poverty perceptions of social workers and physicians in israel
TRANSCRIPT

This article was downloaded by: [University of Cambridge]On: 08 October 2014, At: 11:18Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registeredoffice: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Social Work in Health CarePublication details, including instructions for authors andsubscription information:http://www.tandfonline.com/loi/wshc20
Poverty Perceptions of Social Workersand Physicians in IsraelMenachem Monnickendam PhD aa Louis and Gabi Weisfeld School of Social Work, Bar Ilan University ,Ramat Gan, IsraelPublished online: 25 Nov 2010.
To cite this article: Menachem Monnickendam PhD (2010) Poverty Perceptions of Social Workers andPhysicians in Israel, Social Work in Health Care, 49:10, 963-980, DOI: 10.1080/00981389.2010.518877
To link to this article: http://dx.doi.org/10.1080/00981389.2010.518877
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the“Content”) contained in the publications on our platform. However, Taylor & Francis,our agents, and our licensors make no representations or warranties whatsoever as tothe accuracy, completeness, or suitability for any purpose of the Content. Any opinionsand views expressed in this publication are the opinions and views of the authors,and are not the views of or endorsed by Taylor & Francis. The accuracy of the Contentshould not be relied upon and should be independently verified with primary sourcesof information. Taylor and Francis shall not be liable for any losses, actions, claims,proceedings, demands, costs, expenses, damages, and other liabilities whatsoever orhowsoever caused arising directly or indirectly in connection with, in relation to or arisingout of the use of the Content.
This article may be used for research, teaching, and private study purposes. Anysubstantial or systematic reproduction, redistribution, reselling, loan, sub-licensing,systematic supply, or distribution in any form to anyone is expressly forbidden. Terms &Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions
Social Work in Health Care, 49:963–980, 2010Copyright © Taylor & Francis Group, LLCISSN: 0098-1389 print/1541-034X onlineDOI: 10.1080/00981389.2010.518877
Poverty Perceptions of Social Workers andPhysicians in Israel
MENACHEM MONNICKENDAM, PhDLouis and Gabi Weisfeld School of Social Work, Bar Ilan University, Ramat Gan, Israel
This qualitative study comparing poverty perceptions of socialworkers (SWs) and primary care physicians (PCPs) employed inIsrael’s public services found that both attributed the poverty oftheir own clients to similar causes—individualistic, structural,fate, and policy—but differed in most of their perspectives andmoral imperatives. The PCPs tended to be more angry, skepti-cal, and accusatory than the SWs, who were more forbearingand accepting. Both believed that those in a position to workshould, but only PCPs held that they should work for any salary.With respect to policy, PCPs looked at the macro, SWs at themicro. The findings suggest that it might be more fruitful to keepinter-professional discussions on the poor and poverty pragmatic,rather than theoretical and principled.
KEYWORDS poverty perception, social worker, primary carephysician, client, patient, moral imperative
Perceptions of poverty—its causes and remedies, as well as perspectiveson persons who are poor—cannot but affect policies toward povertyand persons living in poverty (Weiss-Gal, Benyamini, Ginzburg & Savaya,2009). Research shows that these perceptions, whether held by profession-als (Sandfort, Kalil & Gottschalk, 1999) or the public at large (Cozarelli,Wilkinson & Tagler, 2001), are associated with the willingness to help alle-viate or end poverty, and with attitudes toward welfare and welfare reform.Other findings show that elites’ perceptions of poverty and of persons who
Received May 11, 2010; accepted August 4, 2010.Address correspondence to Menachem Monnickendam, PhD, Director, Graduate Studies,
Louis and Gabi Weisfeld School of Social Work, Bar Ilan University, Ramat Gan, 52900, Israel.E-mail: [email protected]
963
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ambr
idge
] at
11:
18 0
8 O
ctob
er 2
014

964 M. Monnickendam
are poor have been pivotal to their initiatives to create collective and publicarrangements for remedying poverty (De Swaan, Manor, Oyen & Reis, 2000).
The present study examines and compares the poverty perceptions ofsocial workers (SWs) and primary care physicians (PCPs) in Israel. In Israel, asin the United States and United Kingdom, many community health clinics andsocial services operate in poor neighborhoods, so that both SWs and PCPsserve poor people. Knowing their poverty perceptions is important becauseof evidence that these perceptions influence their service delivery. Benson(2000) found that U.S. physicians treat patients they perceive as temporarilypoor differently from those they perceive as chronically poor. Research onSWs employed in social service departments in the United Kingdom (Dowling,1999, p. 108) shows that their view of clients as deserving or undeservingaffected whether or not they gave them financial assistance. The same studyfound that SWs perceptions of their departments’ role with regard to povertyinfluenced their handling of poor clients’ financial problems as well as thesensitivity of service delivery to the circumstances of the poor. A recentstudy in Israel linked SWs’ failure to develop services that are sensitive tothe circumstances of the poor with their uncertainty as to their professionalrole and responsibilities with regard to poverty and their not perceivingthe poor as a target population (Monnickendam, Katz, & Monnickendam,2010). According to Strier (2008), understanding the differences in povertyperceptions of agencies and clients was conducive to overcoming obstaclesto effective service delivery. Research in Israel and Belgium shows that PCPs’poverty perceptions were associated with their waiving user-fees for visits,donating medical samples, and using simple language in their encounterswith patients living in poverty (Willems, Swinnen & De Maeseneer, 2005;Monnickendam, Monnickendam, Katz, & Katan, 2007).
Both social work and medical literature stress the need for improvedteamwork to provide better community health care for the poor (Green,2000; Russel, 2006). Comparing the perceptions of SWs and PCPs is impor-tant because of the possible impact of their poverty perceptions on theirability to work collaboratively. Two studies on the collaboration of SWsand PCPs found that their cooperation was enhanced when they agreed notonly on the medical issues but, more importantly, on the “nature and defi-nition” of the patient (Carpenter & Hewstone, 1996; Hudson, 2002), that is,when they held similar views of the patient in the environment. The find-ings do not mean that when SWs and PCPs hold similar views on the “natureand definition” of the patient, they will necessarily agree on the treatmentgoals, treatment approach, and so on. They do suggest, however, that suchsimilarity is conducive to collaboration.
