policy evaluation
DESCRIPTION
Policy Evaluation. Exploring the Dynamic and Democratic Dimensions of Health Protection Policies. Bobby Milstein Syndemics Prevention Network Centers for Disease Control and Prevention [email protected] http://www.cdc.gov/syndemics. Edinburgh Evaluation Summer School Edinburgh, Scotland - PowerPoint PPT PresentationTRANSCRIPT

Syndemics
Prevention Network
Edinburgh Evaluation Summer SchoolEdinburgh, Scotland
June 6, 2007
Exploring the Dynamic and Democratic Dimensions of Health Protection Policies
Bobby Milstein Syndemics Prevention NetworkCenters for Disease Control and
http://www.cdc.gov/syndemics
Policy Evaluation

Syndemics
Prevention Network
Appreciating the Unique Character of Evaluative Inquiry
“It is easier to find facts than it is to face them.”
Centers for Disease Control and Prevention. What procedures are available for planning and evaluating initiatives to prevent syndemics? Syndemics Prevention Network, 2001. Available at <http://www.cdc.gov/syndemics/overview-planeval.htm>.
Questions of Fact(descriptions, associations, effects)
ResearchSystematic
MethodsEvaluation
Questions of Values(merit, worth, significance)

Syndemics
Prevention Network
Picture a Neighborhood Where…
• Conditions are not supportive of healthy living
• People are either afflicted by or at risk for numerous mutually reinforcing health problems
• Citizen leaders are making an effort to alleviate afflictions and improve living conditions, but their power is limited
• More could be done through better local organizing and with effective assistance from outside allies (e.g., philanthropy, government)James Nachtwey in Sachs J. How to end poverty.
Time Magazine 2005 March 14.
How does public health policy typically proceed in such circumstances?
Which forms of policy planning and evaluation are most relevant and promising?

Syndemics
Prevention Network
Policy Planning & EvaluationEngages Questions of Social Navigation
Prevalence of Diagnosed Diabetes, US
0
10
20
30
40
1980 1990 2000 2010 2020 2030 2040 2050
Mill
ion
pe
op
le
HistoricalData
Markov Model Constants• Incidence rates (%/yr)• Death rates (%/yr)• Diagnosed fractions(Based on year 2000 data, per demographic segment)
Honeycutt A, Boyle J, Broglio K, Thompson T, Hoerger T, Geiss L, Narayan K. A dynamic markov model for forecasting diabetes prevalence in the United States through 2050. Health Care Management Science 2003;6:155-164.
Jones AP, Homer JB, Murphy DL, Essien JDK, Milstein B, Seville DA. Understanding diabetes population dynamics through simulation modeling and experimentation. American Journal of Public Health 2006;96(3):488-494.
Markov Forecasting Model
Trend is not destiny!
How?
Why?
Where?
Who?
What?

Syndemics
Prevention Network
Modern public health policy—and evaluation—are becoming more…
• Inter-connected (ecological, multi-causal, dynamic, systems-oriented) Concerned more with leverage than control
• Public (broad-based, partner-oriented, citizen-led, inter-sector, democratic) Concerned with many interests and mutual-accountability
• Questioning (evaluative, reflexive, critical, practical)Concerned with creating and protecting values like health, equity,dignity, security, satisfaction, justice, wealth, and freedom in both means and ends
A Field in Transition

Syndemics
Prevention Network
Left Unexamined…
• Singular “program” as the unit of inquiry (N=1 organizational depth)
• Dynamic aspects of program effectiveness (e.g., better-before-worse patterns of change)
• Democratic aspects of public health work (e.g., alignment among multiple actors, including those who are not professionals and who may be pursuing other goals)
• Evaluative aspects of planning
Milstein B, Wetterall S, CDC Evaluation Working Group. Framework for program evaluation in public health. MMWR Recommendations and Reports 1999;48(RR-11):1-40. Available at <http://www.cdc.gov/mmwr/PDF/RR/RR4811.pdf>.
Framework for Program Evaluation“Both a synthesis of existing evaluation practices
and a standard for further improvement.”

Syndemics
Prevention Network
Are We Posing Questions About Attribution or Contribution?
“…if a program’s activities are aligned with those
of other programs operating in the same setting,
certain effects (e.g., the creation of new laws or
policies) cannot be attributed solely to one
program or another. In such situations, the goal
for evaluation is to gather credible evidence that
describes each program’s contribution in the
combined change effort. Establishing
accountability for program results is predicated
on an ability to conduct evaluations that assess
both of these kinds of effects.” p.11-12
Calls into question the conditions in which one focuses on a “program” as the unit of analysis

Syndemics
Prevention Network
• Locating categorical disease or risk prevention programs within a broader system of health protection
• Constructing credible knowledge without comparison/control groups
• Differentiating questions that focus on attribution vs. contribution
• Balancing trade-offs between short- and long-term effects
• Avoiding the pitfalls of professonalism (e.g., over-specialization, arrogance, reinforcement of the status quo)
• Harnessing the power of intersectoral and citizen-led public work
• Defining standards and values for judgment
• Others…
Serious Challenges for Planners and Evaluators

Syndemics
Prevention Network
Topics for Today
• Health Protection Policy in a Dynamic and Democratic World– Concepts, keywords, structures
• Looking Backward, Looking Forward
– Retrospectively evaluating past policy
– Prospectively crafting/evaluating future policy
• Highlighting One Promising Methodology
– System Dynamics simulation modeling
• Questions and Discussion Throughout

Syndemics
Prevention Network
Defining Keywords
Adapted from:
Milio N. Glossary: healthy public policy. Journal of Epidemiology and Community Health 2001;55(9):622-623.
Forrester JW. Policies and decisions. In: Industrial Dynamics. Cambridge, MA: MIT Press; 1961. p. 93-108.
Bennett T, Grossberg L, Morris M. New keywords: a revised vocabulary of culture and society. Malden, MA: Blackwell Pub., 2005.
Scriven M. Evaluation thesaurus. 4th ed Newbury Park, CA: Sage Publications, 1991.
Policy evaluation is…
Policy is…• The plans, programs, principles, or more broadly the
course of action of some actor(s), which may include a degree of deliberate inaction as well
• Explicit or implicit rules for deciding how to respond to circumstances and pressures
• Priorities guiding resource allocation
• The systematic process of determining—and improving—the merit, worth, or significance of decisions about what to do, or not to do, in a given domain
• The articulation and assessment of alternative possible futures, each corresponding to a different policy
Syndemics
Prevention Network
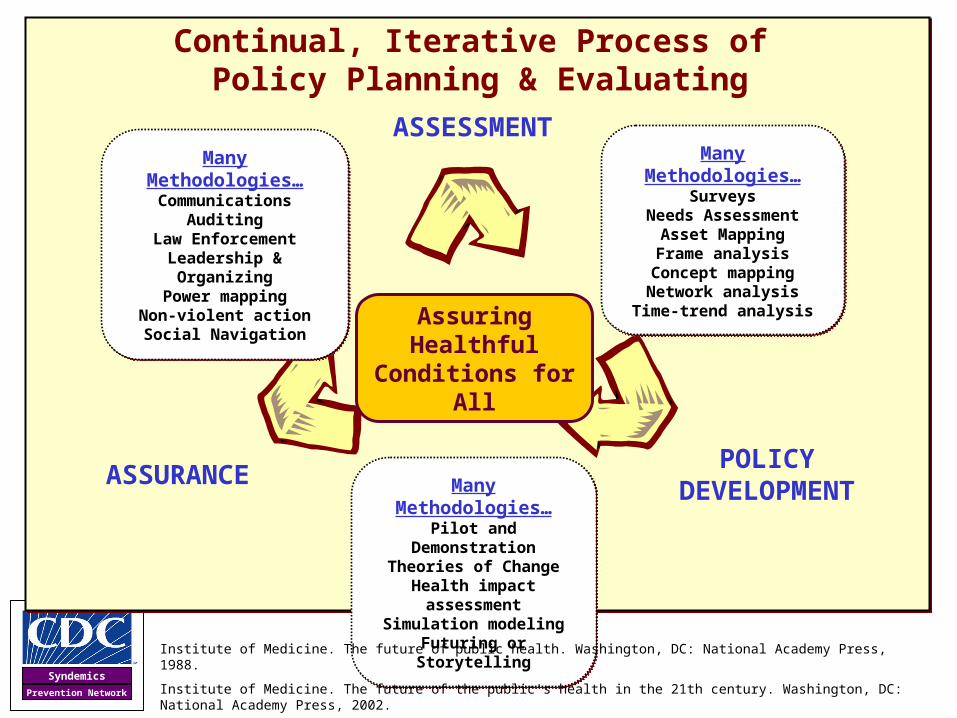
Policy is our general approach toward a particular problem or area of concern…
Continual, Iterative Process of Policy Planning & Evaluating
POLICYDEVELOPMENT
ASSESSMENT
ASSURANCE
Assuring Healthful Conditions for All
Many Methodologies…Pilot and Demonstration
Theories of ChangeHealth impact assessment
Simulation modelingFuturing or Storytelling
Many Methodologies…Pilot and Demonstration
Theories of ChangeHealth impact assessment
Simulation modelingFuturing or Storytelling
Many Methodologies…Communications
AuditingLaw Enforcement
Leadership & OrganizingPower mapping
Non-violent actionSocial Navigation
Many Methodologies…Communications
AuditingLaw Enforcement
Leadership & OrganizingPower mapping
Non-violent actionSocial Navigation
Many Methodologies…Surveys
Needs AssessmentAsset MappingFrame analysis
Concept mappingNetwork analysis
Time-trend analysis
Many Methodologies…Surveys
Needs AssessmentAsset MappingFrame analysis
Concept mappingNetwork analysis
Time-trend analysis
Institute of Medicine. The future of public health. Washington, DC: National Academy Press, 1988.
Institute of Medicine. The future of the public's health in the 21th century. Washington, DC: National Academy Press, 2002.
Syndemics
Prevention Network
Defining Keywords
Walt G. Health policy: an introduction to process and power. Atlantic Highlands, NJ: Zed Books, 1994.
Ignatieff M. The grey empitness inside John Major. The Observer 1992 November 15; 25.
“Policy is the selection of non-contradictory means to achieve non-contradictory ends over the medium to long term. Policy is the thread of conviction that keeps a government from
becoming the prisoner of events.”
-- Michael Ignatieff
Artist: Boyce Watt
Policy vs. Decisions
• Policy usually involves a series of specific decisions, programs, actions
• But the distinction is blurry– Policy makers never start from a blank
sheet of possibilities– Ad hoc decisions may together add up to
forceful implicit policy

Syndemics
Prevention Network
Events
Pattern
Events
WaterTemperature
FloodDamage
Economic Activity& Emissions
WaterLevel
Structure
R
Melting

Syndemics
Prevention Network
Time Series Models
Describe trends
Multivariate Stat Models
Identify historical trend drivers and correlates
Patterns
Structure
Events
Increasing:
• Depth of causal theory
• Robustness for longer-term projection
• Value for developing policy insights
• Degrees of uncertainty
Increasing:
• Depth of causal theory
• Robustness for longer-term projection
• Value for developing policy insights
• Degrees of uncertaintyDynamic Simulation Models
Anticipate new trends, learn about policy consequences,
and set justifiable goals
Tools for Policy Planning & Evaluation

Syndemics
Prevention Network
Consider the Track Record…
Sterman JD. Learning from evidence in a complex world. American Journal of Public Health 2006;96(3):505-514.
Forrester JW. Counterintuitive behavior of social systems. Technology Review 1971;73(3):53-68.
• Low tar and low nicotine cigarettesLead to greater carcinogen intake
• Fad dietsProduce diet failure and weight gain
• Antibiotic & pesticide useStimulate resistant strains
• Road building to ease congestion Attracts development, increases traffic, delays, and pollution
• Air-conditioning useRaises neighborhood heat
• Forest fire suppressionBuilds deadwood fueling larger, hotter, more dangerous fires
• War on drugs Raises price and attracts supply
• Suppressing dissent Inspires radicalization and extremism

Syndemics
Prevention Network
Policy Resistance is…
“The tendency for interventions to be delayed, diluted, or defeated
by the response of the system to the intervention itself.”
Meadows DH, Richardson J, Bruckmann G. Groping in the Dark: The First Decade of Global Modelling. Wiley: New York, 1985.
-- Meadows, Richardson & Bruckmann
Defining Keywords

Syndemics
Prevention Network
Seeking High-Leverage Policies
Wall painting in the Stanzino delle Matematiche in the Galleria degli Uffizi (Florence, Italy). Painted by Giulio Parigi in the years 1599-1600.
“Give me a firm place to stand and I will move the earth.”
-- Archimedes
Meadows DH. Leverage points: places to intervene in a system. Sustainability Institute, 1999. Available at <http://www.sustainabilityinstitute.org/pubs/Leverage_Points.pdf>.

