polymer-based oral peptide nanomedicinescampus.usal.es/~magalan/pics/articulos/herrero et al ther...
TRANSCRIPT

657ISSN 2041-5990Therapeutic Delivery (2012) 3(5), 657–66810.4155/TDE.12.40 © 2012 Future Science Ltd
Review
Peptides and proteins have been used as biopharmaceuticals since the discovery of insulin in 1922, mainly due to their high activity, specificity and effectiveness compared with more conventional drugs [1,2]. The increasing evidence of the therapeutic potential of these macromolecules has led not only to the production of these compounds in large quantities, but has also attracted the interest of the scientific community [3]. In fact, the development of peptide therapeutics represent a steadily growing market strategy, with 51 compounds approved by 2010, while 132 candidates were in clinical development, of which 15 were in Phase III [4]. As a general tendency, peptide candidates for metabolic disorders such as diabetes, obesity and osteoporosis that are prevalent in a sedentary, aging population are likely to enter the development pipeline in increasing numbers [5].
Unfortunately, due to their instability and restricted permeability, most of these marketed peptides have to be administered parenterally in current medical practice. This modality of administration has several important drawbacks such as pain upon injection, short halflives in bloodstream, which makes repeated administration and high doses necessary, low patient compliance, sterility requirements and high cost of operation. Therefore, alternative ways of administration are currently being explored such as pulmonary, nasal, buccal, rectal, ocular, vaginal, transdermal and, in particular, the oral route, which is generally recognized to be the most convenient modality of administration [3]. Indeed, oral delivery is potentially cost effective, has the highest patient compliance and could overall contribute to great advances in classical
therapies, leading to new methods of treatment and diagnosis of important diseases [6]. As an additional advantage, the oral route is also the ideal way for delivering certain peptides [7] as it mimics physiological pathways by which they may reach their site of action. For example, oral insulin absorption by the portal vein would directly lead insulin to the target organs, thus reducing adverse systemic effects (see ‘Nanotechnology approaches for oral insulin delivery: a case study’, below).
Despite all the efforts dedicated so far, the development of a convenient oral formulation for peptides still remains a challenge. As discussed below in further detail, the major obstacle to achieve oral peptide and protein delivery is the highly restrictive nature of the GI tract, which is specialized in degrading such compounds and does not allow their transport across the intestinal mucosa [8,9]. In particular, the extreme pH conditions and high enzymatic activity of the GI tract are critical impediments to oral peptide delivery, leading to conformational changes, inactivation and degradation [10,11]. These processes comprise hydrolytic peptide degradation by peptidases and chemical modifications such as oxidation, phosphorylation or deamidation [10].
Regarding physical and biological barriers, the first and probably most relevant barrier is the mucus overlying the intestinal mucosa. Foreign particles are efficiently retained in the mucus layer by adhesion and/or steric impediment, and then removed by means of physio logical clearance mechanisms.
As a next step, the drug molecules also need to cross the epithelial barrier by means of transcellular or paracellular pathways [12,13]. The
Polymer-based oral peptide nanomedicines
Oral peptide delivery has been one of the major challenges of pharmaceutical sciences as it could lead to a great improvement of classical therapies, such as insulin, alongside making an important number of new therapies feasible. Successful oral delivery needs to fulfill two key tasks: to protect the macromolecules from degradation in the GI tract and to shuttle them across the intestinal epithelium in a safe and efficient fashion. Over the last decade, there have been numerous approaches based on the chemical modification of peptides and on the use of permeation enhancers, enzyme inhibitors and drug-delivery systems. Among the approaches developed to overcome these restrictions, the design of nanocarriers seems to be a particularly promising approach. This article is an overview on the state of the art of oral-peptide formulation strategies, with special attention to insulin delivery and the use of polymeric nanocarriers as delivery systems.
Edgar P Herrero1, Maria Jose Alonso1,2 & Noemi Csaba*1,2
1Department of Pharmacy & Pharmaceutical Technology, School of Pharmacy, Campus Vida, University of Santiago de Compostela, 15782 Santiago de Compostela, Spain 2Center for Research in Molecular Medicine & Chronic Diseases, Av. Barcelona s/n, Campus Vida, University of Santiago de Compostela, 15707 Santiago de Compostela, Spain *Author for correspondence: Tel.: +34 881815252 Fax: +34 981547148 E-mail: [email protected]
For reprint orders, please contact [email protected]

Review | Herrero, Alonso & Csaba
Therapeutic Delivery (2012) 3(5)658 future science group
intestinal epithelium also comprises a small proportion of mucosaassociated lymphoid tissue (i.e., Peyer’s patches), which allowa the uptake of material via the M cells and thereby the transport to the lymphatics and into the systemic circulation. Mcell mediated transport has been widely investigated for drug delivery due to the high transcytotic capacity of these cells for particulated materials [14–16]. Since this uptake mechanism is mediated by lymphatic tissues, it has been considered particularly interesting for the oral delivery of antigenic proteins or peptides for vaccination. Several clinical trials have already been conducted on this approach; however, to our knowledge; there is still no clear evidence on the effectiveness of this route for immunization [201].
Strategies & alternatives to improve oral peptide deliveryCurrently, only a couple of peptides such as cyclosporin A (a hydrophobic peptide) and desmopressin (for which a very low bioavailability is required and has a relatively low production cost) can be administered orally. There have been a great number of pharmaceutical strategies to develop effective oral peptide formulations, including coadministration of enzyme inhibitors, permeation enhancers and/or chemical modification of peptides.
� Permeation enhancers & enzyme inhibitorsPermeation enhancers make mucosal surfaces more permeable by temporally disrupting the physical barriers by means of increasing membrane fluidity, decreasing mucus viscosity and/or opening tight junctions [17]. However, they may not only produce the transport of the desired drug, but also the absorption of potentially toxic molecules. As a consequence, they can induce undesirable side effects and epithelial damage, which is a general concern to their implementation. Nevertheless, there are several reports in the literature indicating the possibility of increasing permeability in a reversible fashion without permanent damage to the epithelia. For instance, macro molecular enhancers, such as chitosan, increase drug transport without important toxic side effects. Recently, melittin and, in particular, its derivates with modified amino acid sequence have also shown promising and reversible permeation enhancer characteristics in both paracellular and transcellular pathways with limited cytotoxicity [18,19]. Another current potential
strategy for increasing epithelial uptake and permeation throughout the intestinal mucosa is the co administration of the cellpenetrating peptides (CPPs) [20,21].
On the other hand, enzyme inhibitors attempt to avoid the degradation of the peptide in the GI tract. The coadministration of enzyme inhibitors with peptides has shown limited success; however, the combination of enzyme inhibitors and permeation enhancers improve the intestinal absorption of peptides [8]. Nevertheless, the use of enzyme inhibitors in longterm therapy has side effects such as the interruption of the digestion of some nutritive proteins, intestinal mucosal damage and the stimulation of protease secretion due to feedback regulation.
� Chemical modificationsPeptides can be chemically modified by the addition of functional groups or by the conjugation to macromolecular entities for improving their absorption across the GI tract without producing serious side effects [22]. The use of the salt form of peptides or the covalent attachment of hydrophilic polymers to peptides can increase solubility and paracellular transport. Polyethylene glycol (PEG) and N(2hydroxypropyl) methacrylamide are attractive hydrophilic polymers to formulate polymer–drug conjugates. Similarly, hydrophobic lipids can be attached to peptides to enhance their trans cellular uptake. Several fatty acids, such as palmitic, butyric, lauric or caprylic acid, have been used to modify peptides, such as desmopressin [23], leucine enkephalin analogue [24] and insulin [25], showing longer plasma halflife, enhanced permeability and better resistance to enzymatic degradation. Other possibility of covalent attachment is to conjugate the peptide to small molecules (cellmembrane transporters or receptors) that trigger endocytosis [17,26,27]. The major drawback of these methodologies is the risk of diminishing the biological activity of the peptide as a consequence of the chemical modification [28].
� Nanoparticulate drug-delivery carriersA promising tool to achieve oral delivery of peptides, protecting them from degradation and enhancing their transport across epithelium, is the immobilization of these macromolecules into drugdelivery carriers. Among the great number of different strategies, the design of particulated nanocarriers has been positioned recently as an especially promising approach. In fact, scientific articles describing nanosystems represent over
Key Terms
Insulin: The most investigated peptide in oral delivery, responsible for regulating carbohydrate metabolism in the body.
