predicted impact of hiv/aids on improved fallow adoption and rural household food security in malawi
TRANSCRIPT
Copyright © 2007 John Wiley & Sons, Ltd and ERP Environment
* Correspondence to: P. H. Thangata, SADC Secretariat, FANR Directorate, Private Bag 0095, Gaborone, Botswana. E-mail: [email protected] or [email protected]
Sustainable DevelopmentSust. Dev. 15, 205–215 (2007)Published online 2 April 2007 in Wiley InterScience(www.interscience.wiley.com) DOI: 10.1002/sd.323
Predicted Impact of HIV/AIDS onImproved Fallow Adoption and RuralHousehold Food Security in Malawi
P. H. Thangata,* P. E. Hildebrand2 and F. Kwesiga3
2Food Resource and Economics Department, University of Florida, Gainesville, Florida, USA3Forum for Agricultural Research Agricultural Research in Africa (FARA), PMB CT 173,
Accra, Ghana
ABSTRACTResearch was conducted to assess the impact of HIV/AIDS on improved fallow adop-tion and rural household food security in Malawi. An ethnographic linear program-ming model was created for a representative household with three scenarios: noillness, adult female illness and adult male illness. Results show that the impact ofHIV/AIDS on food production depends on the patient’s gender. If a male head ofhousehold is sick and later dies, available field labour is reduced as family membersare expected to care for him and, consequently, less food and cash crops are pro-duced, which creates a food insecure household. However, when a woman is sick andlater dies, the effect on male labour is not as great, as males are not care-givers. Weconclude that in an HIV/AIDS environment, agroforestry adoption is more feasible in households in which available labour is undisrupted for longer periods of time.Copyright © 2007 John Wiley & Sons, Ltd and ERP Environment.
Received 1 August 2005; revised 5 February 2007; accepted 15 February 2007
Keywords: Africa; agroforestry; rural food security; HIV/AIDS; Malawi; improved fallows; smallholder
Introduction
IN MALAWI, ALMOST 90% OF THE POPULATION IS RURAL AND DERIVES ITS LIVELIHOOD FROM FARMING
small landholdings, contributing about 85% of total agricultural production. However, soil fertility
depletion is one of the problems contributing to lower yields and potential food insecurity in small-
holder households. The complete removal of subsidies for mineral fertilizers in 1998 (Zeller et al.,1998) meant that most farmers can no longer afford them. Although replenishing soil fertility can be
achieved with either organic or inorganic fertilizers, the only feasible option for many smallholder
farmers in Malawi is to use organic fertilizers. Agroforestry systems including improved fallows are a
promising technology to restore the soil fertility in smallholder farms. However, agroforestry activities
increase labour use considerably.
206 P. H. Thangata et al.
Rural food insecurity in Malawi has been compounded by the prevalence of HIV/AIDS since the first
confirmed case in 1985. By 1996 AIDS had become the leading cause of death among Malawi’s popu-
lation aged 15–49, even though the Malawi government began implementing a number of policy, insti-
tutional and operational strategies to prevent and mitigate the spread of HIV/AIDS. At the time of this
study, no comprehensive research had been carried out to assess the impact of HIV/AIDS on food secu-
rity in rural areas (Kakhobwe, 1999).
As is the case in other sub-Saharan African countries, the smallholder agriculture sector in Malawi
depends on family labour, which is among the most constraining of socioeconomic factors in small-
holder systems. The HIV/AIDS epidemic impacts on human health and hence on crop production in
smallholder farming systems, due to a reduction in available household field labour for long periods
(Villarreal, 2001). As conditions for food insecurity persist, the range of options for resource-poor
farmers to overcome food deficits becomes more limited. Additionally, a reduction in available house-
hold labour leads to a decline in the amount of land that can be cultivated and a decrease in the range
of crops that can be grown. Potential cash income is also lost due to illness and death of individuals and
the task of caring for these patients (Haslwimmer, 1996).
Given that HIV/AIDS affects the labour force, the epidemic is no longer just a health issue, but an
agricultural problem as well. When a member of the family is sick, the whole family is affected due to
a reduction in household labour for long periods of time as members have to divert time to care for the
sick and eventually neglect farm or off-farm activities (Haslwimmer, 1996). The HIV/AIDS epidemic
is therefore a family disease (Pequegnat et al., 2001) because of the dynamic interactions among family
members (Robbins et al., 1998). Thus, vulnerability to diseases in rural households is vulnerability to
food insecurity.
In times of food shortages and non-HIV/AIDS situations, the most common coping strategies in rural
Malawi have been (1) ganyu, working in other farmers’ fields for payment in cash or kind, and/or (2)
changing food consumption to fewer meals per day or per week. In many households affected by
HIV/AIDS, ganyu is often no longer an option. Even in households with surplus labour, the problem is
compounded by fewer opportunities for off-farm labour, and more expenses caring for the sick, or on
funerals, resulting in less money available for purchasing food and other household requirements (FAO,
2002; UNAIDS, 1997). Therefore, dietary change is often the only available option and poverty is
exacerbated.
