portal embolization increasing liver volume and function€¦ · · 2015-12-10– the future...
TRANSCRIPT

5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015
Portal Embolization Increasing Liver Volume and
Function
Juan Carlos García-Valdecasas Salgado Jefe de Servicio de Cirugía
Catedrático de Cirugía Hospital Clínic. Universidad de Barcelona

5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015
• MULTIPLES ESCENARIOS – Según la Magnitud: – Tamaño, Número, Localización, – Indice de Afectación Hepática – Según el Tiempo de Aparición: – Sincrónicas y Metacrónicas – Según Respuesta al Tratamiento QT
– POSIBILIDAD DE RESECCION
Enfermedad metastásica CCR

5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015 Definition of Resectability….
• In the context of the metastatic disease – Loco/Regional Recurrence – Concomitant Metastases
• Any Patient – In whom all disease can be remove with a
negative margin* – Who has an adequate remnant hepatic
volume/reserve * De Haas RJ et al Ann Surg 248:626-637, 2008

5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015
• Increased Safety • Increased knowledge
– Understanding Segmental Anatomy • Vascular and biliary tract distribution
– Understanding Postoperative Immediate Function • Acute Liver Failure
Limits of Resectability….
• Importance of – The Future Liver Remnant Volume

5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015 Strategies to Liver Resection….
• Strategies to downsize metastatic disease 1. Neoadjuvant Chemotherapy
• Strategies to increase FLR volume 1. Interventional Radiology
• Portal Vein Embolization
2. Surgical Approach a. Two Stage Hepatectomy b. Two-stage Partition and Hepatectomy (ALPPS) c. Vascular Resection and Reconstruction d. “In situ” Hypothermic Liver Perfusion

5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
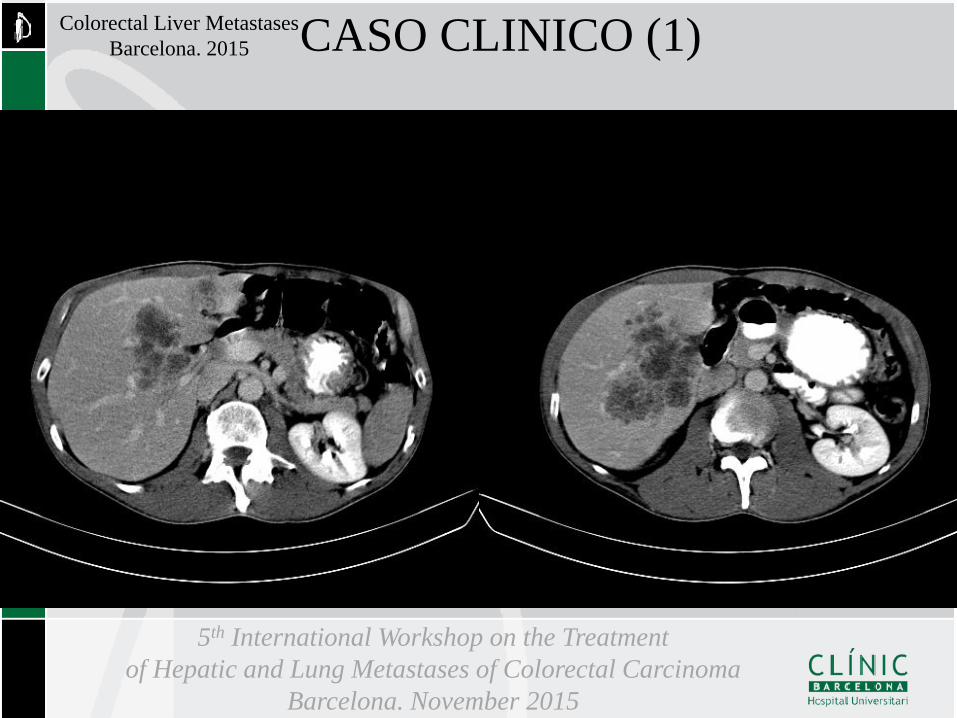
Colorectal Liver Metastases Barcelona. 2015 CASO CLINICO (1)
5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015 CASO CLINICO (1)