The comparison of SWs’ and PCPs’ poverty perceptions presentedin this article is based on a qualitative study querying the interviewees’perceptions of the clients and patients whom they believe to be poor.“Poverty perceptions” in this study refer to the composite of attributions for
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ambr
idge
] at
11:
18 0
8 O
ctob
er 2
014

Poverty Perceptions of Social Workers and Physicians in Israel 965
poverty and perspectives on persons who are poor. “Attributions” refers toexplicit causal beliefs about poor persons. “Perspectives” includes attitudes(e.g., favorable or unfavorable evaluation of poor persons) and affective(e.g., feelings or other emotional responses) and cognitive components(Cozzarelli et al., 2001; Cozzarelli, Tagler, & Wilkinson, 2002).
In its broad outlines the current study follows previous studies thathave identified three main attributions for poverty: individual, structural, andfatalistic. Individual attribution holds that poverty is caused by the person’sown behaviors (e.g., lack of effort, laziness). Structural attribution holds thatpoverty is caused by forces external to the individual (e.g., discrimination,low wages, deprivation due to class, race, or ethnicity). Fatalistic attributionholds that poverty is caused by inherent or otherwise unavoidable propertiesof the individual (e.g., lack of ability, disability, illness) (Bullock, FraserWyche, & Williams, 2001; Cozzarelli et al., 2001).
Numerous studies have been carried out on the poverty perceptions ofsocial workers and social work students in a wide variety of countries. Alongwith variations both within and between countries, most of the studies foundthat their subjects tended to attribute poverty more to social and structuralfactors than to individual ones (e.g.„ Rehner, Ishee, Salloum, & Velasques,1997; Sun, 2001; Weiss Gal et al., 2009). Much sparser research on physicians’and medical students’ poverty perceptions tends to show, in contrast, thateven though these professionals are aware of the social and structural factorsthat contribute to poverty, they are more prone to attribute poverty to causeswithin the individual’s control, such as lack of effort (Wear, Aultman, Varley& Zarconi, 2006; Willems et al., 2005).
The present study goes beyond the previous research by comparing thepoverty perceptions of SWs and PCPs. To the knowledge of the author, nosuch comparison has been published to date. Only one study of povertyperceptions includes both social workers and physicians; but in it physi-cians are included with other professionals and their responses not analyzedseparately (Weiss and Gal, 2007).
The study differs from most previous studies of poverty perceptions,which inquire about poor persons in general, in that it taps the intervie-wees’ perceptions of the clients they serve whom they believe to be poor.This approach was chosen both because it frees the researcher from the needto define poverty by some external standard (e.g., absolute poverty, incomepoverty, relative poverty), which is not relevant to a study of perceptions,and because perceptions of specific persons are likely to be better predic-tors of behavior than perceptions of abstract poor persons. According tothe theory of planned behavior, the more specific the behaviors and behav-ioral intentions that are queried, the greater the predictive power of theattitudes expressed (e.g., Ajzen, 1991, 2002; Armitage and Conner, 2001).The supposition is that perceptions regarding specific persons are morelikely to reflect the real feelings and beliefs of those questioned on whether
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ambr
idge
] at
11:
18 0
8 O
ctob
er 2
014

966 M. Monnickendam
and how the poverty of their patients or clients can be alleviated, than whenrelating to poor persons in the abstract.
METHOD
Setting
Israel is a multifaceted society of about seven million inhabitants, char-acterized by overlapping and intersecting cultural and socioeconomicdimensions. About 20% of its citizens are non-Jews (largely Arab Muslimsand Christians), 5–6% ultra-orthodox Jews, 15% Jewish immigrants from theformer Soviet Union. There are also about 70,000 Ethiopian Jews who immi-grated to Israel over the last 20 years (CBS, 2010). The issue of povertysurfaced during the winter of 2003/2004, when Israel was at the peak ofa severe economic crisis, accompanied by a real cut in social expenditure,dramatically increased unemployment (10.7% in 2003) and poverty in theweakest population groups (Achdut, Cohen, & Endweld, 2005). The reces-sion led to high unemployment of well educated, highly skilled IT workerswho, upon exhausting their means were labeled “new poor” (Latet, 2006).During that period child support was slashed sharply to induce parents oflarge families to join the labor market.
Israel has a large, centralized, mainly government-funded welfare sys-tem. By law, council social services (CSS), funded by the Ministry of Welfareand run in accord with government directives, operate in every municipal-ity. They provide a wide-range of in-kind assistance and services, includingchild and family services, services to the aged, personal counseling, referralservices, and others. The directors of the CSSs are all ACSWs.
Under Israel’s national health care system, most primary health careis delivered through health maintenance organization (HMO)–operatedcommunity health clinics (CHC), which provide universal health care, irre-spective of age, ethnicity, socioeconomic status, or religion, at nominal rates.Between 1997 and 2004 the proportion of out-of-pocket health expendituresrelative to the total per person health expenditure increased from 24% to30%, with the largest increase found in the two lowest income deciles (Kop,2005). In Israel collaboration between SWs and PCPs is strongly supportedby the HMOs and the Ministry of Welfare, but as in practice there is noadministrative framework for such collaboration, in practice it occurs largelyon an ad hoc basis, if at all.
Participants
The study participants are a purposive sample of SWs who are directors ofCSSs and of administrative physicians and PCPs who work in the CHCs of oneof the country’s largest HMOs. To reflect the socioeconomic and multi-culturaldiversity of Israeli society, the study included CSSs representing all ten clusters
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ambr
idge
] at
11:
18 0
8 O
ctob
er 2
014

Poverty Perceptions of Social Workers and Physicians in Israel 967
on the local authorities’ socioeconomic index. This also ensured that the PCPsand SWs dealt with and referred to the same client populations, albeit notnecessarily the same clients. Because PCPs working in CHCs in the top threeclusters declined to participate, the CHCs in the study represent the lowestseven clusters (CBS, 2010). Within the clusters, CSSs and CHCs were selectedto represent chronic poor, new poor, Muslim and Christian poor, the ultra-orthodox, and Ethiopian and former Soviet-Union immigrants. Of the 26 SWsand 37 PCPs approached, 17 SWs and 16 PCPs agreed to participate. Non-participation was uniformly explained by lack of time. Of the participatingSWs, 4 had a BSW and 13 a MSW. Fifteen were female, two male. Their agesranged from 41 to 66. The PCPs were nine females and six males, rangingin age between 35 and 66.