The Malawi government is one of the African governments that have, in recent years, introduced ini-
tiatives to make anti-retroviral drugs (ARVs) more accessible to people living with HIV/AIDS. However,
the success of these initiatives rests partly on the food security and nutritional status of their
beneficiaries, as ARVs are known to be potentially harmful when taken on an empty stomach. Nutri-
tion and food availability are major determinants of human health and functional performance (Wagner,
1986). Managing the interactions between ARVs and food and nutrition is a critical factor in improv-
ing the quality of life of people living with HIV/AIDS (Castleman et al., 2003). Good nutrition reinforces
the effect of drugs that may be taken by infected people (FAO, 2002). When infected with the HIV virus,
the immune system works hard to fight infection so people living with HIV and those with AIDS have
increased nutritional requirements (FAO, 2002; Epstein, 1995). Improving the productivity and diver-
sity of food crops is essential to attaining food security and mitigating the impact of HIV/AIDS.
Agroforestry can play an important role in helping to reduce the vulnerability of families affected with
HIV/AIDS. It is one of the six sustainable agricultural production practices for soil fertility improve-
ment and productivity, critical for sustainable land use, poverty alleviation and income generation among
smallholder farmers, especially those in marginal and degraded lands (Khan and Khisa, 2000; Chianu
and Tsujii, 2004). Agroforestry has also been used as wood fuel, timber, poles and fodder and for soil-
erosion control, among other uses (Tenge et al., 2004; Kajembe et al., 2005; Okoba and De Graaff, 2005).
Copyright © 2007 John Wiley & Sons, Ltd and ERP Environment Sust. Dev. 15, 205–215 (2007)DOI: 10.1002/sd

HIV/AIDS and Improved Fallow Adoption and Rural Household Food Security in Malawi 207
Besides improving soil fertility and improving the productivity of food crops, and the many other uses
of agroforestry, the adoption of agroforestry technologies can increase the diversity of food available
(Khan and Khisa, 2000). For severely cash constrained farmers (which is the case for the majority of
smallholders in Malawi), the cash saved when they use agroforestry methods to sustain soil fertility (as
opposed to purchased chemical fertilizers) can be used for other household needs. Importantly, in the
context of vulnerable, poor families, this modest cash reserve can help protect households from selling
assets to meet expenses when a member of the household is sick or dies. Furthermore, the production
of indigenous fruits in agroforestry systems can also improve household nutrition through increased
fruit availability – which is of considerable significance in the Malawi context, where malnutrition is a
major problem for poor families (Conroy et al., unpublished report). Last, some agroforestry species can
provide alternative remedies to treat opportunistic infections traceable to HIV/AIDS. A comprehensive
discussion on how agroforestry can mitigate the impacts of HIV/AIDS is given by Kwesiga et al. (2004).
This paper evaluates the impact of HIV/AIDS on labour availability and on the potential for adoption
of one agroforestry technology – improved fallows of sesbania (Sesbania sesban (L) Merr.) and tephrosia
(Tephrosia vogelii Hook, f.). The study was carried out as part of a larger project evaluating the potential
for agroforestry adoption and carbon sequestration in agroforestry systems (Thangata, 2002). This part
of the study tested the hypothesis that adoptability of agroforestry depends on household composition,
and so on available labour. The study specifically focused on who in the household is affected, and on
the effects of HIV/AIDS on food production in a household.
The paper is arranged as follows: after this introduction, the next section deals with the materials and
methods of the study. After this, there is a model framework and model scenario section that is followed
by the results section. This is followed by discussion and conclusions.
We would like to underscore that any disease reduces available labour in a household and reduces
household productivity. The choice to use HIV/AIDS in this study was because the illness reduces labour
for long periods of time and therefore it is easy to track time lost, for example the time between when
one gets sick and the time one dies. We note also that in the rural areas it is sometimes impossible to
distinguish the physical signs of HIV/AIDS from those of poverty and malnutrition.
Materials and Methods
The study was conducted in central Malawi, specifically Kasungu district. Data were collected from Sep-
tember to December 1999 and again between June and August 2001. Details regarding the area and
methodology are found in the work of Thangata et al. (2002). To understand the role played by central
government, meetings were conducted with the district commissioner and the district health officer.
Later, interviews were held with hospital personnel, NGOs and farmers to learn about HIV/AIDS pro-
grams in the area and what information about HIV/AIDS already existed. No formal questionnaires
were used. From past experience working in the villages, people are reluctant to discuss HIV/AIDS and
therefore a questionnaire would not have been appropriate. Farmers, including those who have cared
for an HIV/AIDS patient, were interviewed primarily about how this affected their work in the fields.
The interviews were conducted in a Sondeo (PRA) manner (Hildebrand, 1981) in the presence of the
extension worker and the health surveillance assistant (HSA) from a local clinic.
A dynamic (10 year) ethnographic linear programme (Bastidas, 2001; Thangata, 2002; Hildebrand
et al., 2003) was developed to model the representative household. This procedure, developed in the
field with the participation of informants, maximizes an objective (in most cases discretionary cash
after meeting necessary cash expenses) subject to the constraints of land, labour, cash, minimum
necessary cash expenses and food consumption for the household.