5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015
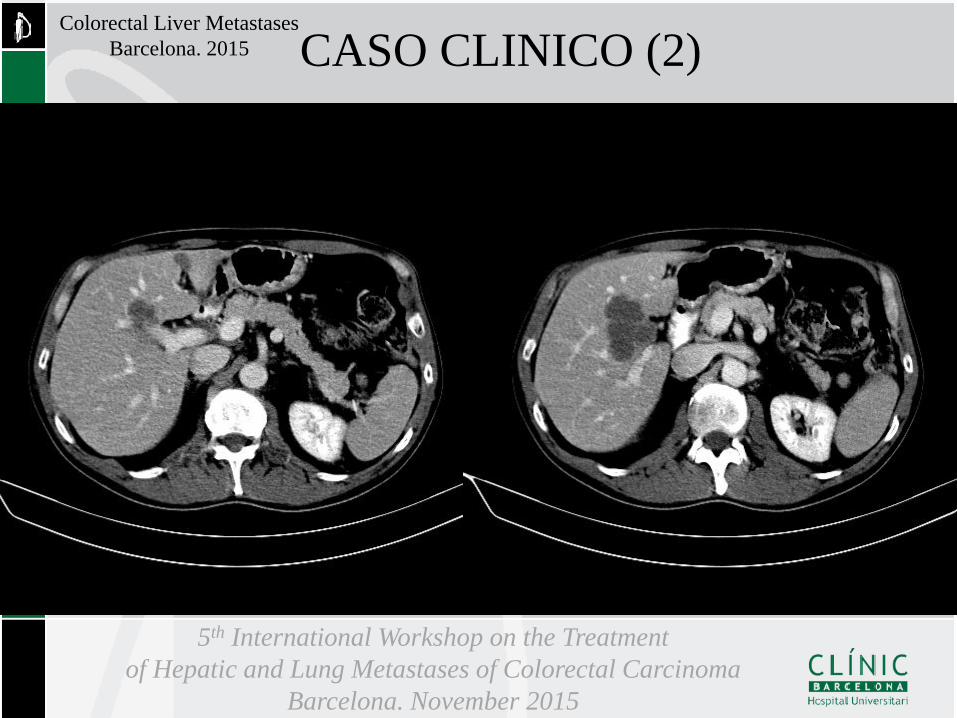
• The role of new Chemotherapy Agents CASO CLINICO (2)
5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015 CASO CLINICO (2)

5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015 CASO CLINICO (3)

5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015 CASO CLINICO (3)

5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015
•2009 (Junio-Noviembre)
•QT neoadyuvante. FOLFOX + RAMUCIRUMAB x7 de •2009 (Octubre)
•TC TORACOABDOMINAL. Disminución significativa •TLV: 1.536 ml. FLR: 387 ml.(25%)
•2009 (Diciembre) •Intervención Qurúrgica: Hemicolectomia derecha y Hepatectomia derecha+Res.Seg.Les. SIII
Enfermedad actual

5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015
Curso Postoperatorio
•Día +5. Insuficiencia Hepática Posthepatectomía
•Bil. 5.4 mg/dL. TºP. 47%. Ascitis.
•Día +15. Alta Hospitalaria
•AP. Higado no tumoral afectado por QT • Síndrome de Obstrucción Sinusoidal

5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015
•2010 (Agosto).
•TAC/PET. Recidiva Unica Hepática y ganglionar •FOLFIRI+Bevacizumab x16
•2010 (Diciembre) •FGS. Varices esofágicas grado I. Ulcera Péptica
•2011 (Mayo). •Plaquetopenia y Esplenomegalia
•2011(Noviembre). •Varices esofágicas (grado II). Circulación Perigástrica •HDA por varices esofágogástricas. Banding x4 •Elastografía Hepática. 10.0 kPa
Evolución

5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015
Evolución •2012 (Octubre). Varices esofágicas grado III •2013 (Diciembre). Encefalopatía Hepática
•Bil 4 mg/dL, Plaquetas 34000 y TP 48%. •2014 (Marzo). QT de mantenimiento (se para)
•Capecitabina + Bevacizumab
•2014 (Septiembre): Nuevo episodio de Encefalopatia •2015 (Febrero). Exitus

5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015 Strategies to Liver Resection….
• Strategies to downsize metastatic disease 1. Neoadjuvant Chemotherapy
• Strategies to increase FLR volume 1. Interventional Radiology
• Portal Vein Embolization
2. Surgical Approach a. Two Stage Hepatectomy b. Two-stage Partition and Hepatectomy (ALPPS) c. Vascular Resection and Reconstruction d. “In situ” Hypothermic Liver Perfusion
5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015
• Objective – Increase FLR Volume and Function
• In order to Avoid PHLF – Incidence: Low. 10%-20%. Associated 65% mortality – Depends on Remnant Liver
– Volume. » FLR/ sFLR Ratio > 20%
– Function. Affected by » Age » Chemotherapy » Fibrosis » Infection
Portal Vein Embolization…

5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015
• Evaluating Liver Volume • Measured Total Liver Volume
– Calculated Liver Volumetry (CT o MR) • Estimated Liver Volume
– Based on Relation between Liver Size and BSA – Based on Relation between Liver Size and Body weight
(LR/BW ratio)
• Future Liver Remnant (FLR) – Expressed as a ratio of the Total Liver Volume
Avoiding PHLF…
Ribero D et al. Ann Surg 258:801-807, 2013

5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015 Portal Vein Embolization…

5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015
• Importance of Preoperative Liver Volumetry
Portal Vein Emnbolization…
FLR and… A. PHLF B. PHLF and Death

5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015
• Importance of a Healthy Liver
Portal Vein Embolization…
• Chemotherapy. Side effects. • Oxaliplatin-based
– Sinusoidal Dilatation – Vascular Congestion – Presinusoidal fibrosis – Venous occlusion
• Irinotecan based – Steatohepatitis
Vauthey JN et al. J Clin Ocol 2006:24;2065 Reddy SK et al. J Am Col Surg 2008:206;96 Karoui M et al. Ann Surg 2006:243;1-7

5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015
….and does not increase overall survival or disease free survival
Scoggins CR et al. Ann Surg Oncol 2009:16;35-41
Preoperative Chemotherapy and Short and Long Term Outcome
Portal Vein Embolization…
A sFLR >30% should be considered

