plex iridica bsmt for slides may - bsmt.org.uk iridica_15may15.pdf · 6/3/15 1 secondaryinformaon...
TRANSCRIPT
6/3/15
1
Secondary informa.on
Mark Wilks, Clinical Scientist, Microbiology Barts Health NHS Trust, London, UK
Barts and the London School of Medicine and Dentistry, Queen Mary
Direct detec.on of infec.on with the Abbo6 Plex-‐ID PCR/ESI system
PCR ESI/MS PlexID Iridica
• Summary: Specimen ( blood, sterile fluid etc) (any) microbe ID in 6-‐8hrs, no enrichment >£150
• Basis of the technology • RADICAL –rapid diagnosis of sepsis study • Understanding what the results mean and how they might effect pa.ent management
• What next? How would you use the technology
6/3/15
2
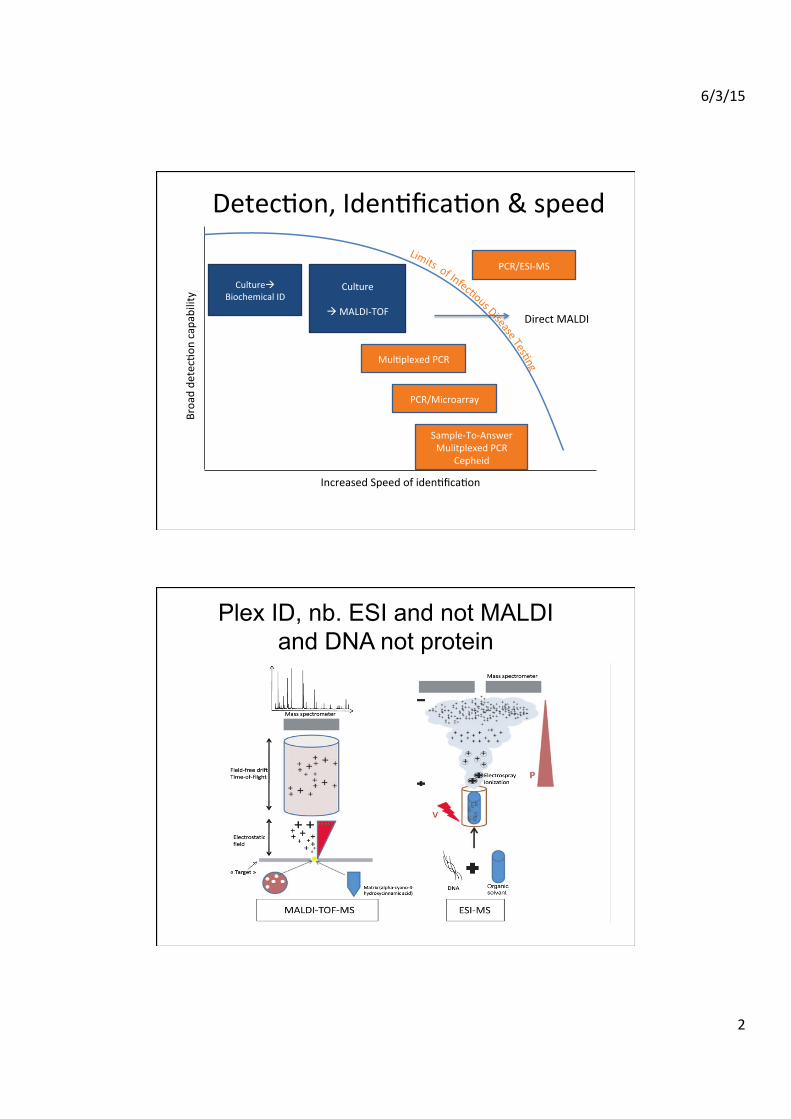
Culture Biochemical ID
Detec.on, Iden.fica.on & speed
Culture
MALDI-‐TOF
Mul.plexed PCR
Sample-‐To-‐Answer Mulitplexed PCR
Cepheid
PCR/Microarray
Increased Speed of iden.fica.on
Broad de
tec.on
capability
PCR/ESI-‐MS
Direct MALDI
Plex ID, nb. ESI and not MALDI and DNA not protein