Copyright © 2007 John Wiley & Sons, Ltd and ERP Environment Sust. Dev. 15, 205–215 (2007)DOI: 10.1002/sd

208 P. H. Thangata et al.
During the study, three general observations of note were made. First, it was observed that at the
household level, when the husband is sick, family members are expected to take care of the man. Family
members have to divert time to care for the patient and eventually neglect farm or off-farm activities.
This means that the work of the husband and the caregivers (household members) in the household is
reduced. Conversely, when the patient is the wife, she is either sent to her parents’ home where her rel-
atives take care of her, or one of her female relatives comes to the husband’s home to take care of the
sick wife. In the former, there is one less member to feed in the affected household, but the receiving
(the wife’s parents) household has another member to feed. In the latter case, the husband continues
to work as before, the household loses the labour of only one member and gains one more member (the
female relative) to be fed who does not contribute to fieldwork. Consequently, from the perspective of
the household of the sick person, when the husband is sick, a larger amount of field labour is lost.
In this paper, modelling the impact of HIV/AIDS on agriculture and agroforestry adoption stems
from the observation that women take more responsibility than men when it comes to taking care of
the sick in the household. Yet, women also provide most of the agricultural labour oriented to food
production for home consumption (Gladwin, 1992), while men’s labour is in most cases intended for
producing commercial crops.
Model Framework
The stages leading to the construction of the HIV/AIDS model are presented in Figure 1. After data col-
lection, a base, no-agroforestry-intervention model was developed and analysed (stage 1). Later, a general
agroforestry model (stage 2) was developed. Stage 3 is an extension of the general agroforestry adoption
model in which a seed-selling incentive was introduced. During the early days of disseminating the
improved fallow technology, ICRAF was buying seed from farmers already testing the technology to give
to new farmers and NGOs promoting agroforestry. Sales of tree seeds amount to a windfall profit for
early adopters and a monetary incentive to adopt improved fallow technologies for late adopters
(Thangata et al., 2002). Additionally, since the agroforestry seeds were bought at a higher price than
maize1, the additional income from seed selling can enhance adoption, even in times of shocks such as
HIV/AIDS, so it became the incentive in the model (stage 3). At stage 4, three models were developed
from stage 3: a model comparing the adoption pattern between male- and female-headed households, a
carbon model, in which a carbon credit incentive was introduced and the HIV/AIDS model (Thangata,
2002; Thangata and Hildebrand, 2006). From Figure 1, it is the HIV/AIDS model on which this paper
reports.
Model Scenarios
A representative, male-headed household with 3.5 ha of land was selected to model three scenarios (stage
4) with a seed-selling option (stage 3), over a 10-year period. The household was representative of the
first 10 households interviewed in 1999. The 10 households were among the 18 farmers who went to
Zambia to view agroforestry trials there by ICRAF in the 1997/98 season (Moyo, 1999). The composi-
tion of the representative household and minimum annual food requirements are presented in Table 1.
The model separates labour inputs by gender and by month; labour supply in any calendar month is
Copyright © 2007 John Wiley & Sons, Ltd and ERP Environment Sust. Dev. 15, 205–215 (2007)DOI: 10.1002/sd
1 Maize selling price was about US$0.09, while agroforestry seeds ranged from US$0.79 to 1.04.

HIV/AIDS and Improved Fallow Adoption and Rural Household Food Security in Malawi 209
Copyright © 2007 John Wiley & Sons, Ltd and ERP Environment Sust. Dev. 15, 205–215 (2007)DOI: 10.1002/sd
ModelStage
1
4
3
2
DATA COLLECTION PRIMARY
(Farm Surveys) +
SECONDARY(Agronomic, Biophysical, Policy)
BASEModel
HIV/AIDSMHHVs
FHH
SEED SELLING
AGROFAdoption Model
CARBONCREDIT
Figure 1. Schematic representation of the modelling stages
HH composition Number Labour/month Food requirements(kg)/year
Maize G/nut Cassava S/potato
Male 1 25 250 100 70 70Female 1 25 250 100 70 70Adolescent males 0 – – – – –Adolescent females 1 12.5 200 100 70 70Child (male 6 yrs) 1 5 150 50 35 35Infants (<5 yrs) 2 – 100 100 70 70Sub total 6 67.5 950 450 315 315Female1 1 – 250 100 70 70Grand total 7 67.5 1200 550 385 385
Table 1. Household composition, annual food requirements per person and labour person days per month in Central Malawi1 Added female member when the wife is sick.
the total amount of labour available from the contribution of all household members. The consumption
constraints in the model reflect the need for the households first to satisfy usual household food con-
sumption levels before marketing any surplus for cash. Modifying household composition (number of
adults, their sex, and the number, age and sex of children) also affects potential adoption of improved
fallow technology. This effect is reported by Thangata (2002).
The scenarios modeled are

210 P. H. Thangata et al.
(1) NO SICKNESS, when there is no person ill in the household;
(2) MALE SICKNESS, when the husband becomes ill with HIV/AIDS in year 4 and dies in year 6, and
(3) FEMALE SICKNESS, when the wife becomes ill with HIV/AIDS in year 4 and dies in year 6.
