powerpoint presentation - suicide_basic - cbhc
TRANSCRIPT

University of Colorado
Depression Center
© M. Allen 2010
1
Driving Toward Zero: Preventing Suicide in Your Organization
September 28,2013
Michael H. Allen, M. D.
Professor of Psychiatry and Emergency Medicine
University of Colorado School of Medicine
Director of Research
University of Colorado Depression Center
Senior Investigator
VISN 19 Mental Illness Research, Education and Clinical Center

University of Colorado
Depression Center
Outline
1. 2012 Stats
2. Individual Level
A. Review of Risk Factors, Warning Signs
B. Suicidal Process
C. “Must Know” Elements of Assessment
D. SAFE – T
E. Joiner’s Model: Desire, Intent, Capability
I. Risk Stratification
II. Cases
F. Intervention
© M. Allen 2010
2

University of Colorado
Depression Center
Outline
3. System
A. Strategy
B. Failures
C. Quality
D. Programmatic Improvements
© M. Allen 2010
3

University of Colorado
Depression Center
© M. Allen 2008
4
Suicide Rates, US and Colorado R
ate
/10
0,0
00
0
5
10
15
20
25
199019
9119
9219
9319
9419
9519
9619
9719
9819
9920
0020
0120
0220
0320
0420
0520
0620
0720
0820
0920
1020
1120
12
Crude rates
Healthy People 2000 Goal 6.1 Reduced 10% to 10.5
Colorado
United
States
1053
http://webappa.cdc.gov/sasweb/ncipc/mortrate10_sy.html

University of Colorado
Depression Center
© M. Allen 2010
5
Suicidal thinking is common
Lifetime ECA, 80’s
Lifetime NCS, 80’s
1 Year ICARIS, ‘94
Ideation 11.2% 13.5% 5.6%
Plan 3.9 2.7
Attempt 3.1 4.6 .7
ECA, lifetime, 1980’s
NCS lifetime, n= 5877, 1990’s
Crosby AE, et al. SLTB 1999; 29:131. n=5238
>10% think about it in their lifetime

University of Colorado
Depression Center
© M. Allen 2010
6
Adolescence
Common over 18 months 6-7 grade
60.5% endorsed at least one item
32.9% thoughts of death and dying
6% thought of killing themselves
Generally declined over this period
2% had persistently high SI
Vander Stoep A, et al. SLTB 2009;39(6):599

University of Colorado
Depression Center
© M. Allen 2010
7
About 4% experience suicidal thoughts each year.
About 1/4 of those with SI make suicidal plans.
About 1/3 of those make an attempt.
About 1 in 15 or 20 die.

University of Colorado
Depression Center
© M. Allen 2010
8
Most do not volunteer the information
Different settings
Community survey
– 44% with SI saw no need for treatment
• 38% received care vs 73%
Mental health centers
– 73% did not report SI
Inpatient or recent discharges
– 78% denied SI and 28% had “contract”

University of Colorado
Depression Center
© M. Allen 2010
9
Most who die, die on first attempt,
78% by the second attempt.
0% 50%
Isometsa,1998
Conwell,1998
Roy, 1982
Subsequent First
Roy A. Arch Gen Psych 1982, 39:1089.
Conwell Y, et al: Am J Geri Psych 1998, 6:122-126.
Isometsa ET : Br J Psychiatry 1998 173: 531-535
56 22 9 13
68 21 6 5
0% 25% 50% 75% 100%
All
Male
>45
2/3 of males over 45

University of Colorado
Depression Center
© M. Allen 2010
10
Most likely to do it,
Least likely to talk about it
Attempters, n = 211
Prior verbalization not correlated with wish
o to die at time of subsequent attempt
Talking related to personality style,
not level of despair
Suffer in silence or
emit coded warning signals
Kovacs, et al. Arch Gen Psych 33:198, 1976

