polypoid adenosquamous carcinosarcoma of the epiglottis ... · polypoid adenosquamous...
TRANSCRIPT

ANNALS O F CLINICAL AND LABORATORY SCIEN CE, Vol. 21, No. 6Copyright © 1991, Institu te for C linical Science, Inc.
Polypoid Adenosquamous Carcinosarcoma of the Epiglottis with Blastomatous Features*
DOUGLAS H. MCGREGOR, M D ,t SAING H. LEE, M D tt and M ICHAEL F. MCMAHON, MD§"
Laboratory Servicet and Surgical Serviced Department o f Veterans Affairs Medical Center,
Kansas City, MO 64128 and
Department o f Pathology and Oncology and Department o f Otorhinolaryngology,
University o f Kansas Medical Center, Kansas City, KS 64128
ABSTRACT
A case is reported of polypoid adenosquamous carcinosarcoma with blastomatous features arising in the epiglottis. A 69-year-old man with hoarseness and sore throat was found to have a six cm pedunculated mass located on the epiglottis. Upon examination by light microscopy, it was found that the tumor was composed of not only well to poorly differentiated in situ and invasive squamous cell carcinoma but also adenocarcinoma with blastomatous features and a malignant primitive stroma, with features of undifferentiated sarcoma and focal chondrosarcomatous differentiation. To the best of our knowledge, this appears to be the second case of laryngeal adenosquam ous carcinosarcoma with blastomatous features reported in the English literature and the third case in the world literature.
Introduction
Squamous cell carcinoma is by far the most common malignant neoplasm occurring in the larynx. A denocarcinom a is much more infrequent; adenosquamous carcinoma and sarcoma of the larynx are rare, and carcinosarcom a is extrem ely
* A ddress re p rin t req u ests to: D . H . M cG regor,M .D ., L aboratory Service, V eterans Affairs M edical C enter, 4801 L inw ood B oulevard , Kansas City, M O 64128.
t D eceased .§ P re se n t address: 9301 W aterford D rive , C ollege
S tation, TX 77840.
rare, with the epithelial com ponent virtually lim ite d to squam ous ce ll carci- noma.2,6’12 The following report docum e n ts a c a s e o f a d e n o s q u a m o u s carcinosarcoma of the epiglottis, which apparently is the second report of such a laryngeal neoplasm in the English literature5 and the third report in the world literature.9 Blastomatous features, comparable to the rare pulmonary blastoma, were also present in the two American cases and probably in the Russian case.
Case ReportA 69-year-old w h ite m ale was ad m itted w ith com
plain ts o f a sore th ro at for ten w eeks, a “m uffled ho t
4130091-7370/91/1100-0413 $01.20 © Institute for Clinical Science, Inc.

414 MCGREGOR, LEE, AND MCMAHON
potato” vo ice ch an g e for six m onths, difficulty sw allow ing, a n d 14 p o u n d s w e ig h t loss in six w eeks. In d ire c t laryngoscopy rev ea led a large exophytic m ass o f th e ep ig lo ttis . E p ig lo ttic b io p sy d em o n stra ted invasive poorly d iffe ren tia ted squam ous cell carcinom a. T otal laryngectom y w as perform ed. T h e p a tie n t su b seq u en tly d e v e lo p ed b ila te ra l cervical tum or recu rren ce , b u t ad d itio n al surgery was no t perfo rm ed . H e w as trea te d w ith rad ia tion an d chem o th erap y an d d ied six m onths follow ing his surgery. A utopsy p e rm iss io n w as n o t ob tained .
T h e laryngectom y sp ec im en (figure 1) m easu red 7 x 6.5 cm in overall d im ensions. A ttached to th e left m ucosal surface o f th e ep ig lo ttis was a p e d u n cu la ted 6 x 5.5 x 3 cm m ass. T h e ex ternal surface of th is m ass was sligh tly nodular, granular, an d yel- low -brow n, an d th e c u t surface was hom ogeneous, soft, a n d tan . T ru e a n d fa lse cords w ere grossly unrem arkab le .