Syndemics
Prevention Network
Public Health Work Literally Involves Redirecting the Course of Change
600
500
400
200
100
501950 1960 1970 1980 1990 1995
Ag
e-a
dju
ste
d D
eath
Rat
e p
er 1
00,
000
Po
pu
lati
on
1955 1965 1975 1985
300
700
Peak Rate
Rate if trend continued
Year
Actual and Expected Death Rates for Coronary Heart Disease, 1950–1998
Marks JS. The burden of chronic disease and the future of public health. CDC Information Sharing Meeting. Atlanta, GA: National Center for Chronic Disease Prevention and Health Promotion; 2003.
Centers for Disease Control and Prevention. Achievements in public health, 1900-1999: decline in deaths from heart disease and stroke -- United States, 1900-1999. MMWR 1999;48(30):649-656. Available at <http://www.cdc.gov/mmwr/preview/mmwrhtml/mm4830a1.htm>
Actual Rate
Overall Decline is Linked to…
• Reduced smoking
• Changes in diet
• Better diagnosis and treatment
• More heath services utilization
Overall Decline is Linked to…
• Reduced smoking
• Changes in diet
• Better diagnosis and treatment
• More heath services utilization
684,000 fewer deaths in 1998 alone
684,000 fewer deaths in 1998 alone

Syndemics
Prevention Network
“Public health is probably the most successful system of science and
technology combined, as well as social policy, that has ever been devised…It is, I think, a paradigmatic model for how you do concerned, humane, directed science.”
-- Richard Rhodes
Rhodes R. Limiting human violence: an emerging scientific challenge. Sarewitz D, editor. Living With the Genie: Governing Science and Technology in the 21st Century; New York, NY: Center for Science, Policy, and Outcomes; 2002.
One Observer's View…
Syndemics
Prevention Network
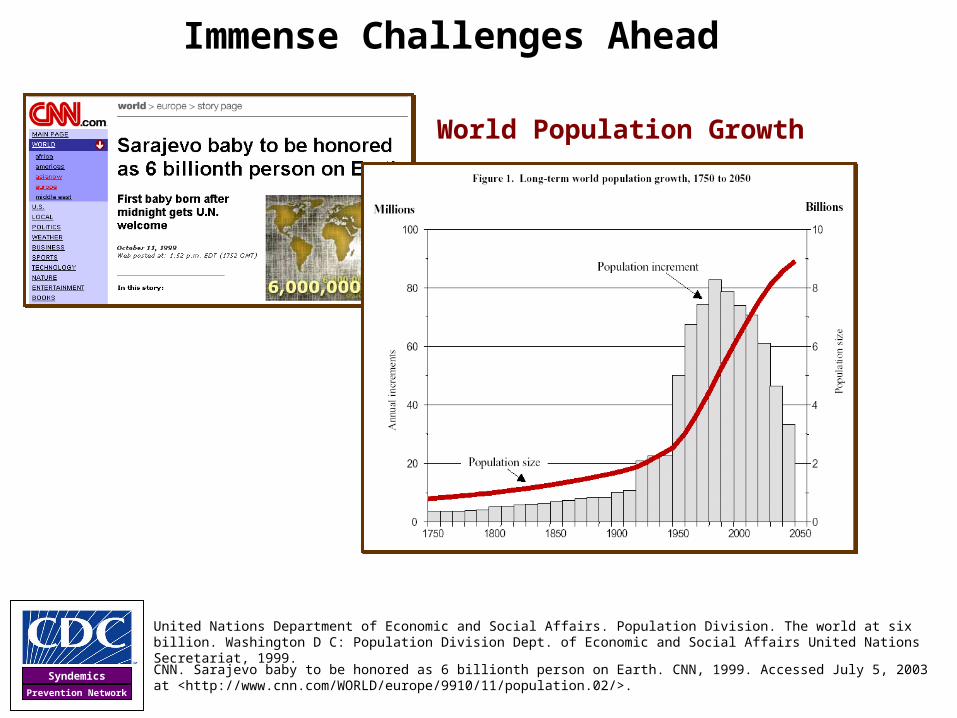
Immense Challenges Ahead
United Nations Department of Economic and Social Affairs. Population Division. The world at six billion. Washington D C: Population Division Dept. of Economic and Social Affairs United Nations Secretariat, 1999.
CNN. Sarajevo baby to be honored as 6 billionth person on Earth. CNN, 1999. Accessed July 5, 2003 at <http://www.cnn.com/WORLD/europe/9910/11/population.02/>.
World Population Growth
Syndemics
Prevention Network
Resource Depletion & Related Conflict

Syndemics
Prevention Network
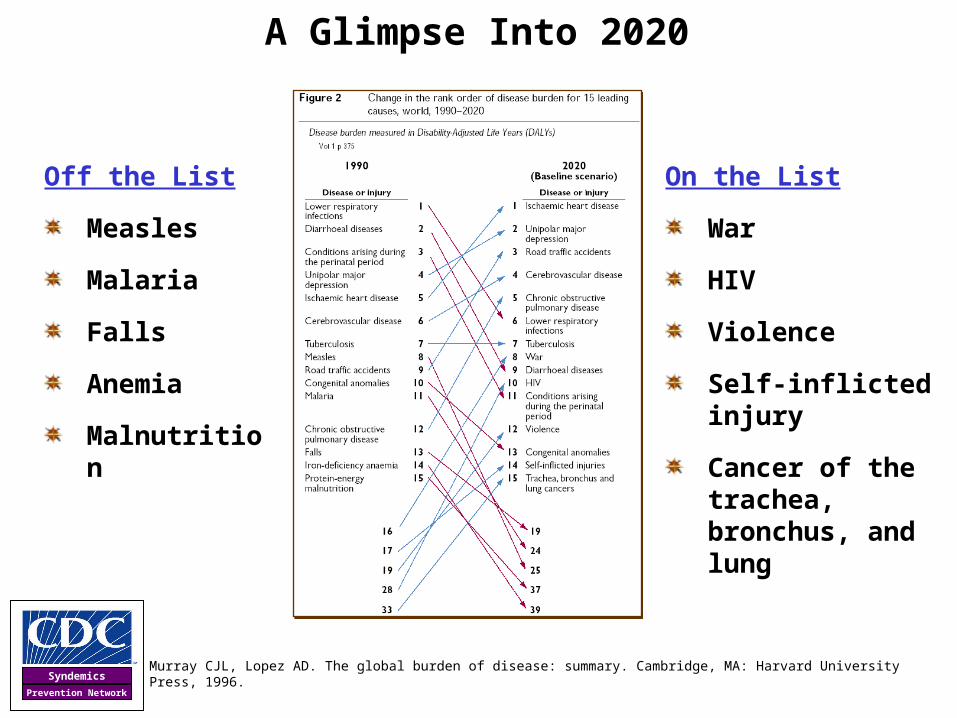
A Glimpse Into 2020
Murray CJL, Lopez AD. The global burden of disease: summary. Cambridge, MA: Harvard University Press, 1996.
Syndemics
Prevention Network
A Glimpse Into 2020
Murray CJL, Lopez AD. The global burden of disease: summary. Cambridge, MA: Harvard University Press, 1996.
On the List
War
HIV
Violence
Self-inflicted injury
Cancer of the trachea, bronchus, and lung
Off the List
Measles
Malaria
Falls
Anemia
Malnutrition

Syndemics
Prevention Network
Broad Dynamics of the Health Protection Enterprise
Prevalence of Vulnerability, Risk, or Disease
Time
HealthProtection
Efforts
-
B
Responsesto Growth
Resources &Resistance
-B
Obstacles
Broader Benefits& Supporters
R
ReinforcersPotentialThreats
The concepts and methods of policy evaluation must engage the basic features of this
dynamic and democratic system
The concepts and methods of policy evaluation must engage the basic features of this
dynamic and democratic system
Size of the Safer, Healthier
Population-
Prevalence of Vulnerability,
Risk, or Disease
B
Taking the Toll
0%
100%
R
Drivers ofGrowth
Values for Health & Equity

Syndemics
Prevention Network
A Complementary Science of Relationships
• Efforts to Reduce Population Health ProblemsProblem, problem solver, response
• Efforts to Organize a System that Assures Healthful Conditions for All Dynamic interaction among multiple problems, problem solvers, and responses
Institute of Medicine. The future of public health. Washington, DC: National Academy Press, 1988.
Institute of Medicine. The future of the public's health in the 21th century. Washington, DC: National Academy Press, 2002.
Bammer G. Integration and implementation sciences: building a new specialisation. Cambridge, MA: The Hauser Center for Nonprofit Organizations, Harvard University 2003.
True innovation occurs when things are put together for the first time that had been separate.
– Arthur Koestler

Syndemics
Prevention Network
Summers J. Soho: a history of London's most colourful neighborhood. Bloomsbury, London, 1989. p. 117.
Broad Street, One Year Later
John Snow Heroic Success or Cautionary Tale?
“No improvements at all had been made...open cesspools are still to be seen...we have all the materials for a fresh epidemic...the water-butts were in deep cellars, close to the undrained cesspool...The overcrowding appears to increase."

Syndemics
Prevention Network
“At least six times since the Depression, the United States has tried and failed to enact a national health insurance program.”
Lee P, Paxman D. Reinventing public health. Annual Reviews of Public Health 1997;18:1-35.
Number of Uninsured Americans, 1976-2003
Himmelstein, Woolhandler, Carrasquillo – Tabulation from CPS and NHIS – Lee & Paxman
Another Prototypical ExampleAttempts to Reform the U.S. Health Care Delivery System

Syndemics
Prevention Network
• Piecemeal approaches
• Failure to address root problems
• Inattention to the larger political and economic system
Heirich M. Rethinking health care: innovation and change in America. Boulder, CO: Westview Press, 1999.
Crafting Health Policies that will Succeed in a Large, Dynamic System
Efforts to reform health care policy have been ineffective because of
“Most of the analytic strategies popular among academics, politicians, and policy makers fail to observe the system as a whole…to discuss processes of mutual change that are occurring, or to analyze how innovations fit into larger nonequilibrium dynamics that are developing.”
-- Max Heirich

Syndemics
Prevention Network
Understanding Dynamic Complexity
Forrester JW. Counterintuitive behavior of social systems. Technology Review 1971;73(3):53-68.
Meadows DH. Leverage points: places to intervene in a system. Sustainability Institute, 1999. Available at <http://www.sustainabilityinstitute.org/pubs/Leverage_Points.pdf>.
Richardson GP. Feedback thought in social science and systems theory. Philadelphia, PA: University of Pennsylvania Press, 1991.
Sterman JD. Business dynamics: systems thinking and modeling for a complex world. Boston, MA: Irwin McGraw-Hill, 2000.

Syndemics
Prevention Network
Changing Views of Population HealthWhat Accounts for Poor Population Health?
• God’s will
• Humors, miasma, ether
• Poor living conditions, immorality (e.g., ?)
• Single disease, single cause (e.g., ?)
• Single disease, multiple causes (e.g., ?)
• Single cause, multiple diseases (e.g., ?)
• Multiple causes, multiple diseases (but no feedback dynamics) (e.g., ?)
• Dynamic feedback among afflictions, living conditions, and public strength (e.g., ?)
1880
1950
1960
1980
2000
1840
Milstein B. Hygeia's constellation: navigating health futures in a dynamic and democratic world [Doctoral Dissertation]. Cincinnati, OH: Union Institute & University; 2006.
Richardson GP. Feedback thought in social science and systems theory. Philadelphia, PA: University of Pennsylvania Press, 1991.

Syndemics
Prevention Network
Placing Health in a Wider Set of Relationships
Health
LivingConditions
Power toAct
This orientation explicitly includes within it our power to craft policies, along with an understanding of the
changing pressures, constraints, and consequences that shape it.
“Health Policy”
“Social Policy”

Syndemics
Prevention Network
Two Orientations
Prospective
Retrospective• What have been the observed consequences of
prior decisions?• For whom? When? Why?
At what cost?• Recommendations to continue or change strategy
• What is the range of plausible consequences of policy options?
• For whom? When? Why? At what cost?
• Which alternative futures are most highly valued, or feared?
• What must be done to move in the desired direction?

Syndemics
Prevention Network
Explicitly recognizes the evaluative aspects of planning:
• Defining problems
• Setting priorities
• Developing options
• Selecting strategies
Risley J. Public policy evaluation. Kalamazoo, MI: The Evaluation Center, Western Michigan University; February 26, 2004. <http://www.wmich.edu/evalctr/evalcafe/risley022604slides.pdf>.
Prospective Policy Evaluation

Syndemics
Prevention Network
When Faced with the Vast Scope of Public Health Threats…
Narrow the Focus and Specialize
• Identify problem
• Formulate policy
• Implement policy
• Evaluate policy
• Repeat steps 1-4, as necessary!
Breeding Ground for Disease (Karen Kasmauski, National Geographic, 2001).