Procedure
A two-stage phenomenological approach was adopted. At the start of both,the participants were informed that the study concerns only clients orpatients whom they themselves served and regarded as poor. In the firststage, two focus groups were conducted: one for the SWs, with 11 par-ticipants, one for the PCPs, with 9 participants. The focus groups wereconducted separately because, in view of the generally unequal power rela-tions between SWs and PCPs (Hudson, 2002), it was believed that the SWswould feel freer to express themselves without the presence of PCPs. Bothgroups were conducted by the author and a colleague, using a focus groupconvener’s manual prepared for the study, which listed the themes to becovered. These were the participants’ attributions for poverty, their attitudestowards the clients or patients they regarded as poor, the affects they dis-played when talking about them, and their beliefs about how their povertymight be alleviated. Each focus group lasted about three hours.
Originally, all the study participants were invited to take part in thefocus groups. The second stage was planned on the presumption that somestudy participants could not attend owing to scheduling difficulties. In thisstage, in-depth interviews were held with the remaining six SWs and sevenPCPs. The interviews were conducted in the participants’ offices, using aninterviewer handbook consisting of questions on both the listed and newthemes raised in the focus group (Krueger, 1994). The interviews, by expe-rienced and trained MSWs, lasted between one and two hours. The focusgroups and interviews were audio recorded, transcribed, and then brokendown into units of meaning (Patton, 2002).
Analyses
The units of meaning were coded and classified within themes and sub-themes. Open coding was used to classify statements within new themes andsub themes dynamically created in the course of content analysis (Denzin
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ambr
idge
] at
11:
18 0
8 O
ctob
er 2
014

968 M. Monnickendam
and Lincoln, 1994). The relationships between the themes were analyzedand conceptualized by axial coding, then collapsed into main and secondaryconstructs (Strauss and Corbin, 1998). Initial coding and classification wascarried out independently by two MSWs with experience in the social serviceand medical systems. In cases of divergence, the final classification wasdetermined in consultation with the author.
FINDINGS
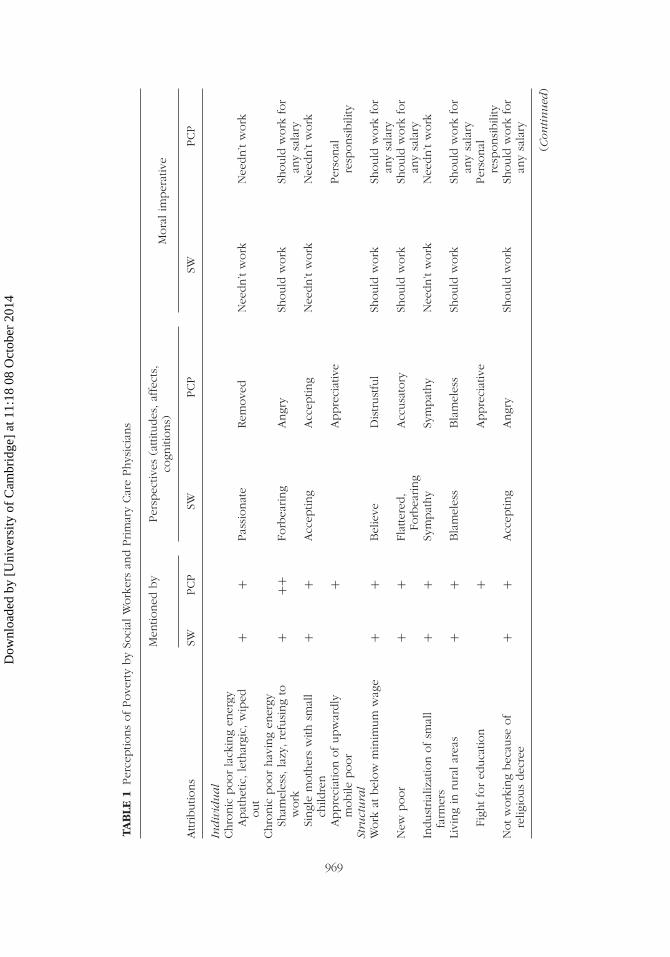
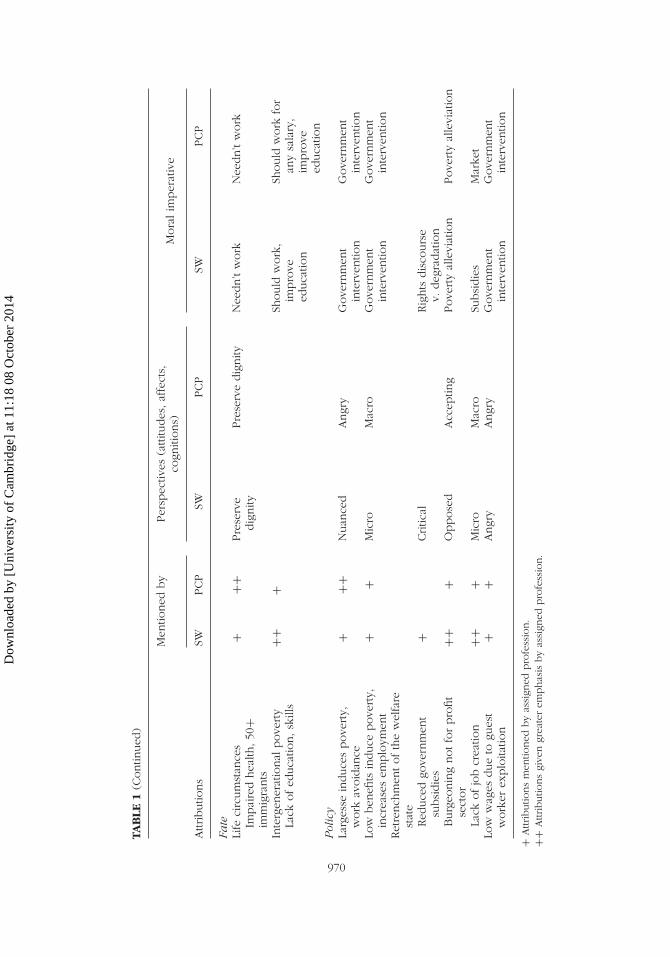
Four main attributions for poverty emerged from the focus groups and per-sonal interviews: individualistic, structural, fate, and policy. Each attributionis presented in a separate section. Each section also compares the emphasis(e.g., frequency of mention) the SWs and PCPs gave to the attribution, theirperspectives (e.g., their attitudes toward and cognitions about the personsor policy they spoke of and the affects they displayed toward them), andtheir “moral imperatives,” defined as their beliefs about how their clientsor the government should act to alleviate their poverty. The findings aresummarized in Table 1.