M icroscopically , th e p o ly p o id ep ig lo ttic tum or d em o n stra ted various h isto log ical patte rns and cell types. Squam ous cell carcinom a, w e ll to poorly diffe ren tia ted , w as seen to arise from th e m ucosa (figu res 2 a n d 3) an d to in v ad e to th e u n d e rly in g e p iglo ttic cartilage. M erg ing a n d in te rm in g led w ith th is invasive squam ous cell carcinom a w ere areas o f n eo p lastic g landular, b lastem atous and m esen ch y m al p ro life ra tio n (figures 4 to 8). T h e g landu lar co m p o n en t w as com posed o f cells w ith sligh t to m o d e r a te n u c le a r h y p e rc h ro m a s ia , m o d e ra te n u c lea r vesicu larity , focal p ro m in en t nucleo li, and rare to m o d era te n u m b ers o f m ito tic figures. T he b lastem atous co m p o n en t (figures 4 to 6) m erg ed an d focally m in g led w ith th e g landu lar com ponent. I t w as co m p o sed o f p lu m p sp in d le -sh ap ed cells w ith vary ing d eg rees o f nu c lear a typia and rare to m o d era te n u m b ers o f m ito tic figures. T h ese b lastem atous areas focally m erg ed w ith a m ore sarco- m atous-appearing m esenchym al com ponent, com p o sed o f cells variab ly a rranged in d isorgan ized , p a ra lle l an d storiform p a tte rn s (figure 7), and rare foci c o n s is te n t w ith ch o n d ro cy tic d iffe ren tia tio n (figure 8) w e re p resen t.
S n o o k ’s re tic u lu m -s ta in e d se c tio n s (figu re 6) dem o n s tra ted re ticu lin fibers su rro u n d in g alm ost all ce lls in th e areas o f b lastem atous and neoplastic m esenchym al p ro life ra tion and a v irtual absence of re ticu lin in th e areas o f squam ous cell carcinom a a n d ad en o carc in o m a. M u cica rm in e an d p e rio d ic acid S ch iff (PAS) sta in after d iastase d igestion dem on stra ted only ra re foci o f in tracytoplasm ic m ucin in th e a d e n o c a rc in o m a to u s a rea s . T h e PAS s ta in sh o w ed sm all am ounts o f d iastase-sensitive m aterial co n sis ten t w ith g lycogen in th e cytoplasm of som e squam ous an d g lan d u la r tum or cells. M asson- trich rom e sta in d em o n stra ted very sm all am ounts o f co llagen d ep o sitio n in th e neop lastic m esenchym al areas, b u t m uscle cells w ere no t id en tified . Bodian sta in w as n eg ative for ne rv e fibers.
Sections s ta in ed for im m unoperox idase-labe led p an k era tin an d ep ith e lia l m em b ran e an tig en dem on stra ted positiv ity in th e cytoplasm o f th e squam ous c e ll c a rc in o m a , th e in te n s i ty o f re ac tio n d im in ish in g w ith d ecreas in g d ifferen tia tion o f the tum or cells. Som e areas o f p lu m p sp in d le cells, difficu lt to d is tin g u ish b e tw e e n poorly d ifferen tia ted
squam ous cell carcinom a, b lastem a, an d sarcom a, focally h a d fa in tly p ositive an tik e ra tin reac tions. T h e m ore d e fin ite b lastem atous an d m esenchym al n eop lastic areas com posed o f m ore e lo n g a ted sp in d le cells w ith in d iv id u a l cell re ticu lum w ere cons isten tly negative for keratin an d ep ith e lia l m em b ran e an tig en an d positive for v im entin .
