practical medical ethics
TRANSCRIPT
Patama Gomutbutra MD.Dip., Thai Board of Family MedicineGrad Cert in Palliative Care APHN,UCSF
Dip., Thai Board of Neurology_____________________________
Practical medical ethics inPalliative care

1. Definition and elements of Palliative care
2. Advance care plan
3. Medical ethics
Outline

Case demonstration
60 years old widow no child. she is known case end stage colon cancer PPS 40% (mostly bed bounded) she was admitted from sepsis and multiorgan failure she developed arrest. She talked with relatives want to die peacfully without CPR. However, she had no formal living will or any surrogate decision maker.
If you are her physician, what would you do.A. CPR
B. Respect her choice let her go

• การดแลแบบบรบาลบรรเทา (Palliative care)
• การดแลในระยะทาย (end of life care)
• การดแลแบบบานพกระยะทาย (Hospice)
1.Definition

WHO’s definition of palliative care
Palliative care NOT for Euthanasia/ Suicide

Palliative care Vs End of life care
EAPC recommendation: standard and norms for hospice and palliative care 2009 http://www.eapcnet.eu/Themes/Organisation/EAPCStandardsNorms.aspx
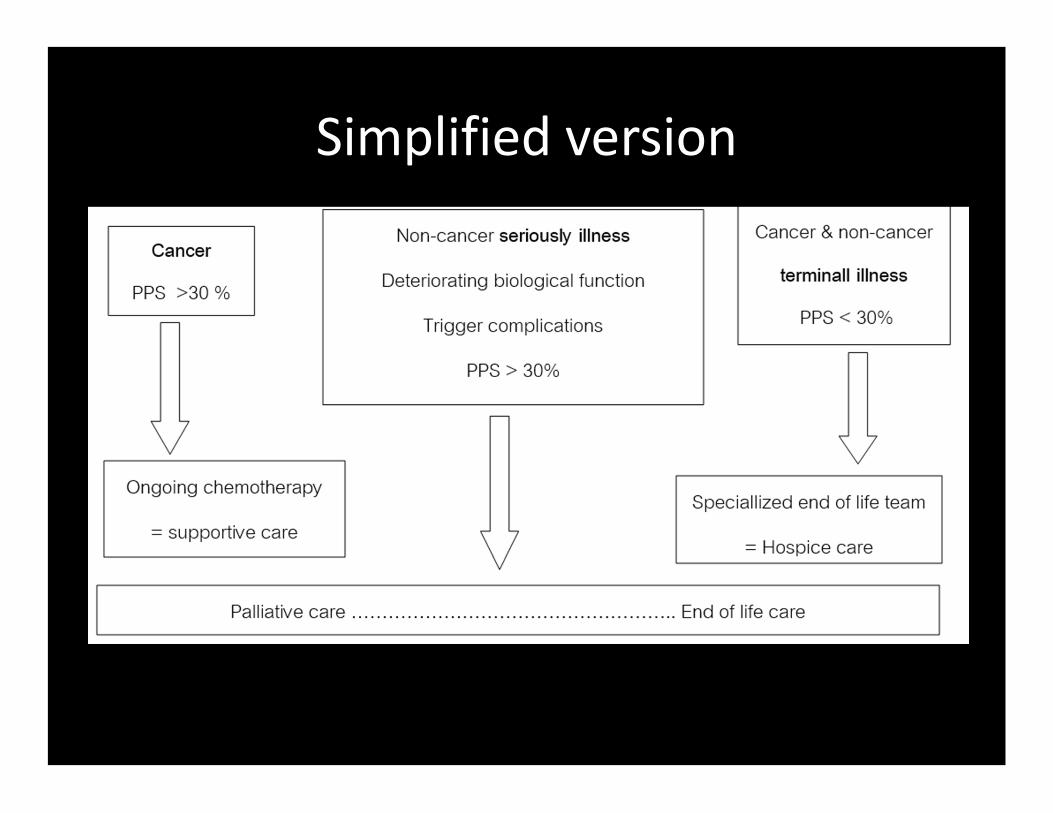
Simplified version
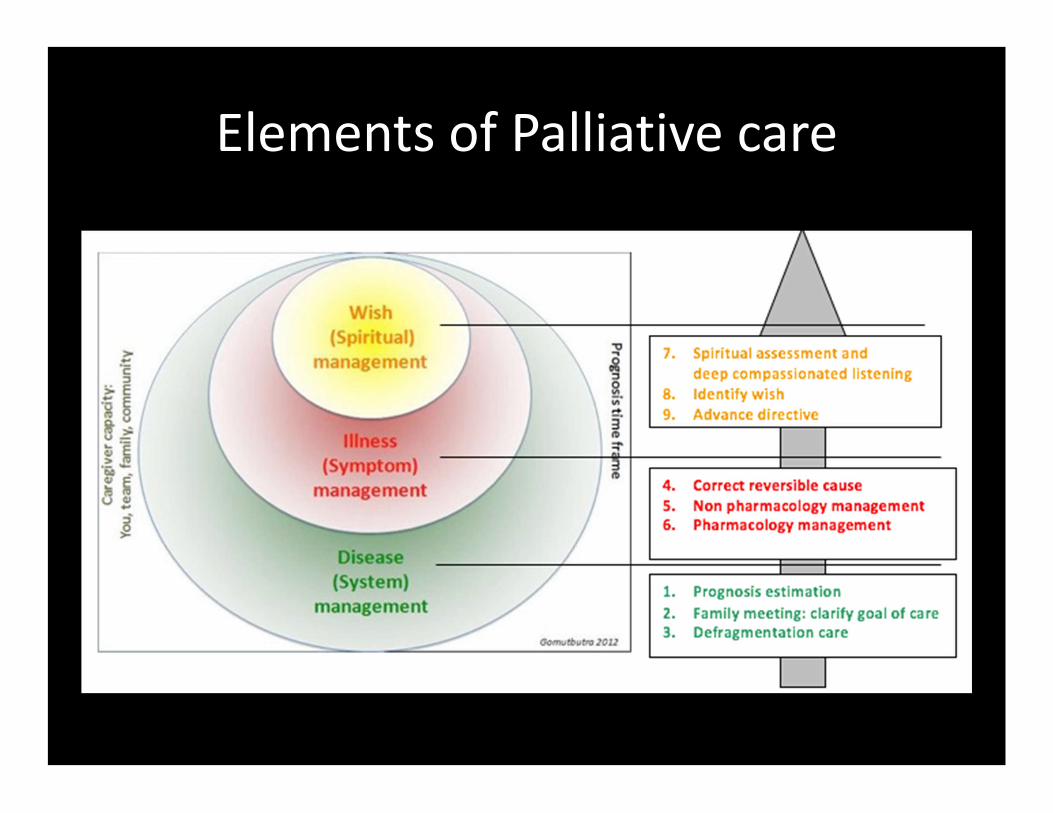
Elements of Palliative care

• Wish
•Living will
•Surrogate decision maker
2.Advance care plan

• Spiritual• Goal oriented • เชน อยากกลบไปเสยชวตท�บาน อยากมสตรตวเพ�อภาวนา อยากหลบไปแบบไมทรมาน อยากกลาวขอบคณ ขอโทษ ใหอภยกบใคร
Patient preference ( Wish )

• Medicolegal • Procedural oriented • เชน การขอรบหรอไมรบการใสทอชวยหายใจ การขอรบหรอไมรบการกดนวดหวใจฟ� นสญญานชพ การขอรบหรอไมรบอาหารทางสายใหอาหาร
Advance directive( Living will )

• Legal (optional)
• Decision maker when patient lack decision capacity
Proxy nominator(Durable Power of Attorney)

