pnina weiss, md - appd · pnina weiss, md [email protected] ... improvement of graduate medical...
TRANSCRIPT

Pnina Weiss, MD
Bruce Herman, MD
Kathleen McGann, MD
Angela Myers, MD
Geoff Fleming, MD
Chris Kennedy, MD

Objectives Increase understanding of milestone-based
competency assessment in pediatric fellowship programs
Demonstrate how to incorporate milestone-based competency assessment into evaluations and feedback to fellows

Milestone reporting to ACGME Resident milestones
May - June 2014
Fellow milestones
Nov - Dec 2014

Why Milestones? For accreditation…..
Allow for continuous monitoring of programs
Provide data for evaluation and research for continuous improvement of graduate medical education
Ensure public accountability by reporting national aggregate competency outcomes by specialty
acgme.org

Why are Milestones Important to YOU?

For fellowship programs…… Provide a descriptive, developmental framework for
clinical competency committees
Support better assessment practices
Enhance opportunities for identification of struggling residents and fellows
Guide curriculum development
acgme.org

For fellows…… Provide more explicit and transparent expectations of
performance
Facilitate better feedback for professional development
Support better self-directed assessment and learning
acgme.org

What is a competent physician?
I know it when I see it
Justice Potter Stewart, in Jacobellis v. Ohio 378 U.S. 184 (1964), regarding pornography

Advances in medical education:
Competency
Outcome

Evaluation/Assessment
Systematic appraisal of skills, behaviors and attitudes of a learner
Info about actual performance can be compared to intended performance
Highlight gaps
Motivate learning

Milestones: part of Pediatrics!
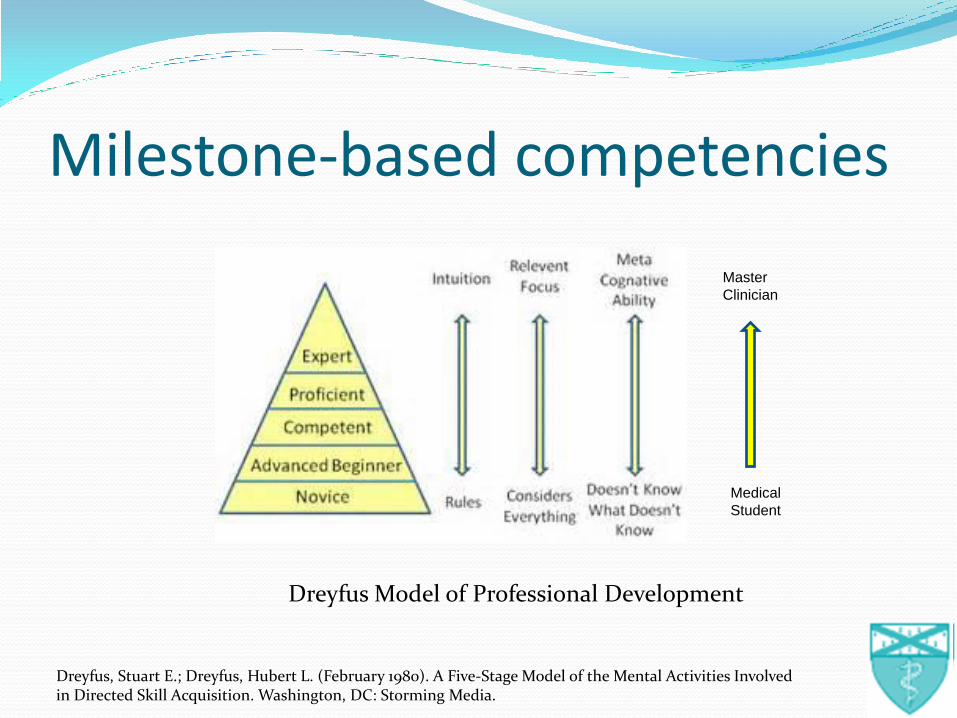
Dreyfus Model of Professional Development
Medical
Student
Master
Clinician
Milestone-based competencies
Dreyfus, Stuart E.; Dreyfus, Hubert L. (February 1980). A Five-Stage Model of the Mental Activities Involved in Directed Skill Acquisition. Washington, DC: Storming Media.

www.abp.org/abpwebsite/publicat/milestones.pdf


p. 125 Great Resource

www.acgme.org/acgmeweb/Portals/0/PDFs/Milestones/PediatricsSubspecialtyMilestones.pdf

March-April 2014
Vol. 14 No. 28
Milestone-based Clinical Competency Assessment: Building blocks!