Syndemics
Prevention Network
Diseases of Disarray
Hardening of the categories
Tension headache between treatment and prevention
Hypocommitment to training
Cultural incompetence
Political phobia
Input obsession
Wiesner PJ. Four disease of disarray in public health. Annals of Epidemiology. 1993;3(2):196-8.
Chambers LW. The new public health: do local public health agencies need a booster (or organizational "fix") to combat the diseases of disarray? Canadian Journal of Public Health 1992;83(5):326-8.

Syndemics
Prevention Network
Dangers of Getting Too Specific
Krug EG, World Health Organization. World report on violence and health. Geneva: World Health Organization, 2002.
Conventional problem solving proliferates problems
Opens a self-reinforcing niche for professional problem solvers
Obscures patterns that transcend any specific problem (e.g., nonviolence is entirely neglected)

Syndemics
Prevention Network
Examples of Nonviolent Action
Albert Einstein Institution. Applications of nonvilolent action. Albert Einstein Institution, 2001.
Powers RS, Vogele WB, Kruegler C, McCarthy RM. Protest, power, and change: an encyclopedia of nonviolent action from ACT-UP to women's suffrage. New York: Garland Pub., 1997.
Dismantling dictatorships
Blocking coups d’état
Defending against foreign invasions and occupations
Providing alternatives to violence in extreme ethnic conflicts
Challenging unjust social and economic systems
Developing, preserving and extending democratic practices, human rights, civil liberties, and freedom of religion
Resisting genocide
“A phenomenon that cuts across ethnic, cultural, religious, geographic,
socioeconomic and other demographic lines.”
-- Albert Einstein Institution

Syndemics
Prevention Network
Systems Archetype
“Fixes that Fail”
Kim DH. Systems archetypes at a glance. Cambridge, MA: Pegasus Communications, Inc., 1994.
Fix
+
ProblemSymptom
-
UnintendedConsequence
+
Delay
+
-B
+R
Characteristic Behavior:
Better before Worse
Syndemics
Prevention Network
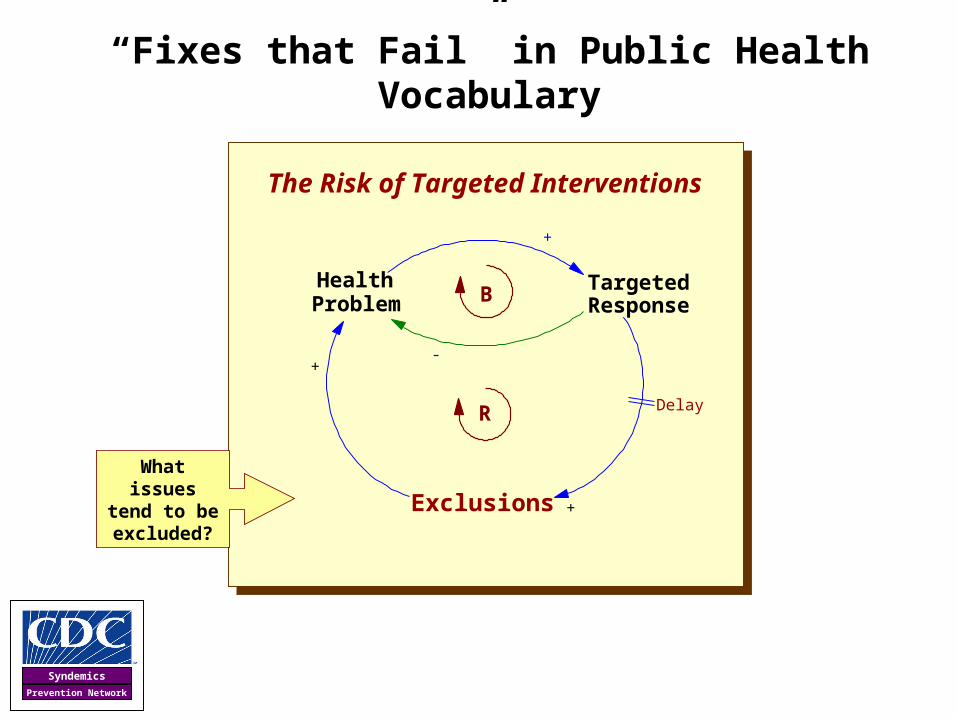
“Fixes that Fail” in Public Health Vocabulary
The Risk of Targeted Interventions
+
HealthProblem -
-
Exclusions
+
+
TargetedResponseB
Delay+R
What issues tend to be excluded?

Syndemics
Prevention Network
Some Categories of Exclusions
Conceptual
Social
Organizational
Political
Disarray
Disorientation
Disparity & Disconnection
Together, these forces may seriously undermine the effectiveness of health protection policy

Syndemics
Prevention Network
Wickelgren I. How the brain 'sees' borders. Science 1992;256(5063):1520-1521.
How Many Triangles Do You See?

Syndemics
Prevention Network
Boundary Judgments(System of Reference)
Observations(Facts)
Evaluations(Values)
Ulrich W. Boundary critique. In: Daellenbach HG, Flood RL, editors. The Informed Student Guide to Management Science. London: Thomson; 2002. p. 41-42. <http://www.geocities.com/csh_home/downloads/ulrich_2002a.pdf>.
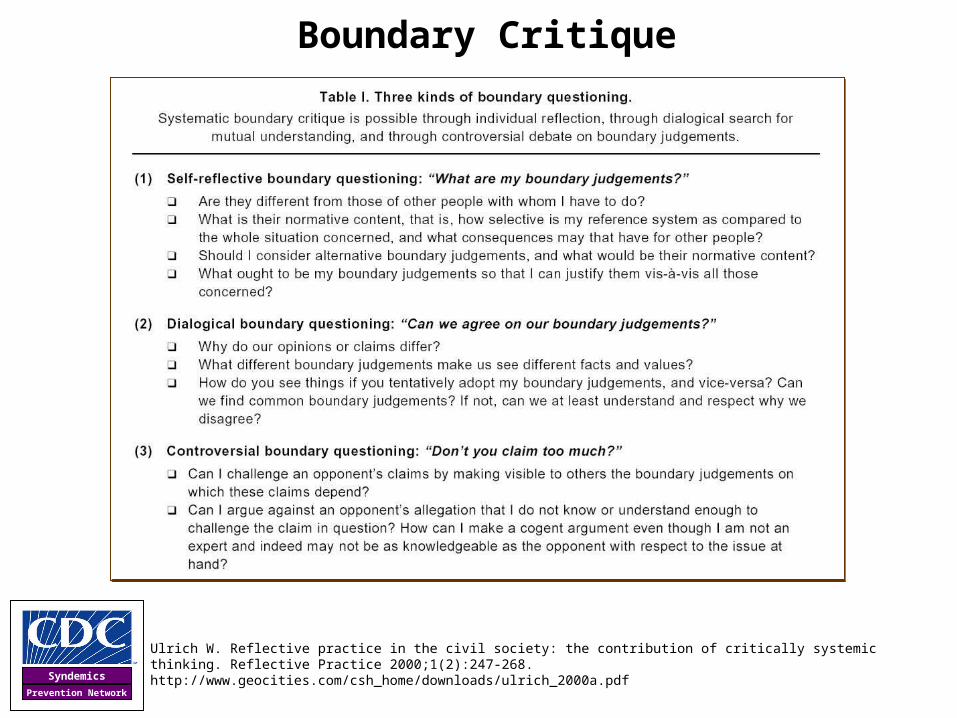
Ulrich W. Reflective practice in the civil society: the contribution of critically systemic thinking. Reflective Practice 2000;1(2):247-268. http://www.geocities.com/csh_home/downloads/ulrich_2000a.pdf
Boundary CritiqueCreating a new theory is not like destroying an old barn and erecting a skyscraper in its
place. It is rather like climbing a mountain, gaining new and wider views, discovering unexpected connections between our starting point and its rich environment.
-- Albert Einstein

Syndemics
Prevention Network
Boundary CritiqueEqualizing Experts and Ordinary Citizens
• “Professional expertise does not protect against the need for making boundary judgements…nor does it provide an objective basis for defining boundary judgements. It’s exactly the other way round: boundary judgements stand for the inevitable selectivity and thus partiality of our propositions.
• It follows that experts cannot justify their boundary judgements (as against those of ordinary citizens) by referring to an advantage of theoretical knowledge and expertise.
• When it comes to the problem of boundary judgements, experts have no natural advantage of competence over lay people.”
Ulrich W. Reflective practice in the civil society: the contribution of critically systemic thinking. Reflective Practice 2000;1(2):247-268.
-- Werner Ulrich

Syndemics
Prevention Network
“You Can Argue with Einstein”
Yankelovich D. Coming to public judgment: making democracy work in a complex world. 1st ed Syracuse, NY: Syracuse University Press, 1991. p. 220.
“For certain purposes, public judgment should
carry more weight than expert opinion – and not simply
because the majority may have more political power than
the individual expert but because the public’s claim to
know is actually stronger than the experts’...the judgment
of the general public can, under some conditions, be
equal or superior in quality to the judgment of experts
and elites who possess far more information, education,
and ability to articulate their views.”
-- Daniel Yankelovich
Syndemics
Prevention Network
Ulrich W. Reflective practice in the civil society: the contribution of critically systemic thinking. Reflective Practice 2000;1(2):247-268. http://www.geocities.com/csh_home/downloads/ulrich_2000a.pdf
Boundary Critique

Syndemics
Prevention Network
Epi·demic
• The term epidemic is an ancient word signifying a kind of relationship wherein something unknown (or unknowable) is put upon the people
• Epidemiology first appeared just over a century ago (in 1873), in the title of J.P. Parkin's book "Epidemiology, or the Remote Cause of Epidemic Diseases“
• Ever since then, the conditions that cause health problems have increasingly become matters of public concern and public work
Elliot G. Twentieth century book of the dead. New York,: C. Scribner, 1972.
Martin PM, Martin-Granel E. 2,500-year evolution of the term epidemic. Emerging Infectious Diseases 2006. Available from http://www.cdc.gov/ncidod/EID/vol12no06/05-1263.htm
National Institutes of Health. A Short History of the National Institutes of Health. Bethesda, MD: 2006. Available from http://history.nih.gov/exhibits/history/
Parkin J. Epidemiology; or the remote cause of epidemic diseases in the animal and the vegetable creation. London: J and A Churchill, 1873.
A representation of the cholera epidemic of the nineteenth century.Source: NIH
“The pioneers of public health did not change nature, or men, but adjusted the active relationship of men to certain aspects of nature so that the relationship became one of watchful and healthy respect.”
-- Gil Elliot

Syndemics
Prevention Network
Syn·demic
• The term syndemic, first used in 1992, strips away the idea that illnesses originate from extraordinary or supernatural forces and places the responsibility for affliction squarely within the public arena
• It acknowledges relationships and signals a commitment to studying population health as a a fragile, dynamic state requiring continual effort to maintain and one that is imperiled when social and physical forces operate in harmful ways
Confounding
Connecting*
Synergism
Syndemic
Events
System
Co-occurring
* Includes several forms of connection or inter-connection such as synergy, intertwining, intersecting, and overlapping
Milstein B. Hygeia's constellation: navigating health futures in a dynamic and democratic world. Doctoral dissertation. Cincinnati, OH: Union Institute and University. November, 2006.
Milstein B. Spotlight on syndemics. Centers for Disease Control and Prevention, 2001. <http://www.cdc.gov/syndemics>

Syndemics
Prevention Network
Milstein B, Homer J. The dynamics of upstream and downstream: why is so hard for the health system to work upstream, and what can be done about it? CDC Futures Health Systems Workgroup; Atlanta, GA; 2003.
TertiaryPrevention
SecondaryPrevention
PrimaryPrevention
TargetedProtection
Society's HealthResponse
Demand forresponse
PublicWork
SaferHealthierPeople Becoming
vulnerable
Becoming saferand healthier
VulnerablePeople Becoming
afflicted
Afflictedwithout
Complications Developingcomplications
Afflicted withComplications
Dying fromcomplications
Health System Dynamics
Adverse LivingConditions
GeneralProtection
Milstein B, Homer J. The dynamics of upstream and downstream: why is so hard for the health system to work upstream, and what can be done about it? CDC Futures Health Systems Work Group; Atlanta, GA; December 3, 2003.
Gerberding JL. CDC's futures initiative. Atlanta, GA: Public Health Training Network; April 12, 2004.
Gerberding JL. FY 2008 CDC Congressional Budget Hearing. Testimony before the Committee on Appropriations, Subcommittee on Labor, Health and Human Services, Education and Related Agencies, United States House of Representatives; Washington, DC; March 9, 2007.
Homer JB, Hirsch GB. System dynamics modeling for public health: background and opportunities. American Journal of Public Health 2006;96(3):452-458.
“One major task that CDC is intending to address is balancing this portfolio of our health system so that there is much greater emphasis placed on health protection, on making sure that we invest the same kind of intense resources into keeping people
healthier or helping them return to a state of health and low vulnerability as we do to disease care and end of life care."
-- Julie Gerberding

