please note: activity presentations are (cme@vindicocme...
TRANSCRIPT

Multifaceted Approaches to Optimize Care for Patients with Obesity
© 2015 Vindico Medical Education
Please note: Activity presentations are
considered intellectual property. These slides
may not be published or posted online without
permission from Vindico Medical Education
Please be respectful of this request so we may
continue to provide you with presentation
materials.
Facilitating Changes in
Behavior – Meeting the Needs
of Patients and Providers
Robert F. Kushner, MD
Professor of Medicine, Feinberg School of Medicine
Director, Center for Lifestyle Medicine, Northwestern Medicine
Chicago, IL
Multifaceted Approaches to Optimize Care for Patients with Obesity
© 2015 Vindico Medical Education
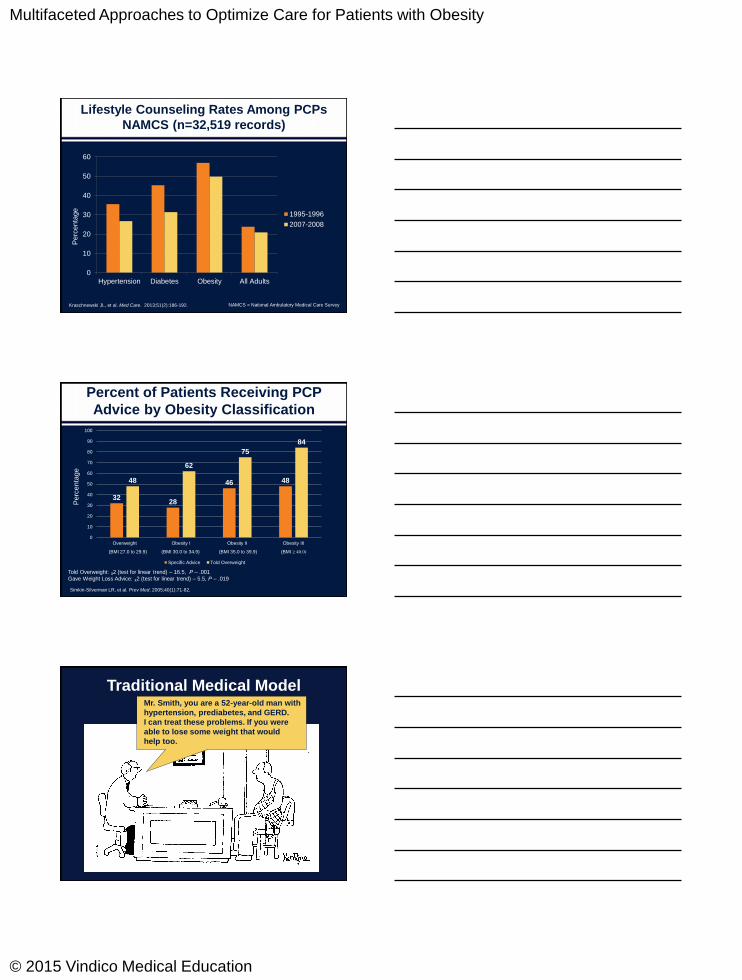
Lifestyle Counseling Rates Among PCPs
NAMCS (n=32,519 records)
0
10
20
30
40
50
60
Hypertension Diabetes Obesity All Adults
1995-1996
2007-2008
Pe
rce
nta
ge
NAMCS = National Ambulatory Medical Care SurveyKraschnewski JL, et al. Med Care. 2013;51(2):186-192.
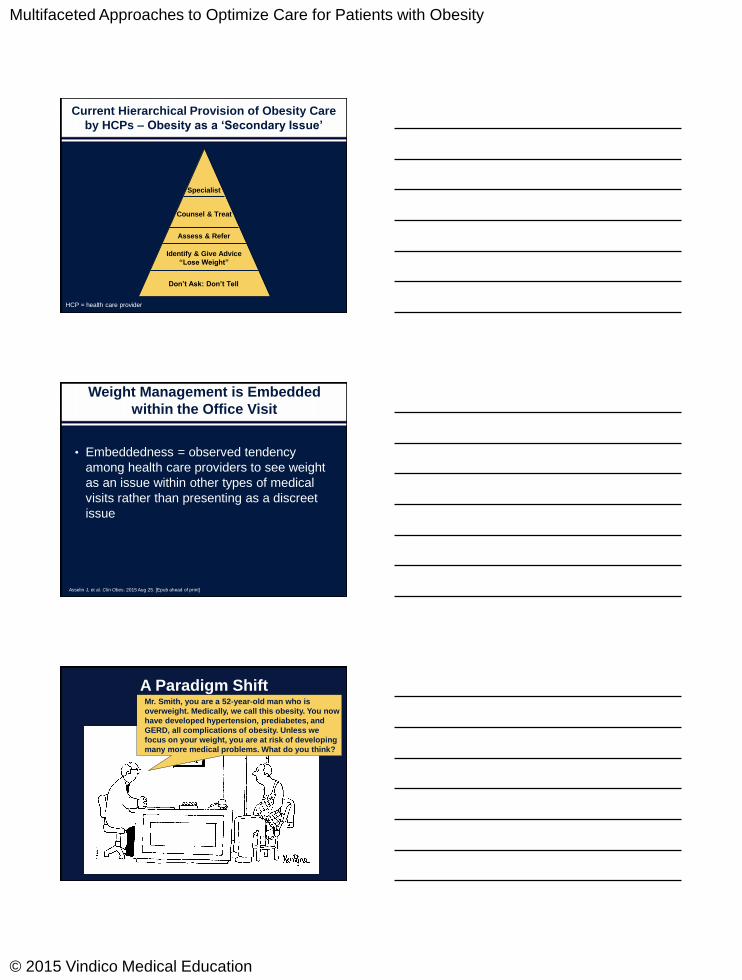
Percent of Patients Receiving PCP
Advice by Obesity Classification
Simkin-Silverman LR, et al. Prev Med. 2005;40(1):71-82.
3228
46 4848
62
75
84
0
10
20
30
40
50
60
70
80
90
100
Overweight Obesity I Obesity II Obesity III
Specific Advice Told Overweight
(BMI 27.0 to 29.9) (BMI 30.0 to 34.9) (BMI 35.0 to 39.9) (BMI ≥ 40.0)
Told Overweight: ᵪ2 (test for linear trend) – 16.5, P – .001
Gave Weight Loss Advice: ᵪ2 (test for linear trend) – 5.5, P – .019
Pe
rce
nta
ge
Mr. Smith, you are a 52-year-old man with
hypertension, prediabetes, and GERD.
I can treat these problems. If you were
able to lose some weight that would
help too.
Traditional Medical Model
Multifaceted Approaches to Optimize Care for Patients with Obesity
© 2015 Vindico Medical Education
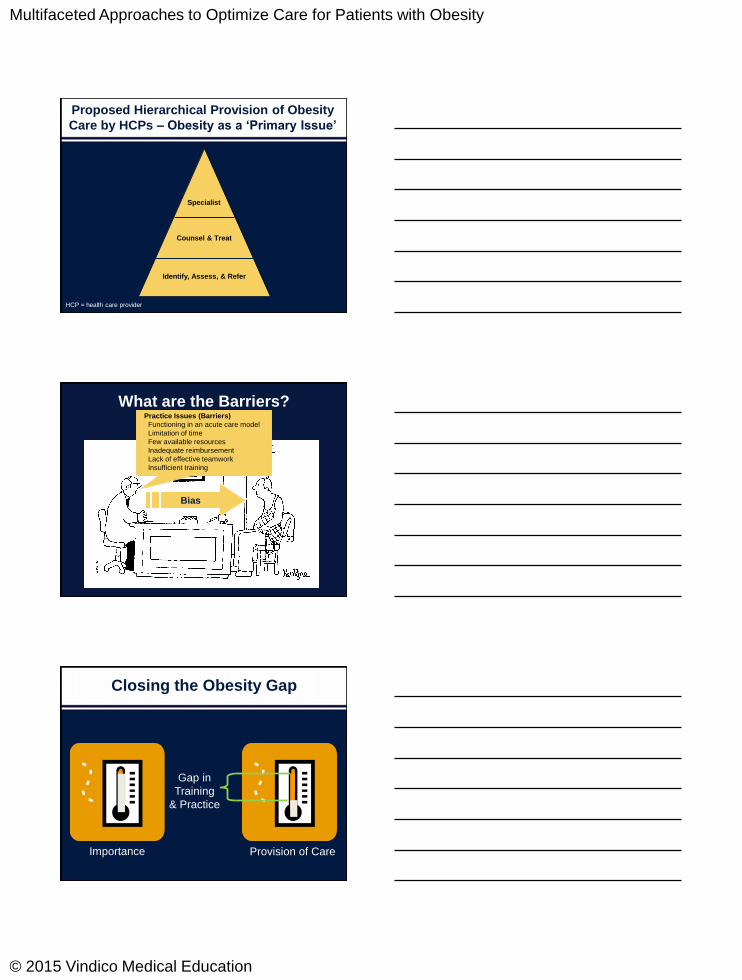
Current Hierarchical Provision of Obesity Care
by HCPs – Obesity as a ‘Secondary Issue’
Don’t Ask: Don’t Tell
Identify & Give Advice
“Lose Weight”
Assess & Refer
Counsel & Treat
Specialist
HCP = health care provider
Weight Management is Embedded