Tool Form Limitation
1. Living will Paper document
Procedure oriented
Medical knowledge
Not available at time need
2.Durable Power of
attorney : DPOA
Designated person Medical knowledge
60% Mismatch between patient
and surrogate will
3.Five wishes© Web based Medical knowledge
4.Physician Orders
for Life Sustaining (
POLST)
Physician order after
discussion with
patient and family
Some physician may feel
discomfort
Advance care plan tools
Living will
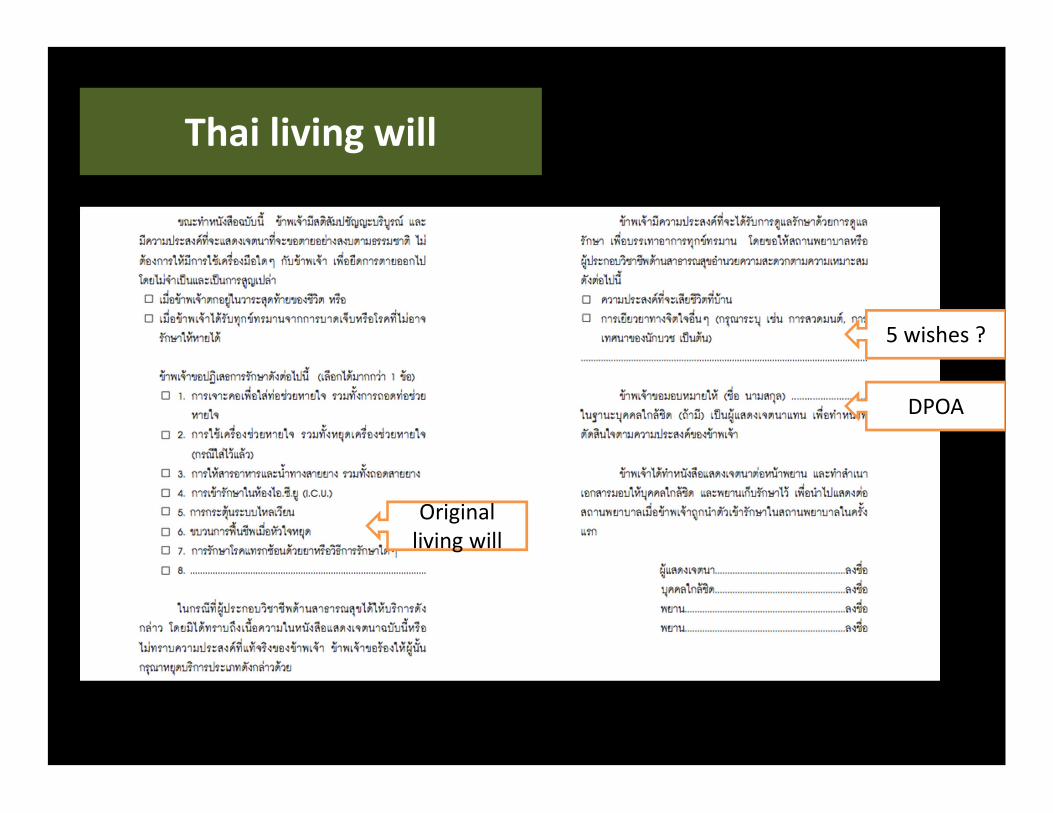
Original living will
DPOA
5 wishes ?
Thai living will