Syndemics
Prevention Network
Understanding Health as Public Work
SaferHealthierPeople
VulnerablePeople
Afflictedwithout
Complications
Afflicted withComplicationsBecoming
vulnerable
Becoming saferand healthier
Becomingafflicted
Developingcomplications
Dying fromcomplications
Adverse LivingConditions
Society's HealthResponse
Demand forresponse
GeneralProtection
TargetedProtection
PrimaryPrevention
SecondaryPrevention
TertiaryPrevention
-
Public Work-
Vulnerable andAfflicted People
Fraction of Adversity,Vulnerability and AfflictionBorne by Disadvantaged
Sub-Groups (Inequity)
-
PublicStrength
Citizen Involvementin Public Life
Social Division

Syndemics
Prevention Network
Evaluating Dynamic, Democratic Policies
How can we learn about the consequences of alternative policies in a system of this kind?
SaferHealthierPeople
VulnerablePeople
Afflictedwithout
Complications
Afflicted withComplicationsBecoming
vulnerable
Becoming saferand healthier
Becomingafflicted
Developingcomplications
Dying fromcomplications
Adverse LivingConditions
Society's HealthResponse
Demand forresponse
GeneralProtection
TargetedProtection
PrimaryPrevention
SecondaryPrevention
TertiaryPrevention
-
Public Work-
Vulnerable andAfflicted People
Fraction of Adversity,Vulnerability and AfflictionBorne by Disadvantaged
Sub-Groups (Inequity)
PublicStrength
-
Citizen Involvementin Public Life
Social Division
Syndemics
Prevention Network
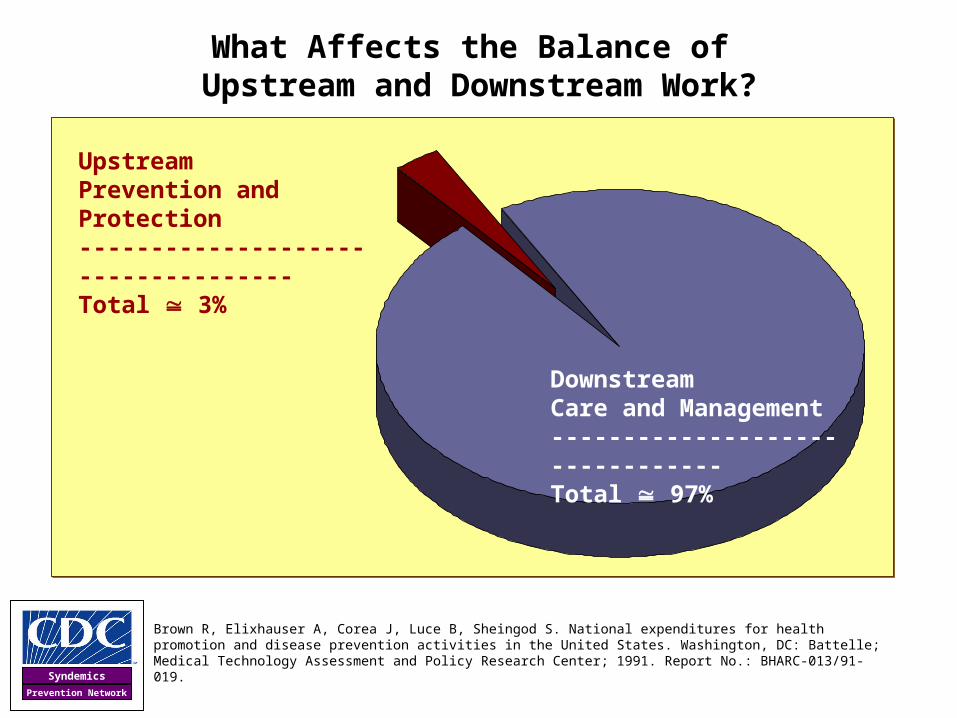
What Affects the Balance of Upstream and Downstream Work?
Upstream Prevention and Protection-----------------------------------Total 3%
Downstream Care and Management--------------------------------Total 97%
Brown R, Elixhauser A, Corea J, Luce B, Sheingod S. National expenditures for health promotion and disease prevention activities in the United States. Washington, DC: Battelle; Medical Technology Assessment and Policy Research Center; 1991. Report No.: BHARC-013/91-019.

Syndemics
Prevention Network
Balancing Two Major Areas of Emphasis
SaferHealthierPeople
VulnerablePeople
Afflictedwithout
ComplicationsAfflicted with
ComplicationsBecomingvulnerable
Becoming saferand healthier
Becomingafflicted
Developingcomplications
Dying fromcomplications
Adverse LivingConditions
Society's HealthResponse
Demand forresponse
GeneralProtection
TargetedProtection
PrimaryPrevention
SecondaryPrevention
TertiaryPrevention
Public Work
World of Providing…
• Education• Screening• Disease management • Pharmaceuticals• Clinical services• Physical and financial access• Etc…
Medical and Public Health Policy
MANAGEMENT OF DISEASES AND RISKS
World of Transforming…
• Deprivation• Dependency• Violence• Disconnection• Environmental decay• Stress• Insecurity• Etc…
By Strengthening…
• Leaders and institutions• Foresight and precaution• The meaning of work• Mutual accountability• Plurality• Democracy• Freedom• Etc…
Healthy Public Policy & Public Work
DEMOCRATIC SELF-GOVERNANCE
Milstein B. Hygeia's constellation: navigating health futures in a dynamic and democratic world. Doctoral dissertation. Cincinnati, OH: Union Institute and University. November, 2006.

Syndemics
Prevention Network
Two Broad Types of Policy
Types of Policy
Upstream Downstream
Type• Macro policy• System-wide scope
• Micro policy• Sector-specific scope
Examples
• Guaranteed living wage• War and the preparation for war• Regulation of “private” corporate
behavior
• Breast cancer screening• Educational testing• Housing vouchers
Procedures • “High politics” • “Low politics”
Crick BR. In defense of politics. 4th ed Chicago, IL: University of Chicago Press, 1993.
Walt G. Health policy: an introduction to process and power. Atlantic Highlands, NJ: Zed Books, 1994.

Syndemics
Prevention Network
Defining Keywords
Crick BR. In defense of politics. 4th ed Chicago, IL: University of Chicago Press, 1993.
Boyte HC. Everyday politics: reconnecting citizens and public life. Philadelphia, PA: University of Pennsylvania Press, 2004.
• PartisanFervent, sometimes militant support for a party, cause, faction, person, or idea, from Middle French, part, “faction”
• PoliticalThe action of diverse people negotiating their differences for common governance, from the Greek, politikos, “of the citizen”
Syndemics
Prevention Network
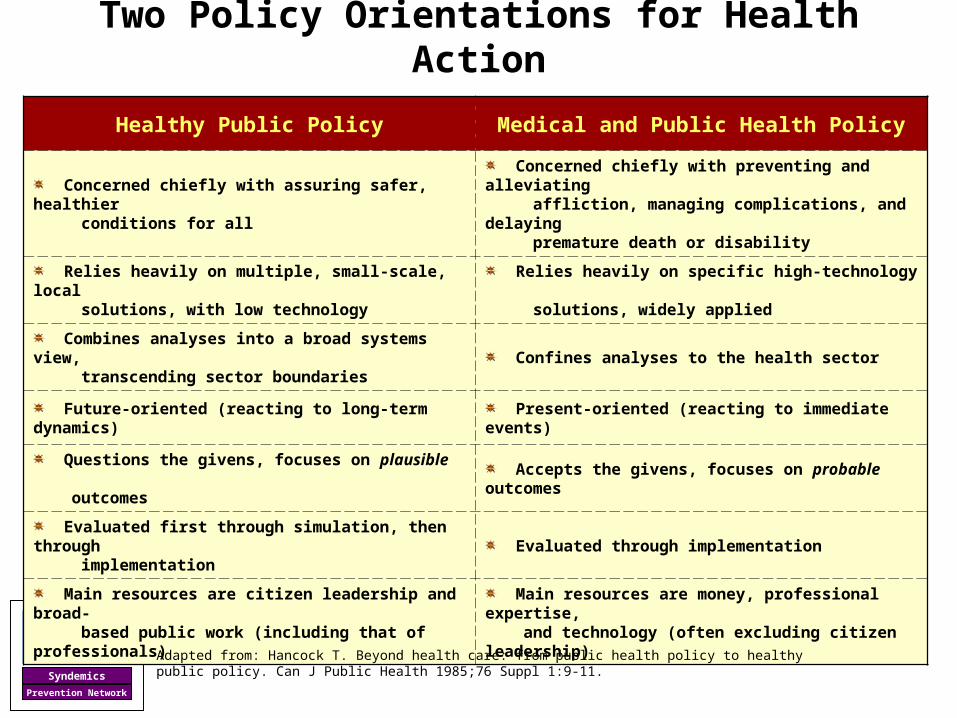
Healthy Public Policy Medical and Public Health Policy
Concerned chiefly with assuring safer, healthier conditions for all
Concerned chiefly with preventing and alleviating affliction, managing complications, and delaying premature death or disability
Relies heavily on multiple, small-scale, local solutions, with low technology
Relies heavily on specific high-technology solutions, widely applied
Combines analyses into a broad systems view, transcending sector boundaries
Confines analyses to the health sector
Future-oriented (reacting to long-term dynamics) Present-oriented (reacting to immediate events)
Questions the givens, focuses on plausible outcomes
Accepts the givens, focuses on probable outcomes
Evaluated first through simulation, then through implementation
Evaluated through implementation
Main resources are citizen leadership and broad- based public work (including that of professionals)
Main resources are money, professional expertise, and technology (often excluding citizen leadership)
Two Policy Orientations for Health Action
Adapted from: Hancock T. Beyond health care: from public health policy to healthy public policy. Can J Public Health 1985;76 Suppl 1:9-11.

Syndemics
Prevention Network
Healthy Public Policy Medical and Public Health Policy
Concerned chiefly with assuring safer, healthier conditions for all
Concerned chiefly with preventing and alleviating affliction, managing complications, and delaying premature death or disability
Relies heavily on multiple, small-scale, local solutions, with low technology
Relies heavily on specific high-technology solutions, widely applied
Combines analyses into a broad systems view, transcending sector boundaries
Confines analyses to the health sector
Future-oriented (reacting to long-term dynamics) Present-oriented (reacting to immediate events)
Questions the givens, focuses on plausible outcomes
Accepts the givens, focuses on probable outcomes
Evaluated first through simulation, then through implementation
Evaluated through implementation
Main resources are citizen leadership and broad- based public work (including that of professionals)
Main resources are money, professional expertise, and technology (often excluding citizen leadership)
Two Policy Orientations for Health Action
Adapted from: Hancock T. Beyond health care: from public health policy to healthy public policy. Can J Public Health 1985;76 Suppl 1:9-11.
Syndemics
Prevention Network
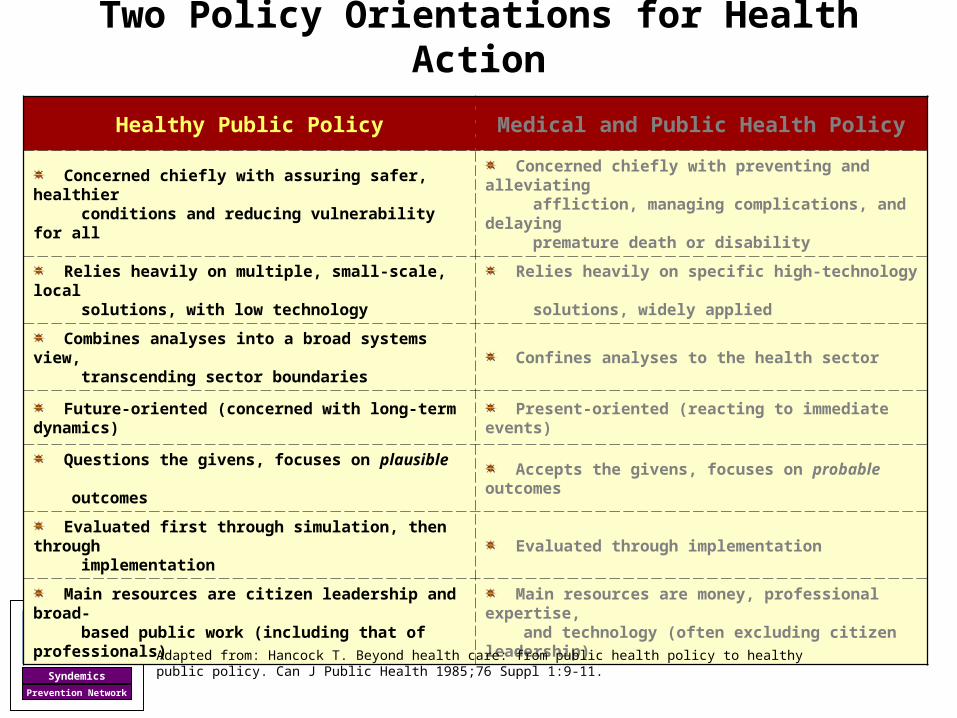
Healthy Public Policy Medical and Public Health Policy
Concerned chiefly with assuring safer, healthier conditions and reducing vulnerability for all
Concerned chiefly with preventing and alleviating affliction, managing complications, and delaying premature death or disability
Relies heavily on multiple, small-scale, local solutions, with low technology
Relies heavily on specific high-technology solutions, widely applied
Combines analyses into a broad systems view, transcending sector boundaries
Confines analyses to the health sector
Future-oriented (concerned with long-term dynamics) Present-oriented (reacting to immediate events)
Questions the givens, focuses on plausible outcomes
Accepts the givens, focuses on probable outcomes
Evaluated first through simulation, then through implementation
Evaluated through implementation
Main resources are citizen leadership and broad- based public work (including that of professionals)
Main resources are money, professional expertise, and technology (often excluding citizen leadership)
Two Policy Orientations for Health Action
Adapted from: Hancock T. Beyond health care: from public health policy to healthy public policy. Can J Public Health 1985;76 Suppl 1:9-11.