within the Office Visit
• Embeddedness = observed tendency
among health care providers to see weight
as an issue within other types of medical
visits rather than presenting as a discreet
issue
Asselin J, et al. Clin Obes. 2015 Aug 25. [Epub ahead of print]
Mr. Smith, you are a 52-year-old man who is
overweight. Medically, we call this obesity. You now
have developed hypertension, prediabetes, and
GERD, all complications of obesity. Unless we
focus on your weight, you are at risk of developing
many more medical problems. What do you think?
A Paradigm Shift
Multifaceted Approaches to Optimize Care for Patients with Obesity
© 2015 Vindico Medical Education
Proposed Hierarchical Provision of Obesity
Care by HCPs – Obesity as a ‘Primary Issue’
Identify, Assess, & Refer
Counsel & Treat
Specialist
HCP = health care provider
Practice Issues (Barriers)
Functioning in an acute care model
Limitation of time
Few available resources
Inadequate reimbursement
Lack of effective teamwork
Insufficient training
Bias
What are the Barriers?
Closing the Obesity Gap
Importance Provision of Care
Gap in
Training
& Practice
Multifaceted Approaches to Optimize Care for Patients with Obesity
© 2015 Vindico Medical Education
Developing Professional
Competence
• “The habitual and judicious use of
communication, knowledge, technical skills,
clinical reasoning, emotions, values, and
reflection in daily practice for the benefit of the
individual and community being served.”
• “Competence builds on a foundation of basic
clinical skills, scientific knowledge, and moral
development.”
Epstein RM, et al. JAMA. 2002;287(2):226-235.
Patient-Physician Communication
Adapted from: Rotor D. Patient Ed and Counseling, 2000.
Patient Power/
Interest
Physician Power/Interest
High
High
Low
Low
Mutuality“Shared decision-making”
Paternalism
“Do what I say!”
Consumerism“What ever you want”
Dysfunctional“Don’t ask: Don’t tell”
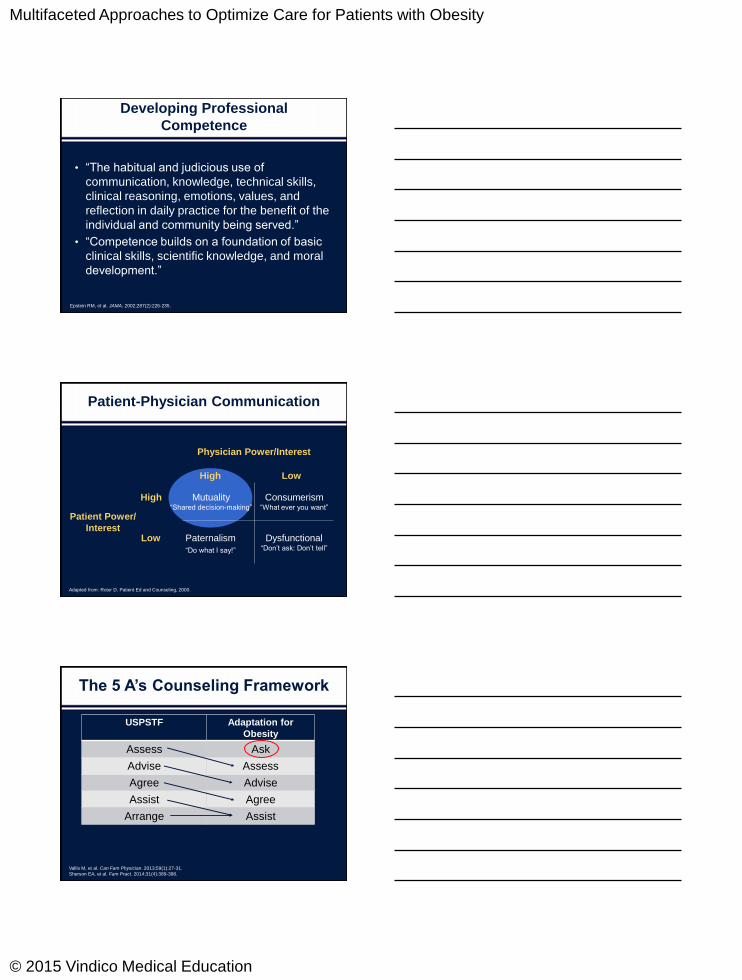
The 5 A’s Counseling Framework
Vallis M, et al. Can Fam Physician. 2013;59(1):27-31.
Sherson EA, et al. Fam Pract. 2014;31(4):389-398.
USPSTF Adaptation for
Obesity
Assess Ask
Advise Assess
Agree Advise
Assist Agree
Arrange Assist