University of Colorado
Depression Center
© M. Allen 2010
11
Particularly True of Adolescents
Risk of Medically Treated Attempts in Adolescents
1999 Youth Risk Behavior Survey
High risk sex
Binge drinking
Drug use
Violence
Eating
Smoking
0
10
20
30
40
50
Od
ds
of
Att
em
pt
1 2 3 4 5# Behaviors
17% of youths 4-6 behaviors - 60% of attempts
1.2% all 6 – 16% of attempts
Miller TR and Taylor DM. SLTB 35(4):425-435, 2005
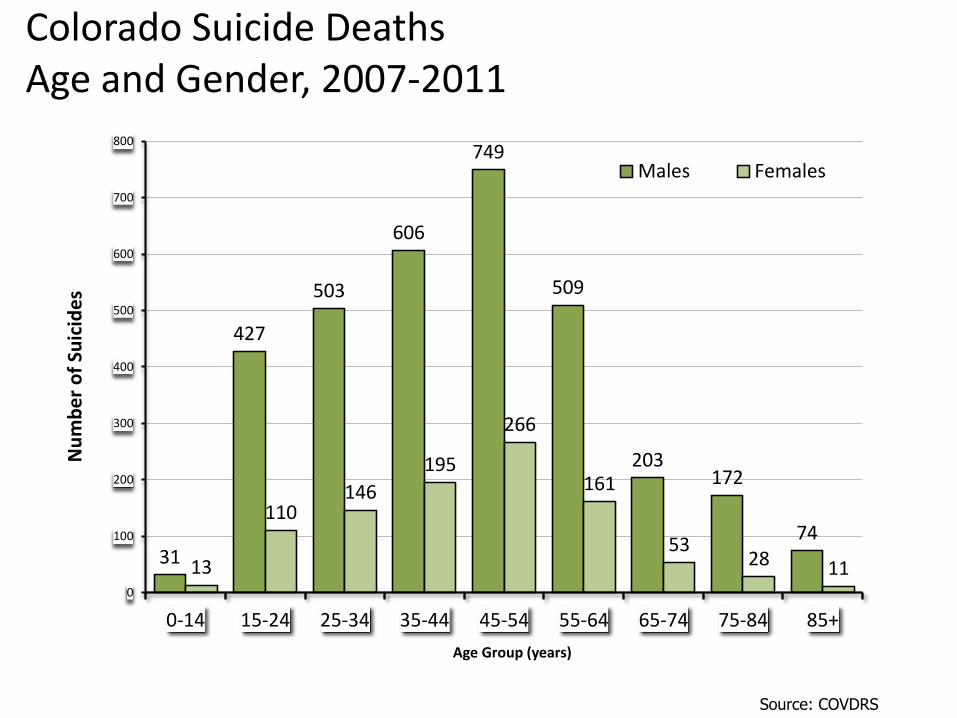
Colorado Suicide Deaths Age and Gender, 2007-2011
Source: COVDRS
31
427
503
606
749
509
203 172
74
13
110 146
195
266
161
53 28 11
0
100
200
300
400
500
600
700
800
0-14 15-24 25-34 35-44 45-54 55-64 65-74 75-84 85+
Nu
mb
er
of
Suic
ide
s
Age Group (years)
Males Females

University of Colorado
Depression Center
© M. Allen 2010
13
Of men who survive an attempt,
almost 1/3 kill themselves over 25 years P
roport
ion S
urv
ivin
g
90%
70%
100%
80%
60%
Men
Women
10 20 30
Suominen, K. Am J Psychiatry 161(3): 562-563, 2004

14
© M. Allen 2008
Violence and Suicide Capability
Conner et al. Am J Psych 2001; 158: 1701
4.61.5
6.9
11.6
1.5
6.9 8
Violent Alcohol
Alone
Violence
Alcohol
Violence
Alone
Male Violent
Male
Violent
Female
Violence sometimes or often increases risk
Particularly for women
Violence + alcohol not additive
Odds ratio, 95% CI

University of Colorado
Depression Center
© M. Allen 2010
15
Suicidal Process
Suicide
Facilitation
Survival
Inhibition
Acute Mood Change
Stress
Vulnerabilty
Joiner T.
Crisis
Safety Plan
Means
Substances
Supervision
Hope, pleasure
Acquired
Genetic Assessment
Risk factors
Warning signs

University of Colorado
Depression Center My Own Top 8 Risk Factors
and Warning Signs
1. Prior attempt with intent to die
2. Worst SI ever
3. Substance abuse (increase)
4. Irritability, (reactive) aggression
5. Severe anxiety, agitation
6. Insomnia
7. Severe mental illness, hospitalization
8. Recent change in reasons for living
o Child/pet care, partner separation