5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015
Current Criteria Increasing FLR volume
Liver Pathology • Indication for PVE Normal Injured
• FLR/TLV <25% <30% • FLR/BWR <0.5% <0,8%
Portal Vein Embolization…
Scoggins CR et al. Ann Surg Oncol 2009:16;35-41 Shindoh J et al J Am Col Surg 2013:126-134

5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015
Portal Vein Embolization…
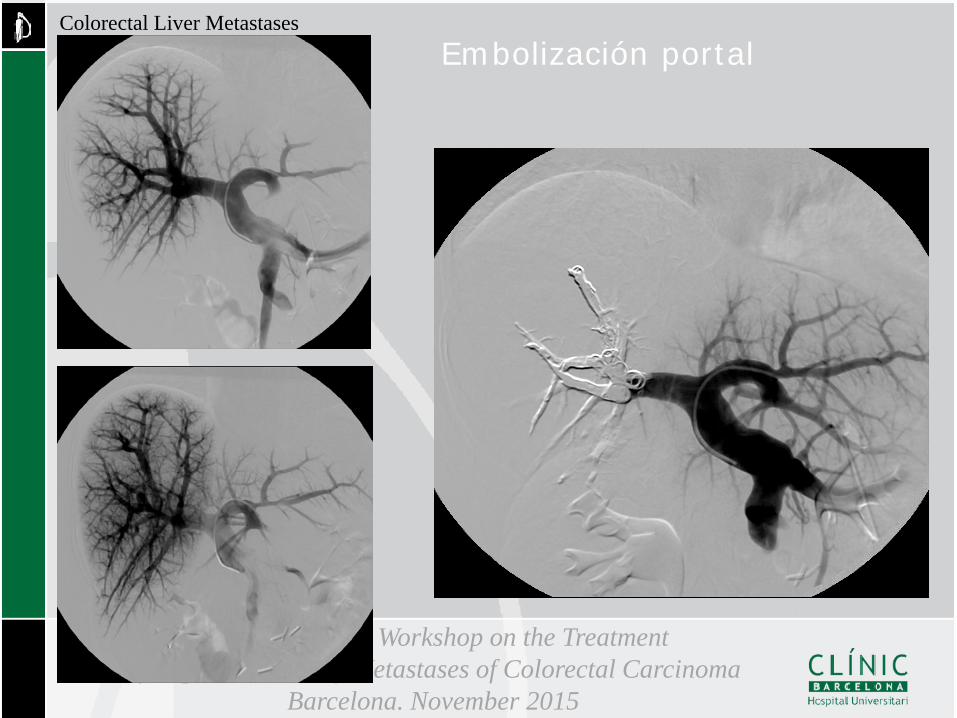
• Portal Vein Embolization • Method
• Great Variability 1. Percutaneous Approach Polivynil Alcohol Trysacryl Microsphere Coils 2. Technique Right Portal Vein (rPVE) rPVE+sIV
5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015 Embolización portal

5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015 Embolización Portal Selectiva

5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015 Imagenes Post embolización Portal

5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015
Volumen preembolización 371,08 cc
Volumen postembolización 559,35 cc

5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015 243,88 ml 387 ml
Incremento del 58,7%

5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015
Shindoh J et al J Am Col Surg 2013:126-134
Study Population

5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015
Shindoh J et al J Am Col Surg 2013:126-134
Portal Vein Embolization…

5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015
Long Term Outcome after rPVE+sIV
Portal Vein Embolization…
Shindoh J et al J Am Col Surg 2013:126-134

5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015
Shindoh J et al J Am Col Surg 2013:126-134

5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015
•Important Messages
•Mortality 5,8% •Morbidity 32,7%
1. Indicated in patients under the age of 60 2. Feasibility of 72% (vs. 95%) 3. Abscence of Stage 1 Morbidity 4. Significant waiting Period. >4 weeks Oncologic Selection (drop out) ALPPS associated to a 20% recurrence at 3 months
Shindoh J et al J Am Col Surg 2013:126-134
5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015
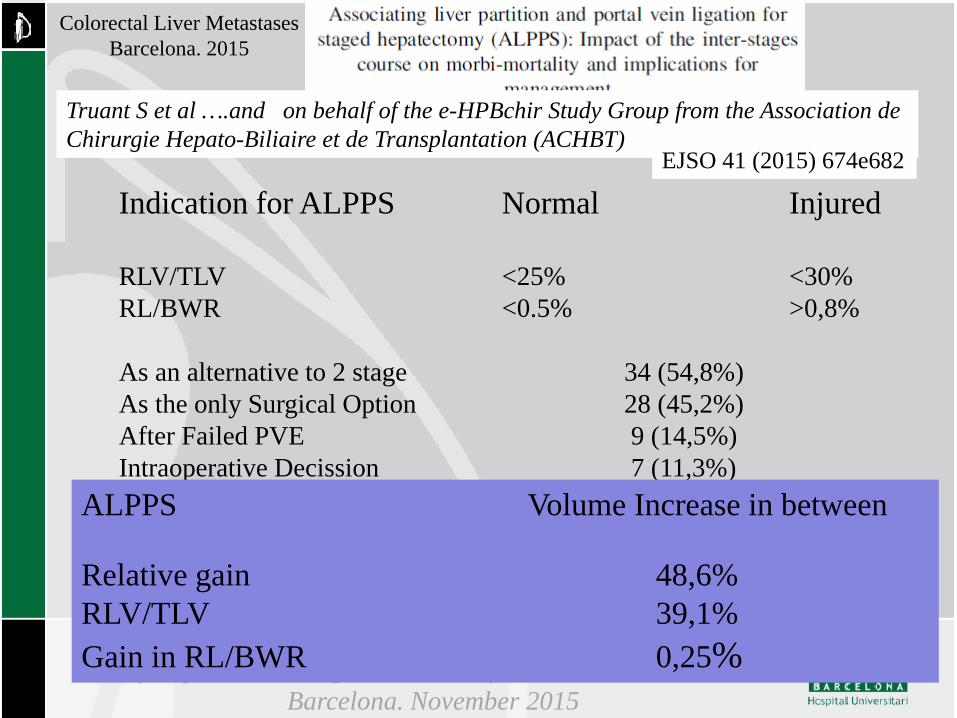
Truant S et al ….and on behalf of the e-HPBchir Study Group from the Association de Chirurgie Hepato-Biliaire et de Transplantation (ACHBT)
EJSO 41 (2015) 674e682
Indication for ALPPS Normal Injured RLV/TLV <25% <30% RL/BWR <0.5% >0,8% As an alternative to 2 stage 34 (54,8%) As the only Surgical Option 28 (45,2%) After Failed PVE 9 (14,5%) Intraoperative Decission 7 (11,3%)
ALPPS Volume Increase in between Relative gain 48,6% RLV/TLV 39,1% Gain in RL/BWR 0,25%