6/3/15
3
E.coli
4364
.06
5380
.64
6254
.64
6315
.49
5096
.01
7157
.65
7273
.87
6410
.90
7870
.62
8368
.99
0
1000
2000
3000
4000
5000 Inte
ns. [
a.u.
]
4000 4500 5000 5500 6000 6500 7000 7500 8000 m/z
ribosomal Protein m/zRL36 4364,33RS32 5095,82RL34 5380,39RL33meth. 6255,39RL32 6315,19RL30 6410,60RL35 7157,74RL29 7273,45RL31 7871,06RS21 8368,76
MALDI-‐TOF -‐ differences in ribosomal proteins basic and abundant
nb single charge/protein
PLEX-‐ID – DNA two strands and mul.ple charge states

6/3/15
4
6/3/15
5

6/3/15
6
Triangula.on iden.fca.on for the gene.c evalua.on of risks (TIGER) IbisT5000

6/3/15
7
Abbot Plex-ID
Plex-‐IDIridica
Pre PCR
Post PCR
Mass spec Bead beater
Mass spec
De-‐salter DNA extractor
T/C

6/3/15
8
• RApid Diagnosis of Infec.ons in the Cri.cAlly ILL (RADICAL)
• Mul.-‐center observa.onal study 528 pa.ents 1. Demonstrate analy.cal performance
2. Imputed clinical and economic value
• Evalua.on of PCR/ESI-‐MS vs. Culture
Scientific publications, case studies/series
Utilize data for reimbursement & economic model
RADICAL trial Abbo6 PLEX ID
Sampling
• Clinical suspicion of a BSI ( pneumonia) • Same venipuncture: ≥5ml EDTA blood and a BC • If mul.ple BC taken, extra 5ml of EDTA blood also taken
• Blood kept at 4˚C for up to 48h and then -‐20˚C • Retrospec.ve analysis in London, Paris or Geneva • (ETAs BALs, PD fluid, synovial fluid also taken)

6/3/15
9
BAC Strip • Detects bacteria, Candida species and 4 an.bio.c resistance markers
• +600 reportable species/groups
• 1) Pneumonia (up to 5 ml BAL) • 2) Sepsis (5 ml blood) • 3) Sterile fluids (up to 5 ml)
Fungal Strip
Kingdom Fungi
Genus Candida
Class Ascomycetes
Genus Fusarium
Genus Aspergillus
Order Mucorales
Genus Cryptococcus
Kingdom Fungi
Kingdom Fungi

6/3/15
10
Viral IC Strip Assay detects:
Herpesviruses (HHV1-‐8) Adenoviruses (A-‐F) Parvovirus (PB19)
Picornavirus (Enterovirus A-‐E)) Polyomaviruses (JC, BK)
Sample: DNA & RNA from Plasma (and others)
21 rep groups
Radical: Pa.ent demographics (n=528)

6/3/15
11
Overall results 616 specms/528 pa.ents PLEX ID 223/616 = 36.2% posi.ve Culture 67/616 = 10.8% posi.ve
Ratio of culture positive: PCR/ESI MS positive for selected organisms
6/3/15
12
‘
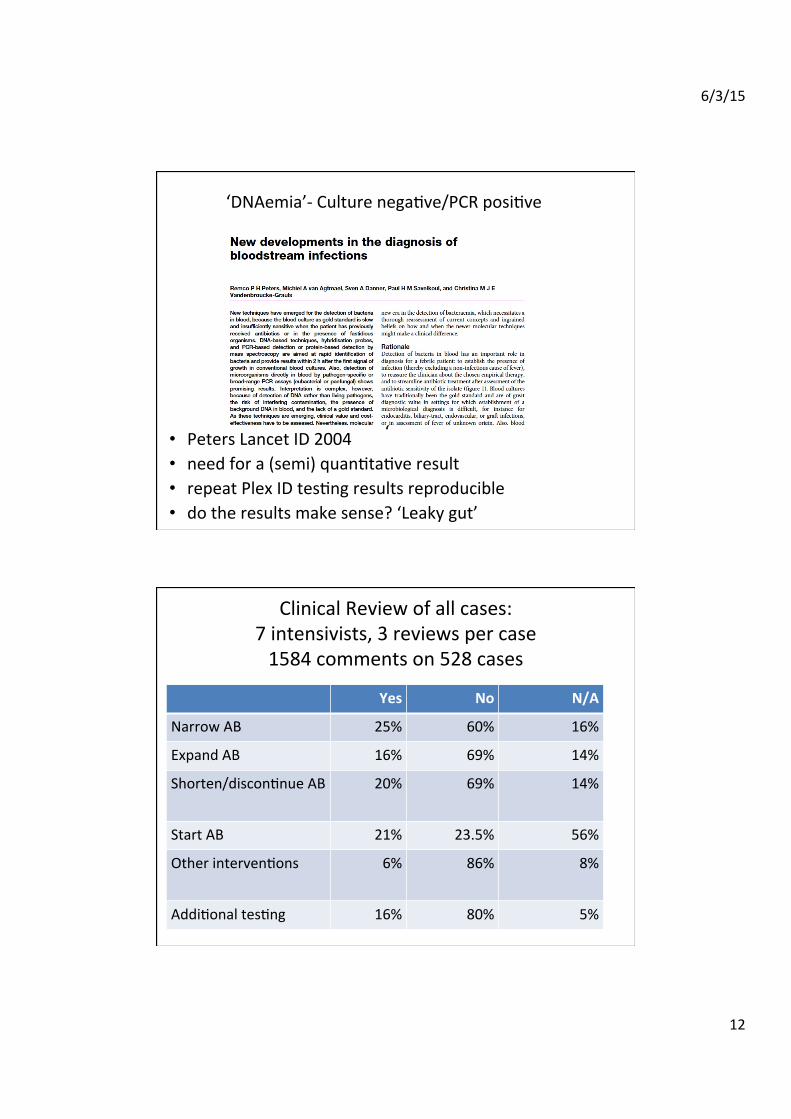
‘DNAemia’-‐ Culture nega.ve/PCR posi.ve
‘
• Peters Lancet ID 2004 • need for a (semi) quan.ta.ve result • repeat Plex ID tes.ng results reproducible • do the results make sense? ‘Leaky gut’
Clinical Review of all cases: 7 intensivists, 3 reviews per case 1584 comments on 528 cases
Yes No N/A
Narrow AB 25% 60% 16%
Expand AB 16% 69% 14%
Shorten/discon.nue AB 20% 69% 14%
Start AB 21% 23.5% 56%
Other interven.ons 6% 86% 8%
Addi.onal tes.ng 16% 80% 5%