Nanotechnology: Within the context of this article, it is the manipulation of biomaterials for the development of functional nanoscale drug-delivery systems.
Chitosan: Natural mucoadhesive biopolymer, widely used in mucosal drug-delivery strategies.
Intestinal absorption: Critical step to oral drug delivery, the process by which substances cross the intestinal barrier and reach blood circulation.
Mucoadhesive: Property of certain biomaterials to adhere to the mucus layer and thereby facilitate the interaction of drug delivery systems with the intestinal barrier.

Polymer-based oral peptide nanomedicines | Review
www.future-science.com 659future science group
35% of all publications related to oral peptide delivery over the last 5 years [202], indicating the growing interest generated in this field. The reason behind this interest is that the submicron size of the nanocarriers and their large specific surface area significantly improves their interaction with the intestinal mucosa, as compared with larger carriers [29,30]. The possible ways of these carrier interactions are illustrated on FiguRe 1.
Nanometric carriers include polymeric nanosystems (mostly nanoparticles and nano capsules) and lipidic systems (nano/microemulsions and selfnanoemulsifying systems). The present review is primarily focused on the application of polymeric biomaterials in the design of nanosystems for oral peptide delivery; however, compositions based on polymercoated lipid nanostructures are also disclosed where relevant (i.e., nanocapsules and surfacemodified solid lipid nanoparticles).
A long list of polymers has been used to generate the nanocarrier structures mentioned above (Table 1). Examples of synthetic polymers relevant for oral delivery include: polyesters (e.g., poly[lactic acid] [PLA]) [31–33], poly[lacticcoglycolic acid] [PLGA] [31,34–39], and poly[ecaprolactone] [40,41]), poly(methyl methacrylates) [42–44], poly(alkyl cyanoacrylates) [45–50] and polyanhydrides [34], which provide adjustable controlled drugrelease profiles from days to weeks. Nanocarriers based on synthetic polymers can be generated by diverse techniques such as nanoprecipitation, solvent evaporation, freeze–drying or spray drying of emulsions and supercritical fluid technology [51–58].
Natural polymers are abundant in nature and relatively inexpensive compared with synthetic polymers and normally offer quicker drugrelease profile [59]. In addition, the generation of nanocarriers with these natural polymers can be usually performed by using mild methods such as ionic gelation, complexation or co acervation with an excellent capacity of peptide association [31,60–62]. Albumin, agar, pectins, cyclodextrins, gelatine, alginate, collagen, dextran and chitosan, and its derivatives, have been extensively investigated in scientific literature for oral peptide delivery [60,61,63–96] (Table 1). Nevertheless, besides these positive characteristics, it is also important to keep in mind that polymers from natural sources may present homogeneity and purity problems, which in general require careful quality assessment.
The appropriate selection and combination of the biomaterials used for the preparation of these systems permit the modulation of their
physicochemical properties, such as hydrophobicity, surface charge and drugrelease profiles. Depending on their composition, these sub cellular size carriers can also provide biodegradable and biocompatible properties, as well as controlled release. Moreover, the use of bioadhesive/mucoadhesive materials can significantly improve the performance of the carriers, allowing prolonged interaction of the delivery system with the mucosal barrier and, hence, increasing the time available for penetration across the mucosal epithelia (see FiguRe 1 for possible carrier interactions) [77,80]. Synthetic polymers such as polyacrylates, cellulose derivatives and natural polymers such as alginate or chitosan derivatives are relevant examples of polymers that have been applied as components for mucoadhesive particles.
An alternative approach for enhancing the interaction of the nanocarriers with the intestinal barrier–carrier penetration is their surface modification with selective ligands that can be recognized by M cells or epithelial cells [51]. Bacterial adhesins, lectins, monoclonal anti bodies and specific amino acid sequences are some examples of such ‘cytoadhesive’ ligands [97].
Intestinal lumen
Particles entrapped
in mucus
Translo
catio
n
Epithelial adhesion
localized delivery
Mucus layerEnterocyte
Figure 1. Possible interactions of nanocarriers with the intestinal barrier.

Review | Herrero, Alonso & Csaba
Therapeutic Delivery (2012) 3(5)660 future science group
Finally, the performance of nanocarriers for oral delivery can also be enhanced by their surface modification with hydrophilic polymers (e.g., PEG and hyaluronic acid). Several studies have shown that the presence of such hydrophilic chains on the surface of the nanocarriers can improve their efficacy by rendering them with enhanced physical and biological stability, and by prolonging the interaction of nanoparticles with the mucosal barrier [32,98].
Nanotechnology approaches for oral insulin delivery: a case studyDiabetes mellitus is a metabolic disease caused by failure of insulin secretion (Type I diabetes) or by insulin resistance combined with reduced
insulin secretion (Type II diabetes), leading to the failure of blood glucose homeostasis and hyperglycemia [99,100]. This disease is the third cause of death in developing countries [101]. It is well known that patients suffering Type I diabetes control their blood glucose levels by means of multiple insulin injections. There are several drawbacks associated to this method (e.g., physiological stress, allergy, pain and lipodystrophy, and risk of hypoglycemia [102]) and, therefore, alternative routes have been widely investigated for improved delivery of insulin [103,104].
As mentioned above, one of the main drawbacks of the current parenteral administration of insulin is that it does not follow the natural dynamics of the insulinrelease profile from the
Table 1. Overview of polymeric nanocarrier compositions for oral peptide delivery.
Polymer System Peptide Ref.
PLA–PEG Nanoparticle Tetanus toxoid [31,32]
PLGA–polyanhydrides Nanoparticle Insulin [34]
PLA–cyclodextrin Nanoparticle BSA [33]
PLGA–HP55 Nanoparticle Insulin [35]
PLGA Nanoparticle Albumin (BSA), insulin and calcitonin
[36–38]
PLGA–chitosan Nanoparticle Tetanus toxoid and calcitonin [31,39]
PCL–eudragit RS Nanoparticle Insulin [40,41]
PCL Nanoparticle Cyclosporine-A [135]
PAA–chitosan–cyclodextrin Nanoparticle Insulin [43]
PMMA–chitosan Nanoparticle Insulin [42,44]
PACA Nanoparticle and nanocapsule
Insulin, calcitonin and octreotide [45–50,136]
Dextran–alginate Nanoparticle Insulin [64,65,72]
Dextran–vitamin B12 Nanoparticle Insulin [66,73]
Dextran–alginate–chitosan Nanoparticle Insulin [74–77]
Dextran–chitosan Nanoparticle Insulin [78,79]
Chitosan Nanoparticle, nanocapsule and SLN
Insulin, calcitonin, BSA, tetanus and diphtheria toxoids and cyclosporine-A
[61,90,91,93–96,137]
Chitosan–alginate Nanoparticle Insulin [80,87]
Chitosan–glucomannan Nanoparticle Insulin [60]
Chitosan–arabic gum Nanoparticle Insulin [92]
Chitosan–cyclodextrin Nanoparticle Glutathione [68,88]
Chitosan–alginate–cyclodextrin
Nanoparticle Insulin [89]
Chitosan–g–PGA Nanoparticle and nanocapsule
Insulin [81–84]
Chitosan–hyaluronic acid Nanoparticle VEGF, PDGF-BB [67]
Chitosan–PASP–PEG Nanoparticle BSA [85]
Chitosan–HPMCP Nanoparticle Insulin [86]
BSA: Bovine serum albumin; HP55: Hypromellose phthalate; HPMCP: Hydroxypropyl methylcellulose phthalate; PAA: Polymethacrylic acid; PACA: Poly(alkylcyanoacrylate; PASP: Poly(l-aspartic acid); PCL: Poly(caprolactone); PEG: Polyethylene glycol; PGA: Polyglycolide; PLA: Poly(lactic acid); PLGA: Poly(lactic-co-glycolic acid); PMMA: Poly(methyl methacrylate); SLN: Solid lipid nanoparticle.
Key Term
Acrylic polymers: Synthetic mucoadhesive polymers, principally used for oral drug delivery.

Polymer-based oral peptide nanomedicines | Review
www.future-science.com 661future science group
pancreas, leading to inappropriate tissue distribution that provides the liver only with a small fraction of the total injected dose [105]. On the contrary, upon oral delivery, absorption by the enterocytes would directly lead insulin to the target organ (liver followed by the pancreas) through the portal vein, which is the natural exposure route for the hormone. This shortened pathway would reduce adverse systemic effects. In addition, early use of an oral insulin formulation in therapy would also be of great benefit for avoiding further diabetic complications and concomitant diseases (e.g., cardiovascular diseases) [102]. Based on this, it is easy to understand that a great portion of the articles and patents related to oral peptide administration refer to insulin (over 90% according to ISI Web of Knowledge) [202].
