post-traumatic adrenal apoplexy - journal of clinical
TRANSCRIPT

J. clin. Pat/i. (1955), 8, 185.
POST-TRAUMATIC ADRENAL APOPLEXYBY
SIMON SEVITTFromn the Pathology Department, Birmingham Accident Hospital and M.R.C. Indiustrial Injuzries
and Burns Research Unit
(RECEIVED FOR PUBLICATION FEBRUARY 25, 1955)
The first description of haemorrhage into theadrenal glands is attributed to Griselius, of Vienna,in 1670 (Doran, 1907). In the nineteenth centurycases, mostly of obscure aetiology, were describedby Rayer (1837), Dickinson (1863), Mattei (1883),Carrington (1885), Churton (1886), and others, andArnaud (1900) collected and reviewed 79 cases.
Since then reports of patients with gross adrenalhaemorrhage have been not infrequent, and thetwo clinico-pathological pictures of adrenalhaemorrhage in the newborn and that associatedwith fulminating meningococcal septicaemia, nowknown as the Waterhouse-Friderichsen syndrome,have been separated. This has left many cases
associated with diverse conditions. In some thehaemorrhage has been spontaneous and unassoci-ated with other disorders (e.g., Pearl and Brunn,1928; Barsoum, 1936; Thorstad, 1942; Falconer,1953). Occasionally extensive adrenal haemor-rhage complicates severe burns (Dudgeon, 1904;Weiskotten, 1919; Harris, 1929; Snelling and Erb,1935); sometimes it is associated with pregnancyor the puerperium (Hall and Hemken, 1936;Keele and Keele, 1942; Hurter, 1946; Dewhurst,1951 ; Crawford, 1951); occasionally the conditioncomplicates ulcerative colitis (Dr. P. N. Coleman,1954, personal communication; Wilson and Roth,1953), agranulocytosis (Seligman, 1932), leukaemia(Lauckner and Hebbert, 1947), pneumonia, septi-caemia, or cellulitis (Lusk and Brumbaugh, 1919;Seligman, 1932; Hall and Hemken, 1936). In otherreports chronic visceral disease has been found(Simmonds, 1902), such as chronic pancreatitis(Lavenson, 1908), hydatid hepatic cyst (Godfrey,1947), tuberculous pyelonephritis (Thorstad, 1942),and secondary carcinoma (Seligman, 1932), andoccasionally fatal adrenal haemorrhage is said tocomplicate an abdominal operation (Taylor, 1930).The first reports of cases following injury were
those of Canton (1863) and Mattei (1883), buthaemorrhage into the adrenals of guinea-pigs wasobserved by Brown-Sequard in 1852 after sectionof the spinal cord. In his review Arnaud con-
N
cluded that only three out of 79 cases were dueto trauma, and Lavenson (1908) could find onlythose reported by Canton and Mattei. In Pearland Brunn's (1928) review there were no new casesattributed to injury, but since then at least sevencases have been reported, three by Seligman (1932)and one each by Chandler (1934), by Snelling andErb (1935), by Thorstad (1942), and by Antonini(quoted by Thorstad).The purpose of this paper is to describe 14 cases
of unilateral or bilateral haemorrhage of theadrenal glands following severe injuries, to dis-cuss the pathogenesis of this condition, and toattempt an assessment of its clinical and patho-logical significance.
The PatientsFrom 1948 to 1954, 50 necropsies were per-
formed in the Birmingham Accident Hospital onpatients who died after severe injuries to the chestor abdomen, and in 13 of these one or bothadrenals were considerably haemorrhagic (26').Another patient (Case 11) with severe lower limbinjuries and only slight abdominal trauma alsohad a unilateral adrenal apoplexy, and these 14patients form the basis of the present study.* Thehaemorrhage was bilateral in three subjects andunilateral in the other 11, nine of which involvedthe right adrenal.Table I lists the age, sex, survival period, type
of accident, and main injuries of each patient,together with any operation performed and sig-nificant complications. Thirteen patients weremales, but this preponderance is probably occu-pational: 12 were adults, six under 40 years ofage. Three fell from a height at work and theremainder were involved in road accidents witha motor or other vehicle. One patient died eightdays after injury and the remainder within fivedays; two of these died within 24 hours and five
*Among the 50 necropsies were two others in each of which asmall central blood clot, 2-3 mm. diameter, was found in oneadrenai. These glands have also been studied, as they show theminimal lesions which may occur.
copyright. on O
ctober 24, 2021 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.8.3.185 on 1 A
ugust 1955. Dow
nloaded from

186 SIMON SEVITT
TABLE ISUMMARY OF TRAUMA IN 14 CASES
Case Sex and Survival Mode of Injury Main Injuries and Other Findings AdrenalNo. Age (Yr.) Period Apoplexy*
I M 57 3 days Fall from a height Fractures 2 to 7 R. ribs; fracture-dislocation R. pelvis. Ab- Bilateral. R.-dominal distension, vomiting. Uraemia (blood urea total. L.-280 mg.%) partial (i)
2 M 39 2 ,, Run over by a lorry Ruptured L. diaphragm. Fractures 7 to I L. ribs, haemo- Bilateralthoraces. Fractures ilium, L. tibia, fibula, femur. Small R.-partial (l)laceration liver, torn jejunum, colon deperitonealized. (Op. L.-partial (Q)-colostomy, etc.)
3 M 36 4 ,, Pinned under a bus Rupture L. kidney, spleen. Cracks R. and L. liver (op. Bilateralsplenectomy, liver packed). Low B.P. (80 40). Uncon- R.-subtotalscious after 18 hours. Oliguria, uraemia (blood urea L.-partial ( )210 mg.%). Cerebral ring haemorrhages +-
4 M 39 26 hours Crushed between a Superficial tear L. liver (op. packed). Biliuria. Traumatic R.-partial (A)lorry and a siding asphyxia. Myocardium bruised. Haemopericardium + +.