E lec tro n m icro sco p ic stu d ies , on fo rm alin -fixed tis su e post-fixed in g lu tara ldehyde, in c lu d e d cells com patib le w ith each o f th e th ree cell ty p es se e n b y lig h t m icroscopy; how ever, u ltrastructu ra l eva lu a t io n w as h in d e r e d b y a u to ly t ic d e g e n e r a t iv e changes. Sufficient m orphologic d e ta il w as re ta in e d in th e n eop lastic m esenchym al areas to d e te rm in e collagen fiber d eposition paralle l to and contiguous w ith th e cytoplasm ic m em brane o f th ese cells.
Discussion
The laryngeal neoplasm reported here is h igh ly unusual in its m orphology. Grossly, it had a prom inent polypoid configuration. Histologically, the tumor was composed of epithelial and mesenchymal components. The epithelial com ponent included well to poorly differentiated in situ and invasive squamous cell carcinoma, and also adenocarcinom a w ith blastomatous features. The mesenchymal com ponen t co n sis ted of a m alignan t p r im it iv e s tro m a , w ith fe a tu re s o f undifferentiated sarcoma and focal chon- d ro sarcom atous d iffe re n tia tio n . T he interm ingling of the non-mucinous adenocarcinom a and the prim itive strom a gave a b las to m a to u s a p p e a ra n c e to the neoplasm.
A diagnosis of laryngeal sarcoma or carcinosarcoma requires considerable caution and should only be made after care- fu l e x c lu s io n o f p u r e e p i t h e l i a l malignancy. This is because of the now w ell-recogn ized laryngeal neoplasm s often referred to as pseudosarcom a.2’12 This variant of squamous cell carcinoma generally takes two forms: carcinom a w ith an a typ ica l b u t n o n -n eo p la s tic stroma, and carcinoma with focal non- mesenchymal spindle cell features. The non-epithelial nature of the mesenchy- m al-appearing areas in the present case w as s u p p o r te d by th e p r e v io u s ly described positive reticulum stain, negative im m unoperoxidase stains for pan-

POLYPOID ADENO SQ UAM O US CARCINOSARCOMA O F TH E EPIGLOTTIS 415
FIGURE 1. Gross ap p earance o f th e laryngectom y specim en; th e p e d u n cu la ted epiglo ttic m ass has b een b isected .
F i g u r e 2 . Squam ous cell carcinom a in situ (on left), w hich focally involved th e surface o f th e p e d u n cu la ted ep ig lo ttic m ass, w ith subm ucosal chronic inflam m ation and fibrosis (on right). (H em atoxylin and eosin stain x l 2 5 ) .
F i g u r e 3. Invasive squam ous cell carcinom a, w hich was a com ponent o f th e tum or focally seen to arise from th e m ucosal in s itu carcinom a. (H em atoxylin and eosin stain X313.
F i g u r e 4 . N eoplastic g landu lar p ro liferation (adenocarcinom a) w ith in te rsp ersed neop lastic strom a (blastem a), m erg ing w ith a sarcom atous proliferation in u p p e r one th ird o f th e figure. (H em atoxylin and eosin stain x50).

FIGURE 5. N eoplastic g lands (adenocarcinom a) w ith neop lastic strom a com posed of p lum p sp in d le cells (blastem a). (H em atoxylin and eosin stain, x 3 1 3 ) .
F i g u r e 6. A rea o f th e tum or com parab le to figure 5, dem onstra ting re ticu lin fibers su rround ing m ost o f th e b lastem atous cells b u t no t the cells o f th e g landular com ponent at th e bottom of th e figure. (W eigert re ticu lum stain, X 3 1 3 ).
FIGURE 7. Sarcom atous area o f the tum or com posed of p lum p to e longated sp ind le cells arranged in d isorganized, p a ralle l an d storiform patterns. (H em atoxylin and eosin stain, x 125).
FIGURE 8. C hondrocy tic d ifferen tia tion focally p re sen t in sarcom atous areas o f the tum or. (H em atoxylin and eosin stain , x 125).
MCGREGOR, LEE, A N D MCMAHON
POLYPOID A D EN O SQ U A M O U S CARCINOSARCOMA O F T H E EPIGLOTTIS 417keratin and ep ithe lia l m em brane an tigen, positive im m unoperoxidase stain fo r v im e n tin , a n d e le c tr o n m ic ro scopic findings.