DPOADPOA

Wish 1: บคคลท�ขาพเจาไววางใจใหตดสนใจแทน "หากขาพเจาหมดสต หรอไมสามารถตดสนใจเองWish 2: ขาพเจาตองการรกษาลกษณะใดWish 3: ความสขสบายท�ขาพเจาหวงใหเปนWish 4: ขาพเจาอยากใหคนท�ดแลปฏบตกบขาพเจาเชนไรWish 5: ส�งใดท�ขาพเจาอยากใหคนท�รกรบร
Five Wishes
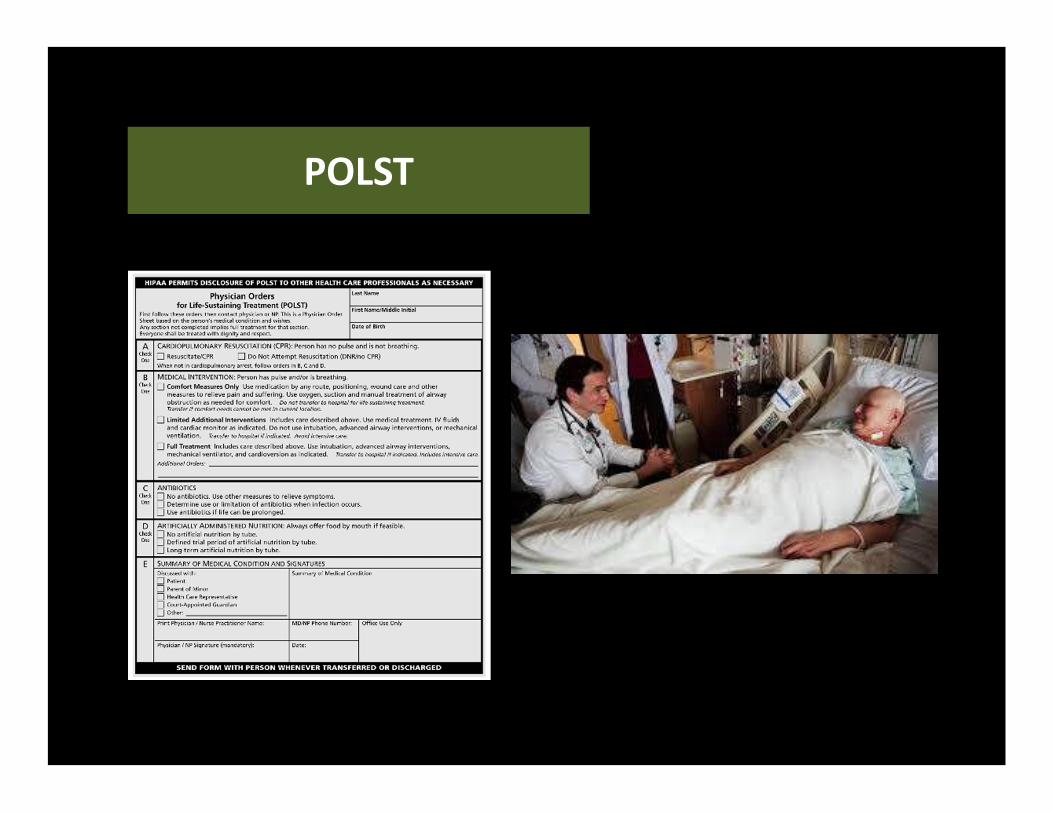
POLST

What really work for Thai ?

http://www.budnet.org/sunset/sites/default/files/Baojai-final-2559-9-26.pdf
• Medical dilemma:When ‘save life’ is not absolute answer
• Medical ethicsA systematic decision making in medical dilemma
* 3.Medical ethics
Common dilemma in palliative care
• If this treatment futile? ( worth or not?)
– Quatitative futile : survival, chance to recovery
– Qualitative futile : Quality of life
• Example
– Antibiotic in end of life penumonia
– Percutaneous gastromy feeding in dementia
– CPR in terminal case
– Anticoagulant in bed bounded stroke

Basic principle
• Autonomy
• Beneficence
• Confidentiality (Loyalty)
• Do No harm (Nonmaeficence)
• Equity (Justice)