Enzyme inhibitors, such as sodium cholate, leupeptin or chicken and duck ovomucoid, decrease the degradation of insulin, increasing the available amount of the peptide for absorption [106,107]. However, the use of these substances for long periods of time produces the intestinal absorption of undesired proteins, perturbation of digestion processes and increased protease secretion [108].
Absorption enhancers, such as bile salts, surfactants, trisodium citrates, ethylenediaminetetraacetic acid [109], zonula occludens toxin [110,111], labrasol [112] and 4CNAB [113], and cellpenetrating peptides, such as octaarginine R8 and lpenetratin [20,21,114], have been used to permeate insulin across the epithelium via the paracellular route by modulating tight junctions. Most of these compounds have shown lack of specificity and some may even produce damage of mucosa and cellular membranes [102]; however, the possibility of opening the tight junctions in a reversible fashion without damaging the epithelia is reported in literature. In fact, macro molecular permeation enhancers, such as chitosan, may increase epithelial transport without toxic side effects.
Modification of the chemical structure of insulin, typically by covalent modifications for increasing the permeation across the epithelium and decreasing the enzymatic degradation, is an opportunity to enhance bioavailability without modifying the mucosal membrane [115]. PEGylation of insulin (Biocon Limited) [116] in a Phase III clinical trial, the development of a hexylinsulinmonoconjugate or HIM 2 (Biocon Limited and Nobex Corporation) [115] that reached Phase III clinical trials, and the conjugation of insulin with B12 vitamin [73,117],
are examples of this interesting approach to improve the oral delivery of insulin by chemical conjugation (Table 2).
Regarding the use of nanocarriers, the efforts to develop an oral insulin nanotech delivery system started in the late 1980s with poly(alkylcyano acrylate) nanocapsules, for which a remarkable hypoglycemic effect has been reported [46]. This pioneering work has opened a new field of research and, since then, there have been over 200 articles describing a variety of nano carriers for developing oral forms of insulin and to a minor extent, other antidiabetic peptides. Besides acrylic polymers, other relevant polymeric biomaterials used for the development of the most promising compositions have been polyesters, such as PLGA or poly(caprolactone), and polyanhydrides, polysaccharides (chitosan, dextran and alginate), polyaminoacids (polyglutamic acid and polyaspartic acid), and their combinations and/or derivatives [202]. Some of these carriers also comprise bioadhesivetargeting entities, such as lectins [118,119], hepatintargeting ligands (biotinphosphatidylethanolamine) [120], cellpenetrating peptides [114] or vitamin B12 [66,73]. In addition, PEG, poloxamers or protease inhibitors have also been included in the nanocompositions as protective agents against insulin degradation [121]. In the following section, the most promising nanocarrier compositions will be presented in more detail. In addition to this information, Table 2 also describes a summary of oral insulin formulations currently in clinical trials, highlighting the progress in the way of translation of current oral technologies into clinical development.
Since the first reports of Damgé and Couvreur [46], the use of acrylic polymers for drug nanocarrier preparation has widely extended, evolving towards a series of other promising systems such as polyacrylate nanoparticles (e.g., poly[isobutylacrylate], poly[isobutylcyanoacrylate] and poly[ethylcyanoacrylate]; Table 1) and ‘smart’ polymethacrylate–PEG complexation hydrogels/nanosystems. In the latter case, the carboxylic groups of the methacrylate component enhance the penetration capacity of the system by promoting the opening of tight junctions, while the presence of the PEG chains promote mucosal adhesion and improves protection against protein degradation. Similar systems have also been developed by combining methacrylic copolymers with chitosan [122]. The pHsensitive character of these systems allows
Review | Herrero, Alonso & Csaba
Therapeutic Delivery (2012) 3(5)662 future science group
enhanced protection of insulin at the acidic pH of the stomach, while at higher pH it promotes interaction and transport through the intestinal mucosa, thereby increasing the bioavailability of the associated peptide.
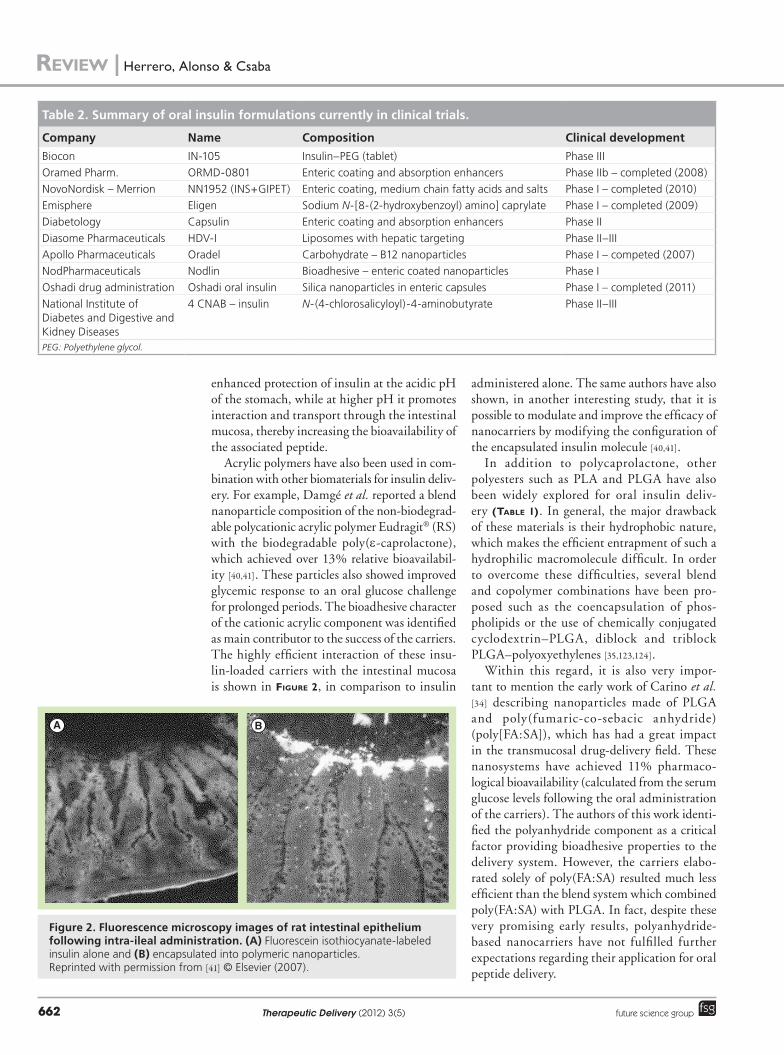
Acrylic polymers have also been used in combination with other biomaterials for insulin delivery. For example, Damgé et al. reported a blend nanoparticle composition of the nonbiodegradable polycationic acrylic polymer Eudragit® (RS) with the biodegradable poly(ecaprolactone), which achieved over 13% relative bioavailability [40,41]. These particles also showed improved glycemic response to an oral glucose challenge for prolonged periods. The bio adhesive character of the cationic acrylic component was identified as main contributor to the success of the carriers. The highly efficient interaction of these insulinloaded carriers with the intestinal mucosa is shown in FiguRe 2, in comparison to insulin
administered alone. The same authors have also shown, in another interesting study, that it is possible to modulate and improve the efficacy of nanocarriers by modifying the configuration of the encapsulated insulin molecule [40,41].
In addition to polycaprolactone, other polyesters such as PLA and PLGA have also been widely explored for oral insulin delivery (Table 1). In general, the major drawback of these materials is their hydrophobic nature, which makes the efficient entrapment of such a hydrophilic macromolecule difficult. In order to overcome these difficulties, several blend and copolymer combinations have been proposed such as the co encapsulation of phospholipids or the use of chemically conjugated cyclodextrin–PLGA, diblock and triblock PLGA–polyoxyethylenes [35,123,124].
Within this regard, it is also very important to mention the early work of Carino et al. [34] describing nanoparticles made of PLGA and poly(fumariccosebacic anhydride) (poly[FA:SA]), which has had a great impact in the transmucosal drugdelivery field. These nanosystems have achieved 11% pharmacological bioavailability (calculated from the serum glucose levels following the oral administration of the carriers). The authors of this work identified the polyanhydride component as a critical factor providing bioadhesive properties to the delivery system. However, the carriers elaborated solely of poly(FA:SA) resulted much less efficient than the blend system which combined poly(FA:SA) with PLGA. In fact, despite these very promising early results, polyanhydridebased nanocarriers have not fulfilled further expectations regarding their application for oral peptide delivery.