5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015
Truant S et al EJSO 2015, 41:674-682
Portal Vein Embolization…

5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015
•Important Messages
•Mortality 12,9% •Morbidity 40,3%
1. Indicated in patients under the age of 60 2. Feasibility of 95,2% (vs. 66-75%) 3. Stage 1 major morbidity Is a prognostic factor of cumulative mortality 5/14 (35,7%) vs 3/48 (6,3%) 4. Waiting beyond 7 days seems to be useless KGR 33,3 ml/day vs 17,2 ml/day 5. Systematic use of PVE before ALPPS ?
Truant S et al EJSO 2015, 41:674-682
Portal Vein Embolization…
5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015
Failure to achieve a two-stage hepatectomy:
what predictive factors and what practical consequences?
Katsunori Imai1,2,5, Carlos Castro Benitez1,2,4, Marc-Antoine Allard1,2.4, Eric Vibert, 1,3,4, Antonio Sa Cunha1,4, Daniel Cherqui1,4, Denis Castaing1,3,4,
Henri Bismuth, Hideo Baba5, René Adam1,2,4 1Centre Hépato-Biliaire, AP-HP, Hôpital Paul Brousse, Villejuif, France 2Inserm, Unité 776, Villejuif, France 3Inserm Unité 785, Villejuif, France 4Université Paris-Sud, Villejuif, France, Villejuif, France 5Department of Gastroenterological Surgery, Kumamoto University, Japan
Courtesy of Rene Adam
5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015
Between January 2000 and December 2012, 845 patients underwent hepatectomy for colorectal liver metastases at Paul Brousse Hospital.
Among these, 125 patients (14.8%) with initially unresectable multiple and bilobar CRLM were scheduled to perform TSH and were enrolled in this study.
Study population

5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015
AIM 1. Identify the independent factors to predict the
failure to achieve two-stage hepatectomy by multivariate logistic analysis.
2. Based on the multivariate logistic model, the predictive model for failure of two-stage hepatectomy was developed.
3. Optimal cut-off values for continuous data were determined by receiver operating characteristic (ROC) curve analysis.

5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015
median range Age 56.1±9.7 57 31-82 Gender 68/57 Body mass index 24.9±4.5 24 17-40 ASA score (I/II/III) 10/95/20 Timing of liver metastasis (synchronous†/metachronous) 112/13 Site of primary tumor (colon/rectum) 93/32 Primary T stage (1-2/3-4) 17/94 Primary N stage (0/1-2) 27/85 CEA at diagnosis (ng/dL) 1187.2±5696.3 83 0.4-48332 CEA at hepatectomy (ng/dL) 65.0±283.4 8 0.4-2960 Tumor number at diagnosis 10.6±6.9 9 2-35 Tumor number at hepatectomy 10.2±6.1 9 2-33 Largest tumor size at diagnosis (mm) 51.2±31.7 45 10-164 Largest tumor size at hepatectomy (mm) 42.4±24.1 37 12-150 Percentage of FLR volume (%) 29.3±7.9 30 15-53 ICG-R15 value (%) 9.6±6.0 8.4 2-33.6 Concomitant extrahepatic disease 34 (27.2%)
Lung 22 Lymph node 7 Peritoneum 5
Background characteristics

5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015
median range
Chemotherapy before 1st-stage hepatectomy 123 (98.4%)
Chemotherapy cycles 12.3±7.3 11 1-34
Chemotherapy lines 1 1-4
1 83
2 26
≥ 3 14
Chemotherapy regimen
1st line (oxaliplatin/irinotecan/both/other) 79/46/4/4
2nd line (oxaliplatin/irinotecan/both/other) 12/22/4/3
3rd line (oxaliplatin/irinotecan/both/other) 1/6/2/2
Use of biologic agents 82 (66.7%)
Tumor progression during 1st-line chemotherapy 14 (11.5%)
Chemotherapy features