6/3/15
13
85 year immunocompetent male PMH hypertension, malaria, 1/52 lower abdominal pain, diarrhea, vomi.ng,
admi6ed to hospital 08/01 for confirmed sepsis/infec.on.
• ICU admission 9/1, abdominal X ray: gastrointes.nal perfora.on
• AB 8/1 cerriaxone and metronidazole • 9/1/ arterial and CVCs • 12/1 imipenem 7 days • 16/1 amikacin 3 days
• BC 9/1: no growth • Blood Plex-‐ID 9/1: Gordonia polyisoprenivorans
• 9/1 Peritoneal fluid culture: no growth • 9/1 Peritoneal fluid Plex-‐ID: 9/1 Acinetobacter baumanii, Bilophila
wardsworthia, Burk (ceno)cepacia, Pantoea agglomerans
77 year old male, pulmonary/respiratory, kidney/renal disease, hypertension, struma nodosa, admi6ed to hospital 06/05 for suspected sepsis/infec.on,
immunocompetent , nephrectomy, relaparotomy due to bleeding
• Date of ICU admission 8/6: haemorrhage
• AB 9/5 tazobactam 4 days • 12/5 caspofungin – ongoing • 15/5 ampicillin +sulbactam 3 days • 17/5 tazobactam 5 days • 19/5 teicoplanin 11 days • 19/5 caspofungin 6 days • 21/5 ciprofloxacin 10 days • 31/5 amox/clavulanic 3 days • 2/6 tazobactam • 12/6 caspofungin
• BC 12/6 : no growth • Blood Plex-‐ID 12/6 : Enterococcus faecium, Van B
• Discharged from ICU 14/6, died 17/6

6/3/15
14
85 yr female, immunocompetent, PMH39.6 degrees, abdominal pain, liver abscess admi6ed to the hospital on 14/06 ? sepsis.
SOFA score 12 • Date of ICU admission 15/6 sepsis/infec.on, shock, CT scan: liver
abscess
• AB 15/6 cerriaxone and metronidazole
• Liver abscess 15/6 culture: Morgenella morganii • Liver abscess Plex-‐ID: M. morganii
• BC 15/6 : no growth • Blood Plex-‐ID 15/6 : F nucleatum, M. morganii • Pleural fluid 15/6 culture no growth • Plueral fluid 15/6 Plex-‐ID Bilophila wadsworthia, M.morganii
67 year old Male, Past Medical History: NIL, admi6ed to the hospital on 27/12
• Admi6ed to ICU on 14/1:RESPIRATORY/VENTILATORY INSUFFICIENCY, infiltrate on Xray, SOFA score 10
• AB Meropenem and Vancomycin 15/1 • Blood culture 15/1: no growth • Blood culture 17/1: ?no growth • BC Plex-‐ID15/1: Mtb complex + Ps aeruginosa • BC Plex-‐ID 17/1: Mtb complex • AB 21/1: Amikacin, clarithromycin, 22/1 rifampicin