Table 2. Summary of oral insulin formulations currently in clinical trials.
Company Name Composition Clinical development
Biocon IN-105 Insulin–PEG (tablet) Phase IIIOramed Pharm. ORMD-0801 Enteric coating and absorption enhancers Phase IIb – completed (2008)NovoNordisk – Merrion NN1952 (INS+GIPET) Enteric coating, medium chain fatty acids and salts Phase I – completed (2010)Emisphere Eligen Sodium N-[8-(2-hydroxybenzoyl) amino] caprylate Phase I – completed (2009)Diabetology Capsulin Enteric coating and absorption enhancers Phase IIDiasome Pharmaceuticals HDV-I Liposomes with hepatic targeting Phase II–IIIApollo Pharmaceuticals Oradel Carbohydrate – B12 nanoparticles Phase I – competed (2007)NodPharmaceuticals Nodlin Bioadhesive – enteric coated nanoparticles Phase IOshadi drug administration Oshadi oral insulin Silica nanoparticles in enteric capsules Phase I – completed (2011)National Institute of Diabetes and Digestive and Kidney Diseases
4 CNAB – insulin N-(4-chlorosalicyloyl)-4-aminobutyrate Phase II–III
PEG: Polyethylene glycol.
A B
Figure 2. Fluorescence microscopy images of rat intestinal epithelium following intra-ileal administration. (A) Fluorescein isothiocyanate-labeled insulin alone and (B) encapsulated into polymeric nanoparticles.Reprinted with permission from [41] © Elsevier (2007).
Polymer-based oral peptide nanomedicines | Review
www.future-science.com 663future science group
The use of polysaccharides represents another important strategy for oral insulin delivery. In fact, chitosan and its derivatives have been one of the most investigated biomaterials in oral delivery. This cationic polysaccharide is mucoadhesive, has pHsensitive properties and penetration enhancer capacity by opening epithelial tight junctions. Nevertheless, as indicated by comparing the in vivo performance of chitosan in solution and as nanoparticles, these attractive properties are not resulting in efficient peptide delivery unless formulated into a nanostructured delivery system [125]. Most of the chitosanbased nanocarriers are prepared by the ionic gelation technique, which allows highly eff icient entrapment of hydrophilic macromolecules. This mild and easy technology, first described by Calvo et al. in 1997, has been attracting great interest over the last few years [61]. Currently, there are more than 100 reports related to the development of such ionically crosslinked nanosystems composed of chitosan and/or other polysaccharides for oral delivery of peptides [126–128]. Most promising recent developments include: composite chitosan–glucomannan, chitosan–dextran and chitosan–alginate nanoparticles [60,80,87] and those based on novel chitosan derivatives such as thiolated chitosans [69–71,129–131] or lauryl succinyl chitosan [132].
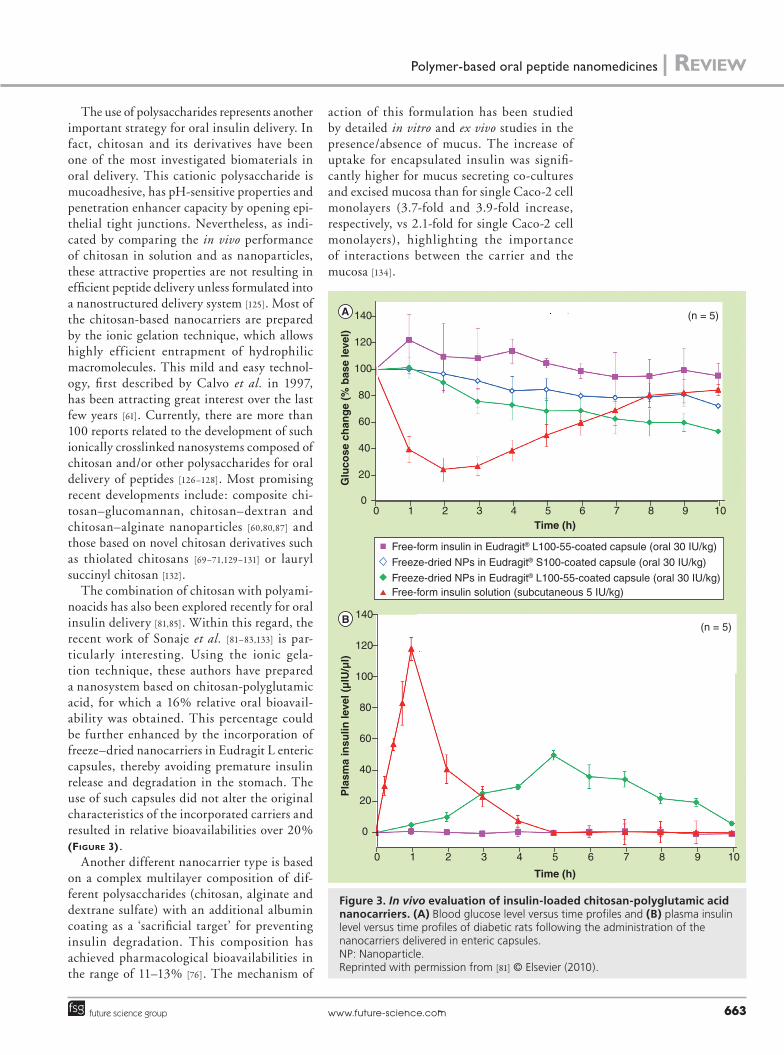
The combination of chitosan with polyaminoacids has also been explored recently for oral insulin delivery [81,85]. Within this regard, the recent work of Sonaje et al. [81–83,133] is particularly interesting. Using the ionic gelation technique, these authors have prepared a nanosystem based on chitosanpolyglutamic acid, for which a 16% relative oral bioavailability was obtained. This percentage could be further enhanced by the incorporation of freeze–dried nanocarriers in Eudragit L enteric capsules, thereby avoiding premature insulin release and degradation in the stomach. The use of such capsules did not alter the original characteristics of the incorporated carriers and resulted in relative bioavailabilities over 20% (FiguRe 3).
Another different nanocarrier type is based on a complex multilayer composition of different polysaccharides (chitosan, alginate and dextrane sulfate) with an additional albumin coating as a ‘sacrificial target’ for preventing insulin degradation. This composition has achieved pharmacological bio availabilities in the range of 11–13% [76]. The mechanism of
action of this formulation has been studied by detailed in vitro and ex vivo studies in the presence/absence of mucus. The increase of uptake for encapsulated insulin was significantly higher for mucus secreting cocultures and excised mucosa than for single Caco2 cell monolayers (3.7fold and 3.9fold increase, respectively, vs 2.1fold for single Caco2 cell monolayers), highlighting the importance of interactions between the carrier and the mucosa [134].
Free-form insulin in Eudragit® L100-55-coated capsule (oral 30 IU/kg)
Free-form insulin solution (subcutaneous 5 IU/kg)
Freeze-dried NPs in Eudragit® S100-coated capsule (oral 30 IU/kg)
Freeze-dried NPs in Eudragit® L100-55-coated capsule (oral 30 IU/kg)
6 7 8 9 10Time (h)
Time (h)
Glu
cose
ch
ang
e (%
bas
e le
vel)
140
120
100
80
60
40
20
00 1 2 3 4 5
6 7 8 9 10
(n = 5)
Pla
sma
insu
lin le
vel (
µlU
/µl)
140
120
100
80
60
40
20
0
0 1 2 3 4 5
A
B
(n = 5)
Figure 3. In vivo evaluation of insulin-loaded chitosan-polyglutamic acid nanocarriers. (A) Blood glucose level versus time profiles and (B) plasma insulin level versus time profiles of diabetic rats following the administration of the nanocarriers delivered in enteric capsules. NP: Nanoparticle. Reprinted with permission from [81] © Elsevier (2010).

Review | Herrero, Alonso & Csaba
Therapeutic Delivery (2012) 3(5)664 future science group
Future perspective & conclusionOverall, there is no doubt that the advances in this field have been significant; however, there remains skepticism of whether these approaches will finally result in a marketed oral insulin product. In fact, despite the number of formulations in clinical trials (Table 2), there has also been a significant number of dropouts. Failure has been associated with high intraindividual variation in insulin absorption at the moderate oral bioavailability levels detected, as well as perceived toxicology issues. This evidence, along with the discovery of new antiobesity, antidiabetes peptides, is currently moving research towards the development of new nanotherapeutic products with a higher chance of success than those attempted to date.