Sudden collapse 3 hr. before death
5 M 21 1 day Kicked by a horse, run Gross rupture R. liver, torn hepatic vein. Haemoperitoneum R.-totalover by cart 4+ + +. Rupture L. renal vein, bruised kidney. Fractures
R. and L. ribs, bilateral haemothorax. Fracture humerus.(Op. liver packed)
6_ M 58 3j days Car accident Fractures 9 to 11 L. ribs, L. haemothorax, rupture pleura. R.-subtotalMultiple fractures calvarium, cerebral laceration. Medul-lary-cerebellar coning. (Op. removal comminuted frac-tures skull.) Sudden collapse day 2
7 M 78 4 ,, Knocked down by a car Fractures 7 R. rib, bloody pleural effusion. Multiple fractures R.-partial (A)pelvis, central dislocated R. hip. Medullary-cerebellarconing. (Op. cystotomy.) Collapsed twice day 3
8 M 70 3j hours Hit by a crane, fell from Fractures R. 1 to 10 ribs, ilium, skull. Amputation both R.-partial (A)a height hands. (Op.-amputation completed.) Post-op. sudden
death. Severe coronary atheroma
9 M 36 5 days Fell off scaffold 25 feet. Ruptured R. liver + l . (Op.-laparotomy.) Fractures R.-partial (i)Hit chest and abdo- sternum, 2 to 9 R. ribs. Infected haemothoraces. Early with diffusemen on way down peritonitis. Bronchopneurnonia haemorrhage
10 M 54 13 ,, Knocked down by a car Bilateral multiple fractures ribs, L. haemopneumothorax, small R.-totalR. haemothorax. Superficial tear R. liver. Fractures skulland slight cerebral haemorrhage. Medullary cerebellarconing. Dislocated elbow. (Op.-reduced)
I I M 38 2 ,, Found lying in the road Bruising round duodenum, hepatic colon. Severe laceration R.-totalbe3iJe a truck and fracture L. thigh; perineal, anal laceration. Com-
pound fracture R. tibia, fibula. Myohaemoglobinuria. (Op.L. thigh amputation, transverse colostomy.) Small myo-cardial rupture. (Myocarditis and fragmentation)
12 F 55 21 hours Knocked down by acar Rupture spleen, L. kidney. (Op. nephrectomy.) Haemoperi- L.-totaltoneum + +. Fractures 3 to 10 L. ribs, small haemo-thorax. Fracture humerus
13 M 5 1j days Run over by a bus Small L. haemothorax, torn pleura (ribs intact). Massive L. L.-partial (A)atelectasis. Capsule tear spleen. L. kidney bruised. Frac-ture pelvis. Severe laceration L. thigh, perineum. (Op.repair of laceration)
14 M 72 8 ,, Knocked down by a Multiple fractures R. ribs, cracks R. liver, ruptured right R.-partial (0)cyclist kidney. (Op.-liver suture.) Post-op. paralytic ileus
(recovered). Bronchopneumonia. Infarct L. kidney
* In total and partial apoplexies the whole or part of the medulla respectively is occupied by haemorrhage (see text). The fractionsindicate the medullary area involved.
on the second day. The mode and nature of manyof the injuries indicated that the abdomen orthorax had been crushed.Thoracic and Abdominal Injuries. - Closed
abdominal or thoracic injuries were found in all14 subjects, in 13 of whom the injuries were severe.Rib fractures on one or both sides were found in10 and were usually associated with a unilateralor bilateral haemothorax; in two patients a
pneumothorax was also present. One patient hada ruptured diaphragm, in another the heart wasbruised and a haemopericardium later proved fatal(Case 4). In eight subjects the abdominal viscerawere injured, seven of whom also suffered a chestinjury: the liver was ruptured or cracked in seven(the main hepatic vein was torn in the one whoreceived 52 pints of blood), the spleens of threewere ruptured or torn, and in one patient the
copyright. on O
ctober 24, 2021 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.8.3.185 on 1 A
ugust 1955. Dow
nloaded from

POST-TRAUMATIC ADRENAL APOPLEXY
bowel was also torn and partly deperitonealized.In five subjects one or other kidney was rupturedor bruised. In one patient (Case 11) abdominalinjury was confined to bruising around theduodenum and hepatic colon.Other Injuries.-These were often severe and
multiple. Significant pelvic injuries were found infive patients who also received injuries to the chestor abdomen. The pelvis was badly fractured inthree patients, in two of whom it was the majorinjury (Cases 1 and 7), but the pelvic viscera wereintact.Three subjects had fractured skulls and cerebral
laceration, and haemorrhage was the major injuryin Case 6.
Other injuries included fractures of the longbones (Cases 2, 5, 11), guillotine amputation ofthe hands (Case 8), and severe lacerations of theperineum, thigh, etc. (Cases 11 and 13). The maininjuries of Case 11 were to the perineum and lowerlimbs.
The AdrenalsBefore describing the adrenals of the present
series, two anatomical types of adrenal haemor-rhage must be distinguished. In the first a blood
clot occupies part or the whole of the medulla andthe cortex is stretched around it. The gland isenlarged and distorted in its transverse axes andmay be 2 cm. or more thick (Fig. 1). This kind,
FIG. 1.-Total apoplexy. Transverse section left adrenal,Case 12, x 2.
4.
FIG. 2.-Subtotal apoplexy. Longitudinal section right adrenal, Case 3, x 2.
187
copyright. on O
ctober 24, 2021 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.8.3.185 on 1 A
ugust 1955. Dow
nloaded from
SIMON SEVITT
with which the present account is concerned, willbe referred to as the centrally haemorrhagic orapoplectic gland. In the second type multiple focalhaemorrhages, which may coalesce, occur in themedulla and cortex, but the gland retains its nor-mal shape. This kind was not found in the pre-sent series but has been described elsewhere(Sevitt, 1955b).