Syndemics
Prevention Network
Looking Backward Retrospective Policy Evaluation

Syndemics
Prevention Network
Adult Per Capita Cigarette Consumption and Major Smoking and Health Events
United States, 1900-1998
U.S. Department of Health and Human Services. Reducing tobacco use: a report of the Surgeon General. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; 2000. Available at <http://www.cdc.gov/tobacco/data_statistics/sgr/sgr_2000/index.htm#full>.
1st SurgeonGeneral’s
Report
1st Smoking-Cancer Concern
NonsmokersRights Movement Begins
BroadcastAd Ban
Federal CigaretteTax Doubles
0
1,000
2,000
3,000
4,000
5,000
1900 1910 1920 1930 1940 1950 1960 1970 1980 1990
Nu
mb
er o
f C
igar
ette
s
Health promotion does not seek to control for secular trends.
It tries to create them!
-- Marshall Kreuter
Health promotion does not seek to control for secular trends.
It tries to create them!
-- Marshall Kreuter

Syndemics
Prevention Network
Tracking Statewide Tobacco Control Efforts
California Department of Health Services. California tobacco control update: the social norm change approach. Sacramento, CA: Tobacco Control Section, California Department of Health Services 2006. <http://www.dhs.ca.gov/tobacco/documents/pubs/CTCUpdate2006.pdf>.

Syndemics
Prevention Network
What was Happening in California?
Comprehensive policy featuring…
• Statewide focus
• Community programs to reduce tobacco use
• Chronic disease programs to reduce the burden of tobacco-related diseases
• School-based efforts
• Enforcement
• Counter-marketing
• Cessation programs
• Surveillance and evaluation
• Administration and management

Syndemics
Prevention Network
Green LW. A federal agency's journey from bootstrap epidemiology to evidence-based practice to practice-based evidence. 4th Annual CDC Evaluation Summer Institute; Atlanta, GA: Centers for Disease Control and Prevention; June 10, 2004. Available at <http://www.chronicdisease.org/SEpresentations/GREEN--CDC%20Evidence-Based%20Prax%20to%20Prax-Based%20Evidence.ppt>.
The Comprehensiveness Imperative
• Interventions by themselves ineffective when taken to scale
• In trying to isolate the essential components of tobacco control programs that made them effective, none could be shown to stand alone
• Any combination of methods was more effective than the individual methods
• The more components, the more effective
• The more components, the better coverage
What was Happening in California?

Syndemics
Prevention Network
Observed blood lead
U.S. Policy Response to Concerns About Elevated Blood Lead Levels
Year
1975 1976 1977 1978 1979 1980 1981
Mean bloodlead levels
(g/dL)
9
10
11
12
13
14
15
16
17
Gasoline lead
Predicted blood lead
Data: National Health and Nutrition Examination Survey II
Lead used ingasoline
(thousandsof tons)
30
40
50
60
70
80
90
100
110
Intervention Effect: Blood lead fell 10 times
more than predicted!
Intervention Effect: Blood lead fell 10 times
more than predicted!
Syndemics
Prevention Network
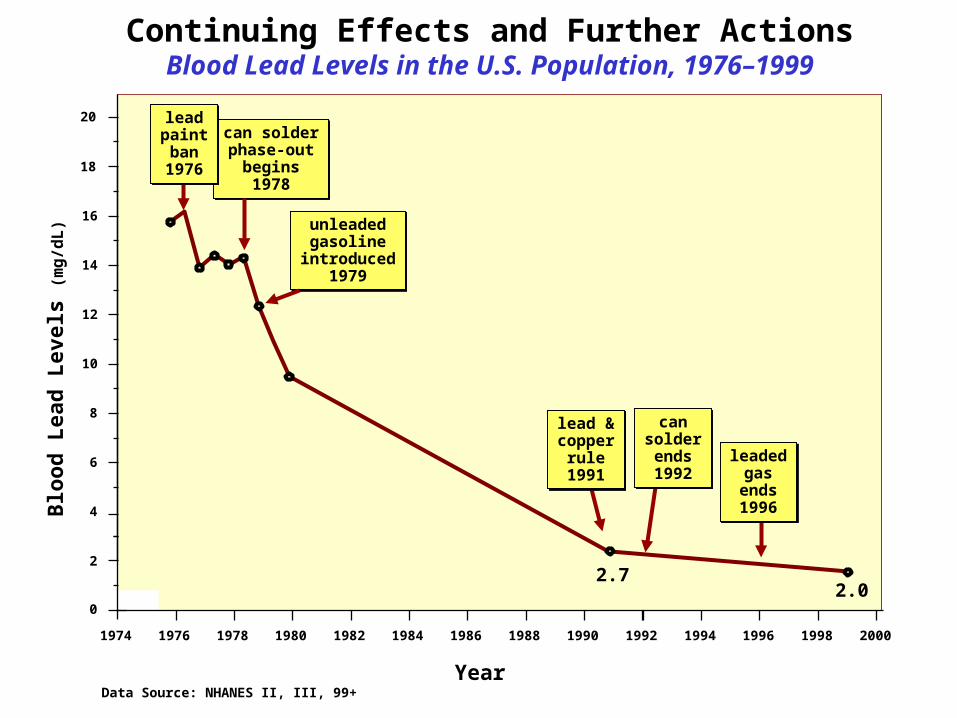
Continuing Effects and Further ActionsBlood Lead Levels in the U.S. Population, 1976–1999
1974 1976 1978 1980 1982 1984 1986 1988 1990 1992 1994 1996 1998 2000
Year
18
2
4
6
8
10
12
14
16
Blo
od
Lea
d L
evel
s (m
g/d
L)
0
2.72.0
unleadedgasoline
introduced1979
unleadedgasoline
introduced1979
can solderphase-out
begins1978
can solderphase-out
begins1978
leadpaintban1976
leadpaintban1976
lead &copper
rule1991
lead &copper
rule1991
cansolderends1992
cansolderends1992
leadedgas
ends1996
leadedgas
ends1996
20
Data Source: NHANES II, III, 99+

Syndemics
Prevention Network
Lead-Based Paint in Housing
• 24 million housing units (25% of the nation’s housing) have significant lead-based paint hazards
• 1.2 million homes with significant lead-based paint hazards housed low income families with children under the age of 6
Source: National Lead-Based Paint Survey (1998-2000)Source: National Lead-Based Paint Survey (1998-2000)

Syndemics
Prevention Network
Puska P. The North Karelia Project: 20 year results and experiences. Helsinki: National Public Health Institute, 1995.
National Public Health Institute. North Karelia international visitor's programme. National Public Health Institute, 2003. Available at <http://www.ktl.fi/eteo/cindi/northkarelia.html>.
Navigational VenturesFinland’s North Karelia Project

Syndemics
Prevention Network
Puska P. The North Karelia Project: 20 year results and experiences. Helsinki: National Public Health Institute, 1995
Focusing the Intervention Policy
Policy A: Focus on High Risk Individuals
Policy B: Focus on Risk Conditions for All
Syndemics
Prevention Network
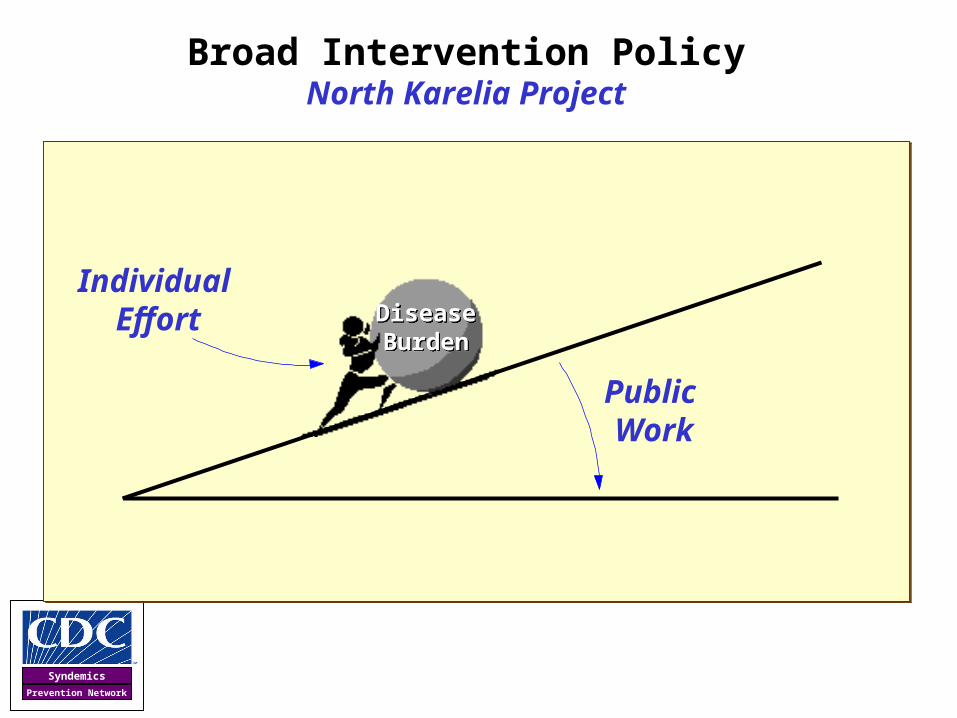
Broad Intervention PolicyNorth Karelia Project
Disease Burden
Disease Burden
Individual Effort
Public Work

Syndemics
Prevention Network
Directing ChangeNorth Karelia Project
Selected Action Strategies
• Medical services, if necessary
• Newspaper coverage: articles, editorials, letters
• TV time: highly rated 30-45 minute shows (no PSAs)
• Housewives’ organization: cooking and dietary choices
• Opinion leaders: role models, support groups, public action
• Tax shifting: tobacco, butter, milk
• Economic Renewal– Decline of dairy – Rise of berry – Rise of vegetable oil and rapeseed oil– Rise of healthier breads, cheeses, sausages, etc
Puska P. The North Karelia Project : 20 year results and experiences. Helsinki: National Public Health Institute, 1995.