University of Colorado
Depression Center
Other Risk Factors or
Warning Signs?
© M. Allen 2010
17
University of Colorado
Depression Center Suicide Assessment Five Step
Evaluation and Triage (SAFE-T)
Suicide inquiry
Risk factors
Protective factors
Risk stratification and intervention
Documentation
© M. Allen 2010
18
SAMHSA
Google “safe t suicide”
http://store.samhsa.gov/shin/content//SMA09-4432/SMA09-4432.pdf

University of Colorado
Depression Center
© M. Allen 2010
19

University of Colorado
Depression Center
© M. Allen 2010
20
Suicidal Desire
Suicidal ideation
Psychological pain
Perceived burden on others
Hopelessness; helplessnes
Mental illness
• Demoralization

University of Colorado
Depression Center
© M. Allen 2010
21
Suicidal Intent
Plan to kill self/other
Preparatory behaviors
Expressed intent to die
Attempt

University of Colorado
Depression Center
© M. Allen 2010
22
Suicidal Capability
History of suicide attempts
Exposure to someone else’s suicide
Exposure to violence
Available means of killing self/other
Intoxication
Chronic intoxication
Acute symptoms of mental illness
• Sleep disturbance, psychotic guilt
Extreme agitation/rage

University of Colorado
Depression Center
© M. Allen 2010
23
Protective Factors or Buffers
Immediate supports
Social supports
Planning for the future
Engagement with others, helpers
Ambivalence about living/dying
Core values/beliefs
Sense of purpose

University of Colorado
Depression Center
© M. Allen 2010
24
High Risk
Role of protective factors unclear
D=Desire C=Capability I=Intent
D C I

University of Colorado
Depression Center
© M. Allen 2010
25
Moderate to High Risk
D=Desire C=Capability I=Intent
Protective factors may influence risk
Desire paired with intent or capability
D I
D C

University of Colorado
Depression Center
© M. Allen 2010
26
Moderate to Low Risk
D=Desire C=Capability I=Intent
Any core factor presenting alone
Source: Joiner, Thomas. Establishing Standards for the Assessment of Suicide
Risk Among Callers to the National Suicide Prevention Lifeline. Suicide and
Life-Threatening Behavior. 2007;37(3):253-365.
D C I

University of Colorado
Depression Center
SAFE-T Stratification
Highest level is most important
© M. Allen 2010
27

University of Colorado
Depression Center
Case
50 year old male career fire fighter
Anniversary of wife’s death
Gambling problem, impending bankruptcy
Appears distraught at work, sent to ER
Complains of severe insomnia
• Meds have not helped
Appears restless, anxious and guarded
Meets criteria for Major Depression
Some thoughts of death but denies SI
© M. Allen 2010
28

University of Colorado
Depression Center
SAFE-T Stratification
Highest level is most important
© M. Allen 2010
29

What is Safety Planning?
• A brief clinical intervention
• Follows risk assessment
• A hierarchical and prioritized list of coping strategies and sources of support
• To be used during or preceding a suicidal crisis
• Involves collaboration between the patient and clinician
Stanley, B., & Brown, G.K. (with Karlin, B., Kemp, J.E., & VonBergen. H.A.). (2008). Safety Plan Treatment Manual to Reduce Suicide Risk: Veteran Version. Retrieved from http://www.sprc.org/library/SafetyPlanTreatmentManualReduceSuicide RiskVeteranVersion.pdf

• Ways to increase collaboration
– Sit side-by-side
– Use a paper form
– Allow the client to write
• Brief instructions using the client’s own words
• Easy to read
• Address barriers and use a problem-solving approach
Tips for Developing a Safety Plan
Stanley, B., & Brown, G.K. (with Karlin, B., Kemp, J.E., & VonBergen. H.A.). (2008). Safety Plan Treatment Manual to Reduce Suicide Risk: Veteran Version. Retrieved from http://www.sprc.org/library/SafetyPlanTreatmentManualReduceSuicide RiskVeteranVersion.pdf

• No-suicide contracts ask patients to promise to stay alive without telling them how to stay alive.
• No-suicide contracts may provide a false sense of assurance to the clinician.
• DON’T USE THEM! No Suicide Contract
“No-Suicide Contracts”


6 Steps of Safety Planning
• Step 1: Recognizing Warning Signs
• Step 2: Using Internal Coping Strategies
• Step 3: Utilizing Social Contacts that Can Serve as a Distraction from Suicidal Thoughts and Who May Offer Support
• Step 4: Contacting Family Members or Friends Who May Offer Help to Resolve the Crisis
• Step 5: Contacting Professionals and Agencies
• Step 6: Reducing the Potential for Use of Lethal Means
44

