpidural (thoracics, AAA, laparotomy)

Commonly used respiratory medications
B-adrenergic agonists (ventolin)
Inhaled / oral steroids (flovent/prednisone)
Leukotriene receptor antagonists (singulair)
Anti-cholinergics(atrovent)
Methylxanthines(theophylline)

Hypertension
Labile blood pressure control
Left ventricular hypertrophyhigher risk of CVA / ischemia
Diureticshigher risk of hypovolemia andmetabolic disturbances

Coronary Artery Disease
Coronay Artery Diseasemyocardial ischemiamyocardial infarctventricular dysfunctionsurgical and anesthetic stress

Cardiac Risk Index
Goldman 1977 – First Cardiac Risk Assessment Tool
Detsky 1986

Aortic Stenosis

Risk Factor Prevalencen (%)
Adjusted OR(95% CI)
High risk surgery 490 (34) 2.6 (1.3 – 5.3)Coronary artery disease 478 (34) 3.8 (1.7 – 8.2)Congestive heart failure 255 (18) 4.3 (2.1 – 8.8)Cerebrovascular disease 140 (10) 3.0 (1.3 – 6.8)Insulin therapy 59 (4) 1.0 (0.3 – 3.8)Creatinine > 177 umol/l 55 (4) 0.9 (0.2 – 3.3)
New Cardiac Risk Index
Validation cohort n = 1422Major cardiac events = 36 (2.5%)
Lee TH. Circulation 1999;100:1043-1049

Revised Cardiac Risk IndexRisk Factor
High risk surgery
History of CAD
History of CHF
History of stroke
Diabetes mellitus
Cr > 177
Risk Factors Events (%) 95% CI
0 0.4 0.05 – 1.51 0.9 0.3 – 2.1 2 6.6 3.9 – 10.3 ≥3 11.0 5.8 – 18.4

NewYork Heart Assoc CHF


Diabetes
End organ damageretinopathy, neuropathy, silent cardiac ischemia, stroke/tia, CAD, PVD
Autonomic dysfunctionorthostatic hypotension, spastic bladder, gastroporesis
Symptomatic hypoglycemia?Difficult Intubation

Diabetes Management (Pre-op)Stop Oral HypoglycemicsTake ½ long acting AM insulinD5w at 75 cc/hr (1cc/kg/hr)Glucoscans
DM1 – simultaneous d5w + insulin infusion (1-2u/hr)avoid DKA – need extra insulin bolus after 8 hrs EVEN if glucoscan normal

GERD
GastroEspohageal RefluxHiatal HerniaPulmonary AspirationRapid Sequence Intubation

Fasting Guidelines
Clear liquids – 2 hrsBreast milk – 4 hrsCow milk / light snack (no fat) – 6 hrsMeat / fried foods – 8 hrs

PregnancyPremedications and anesthetic agents
uroplacental blood flowteratogensspontaneous abortionfull stomachdrug response/ elimination/ protein binding

Kidney diseaseVolume status (HD <24hrs prior to sx)CADAnemiaElectrolytes (K, Na)MucomystDrug EliminationBleeding – plt dysfunctionNutrition (nephrotic)IV access

Risk Factors for Post-op ARF
Kheterpal S. Anesthesiology 2007;107:869-70

Kheterpal S. Anesthesiology 2007;107:869-70

HepaticDrug metabolismUremia/encephalopathyArteriovenous shunts /
varicesHepatorenal syndromeElectrolytes (hypoNa hypoK
met.alkalosis)Glycogen storesMalnutrition / AlbuminBleeding (vit K – 2,7,9,10,
prot C S)

Hepatic disease
Operative Mortality 0-10% 4-31% 19-76%

Anesthetic Plan
1) Patient Assessment2) List of considerations3) Anesthetic Plan

Considerations
A consideration is a factor that you must “consider” when planning your anesthetic1) Surgical considerations
Can plan without any information aboutthe patient
2) Patient considerationsBased on medical condition of the patient

Let’s Give an Anesthetic …

Surgical ConsiderationsBody Part / Location
Regional vs GeneralPain management
DurationPositionAirway managementMonitorsExpected Blood Loss – IV size, IV tubing, Blood
warmer, Crossmatch, iSTAT, Level 1, Cell SaverPost-op Disposition – PACU, ICU

Anesthetic Plan
• Pre-op– Preop Eval, Consent, Premeds
• Intra-op– Monitors, IV access, Airway, Pain, Position,
Duration, Induction, Maintenance, Emergence, Complications
• Post-op– Pain control, disposition, complications