Individual
The individual attributions for poverty essentially viewed it as merited bythe person’s behavior. Both SWs and PCPs tended to refer to those whosepoverty they considered merited either as chronic poor lacking energy or aschronic poor having energy. As they presented it, neither type did anythingto alleviate their poverty, either because they lacked the energy or will orbecause they misused or misdirected the energy they had.
Both SWs and PCPs described those they viewed as lacking in energyas “apathetic” and “lethargic” individuals who accepted their poverty and feltno need to change it. Neither suggested that they should go out and findemployment; both implied that they regarded their situation as irremediableand that there was no point in trying to do anything about it. The maindifference between the SWs and PCPs with regard to this poor was theiraffect. The SWs conveyed distress and even despair that was absent from thePCPs statements. Many of the SWs described these poor as “wiped out”—aterm whose original Hebrew connotes utter helplessness and despair—andsome added despairingly themselves: “even if we offer help, they don’trespond.”
Both SWs and PCPs described the poor persons they viewed as hav-ing energy as “active” persons who “do things,” but who preferred gettingincome support to working. Both criticized them as “lazy” and “shameless”and spoke disapprovingly of the energetic able bodied poor who refused totake low paying menial jobs “that only foreign workers will do.” With this,
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ambr
idge
] at
11:
18 0
8 O
ctob
er 2
014
TAB
LE1
Per
ceptio
ns
ofPove
rty
by
Soci
alW
ork
ers
and
Prim
ary
Car
ePhys
icia
ns
Men
tioned
by
Per
spec
tives
(attitu
des
,af
fect
s,co
gniti
ons)
Mora
lim
per
ativ
e
Attributio
ns
SWPCP
SWPCP
SWPCP
Ind
ivid
ua
lChro
nic
poor
lack
ing
ener
gyA
pat
het
ic,le
thar
gic,
wip
edout
++
Pas
sionat
eRem
ove
dN
eedn’t
work
Nee
dn’t
work
Chro
nic
poor
hav
ing
ener
gySh
amel
ess,
lazy
,re
fusi
ng
tow
ork
+++
Forb
earing
Angr
ySh
ould
work
Should
work
for
any
sala
rySi
ngl
em
oth
ers
with
smal
lch
ildre
n+
+A
ccep
ting
Acc
eptin
gN
eedn’t
work
Nee
dn’t
work
Appre
ciat
ion
ofupw
ardly
mobile
poor
+A
ppre
ciat
ive
Per
sonal
resp
onsi
bili
tySt
ruct
ura
lW
ork
atbel
ow
min
imum
wag
e+
+B
elie
veD
istrust
ful
Should
work
Should
work
for
any
sala
ryN
ewpoor
++
Flat
tere
d,
Forb
earing
Acc
usa
tory
Should
work
Should
work
for
any
sala
ryIn
dust
rial
izat
ion
ofsm
all
farm
ers
++
Sym
pat
hy
Sym
pat
hy
Nee
dn’t
work
Nee
dn’t
work
Livi
ng
inru
ralar
eas
++
Bla
mel
ess
Bla
mel
ess
Should
work
Should
work
for
any
sala
ryFi
ghtfo
red
uca
tion
+A
ppre
ciat
ive
Per
sonal
resp
onsi
bili
tyN
otw
ork
ing
bec
ause
of
relig
ious
dec
ree
++
Acc
eptin
gA
ngr
ySh
ould
work
Should
work
for
any
sala
ry
(Con
tin
ued
)
969
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ambr
idge
] at
11:
18 0
8 O
ctob
er 2
014
TAB
LE1
(Contin
ued
)
Men
tioned
by
Per
spec
tives
(attitu
des
,af
fect
s,co
gniti
ons)
Mora
lim
per
ativ
e
Attributio
ns
SWPCP
SWPCP
SWPCP
Fate
Life
circ
um
stan
ces
Impai
red
hea
lth,50
+im
mig
rants
+++
Pre
serv
edig
nity
Pre
serv
edig
nity
Nee
dn’t
work
Nee
dn’t
work
Inte
rgen
erat
ional
pove
rty
Lack
ofed
uca
tion,sk
ills
+++
Should
work
,im
pro
veed
uca
tion
Should
work
for
any
sala
ry,
impro
veed
uca
tion
Pol
icy
Larg
esse
induce
spove
rty,
work
avoid
ance
+++
Nuan
ced
Angr
yG
ove
rnm
ent
inte
rven
tion
Gove
rnm
ent
inte
rven
tion
Low
ben
efits
induce
pove
rty,
incr
ease
sem
plo
ymen
t+
+M
icro
Mac
roG
ove
rnm
ent
inte
rven
tion
Gove
rnm
ent
inte
rven
tion
Ret
rench
men
tofth
ew
elfa
rest
ate
Red
uce
dgo
vern
men
tsu
bsi
die
s+
Critic
alRig
hts
dis
cours
ev.
deg
radat
ion
Burg
eonin
gnotfo
rpro
fit
sect
or
+++
Oppose
dA
ccep
ting
Pove
rty
alle
viat
ion
Pove
rty
alle
viat
ion
Lack
ofjo
bcr
eatio
n++
+M
icro
Mac
roSu
bsi
die
sM
arke
tLo
ww
ages
due
togu
est
work
erex
plo
itatio
n+
+A
ngr
yA
ngr
yG
ove
rnm
ent
inte
rven
tion
Gove
rnm
ent
inte
rven
tion
+A
ttributio
ns
men
tioned
by
assi
gned
pro
fess
ion.
++A
ttributio
ns
give
ngr
eate
rem
phas
isby
assi
gned
pro
fess
ion.