As a consequence of the significant efforts oriented to the design of nanostructures for overcoming critical barriers associated to the oral route of administration, it has become clear that there are a number of interconnected features that need to be taken into account in the design of new nanocarriers:
�Particle size distribution and, thereby, the specific surface area, is a critical parameter in terms of the capacity of nanocarriers to interact with the intestinal mucosa. It is suggested that the upper size limit for this functional ability depends on the nanocarrier composition and shape;
�The stability of the nanostructures in the biological fluids is another determinant factor as it affects size distribution after in vivo administration as well as the premature delivery and/or degradation of the associated active compound;
�Surface chemical composition and, thus, the lipophilicity, fluidity and surface charge may influence the stability of the nanocarrier in the biological environment and also its ability to interact with and be transported across the barrier;
�The internal chemical composition, together with hydrophilicity, rigidity and porosity may influence the stability and delivery rate of the associated peptides;
�The targeting or affinity of the nanocarriers for specific apical membrane receptors may be critical for overcoming biological barriers;
It should be kept in mind that these five parameters together may have an impact on the biocompatibility, biodegradability and potential immune responses of the nanostructures.
It has also become clear that there is still a need to generate and integrate more knowledge for the proper design of oral nanocarriers. In particular, it would be critical to understand in detail the interaction of nanomaterials with the intestinal mucosa, at the cell and tissue levels, as well as their biodistribution, kinetics and toxicological–immuno logical responses in order to advance towards making oral peptide delivery a reality.
Taken as a whole, research and development of peptidebased therapeutics is a dynamic field of research, with increasing numbers of candidates entering clinical studies in a wide variety of therapeutic categories. There is no doubt that pharmaceutical and biotechnology industries will continue to focus on these versatile molecules in association with the development of new formulation and delivery technologies.
Financial & competing interests disclosureThe authors acknowledge financial support from the EC FP7 project TRANS-INT (Ref. 281035) from the Xunta de Galicia and from the Competitive Reference Groups/FEDER Funds (Ref. 2010/18). The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materi-als discussed in the manuscript apart from those disclosed. No writing assistance was utilized in the production of this manuscript.
Executive summary
General aspects of oral peptide delivery
� Critical barriers to oral peptide administration and main delivery strategies are discussed.Evolution of polymeric nanocarriers illustrated through the example of insulin
� Milestones in the development of polymeric oral nanocarriers: a historical overview.
� Recent polymer-based strategies for the oral delivery of insulin reviewed.Analysis of critical factors affecting the efficacy of oral nanocarriers
� Current standpoint of oral peptide delivery technologies are discussed.
� Future trends and perspectives are discussed.

Polymer-based oral peptide nanomedicines | Review
www.future-science.com 665future science group
References1 Walsh G. Biopharmaceutical benchmarks
2006. Nat. Biotechnol. 24(7), 769–776 (2006).
2 JohnsonLeger C, Power CA, Shomade G, Shaw JP, El Proudfoot EI. Protein therapeutics – lessons learned and a view of the future. Exp. Opin. Biol. Ther. 6(1), 1–7 (2006).
3 Degim IT, Celebi N. Controlled delivery of peptides and proteins. Curr. Pharm. Des. 13(1), 99–117 (2007).
4 Reichert J. Development trends for peptide therapeutics: a comprehensive quantitative analysis of peptide therapeutics in clinical development. In: Peptide Therapeutics Foundation. Peptide Therapeutics Foundation, Macmillan Publishers, London, UK (2010).
5 Adessi C, Soto C. Converting a peptide into a drug: strategies to improve stability and bioavailability. Curr. Med. Chem. 9(9), 963–978 (2002).
6 Shaji J, Patole V. Protein and peptide drug delivery: oral approaches. Ind. J. Pharm. Sci. 70(3), 269–277 (2008).
7 Hoffman A, Ziv E. Pharmacokinetic considerations of new insulin formulations and routes of administration. Clin. Pharm. 33(4), 285–301 (1997).
8 BernkopSchnurch A, Walker G. Multifunctional matrices for oral peptide delivery. Crit. Rev. Ther. Drug Carr. Syst. 18(5), 459–501 (2001).
9 Gabor F, Bogner E, Weissenboeck A, Wirth M. The lectincell interaction and its implications to intestinal lectinmediated drug delivery. Adv. Drug Deliv. Rev. 56(4), 459–480 (2004).
10 Lee VHL, Traver RD, Taub ME. Enzymatic barriers to peptide and protein drug delivery. In: Peptide and Protein Drug Delivery. Lee VHL (Ed.). Marcel Dekker Inc., NY, USA (1991).
11 Woodley JF. Enzymatic barriers for GI peptide and protein delivery. Crit. Rev. Ther. Drug Carr. Syst. 11(2–3), 61–95 (1994).
12 Salama NN, Eddington ND, Fasano A. Tight junction modulation and its relationship to drug delivery. Adv. Drug Deliv. Rev. 58(1), 15–28 (2006).
13 Ward PD, Tippin TK, Thakker DR. Enhancing paracellular permeability by modulating epithelial tight junctions. Pharm. Sci. Technol. Today 3(10), 346–358 (2000).
14 Borges O, CordeirodaSilva A, Romeijn SG et al. Uptake studies in rat Peyer’s patches, cytotoxicity and release studies of alginate
coated chitosan nanoparticles for mucosal vaccination. J. Control. Release 114(3), 348–358 (2006).
15 Wu ZH, Ping QN, Wei Y, Lai JM. Hypoglycemic efficacy of chitosancoated insulin liposomes after oral administration in mice. Acta Pharm. Sin. 25(7), 966–972 (2004).
16 Adams G, Wang N, Cui Y. Future alternative therapies in a quest to halt aberrations in diabetes mellitus. Biomed. Pharm. 59(6), 296–301 (2005).
17 RubioAliaga I, Daniel H. Mammalian peptide transporters as targets for drug delivery. Trends Pharm. Sci. 23(9), 434–440 (2002).
18 Maher S, Feighery L, Brayden D, McClean SN. Melittin as a permeability enhancer II: in vitro investigations in human mucus secreting intestinal monolayers and rat colonic mucosae. Pharm. Res. 24(7), 1346–1356 (2007).
19 Maher S, Devocelle M, Ryan SA, McClean SN, Brayden DJ. Impact of amino acid replacements on in vitro permeation enhancement and cytotoxicity of the intestinal absorption promoter, melittin. Int. J. Pharm. 387(1–2), 154–160 (2010).
20 Kamei N, Morishita M, Kanayama Y et al. Molecular imaging analysis of intestinal insulin absorption boosted by cellpenetrating peptides by using positron emission tomography. J. Control. Release 146(1), 16–22 (2010).
21 Kamei N, Morishita M, Takayama K. Importance of intermolecular interaction on the improvement of intestinal therapeutic peptide/protein absorption using cellpenetrating peptides. J. Control. Release 136(3), 179–186 (2009).
22 Duncan R. Polymer conjugates as anticancer nanomedicines. Nat. Rev. Cancer 6(9), 688–701 (2006).
23 Kahns AH, Buur A, Bundgaard H. Prodrugs of peptides. Synthesis and evaluation of various esters of desmopressin (dDAVP). Pharm. Res. 10(1), 68–74 (1993).
24 Uchiyama T, Kotani A, Tatsumi H et al. Development of novel lipophilic derivatives of DADLE (leucine enkephalin analogue): intestinal permeability characteristics of DADLE derivatives in rats. Pharm. Res. 17(12), 1461–1467 (2000).
25 Asada H, Douen T, Mizokoshi Y et al. Stability of acyl derivatives of insulin in the small intestine: relative importance of insulin association characteristics in aqueous solution. Pharm. Res. 11(8), 1115–1120 (1994).
26 Swaan PW. Recent advances in intestinal macromolecular drug delivery via receptormediated transport pathways. Pharm. Res. 15(6), 826–834 (1998).
27 Oh DM, Han HK, Amidon GL. Drug transport and targeting. Intestinal transport. Pharm. Biotechnol. 12, 59–88 (1999).
28 Pauletti GM, Gangwar S, Knipp GT et al. Structural requirements for intestinal absorption of peptide drugs. J. Control. Release 41(1–2), 3–17 (1996).