5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015
median range Interval chemotherapy 60 (74.1%) Time interval between 1st- and 2nd-stage (month) 4.0±3.0 3.2 1.1-15.7 Major hepatectomy 75 (92.6%) Type of procedure
anatomical 64 anatomical + limited 16 limited 1
Concomitant use of local ablation therapy 5 (6.2%) radiofrequency ablation 5 cryotherapy 0
Vascular clamping 69 (85.2%) Clamping time 41.6±18.0 43 12-85 Blood loss (g) 1320.9±1375.2 1000 170-6900 Operating time (min) 399.8±104.8 391 190-894 Blood transfusion 41 (50.6%) Number of resected nodule* 7.4±5.4 7 0-26 Resection margin status (R0/R1/Rx**) 35/44/5 In-hospital stay 11.5±6.3 10.5 3-76
Operative features (2nd-stage, n=81)
*including the nodule treated with local ablation therapy **treated with local ablation therapy

5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015
1st-stage (n=125) Major complication (Clavian-Dindo ≥ III) 18 (14.4%)
III/IV/V 14/4/1* fluid collection 7 bile leakage 2 transient liver failure 2 intraabdominal bleeding 1 transient renal failure 1 intraabdominal abscess 1 anastomotic leakage 1 urinary tract obstruction due to infection 1 sepsis 1 acute coronary syndrome 1
90-day mortality 1 (0.8%) 2nd-stage (n=81)
Major complication (Clavian-Dindo ≥ III) 27 (33.3%) III/IV/V 18/9/2** bile leakage 10 fluid collection 5 transient liver failure 6 intraabdominal bleeding 2 catheter infection 1 abdominal wall abscess 1 sepsis 1 transient renal failure 1 fetal liver failure 2
90-day mortality 2 (1.6%)
Complication