6/3/15
15
Sample: 000203902Plate: 0D000002968CA151100213Slot: 4Assay Database: RDL44.47.39Error:
Fungi
Control
Assay: BCAL5lAssay Protocol: NextPLE( BAC Assay RUOProtocol Version: 1,0.0.9154Analysis Serven SPS.1.3.9225/REL-GenX-V09R001-9221
ltlicrobe Q Score L"evel0.99 667
ltlicrobe Q Score
Q Sgole LevelControl 0.97 58
Sampfe: L4AL24786Plate: 0D000002968CA151100213Slot 5Assay Database: RDL44.47.39Error:
Fungi
Itlarker
Control
Assay: BCAL5lAssay Protocol: NeltPLD( BAC Assay RUOProtocol Version: 1.0.0.9154Analysis Server: SPS, 1.3.9225IREL-GenX-V09R001-9221
Microbe QScore Level0.96 L7
Microbe Q ScoreNot
Marker Result Q ScoR"-"_-- _-- " !:*gvgNot detected nla nla
IW]W4[i{l$rwNot detected nla nla
I : ryh" '
il ilicrobeControl 0.97 83
PAGE 1 OF 1 -.. FOR RESEARCH USE ONLY. NOT FOR USE IN DIAGNOSTIC PROCEDURES.
Case 203 2nd Plex ID specm
1yr old boy Arthri.s ler elbow All viro and Micro -‐ ve Il12/TNF alpha
Mtb by PLEX ID? • 1st Run adjacent specimens:
– Radical Case 302 2nd specn: M tb complex high level – Child MH ler elbow: M tb complex low level
• Clean everything with bleach and rerun – Radical Case 302 2nd specn: M tb complex high level – Child MH ler elbow: M tb complex low level
• Other samples – Radical Case 302 1st specn: M tb complex plus Ps aeruginosa
– Child MH ler elbow virology lab sample M tb complex • What to do?
6/3/15
16
What to do • Radical -‐ blind study-‐ unethical to leave -‐ unblind, MDR TB not known to ICU
• 1yr old boy, no risk factors, no travel, • tested .ssue around the joint nega.ve • test not CE marked -‐ abnormal LFTs • grew Mtb 1 month later • VNTR typing – BCG • an. tuberculosis treatment started
Using Iridica -‐ rule in/rule out infec.on
• Rule in • Accurate, rapid ID of wide range of pathogens
• Mixed infec.ons • End sequen.al tes.ng
-‐look for everything on day 1 • Unaffected by prior an.bio.c treatment
• Rule out • Rely on High NPV • Stop treatment/don’t start
• Need high sensi.vity • High confidence to stop treatment/not start

6/3/15
17
Rule out-‐ importance of a high NPV
• Invasive fungal infec.on • Poor diagnos.c tests • Over use of prophylaxis • Barts Health an.fungal spend £1.9M per annum
• Neonatal infec.ons • BC: difficult to get adequate blood vol, slow
• Serious consequences of overuse of an.bio.cs – Kuppala 2014 – AB treatment, no sepsis 2,3 X NEC, LOS, death
Acknowledgments/Conflicts of Interest
•
• Abbo6 for support for study-‐ machine, reagents • Travel expenses ( not yet claimed) • RADICAL group for access to data • Ronan Murphy for analysis •
6/3/15
18
Further reading excellent review: Buchan and Ledeboer Clin Micro Rev 2014
Why has the adop.on of molecular methods in diagnos.c microbiology so
slow
6/3/15
19
Inate conserva.sm?
• Rapid adop.on of MALDI-‐TOF, – high capital cost, low running cost
• Wrong test/wrong price – 40 enteric pathogens £50 – Detect Candida direct from blood £200 – ID from posi.ve Blood cultures £100-‐200
Nice test, shame about the price • Single target
– Cepheid £20-‐50 – e.g. TB, MRSA, C diff, CRO
• Syndromic (£100-‐200) – Cure.s Varyo – e.g.resp, orthorpaedic – BioFire FilmArray (BioM) – e.g Ebola, resp, GI, BC, panels
• Everything – Abbo6 Iridica – all bacteria, all fungi, viruses £100-‐200
• User friendly NGS easy to understand interface – Illumina MiSeq BioMerieux – Pathogenica ( BioInova.ons)