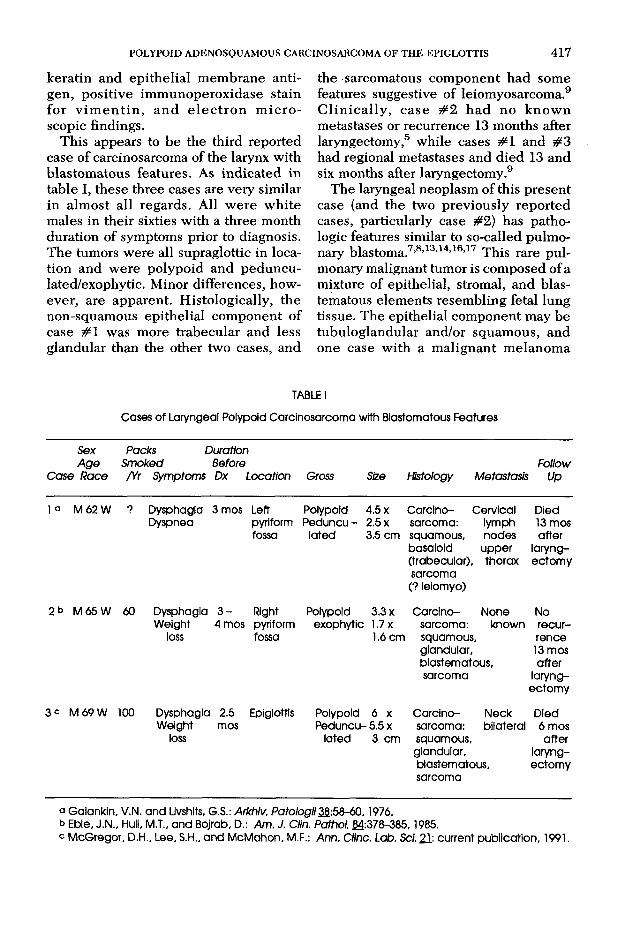
This appears to be the third reported case of carcinosarcoma of the larynx with blastom atous features. As ind ica ted in table I, these three cases are very similar in alm ost all regards. All w ere w hite males in their sixties w ith a three month duration of symptoms prior to diagnosis. The tumors were all supraglottic in location and w ere polypoid and pedunculated/exophytic. M inor differences, however, are apparent. H istologically, the non-squam ous epithelial com ponent of case # 1 was more trabecular and less glandular than the other two cases, and
the sarcomatous com ponent had some features suggestive of leiomyosarcoma.9 C lin ic a lly , case # 2 h a d no k n o w n métastasés or recurrence 13 months after laryngectomy,5 while cases # 1 and # 3 had regional métastasés and d ied 13 and six months after laryngectomy.9
The laryngeal neoplasm of this present case (and the two previously reported cases, particularly case #2) has pathologic features similar to so-called pulm onary blastoma.7’8’13,14,16’17 This rare pulmonary malignant tum or is com posed of a mixture of epithelial, stromal, and blas- tematous elem ents resem bling fetal lung tissue. The epithelial com ponent may be tubuloglandular and/or squam ous, and one case w ith a m alignant m elanom a
TABLE ICases of Laryngeal Polypoid Carcinosarcoma with Blastomatous Features
Sex Packs DurattonAge Smoked Before Follow
Case Race /Yr Symptoms Dx Location Gross Size Histology Metastasis Up
1a M 62 W ? Dysphagia 3 mos Left Polypoid 4.5 x Carclno- Cervical DiedDyspnea pyriform Peduncu- 2.5 x sarcoma: lymph 13 mos
fossa lated 3.5 cm squamous, nodes afterbasalold upper laryng- (trabecular), thorax ectomy sarcoma (? leiomyo)
2b M 65 W 60 Dysphagia 3 - Right Polypoid 3.3 x Carcino- None NoWeight 4 mos pyriform exophytic 1.7 x sarcoma: known recur
loss fossa 1.6 cm squamous. renceglandular. 13 mosblast ematous. aftersarcoma laryng
ectomy3 c M 69 W 100 Dysphagia 2.5 Epiglottis Polypoid 6 x Carcino- Neck Died
Weight mos Peduncu- 5.5 x sarcoma: bilateral 6 mosloss lated 3 cm squamous. after
glandular. laryngblastematous. ectomysarcoma
a Galankin, V.N. and Livshits. G.S.: Arkhiv. Patologii¿2:58-60,1976.b Eble, J.N., Hull, M.T., and Bojrab, D.: Am. J. Clin. Pathol. 24:378-385,1985.c McGregor, D.H., Lee, S.H., and McMahon, M.F.: Ann. Cline. Lab. Sci. 21: current publication, 1991.