Domains (of Competence)* Patient Care
Medical Knowledge
Practice-Based Learning Improvement
Interpersonal & Communication Skills
Professionalism
System-Based Practice
Personal and Professional Development
*“Competencies”

Domains Divided into Competencies* Patient Care
1. Develop and carry out management plans
2. Gather essential and accurate information about the patient
3. Provide transfer of care that ensures seamless transitions
* “Subcompetencies”

Competencies divided into milestones
PC7. Develop and carry out management plans
Master
Clinician
Novice
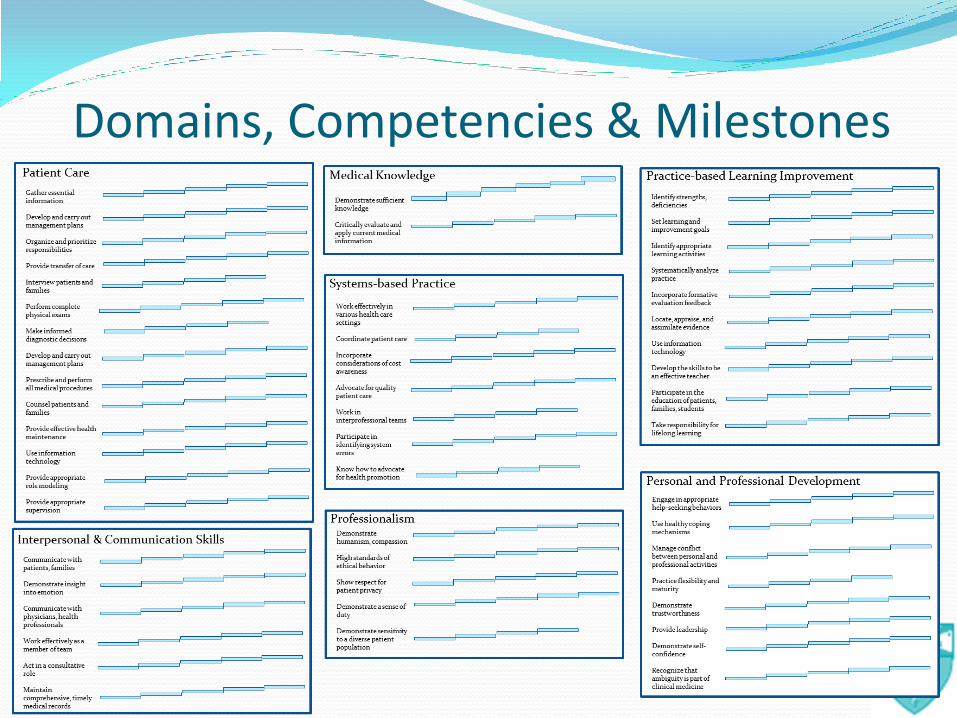
Domains, Competencies & Milestones

Entrustable professional activities (EPA)

Entrustable professional activities (EPA)
Essential routine care activities that define a specialty or competency; describes a unit of work
Can the trainee be entrusted to perform them without direct supervision?

EPAs for Subspecialties Shared with Pediatrics
Apply public health principles and improvement methodology to improve care for populations
Facilitate handovers to another health care provider
Common to all subspecialties Engage in scholarly activities through the discovery,
application and dissemination of new knowledge Lead within the subspecialty profession
Subspecialty -specific Care for patients with acute _____ problems Provide care for patients with chronic ______ problems

EPAs mapped to competencies and milestones

Milestones

21 Milestone-based competencies for reporting to ACGME

“Milestone assessment”
Selecting a response in between levels: milestones in lower levels have been substantially demonstrated as well as some milestones in higher level
Selecting a response in the middle of a level: milestones in that level and lower levels have been substantially demonstrated
www.acgme.org/acgmeweb/Portals/0/PDFs/Milestones/PediatricsSubspecialtyMilestones.pdf
PC7.