In the present series in every gland the essen-tial lesion was a central, firm, clotted haemorrhage,usually thickest in the centre, occupying a part orthe whole of the medulla (Figs. 1 to 3). The clot,which distended the gland antero-posteriorly, wassurrounded by the narrow, sometimes thinned andstretched cortex, which it frequently invaded andsometimes ruptured. In one patient the clot wasthickest eccentrically (Case 8), but otherwise thethickest part of the haemorrhage was in the middle.
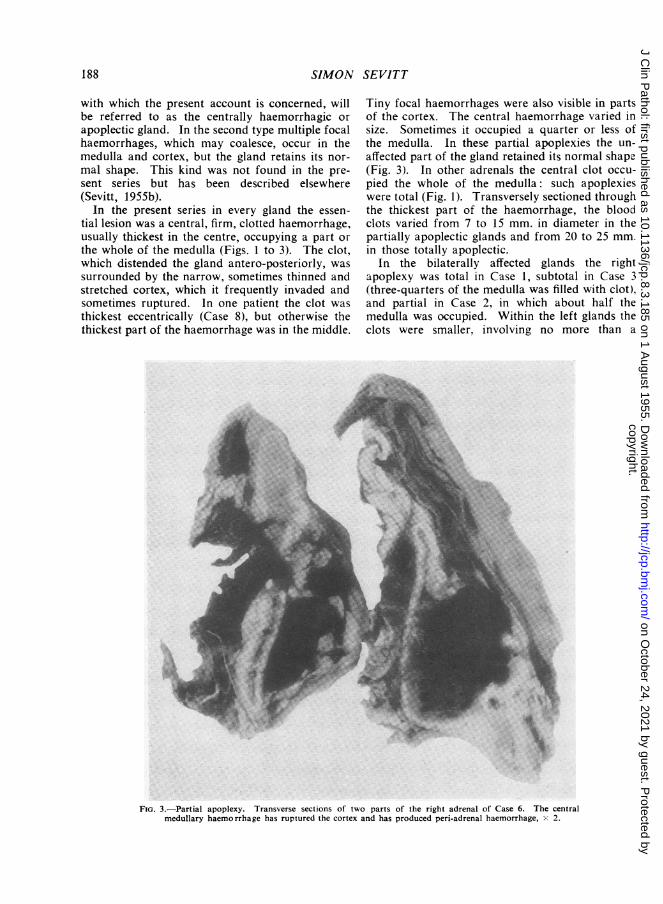
Tiny focal haemorrhages were also visible in partsof the cortex. The central haemorrhage varied insize. Sometimes it occupied a quarter or less ofthe medulla. In these partial apoplexies the un-affected part of the gland retained its normal shape(Fig. 3). In other adrenals the central clot occu-pied the whole of the medulla: such apoplexieswere total (Fig. 1). Transversely sectioned throughthe thickest part of the haemorrhage, the bloodclots varied from 7 to 15 mm. in diameter in thepartially apoplectic glands and from 20 to 25 mm.in those totally apoplectic.
In the bilaterally affected glands the rightapoplexy was total in Case 1, subtotal in Case 3(three-quarters of the medulla was filled with clot),and partial in Case 2, in which about half themedulla was occupied. Within the left glands theclots were smaller. involving no more than a
FIG. 3.-Partial apoplexy. Transverse sections of two parts of the right adrenal of Case 6. The centralmedullary haemorrhage has ruptured the cortex and has produced peri-adrenal haemorrhage, x 2.
188
copyright. on O
ctober 24, 2021 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.8.3.185 on 1 A
ugust 1955. Dow
nloaded from

POST-TRAUMATIC ADRENAL APOPLEXY
quarter of the medulla. Four of the unilaterallyaffected adrenals were totally apoplectic (Cases 5,10, 11, and 12), one subtotally (Case 6), and theremaining six were partially affected. In one ofthese (Case 9) the clot had ruptured through thecortex and a diffuse haemorrhage was presentthroughout most of the organ.
Periadrenal Haemorrhage and Rupture of theCortex.-Haemorrhage or bruising of the peri-adrenal tissues of 10 glands was visible through theposterior peritoneum. This haemorrhage wasnever gross: it was always less than a centimetrethick and in four cases was merely a bruising ofthe periadrenal fat. In four patients it was asso-ciated with a local rupture of the cortex (Fig. 3)through which the central and external haemor-rhages communicated (Cases 3 (right gland), 4, 6,and 8). Since similar haemorrhage was also foundoutside the intact glands and sometimes in otherinjured patients, it can arise independently ofintra-adrenal haemorrhage.
Histology.-The right and left glands were fixedin 10% formol saline and paraffin sections werecut at 5t. These were stained with haematoxylinand eosin, by Perl's method for iron, by Weigert'sfibrin method, and Verhoef's and Van Gieson'stechniques for elastica, smooth muscle, and con-nective tissue of blood vessels.The central blood clots which had completely
or almost completely destroyed the medullarytissue were formed of densely packed erythro-cytes lying within an irregular and often poorfibrin network. The haemorrhage was recent:red cell dehaemoglobinization, haemosiderin pig-ment and organization of the periphery of the clotwere absent. In some glands a dense, narrowlayer of leucocytes near the edge of part of theclot was externally layered by further haemor-rhage, suggesting that the bleeding may haveoccurred in two stages.The central haemorrhage irregularly invaded the
cortex, in some places as far as the capsule, inothers to the zona reticularis or fasciculata. Theboundary of the haemorrhagic area was ofteninfiltrated by polymorphonuclear leucocytes whichsometimes invaded the reticularis where thehaemorrhage was confined to the medulla.
Discrete, often multiple foci of cortical haemor-rhage were also seen.
