poliomyelitis1
TRANSCRIPT
Poliomyelitis
By: Dr. Masoud Shayesteh Azar
Associate Professor, Orthopaedic Department,
Mazandaran University


Poliomyelitis
polio= gray matter
Myelitis= inflammation of the spinal cord

Poliomyelitis
First described by Michael Underwood in 1789
First outbreak described in U.S. in 1843
21,000 paralytic cases reported in the U. S. in 1952
Global eradication in near future
Poliomyelitis
Poliomyelitis, literally meaning “gray spinal
cord inflammation
It is a viral infection
There are three types of poliovirus and
many strains of each type
It is contagious: usually spread from person
to person.
Only harmful to humans
The Poliovirus
Virus localized in the anterior horn cells of the spinal cord and certain brain steam motor nuclei.

Poliovirus
Enterovirus (RNA)
Three serotypes: 1, 2, 3
Minimal heterotypic immunity between serotypes
Rapidly inactivated by heat, formaldehyde, chlorine, ultraviolet light


Poliomyelitis Pathogenesis
Entry into mouth
Replication in pharynx, GI tract, local lymphatics
Hematologic spread to lymphatics and central nervous system
Viral spread along nerve fibers
Destruction of motor neurons

Poliomyelitis Pathogenesis
The ant. Horn motor cells may be damaged
by viral multiplication or toxic byproducts of
the virus or indirectly by ischemia, edema,
and hemorrhage in the glial tissues.
Destruction of the spinal cord occurs focally
and within 3 days wallerian degeneration is
evident.

poliomyelitis
Most affects children under the age of 5
years in developing tropical countries.
Incubation period ranges from 6 to 20 days

What are the symptoms?
Acute stage: generally lasts 7 to 10 days.
Many include fever, pharyngitis, headache,
anorexia, nausea, and vomiting. Illness may
progress to aseptic meningitis and
menigoencephalitis in 1% to 4% of patients.
These patients develop a higher fever &
sever headache with stiffness of the neck
and back.
What are the symptoms?
Paralytic disease occurs 0.1% to 1% of those
who become infected with the polio virus.
Paralysis of the respiratory muscles or from
cardiac arrest if the neurons in the medulla
oblongata are destroyed.

Clinical course
Symptoms range :from mild malaise to
generalized encephalomyelitis with
widespread paralysis.
Hyperesthesia or paresthesia in the
extremities and muscular pain is common.
Muscles are tender even to gentle palpation.
Poliomyelitis
According to Sharrard, weakness is clinically
detectable only when more than 60% of the
nerve cells supplying the muscle have been
destroyed.
Paralysis occurs twice as often in the lower
extremity as in upper extremity.
Poliomyelitis
The most commonly affected muscles are the
Quadriceps, glutei, tibialis anterior, medial
hamstrings, and hip flexors.
Deltoid, triceps, and pectoralis major.


Poliomyelitis
Patients have some or full recovery from
paralysis, most clinical recovery occurs
during the 1 month and almost complete
within 6 months.
Limited recovery may occur for about 2
years.

Poliomyelitis
In cases with paralysis superficial reflexes
usually are absent first, and deep tendon
reflexes disappear when the muscle group
is paralyzed.
DDX.: Guillain-Barre syndrome, and other
forms of encephalomyelitis


Treatment in the acute stage
Bed rest, analgesics, hot packs, and
anatomical positioning of the limbs
gentle passive ROM exercises of all joints
Treatment in the acute stage
close monitoring of respiratory and
cardiovascular functioning is essential during
the acute stage of poliomyelitis along with
fever control and pain relievers for muscle
spasms.
Mechanical ventilation, respiratory therapy may
be needed depending of the severity of
patients.

Convalescent stage
From 2 days after the temperature return to
normal and continues for 2 years
Muscle power improves
Physical therapy is recommended for full
recovery.
Passive stretching exercises and wedging
casts can be used for mild to moderate
contractures.

Convalescent stage
Surgical release of tight fascia and muscle
aponeuroses and lengthening of tendons
may be necessary for contractures
persisting longer than 6 months.
Orthoses should be used until no further
recovery is anticipated.

Chronic stage
24 months after the active illness:
The goals of treatment include correcting any
significant muscle imbalance and
preventing or correcting soft tissue or bony
deformities.


Chronic stage
Static joint instability can be controlled by
Orthoses.
Dynamic joint instability result in a fixed
deformity that cannot be controlled by
Orthoses.
Chronic stage
Soft tissue surgery, such as tendon transfers,
should be done in young children before
the development of any fixed bony
changes.
Bony procedures for correcting a deformity
can be delayed until skeletal growth is near
completion.