5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015
median range
Total number of removed tumor* 9.0±7.4 7 0-32
Size of largest tumor removed 35.9±23.7 30 0-130
Resection margin status (R0/R1 or Rx**/R2) 13/68/44
90-day mortality 3 (2.4%)
Total results of two-stage hepatectomy (n=125)
*including the nodule treated with local ablation therapy **treated with local ablation therapy
5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015
100
0
80
60
40
20
0 1 2 3 5 4 6 7 8 9
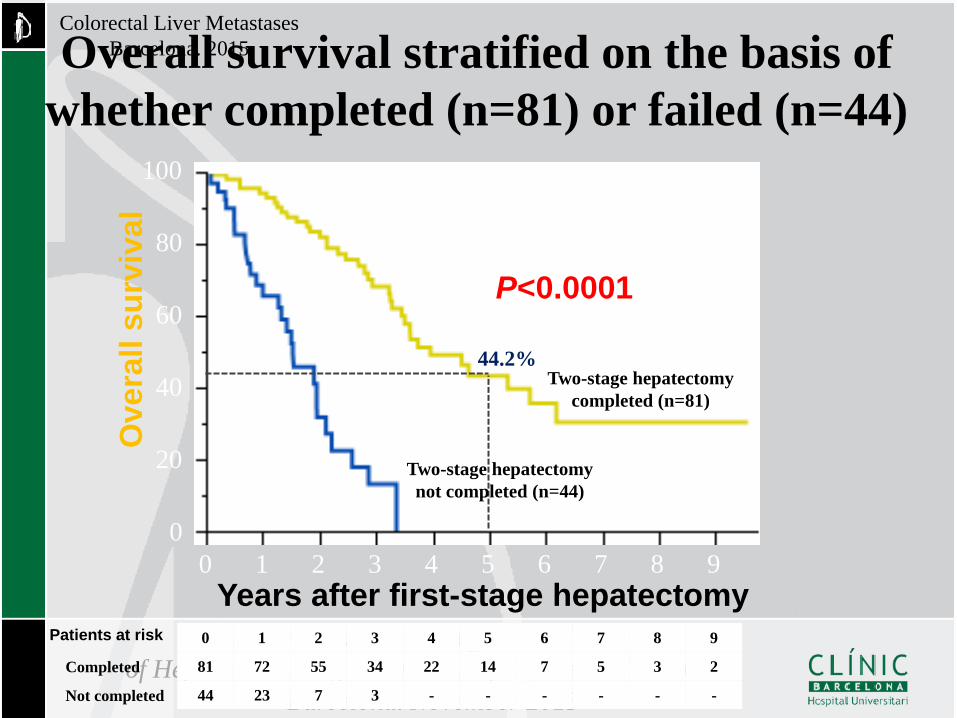
Overall survival stratified on the basis of whether completed (n=81) or failed (n=44)
Years after first-stage hepatectomy
Ove
rall
surv
ival
0 1 2 3 4 5 6 7 8 9
81 72 55 34 22 14 7 5 3 2
44 23 7 3 - - - - - -
Patients at risk
P<0.0001
44.2% Two-stage hepatectomy
completed (n=81)
Two-stage hepatectomy not completed (n=44)
Completed
Not completed
5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015
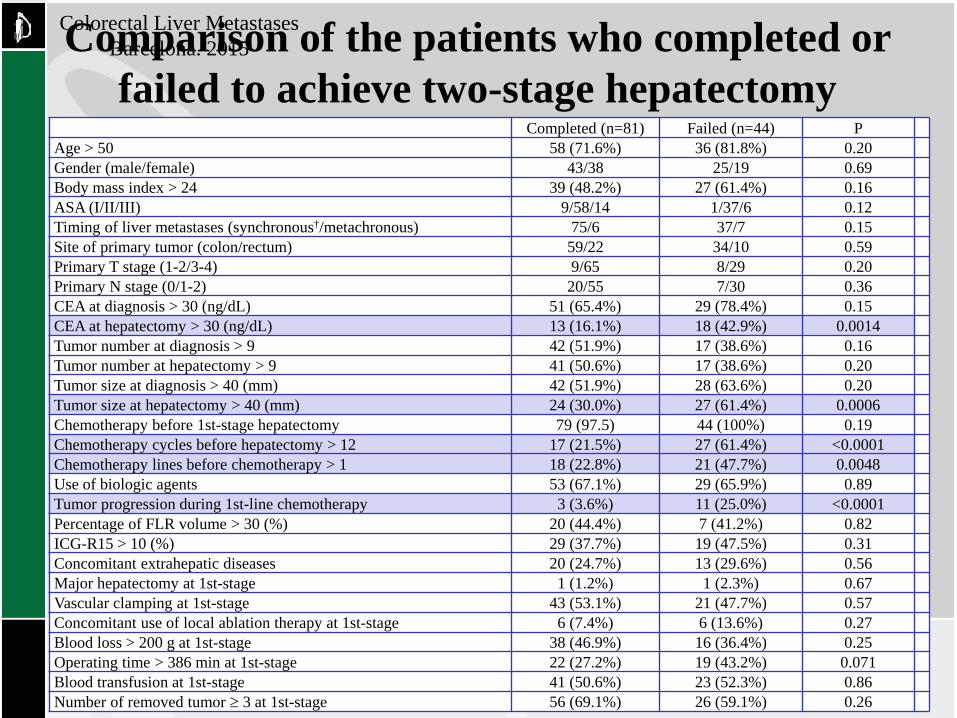
Completed (n=81) Failed (n=44) P Age > 50 58 (71.6%) 36 (81.8%) 0.20 Gender (male/female) 43/38 25/19 0.69 Body mass index > 24 39 (48.2%) 27 (61.4%) 0.16 ASA (I/II/III) 9/58/14 1/37/6 0.12 Timing of liver metastases (synchronous†/metachronous) 75/6 37/7 0.15 Site of primary tumor (colon/rectum) 59/22 34/10 0.59 Primary T stage (1-2/3-4) 9/65 8/29 0.20 Primary N stage (0/1-2) 20/55 7/30 0.36 CEA at diagnosis > 30 (ng/dL) 51 (65.4%) 29 (78.4%) 0.15 CEA at hepatectomy > 30 (ng/dL) 13 (16.1%) 18 (42.9%) 0.0014 Tumor number at diagnosis > 9 42 (51.9%) 17 (38.6%) 0.16 Tumor number at hepatectomy > 9 41 (50.6%) 17 (38.6%) 0.20 Tumor size at diagnosis > 40 (mm) 42 (51.9%) 28 (63.6%) 0.20 Tumor size at hepatectomy > 40 (mm) 24 (30.0%) 27 (61.4%) 0.0006 Chemotherapy before 1st-stage hepatectomy 79 (97.5) 44 (100%) 0.19 Chemotherapy cycles before hepatectomy > 12 17 (21.5%) 27 (61.4%) <0.0001 Chemotherapy lines before chemotherapy > 1 18 (22.8%) 21 (47.7%) 0.0048 Use of biologic agents 53 (67.1%) 29 (65.9%) 0.89 Tumor progression during 1st-line chemotherapy 3 (3.6%) 11 (25.0%) <0.0001 Percentage of FLR volume > 30 (%) 20 (44.4%) 7 (41.2%) 0.82 ICG-R15 > 10 (%) 29 (37.7%) 19 (47.5%) 0.31 Concomitant extrahepatic diseases 20 (24.7%) 13 (29.6%) 0.56 Major hepatectomy at 1st-stage 1 (1.2%) 1 (2.3%) 0.67 Vascular clamping at 1st-stage 43 (53.1%) 21 (47.7%) 0.57 Concomitant use of local ablation therapy at 1st-stage 6 (7.4%) 6 (13.6%) 0.27 Blood loss > 200 g at 1st-stage 38 (46.9%) 16 (36.4%) 0.25 Operating time > 386 min at 1st-stage 22 (27.2%) 19 (43.2%) 0.071 Blood transfusion at 1st-stage 41 (50.6%) 23 (52.3%) 0.86 Number of removed tumor ≥ 3 at 1st-stage 56 (69.1%) 26 (59.1%) 0.26
Comparison of the patients who completed or failed to achieve two-stage hepatectomy