Cortical necrosis was either associated withhaemorrhage or was free of haemorrhage.Haemorrhagic necrosis was more extensive insome (e.g., Cases 6, 10, and 12) than in others(e.g., Cases 7, 8, 14). The necrotic areas were
usually coextensive with the haemorrhage, some-times extended beyond it, and some discrete fociwere found histologically remote from the centralclot.
Foci of necrosis without haemorrhage were alsopresent in every gland. In some places the zonare:icularis and inner fasciculata bordering thecentral clot were necrotic ; often irregular focalzones of necrosis involved the fasciculata or lesscommonly the glomerulosa. The epithelial cellswere necrotic, but the cortical architecture wasoften intact and the sinusoids sometimes congested.In the affected parts the epithelial cell nuclei hadusually disappeared, but occasionally they weredense and pyknotic: the cytoplasm was eitheruniformly eosinophilic or had been partially dis-integrated by multiple vacuoles. Many necroticareas were loosely infiltrated by polymorpho-nuclear leucocytes which were denser at the peri-phery. In some an eosinophilic, albuminous ex-udate was present, particularly in zones borderingthe central haemorrhage, and in one gland theexudate was partly fibrinous (Case 1, right gland).Some necrotic areas were bordered by haemor-rhage, others by normal cortex. The necrosis wasprobably the result of ischaemia from local pres-sure or near-by haemorrhage. However, in everygland much of the cortex was normal, in somethe major part.
Pathogenesis of Post-traumatic Adrenal ApoplexyMost of the bleeding comes not from the solid
cortex but from the looser medulla and juxta-medullary cortex. It will be shown that ruptureof small vessels, mainly sinusoids and venules, isprobably brought about by a temporary compres-sion of the gland.The Vessels.-The adrenal has a rich blood
supply from three or more arteries which passthrough the capsule and break up into a sinusoidalnetwork in the cortex. Drainage is effectedthrough a single emissary vein which passesthrough the medulla, where it is joined by tribu-tary vessels which drain the medulla and the juxta-medullary cortex.Medium-sized and small venules were always
found at the periphery of the clot, usually in thejuxta-medullary cortex, and occasionally withinthe clot. In 12 of the 17 glands small tears,fissures, or ruptures were present in the walls ofvenules possessing a smooth muscle coat and inendothelial-lined channels. Similar ruptures wereseen in the two glands containing the small centralclots referred to in the footnote on page 185.Either part or the whole thickness of the wall was
189
copyright. on O
ctober 24, 2021 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.8.3.185 on 1 A
ugust 1955. Dow
nloaded from

SIMON SEVITT
torn and a trickle of red cells could often be seenin the gap. The venous walls were often oedema-tous, occasionally necrotic, and sometimes infil-trated by polymorphonuclear leucocytes.Venous thrombosis has been stressed by various
writers as the important factor producing adrenalhaemorrhage (e.g., Hall and Hemken, 1936; Keeleand Keele, 1942). In the present series venousthrombi were found in only one gland (right gland,Case 2). Here a few medium-sized veins con-tained hyaline thrombi, but torn venules werealso present. The venous thrombosis probablydeveloped after the haemorrhage had occurred.In two glands hyaline thrombosis of some corticalsinusoids was present which must also have beenpost-haemorrhagic. The arteries and arterioleswere intact and never thrombosed.Mechanism of the Apoplexy.--Deeply hidden
behind the abdominal cavity and protected by theliver and other organs in front and by the spinalcolumn behind, the small adrenals are considerablyprotected from the effects of violence. For ex-ternally applied forces to act on an adrenal theymust pass through and act upon the surroundingstructures and organs. These tissues are likely tobe injured if the adrenal becomes haemorrhagic.Therefore if the apoplexy is due to an antero-posterior crushing injury the haemorrhagic adrenaland injured viscera would be found on the sameside. An alternative possibility is that haemor-rhage is the result of an acute rise of intra-adrenalvenous pressure resulting from sudden and severecompression of the inferior vena cava during thecrushing injury.
Consider Case 12, a woman in whom a leftadrenal apoplexy was found. She was knockeddown and probably run over by a car; the spleenand left kidney were ruptured and the left thoraciccage fractured. Both the adrenal haemorrhageand the main thoraco-abdominal injuries were onthe left side in this patient and in Case 13. Ofthe nine patients with right-sided apoplexy, eighthad thoraco-abdominal injuries and in six majoripsilateral injuries were present (Cases 5, 7, 8, 9,10, and 14). For example, in Case 14, the rightribs were fractured, the right side of the liverwas cracked, the right kidney was torn, and theright adrenal was haemorrhagic. In Case 4 thebruising of the heart was probably due to crushingof the chest.
In one patient (Case 6) there was an apparentcontradiction between the left-sided chest injuryand the right-sided adrenal apoplexy. Hisapoplexy may have been the result of obliqueforces transmitted to the right side of the liver,
which might then have crushed the adrenal againstthe vertebral column. Oblique forces might alsoexplain the apoplexy of Case 11, in which the evi-dence of thoraco-abdominal trauma was confinedto bruising around the duodenum and hepaticcolon.Of those with both glands haemorrhagic, Case 1
fell from a height and had severe right-sided in-juries, Case 2 was run over by a lorry and exten-sive crush injuries of the chest and abdomen werepresent, and in Case 3, a man who was pinnedunder a bus, the upper abdomen was crushedand injured.