Clinical Competency Committee:
July 2013
Composition
At least 3 faculty
May include non-physician members of the health care team
Responsibilities
Review all fellow evaluations semi-annually
Prepare and assure the reporting of Milestones evaluations of each fellow semi-annually to ACGME
Advise the program director regarding fellow progress, including promotion, remediation, and dismissal

CCC maps fellow to the milestones
www.acgme.org/acgmeweb/Portals/0/PDFs/Milestones/PediatricsSubspecialtyMilestones.pdf
PC7.

You are the CCC! Materials WORKSHOP 17: FELLOW VIGNETTES for CCC Packet: CCC Evaluation Form (Fellow) APPD JJ-TT Evals Process Choose Chair Map fellows to milestones in each competency (7)- 15 mins List challenges/potential solutions-10 mins Chair will report to us

Challenges?

Challenges Useful evaluation tool?
CCC- inefficient?
Milestones -difficult to understand
Faculty
Lack of knowledge
Faculty fatigue
Lack of data

Usefulness of an evaluation tool
Reliability
Validity
Acceptability by learner and faculty
Impact on future learning
Costs
Van Der Vleuten CPM. The assessment of professional competence: developments, research and practical implications. Adv Health Sci Educ 1996;1:41-67 Epstein RM. Assessment in Medical Education. NEJM 2007;356:387-96

Improve effectiveness of CCC?

Improve effectiveness of CCC?

Suggestions to improve effectiveness Faculty & Self Education Process
PLAN!!!!! Budget at least 40 mins/fellow the first time Distribute CCC eval forms ahead of time; have faculty fill out
beforehand Decide on how to reach consensus Have copy of CCC eval form available for each member at meeting Review evals at start of meeting to highlight problem areas Go by competency and map all fellows before going to next competency Record comments after each competency is mapped Include comments and competencies outside of the 21 if needed to
document problem areas Feedback to fellow!

Understandability: Subspecialty “milestones” 101

Suggestions to improve your familiarity with milestones Read them
Self-evaluation using milestones
Resources http://www.pedsubs.org/Webinar/webinar.cfm
http://pedsubs.org/issues/pdfs/SlidesForFeb182014CoPS%20WebinarV20.pdf
http://www.acgme.org/acgmeweb/tabid/442/GraduateMedicalEducation/SlidePresentationsforFacultyDevelopment.aspx

Faculty development Education
Minimize evaluator fatigue

Suggestions for faculty education Generic training for ALL faculty More intensive training for CCC members
Prepare CCC members for time commitment!
Venue: faculty meeting, special meetings Self-evaluations Resources (previous slide) Walk through CCC meeting Use vignettes (written or video)
Evaluator fatigue Don’t use all competencies; limit to a few Phase in the # of milestone-based competencies

Not enough data?

Milestone-based evaluations

Milestone-based evaluations

Milestone-based evaluations

Evaluations
Milesto
ne
Ro
tati
on
Sem
ian
nu
al
facu
lty
Clin
ic
Am
bu
lato
ry
CE
X
Resid
en
t
Stu
den
t
Sta
fr
Pati
en
t
Pro
ced
ure
Teach
ing
Sig
no
ut
J C
lub
CC
C
Self
12 23 10 5 6 5 3 2 1 2 1 2 22 22
Transfer PC3 x x x x x
Make informed decision PC6 x x x x x x
Carry out plan PC7 x x x x x
Role model PC12 x x x x x
M edical procedures PC8 x x x x
Evidence MK2 x x x x x x x
Identify strength PBLI1 x x x x
Analyze practice using QI PBLI4 x x x
Information technology PBLI7 x x x x x
Educate pts, students PBLI9 x x x x x x x x
Effective teacher PBLI8 x
Communicate w/ pts ICS 1 x x x
Communicate w / MDs ICS3 x x x x x
Work as team member/leader ICS4 x x x x x x
Consultant ICS5 x x x x x
M edical records ICS6 x x x x x
Humanism, compassion PROF1 x x x x
High standards ethics PROF2 x x x x x x x x
TrustworthyPPD5 x x x x
Ambiguity PPD8 x x x
Leadership skills PPD6 x x x x x
Coordinate healthcare SBP2 x x x x x
Work in teams/pt safety SBP5 x x x x
Work in health care settings SBP1 x x x
Incorporate cost SBP3 x x x x
Identify systems error SBP 6 x x x