Multifaceted Approaches to Optimize Care for Patients with Obesity
© 2015 Vindico Medical Education
The 5 A’s Counseling Framework
Ask/Assess • Weight history
• Contributions to weight gain
• Past treatment attempts
• Diet and physical activity patterns
• Physical examination and pertinent laboratory tests
Advise • Perception of health problems associated with excess
weight
• Explain complications of excess weight
• Explain benefit of weight loss to improve health
• Explore treatment options
• Provide strategies for weight management
Agree • Decide upon a collaborative-based treatment plan
Assist • Discuss potential barriers to implement treatment plan
• Provide handouts
Arrange • Discuss follow up plans and/or referrals
Motivational Interviewing (MI)
• Motivational interviewing is a collaborative,
goal-oriented approach of communication
to elicit behavior change in patients.
• The approach is designed to identify and
resolve ambivalence toward a specific goal
by connecting necessary changes to
incentives that reduce barriers for change.
Motivational Interviewing. 2nd Ed, Miller WR and Rollnick S, eds. The Guilford Press, New York, 2002.
Motivational Interviewing Skills
• Ask– Ask open-ended questions inviting the patient to
consider how and why they might change.
• Listen
– Understand the patient’s experience and summarize with reflective listening.
• Inform– Ask permission to provide information, then ask
what the implications might be for the patient.
Rollnick S, et al. BMJ. 2010;340:c1900.

Multifaceted Approaches to Optimize Care for Patients with Obesity
© 2015 Vindico Medical Education
Moving to a New Paradigm
in Obesity Care
Adapted from: Tsai AG, et al. J Gen Intern Med. 2009;24(9):1073-1079; Carvajal R, et al. Ann N Y Acad Sci. 2013;1281:191-206.
Assess and treat obesity-related
co-morbid conditions
Assess motivation for weight
management
HCP provides
weight
management
HCP referral for
weight
management
HCP and
colleagues offer
collaborative care
HCP referral to
obesity medicine
specialist
LM counseling,
(pharmacotherapy)
Commercial or
web-based, RD,
disease
management
(NP, PA, RN, RD,
PsyD, coaches),
LM counseling,
pharmacotherapy
Team approach,
LM counseling,
VLCD,
pharmacotherapy,
bariatric surgery
Shared decision-
making (SDM)
• Requires competency in and a thorough understanding of the
treatment of obesity and the genetic, biologic, environmental, social,
and behavioral factors that contribute to obesity.
• Employs therapeutic interventions including diet, physical activity,
behavioral change, and pharmacotherapy.
• Utilizes a comprehensive approach, and such as nutritionists,
exercise physiologists, psychologists and bariatric surgeons as
indicated to achieve optimal results.
• Maintains competency in providing pre-, peri-, and post-surgical care
of bariatric surgery patients, promotes the prevention of obesity, and
advocates for those who suffer from obesity.
American Board of Obesity Medicine: www.abom.org.
Conclusion
• Obesity care is currently embedded within the office visit.
• Making obesity a primary concern will require increased competency in obesity care along with changes in the medical practice system.
• Use of the 5 A’s counseling framework and motivational interviewing (MI) is intended to facilitate behavior change.

Multifaceted Approaches to Optimize Care for Patients with Obesity
© 2015 Vindico Medical Education
Achieving a Comfort Zone
with Pharmacotherapy
Scott Kahan, MD, MPH, FTOSDirector, National Center for Weight and Wellness
Medical Director, Strategies To Overcome and Prevent
(STOP) Obesity Alliance
George Washington University
Washington, DC
Obesity Is Significantly
Under-Treated
0
25
50
75
100
Hypertension Diabetes Depression Obesity
Affected
Treated (Medication)
# o
f P
atie
nts
(Millio
ns)
Xia Y, et al. Obesity. 2015;23(8):1721-28.