Therefore the trauma in most patients corre-sponded with the side of the adrenal apoplexyand crushing injuries could be implicated. Theconclusions cannot be escaped that post-traumaticadrenal haemorrhage is the result of directviolence.Blood Transfusion.-Incompatible transfusion
has been incriminated in some cases of adrenalhaemorrhage (Snelling and Erb, 1935; Hurter,1946 ; Crawford, 1951). On admission the patientswere shocked and were urgently transfused. Infour subjects one to four bottles of Group 0Rhesus-negative (D-negative) blood were givenfirst and were followed by blood of the homo-logous ABO and Rhesus (D) type. The remainderreceived only homologous blood after rapid ABOgrouping and Rhesus typing, the results of whichwere confirmed by a slower method. Cross-matching of the first bottles of blood with thepatient's serum was not possible before transfusionbut was always performed later. All the cross-matches were carried out in both saline andalbumin suspension at 370 C. and no incompati-bility was detected.Four of the patients received two, three, or
four bottles of blood; six were given 10 to 12bottles and the remainder 6, 16, 21, and 52 bottlesrespectively. There was no clinical or laboratoryevidence of adverse reaction. The haemoglobin-uria found in Case 11 was due to myohaemoglobin.
Sigicance of Adrenal Apoplexy after TraumaAll the patients were severely injured and only
in Cases 4 and 8 was death sudden and unexpected.Necropsies revealed a haemopericardium in theformer and severe coronary atheroma in the latter.The post-mortem findings in Cases 5, 6, and 9indicated that the injuries were too severe to expectsurvival, and that the death of Case 12 was due tohaemorrhage from a ruptured spleen. Both Cases7 and 14 were over 70 years of age. In Cases 10,11, and 13 adrenal haemorrhage was judged to
190
copyright. on O
ctober 24, 2021 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.8.3.185 on 1 A
ugust 1955. Dow
nloaded from

POST-TRA UMATIC ADRENAL APOPLEXY
have a possible but doubtful clinical significance,and in the remaining three it may have contributedto the deaths of the patients, since the lesionswere bilateral (Cases 1, 2, 3). However, the fataloutcome of even these patients was not surprising,since not only were the injuries severe but two ofthem developed renal failure (Cases 1 and 3) andthe other had had intestinal injuries (Case 2).Nevertheless the adrenal haemorrhage may haveproduced its own physiopathological disorder andhave been responsible for the abdominal distensionand vomiting in Case 1, the low blood pressure inCase 3, and the sudden collapse of Cases 6 and 7.TIhe possibility that the adrenal haemorrhageplayed a contributory role in the deaths of theseand other patients cannot be excluded on clinicalgrounds.
Histological Tests of Adrenocortical HyperactivityThe influence of adrenal haemorrhage on
cortical activity might be assessed by two histo-logical tests. One of these is based on the numberof eosinophil leucocytes in the spleen (Sevitt,1955a, 1955b) and the other upon the depletionof cortical lipoid in the hyperactive adrenal cortex.
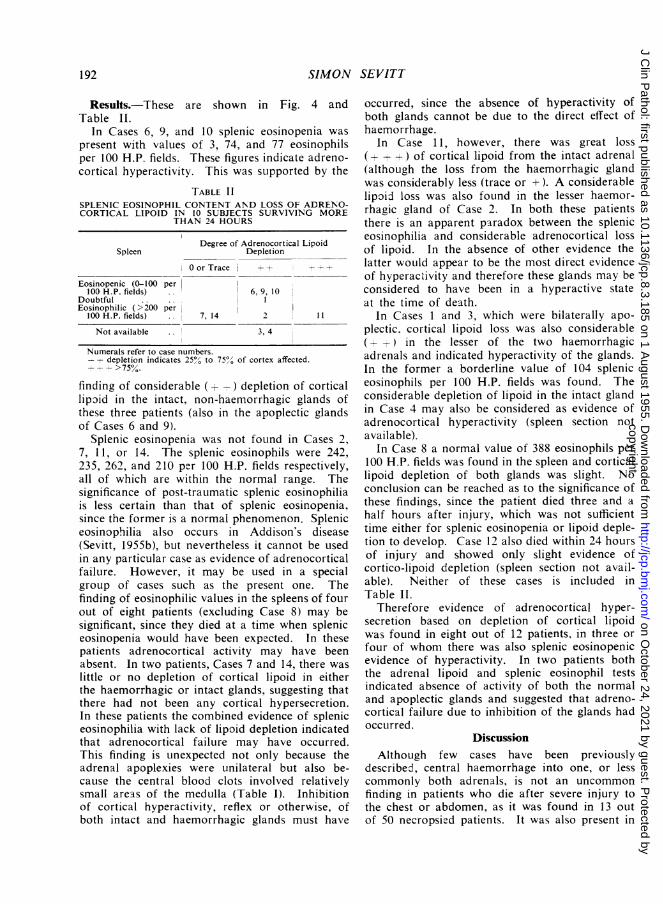
Splenic Eosinopenia.-Elsewhere it has beenshown that the normal spleen contains manyeosinophil leucocytes, that within 12 to 24 hoursof injury eosinopenia occurs and is found in thosewho die during the next few days (Sevitt, 1955a;Sevitt, 1955b). It was also found that spleniceosinopenia reflects blood eosinopenia, and, sincethe latter is due to adrenocortical hyperactivity,the former was postulated as also reflecting thisactivity. Splenic eosinopenia therefore may beused as post-mortem evidence of adrenocorticalhyperactivity. The normal range of eosinophilsin the spleen varies from 200 to 700 per 100 highpower (H.P.) fields (x 378) in 5,u paraffin sectionsand never falls below 100 per 100 H.P. fields.Values below 100 indicate eosinopania. In Fig. 4the shaded area represents the limits of the ex-pected values after severe trauma. Up to a fewhours of injury the normal range of splenic eosino-phils is always present: thereafter and up to 24hours after trauma-the transition period-eithernormal, intermediate, or definite eosinopenicvalues may occur.
Paraffin blocks of spleens were available in nineof the 14 cases. Sections were cut at 5,u and werestained by carbol-chromotrope and haematoxylin(Lendrum, 1944) which coloured the eosinophilgranules a bright red. The number of eosinophil
leucocytes in 200 H.P. fields from two sectionswas counted and the results expressed per 100 H.P.fields.
