ppid advances in diagnostics and disease recognition · 11/27/2017 1 re-thinking ppid advances in...
TRANSCRIPT
11/27/2017
1
Re-thinking PPID
Advances in Diagnostics and
Disease Recognition
2
Craig F. Shoemaker DVM, MS
Professional Service
Boehringer-Ingelheim Vetmedica Inc.
3
Disclosures
Employed by Boehringer Ingelheim Animal Health
Overview
• Overview of PPID
• Clinical signs
• Diagnostic
– EEG Updates
• I.D. PPID
• Treatment/Management
• Additional considerations
• Take homes
4
Terminology
• PPID is the most common endocrine disorder in horses
• Equine Cushing's Disease should now be identified as:
• Pituitary Pars Intermedia Dysfunction (PPID)
5
Cushing’s Disease in Dogs/Man
• PU/PD
• Polyphagia
• Abdominal enlargement
• Lethargy
• Alopecia, pruritis
• Thin skin, pyoderma
• Panting
• Infertility

11/27/2017
2
Anatomy of the Equine Pituitary Gland
Three regions:
Pars distalis
Pars intermedia
Pars nervosa
Dopamine
7
Pathophysiology of PPID
• Dopamine interacts with D2 receptors in PI melanotrophs and inhibits activity
• Dopaminergic neurons undergo oxidative damage with aging
• Accelerated process in some horses
• As dopaminergic neurons are lost, melanotrophs are less inhibited
• Hyperplasia develops and melanotrophs secrete more hormones
• Permissive environment for neoplasia; functional pituitary adenomas develop
(McFarlane et al., J Neuroendocrinol 2005)
(Courtesy of Dianne McFarlane)
Pathophysiology
of PPID
(McFarlane D, et al. Nitration and increased alpha-synuclein expression associated with dopaminergic
neurodegeneration in equine pituitary pars intermedia dysfunction. J Neuroendocrinol 17:73-80, 2005.)
• In part, a consequence of oxidative damage
• Accumulation of misfolded α-synuclein in dopaminergic nerve terminals, similar to patients with Parkinson’s disease
• Both diseases are slowly progressive
• But why don’t PPID horses shake?
PPID and Parkinson's:
Loss of Dopaminergic Neurons
Risk Factors: Who Gets PPID?
• Risk Factors: Age, Breed
– Ponies are more susceptible
• Morgan horses
• Paso Fino
• Arabian
• Quarter horses
• Saddlebreds
• Warmbloods
• TWH
• 15-30% horses/ponies > 15 years of age
Rohrbach, Andrews F. Sommerdahl C. et al. J Vet Intern Med 2012
Frank N, Geor R. Bailey S. Durham A. and Johnson P, J Vet Intern Med 2006
What about horses younger than 15yr?
11
Risk Factors
12
Equine Metabolic Syndrome (EMS)
• Genetic predisposition to obesity
• Accompanied by insulin dysregulation (ID)
• Increased laminitis risk
– Accelerated degeneration of dopaminergic neurons
– Transitional period between diseases
– PPID developing in younger horses
– PPID exacerbates ID

11/27/2017
3
PPID Clinical Signs: Early vs.Late
Early
• Decreased athletic performance
• Change in attitude/lethargy
• Regional hypertrichosis
• Delayed haircoat shedding
• Skeletal muscle atrophy
• Typically beginning along the topline
• Regional Adiposity
• Laminitis
Advanced • Lethargy
• Generalized hypertrichosis
• Loss of seasonal haircoat shedding
• Skeletal muscle atrophy
• Rounded abdomen
• Abnormal sweating (increased or decreased)
• Polyuria/polydipsia
• Recurrent infections
• Regional adiposity
• Absent reproductive cycle / infertility
• Laminitis
• Seizure like activity/blindness
• Parasitism
• Tendon laxity/desmitis
13
Clinical Signs:
Change in Body Conformation/Condition
• Too FAT in some places
• Cresty neck
• Fat pads at tail head
• Bulging supraorbital fat
“Regional Adiposity”
• Too THIN in others
• Loss of topline muscle mass
• Swayed back
• Ribs visible
• Advanced: Rounded abdomen (pot-bellied)
"He's just getting old" 14
Early Signs
• Change in attitude:
• Little more lethargic
• Is he really that old?
• Delayed shedding of winter hairs
• Compare to other horses in the barn
• Discolored hairs
• Slow gradual loss of muscle mass
• Over the topline
• Unexplained Laminitis
(unconfirmed cause)
15
Abnormal Shedding
16
Abnormal Shedding
17
Abnormal Shedding
18