Multifaceted Approaches to Optimize Care for Patients with Obesity
© 2015 Vindico Medical Education
FDA-Approved Obesity
Pharmacotherapy Options
• Phentermine (and other noradrenergic agents)
• Orlistat
• Lorcaserin
• Phentermine / topiramate ER
• Naltrexone SR / bupropion SR
• Liraglutide 3.0 mg
Indications: Adjunct to behavioral modification in
BMI >30 kg/m2 or 27-30 kg/m2 with comorbidities
Phentermine
• Sympathomimetic amine
• Approved 1959
• Short-term use; schedule IV
• Dosing: 15-37.5mg qAM
• Contraindications/warnings:
Pregnancy, nursing, MAOI
use, glaucoma, drug abuse
history, hyperthyroidism,
uncontrolled hypertension,
tachycardia, history of CAD,
CHF, stroke
• Lipase inhibitor
• Approved 1999
• Long-term use; not scheduled
• 120 mg TID with meals (Rx) or
60 mg TID (OTC)
• Use MVI with fat-soluble
vitamins at bedtime
• Contraindications: pregnancy,
chronic malabsorption
syndrome, cholestasis
• Gastrointestinal AEs
Phentermine [package insert]. Cranford, NJ: Alpex Pharma SA: 2011. Orlistat [package insert]. South San Francisco,
CA: Genentech: 2012; Orlistat [package insert]. Moon Township, PA: GlaxoSmithKline: 2011.
Orlistat
Lorcaserin
• Selective 5HT-2c receptor agonist
• Increases satiety
• Approved in 2012
• Long-term use; schedule IV
• Single dose: 10 mg BID;
discontinue if <5% BWL after 12
weeks
• Contraindications: pregnancy
• Warnings: coadministration with
serotonergic agents; valvular heart
disease; psychiatric disorders,
priapism
Belviq [Prescribing Information]. Woodcliff Lake, NJ: Eisai Inc; 2012. Fidler MC, et al. J Clin Endocrinol Metab.
2011;96:3067. Smith SR, et al. N Engl J Med. 2010;363(3):245. Smith SR, et al. Obesity. 2014: 22:2137-46. Reprinted with
permission.

Multifaceted Approaches to Optimize Care for Patients with Obesity
© 2015 Vindico Medical Education
Lorcaserin: Weight Change over 2 Years
Smith SR, et al. N Engl J Med. 2010;363:245-256. Reprinted with permission.
Lorcaserin: Weight Change over 2 Years
Smith SR, et al. N Engl J Med. 2010;363:245-256. Reprinted with permission.
Endpoint Lorcaserin Placebo P
Waist circumference
(cm)
−6.8 −3.9 <0.001
SBP/DBP (mm Hg) −1.4/−1.1 −0.8/−0.6 0.04/0.01
Cholesterol (% Δ)
Total
LDL
HDL
−0.90
2.87
0.05
0.57
4.03
−0.21
0.001
0.049
0.72
Triglycerides (%) −6.15 −0.14 <0.001
A1c -0.9 -0.4 <0.001
Heart rate (bpm) −2.0 −1.6 0.049
Beck depression II −1.1 −0.9 0.26
Key Secondary Endpoints
Smith SR, et al. NEJM. 2010;363:245-256. O’Neil PM, et al. Obesity. 2012;20:1426-1436.

Multifaceted Approaches to Optimize Care for Patients with Obesity
© 2015 Vindico Medical Education
N (%) Lorcaserin
(N = 3195)
Placebo
(N = 3185)
Headache 537 (16.8) 321 (10.1)
Dizziness 270 (8.5) 122 (3.8)
Nausea 264 (8.3) 170 (5.3)
Constipation 186 (5.8) 125 (3.9)
Fatigue 229 (7.2) 114 (3.6)
Dry mouth 169 (5.3) 74 (2.3)
Lorcaserin: Adverse Events Reported
by 5% or More in Any Group
Smith SR, et al. N Engl J Med. 2010;363:245-256. O’Neil PM, et al. Obesity. 2012;20:1426-1436.
• Phentermine: blunts appetite
• Topiramate: prolongs satiety
• Approved in 2012
• Long-term use; schedule IV
• 4 fixed doses (3.75/23mg
increments)
• Titrate if <3% weight loss at 12 wk
• REMS: teratogenicity
• Contraindications: pregnancy,
glaucoma, MAOIs, hyperthyroidism
Phentermine and topiramate extended-release [package insert]. Mountain View, CA: Vivus; 2012.
Garvey WT, et al. Am J Clin Nutr. 2012;95(2):297-308.Reprinted with permission.
Phentermine / Topiramate ER
Phentermine / Topiramate ER
Prevents Progression to T2DM
3.7%
1.7%
0.9%
0
0.5
1
1.5
2
2.5
3
3.5
4
Placebo Phen/TPM ER 7.5/46 mg Phen/TPM ER 15/92 mg
Pro
gre
ss
ors
pe
r y
ea
r (%
)
Garvey WT, et al. Am J Clin Nutr. 2012;95:297-308.
76%
54%
Annualized Incidence of T2DM