Apply to everyday practice
1. Medical indication
2. Quality of life
3. Patient preference
4. Contextual feature
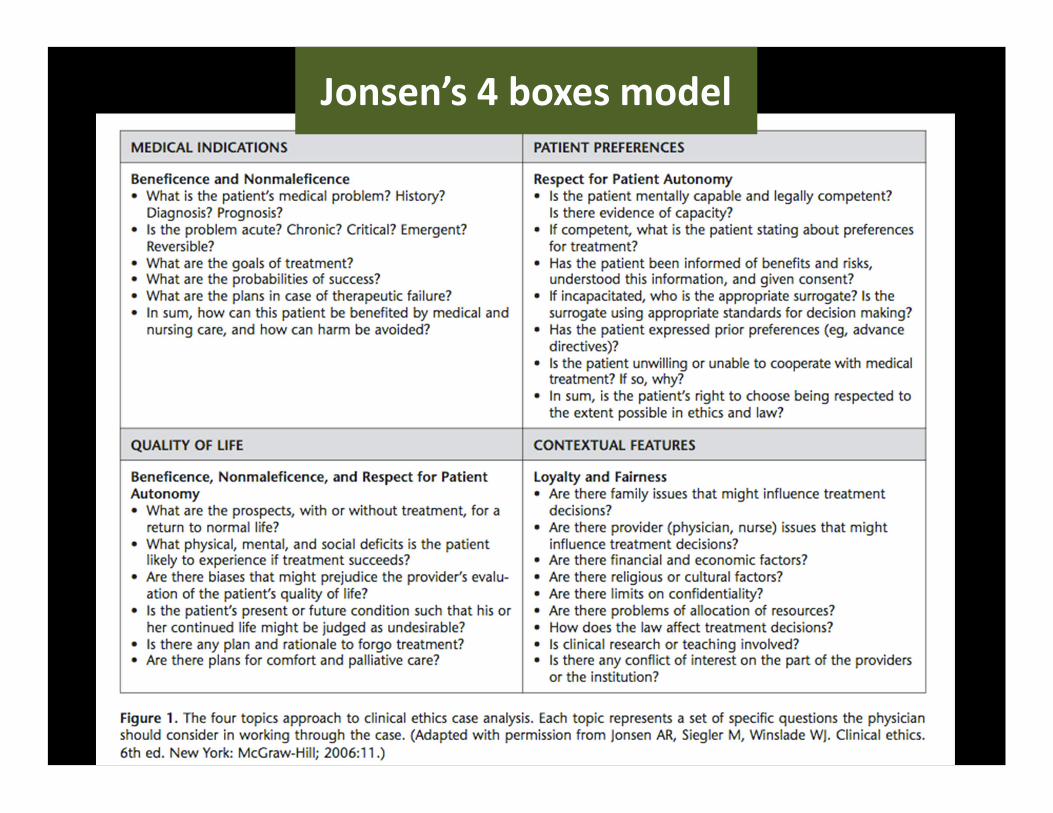
Jonsen’s 4 boxes model