As reported by Thangata (2002), in dynamic modelling, the first season is started with an arbitrary
amount of beginning cash available. Therefore, the first year is not necessarily representative. Starting
from year 1, unused cash can be transferred to the following season. The arbitrary initial cash amount
can also affect the second year. By the third year, this effect normally disappears. Therefore, the first
two years are not reported in this study. Another issue to take into account in mathematical program-
ming in general is end-of-planning-horizon effects. These effects are when the model ‘chops off’ the
analysis at some finite time in the future (Grinold, 1983; Schrage, 1997). Because there is no long term
future in the model in the last years of the dynamic program, the model sees no benefits from certain
activities in these years (such as livestock production or multi-year agroforestry practices), so it elimi-
nates these activities from the ‘optimal solution’ in the last years of the program. In our 10-year model,
improved fallows planted in the ninth and 10th years do not yield any benefits until the 11th year, or
after, when the model has ended. Because the model chooses only those activities that are of benefit to
the farm in the ninth and 10th years it drops agroforestry activities from the simulated results in those
last two years. To reflect the above dynamic modelling characteristics, only results from years three to
eight are reported.
Results
No Sickness Scenario
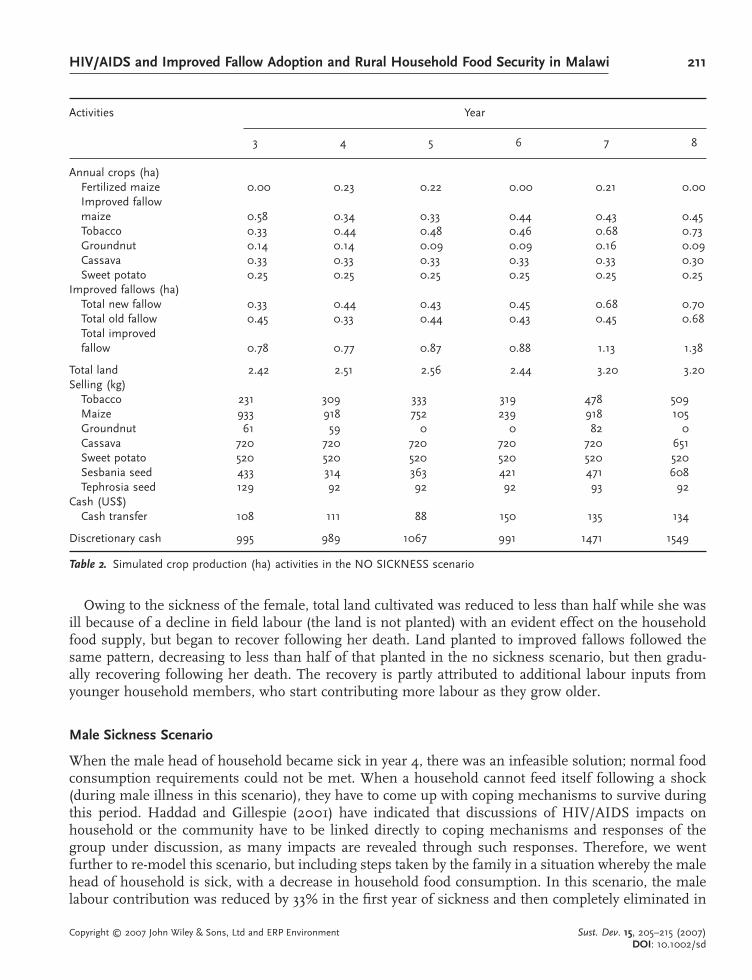
In the case of no HIV/AIDS in the household (Table 2), consumption requirements were met and some
maize (the main food crop) and other food crops were sold. The household was able to feed itself through-
out the period and therefore was food secure. In year 3 nearly one-third of the land was in improved
fallow and this proportion gradually increased to about 43% in year 8. More than half of the maize area
was on land previously planted to improved fallows, and in years 6 and 8 improved fallow maize com-
pletely replaced fertilized maize. The household did not need to use credit to finance the adoption of
the new technologies as it was able to transfer sufficient cash from year to year for production activities
and other necessary expenses in the following season and had discretionary cash (the variable maxi-
mized in the model) available each year. Of particular importance in this option was the use of the seed
selling incentive offered by ICRAF. Agroforestry technologies, like other cropping enterprises, require
seed to replace harvested trees and to plant new areas. This seed can be produced locally and is poten-
tially an attractive cash crop. This enterprise is partly responsible for the relatively well-off status of the
household, in comparison to no seed selling, and was considered to be critical in the establishment of
the improved fallow option.
Female Sickness Scenario
When the female was infected with HIV/AIDS in year 4 and died in year 6, the household was still able
to produce enough maize and other food crops for home consumption (Table 3), but unable to produce
enough maize to sell beginning in year 4. Beginning in year 5, the area in new fallow dropped to about
half, reducing the cash available from improved fallow seed selling, and the area in improved fallow
maize dropped to about half of the no sickness scenario. There was still some discretionary cash avail-
able, but it initially dropped to about one-fifth of the no sickness scenario.