5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015
RR 95%CI P
CEA at hepatectomy > 30 (ng/dL) 2.73 1.08-7.05 0.034
Tumor size at hepatectomy > 40 (mm) 2.89 1.07-7.97 0.036
Chemotherapy cycles before hepatectomy > 12 3.46 1.35-9.05 0.0098
Tumor progression during 1st-line chemotherapy 6.56 1.53-35.63 0.01
Multivariate logistic regression analysis of predictive factors for failure of two-stage
hepatectomy
*Cut-off values were determined by ROC analysis
5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015
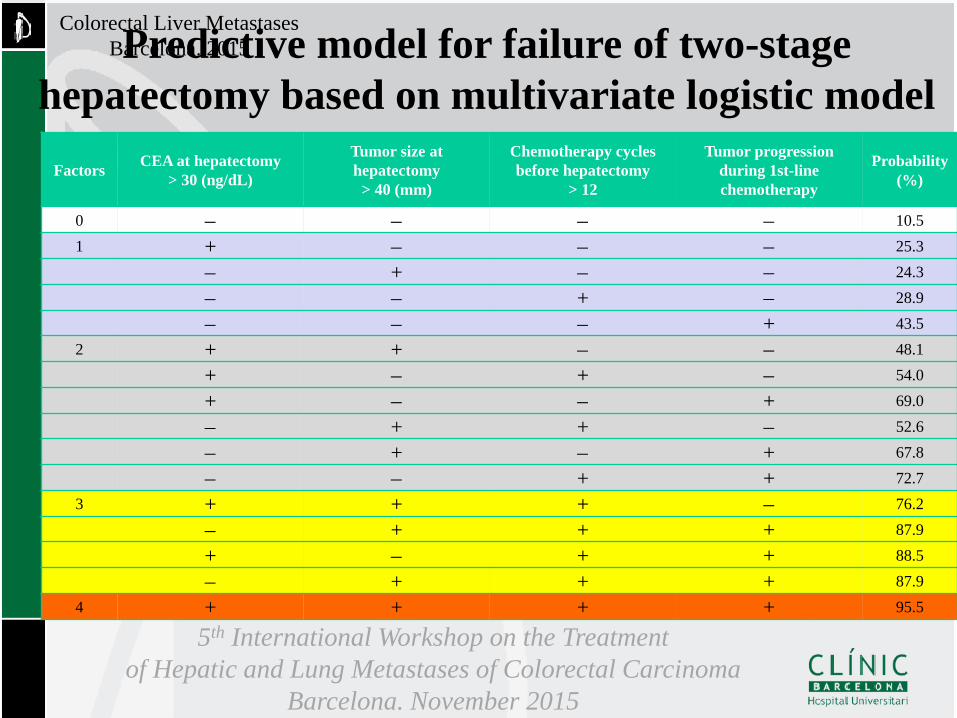
Factors CEA at hepatectomy > 30 (ng/dL)
Tumor size at hepatectomy
> 40 (mm)
Chemotherapy cycles before hepatectomy
> 12
Tumor progression during 1st-line chemotherapy
Probability (%)
0 − − − − 10.5 1 + − − − 25.3
− + − − 24.3 − − + − 28.9
− − − + 43.5 2 + + − − 48.1
+ − + − 54.0 + − − + 69.0 − + + − 52.6
− + − + 67.8 − − + + 72.7 3 + + + − 76.2 − + + + 87.9 + − + + 88.5 − + + + 87.9 4 + + + + 95.5
Predictive model for failure of two-stage hepatectomy based on multivariate logistic model

5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015 Receiver operating characteristic (ROC) curve of the proposed predictive model
Sens
itivi
ty
1-specificity
1.0
0
0.8
0.2
0.6
0.4
1.0 0 0.8 0.2 0.6 0.4
The c-index: 0.81
5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015
Years after first-stage hepatectomy
Ove
rall
surv
ival
Years after first-stage hepatectomy
0
100
20
80
60
40
Ove
rall
surv
ival
0 1 9 2 3 4 5 6 7 8
0 1 2 3 4 5 6 7 8 9
44 36 27 17 11 8 2 2 1 1
31 27 19 8 5 2 2 - - -
30 21 12 8 5 3 3 3 2 1
11 5 2 1 - - - - - -
4 2 - - - - - - - -
Patients at risk
0
100
20
80
60
40
0 1 9 2 3 4 5 6 7 8
0 1 2 3 4 5 6 7 8 9
105 84 58 33 21 13 7 5 3 2
15 7 2 1 - - - - - -
Patients at risk Score
0-2
3-4
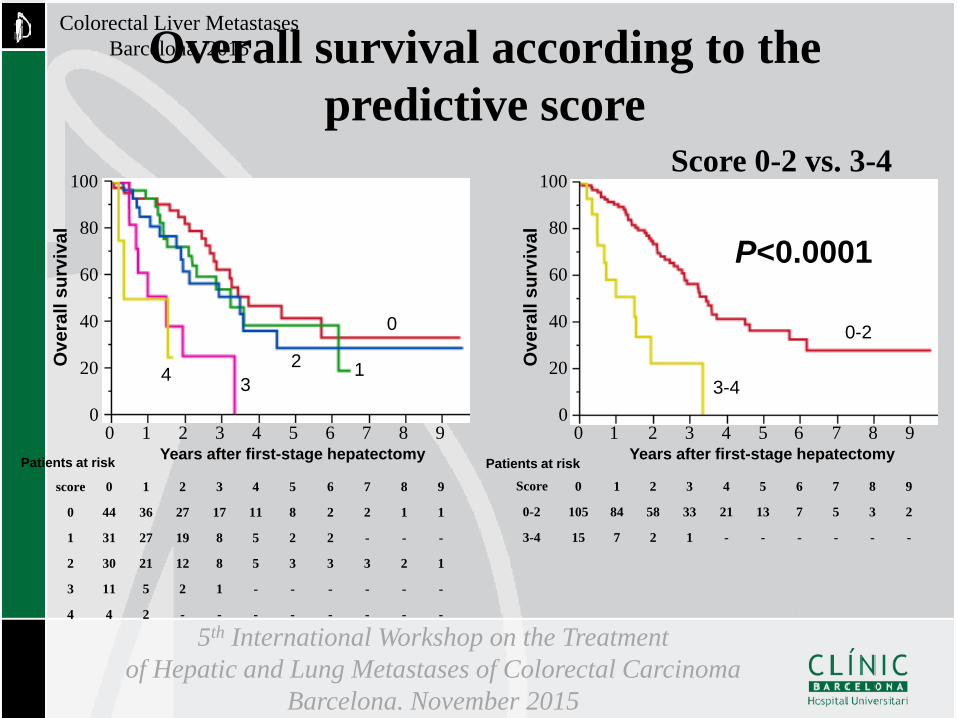
P<0.0001
0
1 2 3
0-2
3-4
Overall survival according to the predictive score
score
0
1
2
3
4
4
Score 0-2 vs. 3-4