Simplified version

1. Medical indication :
– Beneficence + Do no harm
– ‘Worth to treat’ Risk vs Benefit by evidence based
– Quantitative measureemnt ie survival, chance to recovery
vs risk of adverse effect
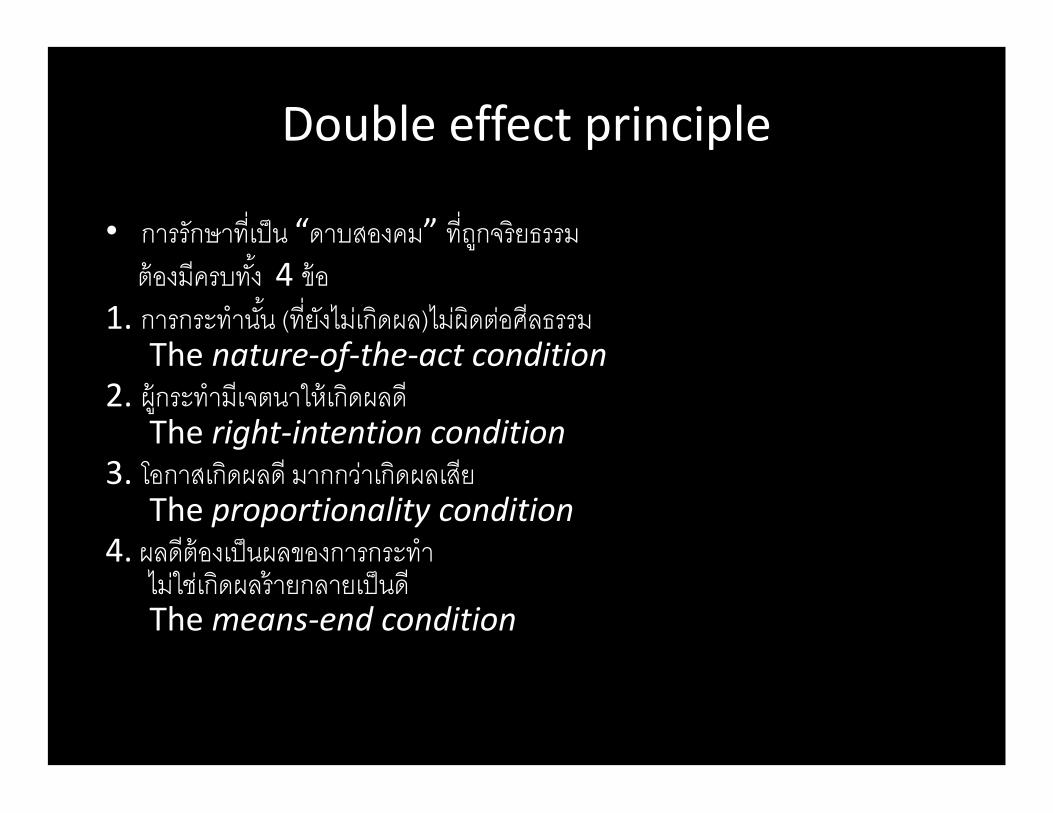
Double effect principle
• การรกษาท�เปน “ดาบสองคม” ท�ถกจรยธรรม ตองมครบท �ง 4 ขอ1. การกระทาน �น (ท�ยงไมเกดผล)ไมผดตอศลธรรม
The nature-of-the-act condition2. ผกระทามเจตนาใหเกดผลด
The right-intention condition3. โอกาสเกดผลด มากกวาเกดผลเสย
The proportionality condition4. ผลดตองเปนผลของการกระทา
ไมใชเกดผลรายกลายเปนดThe means-end condition
Double effect principleDouble effect principle

Double effect principle : Vaccine
การผลตยา และฉดยา
= Morally neutralผฉดมเจตนา ปองกนโรค
= Good intentionผลขางเคยงรายแรง (เชน ตบวาย) มได แตโอกาสเกดข�นนอย
= Good effect outweighs bad effectผลของการปองกนโรค เกดจากการฉดยา ไมไดเกดจากตบวาย
= Good ends not justify by evil means

Double effect principle : Terminal sedation
การใหยาโดยแพทย (ไมใชใหใครส�งยาใหกได)
= Morally neutralมเจตนาบรรเทาอาการเจบปวดทรนทราย
= Good intentionขนาดท�ให ปรบตามความอาการ โอกาสกดการหายใจมไดแตนอย
= Good effect outweighs bad effectผลของการบรรเทา เกดจากการหลบ ไมไดเกดจากกดการหายใจ
= Good ends not justify by evil means
* จงไมควรเขยนวา drip morphine for good death

2. Quality of life :
– Beneficence + autonomy
– ‘Worth to treat’ concern well being
– “Well being” in patient’s view
– Function ie ADL = predictive factorPerception = true indicator
3. Patient preference
– Autonomy
– Individual value vs Decision making capacity
– Patient’s advance care plan

1. General cognition : Awake + AttentionDepression and uncontroled symptom
2. Understand information : Tell me your understand about ‘Endotracheal tube’
3. Know consequence : Why you choose no Endotracheal tube
Decision making capacity test
4. Contextual feature
- Justice and Confidentiality
4.1 Family
– Family dynamics
– Care giver burden
4.2 Health care provider
– Cost
– Resource allocation
4.2 Society and religious value
- Reputation