ID - 43 yr old female with brain tumour and seizure disorderSx – TAH BSO for Ovarian Mass , Possible StagingPMHx – Brain tumour (inoperable glioma – radiation/chemo)
Seizure d/o (last sz Dec 08)Ovarian Mass
ROS - > 4 mets. No GERDPSHx – Brain Bx, Bladder Susp, Knee Arthroscopy (uneventful)Meds – Decadron, Dilantin, Gabapentin, Venlafaxine, RanitidineAll – Penicillin (hives), nuts, shellfish, sulphaSx Hx – no smoke / ETOHO/E - ? Elevated ICP

Anesthetic Plan
• Pre-op– Preop Eval, Consent, Premeds
• Intra-op– Monitors, IV access, Airway, Pain, Position,
Duration, Induction, Maintenance, Emergence, Complications
• Post-op– Pain control, disposition, complications

PreMeds – 1-2mg midazolamAccess/Monitors – 18g , RL at 100cc/hr, stnd CAS monitors,
PNS, +/- art lineRegional – no, possible ICP issuesInduction – no need for RSI, poss ICP
propofol(1.5-3 mg/kg), ROC(0.6-1 mg/kg), lidocaine(1-2mg/kg), remi(infusion)
A/W – mask 4, ETT 7, Mac 3, Pressure control(7cc/kg, max 35mmHg) +/- hyperventilation
Maintenance – Remi(infusion), Des <1 MAC, ROC(infusion), mannitol / lasix / dilantin
Emergence – reversal of NMB(neo 0.06/kg, glyco0.2mg/cc of neo), PONV (ondans/dex), extubate awake (on remi infusion)
Post-Op – PCA (hydromorph 0.2mg q6 min)Disposition – PACU, wardPossible Issues – ICP, Sz, ROC (dilantin), PONV, bleeding,
DVT risk

Informed Consent

Informed Consent
Discuss anesthetic plan and alternatives :Endotracheal intubationMechanical ventilationInvasive monitorsRegional anesthesia techniquesBlood product transfusionPostoperative ICU

Alternatives
To the suggested anesthetic plan in case of:
staff preferencefailed procedurechange in clinical circumstance

Risks of Anesthesia-related procedures
Disclose in a way that a reasonable person would find helpful in making a decision
Complications that occur frequently
Complications that are most severe

Regional Anesthesia
H/A, infection, bleeding, nerve injury, allergic reactions, possible failure

General AnesthesiaSore throatHoarsenessNausea and vomitingDental injuryAllergic reactionIntraoperative awarenessPulmonary/ cardiac injuryStroke / deathPostoperative intubationICU admission

Blood TransfusionFeverInfectious hepatitisHIVHemolytic reactions
Table 1. Risk of transfusion-transmitted infection in Canada* Residual Risk per RBC or
Platelet Unit
Kleinman, S. et al
Residual Risk per 1,000,000 donations (95% CI)***
Chiavetta, J. et alHIV 1/4,700,000 0.24 (0.03-0.62)+HCV 1/3,100,000 0.70 (0.08-3.13)HBV 1/31,000 to 1/82,000 * 8.52 (4.44-15.11)++HTLV I/II 1/1,900,000 ** 0.67 (0.24-1.42)

Vascular Cannulation
• Peripheral nerve injury• Tendon injury• Blood vessel injury• Hemothorax• Pneumothorax• Infection• Air embolism / vascular collapse

Extenuating Circumstances
Procedures may proceed without consent if in emergency situation

Infection Control

Infection ControlPrevention of transmission
Btw patients, btw patients and personnel, viceversa
Prevention of infectious complicationsIVs, art lines, triple lumens, catheters, nerve blocks, spinal anesthetics
Avoidance of anesthesia-related complicationsAspiration
Prevention of Surgical Wound InfectionsPeriop antibiotics

Transmission of Infection

Transmission-based Precautions
1) Standard Precautions
2) Contact3) Airborne4) Droplet