5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015
Proposed predictive model by CEA, tumor size, preoperative chemotherapy cycles, and response to chemotherapy contribute to the selection of appropriate patients who expected to benefit from the strategy of two-stage hepatectomy
Patients with ≥ 3 factors should be contraindicated because of their higher failure rate.
Avoidance of these risk factors significantly reduces the risk of drop-out and is crucial for the long-term survival.
Conclusions

5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015 Resumen
• La Embolización de la Vena Porta – Capaz de mejorar el índice de resecabilidad aumentando el tamaño
de Volumen Hepático Residual (72%). – La capacidad de estimulación está condicionada por la Edad,
Fibrosis, Quimioterapia, Infección… – Se asocia a una Morbididad (33%)y Mortalidad (5%) razonable – La presencia de CEA elevado, Tamaño tumoral por encima de 4
cm, Ausencia de Respuesta a la QT, y el empleo de mas de 12 ciclos, son factores de mal pronóstico
– Es necesario un seguimiento a largo plazo para conocer las verdaderas consecuencias de tratamiento médico-quirúrgico.

5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015

5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015

5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015 Impact for expanding criteria for resectability…
Factores asociados •Edad superior a 70 años •Patología asociada •Quimioterapia Previa •Afectación hepática extensa •Tumores > 3 cm •Transfusión sanguinea* •Isquemia hepática alargada
Mortalidad: 0-6% Morbididad:22-45%
De Haas RJ et al Ann Surg 2011:253;1069

5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015
Laurent C et al Br J Surg 2003;90:1131
Impact for expanding criteria for resectability…
Supervivencia 3 años 5 años Global 53% 36% Sin Complicaciones 61% 43% ConComplicacines 21% 12% 0.001
Mortalidad: 3% Morbididad:30%

5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015
De Haas RJ et al Ann Surg 2011;253:1069
Impact for expanding criteria for resectability…
Supervivencia 3 años 5 años Sin Complicaciones 66% 52% Con Complicacines 60% 42% 0.001
Mortalidad: 1.3% Morbididad: 33%

5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015
• “A priori” –HEALTHY LIVER…
Definition of Resectability….

5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015
• Chemotherapy. Side effects. • Oxaliplatin-based
– Sinusoidal Dilatation – Vascular Congestion – Presinusoidal fibrosis – Venous occlusion
• Irinotecan based – Steatohepatitis
Definition of Resectability….
Vauthey JN et al. J Clin Ocol 2006:24;2065 Reddy SK et al. J Am Col Surg 2008:206;96 Karoui M et al. Ann Surg 2006:243;1-7
5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015 Chemotherapy Side effects. Postoperative Liver Faiulure

5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015
• Diagnóstico. Enfermedad Hepática Metástasica • Planteamiento quirúrgico. Hepatectomía
derecha reglada • Intervención. Hepatectomía
– Pérdidas de 375 ml. sin Exclusión Vascular – Protocolo: Somatostatina.
• Bolus. 250-500 µg en bolus • 250 µg/hora durante 7 dias
• Curso Postoperatorio – Insuficiencia hepática postoperatoria
Definition of Resectability….
5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015
• Curso Postoperatorio • Dias 1 a 3. Buen estado general • Dias 4 a 10. Deterioro Porogresivo
– Encefalopatía. – Alteración de la función.
• Bi. 10 mg y T.Protrombina. 20%
• Colocación del MARS – Cuatro sesiones
• A partir de entonces mejoría progresiva
Definition of Resectability….

5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015
Chemotherapy Side effects. Postoperative liver Faiulure

5th International Workshop on the Treatment of Hepatic and Lung Metastases of Colorectal Carcinoma
Barcelona. November 2015
Colorectal Liver Metastases Barcelona. 2015 Estrategia Terapéutica….
• In the context of the metastatic disease – Loco/Regional Recurrence – Concomitant Metastases
• Any Patient – In whom all disease can be remove with a
negative margin* – Who has a remnant hepatic volume/reserve
* De Haas RJ et al Ann Surg 248:626-637, 2008