418 MCGREGOR, LEE, AND MCMAHON
com ponent has been reported.4 The stromal com ponent may be undifferentiated, c a r t i la g in o u s , m y o g e n o u s 10 a n d /o r osseous. The blastem atous com ponent, the characteristic feature o f this neoplasm , consists of a prim itive m esenchyme, which focally may show a transition to the d ifferen tia ted strom al and occasionally epithelial components. The em bryological derivation of th is neo plasm is presently uncertain. I t does not represent a teratocarcinoma, since these contain organoid structures and no blastem atous com ponent.11 It may best be considered a form of carcinosarcoma,16 although some reports of immunohisto- chemical studies suggest rather a bipha- sic tum or.1,3 W hether or not it is derived from tw o germ layers, ec toderm and endoderm , or from a pluripotential cell that gives rise to epithelial and m esenchymal elem ents, however, is debatable.
Regardless of the derivation of these rare pulm onary m alignant neoplasm s, their similarity to the present (and two p re v io u s ly rep o rted ) la ry n g e a l n e o plasm s is clearly evident. Com parable extrapulm onary presentation has been p rev iously rep o rted in the nasopharynx.15 Furtherm ore, this occurrence of similar neoplasms in these two areas is not surprising, in view of the common embryologie origin of the lungs, bronchi and larynx-the ventral wall groove in the branchial arch region of the foregut.
In summ ary, this unusual neoplasm appears to be the third reported case of la ry n g ea l adenosquam ous carc inom a with blastomatous features, a tum or with pathologic features sim ilar to pulm onary blastoma.
A ck n o w led g m en ts
T h e au tho rs g ratefu lly acknow ledge: rev iew o f h isto log ical sections by Jo h n G. Batsakis, M D , M .D. A nderson H ospita l and T um or In s titu te , an d V inc e n t J. H yam s, M D an d D en n is K. H effner, M D, A rm ed F o rces In s titu te o f Pathology; transla tion of
r e f e r e n c e 9 b y G e o rg e M e ln y k o v y c h , P h D , R esearch S erv ice , K ansas C ity V e te ran s A ffairs M edical C en te r; tech n ica l assistance b y th e H isto logy S ec tion , L ab ora to ry S erv ice , K ansas C ity V eterans Affairs M edical C e n te r; a n d secre ta ria l assistance by Joyce C apps.
References
1. A d d i s , B. J. and C o r r i n , B.: Pu lm onary b lastom a, carcinosarcom a an d sp in d le -c e ll carc inom a: A n im m unoh istochem ical s tudy o f keratin in te rm ed ia te filam ents. J. Pathol. 147:291 - 301, 1985.
2. B a t s a k i s , J. G .: Tum ors o f th e H ead a n d N eck. C lin ica l a n d P athological C onsidera tions, 2nd ed ition . B altim ore, W illiam s a n d W ilkins, 1979, pp . 89, 206, 217-219.