29 Desai MP, Labhasetwar V, Walter E, Levy RJ, Amidon GL. The mechanism of uptake of biodegradable microparticles in Caco2 cells is size dependent. Pharm. Res. 14(11), 1568–1573 (1997).
30 Koziara JM, Lockman PR, Allen DD, Mumper RJ. In situ blood–brain barrier transport of nanoparticles. Pharm. Res. 20(11), 1772–1778 (2003).
31 Vila A, Sanchez A, Tobio M, Calvo P, Alonso MJ. Design of biodegradable particles for protein delivery. J. Control. Release 78(1–3), 15–24 (2002).
32 Tobío M, Sánchez A, Vila A et al. The role of PEG on the stability in digestive fluids and in vivo fate of PEG–PLA nanoparticles following oral administration. Coll. Surf. B Biointerfaces 18(3–4), 315–323 (2000).
33 Gao H, Wang YN, Fan YG, Ma JB. Synthesis of a biodegradable tadpoleshaped polymer via the coupling reaction of polylactide onto mono(6(2aminoethyl)amino6deoxy)cyclodextrin and its properties as the new carrier of protein delivery system. J. Control. Release 107(1), 158–173 (2005).
34 Carino GP, Jacob JS, Mathiowitz E. Nanosphere based oral insulin delivery. J. Control. Release 65(1–2), 261–269 (2000).
35 Cui FD, Tao AJ, Cun DM, Zhang LQ, Shi K. Preparation of insulin loaded PLGA–Hp55 nanoparticles for oral delivery. J. Pharm. Sci. 96(2), 421–427 (2007).
36 Gutierro I, Hernandez RM, Igartua M, Gascon AR, Pedraz JL. Size dependent immune response after subcutaneous, oral and intranasal administration of BSA loaded nanospheres. Vaccine 21(1–2), 67–77 (2002).
37 Satheesh Kumar P, Ramakrishna S, Ram Saini T, Diwan PV. Influence of microencapsulation method and peptide loading on formulation of poly(lactidecoglycolide) insulin nanoparticles. Die Pharmazie Int. J. Pharm. Sci. 61(7), 613–617 (2006).
38 Yoo HS, Park TG. Biodegradable nanoparticles containing protein–fatty acid complexes for oral delivery of salmon calcitonin. J. Pharm. Sci. 93(2), 488–495 (2004).

Review | Herrero, Alonso & Csaba
Therapeutic Delivery (2012) 3(5)666 future science group
39 Kawashima Y, Yamamoto H, Takeuchi H, Kuno Y. Mucoadhesive dllactide/glycolide copolymer nanospheres coated with chitosan to improve oral delivery of elcatonin. Pharm. Dev. Technol. 5(1), 77–85 (2000).
40 Damgé C, Socha M, Ubrich N, Maincent P. Poly(ecaprolactone)/eudragit nanoparticles for oral delivery of aspartinsulin in the treatment of diabetes. J. Pharm. Sci. 99(2), 879–889 (2010).
41 Damgé C, Maincent P, Ubrich N. Oral delivery of insulin associated to polymeric nanoparticles in diabetic rats. J. Control. Release 117(2), 163–170 (2007).
42 Cui F, Qian F, Zhao Z, Yin L, Tang C, Yin C. Preparation, characterization, and oral delivery of insulin loaded carboxylated chitosan grafted poly(methyl methacrylate) nanoparticles. Biomacromolecules 10(5), 1253–1258 (2009).
43 Sajeesh S, Sharma CP. Cyclodextrininsulin complex encapsulated polymethacrylic acid based nanoparticles for oral insulin delivery. Int. J. Pharm. 325(1–2), 147–154 (2006).
44 TorresLugo M, Peppas NA. Preparation and characterization of P(MAAgEG) nanospheres for protein delivery applications. J. Nanopart. Res. 4(1), 73–81 (2002).
45 Vauthier C, Dubernet C, Fattal E, PintoAlphandary H, Couvreur P. Poly(alkylcyanoacrylates) as biodegradable materials for biomedical applications. Adv. Drug Deliv. Rev. 55(4), 519–548 (2003).
46 Damgé C, Couvreur P. A new approach for oral administration of insulin using polyalkylcyanoacrylate nanocapsules as a drug carrier. Diabetes 37(2), 246–251 (1988).
47 Lowe PJ, Temple CS. Calcitonin and Insulin in Isobutylcyanoacrylate Nanocapsules: Protection Against Proteases and Effect on Intestinal Absorption in Rats. Blackwell Publishing Ltd, London, UK, 547–552 (1994).
48 Damgé C, Vonderscher J, Marbach P, Pinget M. Poly(alkyl cyanoacrylate) nanocapsules as a delivery system in the rat for octreotide, a longacting somatostatin analogue. J. Pharm. Pharmacol. 49(10), 949–954 (1997).
49 Graf A, Rades T, Hook SM. Oral insulin delivery using nanoparticles based on microemulsions with different structuretypes: optimisation and in vivo evaluation. Eur. J. Pharm. Sci. 37(1), 53–61 (2009).
50 Mesiha MS, Sidhom MB, Fasipe B. Oral and subcutaneous absorption of insulin poly(isobutylcyanoacrylate) nanoparticles. Int. J. Pharm. 288(2), 289–293 (2005).
51 des Rieux A, Fievez V, Garinot M, Schneider YJ, Preat VR. Nanoparticles as potential oral
delivery systems of proteins and vaccines: a mechanistic approach. J. Control. Release 116(1), 1–27 (2006).
52 Krause HJ, Schwarz A, Rohdewald P. Polylactic acid nanoparticles, a colloidal drug delivery system for lipophilic drugs. Int. J. Pharm. 27(2–3), 145–155 (1985).
53 Fonseca C, Simoes SR, Gaspar RR. Paclitaxelloaded PLGA nanoparticles: preparation, physicochemical characterization and in vitro antitumoral activity. J. Control. Release 83(2), 273–286 (2002).
54 Lemoine D, Preat V. Polymeric nanoparticles as delivery system for influenza virus glycoproteins. J. Control. Release 54(1), 15–27 (1998).
55 Leo E, Brina B, Forni F, Vandelli MA. In vitro evaluation of PLA nanoparticles containing a lipophilic drug in watersoluble or insoluble form. Int. J. Pharm. 278(1), 133–141 (2004).
56 Dillen K, Vandervoort J, Van den Mooter G, Verheyden L, Ludwig A. Factorial design, physicochemical characterisation and activity of ciprofloxacin–PLGA nanoparticles. Int. J. Pharm. 275(1–2), 171–187 (2004).
57 Langer RS, Peppas NA. Present and future applications of biomaterials in controlled drug delivery systems. Biomaterials 2(4), 201–214 (1981).
58 Zambaux MF, Bonneaux F, Gref R, Dellacherie E, Vigneron C. Preparation and characterization of protein Cloaded PLA nanoparticles. J. Control. Release 60(2–3), 179–188 (1999).
59 GalindoRodriguez SA, Allemann E, Fessi H, Doelker E. Polymeric nanoparticles for oral delivery of drugs and vaccines: a critical evaluation of in vivo studies. 22(5), 419–464 (2005).
60 AlonsoSande MA, Cuna M, RemunanLopez C, TeijeiroOsorio DE, AlonsoLebrero JL, Alonso MAJ. Formation of new glucomannanchitosan nanoparticles and study of their ability to associate and deliver proteins. Macromolecules 39(12), 4152–4158 (2006).
61 Calvo P, RemunanLopez C, VilaJato JL, Alonso MAJ. Chitosan and chitosan/ethylene oxidepropylene oxide block copolymer nanoparticles as novel carriers for proteins and vaccines. Pharm. Res. 14(10), 1431–1436 (1997).
62 Calvo P, RemuñánLópez C, VilaJato JL, Alonso MJ. Novel hydrophilic chitosanpolyethylene oxide nanoparticles as protein carriers. J. Appl. Polym. Sci. 63(1), 125–132 (1997).
63 Balthasar S, Michaelis K, Dinauer N, von Briesen H, Kreuter JR, Langer K. Preparation
and characterisation of antibody modified gelatin nanoparticles as drug carrier system for uptake in lymphocytes. Biomaterials 26(15), 2723–2732 (2005).
64 Reis CP, Ribeiro AJ, Houng S, Veiga F, Neufeld RJ. Nanoparticulate delivery system for insulin: design, characterization and in vitro/in vivo bioactivity. Eur. J. Pharm. Sci. 30(5), 392–397 (2007).
