posterior dislocation of meniscal bearing insert in mobile bearing unicompartmental knee...
TRANSCRIPT

The Journal of Arthroplasty Vol. 27 No. 3 2012
Case Report
From thHospitals Ndics, Luton
SubmitThe Co
found at dReprint
MCh (OrthLuton andLU4 0DZ L
© 20120883-5doi:10.1
PosteriorDislocationofMeniscal Bearing Insert inMobile Bearing Unicompartmental KneeArthroplasty Mimicking a Baker Cyst
Vinay Kumar Singh, MBBS, D'Ortho, MRCS, MCh (Orth), Dip. SICOT,*Sunil Apsingi, MBBS, MS, MRCS,y Saikrishna Balakrishnan, MBBS, MRCS,y
and Sanjiv Manjure, MS, FRCS, FRCS(Orth)y
Abstract: Unicompartmental knee arthroplasty (UKA) is a well-established procedure for isolatedmedial compartment osteoarthritis. Meniscal dislocation is a well-recognized complication inmobile bearing UKA especially when performed for the lateral compartment. Dislocation in medialUKA is relatively uncommon and is usually anterior when encountered. We would like to report acase of posterior dislocation of the bearing insert in a mobile bearing medial UKA presenting as aBaker cyst, which was subsequently revised to total knee arthroplasty. Keywords: unicompart-mental knee arthroplasty (UKA), posterior, dislocation, Baker cyst.© 2012 Elsevier Inc. All rights reserved.
Congruent mobile bearing Oxford knee replacementwas first introduced in 1978 by Goodfellow andO' Connor, and the first Oxford UKA was performedin 1982 [1-4]. Since its inception, UKA has been per-formed extensively and is widely accepted as a reliabletreatment option for isolated unicompartmental kneearthritis [1-4].Oxford UKA is based on the principle of achieving
near-normal knee kinematics by using an unconstrainedfully congruent mobile bearing polyethylene insert,which is functionally equivalent to a natural meniscus[1-4]. Full congruity throughout the full range ofmovement is achieved by the spherical femoral compo-nent [1-4]. Long-term results of medial UKA haveshown survival rates of 95% at 10 years [1-4]. Meniscaldislocation rate for medial UKA is 1 in 200 and 10% inlateral UKA [4]. Dislocation, when it happens, is usually
e *Trauma and Orthopaedics Surgery, Luton and DunstableHS Foundation Trust, Luton, UK; and yTrauma and Orthopae-and Dunstable Hospitals NHS Foundation Trust, Luton, UK.ted October 6, 2010; accepted April 27, 2011.nflict of Interest statement associated with this article can beoi:10.1016/j.arth.2011.04.045.requests: Vinay Kumar Singh, MBBS, D'Ortho, MRCS,), Dip. SICOT, Registrar Trauma and Orthopaedics Surgery,Dunstable Hospitals NHS Foundation Trust, Lewsey Road,uton, UK.Elsevier Inc. All rights reserved.
403/2703-0034$36.00/0016/j.arth.2011.04.045
494.e
anterior and rare in other directions [4-7]. We reportwhat we believe is the first case of posterior dislocationof the meniscal bearing in a mobile bearing UKA, whichpresented as a Baker cyst.
Case ReportA 61-year-old female patient with isolated medial
compartment osteoarthritis underwent an Oxford me-dial UKA (Biomet UK Ltd, Bridgend, South Wales,United Kingdom) in February 2006 through a standardmedial parapatellar approach. An Oxford UKA wasperformed with a small femur, 44-mm tibia with 4-mmpolyethylene meniscal bearing. The intraoperative andpostoperative periods were uneventful. At 6-monthfollow-up, she was asymptomatic. Clinical examinationof the knee showed no evidence of instability, and therange of movement was 0° to 110°. Eleven months afterthe UKA, she had sudden onset knee pain when shecaught her foot in the duvet while turning in bed. Thepain was associated with prominence of her veins withslight discoloration below the knee. She was still able toweight bear andmobilize with the help of painkillers anddid not seek any medical advice. Her pain and symptomsgradually improved. Four weeks later, she was reviewedin the orthopedic clinic for her annual follow-up whereshe complained of pain behind the operated knee.Clinical examination showed a range of movementfrom 0° to 120° and a tender swelling in the poplitealfossa and calf suggestive of a possible deep vein
13

Fig. 1. Anteroposterior and lateral radiographs showingdislocated mobile bearing polyethylene.