Multifaceted Approaches to Optimize Care for Patients with Obesity
© 2015 Vindico Medical Education
Patients with Extreme Obesity (BMI >45)
Kahan S, et al. Poster: The Obesity Society, Nov 2015.
22.4
8.6
3.5 3.5
64.1
30.8
10.3
5.1
83.1
69
50.7
28.2
0
10
20
30
40
50
60
70
80
90
Weight loss of ≥5% Weight loss of ≥10% Weight loss of ≥15% Weight loss of ≥20%
Placebo Phentermine / Topiramate ER 3.75/23 (n=39)
Phentermine / Topiramate ER 15/92 (n=71)
**
**
**
**
**
*
*
* P ≤ .01 vs. placebo
** P ≤ .001 vs. placebo
Phentermine/Topiramate ER: Adverse Reactions
Leading to Treatment Discontinuation
Placebo
(n=1561), %
Phentermine/
Topiramate ER
3.75 mg/23 mg
(n=240), %
Phentermine/
Topiramate ER
7.5 mg/46 mg
(n=498), %
Phentermine/
Topiramate ER
15 mg/92 mg
(n=1580), %
Vision blurred 0.5 2.1 0.8 0.7
Headache 0.6 1.7 0.2 0.8
Irritability 0.1 0.8 0.8 1.1
Dizziness 0.2 0.4 1.2 0.8
Paraesthesia 0.0 0.4 1.0 1.1
Insomnia 0.4 0.0 0.4 1.6
Depression 0.2 0.0 0.8 1.3
Anxiety 0.3 0.0 0.2 1.1
Qsymia (phentermine and topiramate) capsules [package insert]. Mountain View, CA: Vivus; 2014.
Billes SK, et al. Pharm Res. 2014;84:1-11.
β-endorphin
α-MSH
-
+MC4 receptor
μ-opioid receptor
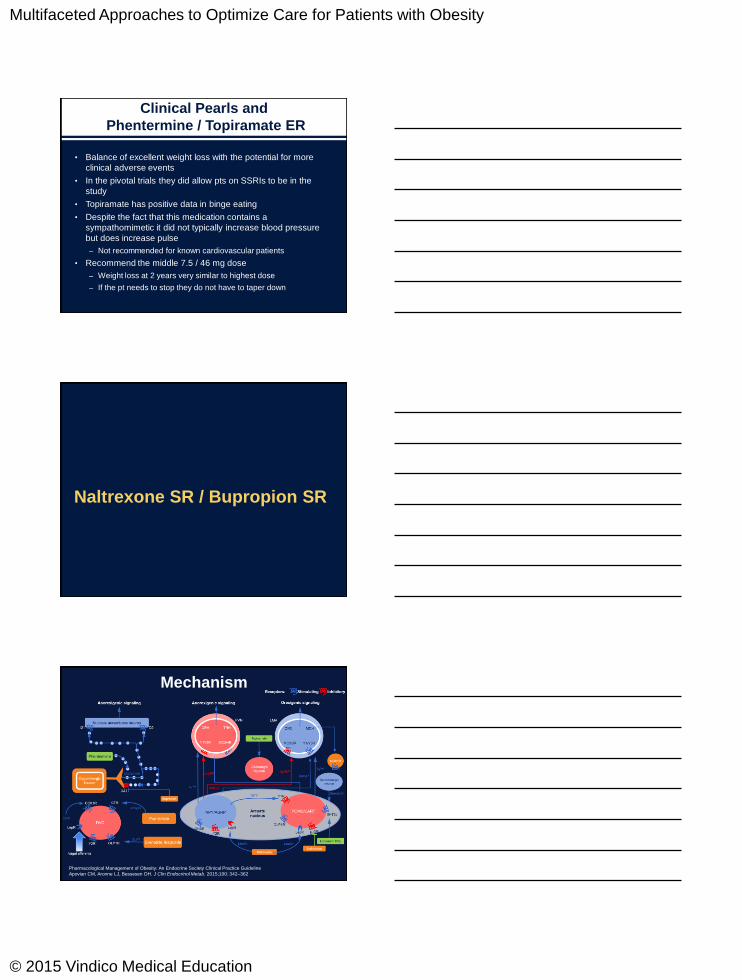
Naltrexone SR / Bupropion SR:
Mechanism of Action

Multifaceted Approaches to Optimize Care for Patients with Obesity
© 2015 Vindico Medical Education
Naltrexone SR / Bupropion SR
• Bupropion: Dopamine/norepinephrine
reuptake inhibitor
• Naltrexone: opioid receptor antagonist
• Approved 2014
• Long-term use; not controlled
• Dosing (8 mg / 90 mg tabs): titrate
weekly to 2 BID
• Consider discontinuation if <5%
weight loss after 12 weeks
• Contraindications: pregnancy,
seizures, uncontrolled HTN, chronic
opioid use, MAOI use
Contrave prescribing information. Takeda Pharmaceuticals. Greenway, et al. Obesity. 2009;17:30-39. Billes, et al. Pharm
Res. 2014; 84;1-11.
-8.1 -8.2
-11.5
-5.9
-1.8-1.4
-7.3
-2.2
-14
-12
-10
-8
-6
-4
-2
0
Naltrexone / Bupropion Placebo
Naltrexone SR / Bupropion SR :
Patients Completing 1 Year of Treatment
Wadden TA, et al. Obesity. 2011;19:110-20. Hollander P, et al. Diab Care. 2013;36(12):4022-9. Greenway, et al. Obesity.
2009;17:30-39. Apovian CM, et al. Obesity. 2013;21(5):935-43. Billes, et al. Pharm Res. 2014; 84;1-11.
COR-I COR-II COR-BMOD COR-DR
% W
eig
ht ch
an
ge
Naltrexone SR/bupropion SR 32/360 mg Placebo
Nausea 32.5% 6.7%
Constipation 19.2% 7.2%
Headache 17.6% 10.4%
Vomiting 10.7% 2.9%
Dizziness 9.9% 3.4%
Insomnia 9.2% 5.9%
Dry mouth 8.1% 2.3%
Subjects discontinuing due to AE:
Overall 24% 12%
Nausea 6.3%
Headache 1.7%
Vomiting 1.1%
Contrave (naltrexone HCL and bupropion HCL) extended-release tablets [package insert]. Deerfield, IL and La Jolla, CA:
Takeda / Orexigen; 2014.
Naltrexone SR / Bupropion SR

Multifaceted Approaches to Optimize Care for Patients with Obesity
© 2015 Vindico Medical Education
Liraglutide 3.0 mg
• GLP-1 receptor agonist
• Multiple actions; effect on weight is
primarily via POMC neurons
• Liraglutide 1.8 mg: type 2 diabetes
• Liraglutide 3.0 mg: obesity treatment
• Long-term use; not controlled
• Dosing: SC; titrate weekly by 0.6 mg
• Discontinue if <4% loss at 16 weeks
• REMS: medullary thyroid carcinoma,
acute pancreatitis
Saxenda (liraglutide) injection [package insert]. Plainsboro, NJ: Novo Nordisk; 2014; Pi-Sunyer X, et al. NEJM. 2015.
Reprinted with permission.
63.2
33.1
14.4
27.1
10.63.5
0
10
20
30
40
50
60
70
≥ 5% ≥ 10% ≥ 15%
Liraglutide Placebo
P<0.001
P<0.001
P<0.001
Pa
tie
nts
(%
)
Liraglutide 3.0 mg for Weight
Maintenance
Data submitted to FDA Endocrinologic and Metabolic Drug Advisory Committee, NDA 206-321, September 11, 2014.
Liraglutide 3.0 mg
% Liraglutide 3.0 mg Placebo Discontinuation
Nausea 39 14 2.9
Diarrhea 21 10 1.4
Vomiting 16 4 1.7
Constipation 19 8
Dyspepsia 9 3
Abdominal pain 5 3
Hypoglycemia in T2DM 23 13
Headache 14 13
Dizziness 7 5
Fatigue 7 4
Increased lipase 5 2
Overall discontinuation: 9.8% vs 4.3%
Saxenda (liraglutide) injection [package insert]. Plainsboro, NJ: Novo Nordisk; 2014.