65 Reis CP, Veiga FJ, Ribeiro AJ, Neufeld RJ, Damgé C. Nanoparticulate biopolymers deliver insulin orally eliciting pharmacological response. J. Pharm. Sci. 97(12), 5290–5305 (2008).
66 Chalasani KB, RussellJones GJ, Jain AK, Diwan PV, Jain SK. Effective oral delivery of insulin in animal models using vitamin B12coated dextran nanoparticles. J. Control. Release 122(2), 141–150 (2007).
67 Parajó Y, D´Angelo I, Welle A, GarciaFuentes M, Alonso MJ. Hyaluronic acid/chitosan nanoparticles as delivery vehicles for VEGF and PDGFBB. Drug Deliv. 17(8), 596–604 (2010).
68 Trapani A, Lopedota A, Franco M et al. A comparative study of chitosan and chitosan/cyclodextrin nanoparticles as potential carriers for the oral delivery of small peptides. Eur. J. Pharm. Biopharm. 75(1), 26–32 (2010).
69 BernkopSchnurch A, Krauland AH, Leitner VM, Palmberger T. Thiomers: potential excipients for noninvasive peptide delivery systems. Eur. J. Pharm. Biopharm. 58(2), 253–263 (2004).
70 Deutel B, Greindl M, Thaurer M, BernkopSchnuerch A. Novel insulin thiomer nanoparticles: in vivo evaluation of an oral drug delivery system. Biomacromolecules 9(1), 278–285 (2008).
71 Roldo M, Hornof M, Caliceti P, BernkopSchnurch A. Mucoadhesive thiolated chitosans as platforms for oral controlled drug delivery: synthesis and in vitro evaluation. Eur. J. Pharm. Biopharm. 57(1), 115–121 (2004).
72 Woitiski CB, Neufeld RJ, Ribeiro ANJ, Veiga F. Colloidal carrier integrating biomaterials for oral insulin delivery: influence of component formulation on physicochemical and biological parameters. Acta Biomater. 5(7), 2475–2484 (2009).
73 Chalasani KB, RussellJones GJ, Yandrapu SK, Diwan PV, Jain SK. A novel vitamin B12nanosphere conjugate carrier system for peroral delivery of insulin. J. Control. Release 117(3), 421–429 (2007).
74 Reis CP, Ribeiro AJ, Veiga F, Neufeld RJ, Damgé C. Polyelectrolyte biomaterial interactions provide nanoparticulate carrier

Polymer-based oral peptide nanomedicines | Review
www.future-science.com 667future science group
for oral insulin delivery. Drug Deliv. 15(2), 127–139 (2008).
75 Pinto Reis C, Neufeld RJ, Ribeiro AJ, Veiga F. Nanoencapsulation II. Biomedical applications and current status of peptide and protein nanoparticulate delivery systems. Nanomed. Nanotechnol. Biol. Med. 2(2), 53–65 (2006).
76 Woitiski CB, Neufeld RJ, Veiga F, Carvalho RA, Figueiredo IV. Pharmacological effect of orally delivered insulin facilitated by multilayered stable nanoparticles. Eur. J. Pharm. Sci. 41(3–4), 556–563 (2010).
77 Florence AT. Nanoparticle uptake by the oral route: fulfilling its potential? Drug Discov. Today Technol. 2(1), 75–81 (2005).
78 Sarmento B, Ribeiro A, Veiga F, Ferreira D, Neufeld R. Oral bioavailability of insulin contained in polysaccharide nanoparticles. Biomacromolecules 8(10), 3054–3060 (2007).
79 Sarmento B, Ribeiro A, Veiga F, Ferreira D. Development and characterization of new insulin containing polysaccharide nanoparticles. Coll. Surf. B Biointerfaces 53(2), 193–202 (2006).
80 Sarmento B, Ribeiro A, Veiga F, Sampaio P, Neufeld R, Ferreira D. Alginate/chitosan nanoparticles are effective for oral insulin delivery. Pharm. Res. 24(12), 2198–2206 (2007).
81 Sonaje K, Chen YJ, Chen HL et al. Entericcoated capsules filled with freeze–dried chitosan/poly(gammaglutamic acid) nanoparticles for oral insulin delivery. Biomaterials 31(12), 3384–3394 (2010).
82 Sonaje K, Lin KJ, Wang JJ et al. Selfassembled pHsensitive nanoparticles: a platform for oral delivery of protein drugs. Adv. Func. Mater. 20(21), 3695–3700 (2010).
83 Sonaje K, Lin KJ, Wey SP et al. Biodistribution, pharmacodynamics and pharmacokinetics of insulin analogues in a rat model: oral delivery using pHresponsive nanoparticles vs subcutaneous injection. Biomaterials 31(26), 6849–6858 (2010).
84 Lin YH, Mi FL, Chen CT et al. Preparation and characterization of nanoparticles shelled with chitosan for oral insulin delivery. Biomacromolecules 8(1), 146–152 (2007).
85 Shu S, Zhang X, Teng D, Wang Z, Li C. Polyelectrolyte nanoparticles based on watersoluble chitosanpoly (laspartic acid)polyethylene glycol for controlled protein release. Carbohyd. Res. 344(10), 1197–1204 (2009).
86 Makhlof A, Tozuka Y, Takeuchi H. Design and evaluation of novel pHsensitive chitosan nanoparticles for oral insulin delivery. Eur. J. Pharm. Sci. 42(5), 445–451 (2011).
87 Goycoolea FM, Lollo G, RemunanLopez C, Quaglia F, Alonso MJ. Chitosanalginate blended nanoparticles as carriers for the transmucosal delivery of macromolecules. Biomacromolecules 10(7), 1736–1743 (2009).
88 Krauland AH, Alonso MJ. Chitosan/cyclodextrin nanoparticles as macromolecular drug delivery system. Int. J. Pharm. 340(1–2), 134–142 (2007).
89 Zhang N, Li J, Jiang W et al. Effective protection and controlled release of insulin by cationiccyclodextrin polymers from alginate/chitosan nanoparticles. Int. J. Pharm. 393(1–2), 213–219 (2010).
90 Prego C, Fabre M, Torres D, Alonso MJ. Efficacy and mechanism of action of chitosan nanocapsules for oral peptide delivery. Pharm. Res. 23(3), 549–556 (2006).
91 Azevedo J, Sizilio R, Brito M et al. Physical and chemical characterization insulinloaded chitosanTPP nanoparticles. J. Therm. Anal. Calorim. 106(3), 685–689 (2011).
92 Avadi MR, Sadeghi AMM, Mohammadpour N et al. Preparation and characterization of insulin nanoparticles using chitosan and Arabic gum with ionic gelation method. Nanomed. Nanotechnol. Biol. Med. 6(1), 58–63 (2010).
93 GarciaFuentes M, Torres D, Alonso MJ. New surfacemodified lipid nanoparticles as delivery vehicles for salmon calcitonin. Int. J. Pharm. 296(1–2), 122–132 (2005).
94 GarciaFuentes M, Prego C, Torres D, Alonso MJ. A comparative study of the potential of solid triglyceride nanostructures coated with chitosan or poly(ethylene glycol) as carriers for oral calcitonin delivery. Eur. J. Pharm. Sci. 25(1), 133–143 (2005).
95 Prego C, Garcia M, Torres D, Alonso MJ. Transmucosal macromolecular drug delivery. J. Control. Release 101(1–3), 151–162 (2005).
96 Prego C, Torres D, Alonso MJ. Chitosan nanocapsules as carriers for oral peptide delivery: effect of chitosan molecular weight and type of salt on the in vitro behaviour and in vivo effectiveness. J. Nanosci. Nanotechnol. 6(9–10), 2921–2928 (2006).
97 Vasir JK, Tambwekar K, Garg S. Bioadhesive microspheres as a controlled drug delivery system. Int. J. Pharm. 255(1–2), 13–32 (2003).
98 Gref R, Quellec P, Sanchez A, Calvo P, Dellacherie E, Alonso MJ. Development and characterization of CyAloaded poly(lactic acid):poly(ethylene glycol)PEG micro and nanoparticles. Comparison with conventional PLA particulate carriers. Eur. J. Pharm. Biopharm. 51(2), 111–118 (2001).
99 Belchetz P, Hammond P. Mosby´s Colour Atlas and Text of Diabetes and Endocrinology. Elsevier Ltd, Burgos, Spain (2004).