11/27/2017
4
Laminitis
19
Chronic laminitis:
• ~60-65% of PPID horses suffer from laminitis
• Insidious episodes that escape owner detection.
• Radiographic prevalence (43%) > clinical
evidence (12%) (Schott, 2011)
• Insulin status
• Main cause of euthanasia
Clinical Signs: Laminitis and PPID
Polyuria/Polydipsia
21
• May go unrecognized
• Freq. filling of water buckets
• Stall wetter than before/smells bad
• Hovering over water source
• Measure intake; provide additional
water sources
Increased Susceptibility to Infection
22
• Decreased WBC function – Immunosuppression
• Solar abscesses; systemic (liver, tongue)
• White line disease
• Dental disease – Sinusitis/tooth root abscesses
• Respiratory
• Skin
• Parasitism – Higher FEC’s
• Other infectious diseases?
Other symptoms
23
• Infertility/inappropriate lactation
• Abnormal sweating or inability to sweat
• Delayed wound healing
• Osteoporosis
• Recurrent tendon/ligament injury
Clinical Signs Associated with
PPID In The Equine Athlete
Kirchherr KF, Baus MR, Kremburg JR, Grubbs ST, Neal DL, and
Keefe TR
11/27/2017
5
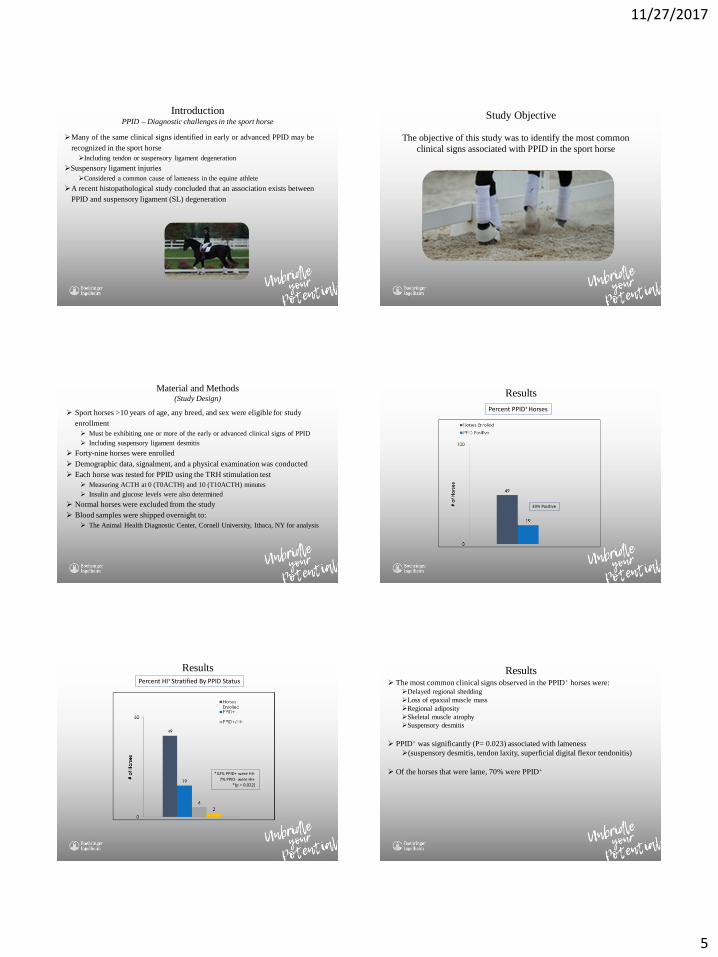
Many of the same clinical signs identified in early or advanced PPID may be
recognized in the sport horse
Including tendon or suspensory ligament degeneration
Suspensory ligament injuries
Considered a common cause of lameness in the equine athlete
A recent histopathological study concluded that an association exists between
PPID and suspensory ligament (SL) degeneration
Introduction PPID – Diagnostic challenges in the sport horse
Study Objective
The objective of this study was to identify the most common
clinical signs associated with PPID in the sport horse
Material and Methods (Study Design)
Sport horses >10 years of age, any breed, and sex were eligible for study
enrollment
Must be exhibiting one or more of the early or advanced clinical signs of PPID
Including suspensory ligament desmitis
Forty-nine horses were enrolled
Demographic data, signalment, and a physical examination was conducted
Each horse was tested for PPID using the TRH stimulation test
Measuring ACTH at 0 (T0ACTH) and 10 (T10ACTH) minutes
Insulin and glucose levels were also determined
Normal horses were excluded from the study
Blood samples were shipped overnight to:
The Animal Health Diagnostic Center, Cornell University, Ithaca, NY for analysis
39% Positive
Percent PPID+ Horses
Results
*32% PPID+ were HI+ 7% PPID- were HI+ *(p = 0.022)
Percent HI+ Stratified By PPID Status
Results Results The most common clinical signs observed in the PPID+ horses were:
Delayed regional shedding
Loss of epaxial muscle mass
Regional adiposity
Skeletal muscle atrophy
Suspensory desmitis
PPID+ was significantly (P= 0.023) associated with lameness
(suspensory desmitis, tendon laxity, superficial digital flexor tendonitis)
Of the horses that were lame, 70% were PPID+