494.e14 The Journal of Arthroplasty Vol. 27 No. 3 March 2012
thrombosis. A Doppler ultrasound was requested, andradiographs of the knee were not taken. The scan ruledout a deep vein thrombosis but confirmed the presence ofa Baker cyst measuring 3.5 × 3.2 × 4.0 cm. Inflammatorymarkers were requested to rule out subclinical infectionand were unremarkable. She was then referred to arevision knee surgeon for further advice and possibleexcision of the cyst. Repeat clinical history was obtained;clinical examination revealed a palpable swelling in theposteromedial aspect of the knee. This was firm and didnot transilluminate. Plain radiographs of the knee wererequested, which showed posterior dislocation of themeniscal mobile bearing (Fig. 1). A magnetic resonance(MR) scan and arteriogram were then requestedpreoperatively to plan surgery (Figs. 2 and 3). Arterio-gram showed slight distortion of the popliteal vein butwas otherwise unremarkable. Magnetic resonance scanshowed the presence of a dislocated meniscal bearing inthe popliteal fossa beneath the subcutaneous tissue andfat. The posteriorly dislocated meniscus was removedthrough a posterior approach as a first stage. The medialUKA was subsequently revised to a navigated Columbus
Fig. 2. Saggital and axial MR scan showing
posterior-stabilized total knee replacement (B. BraunUKLtd) as a second-stage procedure (Fig. 4). Unicompart-mental knee arthroplasty was revised to totalknee arthroplasty (TKA) using, 2+ tibia, size 4 femurwith 10-mm polyethylene. Mild posterior laxity wasobserved intraoperatively during the revision procedurewith loosening of the tibial and femoral components.Tissue samples and swabs taken during the procedure didnot grow any organisms to suggest infection of theprosthesis. She had full resolution of her symptomspostsurgery and is mobilizing independently with a kneerange of movement of 0° to 100°.
DiscussionOxford UKA is a mobile bearing knee replacement.
The current trend toward minimally invasive surgeryhas rekindled enthusiasm for these devices despite thefact that most studies, with some notable exceptions,have shown a slightly worse survivorship for UKAcompared with TKA [1,3,8].Proponents of mobile bearing knee replacements
recommend its use due to near-normal physiologicknee kinematics reducing wear and early failure causedby high contact stress and early loosening caused byoverconstraint in a fixed bearing knee replacement[9,10]. The greatest documented advantage of UKA overTKA is faster recovery and rehabilitation.On the contrary, compared with fixed bearing designs,
mobile bearing knee implants are less forgiving to softtissue imbalance [1-4]. There is increased risk of bearinginstability and dislocation failing adequate soft tissuebalance or unequal flexion and extension gaps [3,4].Dislocation of the bearing is significantly higher in
lateral UKA in comparison with medial UKA [1-4].Increased dislocation in lateral UKA is primarily dueto the fact that the medial collateral ligament is tightand lateral collateral ligament lax in flexion. Therefore,the medial compartment gets distracted by only 2 mmon average in comparison with 7 mm on the lateral
dislocated polyethylene in popliteal fossa.
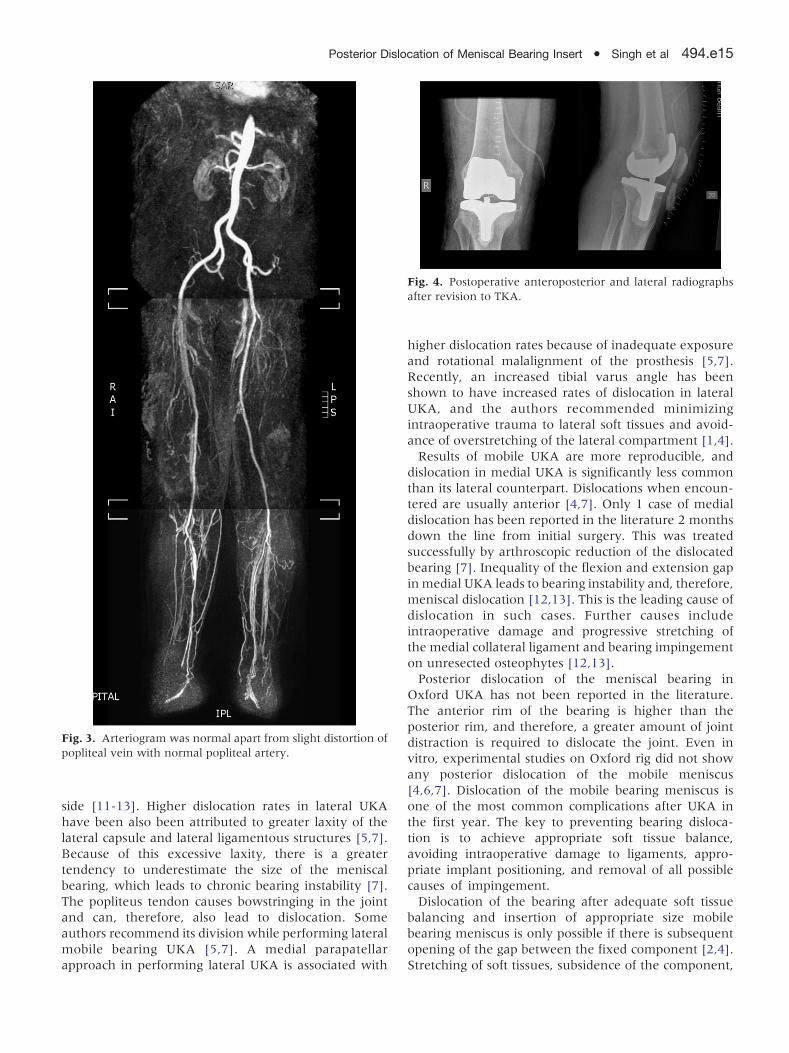
Fig. 3. Arteriogram was normal apart from slight distortion ofpopliteal vein with normal popliteal artery.
Fig. 4. Postoperative anteroposterior and lateral radiographsafter revision to TKA.
Posterior Dislocation of Meniscal Bearing Insert � Singh et al 494.e15
side [11-13]. Higher dislocation rates in lateral UKAhave been also been attributed to greater laxity of thelateral capsule and lateral ligamentous structures [5,7].Because of this excessive laxity, there is a greatertendency to underestimate the size of the meniscalbearing, which leads to chronic bearing instability [7].The popliteus tendon causes bowstringing in the jointand can, therefore, also lead to dislocation. Someauthors recommend its division while performing lateralmobile bearing UKA [5,7]. A medial parapatellarapproach in performing lateral UKA is associated with