970
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ambr
idge
] at
11:
18 0
8 O
ctob
er 2
014
Poverty Perceptions of Social Workers and Physicians in Israel 971
both made exceptions for single mothers with small children and statedthat it was better that they receive income support than go out to workso that they can be with their children. The PCPs, however, were muchmore critical of the energetic poor than the SWs. They were more proneto declare that people who could work should, at whatever wage, evenless than the legal minimum, and much prone to express anger at the easewith which persons can get income support (e.g., “anyone can sign up”).Quite a number of the PCPs stated angrily that many of the energetic poorcheated and abused the system. As one PCP remarked, “they say that theirback hurts, no physician can dispute that. They live at the public expense.They’re modern-day beggars.” No one in the focus group where he madethis statement disputed him. SWs, in contrast, tended to share the view oftheir energetic poor clients that there was no point in working for sub-subsistence wages and to point out that such wages “kill” the motivationto work and cause many poor persons “to give up.” When asked whetherthey condoned a poor person’s refusing work that paid less than minimumwage, they replied in the negative; nonetheless, unlike the PCPs. they wouldnot come out and say that persons who needed money should work forwhatever wages they could get.
Yet another difference was that the PCPs, but not the SWs, pointed outthat there were some energetic poor who managed to extricate themselvesfrom their poverty. In particular, they spoke of immigrants from Ethiopia andthe former Soviet Union who attended university. One PCP said: “althoughit may take them longer, they have the will to succeed and become elec-trical engineers, clinical social workers, and to advance themselves.” Theirstatements about these immigrants contain a mixture of admiration for theirtenacity and will and severe criticism of all those able and energetic poorwho do not act with similar determination to improve their lot.
Structural
Both the PCPs and SWs attributed structural causes to the poverty of fivegroups of persons:
1. Persons who worked at jobs that paid below minimum wage. There wereboth PCPs and SWs who noted that some of the persons who are pooractually worked, but earned so little that they remained poor. With this,quite a few of the PCPs seemed to doubt that the earnings of the workingpoor were as low as they said. Distant and mistrustful, they qualified theirstatements about the earnings of these poor with the words “they say.”No SW used this qualifier. The PCPs and SWs also differed in their moralimperatives for these poor. Most of the PCPs stated that they should workeven if doing so does not lift them out of poverty. Most of the SWs stated,more sympathetically, that even though in principle everyone should
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ambr
idge
] at
11:
18 0
8 O
ctob
er 2
014

972 M. Monnickendam
work, there is no point in laboring at jobs that pay below minimumwage.
2. High tech workers who lost their jobs when the IT bubble burst. BothPCPs and SWs distinguished them from most of the other poor, empha-sizing their high level of skill and education, and labeling them as “newpoor.” Their attitudes toward them were quite different, however. The PCstended to blame them for what they saw as their “consumerism,” “livingabove their means,” and failure to plan for their layoffs, which, some PCPsmaintained, should have been anticipated. Making no allowances for thenewness of their poverty or for their social status, they expected them towork at whatever jobs they could find. Most of the SWs, in contrast, weresympathetic and reluctant to “break” them—as they saw it—by requiringthem to work at menial, low paying jobs. In the words of one SW, “whenthey [high tech workers] are laid off, they really fall hard.” Furthermore,quite a few of the SWs seem to have viewed them as occupying a higherstatus than themselves and to be both uneasy and flattered by havingthem as clients: “These are people I never imagined would be poor, andnow they come and ask for my help.”
3. Arab farmers, 50 years old and over, who had lost their small farms asa result of the industrialization of agriculture and had no marketableskills. These farmers were mentioned only by the Arab interviewees.Both the PCPs and SWs among them viewed these farmers sympathet-ically. Both saw them as elderly, exhausted men, without the resources(e.g., education, energy) needed to enter the labor market. Both said itwas inappropriate to demand that they find alterative employment.
4. Persons living in economically deprived communities in the peripheryof the country. These are outlying communities where services (e.g.,schools, health care) are notoriously poor. Both PCPs and SWs attributedthe poverty of this group to economic conditions in these communities.They reported that many small businesses go bankrupt and that jobs arelower paying and unemployment rates substantially higher than in thecenter. Both PCPs and SWs expressed the view that for some subgroupsin these communities (the ultra-orthodox, immigrants from Ethiopia andparts of the former Soviet Union), who had the additional disadvantageof lacking appropriate work skills, poverty was almost inescapable. Thesepersons, they stated, were not to be blamed for their poverty. With this,the PCPs’ and SWs’ attitudes were not identical. Once again, some PCPsdeclared emphatically that these objective difficulties do not free personsof responsibility and that the persons who are poor in these communi-ties should go out and work for any salary. Once again they expressedadmiration for those who made determined efforts to break the cycle ofpoverty, pointing to parents who refused to compromise on educationand sent their children to (highly subsidized) boarding schools outside ofthe community: As one PCP put it: “They get ahead, and became pilots
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ambr
idge
] at
11:
18 0
8 O
ctob
er 2
014
Poverty Perceptions of Social Workers and Physicians in Israel 973
[a very high status profession in Israel] and lawyers.” SWs, in contrast,were less critical, but said nothing about parents’ efforts to extricate theirchildren from poverty.
5. The ultra-orthodox, a community of highly observant Jews, who valuereligious study above work. Both PCPs and SWs viewed the poverty ofthe ultra-orthodox as chosen by an empowered population for whom notworking is normative. However, once again, while the SWs tended tobe accepting, the PCPs expressed anger. In their view, the non-workingultra-orthodox “exploited the public by using their religiosity to receivegovernment subsidies and stipends.” Nonetheless, they explicitly rejecteddiscontinuing the assistance, because “according to the Jewish religion,people must give and help.”
Fate
Both SWs and PCPs identified the same three groups of persons or groupswhose poverty they attributed to personal features over which the individualhad no control. The most obvious were persons with physical or mentaldisabilities or poor health. The PCPs talked about these poor more thanthe SWs, but neither talked about them very much, nor judged them, oreven raised the idea that they should—or could—do anything to changetheir situation.
The most talked about group consisted of 50+-year-old immigrantsfrom Ethiopia and the former Soviet Union who, as both SWs and PCPsexplained, arrived in Israel with no marketable skills and, through no faultof their own, could not acquire any. In the words of a PCP: “They are tooold to learn the language, the jobs [in Israel] are different [from those inEthiopia or the former USSR], they don’t understand the culture of the work-place, they get fired, and then they work for a pittance, and in the end theyremain poor.” Virtually all the PCPs and SWs condoned these immigrantsnot working. Both opposed telling them to look for low paying menial jobs,even if they might be able to get them. Both stated that it was their dutyas professionals to refrain from further undermining their dignity and self-respect by pressuring them to work. Both believed that the welfare systemcan and should absorb the cost of providing them with income support.As one SW put it: “What do you want from them? Nothing will happen ifthey don’t work.”