Case demonstration
60 years old widow no child. she is known case end stage colon cancer PPS 40% (mostly bed bounded) she was admitted from sepsis and multiorgan failure she developed arrest. She talked with relatives want to die peacfully without CPR .However, she had no formal living will or any surrogate decision maker.
If you are her physician, what would you do.A. CPR
B. Respect her choice let her go
From 100 metastatic cancer who received CPRhow many survival to discharge?
A. 0
B. 5
C. 15
D. 30


Apply to everyday practice
1. Medical indication : -
2. Quality of life : -
3. Patient preference : +/- (no living will)
4. Contextual feature : - (ICU?)
Sum : - not encourage CPR

Exercise cases :A
60 years old widow no child.she is known case end stage colon cancer PPS 40% (mostly bed bounded) suffered from depression took overdose morphine : she was brought to ER with coma and reparatory depression (RR=6/min), she write in notepad that ‘No need helping, please let me go’. However, she had no formal living will or any surrogate decision maker.
If you are ER physician, what would you do.A. Intubation
B. Respect her choice let her go

Analysis
1. Medical indication : + Since cause is toxicity-> high chance of reversibility
2. Quality of life : -After reverse she may worsen PPS worsen spiritual suffering
3. Patient preference : + /-Her decision cannot count due to under depressionNo living will (the decision during intact capacity)
4. Contextual feature : +
Social and religious values negative to suicide
Sum : + encourage intubation

Exercise cases :B
60 years old widow no child. she is known case end stage colon cancer PPS 40% (mostly bed bounded) she was brought by 1669 after her relative found arrest (cause?),She had formal living will indicated that do not need intubation, CPR.
If you are her physician, what would you do.A. CPR and intubation
B. Respect her choice let her go
Analysis1. Medical indication : + /-
Since we don’t know it potential reversible (+) ie electrolyte imbalance or non-reversible (-) ie massive pulmonary embolii.
2. Quality of life : -cerebral anoxia ->she likely to worsen PPS Patient
3. preference : -living will
4. Contextual feature : +/-
It may took heavily investigation, ventilator need
Sum : - not encourage CPR

Exercise cases :C
60 years old married. she is known case end stage colon cancer PPS 40% (mostly bed bounded) she developed severe dyspnea and fever suspected aspiration pneumonia. She had formal living will indicated that do not need intubation. However her daughter want to save her life because fear of others might blame her if she refuse the treatment.
If you are her physician, what would you do.A. Intubation and antibiotics
B. Respect her choice let her go
Analysis
1. Medical indication : +/-End of life pneumonia is uncertained prognosis
2. Quality of life : +/-Since dyspnea may be contributed by infectionbut long intubation may increase suffering
3. Patient preference : -She had clear living will
4. Contextual feature : +
Her family issue
Sum : +/- Need discussion with her relatives
Exercise cases :D
80 years old married with advance alzheimer disease she develop difficult swallowing and poor intake. Her PPS is 30% (Complete bed bounded, totally care need). Her family worry if she should receive parenteral nutrition. Her daughter, only care giver, is economic strain single mom.
If you are her physician, what would you do.A. Advise PEG
B. Advise oral per mounth as tolerate
Analysis
1. Medical indication : +/-Evidence based showed PEG did not increase survival in advance dementia. However no RCTs
2. Quality of life : +/-Low intake not cause hungry It is part of catabolic stage
3. Patient preference : +/-She had no living will
4. Contextual feature : -
Increase burden to care giver
Sum : - Oral per mouth as tolerate

1. Palliative elements “3S”System, Symptom, Spiritual
2. Advance care plan Wish = GoalLiving will = Procedure +/- DPOA
3. Medical ethics in everyday life 4 boxes : Indication, QOL, Preference, Context
Take home massage