Multifaceted Approaches to Optimize Care for Patients with Obesity
© 2015 Vindico Medical Education
Combination Therapy
Adapted from Wadden, et al. NEJM. 2005.
Medication alone
Lifestyle modification alone
Medication + brief therapy
Combined therapy
Placebo alone
Thank you
Scott Kahan, MD, MPH

Multifaceted Approaches to Optimize Care for Patients with Obesity
© 2015 Vindico Medical Education
Getting Back to the Basics –
Patient Selection for
Pharmacotherapy
Ken Fujioka, MD
Director of Nutrition and Metabolic Research
Scripps Clinic Dept. of Endocrine
Addressing Individual Patient Needs
and Preferences
• Treat obesity like any disease and work it up like a disease
• History– cause of obesity
Portion control, snacking, binge, low activity level, Craving of specific foods etc.
– comorbid diseases
– current meds
– patient expectations – on weight loss
– personal profile – wants to get pregnant?
Physical
• General: is the patient depressed
• BMI: is it over 35 kg/m2 with a co-morbidity
• Waist circumference
• Thyroid exam - nodule?
• Cardiac – Heart rate and blood pressure

Multifaceted Approaches to Optimize Care for Patients with Obesity
© 2015 Vindico Medical Education
Treatment Plan
• Medications
– Diabetic meds with weight loss
GLP-1 receptor agonists, SGLT-2 inhibitors
– Weight loss medications
Lorcaserin, Phentermine / Topiramate ER,
Naltrexone SR / Bupropion SR, Liraglutide 3.0 mg
• Bariatric Surgery
– Sleeve gastrectomy vs bypass
• Failed bariatric surgery
– Conversion to bypass
– Add weight loss medications
• Everyone gets Diet and Lifestyle modification
Lorcaserin
Mechanism
Pharmacological Management of Obesity: An Endocrine Society Clinical Practice Guideline
Apovian CM, Aronne LJ, Bessesen DH. J Clin Endocrinol Metab. 2015;100: 342–362

Multifaceted Approaches to Optimize Care for Patients with Obesity
© 2015 Vindico Medical Education
Mechanism
Pharmacological Management of Obesity: An Endocrine Society Clinical Practice Guideline
Apovian CM, Aronne LJ, Bessesen DH. J Clin Endocrinol Metab. 2015;100: 342–362
Discontinuation Rates
Due to Drug AEs
• Placebo – 6.7%
• Lorcaserin – 8.6%
– Headache – 1.3% vs 0.8%
– Depression – 0.9% vs 0.5%
– Dizziness – 0.7% vs. 0.2%
Lorcaserin (Prescribing Information) Woodcliff Lake, NJ Eisai Inc. 2012
Clinical Practice Pearls
• This is a safe drug with no stimulating effects
– Can be considered in the Cardiovascular patient #
• If you have a patient on SSRIs or other
serotonin medications then use with caution
• Hypoglycemia a risk in diabetic patients on
sulfonylureas and insulin
• The patient with portion control issues or
Satiety
# Pharmacological Management of Obesity: An Endocrine Society Clinical Practice Guideline
Apovian CM, Aronne LJ, Bessesen DH. J Clin Endocrinol Metab. 2015;100: 342–362