700r
6OO3
00
400La
-J
A.200
0
00
"cx
u.J
a. 501_t)
zs
0 ;
SME~~EOSINOPIL IN POST-TRjWMATIC ADRNAL APOLEY
'.S a- .
'I..2..,.'.~~~~~~~~~~~1
.._,|t,.6
0 12 24 2HOURSSURVIVAL
3 4DAYS
PERIOD
5 6 7 8
FIG. 4.
Depletion of Cortical Lipoid-The normal rest-ing adrenal cortex contains abundant sudanophillPpoid in all its zones. Depletion of lipoid fromthe human adrenal occurs after severe haemor-rhage and injury (Elliott, 1914; Urechia, Manta,and Bumbacescu, 1940), and is usually associatedwith splenic eosinopenia (Sevitt, 1955b). Signifi-cant loss of cortical lipoid will therefore be inter-preted as indicating adrenocortical hypersecretion.Conversely, if lipoid depletion, which is expectedafter injury, does not occur, its absence will beinterpreted as indicating absence of adrenocorticalhypersecretion.
In 12 of the 14 cases both adrenal glands wereavailable for study. Frozen sections were cut at10 to 15,u, stained with Sudan IV or oil red andcounterstained with haematoxylin or light green.Adrenocortical depletion of lipoid was assessedhistologically as 0, trace, +, + +, and + + +(see footnote of Table II).
191
O *
I
copyright. on O
ctober 24, 2021 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.8.3.185 on 1 A
ugust 1955. Dow
nloaded from
1SIMON SEVITT
Results.-These are shown in Fig. 4 andTable II.
In Cases 6, 9, and 10 splenic eosinopenia waspresent with values of 3, 74, and 77 eosinophilsper 100 H.P. fields. These figures indicate adreno-cortical hyperactivity. This was supported by the
TABLE IISPLENIC EOSINOPHIL CONTENT AND LOSS OF ADRENO-CORTICAL LIPOID IN 10 SUBJECTS SURVIVING MORE
THAN 24 HOURS
SpleenDegree of Adrenocortical Lipoid
Depletion
0 or Tracej4+
Eosinopenic (0-100 per100 H.P. fields) .. 6, 9, 10
DoubtfulEosinophilic (>200 per
100 H.P. fields) 7, 14 2 11
Not available 3, 4
Numerals refer to case numbers.-+ depletion indicates 25/,' to 75,'O of cortex affected.
+ _ > 75%.
finding of considerable ( +-) depletion of corticallipoid in the intact, non-haemorrhagic glands ofthese three patients (also in the apoplectic glandsof Cases 6 and 9).
Splenic eosinopenia was not found in Cases 2,7, 1 1, or 14. The splenic eosinophils were 242,235, 262, and 210 per 100 H.P. fields respectively,all of which are within the normal range. Thesignificance of post-traumatic splenic eosinophiliais less certain than that of splenic eosinopenia,since the former is a normal phenomenon. Spleniceosinophilia also occurs in Addison's disease(Sevitt, 1955b), but nevertheless it cannot be usedin any particular case as evidence of adrenocorticalfailure. However, it may be used in a specialgroup of cases such as the present one. Thefinding of eosinophilic values in the spleens of fourout of eight patients (excluding Case 8) may besignificant, since they died at a time when spleniceosinopenia would have been expected. In thesepatients adrenocortical activity may have beenabsent. In two patients, Cases 7 and 14, there waslittle or no depletion of cortical lipoid in eitherthe haemorrhagic or intact glands, suggesting thatthere had not been any cortical hypersecretion.In these patients the combined evidence of spleniceosinophilia with lack of lipoid depletion indicatedthat adrenocortical failure may have occurred.This finding is unexpected not only because theadrenal apoplexies were unilateral but also be-cause the central blood clots involved relativelysmall areas of the medulla (Table I). Inhibitionof cortical hyperactivity, reflex or otherwise, ofboth intact and haemorrhagic glands must have
occurred, since the absence of hyperactivity ofboth glands cannot be due to the direct effect ofhaemorrhage.
In Case 11, however, there was great loss(-r- -+ ) of cortical lipoid from the intact adrenal(although the loss from the haemorrhagic glandwas considerably less (trace or +). A considerablelipoid loss was also found in the lesser haemor-rhagic gland of Case 2. In both these patientsthere is an apparent paradox between the spleniceosinophilia and considerable adrenocortical lossof lipoid. In the absence of other evidence thelatter would appear to be the most direct evidenceof hyperactivity and therefore these glands may beconsidered to have been in a hyperactive stateat the time of death.
In Cases 1 and 3, which were bilaterally apo-plectic. cortical lipoid loss was also considerable(- ) in the lesser of the two haemorrhagicadrenals and indicated hyperactivity of the glands.In the former a borderline value of 104 spleniceosinophils per 100 H.P. fields was found. Theconsiderable depletion of lipoid in the intact glandin Case 4 may also be considered as evidence ofadrenocortical hyperactivity (spleen section notavailable).
In Case 8 a normal value of 388 eosinophils per100 H.P. fields was found in the spleen and corticallipoid depletion of both glands was slight. Noconclusion can be reached as to the significance ofthese findings, since the patient died three and ahalf hours after injury, which was not sufficienttime either for splenic eosinopenia or lipoid deple-tion to develop. Case 12 also died within 24 hoursof injury and showed only slight evidence ofcortico-lipoid depletion (spleen section not avail-able). Neither of these cases is included inTable II.
Therefore evidence of adrenocortical hyper-secretion based on depletion of cortical lipoidwas found in eight out of 12 patients, in three orfour of whom there was also splenic eosinopenicevidence of hyperactivity. In two patients boththe adrenal lipoid and splenic eosinophil testsindicated absence of activity of both the normaland apoplectic glands and suggested that adreno-cortical failure due to inhibition of the glands hadoccurred.