Feedback
Information communicated to a learner to modify thinking or behavior to improve learning

Perfect timing for semiannual meetings with fellow!
CCC meet (Nov, May)
Report milestones to ACGME (Nov/Dec, May/June)
Semiannual meeting with fellow (Dec, June)


Better formative feedback
Needs improvement
Develops and carries out management plans based on directives from others, either from the health care organization or the supervising physician. Unable to adjust plans based on individual patient differences or preferences. Communication about the plan is unidirectional from the practitioner to the patient and family.
To improve you should strive for: Develops and carries out management
plans based on one’s theoretical knowledge and/or directives from others. Can adapt plans to the individual patient, but only within the framework of one’s own theoretical knowledge. Unable to focus on key information, so conclusions are often from arbitrary, poorly prioritized, and time-limited information gathering. Management plans based on the framework of one’s own assumptions and values.
Develop and carry out management plans
Effective feedback Constructive Timely Ongoing Consistent By authoritative person over extended duration of time Face-to-face Concrete Goal-oriented Focused on product, not learner Understandable
“Complex feedback is likely to be ignored or its main messages lost”
Archer JC. State of the Science in Health Professional Education: Effective Feedback. Med Ed 2010; 44: 101-108

Giving your (problem) fellow feedback….. Materials
B. WORKSHOP 17: FELLOW MINIVIGNETTES for SELECTION of MILESTONE-BASED COMPETENCY
Table of Contents-Appendix of Abbreviated Pediatric Milestones
Milestones- paper, on-line (www.abp.org) or APPD meeting website
Process
Groups assigned Fellows #1-7
Select 2 competencies and plot to competency/milestone level(1 will NOT be part of 21)- as a group
Break into pairs
Give your fellow constructive feedback using the milestones
Report back the competency/milestone that you used

#1: Your fellow always runs behind the 8-ball She comes in 30 minutes before morning rounds. She examines the patients on your service, but when the service is busy does not always get to examine the consults before you round together. When paged in the afternoon for a nonurgent consult, she often puts it off till the following day (a day that you both have clinic). She starts to write the notes immediately after rounds instead of heading over to discuss the discharge plans on your patients with the residents. She sometimes seems to “forget” to follow up on important labs or tasks. Sometimes she dismissively says that she’s “pretty sure they were normal.” You find yourself checking on the critical labs and ensuring that the “to do” list is complete.
PC2 Organize and prioritize responsibilities to provide patient care that is safe, effective and efficient
PPD5. Demonstrate trustworthiness that makes colleagues feel secure when one is responsible for the care of patients

#2: Your new fellow has trouble getting along with others After the first month, your nurse pages you with an update because she says jokingly that she’d rather ask you than the fellow. Upon questioning, she confides that the fellow has been abrupt with her and makes her feel stupid for calling. According to your faculty, he is distant. He is respectful to them but has a short fuse with support staff. He is efficient but doesn’t seem to do much outside reading. During your next rotation with him, you overhear him snap at the respiratory therapist for suggesting a ventilator change. When you sit down with him to discuss his behavior, he breaks down and says that he is having issues with his personal life.
PPD2 Use healthy coping mechanisms to respond to stress PC12: Provide appropriate role modeling Prof2: Professional conduct SBP5. Work in interprofessional teams to enhance patient safety and
improve patient care quality

#3: Your fellow is intellectually lazy She accurately obtains and presents the history on new patients and comes up with a basic plan. For your new admission, you discuss the reason for starting an additional medication. You describe the pharmacokinetics and evidence-based rationale for it. You later read her progress note and find that she has rewritten almost verbatim your discussion. The next day after discussing a new consult, you suggest some additional reading material. Again, you find that she has just rewritten your own words in the discussion in the consult note. She says that she didn’t get to the outside reading. This pattern continues for the rest of your week together.
PBLI3. Identify and perform appropriate learning activities to guide personal and professional development
MK2 Critically evaluate and apply current medical information and scientific evidence for patient care
ICS5. Act in a consultative role to other physicians and health professionals