Multifaceted Approaches to Optimize Care for Patients with Obesity
© 2015 Vindico Medical Education
Phentermine / Topiramate ER
Mechanism
Pharmacological Management of Obesity: An Endocrine Society Clinical Practice Guideline
Apovian CM, Aronne LJ, Bessesen DH. J Clin Endocrinol Metab. 2015;100: 342–362
Mechanism
Pharmacological Management of Obesity: An Endocrine Society Clinical Practice Guideline
Apovian CM, Aronne LJ, Bessesen DH. J Clin Endocrinol Metab. 2015;100: 342–362
Multifaceted Approaches to Optimize Care for Patients with Obesity
© 2015 Vindico Medical Education
Topiramate
• Very potent weight loss agent
– Positive studies in Binge Eating
• Significant number of potential Adverse Events
– REMS program: potential for teratogenicity, cleft lip and cleft
palate
Increased heart rate
Suicide and mood and sleep disorders
Acute myopia and glaucoma
Cognitive impairment
Metabolic acidosis
Creatinine elevations
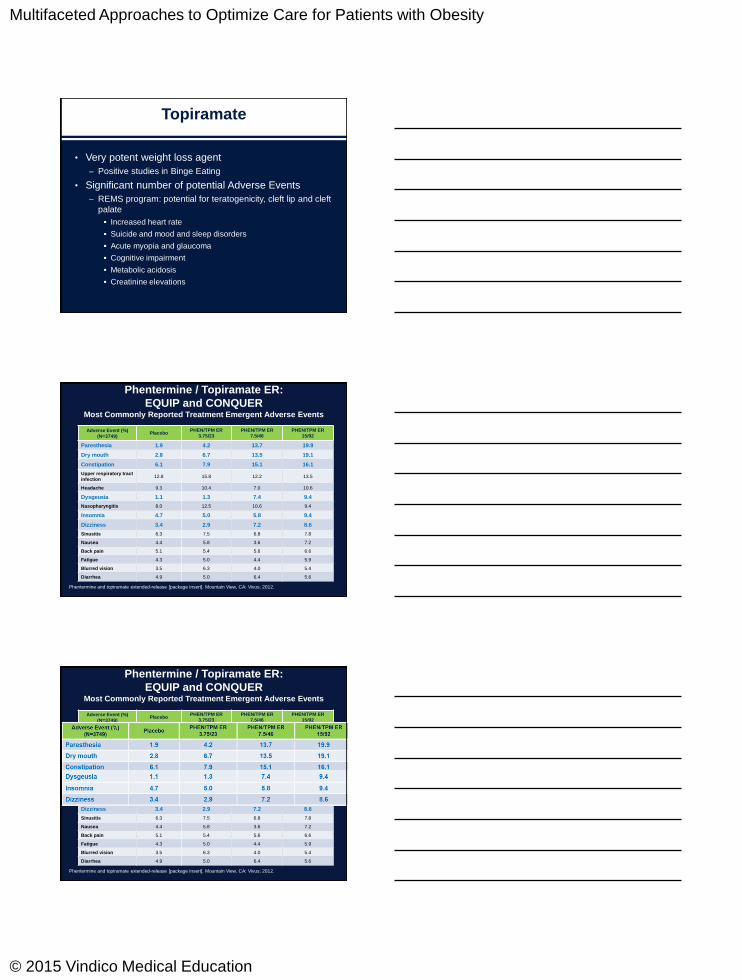
Phentermine / Topiramate ER:
EQUIP and CONQUERMost Commonly Reported Treatment Emergent Adverse Events
Phentermine and topiramate extended-release [package insert]. Mountain View, CA: Vivus; 2012.
Adverse Event (%)
(N=3749)Placebo
PHEN/TPM ER
3.75/23
PHEN/TPM ER
7.5/46
PHEN/TPM ER
15/92
Paresthesia 1.9 4.2 13.7 19.9
Dry mouth 2.8 6.7 13.5 19.1
Constipation 6.1 7.9 15.1 16.1
Upper respiratory tract
infection12.8 15.8 12.2 13.5
Headache 9.3 10.4 7.0 10.6
Dysgeusia 1.1 1.3 7.4 9.4
Nasopharyngitis 8.0 12.5 10.6 9.4
Insomnia 4.7 5.0 5.8 9.4
Dizziness 3.4 2.9 7.2 8.6
Sinusitis 6.3 7.5 6.8 7.8
Nausea 4.4 5.8 3.6 7.2
Back pain 5.1 5.4 5.6 6.6
Fatigue 4.3 5.0 4.4 5.9
Blurred vision 3.5 6.3 4.0 5.4
Diarrhea 4.9 5.0 6.4 5.6
Phentermine / Topiramate ER:
EQUIP and CONQUERMost Commonly Reported Treatment Emergent Adverse Events
Phentermine and topiramate extended-release [package insert]. Mountain View, CA: Vivus; 2012.
Adverse Event (%)
(N=3749)Placebo
PHEN/TPM ER
3.75/23
PHEN/TPM ER
7.5/46
PHEN/TPM ER
15/92
Paresthesia 1.9 4.2 13.7 19.9
Dry mouth 2.8 6.7 13.5 19.1
Constipation 6.1 7.9 15.1 16.1
Upper respiratory tract
infection12.8 15.8 12.2 13.5
Headache 9.3 10.4 7.0 10.6
Dysgeusia 1.1 1.3 7.4 9.4
Nasopharyngitis 8.0 12.5 10.6 9.4
Insomnia 4.7 5.0 5.8 9.4
Dizziness 3.4 2.9 7.2 8.6
Sinusitis 6.3 7.5 6.8 7.8
Nausea 4.4 5.8 3.6 7.2
Back pain 5.1 5.4 5.6 6.6
Fatigue 4.3 5.0 4.4 5.9
Blurred vision 3.5 6.3 4.0 5.4
Diarrhea 4.9 5.0 6.4 5.6
Multifaceted Approaches to Optimize Care for Patients with Obesity
© 2015 Vindico Medical Education
Clinical Pearls and
Phentermine / Topiramate ER
• Balance of excellent weight loss with the potential for more
clinical adverse events
• In the pivotal trials they did allow pts on SSRIs to be in the
study
• Topiramate has positive data in binge eating
• Despite the fact that this medication contains a
sympathomimetic it did not typically increase blood pressure
but does increase pulse
– Not recommended for known cardiovascular patients
• Recommend the middle 7.5 / 46 mg dose
– Weight loss at 2 years very similar to highest dose
– If the pt needs to stop they do not have to taper down
Naltrexone SR / Bupropion SR
Mechanism
Pharmacological Management of Obesity: An Endocrine Society Clinical Practice Guideline
Apovian CM, Aronne LJ, Bessesen DH. J Clin Endocrinol Metab. 2015;100: 342–362

Multifaceted Approaches to Optimize Care for Patients with Obesity
© 2015 Vindico Medical Education
Mechanism
Pharmacological Management of Obesity: An Endocrine Society Clinical Practice Guideline
Apovian CM, Aronne LJ, Bessesen DH. J Clin Endocrinol Metab. 2015;100: 342–362
COR-1: Change in Selected Items from the
Control of Eating Questionnaire at Week 56
Greenway FL, Fujioka K, Plodkowsky R, et al. Lancet. 2010;376, 595-605.
*P <.05 vs placebo.
How hungry have you felt?
How full have you felt?
How difficult has it been
to control your eating?
How difficult has it been
to resist any food cravings?
How often have you eaten
in response to food cravings
How often have you had
food cravings for starchy foods?
-20 -15 -10 -5 0 -5
Less Change from baseline (mm) More
*
**
**
*
*
*
Placebo (n=511)
Naltrexone 16 mg plus
bupropion (n=471)
Naltrexone 32 mg plus
bupropion (n=471)
Adverse Events
• Nausea
– Forced Titration in studies
• Constipation
• Headache
• Vomiting
• Dizziness
• Insomnia
– Take second dose late afternoon
• Dry mouth
Table 3. Adverse Reactions Reported by Obese or Overweight Patients
With an Incidence (%) of at Least 2% Among Patients Treated with
Naltrexone SR / Bupropion SR and More Common than with Placebo
Naltrexone SR / Bupropion SR
Multifaceted Approaches to Optimize Care for Patients with Obesity
© 2015 Vindico Medical Education
Drug-Drug and Other Interactions
• Ticlopidine and Clopidogrel (Plavix)
– Decrease dose to 1 BID
• Seizure risk with bupropion thus do not give
to patients with a seizure history
• 1 to 2 mm Hg rise in blood pressure and
pulse (check BP the first 12 weeks)
• Do not give to patient on chronic opioids
Clinical Pearls
Naltrexone SR / Bupropion SR
• Bupropion a known anti-depressant thus useful in
the depressed patient
– Be cautious with combining with other depression
meds (potential for interaction)
• Has the potential to work on “Cravings” and food
reward type eating
• Recommend slow titration, (or back titration) and
may not need to go to the highest dose
• If patient has insomnia may need to take second
dose earlier in the day.
Liraglutide 3.0 mg