Copyright © 2007 John Wiley & Sons, Ltd and ERP Environment Sust. Dev. 15, 205–215 (2007)DOI: 10.1002/sd
HIV/AIDS and Improved Fallow Adoption and Rural Household Food Security in Malawi 211
Owing to the sickness of the female, total land cultivated was reduced to less than half while she was
ill because of a decline in field labour (the land is not planted) with an evident effect on the household
food supply, but began to recover following her death. Land planted to improved fallows followed the
same pattern, decreasing to less than half of that planted in the no sickness scenario, but then gradu-
ally recovering following her death. The recovery is partly attributed to additional labour inputs from
younger household members, who start contributing more labour as they grow older.
Male Sickness Scenario
When the male head of household became sick in year 4, there was an infeasible solution; normal food
consumption requirements could not be met. When a household cannot feed itself following a shock
(during male illness in this scenario), they have to come up with coping mechanisms to survive during
this period. Haddad and Gillespie (2001) have indicated that discussions of HIV/AIDS impacts on
household or the community have to be linked directly to coping mechanisms and responses of the
group under discussion, as many impacts are revealed through such responses. Therefore, we went
further to re-model this scenario, but including steps taken by the family in a situation whereby the male
head of household is sick, with a decrease in household food consumption. In this scenario, the male
labour contribution was reduced by 33% in the first year of sickness and then completely eliminated in
Copyright © 2007 John Wiley & Sons, Ltd and ERP Environment Sust. Dev. 15, 205–215 (2007)DOI: 10.1002/sd
Activities Year
3 4 5 6 7 8
Annual crops (ha)Fertilized maize 0.00 0.23 0.22 0.00 0.21 0.00Improved fallowmaize 0.58 0.34 0.33 0.44 0.43 0.45Tobacco 0.33 0.44 0.48 0.46 0.68 0.73Groundnut 0.14 0.14 0.09 0.09 0.16 0.09Cassava 0.33 0.33 0.33 0.33 0.33 0.30Sweet potato 0.25 0.25 0.25 0.25 0.25 0.25
Improved fallows (ha)Total new fallow 0.33 0.44 0.43 0.45 0.68 0.70Total old fallow 0.45 0.33 0.44 0.43 0.45 0.68Total improvedfallow 0.78 0.77 0.87 0.88 1.13 1.38
Total land 2.42 2.51 2.56 2.44 3.20 3.20Selling (kg)
Tobacco 231 309 333 319 478 509Maize 933 918 752 239 918 105Groundnut 61 59 0 0 82 0Cassava 720 720 720 720 720 651Sweet potato 520 520 520 520 520 520Sesbania seed 433 314 363 421 471 608Tephrosia seed 129 92 92 92 93 92
Cash (US$)Cash transfer 108 111 88 150 135 134
Discretionary cash 995 989 1067 991 1471 1549
Table 2. Simulated crop production (ha) activities in the NO SICKNESS scenario

212 P. H. Thangata et al.
the second year onwards (after death). Labour contribution from other household members is reduced
as they take care of the sick household head, but becomes available again after the death of the sick
member. Labour from the male child (see Table 1) was considered in the later part of the model as he
grew to an adolescent male.
In the past, the coping strategy used by most people when they were food deficient was ganyu.
However, ganyu is much less feasible with HIV/AIDS in the household, due either to being weak from
diseases or lack of surplus labour. Changing consumption to fewer meals is, therefore, the common
coping strategy. To model what could happen for the household to survive the illness and death of the
male head, the model was solved at different food reduction rates. It was found that the household
needed to reduce its consumption requirements by 30% to give a feasible solution. This is entirely con-
sistent with the behavior of poor families in Malawi. In the food crisis years of 2002 and 2005, reduc-
tions in food intakes of this order of magnitude have been reported. While the weakest succumb to
hunger, households survive by reducing the number of meals, eating wild grains and grass and selling
what few assets they have to gain food to survive (Conroy et al., unpublished report).