11/27/2017
6
Diagnostics
31
• Nicholas Frank, DVM, PhD, DACVIM
• Frank Andrews, DVM, MS, DACVIM
• Ben Buchanan, DVM, DACVIM, DACVECC
• Andy Durham, BSc, BVSc, CertEP, DECEIM, MRCVS
• Janice Kritchevsky, VMD, MS, DACVIM
• Dianne McFarlane, DVM, PhD, DACVIM
• Hal Schott, DVM, PhD, DACVIM
http://sites.tufts.edu/equineendogroup/
TRH Stimulation
34
TRH Stimulation
Interpretation of Results
35
Thyrotropin Releasing Hormone (TRH)
36
Sources:
• Reagent grade from Sigma; expensive
• Protirelin- Compounded from Wedgewood
– Validated by EEG
– 1mg/ml
– 1ml vial $45.00
– 5ml vial $60.00
– Can be frozen
11/27/2017
7
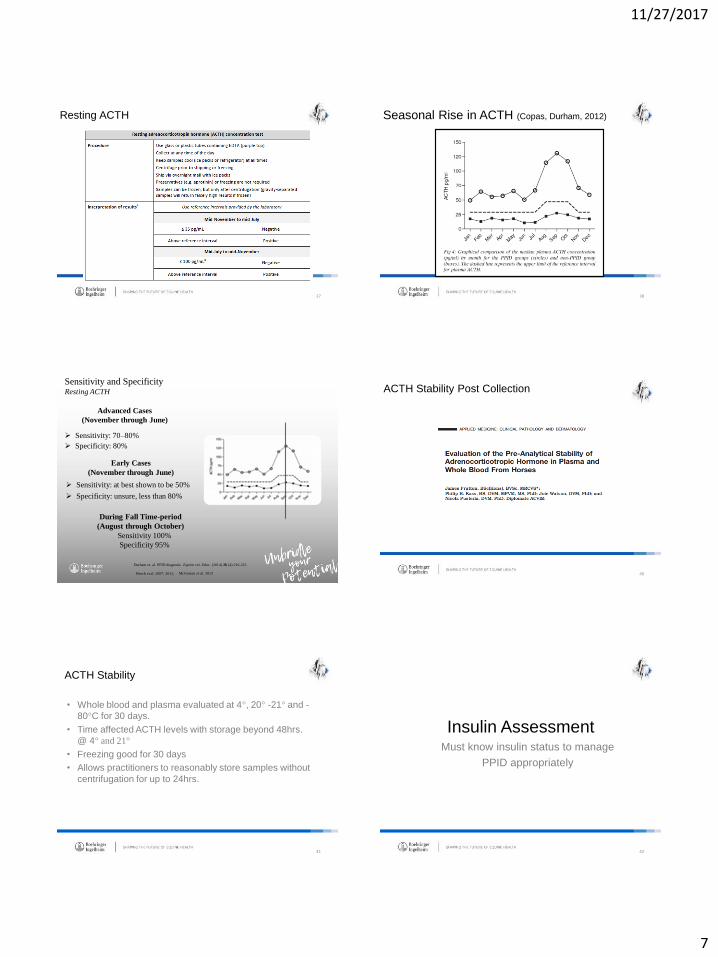
Resting ACTH
37
Seasonal Rise in ACTH (Copas, Durham, 2012)
38
Sensitivity and Specificity Resting ACTH
Sensitivity: 70–80%
Specificity: 80%
39 Beech et al. 2007; 2011;
Durham et. al. PPID diagnosis. Equine vet. Educ. (2014) 26 (4) 216-223
McGowan et al. 2013
Advanced Cases
(November through June)
Early Cases
(November through June)
Sensitivity: at best shown to be 50%
Specificity: unsure, less than 80%
During Fall Time-period
(August through October)
Sensitivity 100%
Specificity 95%
ACTH Stability Post Collection
40
ACTH Stability
41
• Whole blood and plasma evaluated at 4°, 20° -21° and -
80°C for 30 days.
• Time affected ACTH levels with storage beyond 48hrs.
@ 4° and 21°
• Freezing good for 30 days
• Allows practitioners to reasonably store samples without
centrifugation for up to 24hrs.
Insulin Assessment
42
Must know insulin status to manage
PPID appropriately