higher dislocation rates because of inadequate exposureand rotational malalignment of the prosthesis [5,7].Recently, an increased tibial varus angle has beenshown to have increased rates of dislocation in lateralUKA, and the authors recommended minimizingintraoperative trauma to lateral soft tissues and avoid-ance of overstretching of the lateral compartment [1,4].Results of mobile UKA are more reproducible, and
dislocation in medial UKA is significantly less commonthan its lateral counterpart. Dislocations when encoun-tered are usually anterior [4,7]. Only 1 case of medialdislocation has been reported in the literature 2 monthsdown the line from initial surgery. This was treatedsuccessfully by arthroscopic reduction of the dislocatedbearing [7]. Inequality of the flexion and extension gapinmedial UKA leads to bearing instability and, therefore,meniscal dislocation [12,13]. This is the leading cause ofdislocation in such cases. Further causes includeintraoperative damage and progressive stretching ofthe medial collateral ligament and bearing impingementon unresected osteophytes [12,13].Posterior dislocation of the meniscal bearing in
Oxford UKA has not been reported in the literature.The anterior rim of the bearing is higher than theposterior rim, and therefore, a greater amount of jointdistraction is required to dislocate the joint. Even invitro, experimental studies on Oxford rig did not showany posterior dislocation of the mobile meniscus[4,6,7]. Dislocation of the mobile bearing meniscus isone of the most common complications after UKA inthe first year. The key to preventing bearing disloca-tion is to achieve appropriate soft tissue balance,avoiding intraoperative damage to ligaments, appro-priate implant positioning, and removal of all possiblecauses of impingement.Dislocation of the bearing after adequate soft tissue
balancing and insertion of appropriate size mobilebearing meniscus is only possible if there is subsequentopening of the gap between the fixed component [2,4].Stretching of soft tissues, subsidence of the component,

494.e16 The Journal of Arthroplasty Vol. 27 No. 3 March 2012
wear of the polyethylene insert, or any unaccustomedtrauma can all lead to opening of the joint [2,4].Dislocation in the present case occurred around a yearafter the UKA and was due to valgus and hyperexten-sion forces on the knee as a result of the foot gettingcaught in the duvet. Dislocation could be due tointraoperative injury to the deep fibers of the medialcollateral ligament and posterior capsule leading tolaxity and bearing dislocation with trivial trauma.Posterior migration of the dislocated bearing insertsubcutaneously could also be explained due to damageto posterior structures while performing tibial resection.Posterior laxity was also observed during the revisionprocedure, which would support the above mechanism.Loosening of the components was due to repeatedmetal-on-metal contact of the tibial and femoralprostheses as the patient continued to mobilize despitedislocation of meniscus due to minimal pain. The acutevascular changes were due to kinking of the poplitealvessels by the dislocated meniscal bearing compromisingcirculation and venous return. Subsequent inferiormigration of the dislocated meniscal bearing awayfrom popliteal vessels due to gravity and surroundingmuscular contraction as the patient mobilized decom-pressed these vessels, leading to resolution of thevascular symptoms [14]. Most of the patient's subse-quent symptoms were due to the mass effect of thedislocated insert with associated surrounding fibrosisleading to pain.Diagnosis of bearing dislocation can be made by
clinical history and physical examination. Plain radio-graphs are diagnostic. In the present case, the diagnosiswas delayed because the patient had minimal symptomsand continued to mobilize. Furthermore, the predomi-nant vascular symptoms distracted the clinician fromthe actual diagnosis, and plain radiographs were notobtained in the first instance.Posterior dislocation of the mobile bearing meniscus is
rare and may mimic a Baker cyst both clinically andradiologically, as was the case in our patient where thedislocated polyethylene insert was reported as a Bakercyst by the radiologist after USG of the knee.