Step 1: Recognize Warning Signs
• Purpose: To help the client identify and pay attention to his or her warning signs
• Recognize the signs that immediately precede a suicidal crisis
• Personal situations, thoughts, images, thinking styles, mood or behavior
• “How will you know when the safety plan should be used?”
• Specific and personalized examples

Step 2: Using Internal Coping Strategies
• Purpose: To take the client’s mind off of problems to prevent escalation of suicidal thoughts
– NOT to solve the client’s problems
• List activities the client can do without contacting another person
• This step helps clients see that they can cope with their suicidal thoughts on their own, even if only for a brief period of time
• Examples: Go for a walk, listen to inspirational music, take a hot shower, play with a pet

Step 2: Using Internal Coping Strategies
• Ask “How likely do you think you would be able to do this step during a time of crisis?”
• Ask “What might stand in the way of you thinking of these activities or doing them if you think of them?”
• Use a collaborative, problem solving approach to address potential roadblocks.

What would safety planning with this patient look like?
64 year old Vietnam Veteran was hospitalized in the context of alcohol use, worsening PTSD
symptoms and suicidal ideation with a plan to shoot himself. He has consistently been denying suicidal ideation since he was admitted to the
hospital following detox 5 days ago. He is requesting discharge from the hospital, stating
that he only experienced suicidal ideation because he was intoxicated.

“VA safety plan quick guide”

University of Colorado
Depression Center
Strategy
© M. Allen 2010
40

University of Colorado
Depression Center
41
© M. Allen 2009
41
Occult SI in 3-11.6% of ED Visits
Study Definition of Ideation Freq (%)
Allen (2013)
CSSRS Passive SI
CSSRS Active SI
Any SI and history or attempt
79/1068 (7.5)
24/1068 (2.25)
12/1068 (3.3)
ED-SAFE Retro Any mention of suicidal behavior 23 / 800 (2.9)
ED-SAFE TAU Any mention of suicidal behavior 2771 / 94,385 (2.9)
NIMH Multicenter
Allen MH, et al. Suicide Life Threat Behav 2013; 42 (3):313-323.

Suicide deaths by circumstance, 2007-2011
Source: COVDRS
N Percent*
Current depressed mood 2,507 62.6
Current mental health problem 1,682 42.0
Left a suicide note 1,603 40.0
Ever treated for mental health problem 1,584 39.5
Disclosed intent to die by suicide 1,539 38.4
Intimate partner problem 1,490 37.2
Crisis within two weeks of the suicide 1,393 34.8
Current mental health treatment 1,323 33.0 Physical health problem 1,277 31.9
Diagnosis of depression 1,251 31.2
History of previous suicide attempts 1,122 28.0
Problem with alcohol 1,075 26.8
Financial problem 903 22.5
Job problem 862 21.5
Problem with other substance 611 15.3 *Percent of total cases with at least one circumstance known; Colorado residents who died in Colorado

University of Colorado
Depression Center
Driving Toward Zero
Aspirational goal
National Strategy
Possible bounded systems
Focus on suicide distinct from
treatment of mood disorders
oNOTE no mention of depression
© M. Allen 2010
43

University of Colorado
Depression Center US Institute of Medicine
“Crossing the Quality Chasm”
Conclusions
“In its current form, habits, and
environment, American health care is
incapable of providing … the quality of
health care it expects and deserves.”
“Current care…honors and protects
unscientific variations in care based on
local habits, unquestioned forms of
autonomy and insufficient curiosity.”
Berwick DM. Health Affairs 21(3):80, 2002

University of Colorado
Depression Center US Institute of Medicine
“Crossing the Quality Chasm”
Six dimensions of care
Safety
Effectiveness
Patient-centeredness
Timeliness
Efficiency
Equity
Berwick DM. Health Affairs 21(3):80, 2002

University of Colorado
Depression Center US Institute of Medicine
“Crossing the Quality Chasm”
Ten simple rules
6. “Do no harm” individual
responsibility
7. Secrecy necessary
Litigation
8. System reactive
9. Reduce costs
10. Traditional prof
roles over system needs
Safety a property
of systems
Quality requires
transparency
Anticipates needs
Reduce waste
Cooperation is a
priority
Berwick DM. Health Affairs 21(3):80, 2002