Syndemics
Prevention Network
Transforming All Dimensionsof the System
Health
LivingConditions
Power toAct
Efforts to Fight Afflictions
Efforts to Improve Adverse Living Conditions
Efforts to Build Power

Syndemics
Prevention Network
Efforts to Fight Afflictions (design/deliver)
• Screening
• Education
• Risk reduction counseling
• Medical/pharmaceutical treatment
• Disease self-management
Directing ChangeNorth Karelia Project

Syndemics
Prevention Network
Efforts to Improve Adverse Living Conditions (develop/promote)
• Tobacco legislation
• Food-labeling requirements
• Margarines and oils
• Low-fat milk
• Low-fat, low-salt, high-fiber bread
• Vegetable-containing sausage (with mushrooms)
• Berry farming and consumption
• Community competitions, morale, and social norms
• State welfare system (at the national, regional, sub-regional, and local levels)
Directing ChangeNorth Karelia Project

Syndemics
Prevention Network
Health Professionals
• Physicians
• Health Educators
• Psychologists
• Epidemiologists
• Sociologists
• Hospital administrators
• Pharmaceutical manufacturers
• Nurses
• Rehabilitation therapists
Other Citizens
• Bakers
• Farmers
• Grocers
• Food scientists, manufacturers
• Restaurant owners
• Housewives
• Entertainers
• Entrepreneurs
• Journalists, media professionals
• Teachers
• School administrators
• Elected representatives
Building PowerNorth Karelia Project

Syndemics
Prevention Network
Charting ProgressNorth Karelia Project
Vartiainen E, Puska P, Pekkanen J, Toumilehto J, Jousilahti P. Changes in risk factors explain changes in mortality from ischaemic heart disease in Finland. British Medical Journal 1994;309(6946):23-27.

Syndemics
Prevention Network
Mortality changes in North Karelia in 1970-1995 (per 100 000, 35-64 years, men, age adjusted)
0
200
400
600
800
1000
1200
1400
1600
All Causes All CVD CHD All Cancers Lung CancerCause of Death
Ra
te p
er
10
0,0
00
1979
1995
-49%
-68%-73%
-44%-71%
Puska P. The North Karelia Project : 20 year results and experiences. Helsinki: National Public Health Institute, 1995.
National Public Health Institute. North Karelia international visitor's programme. National Public Health Institute, 2003. Accessed May 30, 2004 at <http://www.ktl.fi/eteo/cindi/northkarelia.html>.
Charting ProgressNorth Karelia Project

Syndemics
Prevention Network
Looking Forward Prospective Policy Evaluation
Featuring Systems Thinking & Modeling

Syndemics
Prevention Network
Milstein B, Homer J. The dynamics of upstream and downstream: why is so hard for the health system to work upstream, and what can be done about it? CDC Futures Health Systems Workgroup; Atlanta, GA; 2003.
TertiaryPrevention
SecondaryPrevention
PrimaryPrevention
TargetedProtection
Society's HealthResponse
Demand forresponse
PublicWork
SaferHealthierPeople Becoming
vulnerable
Becoming saferand healthier
VulnerablePeople Becoming
afflicted
Afflictedwithout
Complications Developingcomplications
Afflicted withComplications
Dying fromcomplications
Health System Dynamics
Adverse LivingConditions
GeneralProtection
Milstein B, Homer J. The dynamics of upstream and downstream: why is so hard for the health system to work upstream, and what can be done about it? CDC Futures Health Systems Work Group; Atlanta, GA; December 3, 2003.
Gerberding JL. CDC's futures initiative. Atlanta, GA: Public Health Training Network; April 12, 2004.
Gerberding JL. FY 2008 CDC Congressional Budget Hearing. Testimony before the Committee on Appropriations, Subcommittee on Labor, Health and Human Services, Education and Related Agencies, United States House of Representatives; Washington, DC; March 9, 2007.
Homer JB, Hirsch GB. System dynamics modeling for public health: background and opportunities. American Journal of Public Health 2006;96(3):452-458.
“One major task that CDC is intending to address is balancing this portfolio of our health system so that there is much greater emphasis placed on health protection, on making sure that we invest the same kind of intense resources into keeping people
healthier or helping them return to a state of health and low vulnerability as we do to disease care and end of life care."
-- Julie Gerberding

Syndemics
Prevention Network
• PossibleWhat may happen?
• PlausibleWhat could happen?
• ProbableWhat will likely happen?
• PreferableWhat do we want to have happen?
Bezold C, Hancock T. An overview of the health futures field. Geneva: WHO Health Futures Consultation; 1983 July 19-23.
“Most organizations plan around what is most likely. In so doing they reinforce what is, even though they want
something very different.”
-- Clement Bezold
Seeing Beyond the Probable

Syndemics
Prevention Network
Diseasemgmt
Riskmgmt
Riskprevention
Urgent &long-term care
A “Bathtub” View of Chronic Illness Dynamics
Low risk
High risk
Mildly ill
Severely ill
Risk onset
Illness onset
Complications onset
Death
Bathtubs = Accumulations = Stocks;
Drains & Faucets = Flows
Bathtubs = Accumulations = Stocks;
Drains & Faucets = Flows
Booth-Sweeney LB, Sterman JD. Bathtub dynamics: initial results of a systems thinking inventory. System Dynamics Review 2000;16(4):249-286.

Syndemics
Prevention Network
Re-Directing the Course of ChangeQuestions Addressed by System Dynamics Modeling
How?
Where?
0
10
20
30
40
50
1960-62 1971-74 1976-80 1988-94 1999-2002
Prevalence of Obese Adults, United States
Why?
Data Source: NHANES
20202010
Who?
What?
Simulation Experiments
in Action Labs

Syndemics
Prevention Network
Simulations for Learning in Dynamic Systems
Morecroft JDW, Sterman J. Modeling for learning organizations. Portland, OR: Productivity Press, 2000.
Sterman JD. Business dynamics: systems thinking and modeling for a complex world. Boston, MA: Irwin McGraw-Hill, 2000.
Multi-stakeholder Dialogue
Dynamic Hypothesis (Causal Structure)
X Y
Plausible Futures (Policy Experiments)
Obese fraction of Adults (Ages 20-74)
0%
10%
20%
30%
40%
50%
1970 1980 1990 2000 2010 2020 2030 2040 2050
Fra
ctio
n o
f p
op
n 2
0-74

Syndemics
Prevention Network
A Model Is…
An inexact representation of the real thing
It helps us understand, explain, anticipate, and make decisions
“All models are wrong, some are useful.”
-- George Box
“All models are wrong, some are useful.”
-- George Box
Syndemics
Prevention Network
CDC Obesity Dynamics Modeling Project Contributors
Core Design Team• Dave Buchner• Andy Dannenberg• Bill Dietz• Deb Galuska• Larry Grummer-Strawn• Anne Hadidx• Robin Hamre• Laura Kettel-Khan• Elizabeth Majestic • Jude McDivitt• Cynthia Ogden• Michael Schooley
System Dynamics Consultants• Jack Homer• Gary Hirsch
Time Series Analysts
• Danika Parchment
• Cynthia Ogden
• Margaret Carroll
• Hatice Zahran
Project Coordinator• Bobby Milstein
Workshop Participants• Atlanta, GA: May 17-18 (N=47)• Lansing, MI: July 26-27 (N=55)
Homer J, Milstein B, Dietz W, Buchner D, Majestic D. Obesity population dynamics: exploring historical growth and plausible futures in the U.S. 24th International Conference of the System Dynamics Society; Nijmegen, The Netherlands; July 26, 2006.
Cover of "The Economist", Dec. 13-19, 2003Cover of "The Economist", Dec. 13-19, 2003.

Syndemics
Prevention Network
Phase 2:
More Detailed Drivers of Change
Obesity Prevalence Over the Decades Two Broad Phases
Consequences Over TimeChanging Prevalence of
Four BMI Categories: 1970-2050
Dynamic Population Weight Framework(BMI Surveillance, Demography, and
Nutritional Science)
Policy Drivers(Trends & Interventions
Affecting Caloric Balance by Age, Sex, BMI Category, etc…)
Phase 1: Calculating Obesity Dynamics
Policy Drivers(Trends & Interventions
Affecting Caloric Balance by Age, Sex, BMI Category, etc…)
Syndemics
Prevention Network
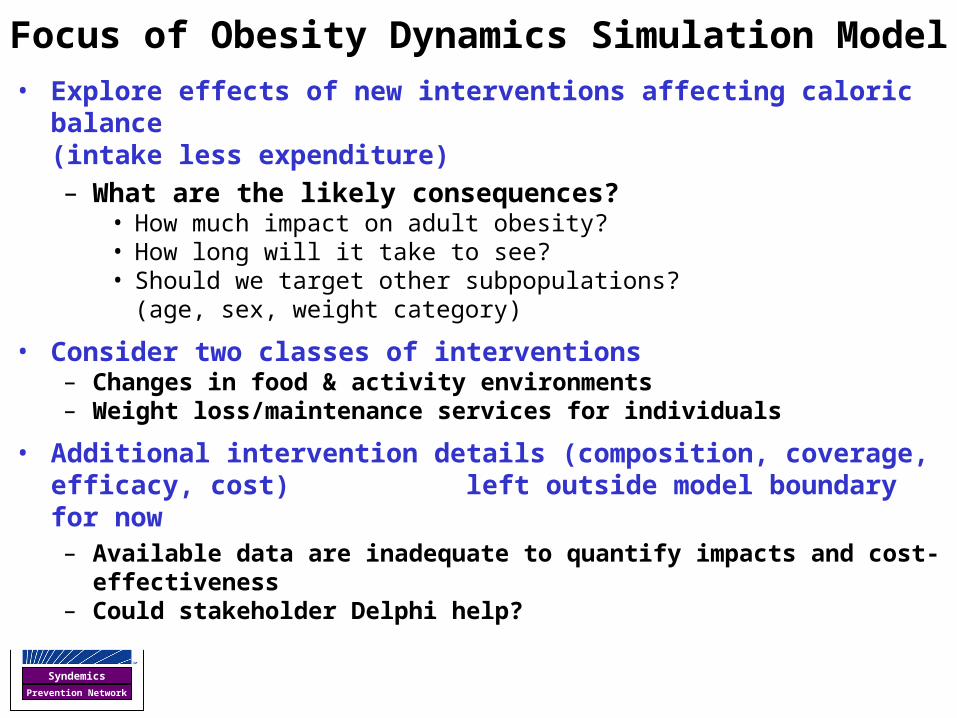
Focus of Obesity Dynamics Simulation Model• Explore effects of new interventions affecting caloric balance
(intake less expenditure) – What are the likely consequences?
• How much impact on adult obesity?• How long will it take to see?• Should we target other subpopulations?
(age, sex, weight category)
• Consider two classes of interventions– Changes in food & activity environments – Weight loss/maintenance services for individuals
• Additional intervention details (composition, coverage, efficacy, cost) left outside model boundary for now– Available data are inadequate to quantify impacts and cost-effectiveness – Could stakeholder Delphi help?

Syndemics
Prevention Network
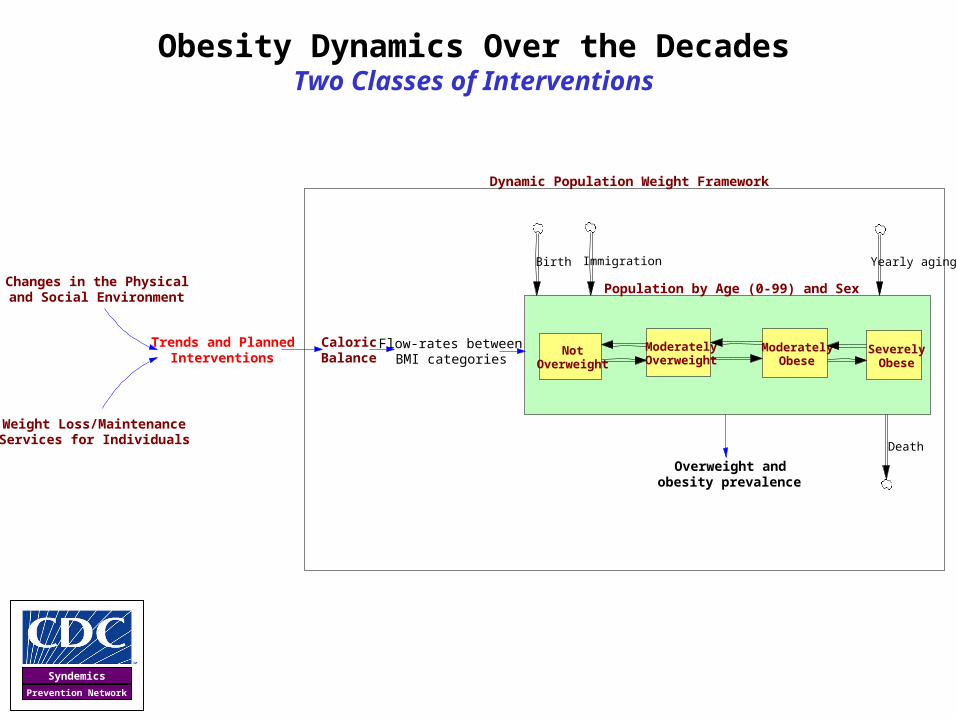
Obesity Dynamics Over the Decades Dynamic Population Weight Framework
Dynamic Population Weight Framework
Population by Age (0-99) and Sex
Flow-rates betweenBMI categories
Overweight andobesity prevalence
Birth Immigration
Death
CaloricBalance
Yearly aging
NotOverweight
ModeratelyOverweight
ModeratelyObese
SeverelyObese

Syndemics
Prevention Network
Obesity Prevalence Over the DecadesDynamic Population Weight Framework
NotOverweight
ModeratelyOverweight
ModeratelyObese
SeverelyObese
NotOverweight
ModeratelyOverweight
ModeratelyObese
SeverelyObese
NotOverweight
ModeratelyOverweight
ModeratelyObese
SeverelyObese
Births Births Births Births
Age 0
Age 1
Age 99
No Change in BMI Category (maintenance flow)
Increase in BMI Category (up-flow)
Decline in BMI Category (down-flow)

Syndemics
Prevention Network
Information Sources
Topic Area Data Source
Prevalence of Overweight and Obesity
BMI prevalence by sex and age (10 age ranges)National Health and Nutrition Examination Survey (1971-2002)
Translating Caloric Balances into BMI Flow-Rates
BMI category cut-points for children and adolescents
CDC Growth Charts
Median BMI within each BMI category National Health and Nutrition Examination Survey (1971-2002)Median height
Average kilocalories per kilogram of weight change
Forbes 1986
Estimating BMI Category Down-Flow Rates
In adults: Self-reported 1-year weight change by sex and age
NHANES (2001-2002) *indicates 7-12% per year*
In children: BMI category changes by grade and starting BMI
Arkansas pre-K through 12th grade assessment (2004-2005) *indicates 15-28% per year*
Population Composition
Population by sex and ageU.S. Census and Vital Statistics (1970-2000 and projected)
Death rates by sex and age
Birth and immigration rates
Influence of BMI on Mortality
Impact of BMI category on death rates by age Flegal, Graubard, et al. 2005.