3. B e r e a n , K., T r u o n g , L. D ., D u d l e y , A. W., e t al.: Im m u noh istochem ica l ch aracte rizatio n o f p u lm o n a ry b la s to m a . A m . J. C lin . P a th o l. 89:773-777, 1988.
4 . C o h e n , R . E ., W e a v e r , M . G ., M o n t e n e g r o ,H . D ., e t al.: Pu lm onary b lastom a w ith m align an t m elanom a com ponent. Arch. Patho l. Lab. M e d . 114:1076-1078, 1990.
5. E b l e , J. N., H u l l , M . T ., a n d B o j r a b , D .: L aryngeal b lastom a. A lig h t an d e lec tro n m icroscopic study o f a novel en tity analogous to p u lm onary b lastom a. Am. J. C lin . Pathol. 84:3 7 8 - 385, 1985.
6. F e r l i t o , A.: H istological classification o f larynx an d hypopharynx cancers an d th e ir clinical im plications. Pathologic aspects o f 2052 m align an t neoplasm s d iag n o sed a t th e O R L D ep artm en t o f P adua U niversity from 1966 to 1976. Acta O to-laryngol. Suppl. 342:1—88, 1976.
7. F r a n c i s , D. an d Ja c o b s e n , M .: Pu lm o n ary b lastom a. C urr. Top. Pathol. 73:256-294, 1983.
8. F u n g , C. H., L o , J. W., YONAN, T. N., e t al.: Pu lm onary b lastom a. An u ltrastructu ra l study w ith a b r ie f rev iew o f lite ra tu re an d a d iscu ssion o f pa thogenesis. C ancer 39 :153-163 ,1977 .
9. G a l a n k in , V. N. and L i v s h i t s , G . S.: C arcinosarcom a o f th e larynx. Arkhiv. Pato logii 3 8 :5 8 - 60, 1976.
10. H e c k m a n , C . J., T r u o n g , L. D ., C a g l e , P. T ., e t al.: Pu lm onary b lastom a w ith rhabdom yo- sarcom atous d ifferen tia tion : An e lec tro n m icroscopic an d im m unohistochem ical study. Am. J. Surg. Pathol. 12:35-40, 1988.
11. H e f f n e r , D. K. an d H y a m s , V. J.: Teratocarci- nosarcom a (m alignant teratom a?) o f th e nasal cavity and paranasal s inuses. A c lin icopatho- logic study o f 20 cases. C an cer 53:2140-2154,1984.
12. H y a m s , V. J., B a t s a k i s , J. G . an d M i c h a e l s , L .: Tum ors o f th e U pper R esp ira tory T ract and

PO LYPOID ADEN O SQ U A M O U S CARCINOSARCOMA O F TH E EPIGLOTTIS 419E ar, A tlas o f T u m o r Pathology, Second Series, F a c ic le 25. W ash ing ton , D .C . A rm ed Forces In s titu te o f Pathology, 1988, pp . 76-82.
13. M c C a n n , M . P., F u , Y.-S. a n d Ka y , S.: Pu lm onary blastom a. A l ig h t an d e lec tro n m icroscopic study. C an cer 38 :789-797 , 1976.
14. M e d b e r y , C ., B i b r o , M . C., P h a r e s , J. C ., e t al.: P u lm onary b lastom a. C ase rep o rt an d lite ra tu re rev iew o f ch em o th erap y experience . C anc e r 53 :2413-2416, 1984.
15. M e i n e c k e , R., B a u e r , F ., S k o u r a s , J., e t al.: B lastom atous tum ors o f th e resp ira to ry tract. C ancer 38 :818-823, 1976.
16. R o t h , J. A. an d E l g u e z a b a l , A.: Pu lm onary b lastom a evo lv ing in to carcinosarcom a. A case study. Am. J. Surg. Pathol. 2 :407-413 , 1978.
17. V a l d e r r a m a , E ., S a l u j a , G., S h e n d e , A., e t al.: Pu lm onary b lastom a. R eport o f tw o cases in ch ild ren . Am. J. Surg. Pathol. 2 :415-422 , 1978.