DiscussionAlthough few cases have been previously
described, central haemorrhage into one, or lesscommonly both adrenals, is not an uncommonfinding in patients who die after severe injury tothe chest or abdomen, as it was found in 13 outof 50 necropsied patients. It was also present in
192
copyright. on O
ctober 24, 2021 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.8.3.185 on 1 A
ugust 1955. Dow
nloaded from

POST-TRAUMATIC ADRENAL APOPLEXY
another severely injured patient with relativelyminor abdominal trauma. It is likely that adrenalapoplexy also occurs in some of those who survivesimilar injuries, but at present those who are
affected are not recognized and neither theincidence nor the clinical significance of thehaemorrhage is known. Their recognition may beimportant, since any morbidity or fatality due toadrenal haemorrhage might be lessened by theadministration of cortisone or other drugs.The mechanism of the haemorrhage and its
central location within the gland are probablydependent on the anatomical relationships andhistological structure of the organ and thepeculiarities of its blood supply. One theory,which is consistent with the data, depends on thefollowing considerations. Parts of both glands liein front of the spinal column against which theycould be compressed when the upper abdomen or
lower thorax is severely crushed. The rightadrenal is more likely to be damaged than theleft because much of its anterior surface is closelyopposed to the liver. This could largely explainwhy nine of the 11 unilateral apiplexies involvedthe right gland. Damage to vessels occurs more
readily within the spongy medulla and looselytextured zona reticularis than within the solidcortex. Rupture of the centrally situated venulesand sinusoids occurs and a central haemorrhagedevelops which distends the peripheral cortex.Thus the typical result of injury to the adrenalis a central haemorrhage just as the classicalresult of trauma to the spleen or liver is a rup-
ture. On the other hand, the central haemor-rhage might follow an acute rise of intra-adrenalvenous pressure resulting from sudden and severe
compression of the inferior vena cava during thecompression of the abdomen. The right adrenalwould also be affected more often than the leftbecause the right adrenal vein drains directly intothe vena cava whilst the left vein first joins therenal vein.Among Snelling and Erb's cases of adrenal
haemorrhage, one followed a head injury, andcerebral injury was also found in two of Selig-man's cases and in Cases 6, 8, and 10. Thequestion arises whether cerebral injury, nervous
stimulation, or shock can produce adrenal haemor-rhage, as this might also explain the contra1ateraladrenal haemorrhages in Case 6 and in Seligman'sCase 1, and also the apoplexy in Case 11, in whichsevere thoraco-abdominal injury was absent. Onthe other hand, the writer has never seen adrenalapoplexy in a not inconsiderable necropsy experi-ence of cerebral, spinal cord, and other severe
injuries, so that adrenal haemorrhage from nervousirritation or shock must be a rare condition if itoccurs at all. It is therefore suggested that theseapparent paradoxes are due to unsuspectedmechanical stresses acting on the adrenal whichreach it through a complex thoracic or abdominalpathway.Any clinico-pathological significance attached to
adrenal apoplexy is probably due to interferencewith cortical rather than medullary function, sinceonly the cortex is essential to life. Cortical activitymay be affected in two ways. First, parts of itare destroyed by haemorrhage or otherwise ren-dered necrotic, but since much remains histologic-ally viable death of tissue probably plays a minorpart in reducing cortical activity. Secondly, thepressure of the central haemorrhage could inter-fere with the venous drainage of the gland andabolish or reduce the venous blood flow, particu-larly when the clot fills the whole medullary space.Formation of hormones may cease, or, if thecapillary blood flow persists, may continue for atime and depletion of cortical lipoid may occureven though the secretions never reach the in-ferior vena cava. This may have occurred, forexample, in the totally apoplectic gland of Case 1in which considerable depletion of cortical lipoidwas found. In partially apoplectic glands thesecretion from the hyperactive cortex will reachthe general circulation, since drainage of thevenous tributaries in the unaffected part of themedulla will continue unless the main vein iscompressed near its place of exit.
Clinical assessment of the significance of theapoplexies was rendered difficult because all thepatients were severely injured, and death wasusually not surprising. However, the possibilitythat certain symptoms were due to the haemor-rhagic adrenals and that acute adrenocorticalfailure played a contributory role in the death ofsome patients could not be excluded.Two histological tests for adrenocortical hyper-
activity, one based on eosinopenia of the spleenand the other upon the depletion of lipoid inthe cortex, were of some value. Evidence ofadrenocortical hyperactivity based on loss ofcortical lipoid was found in eight out of 12patients, in three (or four) of whom there wasalso splenic eosinopenia. Certainly in these threeor four patients physiological failure of corticalactivity had not occurred. On the other hand,the finding of splenic eosinophilia in four out ofeight patients who died at a time after injury wheneosinopenia would have been expected suggestedthat adrenocortical hyperactivity may have been
193
copyright. on O
ctober 24, 2021 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.8.3.185 on 1 A
ugust 1955. Dow
nloaded from

SIMON SEVITT
absent and that physiological failure may haveoccurred. In two cases the absence of scanty lossof cortical lipoid from both the intact and apo-plectic glands supported this. As only one glandwas haemorrhagic, activity of the cortex of theintact gland must have been inhibited. In theother two patients the considerable loss of corticallipoid was local evidence of cortical hypersecretion,but in the bilaterally haemorrhagic subject theendocrine secreted may never have reached thesystemic circulation because of possible pressureon the central adrenal veins. This cannot explainthe association of splenic eosinophilia with severeloss of lipoid in the patient with unilateral adrenalhaemorrhage, but a similar association occasion-ally occurs in patients with intact adrenals (Sevitt,1955b).