Syndemics
Prevention Network
(a) Overweight fraction
0%
20%
40%
60%
80%
1970 1975 1980 1985 1990 1995 2000 2005
Fra
ctio
n o
f w
om
en a
ge
55-6
4
NHANES Simulated
(b) Obese fraction
0%
10%
20%
30%
40%
50%
1970 1975 1980 1985 1990 1995 2000 2005
Fra
ctio
n o
f w
om
en a
ge
55-6
4
NHANES Simulated
(c) Severely obese fraction
0%
5%
10%
15%
20%
25%
1970 1975 1980 1985 1990 1995 2000 2005
Fra
ctio
n o
f w
om
en a
ge
55-6
4
NHANES Simulated
Reproducing Historical Trends One of 20 {sex, age} Subgroups: Females age 55-64
Note: S-shaped curves, with inflection in the 1990s
Syndemics
Prevention Network
Obesity Dynamics Over the DecadesTwo Classes of Interventions
Dynamic Population Weight Framework
Population by Age (0-99) and Sex
Flow-rates betweenBMI categories
Overweight andobesity prevalence
Birth Immigration
Death
CaloricBalance
Yearly aging
NotOverweight
ModeratelyOverweight
ModeratelyObese
SeverelyObese
Trends and PlannedInterventions
Changes in the Physicaland Social Environment
Weight Loss/MaintenanceServices for Individuals

Syndemics
Prevention Network
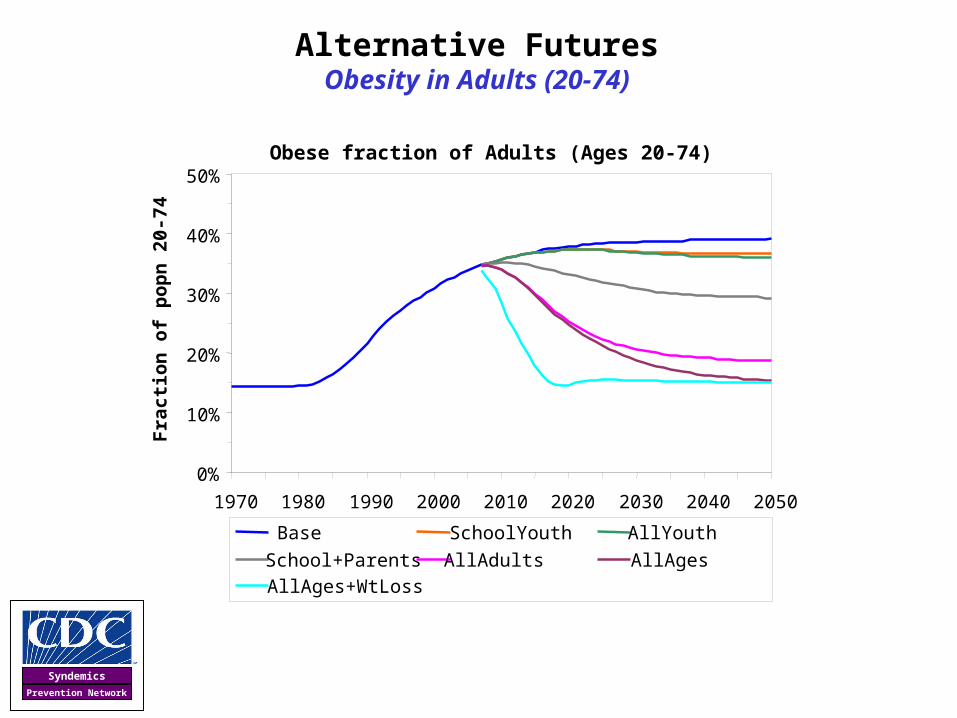
Assumptions for Future Scenarios
Base Case• Caloric balances stay at 2000 values through 2050
Altering Food and Activity Environments
• Reduce caloric balances to their 1970 values by 2015
• Focused on
– ‘School Youth’: youth ages 6-19
– ‘All Youth’: all youth ages 0-19
– ‘School+Parents’: school youth plus their parents
– ‘All Adults’: all adults ages 20+
– ‘All Ages’: all youth and adults
Subsidized Weight Loss Programs for Obese Individuals
• Net daily caloric reduction of program is 40 calories/day (translates to 1.8 kg weight loss per year)
• Fully effective by 2010 and terminated by 2020
Syndemics
Prevention Network
Alternative FuturesObesity in Adults (20-74)
Obese fraction of Adults (Ages 20-74)
0%
10%
20%
30%
40%
50%
1970 1980 1990 2000 2010 2020 2030 2040 2050
Fra
cti
on
of
po
pn
20-
74
Base SchoolYouth AllYouth
School+Parents AllAdults AllAges
AllAges+WtLoss

Syndemics
Prevention Network
U.S. policy discourse is primarily focused on:
• Prevention among school-aged youth
• Medical treatment for the severely obese
Syndemics
Prevention Network
Findings & Limitations
• This model improves our understanding of obesity dynamics and supports pragmatic planning and evaluation– Traces plausible impacts of intervention and addresses questions of
whom to target, by how much, and by when
– Inflection point in obesity probably occurred during the 1990s
– Impacts of changing environments on adult obesity take decades to play out fully: “Carryover effect”
– Youth interventions have only small impact on overall adult obesity (assuming adult habits are determined primarily by adult environment)
– Effective weight-loss for the obese could greatly accelerate progress—but is there a realistic alternative to risky bariatric surgery?
• But it has limitations related to its narrow scope – Does not indicate exact nature of trends and interventions affecting
caloric intake, nor cost-effectiveness nor likely socio-political responses (reinforcing or resistant) of interventions
– Concentrating on detailed life stage data came at expense of a broader analysis of trends, interventions, and feedback effects

Syndemics
Prevention Network
Mokdad AH, Bowman BA, Ford ES, Vinicor F, Marks JS, Koplan JP. The continuing epidemics of obesity and diabetes in the United States. Journal of the American Medical Association 2001;286(10):1195-200.
Kaufman FR. Diabesity: the obesity-diabetes epidemic that threatens America--and what we must do to stop it. New York, NY: Bantam Books, 2005.

Syndemics
Prevention Network
CDC Diabetes System Modeling ProjectDiscovering Stock-Flow Dynamics Through Action Labs
Jones AP, Homer JB, Murphy DL, Essien JDK, Milstein B, Seville DA. Understanding diabetes population dynamics through simulation modeling and experimentation. American Journal of Public Health 2006;96(3):488-494.

Syndemics
Prevention Network
Project Background
• Diabetes programs face tough challenges and questions
– Pressure for results on disease burden, not just behavioral change
– Diabetes Prevention Program indicates primary prevention is possible, but may be difficult and costly
– What is achievable on a population level?
– How should funds be allocated?
• Standard epidemiological models rarely address such policy questions
• Starting Fall 2003, CDC initiates System Dynamics modeling project
• Starting Spring 2005, some states join as collaborators in further developing and using the SD model

Syndemics
Prevention Network
Inflow
Volume
Outflow
Developing
Burden ofDiabetes
Total Prevalence(people with diabetes)
Unhealthy Days(per person with
diabetes)
Costs(per person with diabetes)
People withDiagnosedDiabetes
Diagnosis Deaths
abPeople withPrediabetes
Developing
DiabetesOnset
c
d
People withNormal
Blood SugarLevels
PrediabetesOnset
Recovering fromPrediabetes
e
DiabetesManagement
DiabetesDetection
Obesity in theGeneral
Population
PrediabetesDetection &
Management
People withUndiagnosed
Diabetes
Deaths
Overview of Diabetes Stock-and-Flow Model

Syndemics
Prevention Network
Overview of Diabetes Stock-and-Flow Model
Inflow
Volume
Outflow
Developing
Burden ofDiabetes
Total Prevalence(people with diabetes)
Unhealthy Days(per person with
diabetes)
Costs(per person with diabetes)
People withDiagnosedDiabetes
Diagnosis Deaths
abPeople withPrediabetes
Developing
DiabetesOnset
c
d
People withNormal
Blood SugarLevels
PreDiabetesOnset
Recovering fromPreDiabetes
e
DiabetesManagement
DiabetesDetection
Obesity in theGeneral
Population
PrediabetesDetection &
Management
People withUndiagnosed
Diabetes
Deaths
Standard boundary
This larger view takes us beyond standard epidemiological models and most intervention programs
Syndemics
Prevention Network
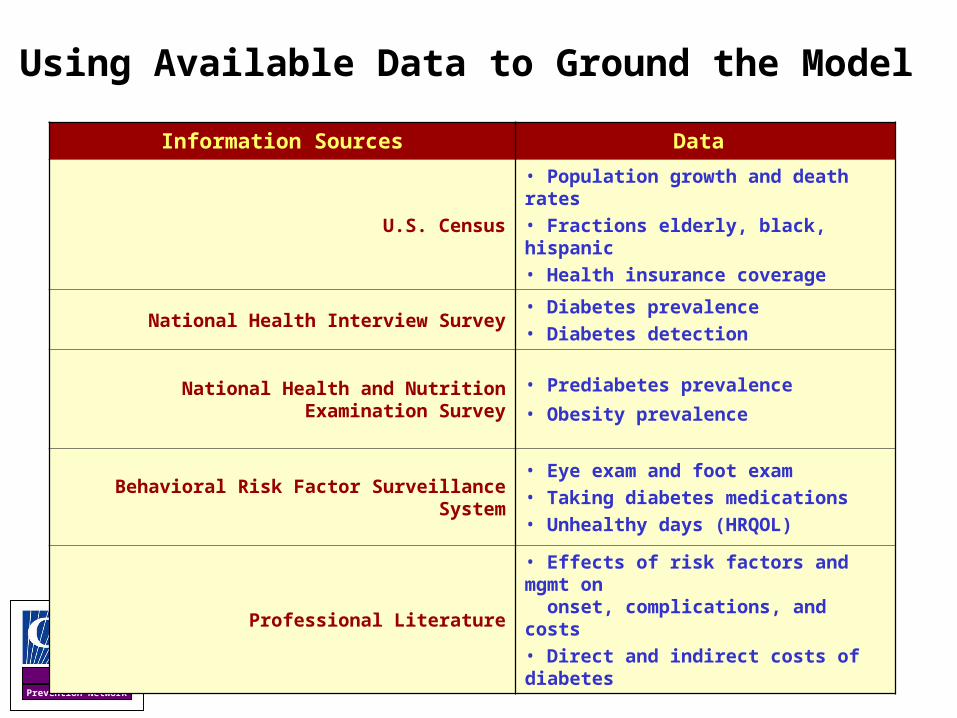
Using Available Data to Ground the Model
Information Sources Data
U.S. Census
• Population growth and death rates• Fractions elderly, black, hispanic• Health insurance coverage
National Health Interview Survey• Diabetes prevalence• Diabetes detection
National Health and Nutrition Examination Survey• Prediabetes prevalence
• Obesity prevalence
Behavioral Risk Factor Surveillance System
• Eye exam and foot exam• Taking diabetes medications• Unhealthy days (HRQOL)
Professional Literature• Effects of risk factors and mgmt on onset, complications, and costs• Direct and indirect costs of diabetes

Syndemics
Prevention Network
One way we establish the model’s value is by looking at its ability to reproduce historical data
(2 variables out of 10 such comparisons)
Diagnosed diabetes per thousand total popn60
45
30
15
0
1980 1984 1988 1992 1996 2000 2004
Model
NHIS
Model
Diagnosed fraction of diabetes popn1
0.8
0.6
0.4
1980 1984 1988 1992 1996 2000 2004
NHANES IIINH
’99 -’00NH II
Homer J. Reference guide for the CDC Diabetes System Model. Atlanta, GA: Division of Diabetes Translation, Centers for Disease Control and Prevention; August, 2006. <<http://sustainer.org/pubs/diabetessystemreference.pdf>.