#4: Your fellow just isn’t doing enough outside reading Medical knowledge isn’t where it should be. In-training exam scores were low, particularly in pathophysiology. He can regurgitate the rules of patient care that you’ve given him, but has read few of the primary sources. When asked why he chose a particular medication, he doesn’t know the rationale. You have suggested multiple times that he read the NIH guidelines. He copied one of the tables and does carry it around to help with management.
MK1: Demonstrate sufficient knowledge of the basic and clinically supportive sciences appropriate to (pediatrics)
PBLI10: Take primary responsibility for lifelong learning to improve knowledge, skills, and practice performance through familiarity with general and experience-specific goals and objectives
MK2: Critically evaluate and apply current medical information and scientific evidence for patient care

#5. Your fellow is passive-aggressive in response to your feedback She worked for two years as a pediatrician in private practice before coming to your program. You had a long discussion with her at the end of her last rotation. You told her that she needs to preround on all the patients on your service and the consults. She needs to read more primary material and expand the depth of her discussions. You correct her choice of medications and explain why they’re less preferred. You are on service with her one month later and you notice the exact same issues. When approached about her behavior, she tells you that that’s the way they did it in her old institution or when she was in private practice.
PBLI5: Incorporate formative evaluation feedback into daily practice
PPD4: Practice flexibility and maturity in adjusting to change with the capacity to alter behavior
PBLI1. Identify strengths, deficiencies, and limits in one’s knowledge and expertise
#6. Your new fellow doesn’t call you when he should He just started and in the space of one week, he admitted a patient to your service without telling you, ordered (incorrect) antibiotics on another without consulting you and failed to contact you for help when one of your patients deteriorated overnight. When you came in that morning, you found the patient in severe distress and had to transfer her to the ICU. When you discussed it with him, he promised to notify you in the future, but didn’t seem convinced that he had done anything wrong.
PPD1. Develop the ability to use self-awareness of knowledge, skills and emotion limitations to engage in appropriate help seeking behaviors
PBLI1: Identify strengths, deficiencies and limits in one’s knowledge and expertise
PPD5: Demonstrate trustworthiness that makes colleagues feel secure when one is responsible for the care of patients
#7. Your fellow is careless with notes Your fellow’s inpatient notes ramble and are full of errors. The HPI is overly detailed. Because of “copy forward,” the interval history is from one week ago, medications that were discontinued are still in medication list, and the problem list is outdated. The physical exam appeared before the interval history. The notes are done in a timely fashion, but you still have to edit for accuracy and correct the many grammatical and spelling errors.
ICS6 Maintain comprehensive, timely and legible medical records
ICS3 Communicate effectively with physicians, other health professionals and health-related agencies
Importance of self-evaluation


References Assessment • Epstein RM. Assessment in Medical Education. NEJM 2007;356:387-96 • Downing SM. Reliability: on the reproducibility of assessment data. Med Ed
2004;38:1006-12 • Van Der Vleuten CPM. The assessment of professional competence: developments,
research and practical implications. Adv Health Sci Educ 1996;1:41-67 Milestones • Hicks PJ, Englander R, Schumacher DJ, et al. Pediatrics milestone project: next steps
toward meaningful outcomes assessment. J Grad Med Educ 2010;2:577-84 • Jones MD, Jr., Rosenberg AA, Gilhooly JT, Carraccio CL. Perspective: Competencies,
outcomes, and controversy--linking professional activities to competencies to improve resident education and practice. Acad Med: JAAMC 2011;86:161-5
• Schumacher DJ, Lewis KO, Burke AE, et al. The Pediatrics Milestones: Initial Evidence for Their Use as Learning Road Maps for Residents. Acad Pediatr;13:40-7
• The Pediatric Milestone Project www.abp.org/abpwebsite/publicat/milestones.pdf
References Feedback
Archer JC. State of the science in health professional education: effective feedback. Med Ed 2010;44:101-8
Hewson MG, Little ML. Giving feedback in medical education: verification of recommended techniques. J Gen Intern Med 1998;13:111-6.
Self-assessment
Gordon MJ. A Review of the validity and accuracy of self-assessments in health professions training. Acad Med 1991; 66:762-769.
Davis DA, Mazmanian PE, Fordis M, Thorpe KE , Perrier L. Accuracy of physician self-assessment compared with observed measures of competence: a systematic review. JAMA 2006; 296:1094-1102.