SummaryCentral apoplexy of one or both adrenal glands
was found in 13 out of 50 patients who died aftersevere closed injuries to chest or abdomen (26%)and in another severely injured patient showingslight evidence of abdominal injury. Evidence isadvanced that crushing of the glands tears themedullary venules and is responsible for thecentral haemorrhage. This stretches the cortex,often invades it, and sometimes ruptures it.The significance of the apoplexies was estimated
by two histological tests of adrenocortical hyper-activity, one based on the eosinophil content ofthe spleen and the other on depletion of adreno-cortical lipoid, particularly in the non-haemor-rhagic glands. Both were in agreement thatcortical hyperactivity had been present in at leastthree or four patients. Evidence of hyperactivitybased on cortical lipoid loss alone was found ineight out of 12 cases examined. The results ofboth tests suggested that adrenocortical failure dueto glandular inhibition had occurred in twopatients with unilateral apoplexy.
AddendumDuring the first few months of 1955, necropsies
were performed on 10 patients with closed thoracic,abdominal, or pelvic injuries and adrenal apoplexywas found in three of them. This makes a totalof 16 out of 60 cases (approximately 27%). Thefirst subject (male, 23 years), who died two daysafter a road accident, sustained multiple right ribfractures and a lacerated lung. He had an incom-plete right adrenal apoplexy. Extreme eosin-openia of the spleen and partial depletion of lipoidfrom the left adrenal cortex indicated adreno-cortical hyperactivity. In the second patient (male,7 years) bilateral adrenal apoplexy appeared to
have precipitated or accelerated his death. Hewas knocked down by a van, sus.ained a compoundfracture of the right tibia and fibula and a rup-tured spleen which was removed. He was trans-fused with 2 pints of blood. Next day, sudden col-lapse was associated with sudden tachycardia (pulse160), respirations 40 and a fall of blood pressureto 90/60. Soon he became unconscious and diedfour hours after his collapse and about two daysafter injury. Necropsy revealed fractures of rightribs 9-12, a central haemorrhagic laceration of theright side of the liver with superficial tears of theleft side, a slight bruise of the right frontal cerebrallobe, and a bilateral total adrenal apoplexy.Histologically there was complete haemorrhagicnecrosis of the medullae and cortices and the latterwere stuffed with lipoid. Unfortunately the spleenhad been discarded. The third patient (male, 78years) fell down the stairs and fractured the ninthand tenth right ribs. He died 10 days later; severecoronary sclerosis, duodenal ulceration, an oldpulmonary empyema, and a partial apoplexy ofboth adrenals (right more than the left) werepresent.
The writer is a part-time member of the scientificstaff of the Medical Research Council.Thanks are due to the surgeons concerned for the
use of the clinical notes, to Mr. D. Gibb, A.I.M.L.T.,for the preparation of the sections, to the photo-graphic department of the hospital, and to my secre-tary, Mrs. M. Swinden.
REFERENCESArnaud, F. (1900). Arch. gen. Med., 9 ser, 4, 5.Barsoum, H. (1936). Brit. med. J., 2, 972.Canton, E. (1863). Trans. path. Soc., Lond., 14, 257.Carrington, R. E. (1885). Ibid., 36, 454.Chandler, L. R. (1934). Surg. Clin. N. Amer., 14, 1319.Churton, T. (1886). Lancet, 1, 245.Crawford, M. D. (1951). J. Path. Bact., 63, 365.Dewhurst, C. J. (1951). Brit. med. J., 2, 22.Dizkinson (1863). Trans. path. Soc. Lond., 14, 256.Doran, A. H. G. (1907). Proc. roy. Soc. Med., 1 (Surg. Sect.), 201.Dudgeon, L. S. (1904). Amer. J. med. Sci., 127, 134.Elliott, T. R. (1914). Quart. J. Med., 8, 47.Falconer, C. D. (1953). Brit. J. Urol., 25, 183.Godfrey, L. W. (1947). Brit. med. J., 1, 181.Hall, E. M., and Hemnken, L. (1936). Arch. intern. Med., 58, 448.Harris, R. I. (1929). Brit. J. Surg., 16, 677.Hurter, L. E. (1946). Proc. roy. Soc. Med., 39, 581.Keele, D. V., and Keele, K. D. (1942). Brtt. med. J., 2, 687.Lavenson, R. S. (1908). Arch. intern. Med., 2, 62.Lauckner, J. R., and Hebbert, F. J. (1947). Glasg. med. J., 28, 366.Lendrum, A. C. (1944). J. Path. Bact., 56, 441.Lusk, F. B., and Brumbaugh, A. (1919). J. Amer. med. Ass., 72,
1062.Mattei, R. (1883). Sperimentale, 51, 386.Pearl, F., and Brunn, H. (1928). Surg. Gynec. Obstet., 47, 393.Rayer, P. (1837). Experience, 1, 17 (quoted by Arnaud, F.).Seligman, B. (1932). Med. J. Rec., 135, 209.Sevitt, S. (1955a). Jourral of Clinical Pa-hglogy, 8, 42.
(1955b). J. Path. Bac'. In the press.Simmonds, M. (1902). Virch. Arch. path. Anat., 170, 242.Snelling, C. E., and Erb, I. H. (1935). J. Pediat., 6, 22.Taylor, G. W. (1930). New Engi. J. Med., 202, 269.Thorstad, M. J. (1942). Amer. J. Surg., 55, 44.Urechia, C. I., Manta, I., and Bumbacescu (1940). Mschr. Psychiat.,
10,, 143.Weiskotten, H. G. (1919). J. Amer. med. Ass., 72, 259.Wilson, D. A. W., and Roth, D. (1953). Ibid., 152, 230.
194
copyright. on O
ctober 24, 2021 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.8.3.185 on 1 A
ugust 1955. Dow
nloaded from