University of Colorado
Depression Center US Institute of Medicine
“Crossing the Quality Chasm”
Ten rules for microsystems
1. Care based on visits
2. Professional autonomy drives
variability
3. Professionals control care
4. Information owned by
providers
5. Decision making based
on training, experience
Care is continuous
Customized to patient
needs, values
Patient controls care
Knowledge shared
Based on evidence,
not vary illogically
Berwick DM. Health Affairs 21(3):80, 2002

University of Colorado
Depression Center
Henry Ford Health System
© M. Allen 2010
48
Active mood disorder
Euthymic mood disorder
Gen’l pop
Henry Ford
Zero

University of Colorado
Depression Center
© M. Allen 2013
49
Preventability of Suicide
Victoria State, Australia
629 psychiatric patient suicides/5 yrs
67% prior attempt
49% attention within the prior 4 weeks
20% preventable
Burgess P, et al: Psych Services 51:1555, 2000

University of Colorado
Depression Center
© M. Allen 2013
50
Preventability of Suicide
National survey, England/Wales, 1 yr
2,370 of 10,040 suicides had MH contact
26 % drug noncompliance
28 % lost to follow up
Last contact, risk “absent” 30 %,
“low” 54 %, “mod” 13 % and “high” 2 %
22% preventable
Appleby L, et al. BMJ 318:1235, 1999

University of Colorado
Depression Center
© M. Allen 2013
51
Preventing the 20 %
Burgess et al, Appleby et al
Relationship
Assessment
– Risk assessment
– Comorbidity, Sx’s unrelated to 1° Dx
Treatment
– 10 % OD of psychotropics
– Nonadherence meds and appts

University of Colorado
Depression Center
© M. Allen 2010
52
Specialty Mental Health
Recommendations
Training
Regular assessment
Structured
Frequent, every visit in some cases
• Criteria for low / moderate / high
Safety planning
Means, environment
Support, supervision
Substance use
Hope, pleasure

University of Colorado
Depression Center
Work Force Preparation
Qualifications are low and training is poor
Psychiatry: 91% - mean 3.6 hrs, 27% skills
Psychology: 50%
Social Work: less that 25%
Marriage and Family Therapists: 6%
Counselors: 2%
No state Continuing Education requirements
Schmitz W, et al. AAS Task Force Rep. SLTB 2012;42(3):292-304

University of Colorado
Depression Center
54
Tools
1. Question Persuade Refer (QPR)
o Different versions
2. Mental Health First Aid (MHFA)
3. Applied Suicide Intervention Skills Trng
(ASIST)
How many have attended one of these?

University of Colorado
Depression Center
© M. Allen 2010
55
Specialty Mental Health
Recommendations
Training
Improved assessment
Structured
Columbia Suicide Severity Rating Scale
Frequent, every visit in some cases
• Criteria for low / moderate / high
• Flagging or communicating risk
Safety planning
Means restriction
Small prescriptions, blister packs

University of Colorado
Depression Center
© M. Allen 2010
56
Specialty Mental Health
Training
Improved assessment
Safety planning
Treatment
• Measurement, eg, depression
• Goal “well”, not better
• Comorbid conditions, eg, anxiety
• Substance Abuse
• Patient centered
Man Therapy PSA
www.mantherapy.org

University of Colorado
Depression Center
© M. Allen 2010
57
Specialty Mental Health
Training
Improved assessment
Safety planning
Treatment
Continuity and outreach
• Relationship issues
• Transitions between settings
• Suicide Prevention Coordinators
• HOME
• Missed appointment policy
• Call or visit
• Mobile Crisis

HOME Program Description
Risk assessment over the phone within 1 business day
Home visit within first week of discharge
-Risk assessment
-Review and revise discharge plan and safety plan
-Meet with support system
-Review upcoming appointments
Follow-up until engaged in care

How the Lifeline Works
• Callers dial 800-273-TALK or 800-SUICIDE
• Callers are connected to closest center
• “Press 1” for Veterans, Military
• Extensive back-up system ensures all calls
are answered
• Crisis workers listen, assess, and link/refer
callers to services, as needed
– Some centers professional, some volunteer
• Chat, text systems

VISN 19 MIRECC Website
http://www.mirecc.va.gov/
visn19/
Research
Education
Clinical Care
Assessment Tools
Fellowship Info
Personnel
Presentations
Study Participation
Contact Us