The third group consisted of the second- and third-generation poor.The SWs were more prone than the PCPs to speak of these poor, as well asmore prone to attribute their poverty specifically to the limited education andlack of occupational skills that, to the minds of the SWs, both resulted frompoverty and caused its perpetuation from generation to generation. With this,the PCPs no less than the SWs viewed second- and third-generation poor asvictims of forces over which they had no control. As one interviewee put it,
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ambr
idge
] at
11:
18 0
8 O
ctob
er 2
014

974 M. Monnickendam
“this is what the children saw, imitated and learned.” Moreover, despite theirattribution of intergenerational poverty to fate, the PCPs and SWs appliedto these poor the moral imperative that they make efforts to improve theirskills and education. However, only the PCPs required them to accept anyand all work they were offered.
Policy
Participants referred to four types of government policies that they believedcontributed to poverty by encouraging counterproductive behaviors.
1. Government largesse. Both PCPs and SWs stated that governmentlargesse, in the form of income support and additional benefits for specificpopulations, contributes to poverty by creating incentives not to work.The PCPs, however, expressed considerably more frustration and angerat the situation. For example, a PCP stated: “In the past, single mothersworked, but no longer. They learned that the state supports them, andthis allows them to breed [sic] too many children and live off the state.”On the other hand, a SW speaking of the benefits received by unskilledformer Soviet Union (FSU) and Ethiopian immigrants expressed a morenuanced critique: “These were normative working people in their culture,but out of concern for the difficulties they would encounter acculturatingto Israel society, the government provided them with many kinds of assis-tance. This enabled them to get by without working when they arrived,but it also taught them to be poor.” Other social workers noted that thereceipt of income support entitles persons to many other benefits (forexample, exemption from municipal taxes, almost free medical services,subsidized bus tickets, school fees), whose total monetary value is oftenhigher than the earning capacity of many unskilled single mothers andimmigrants.
2. Low benefits for those who needed assistance. Here, the participants’ atti-tudes varied with the group in question. Both PCPs and SWs criticized thelow level of income support for single elderly persons and for immigrantsclose to retirement age, stating that these persons deserved state benefitsand should receive sufficient income support to enable them to live indignity. With this, both expressed ambivalence regarding low benefits forlarge families. They agreed that the generous child support of the past hadinduced work avoidance and that it was rightly reduced.1 The followingobservation by an SW was made by PCPs as well: “The fact is, peoplestarted doing something, they had no choice.” But they also criticized thesuddenness and severity of the cuts, noting that families with many smallchildren suddenly lost up to 50% of their income with no time to adaptto the change.
At the same time, the SWs and PCPs spoke from different perspec-tives and expressed different concerns. The PCPs generally adopted a
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ambr
idge
] at
11:
18 0
8 O
ctob
er 2
014

Poverty Perceptions of Social Workers and Physicians in Israel 975
macro perspective, stressing the need to solve “child poverty”—that is,of the need for policy solutions to a social problem. The SWs adopted amicro perspective, emphasizing the need to solve the problems of “poorchildren in poor families” through professional intervention.
3. Retrenchment of the welfare state. The participants criticized three aspectsof the retrenchment of the welfare state: the reduction of the once amplegovernment subsidies for basic goods and services (from bread and milkthrough transportation and higher education), the resultant burgeoning ofthe not for profit sector to fill the shortfall, and the lack of proactive jobcreation.
Only the social workers referred to the reduction of governmentsubsidies for goods and services. As a rule they regarded the universalsubsidies provided to all residents through the end of the 1980s and 1990sas basic social entitlements and viewed their sharp reduction or elimina-tion as having forced poor persons to degrade themselves by asking forhandouts. As one SW put it: “now one is forced to degrade oneself andto beg for every little thing—food, clothing, reductions on school booksand class trips, medicines, and local taxes.”
Both SWs and PCPs were critical of the not-for-profit sector. Bothmaintained that this sector should restrict its activities to providing ser-vices that could alleviate poverty; both gave vocational training as anexample of such services; and both objected vehemently to the provi-sion of food by this sector, which they believed perpetuated poverty.The SWs’ criticisms, however, were more global and emphatic than thePCPs’ who tended to accept the existence of the sector and objectedonly to the direction it chose. The SWs maintained that by stepping intothe void in the funding and provision of essential goods and servicesleft by the retrenchment of the welfare state, the not for profit sectorwas enabling the government to assuage its conscience and pawn off itsresponsibilities.
Lack of job creation: Both the PCPs and the SWs placed the respon-sibility for alleviating poverty on the government and criticized it for notdoing enough to create jobs. Both stated that the government shouldprovide subsidies for small businesses and for factories that employedlow- or non-skilled workers. However, the PCPs expressed reservationsthat the social workers did not. They pointed out that subsidies createtheir own economic distortions and that a balance is needed betweenIsrael’s former socialist ideology and the now prevailing neo-liberalism.For example one PCP stated: “The Bolsheviks provide work, the capital-ists let the market create work. Israel has to find the balance betweenthese approaches.”
4. Exploitation of guest workers. Both SWs and PCPs observed that guestworkers and non-skilled Israelis compete for the same jobs, and bothattributed the below minimum wage salaries often paid to unskilled
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ambr
idge
] at
11:
18 0
8 O
ctob
er 2
014

976 M. Monnickendam
Israelis to the sub-subsistence salaries paid to guest workers. Both empha-sized that such salaries cause many working families who are “basicallyfunctional, good and warm” to slide into a viscous and expanding circleof debt, electricity cutoffs, and sometimes even jail for debt default. Bothcriticized the government for its deliberate non-intervention to stop theexploitation.
DISCUSSION
The study found both similarities and differences in the professionals’poverty perceptions. Both SWs and PCPs attributed poverty to all fourcauses—individual, structural, fate, and policy—and to most of the samesub-causes. These findings raise questions about previous findings that socialworkers tend to make structural attributions for poverty, while physiciansmake individualistic ones (Weiss-Gal et al., 2009; Wear et al., 2006). A pos-sible explanation for the difference between previous findings may be thatthe present study focused on the participants’ own clients, not on povertyor poor persons in general, thereby encouraging more varied attributionsbased on personal experience rather than stereotypes.