ConclusionPosterior dislocation of the meniscal bearing in
medial mobile bearing UKA is rare and may presentwith vascular symptoms due to tamponade of thepopliteal vessels. A high index of suspicion is necessaryfor timely diagnosis and management. The patientmay be able to walk with minimal symptoms after
dislocation of the meniscal bearing. The dislocatedpolyethylene meniscal bearing may generate imagessimilar to a Baker cyst, leading to incorrect diagnosis andinappropriate management.
References1. Svard UCG, Price AJ. Oxford medial unicompartmental
knee arthroplasty: a survival analysis of an independentseries. J Bone Joint Surg [Br] 2001;83-B:191.
2. Goodfellow J, O'Connor J. The mechanics of the knee andprosthesis design. J Bone Joint Surg [Br] 1978;60-B:358.
3. Murray DW, Goodfellow JW, O'Connor JJ. The Oxfordunicompartmental arthroplasty: a ten-year survival study.J Bone Joint Surg [Br] 1998;80-B:983.
4. Robinson BJ, Rees JL, Price AJ, et al. Dislocation of thebearing of the Oxford lateral unicompartmental arthro-plasty. A radiological assessment. J Bone Joint Surg [Br]2002;84-5:653.
5. Robinson BJ, Rees JL, Price AJ, et al. A kinematic studyof lateral unicompartmental arthroplasty. Knee 2002;9-3:237.
6. Weale AE, Feikes J, Prothero D, et al. In vitro evaluationof the resistance to dislocation of meniscal-bearing totalknee prosthesis between 30 degrees and 90 degrees ofknee flexion. J Arthroplasty 2002;17-4:475.
7. Verhaven E, Handelberg F, Casteleyn PP, et al. Meniscalbearing dislocation in the Oxford knee. Acta Orthop Belg1991;57-4:430.
8. Lewold S, Goodman S, Knutson K, et al. Oxford meniscalbearing knee versus the Marmor knee in unicompart-mental arthroplasty for arthrosis: a Swedish multi-centresurvival study. J Arthroplasty 1995;10:722.
9. Argenson JN, O'Connor JJ. Polyethylene wear inmeniscal knee replacement: a one to nine-year retrievalanalysis of the Oxford knee. J Bone Joint Surg [Br]1992;74-B:228.
10. Psychoyios V, Crawford RW, O'Connor JJ, et al. Wear ofcongruent meniscal bearings in unicompartmental kneearthroplasty: a retrieval study of 16 specimens. J BoneJoint Surg [Br] 1998;80-B:976.
11. Tokuhara Y, Kadoya Y, Nakagawa S, et al. The flexiongap in normal knees. An MRI study. J Bone Joint Surg Br2004;86-8:1133.
12. Pandit H, Jenkins C, Beard DJ, et al. Mobile bearingdislocation in lateral unicompartmental knee replacement.Knee 2010;17-6:392.
13. Song MH, Kim BH, Ahn SJ, et al. Early complicationsafter minimally invasive mobile-bearing medial unicom-partmental knee arthroplasty. J Arthroplasty 2009;24-8:1281.
14. Rapp LG, Arce CA, McKenzie R, et al. Incidence ofintracranial bullet fragment migration. Neurol Res 1999;21-5:475.