11/27/2017
8
Fasting Insulin
44
Insulin Assessment
Oral Sugar Test
45
ID PPID
46
Purpose: To gather clinical information that includes signalment, clinical signs, resting ACTH, fasting insulin, and fasting glucose results obtained at diagnosis from horses within the US that have at least one clinical sign associated with PPID.
ACTH TESTING OVERALL RESULTS
47
526
217
0
100
200
300
400
500
600
# o
f H
ors
es
Samples Submitted
PPID Positive
41% Positive
PPID Master_537 n= 537
Percent PPID+ Horses
Age Groups of Horses Enrolled n=526
48
33
103
158
137
69
26
0
20
40
60
80
100
120
140
160
180
Under 10 10--15 15--20 20--25 25--30 30 and older
# o
f H
ors
es
*2 horses with unknown age
PPID by age table n= 526

11/27/2017
9
PPID+ Horses
49
4
21
52
70
51
19
33
103
158
137
69
26
0
20
40
60
80
100
120
140
160
180
under 10 10--15 15-20 20-25 25-30 30 andolder
# o
f H
ors
es
PPID positive
Total
12%
20%
33%
51%
74%
73%
PPID by age table n= 526
PPID+ Horses By Age
Clinical Signs Present At Initial Diagnosis
50
294
267
181 181 170 161 161
51 50 44 42 38
0
50
100
150
200
250
300
350
Delayedshedding
Cresty neck Decreasedathletic
behavior
Laminitis Loss ofmuscle mass
Weight loss Potbelly/weight
gain
Excessiveurination
Excessivethirst
Abnormalsweating
Recurrentinfections
Other
# o
f H
ors
es
*Categories are NOT Mutually Exclusive
and are Independent of ACTH test results
Clinical Signs Table n= 537 11 horses had missing ACTH value
Results
51
Five-hundred fifteen horses in final data
66 breeds/cross-breeds represented
222 (43%) were PPID+
203 (39.4%) were HI+*
Further stratified into1 of 4 groups
(PPID+/HI-)
(PPID+/HI+)
(PPID-/HI+)
(PPID-/HI-)
*IR = Insulin resistant
Results
52
Of the 515 horses:
115 (22.3%) were PPID+/HI-
97 (18.8%) were PPID+/HI+
106 (20.6%) were PPID-/HI+
197 (38.3%) were (PPID-/HI-)
318 (61.7%) horses diagnosed with endocrine disease
Treatment
53
• Prascend® gold standard of care
• Only FDA licensed product
– Dopamine agonist
– Safety and efficacy studies
– Product support
– 1mg 60 and 160 tablet blister packs
– Easily administered
– Demonstrated STABILITY!
– Improves quality of life
Pergolide Cloud/Veil
54
• Horses occasionally appear depressed when treatment
initiated; may show inappetance
• Practical approach:
– Stop treatment for 2 days
– Start treatment at .5mg/day
– Gradually return to full treatment dose

11/27/2017
10
Treatment and monitoring
55
• Perform baseline diagnostics (ACTH or TRH stim.)
• (Initiate Prascend® tx. (.5mg 250 kg pony/1.0mg 500kg)
• Retest with same test in 30 days
– May take 2 months to assess clinical signs
• Initial response (first 30 days)
– Incr. activity, improved attitude, PU/PD, hyperglycemia
• Long term response (1-12 months)
– Imprv. hair coat, incr. skeletal mm. mass, fewer infections
and episodes of laminitis
Uncle Sam- 6 mo. treatment
56
Brown- 6 mo. treatment
57
Phantom- 6 mo. treatment
58
59
Other Considerations
60
• Switching from compounded pergolide
– Current status of horse
– If well controlled consider lower Prascend® dose (50% reduction)
– Retest after 30 days

11/27/2017
11
Other Considerations
61
• Removing horses from pergolide
– Missing doses due to exhibition/competition
• ACTH may begin to rise in 48 hours
– 3/6 50% rise by day 2
– 6/6 by day 10
• Risk of worsening clinical signs is low
• USEF considering exemption rule
Other Considerations
62
• Diet and Exercise
– Feed selection based on body score and oral sugar
test
– Normal insulin; normal diet and pasture
– Obese (>7/9) lower energy diet/exercise
– Insulin dysregulation; lower NSC and limit pasture
– Dietary supplements?
Other Considerations
63
• Wellness care
– Should include dentistry and parasite control
– Foot care
– Inadequate control predisposes to infections
– Attention to body condition
– Diet; insulin dysregulation
Summary
64
• Treatment of PPID is truly individualized
medicine
• Test any time of year using resting ACTH • Dynamic test with seasonal reference ranges
• TRH stimulation mid Nov. to mid July • Early cases or where lab work does not “fit”
• No seasonally adjusted reference ranges
• Insulin/glucose status must be known
Manage the “whole horse” not just endocrine test results
Questions?
65