Table 4 shows results from the male sickness scenario, when the household has to reduce its food
consumption while the male head is sick and after his death (the death of the male will release a small
amount of food but this is heavily discounted by the loss of his labour). Not only was food consumption
reduced, but tobacco land (the main source of cash other than selling seed from the improved fallow)
Copyright © 2007 John Wiley & Sons, Ltd and ERP Environment Sust. Dev. 15, 205–215 (2007)DOI: 10.1002/sd
Activities Year
3 4 5 6 7 8
Annual crops (ha)Fertilized maize 0.42 0.06 0.20 0.10 0.15 0.12Improved fallowmaize 0.58 0.34 0.20 0.20 0.20 0.23Tobacco 0.30 0.05 0.13 0.20 0.46 0.50Groundnut 0.19 0.10 0.10 0.09 0.15 0.08Cassava 0.33 0.05 0.31 0.33 0.33 0.33Sweet potato 0.25 0.13 0.05 0.25 0.25 0.25
Improved fallows (ha)Total new fallow 0.20 0.20 0.20 0.23 0.54 0.54Total old fallow 0.45 0.20 0.20 0.20 0.23 0.54Total improvedfallow 0.65 0.40 0.40 0.43 0.77 1.08
Total land 2.72 1.12 1.39 1.60 2.31 2.58Selling (kg)
Tobacco 212 35 92 137 323 348Maize 2724 0 0 0 0 0Groundnut 109 0 0 17 86 0Cassava 720 0 666 735 735 735Sweet potato 520 212 0 535 535 535Sesbania seed 410 203 125 130 201 369Tephrosia seed 129 92 92 92 93 102
Cash (US$)Cash transfer 23 49 49 101 103 135
Discretionary cash 1207 140 235 373 843 998
Table 3. Simulated crop production (ha) activities, amounts sold and end year cash (US$) in the FEMALE SICKNESS scenario
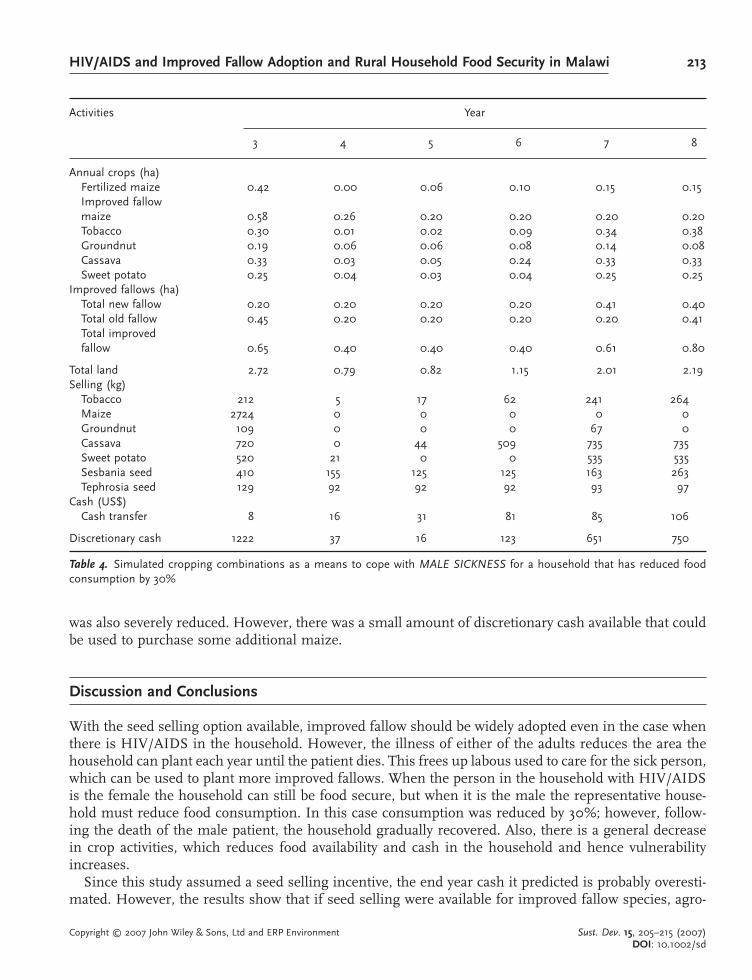
HIV/AIDS and Improved Fallow Adoption and Rural Household Food Security in Malawi 213
was also severely reduced. However, there was a small amount of discretionary cash available that could
be used to purchase some additional maize.
Discussion and Conclusions
With the seed selling option available, improved fallow should be widely adopted even in the case when
there is HIV/AIDS in the household. However, the illness of either of the adults reduces the area the
household can plant each year until the patient dies. This frees up labous used to care for the sick person,
which can be used to plant more improved fallows. When the person in the household with HIV/AIDS
is the female the household can still be food secure, but when it is the male the representative house-
hold must reduce food consumption. In this case consumption was reduced by 30%; however, follow-
ing the death of the male patient, the household gradually recovered. Also, there is a general decrease
in crop activities, which reduces food availability and cash in the household and hence vulnerability
increases.
Since this study assumed a seed selling incentive, the end year cash it predicted is probably overesti-
mated. However, the results show that if seed selling were available for improved fallow species, agro-
Copyright © 2007 John Wiley & Sons, Ltd and ERP Environment Sust. Dev. 15, 205–215 (2007)DOI: 10.1002/sd
Activities Year
3 4 5 6 7 8
Annual crops (ha)Fertilized maize 0.42 0.00 0.06 0.10 0.15 0.15Improved fallowmaize 0.58 0.26 0.20 0.20 0.20 0.20Tobacco 0.30 0.01 0.02 0.09 0.34 0.38Groundnut 0.19 0.06 0.06 0.08 0.14 0.08Cassava 0.33 0.03 0.05 0.24 0.33 0.33Sweet potato 0.25 0.04 0.03 0.04 0.25 0.25
Improved fallows (ha)Total new fallow 0.20 0.20 0.20 0.20 0.41 0.40Total old fallow 0.45 0.20 0.20 0.20 0.20 0.41Total improvedfallow 0.65 0.40 0.40 0.40 0.61 0.80
Total land 2.72 0.79 0.82 1.15 2.01 2.19Selling (kg)
Tobacco 212 5 17 62 241 264Maize 2724 0 0 0 0 0Groundnut 109 0 0 0 67 0Cassava 720 0 44 509 735 735Sweet potato 520 21 0 0 535 535Sesbania seed 410 155 125 125 163 263Tephrosia seed 129 92 92 92 93 97
Cash (US$)Cash transfer 8 16 31 81 85 106
Discretionary cash 1222 37 16 123 651 750
Table 4. Simulated cropping combinations as a means to cope with MALE SICKNESS for a household that has reduced foodconsumption by 30%