The SWs and PCPs were also similar in some of their perspectives andmoral imperatives. Both were critical of the chronic poor lacking in energyand reached the conclusion that it was pointless to try to get them to work.Both were accepting of non-working single mothers and sympathetic towardpoor farmers put out of work by industrialization. Both believed it impor-tant to preserve the dignity of those who were poor because of ill healthor immigration, both viewed their not working as moral, and both wereangered by the exploitation of guest workers.
The differences were of several kinds. One set of differences seemsto be anchored in their daily work within their professions. The greateremphasis the PCPs placed on the impaired health of their clients and thatthe SWs placed on intergenerational poverty, the burgeoning not-for-profitsector, and the lack of job creation can all be explained by the situationsthey encounter in their work. It is also understandable that none of thePCPs pointed to reduced government subsidies as a cause of poverty, sincethey are probably unfamiliar with this aspect of service delivery.
The other set of differences seems to be more substantive. The PCPstended to be more angry, distrustful, and accusatory of their poor clientsthan the SWs. They were angry about those they perceived as lazy andrefusing to work, whereas SWs tended to be forbearing. They were angryat those who did not work because of religious decree, whereas SWs wereaccepting. They were angrier than SWs at what they believed to be harmfulgovernment largesse. Moreover, whereas SWs believed clients who reportedthat they were paid less than minimum wage, PCPs were skeptical of this
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ambr
idge
] at
11:
18 0
8 O
ctob
er 2
014

Poverty Perceptions of Social Workers and Physicians in Israel 977
claim. Whereas SWs believed that those who were in a position to workshould, PCPs went further to state that they should work at any salary theywere offered. These differences may stem from the especially strong empha-sis in social work education and socialization on the values of acceptance,tolerance, and non-judgmentalism (Dominelli, 2004, p. 66).
Moreover, only the PCPs expressed admiration for the upwardly mobilepoor and for those rural poor who struggled to provide their children withthe best possible education. Along with their greater anger, this admirationimplies that the PCPs believe that at least some of their patients can domore to pull themselves out of their poverty. While this is a critical andjudgmental view, it is also, at heart, an optimistic one, which credits patientswith the ability to find work and make a better future for themselves andtheir children. The SWs, in contrast, focused almost solely on their clients’hardships and weaknesses and conveyed little expectation or hope that theywould overcome their poverty.
On policy issues, the PCPs and SWs did not so much disagree as viewthe policies from a different angle. By and large PCPs looked at the macro,the systemic, the normative, the position of the poor relative to the generalpopulation, and at ideological aspects of the retrenchment of the welfarestate (Narhi, 2002). SWs focused on the micro, the practical, the situationof “their” poor clients relative to other poor persons, and the utilitarianaspects of the retrenchment of the welfare state. It seems that the SWs whoparticipated in this study represent the “first psycho, then social” orientationtype identified by Buchbinder, Eisikovits, and Karnieli-Miller (2004). SWs ofthis type tend to be distant from larger social forces, focus predominantlyon intrapsychic etiological explanations of client problems, marginalize thesocial aspects of the problems, and justify their limited belief in change byobjective impediments. The PCPs participating in this study, who clearlyconsidered the larger social forces, focused more on the medical than thesocial aspects of their patients’ problems.
The study has a number of limitations. As a qualitative examination, itemployed a small, purposive sample and further study must be undertakento ensure that the findings are not colored by individual differences betweenthe members of the two groups. Moreover, given that collaboration betweenSWs and PCPs is not institutionalized, it cannot be assumed that they haveprior experience with interagency collaboration. It cannot be ruled out thatthe fact that the author led the focus groups may have subtly influencedthe discussions to confirm his assumptions. Nor can it be ruled out that theauthor’s determination of the final classification in cases of divergence andhis prior knowledge of the common classification of poverty perceptions didnot influence the analysis. Further limitations concern both the impossibilityof generalizing from phenomenological studies and the fact that perceptionsare not unrelated to culture and local conditions. Thus care must be takenwhen considering the applicability of the findings outside of Israel.
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ambr
idge
] at
11:
18 0
8 O
ctob
er 2
014

978 M. Monnickendam
Nevertheless, the study is the first comparison of the poverty percep-tions of SWs and PCPs. Broader and deeper than most previous studies ofthe poverty perceptions of either group, it provides a rich and nuanced pic-ture of their causal attributions, perspectives, and moral imperatives. It alsoreveals two sets of findings not previously noted in the literature, whichhave both theoretical and practical implications.
One set of findings is that, on the whole, while the PCPs and SWsshared a similar view of the causes of poverty, they differed in many oftheir perspectives and moral imperatives. The questions of whether theiragreement provides sufficient grounds for fruitful collaboration on sharedpatients/clients and whether their differences can be sufficiently bridged orworked out to enable such collaboration are beyond the scope of this study.
However, these findings raise questions about the widely assumedassociation in the literature between persons’ perceptions of the causes ofpoverty and the remedies they would propose. The study participants spokeextensively of what they thought should be done to alleviate the povertyof their clients/ patients, whether by the persons themselves or by the gov-ernment. I have termed this their “moral imperative” because of the strongemotional and value components they brought to bear. From the standpointof theory, the disconnect between the participants’ causal perceptions andtheir perspectives and moral imperatives implies that the study of povertyperceptions as a determinant of action should incorporate additional vari-ables such as respondents’ background features. From a practical standpoint,they suggest that it might be more fruitful to keep inter-professional discus-sions pragmatic and focused on solving the problem at hand rather thantheoretical and principled.
The other new set of findings concerns policy. Policy in this studyemerged as a causal attribution for poverty, in addition to individual andstructural factors and fate. This finding means that both social workers andprimary care physicians recognize the role of policy in both the deepeningand alleviation of poverty. Moreover, the findings in the policy categorysuggest that the members of both professions have given thought to and caredeeply about the policies that affect their clients/patients. These findingssuggest that it is worth soliciting the opinions of both SWs and PCPs onrelevant policy matters and encouraging them to become involved, whetherseparately or in cooperation, in policy practice efforts.
NOTE
1. Income tax reductions for dependants are very low in Israel. To make up for this, for manyyears the government provided child allowances, which increased in accord with the number of childrenin the family. The problem with the allowances, as many saw it, was that for every additional child, theper child allowance was larger than for the previous child. This, the critics claimed, encouraged largefamilies.