Standard PrecautionsHand hygieneAppropriate use of glovesAppropriate use of aprons and other personal protective
equipmentAppropriate handling and disposal of waste and sharps Appropriate handling and management of clean and used
linen Isolation of patients with certain infections Keeping the healthcare environment free of clutter for ease
of cleaning Appropriate decontamination of healthcare equipment in
line with IPC principles and manufacturers instructions.
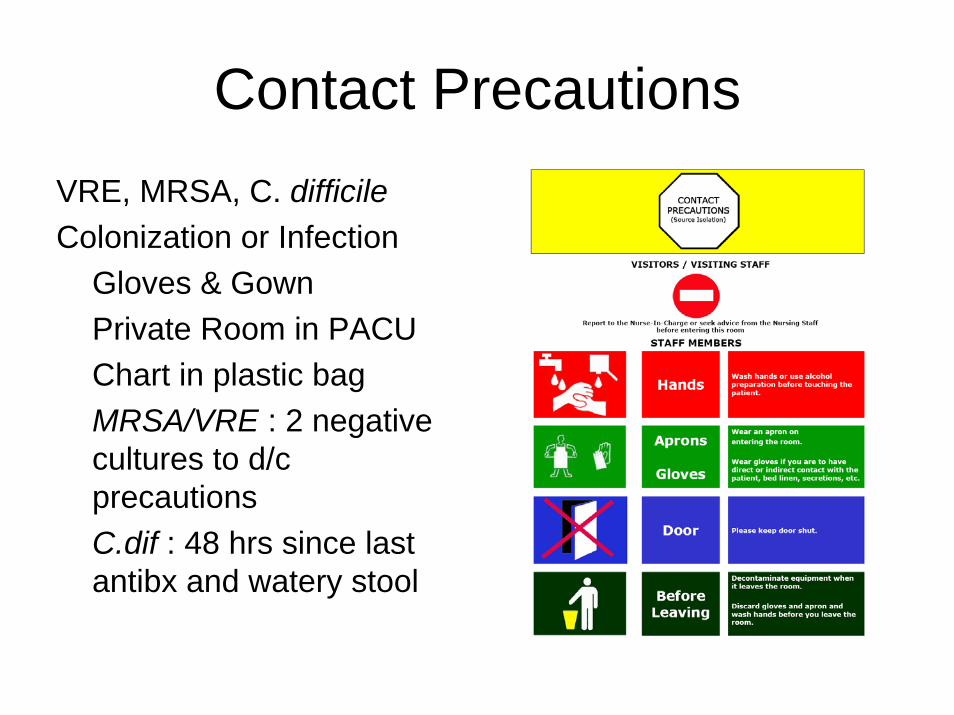
Contact PrecautionsVRE, MRSA, C. difficileColonization or Infection
Gloves & GownPrivate Room in PACUChart in plastic bagMRSA/VRE : 2 negative cultures to d/cprecautionsC.dif : 48 hrs since last antibx and watery stool

Droplet PrecautionsInfectious agents that are
present in larger propletsproduced by coughing, sneezing, talking
N. meningitidis, H.influenzae, M. pneumoniae, adenovirus, rubella virus
Maskwithin 3 feet of infected/colonized individualpatient should wear mask for transport

Airborne PrecautionsInfectious agents that
remain suspended in the air
M. tuberculosis, varicellazoster virus, ebola virus, SARS, coronavirus, rubeola (measles)
N95 respiratorsneed a fit test
Negative-pressure isolation room

Prevention
Occupational ExposureBlood Borne : HIV, HBV, HCVNeedle stick, Open cuts, Eye splash, Ampules, Scalples
Wash w soapReport Exposure
Serology testing, postexposureprophylaxis (PEP), counseling


Antibiotic Prophylaxis

Bacterial Endocarditis

SBE ProphylaxisProsthetic cardiac valve or prosthetic material used for cardiac valve repair
Previous Endocarditis
Congenital heart disease (CHD)*
Unrepaired cyanotic CHD, including palliative shunts and conduits
Completely repaired congenital heart defect with prosthetic material or device, whether placed by surgery or by catheter intervention, during the first 6 months after the procedure
Repaired CHD with residual defects at the site or adjacent to the site of a prosthetic patch or prosthetic device (which inhibit endothelialization)Cardiac transplantation recipients who develop cardiac valvulopathy

http://www.ottawa-anesthesia.org/reading.shtml
• Preoperative Assessment Annotated Bibliography• This site hosts all reference material for residents rotating through
PAU. Key references and brief descriptions of the articles are provided below. Residents will be expected familiarize themselves with this information during the course of their rotation. Supplemental readings have been provided for those wanting to explore a topic in greater depth as follows:
• Cardiovascular• Pulmonary• Thrombosis and Hemostasis• Endocrinology• Preoperative testing• Fasting Guidelines• Organization of Preoperative Clinics