214 P. H. Thangata et al.
forestry could be expected to be adopted even by households that have limited labour. We also note that
there are many other variables that were not included in the models. Such variables as extended time
of mourning, when no farming activities can be carried out, can have an adverse effect on labour avail-
ability during periods in which deaths are frequent. In this study a lump sum was included as a con-
straint for minimum necessary expenses. Since the study did not include the cost of funerals, we also
note that such variables could substantially decrease the discretionary cash. Further, there would prob-
ably be a reduction in the amount of labour that those in the household who are not sick would be able
to contribute. This effect was not included in the model.
Several implications for policy and future research can be derived from this research. First, because
labour is such an important determinant in undertaking production activities, future improved fallow
research should look into less labour demanding technologies that would also improve food production
in rural agricultural systems.
Second, this study looked at a small area in Malawi. It is therefore suggested that a countrywide inter-
departmental (agriculture and health) survey to assess the overall impact of HIV/AIDS on smallholder
farming in Malawi is necessary. Such a study would provide information to stakeholders to formulate
policies that would assist the local people.
Third, in Malawi, the agricultural extension services have offices in each Extension Planning Area and
an agent in each village section. While conducting this study, there was cooperation between the exten-
sion services and the health personnel from the local clinic. It would be useful to explore the possibil-
ity of training extension workers as AIDS counselors. This is because extension workers cover a large
area and visit farmers almost everyday and are therefore in touch with the community. On the other
hand, the farmers have to travel to the nearest clinic whenever they are sick. Coordination between the
agricultural extension and health departments would also help to facilitate reporting of the sick and
infirm to the health services and thereby improve disease assessment in the rural communities. This
close collaboration might also assist the health personnel, as the extension agent would report on any
major sickness or outbreaks in the area.
Last, in this study, households in which the male head was ill were predicted to be more adversely
affected than households with an ill female spouse. Programs targeting female headed households can
help improve their accessibility to food in times of illness and after the death of their spouse. We note
that households with different compositions would be affected differently; therefore, it would be useful
to model several kinds of household. Nutrition is very important in the management of HIV/AIDS. It
is therefore proposed that ICRAF-SA scale up options such as indigenous fruit trees and nutritional
gardens, which can bring in income and nutritional benefits to rural households, especially those that
are food insecure or HIV/AIDS affected.
Acknowledgments
This research was supported in part by The Rockefeller Foundation and a grant from the Compton Foundation through theUniversity of Florida. We thank them. We would also like to thank Dr. Goran Hyden for his contribution to this research.
The authors alone are responsible for the views and analysis expressed in this paper.
References
Bastidas EP. 2001. Assessing Potential Response to Changes in the Livelihood System of Diverse, Limited-Resource Farm Householdsin Carchi, Ecuador, PhD dissertation, Food and Resource Economics, University of Florida.
Castleman T, Eleonore Seumo-Fosso, Bruce Cogill. 2003. Food and Nutrition Implications of Antiretroviral Therapy in ResourceLimited Settings, Academy for Educational Development Technical Note 7. Food and Nutrition Technical Assistance Project:
Washington, DC.
Copyright © 2007 John Wiley & Sons, Ltd and ERP Environment Sust. Dev. 15, 205–215 (2007)DOI: 10.1002/sd

HIV/AIDS and Improved Fallow Adoption and Rural Household Food Security in Malawi 215
Chianu JN, Tsujii H. 2004. Missing links in sustainable food production in West Africa: the case of the savannas of northern
Nigeria. Sustainable Development 12: 212–222.
Conroy A. 2006a. Health and Disease in Malawi. In Poverty, AIDS and hunger; breaking the poverty trap in Malawi, Conroy A,
Blackie MJ, Whiteside A, Malewezi J, Sachs J (eds). Basingstoke, Hampshire: Palgrave-MacMillan; 33–48.
Conroy A. 2006b. Malawi and the Poverty Trap-A First Person Account. In Poverty, AIDS and hunger; breaking the poverty trap in Malawi, Conroy A, Blackie MJ, Whiteside A, Malewezi J, Sachs J (eds). Basingstoke, Hampshire: Palgrave-
MacMillan; 118–137.
Epstein L. 1995. Food for People Living with HIV/AIDS Vol. 1. Network of Zambian People Living with HIV/AIDS (NZP) Lusaka.
FAO. 2002. Focus: Food Insecurity and AIDS: a Vicious Circle. http://www.fao.org/Focus/E/aids/aids1-e.htm [9 February 2002].