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ambr
idge
] at
11:
18 0
8 O
ctob
er 2
014

Poverty Perceptions of Social Workers and Physicians in Israel 979
REFERENCES
Achdut, L., Cohen, R., & Endweld, M. (2005). Trends of development in poverty,in L. Achdut (ed.), Annual Review—2004 (pp. E63–E74). Jerusalem, Israel: TheNational Insurance Institute of Israel.
Ajzen, I. (1991). The theory of planned behavior. Organizational Behavior andHuman Decision Processes, 50, 179–211.
Ajzen, I. (2002). Constructing a TpB Questionnaire: Conceptual and method-ological considerations, Working Paper, University of Massachusetts, Amherst,September 2002. Retrieved from http://www.people.umass.edu/aizen/pdf/tpb.measurement.pdf
Armitage, C.J., & Conner M. (2001). Efficacy of the theory of planned behaviour: Ameta-analytic review. British Journal of Social Psychology, 40, 471–499.
Benson, D.S. (2000). Providing health care to human beings trapped in the povertyculture—Reconciling the inner self with the business of health care. PhysicianExecutive, 26 , 28–32.
Buchbinder, E., Eisikovits, Z., & Karnieli-Miller, O. (2004). Social workers’ percep-tions of the balance between the psychological and the social. Social ServiceReview, 78, 531–552.
Bullock, H.E., Fraser Wyche, K., & Williams,W.R. (2001). Media images of the poor.Journal of Social Issues, 57 , 229–246.
Carpenter, J., & Hewstone, M. (1996). Shared learning for doctors and socialworkers: Evaluation of a programme. British Journal of Social Work, 26 ,239–257.
CBS (Central Bureau of Statistics). (2010). Retrieved from http://www.cbs.gov.il/www/population/profil.pdf
Cozzarelli, C., Wilkinson, A.V., & Tagler, M.J. (2001). Attitudes toward the poor andattributions for poverty. Journal of Social Issues, 57 , 207–227.
Cozzarelli, C., Tagler, M.J., & Wilkinson, A.V. (2002). Do middle-class studentsperceive poor women and poor men differently? Sex Roles, 47 , 519–529.
Denzin, N.K., & Lincoln, Y.S. (1994). Handbook of Qualitative Research. ThousandOaks, CA: Sage.
De Swaan, A., Manor, J., Quyen, E., & Reis, P.E. (2000). Elite perceptions of the poor:Reflections for a comparative research project. Current Sociology, 48(1), 43–54.
Dominelli, L. (2004). Social Work: Theory and Practice for a Changing Profession.Cambridge, UK: Polity Press.
Dowling, M. (1999). Social Work and Poverty. Attitudes and Actions. Aldershot, UK:Ashgate.
Green, R. (2000). Applying a community needs profiling approach to tackling serviceuser poverty. British Journal of Social Work, 30, 287–303.
Hudson, B. (2002). Interprofessionality in health and social care: The Achilles’ heelof partnership? Journal of Interprofessional Care, 16 , 7–17.
Kop, Y. (2005). The 2005 Annual Report on Israel’s Social Services. Jerusalem, Israel:Taub Center for Social Policy Studies in Israel.
Krueger, R.A. (1994). Focus Groups. (2nd ed.) London, UK: Sage.Krumer-Nevo, M., Weiss, I., & Monnickendam, M. (2009). Poverty aware social work
practice: A conceptual framework for social work education. Journal of SocialWork Education. 45, 225–243.
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ambr
idge
] at
11:
18 0
8 O
ctob
er 2
014

980 M. Monnickendam
Latet. (2006). Poverty Trends among Food Distribution Associations. Latet,Israel Humanitarian Aid. Retrieved from http://www.latet.org.il/evia/oni2004/report2.pdf
Monnickendam, M., Katz. C., & Monnickendam, M.S. (2010). Social workers servingpoor clients: Perceptions of poverty and service policy. British Journal of SocialWork, 40, 911–927.
Monnickendam, M., Monnickendam, M.S., Katz, C., & Katan, J. (2007). Health carefor the poor: An exploration of primary-care physicians’ perceptions of poorpatients and of their service policy. Social Science & Medicine, 64, 1463–1474.
Patton, M.Q. (2002). Qualitative Research & Evaluation Methods. Thousand Oaks,CA: Sage.
Narhi, K. (2002). Social workers conceptions of how the local living environment isrelated to social exclusion. European Journal of Social Work, 5, 255–267.
Rehner, T., Ishee, J., Salloum, M., & Velasques, D. (1997). Mississippi social workers’attitudes toward poverty and the poor. Journal of Social Work Education, 33,131–142.
Russel, L.D. (2006). Revolutionizing the training of clinicians for the poor andunderserved. Journal of Health Care for the Poor and Underserved, 17 , 6–11.
Sandfort, J.R., Kalil, A., & Gottschalk, J.A. (1999). The mirror has two faces. Welfareclients and front-line workers view policy reforms. Journal of Poverty, 3(3),71–91.
Strauss, A., & Corbin, J.M. (1998). Basics of Qualitative Research: Techniques andProcedures for Developing Grounded Theory (2nd ed.). Thousand Oaks, CA:Sage.
Strier, R. (2008). Client and worker perceptions of poverty: Implications for practiceand research. Families in Society, 89(3), 14–24.
Sun, A.P. (2001). Perceptions among social work and non-social work studentsconcerning causes of poverty. Journal of Social Work Education, 37 , 161–173.
Wear, D., Aultman, J.M., Varley, J., & Zarconi, J. (2006). Making fun of patients:Medical students’ perceptions and use of derogatory and cynical humor inclinical settings. Academic Medicine, 81, 454–462.
Weiss, I., & Gal, J. (2007). Poverty in the eyes of the beholder: Social workerscompared to other middle-class professionals. British Journal of Social Work,37 , 893–908.
Willems, S.J., Swinnen, W., & De Maeseneer, J.M. (2005). The GP’s perception ofpoverty: A qualitative study. Family Practice, 22, 177–183.
Weiss Gal, I., Benyamini, Y., Ginzburg, K., Savaya, R., & Peled, E. (2009). Socialworkers’ and service users’ causal attributions for poverty. Social Work, 54,125–133.
Dow
nloa
ded
by [
Uni
vers
ity o
f C
ambr
idge
] at
11:
18 0
8 O
ctob
er 2
014