100 Wong TW. Design of oral insulin delivery systems. J. Drug Target. 18(2), 79–92 (2010).
101 Gupta A, Jha KK, Arora R. Insulin durg delivery: strategies and technologies. Pharm. Res. 4, 154–168 (2010).
102 Sabetsky V, Ekblom J. Insulin: a new era for an old hormone. Pharm. Res. 61(1), 1–4 (2010).
103 Thomas F. Advances in insulin delivery systems and devices: beyond the vial and syringe. Insulin 1(3), 99–108 (2006).
104 Peppas NA, Kavimandan NJ. Nanoscale analysis of protein and peptide absorption: insulin absorption using complexation and pHsensitive hydrogels as delivery vehicles. Eur. J. Pharm. Sci. 29(3–4), 183–197 (2006).
105 Morishita M, Goto T, Nakamura K, Lowman AM, Takayama K, Peppas NA. Novel oral insulin delivery systems based on complexation polymer hydrogels: single and multiple administration studies in type 1 and 2 diabetic rats. J. Control. Release 110(3), 587–594 (2006).
106 Liu H, Tang R, Pan WS, Zhang Y. Potential utility of various protease inhibitors for improving the intestinal absorption of insulin in rats. J. Pharm. Pharmacol. 55(11), 1523–1529 (2003).
107 Agarwal V, Reddy IK, Khan MA. Oral delivery of proteins: effect of chicken and duck ovomucoid on the stability of insulin in the presence of achymotrypsin and trypsin. Pharm. Pharmacol. Commun. 6(5), 223–227 (2000).
108 Shah RB, Ahsan F, Khan MA. Oral delivery of proteins: progress and prognostication. Crit. Rev. Ther. Drug Carrier Syst. 19(2), 135–169 (2002).
109 Li CL, Deng YJ. Oilbased formulations for oral delivery of insulin. J. Pharm. Pharmacol. 56(9), 1101–1107 (2004).
110 Cox DS, Raje S, Gao HL, Salama NN, Eddington ND. Enhanced permeability of molecular weight markers and poorly bioavailable compounds across Caco2 cell monolayers using the absorption enhancer, zonula occludens toxin. Pharm. Res. 19(11), 1680–1688 (2002).
111 Karyekar CS, Fasano A, Raje S, Lu R, Dowling TC, Eddington ND. Zonula occludens toxin increases the permeability of molecular weight markers and chemotherapeutic agents across the bovine brain microvessel endothelial cells. J. Pharm. Sci. 92(2), 414–423 (2003).
Review | Herrero, Alonso & Csaba
Therapeutic Delivery (2012) 3(5)668 future science group
112 Eaimtrakarn S, Prasad YVR, Ohno T et al. Absorption enhancing effect of Labrasol on the intestinal absorption of insulin in rats. J. Drug Target. 10(3), 255–260 (2002).
113 Kapitza C, Zijlstra E, Heinemann L, Castelli MC, Riley G, Heise T. Oral insulin: a comparison with subcutaneous regular human insulin in patients with type 2 diabetes. Diabetes Care 33(6), 1288–1290 (2010).
114 Kamei N, Morishita M, Eda Y, Ida N, Nishio R, Takayama K. Usefulness of cellpenetrating peptides to improve intestinal insulin absorption. J. Control. Release 132(1), 21–25 (2008).
115 Clement S, Dandona P, Still JG, Kosutic G. Oral modified insulin (HIM2) in patients with type 1 diabetes mellitus: results from a phase I/II clinical trial. Metabolism 53(1), 54–58 (2004).
116 Hazra P, Adhikary L, Dave N et al. Development of a process to manufacture PEGylated orally bioavailable insulin. Biotechnol. Prog. 26(6), 1695–1704 (2010).
117 Petrus AK, Allis DG, Smith RP, Fairchild TJ, Doyle RP. Exploring the implications of vitamin B12 conjugation to insulin on insulin receptor binding. ChemMedChem 4(3), 421–426 (2009).
118 Wood KM, Stone G, Peppas NA. Lectin functionalized complexation hydrogels for oral protein delivery. J. Control. Release 116(2), 66–68 (2006).
119 Makhlof A, Werle M, Tozuka Y, Takeuchi H. A mucoadhesive nanoparticulate system for the simultaneous delivery of macromolecules and permeation enhancers to the intestinal mucosa. J. Control. Release 149(1), 81–88 (2011).
120 Geho WB, Geho HC, Lau JR, Gana TJ. Hepaticdirected vesicle insulin: a review of formulation development and preclinical evaluation. Diabetes Technol. Soc. 3(6), 1451–1459 (2009).
121 Woitiski CB, Carvalho RA, Ribeiro AJ, Neufeld RJ, Veiga F. Strategies toward the
improved oral delivery of insulin nanoparticles via gastrointestinal uptake and translocation. BioDrugs 22(4), 223–237 (2008).
122 Li MG, Lu WL, Wang HC et al. Distribution, transition, adhesion and release of insulin loaded nanoparticles in the gut of rats. Int. J. Pharm. 329(1–2), 182–191 (2007).
123 Davaran S, Omidi Y, Rashidi MR et al. Preparation and in vitro evaluation of linear and starbranched PLGA nanoparticles for insulin delivery. J. Bioact. Compat. Polym. 23(2), 115–131 (2008).
124 Xiong XY, Li YP, Li ZL et al. Vesicles from pluronic/poly(lactic acid) block copolymers as new carriers for oral insulin delivery. J. Control. Release 120(1–2), 11–17 (2007).
125 Pan Y, Li YJ, Zhao HY et al. Bioadhesive polysaccharide in protein delivery system: chitosan nanoparticles improve the intestinal absorption of insulin in vivo. Int. J. Pharm. 249(1–2), 139–147 (2002).
126 Prego C, Torres D, Alonso MJ. The potential of chitosan for the oral administration of peptides. Exp. Opin. Drug Deliv. 2(5), 843–854 (2005).
127 Csaba N, GarciaFuentes M, Alonso MJ. The performance of nanocarriers for transmucosal drug delivery. Exp. Opin. Drug Deliv. 3(4), 463–478 (2006).
128 de la Fuente M, Csaba N, GarciaFuentes M, Alonso MJ. Nanoparticles as protein and gene carriers to mucosal surfaces. Nanomedicine 3(6), 845–857 (2008).
129 Krauland AH, Guggi D, BernkopSchnurch A. Oral insulin delivery: the potential of thiolated chitosaninsulin tablets on nondiabetic rats. J. Control. Release 95(3), 547–555 (2004).
130 BernkopSchnurch A. Thiomers: a new generation of mucoadhesive polymers. Adv. Drug Deliv. Rev. 57(11), 1569–1582 (2005).
131 Werle M, Takeuchi H, BernkopSchnürch A. Modified chitosans for oral drug delivery. J. Pharm. Sci. 98(5), 1643–1656 (2009).
132 Rekha MR, Sharma CP. Synthesis and evaluation of lauryl succinyl chitosan particles towards oral insulin delivery and absorption. J. Control. Release 135(2), 144–151 (2009).
133 Sonaje K, Lin YH, Juang JH, Wey SP, Chen CT, Sung HW. In vivo evaluation of safety and efficacy of selfassembled nanoparticles for oral insulin delivery. Biomaterials 30(12), 2329–2339 (2009).
134 Woitiski CB, Sarmento B, Carvalho RA, Neufeld RJ, Veiga F. Facilitated nanoscale delivery of insulin across intestinal membrane models. Int. J. Pharm. 412(1–2), 123–131 (2011).
135 Varela MC, Guzman M, Molpeceres J, del Rosario Aberturas M, RodriguezPuyol D, RodriguezPuyol M. Cyclosporineloaded polycaprolactone nanoparticles: immunosuppression and nephrotoxicity in rats. Eur. J. Pharm. Sci. 12(4), 471–478 (2001).
136 Graf A, McDowell A, Rades T. Poly(alkycyanoacrylate) nanoparticles for enhanced delivery of therapeutics: is there real potential? Exp. Opin. Drug Deliv. 6(4), 371–387 (2009).
137 ElShabouri MH. Positively charged nanoparticles for improving the oral bioavailability of cyclosporinA. Int. J. Pharm. 249(1–2), 101–108 (2002).
� Websites201 Clinical Trials.
www.clinicaltrials.gov (Accessed 25 October 2011)
202 ISI Web of Knowledge. www.webofknowledge.com (Accessed 25 October 2011)