Gladwin CH. 1992. Gendered impacts of fertilizer subsidy removal programs in Malawi and Cameroon. Agricultural Econom-ics 7: 141–153.
Grinold RC. 1983. Model building techniques for the correction of end effects in multistage convex programs. OperationsResearch 31: 407–431.
Haddad L, Gillespie, S. 2001. Effective food and nutrition policy responses to HIV/AIDS: what we know and what we need to
know. Journal of International Development 13: 487–511.
Haslwimmer M. 1996. AIDS and Agriculture in Sub-Saharan Africa. FAO Farm Management and Production Economics Service
(AGSP). http://www.fao.org/waicent/faoinfo/sustdev/WPdirect/WPre0003.htm [2 September 2001].
Hildebrand PE. 1981. Combining disciplines in rapid appraisal. The Sondeo approach Agricultural Administration 8: 423–432.
Hildebrand PE, Breuer NE, Cabrera VE, Sullivan AJ. 2003. Modeling Diverse Livelihood Strategies in Rural Livelihood SystemsUsing Ethnographic Linear Programming, Staff Paper 03-5, Food and Resource Economics, University of Florida.
Kajembe GC, Julius F, Nduwamungu J, Mtakwa, PW, Nyange DA. 2005. Impact of indigenous-based interventions on land
conservation: a case study of a soil conservation and agroforestry project, Arumeru district, Tanzania. Land Degradationand Development 16: 311–325.
Kakhobwe P. 1999. A Decade of AIDS Research in Malawi 1989–1999. National AIDS Control Programme Strategic Planning
Unit: Lilongwe, Malawi.
Khan NA, Khisa SK. 2000. Sustainable land management with rubber based agroforestry: a Bangladeshi example of uplands
community development. Sustainable Development 8: 1–10.
Kwesiga F, Thangata PH, Agumya A, Mitti J, Jacquet de Haveskercke, C. 2004. Reviewing Agroforestry Technologies Through anHIV/AIDS Lens: Opportunities and Benefits for Agroforestry to Mitigate the Impacts of HIV/AIDS in Southern Africa, World
Agroforestry Congress proceedings, Orlando, FL, 2004.
Moyo N. 1999. Strategies and operational planning for the dissemination of agroforestry and tree crops in Malawi. In Pro-ceedings of the ICRAF-GTZ/ITFSP Joint Dissemination Workshop, Mangochi, Malawi, May, 26–29, 1999, Bohringer A (ed);
ICRAF, Zomba, Malawi; 12–13.
Okoba BO, De Graaff J. 2005. Farmers’ knowledge and perceptions of soil erosion and conservation measures in the central
highlands, Kenya. Land Degradation and Development 16: 475–487.
Pequegnat W, Bauman LJ, Bray JH, DiClemente R, DiIorio C, Hoppe SK, Jemmott LS, Krauss B, Miles M, Paikoff R, Rapkin
B, Rotheram-Borus MJ, Szapocznik J. 2001. Measurement of the role of families in prevention and adaptation to
HIV/AIDS. AIDS and Behavior 5: 1–19.
Robbins MS, Szapocznik J, Alexander JF, Miller J. 1998. Family systems therapy with children and adolescents. In Compre-hensive Clinical Psychiatry: Vol.5. Children and Adolescents: Clinical Formulation and Treatment, Hersen M, Bellack AS,
Ollendick TH (eds). Elsevier: Oxford; 149–480.
Schrage LE. 1997. Optimization Modelling with LINDO, 5th edn. Brooks/Cole: Pacific Grove, CA.
Tenge AJ, De Graaff J, Hella JP. 2004. Social and economic factors affecting the adoption of soil and water conservation in
West Usambara highlands, Tanzania. Land Degradation and Development 15: 99–114.
Thangata PH. 2002. The Potential for Agroforestry Adoption and Carbon Sequestration in Smallholder Agroecosystems of Malawi: anEthnographic Linear Programming Approach, PhD Dissertation, Natural Resources and Environment, University of Florida,
Gainesville, FL.
Thangata PH, Hildebrand PE. 2006. Carbon Stocks in Smallholder Agroecosystems in Malawi: a Farming Systems Approach. Poster
presentation at the Seventh European IFSA Symposium, Wageningen, The Netherlands, 2006.
Thangata PH, Hildebrand PE, Gladwin C. 2002. Modeling agroforestry adoption and household decision making in Malawi.
African Studies Quarterly 6(1/2). http://web.africa.ufl.edu/asq/v6/v6i1a11.htm [6 August 2002].
UNAIDS. 1997. Women and AIDS, Joint United Nations Programme on HIV/AIDS. http://www.unaids.org [10 February 2002].
Villarreal M. 2001. HIV/AIDS and Food Security, European Media Seminar on Global Food Security, Stockholm, 2001.
Zeller M, Diagne A, Mataya C. 1998. Market access by smallholder farmers in Malawi: implication for technology adoption,
agricultural productivity and crop income. Agriculture Economics 19: 219–229.
Copyright © 2007 John Wiley & Sons, Ltd and ERP Environment Sust. Dev. 15, 205–215 (2007)DOI: 10.1002/sd