Global eradication in near future
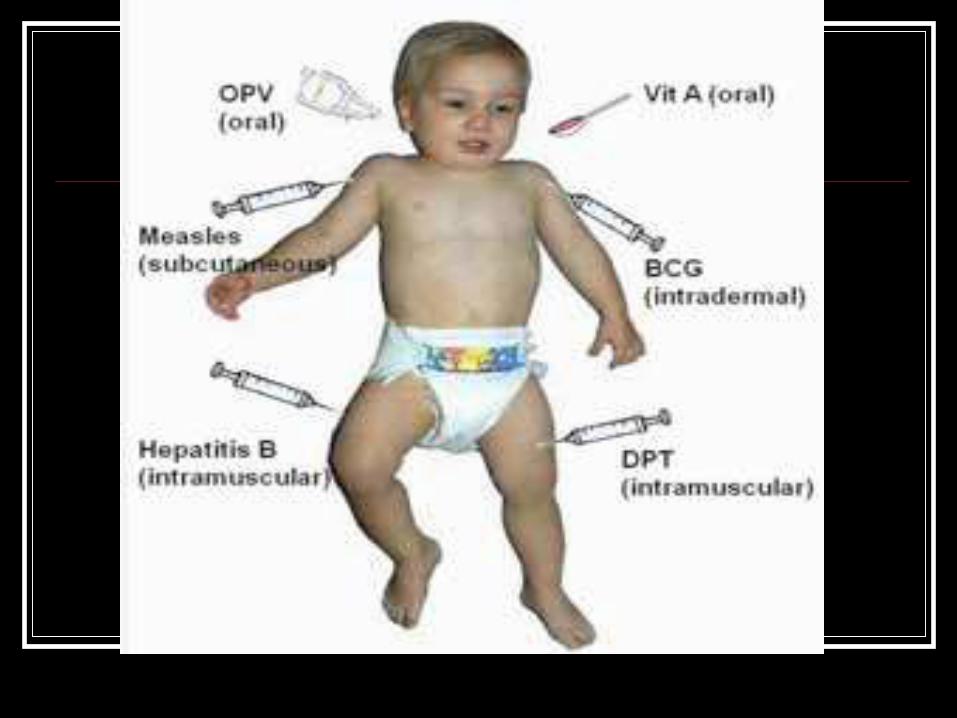
Prevention
Prevention
Prevention
Immunization of the young continues



Wild Poliovirus 1988
National Immunization Program
Centers for Disease Control and Prevention
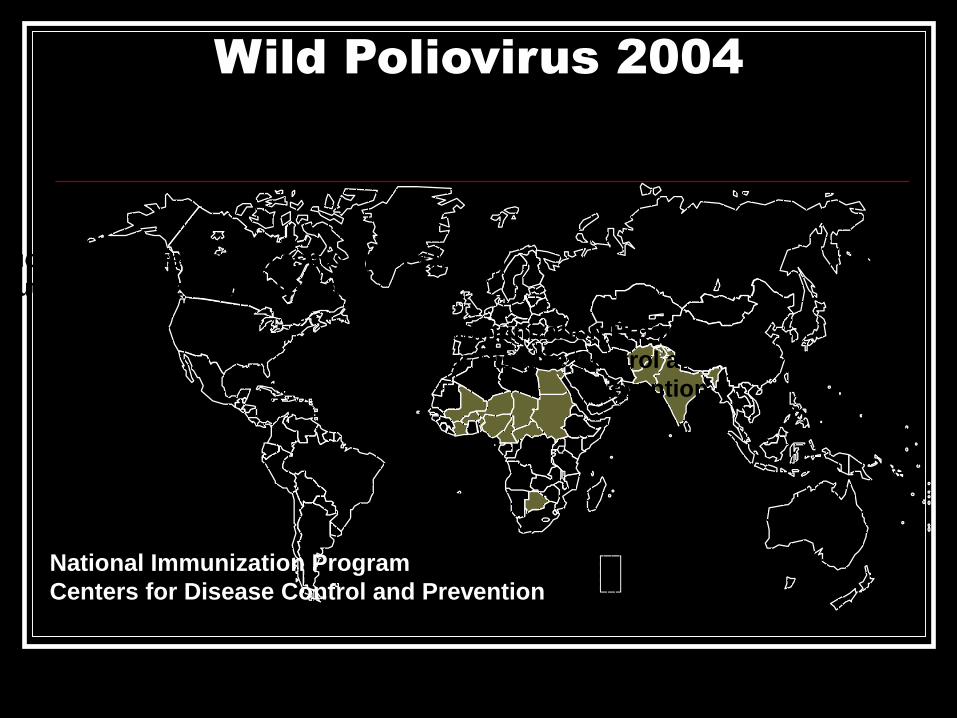
Wild Poliovirus 2004
National Immunization Program
Centers for Disease Control and
Prevention
National Immunization Program
Centers for Disease Control and Prevention
National Immunization Program
Centers for Disease Control and Prevention

Study
We study 246 patient with polio in Sari
Male:156 cases (63/4%)
female: 90 cases (36/6%)
age :22 to 63 years old main age 46/3
One lower limb: 164 cases (66/6%)
Both lower limb: 62 cases (25/2 %)
Both lower limb together with upper limb 10
cases (4/1% )

Result:
From 246 patients ;108 used brace
56 patients needs brace but not used
187 operation has down for these patients
97 patients more than one operation has down
82 patients have mild symptoms and don’t need
To any operation or brace.

Result:
From 187 operation :
53 cases; ankle triple arthrodesis
81 cases; tendon transfer EHL to dorsum
foot
10 cases; other kind of tendon transfers
11 cases; ATL
8 cases; lower limb lengthening
Result:
2 cases; Ephypisodesis
1 case; ankle fusion
23 cases; toe deformity correction
53 cases; soft tissue release for knee and hip
flexion contracture
37 cases; osteotomy around knee

Result:
Very important point
No any new case in last 10 years
reported.