Syndemics
Prevention Network
Prevalence=92 AND RISING
Although we expect obesity to increase little after 2006, diabetes keeps growing robustly for another 20-25 years
Obese Fraction and Diabetes per Thousand1300.7
850.35
400
1980 1990 2000 2010 2020 2030 2040 2050Time (Year)
Diabetes Prevalenc
e
Obesity Prevalenc
e
Diabetes prevalence keeps growing after
obesity stopsWHY?
With high (even if flat) onset, prevalence tub
keeps filling until deaths (4-5%/yr)=onset
Onset=6.3 per thou
Estimated 2006 values
Death=3.8 per thou
Prevalence=92 / thou

Syndemics
Prevention Network
Unhealthy days impact of prevalence growth, as affected by diabetes management: Past and one possible future
Unhealthy Days per Thou and Frac ManagedObese Fraction and Diabetes per Thousand1300.7
850.35
400
1980 1990 2000 2010 2020 2030 2040 2050Time (Year)
Diabetes Prevalenc
e
Obesity Prevalenc
e
5000.65
25001980 1990 2000 2010 2020 2030 2040 2050
3750.325
Unhealthy Daysfrom Diabetes
Managed
fraction
Diabetes prevalence keeps growing after
obesity stops
If disease management gains end, the burden
grows

Syndemics
Prevention Network
Further Increases in Diabetes Management
People with Diabetes per Thousand Adults150
125
100
75
501980 1990 2000 2010 2020 2030 2040 2050
Monthly Unhealthy Days from Diabetes per Thou500
450
400
350
300
250
1980 1990 2000 2010 2020 2030 2040 2050
Base
Diab mgt Base
More people living with diabetes
Keeping the burden at bay for nine years
longer
Diab mgt
Increase fraction of diagnosed diabetes getting managed from 58% to 80% by 2015. (No change in the mix of conventional and intensive.) What do you think will happen?
Diabetes mgmt does nothing to slow the growth of prevalence—in fact, it
increases it. As soon as diabetes mgmt stops
improving, unhealthy days start to grow as fast as
prevalence.

Syndemics
Prevention Network
Managing Prediabetes AND Reducing Obesity
The more you reduce obesity, the sooner you
stop the growth in diabetes—and the more
you bring it down
… Same with the burden of diabetes
People with Diabetes per Thousand Adults150
125
100
75
50
1980 1990 2000 2010 2020 2030 2040 2050
Monthly Unhealthy Days from Diabetes per Thou500
450
400
350
300
250
1980 1990 2000 2010 2020 2030 2040 2050
Base
PreD mgmt
PreD & Ob 25%
PreD & Ob 18%
Base
PreD mgmt
PreD & Ob 18%
PreD & Ob 25%
What do you think will happen if, in addition to PreD mgmt, obesity is reduced moderately by 2030? What if it is reduced even more?

Syndemics
Prevention Network
Intervening Effectively Upstream AND Downstream
People with Diabetes per Thousand Adults150
125
100
75
50
1980 1990 2000 2010 2020 2030 2040 2050
Monthly Unhealthy Days from Diabetes per Thou500
450
400
350
300
250
1980 1990 2000 2010 2020 2030 2040 2050
Base
PreD mgmt PreD mgmt
Base
PreD & Ob 25%
Pred & Ob 25%
All 3 --PreD & Ob 25% & Diab mgmt
All 3
With a combination of effective upstream and downstream interventions we could hold the burden of diabetes nearly flat
through 2050!
With pure upstream intervention, burden still grows for many years before turning around. What do you think will happen if we add the prior diabetes mgmt intervention on top of the PreD+Ob25 one?

Syndemics
Prevention Network
Healthy People 2010 Diabetes Objectives:What Can We Accomplish?
-11%7.88.8 per 1,000
Reduce Diabetes–related Deaths Among Diagnosed
(5-6)
-38%2540 per 1,000
Reduce Prevalence of Diagnosed Diabetes
(5-3)
-29%2.53.5per 1,000
Reduce New Cases of Diabetes (5-2)
Increase Diabetes Diagnosis (5-4)
+18%80%68%
Percent Change
HP 2010 Target
Baseline
U.S. Department of Health and Human Services. Healthy People 2010. Washington DC: Office of Disease Prevention and Health Promotion, U.S. Department of Health and Human Services; 2000. http://www.healthypeople.gov/Document/HTML/Volume1/05Diabetes.htm

Syndemics
Prevention Network
20
30
40
50
60
70
1980 1985 1990 1995 2000 2005 2010
Pe
op
le w
ith
dia
gn
ose
d d
iab
ete
s p
er
1,0
00
Reported Simulated
Status Quo
Meet Detection Objective (5-4)
Meet Onset Objective (5-2)
HP 2010 Objective (5-3)
HP 2000 Objective
History and Futures for Diabetes PrevalenceReported Trends, HP Objectives, and Simulation Results
A
B
C
D
E
F
G
H
I
Milstein B, Jones A, Homer J, Murphy D, Essien J, Seville D. Charting plausible futures for diabetes prevalence: a role for system dynamics simulation modeling. Preventing Chronic Disease 2007 (in press).
Does this imply failure of the national policy?
Or a problem in the goal-setting process itself?
Does this imply failure of the national policy?
Or a problem in the goal-setting process itself?

Syndemics
Prevention Network
Connecting the ObjectivesPopulation Flows and Dynamic Accounting 101
It is impossible for any policy to reduce prevalence
38% by 2010!
People withUndiagnosed
Diabetes
People withDiagnosedDiabetes Dying from Diabetes
Complications
DiagnosedOnset
InitialOnset
PeoplewithoutDiabetes
As would stepped-up detection effort
Reduced death wouldadd further to prevalence
With a diagnosed onset flow of
1.1 mill/yr
And a death flow of 0.5 mill/yr
(4%/yr rate)
The targeted 29% reduction in diagnosed onset can only
slow the growth in prevalence
Milstein B, Jones A, Homer J, Murphy D, Essien J, Seville D. Charting plausible futures for diabetes prevalence: a role for system dynamics simulation modeling. Preventing Chronic Disease 2007 (in press).
Syndemics
Prevention Network
• All models, including simulations, are incomplete and imprecise
• But some are better than others and capture more important aspects of the real world’s dynamic complexity
• A valuable model is one that can help us understand and anticipate better than we do with the unaided mind
How Should We Value Simulation Studies?
Artist: Rene Magritte
Sterman JD. All models are wrong: reflections on becoming a systems scientist. System Dynamics Review 2002;18(4):501-531.
Meadows DH, Richardson J, Bruckmann G. Groping in the dark: the first decade of global modelling. New York, NY: Wiley, 1982.
Forrester JW. Counterintuitive behavior of social systems. Technology Review 1971;73(3):53-68.
“All models are wrong, some are useful.”
-- George Box

Syndemics
Prevention Network
Sterman J. Business dynamics: systems thinking and modeling for a complex world. Boston, MA: Irwin McGraw-Hill, 2000.
Barriers to Learning in Dynamic Systems

Syndemics
Prevention Network
But We Can Create Virtual Worlds for Learning
Sterman J. Business dynamics: systems thinking and modeling for a complex world. Boston, MA: Irwin McGraw-Hill, 2000.
“In [dynamically complex] circumstances simulation becomes the only reliable way to test a hypothesis and evaluate the likely effects of policies."
-- John Sterman

Syndemics
Prevention Network
Learning In and About Dynamic Systems
Benefits of Simulation
• Formal means of evaluating options
• Experimental control of conditions
• Compressed time
• Complete, undistorted results
• Actions can be stopped or reversed
• Tests for extreme conditions
• Early warning of unintended effects
• Opportunity to assemble stronger support
• Visceral engagement and learning
Complexity Hinders
• Generation of evidence (by eroding the conditions for experimentation)
• Learning from evidence (by demanding new heuristics for interpretation)
• Acting upon evidence (by including the behaviors of other powerful actors)
Sterman JD. Learning from evidence in a complex world. American Journal of Public Health (in press).
Sterman JD. Business Dynamics: Systems Thinking and Modeling for a Complex World. Boston, MA: Irwin McGraw-Hill, 2000.
“In [dynamically complex] circumstances simulation becomes the only reliable way to test a hypothesis and evaluate the likely effects of policies."
-- John Sterman

Syndemics
Prevention Network
“Simulation is a third way of doing science.
Like deduction, it starts with a set of explicit
assumptions. But unlike deduction, it does not
prove theorems. Instead, a simulation generates
data that can be analyzed inductively. Unlike
typical induction, however, the simulated data
comes from a rigorously specified set of rules
rather than direct measurement of the real world.
While induction can be used to find patterns in
data, and deduction can be used to find
consequences of assumptions, simulation
modeling can be used as an aid to intuition.”
-- Robert Axelrod
Axelrod R. Advancing the art of simulation in the social sciences. In: Conte R, Hegselmann R, Terna P, editors. Simulating Social Phenomena. New York, NY: Springer; 1997. p. 21-40. <http://www.pscs.umich.edu/pub/papers/AdvancingArtofSim.pdf>.
Sterman JD. Business Dynamics: Systems Thinking and Modeling for a Complex World. Boston, MA: Irwin McGraw-Hill, 2000.
Simulation ExperimentsOpen a Third Branch of Science
“The complexity of our mental models vastly exceeds our ability to understand their implications without simulation."
-- John Sterman
How?
Where?
0
10
20
30
40
50
1960-62 1971-74 1976-80 1988-94 1999-2002
Prevalence of Obese Adults, United States
Why?
Data Source: NHANES 20202010
Who?
What?

Syndemics
Prevention Network
An Alternative Philosophical Tradition
Shook J. The pragmatism cybrary. 2006. Available at <http://www.pragmatism.org/>.
Addams J. Democracy and social ethics. Urbana, IL: University of Illinois Press, 2002.
West C. The American evasion of philosophy: a genealogy of pragmatism. Madison, WI: University of Wisconsin Press, 1989.
"Grant an idea or belief to be true…what concrete difference will its being true make in anyone's actual life?
-- William James
Pragmatism• Begins with a response to a perplexity or injustice
in the world• Learning through action and reflection• Asks, “How does this work make a difference?”
Positivism • Begins with a theory about the world• Learning through observation and falsification• Asks, “Is this theory true?”
We are not talking about theories to explain, but conceptual, methodological, and moral orientations: the frames of reference
that shape how we think, how we act, how we learn, and what we value

Syndemics
Prevention Network
A Navigational View of Public Health Work
Thompson N. Reflections on voyaging and home. Polynesian Voyaging Society, 2001. Accessed July 18 at <http://leahi.kcc.hawaii.edu/org/pvs/malama/voyaginghome.html>.
Milstein B. Hygeia's constellation: navigating health futures in a dynamic and democratic world. Doctoral dissertation. Cincinnati, OH: Union Institute and University. November, 2006.
Where we want to go?
How do we prepare to get there?
Where do you want your children to live?
Where you do want to live?

Syndemics
Prevention Network
A Navigational View of Public Health Work
"How do you know," I asked, "that in twenty years those
things that you consider special are still going to be
here?" At first they all raised their hands but when they
really digested the question every single one of them
put their hands down. In the end, there was not a single
hand up. No one could answer that question.
It was the most uncomfortable moment of silence that I
can remember…That was the defining moment for me. I
recognized that I have to participate in answering that
question otherwise I am not taking responsibility for the
place I love and the people I love.”
-- Nainoa Thompson
Thompson N. Reflections on voyaging and home. Polynesian Voyaging Society, 2001. Accessed July 18 at <http://leahi.kcc.hawaii.edu/org/pvs/malama/voyaginghome.html>.
Milstein B. Hygeia's constellation: navigating health futures in a dynamic and democratic world. Doctoral dissertation. Cincinnati, OH: Union Institute and University. November, 2006.