Multifaceted Approaches to Optimize Care for Patients with Obesity
© 2015 Vindico Medical Education
Mechanism
Pharmacological Management of Obesity: An Endocrine Society Clinical Practice Guideline
Apovian CM, Aronne LJ, Bessesen DH. J Clin Endocrinol Metab. 2015;100: 342–362
Mechanism
Pharmacological Management of Obesity: An Endocrine Society Clinical Practice Guideline
Apovian CM, Aronne LJ, Bessesen DH. J Clin Endocrinol Metab. 2015;100: 342–362
Liraglutide 3.0 mg Delayed Time
to Onset of T2DM
Time to onset of T2DM, Weibull analysis
Time to onset of T2DM over 3 years:
• 2.7 times longer
95% CI [1.9; 3.9] (p<0.0001)
Estimated hazard ratio at week 160
(liraglutide 3.0 mg/placebo):
• HR = 0.207 (p<0.0001)
• Risk reduction: 79.3%
Numbers needed to treat (NNT):
• 14 / 3 years88
90
92
94
96
98
100
0 16 32 48 64 80 96 112 128 144 160
γ=2.68
SPlacebo(60)
SLira(160)
Part
icip
an
ts n
ot
dia
gn
osed
with
T2
DM
(%
)
Week
Liraglutide 3.0 mg Placebo
The time of onset of T2DM occurs in between the first of the two required registrations of elevated HbA1c, FPG or 2-hour OGTT plasma glucose, and the diabetes
assessment visit prior to the first registration. The estimated survival time is based on an analysis of time to onset of T2DM analyzed in a Weibull model that includes
treatment, sex and baseline BMI stratum as fixed factors and baseline FPG value as covariate. BMI, body mass index; FAS, full analysis set; FPG, fasting plasma
glucose; HbA1c, glycosylated hemoglobin; HR, hazard ratio; NNT, number needed to treat; OGTT, oral glucose tolerance test; T2DM, type 2 diabetes mellitus
le Roux et al. Obesity Week 2015, 2–6 November 2015, Poster T-P-LB-3843
Multifaceted Approaches to Optimize Care for Patients with Obesity
© 2015 Vindico Medical Education
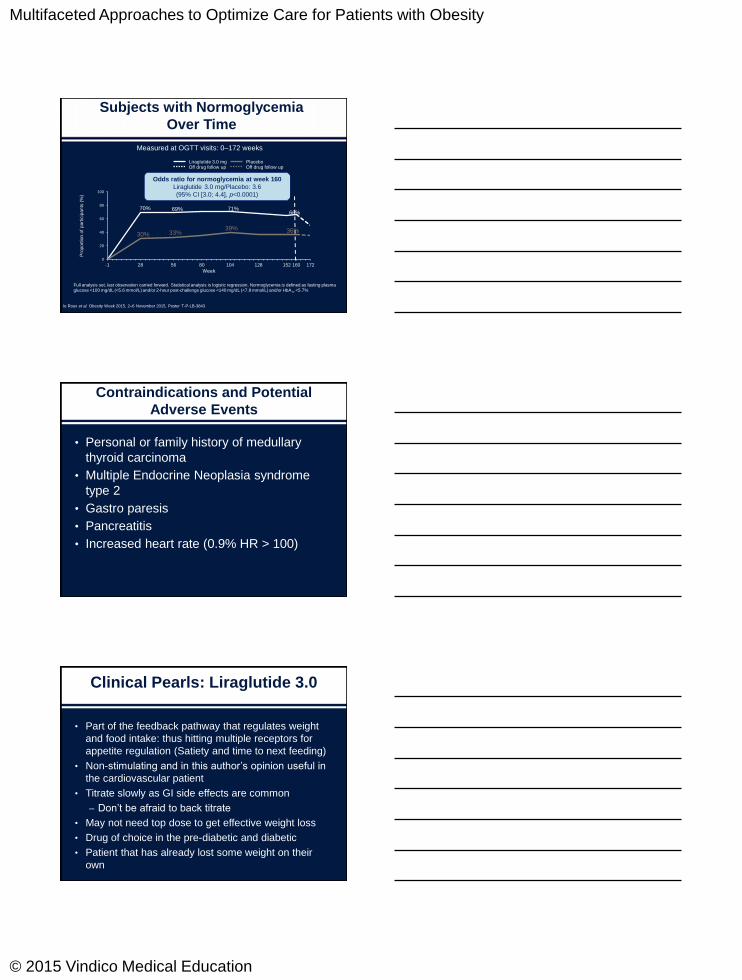
Subjects with Normoglycemia
Over Time
0
20
40
60
80
100
-1 28 56 80 104 128 152 160 172
Liraglutide 3.0 mg PlaceboOff drug follow up Off drug follow up
Pro
port
ion
of
part
icip
an
ts (
%)
Week
Full analysis set, last observation carried forward. Statistical analysis is logistic regression. Normoglycemia is defined as fasting plasma
glucose <100 mg/dL (<5.6 mmol/L) and/or 2-hour post-challenge glucose <140 mg/dL (<7.8 mmol/L) and/or HbA1c <5.7%
66%
36%
Odds ratio for normoglycemia at week 160
Liraglutide 3.0 mg/Placebo: 3.6
(95% CI [3.0; 4.4], p<0.0001)
71%
39%
69%
33%
70%
30%
le Roux et al. Obesity Week 2015, 2–6 November 2015, Poster T-P-LB-3843
Measured at OGTT visits: 0–172 weeks
Contraindications and Potential
Adverse Events
• Personal or family history of medullary
thyroid carcinoma
• Multiple Endocrine Neoplasia syndrome
type 2
• Gastro paresis
• Pancreatitis
• Increased heart rate (0.9% HR > 100)
Clinical Pearls: Liraglutide 3.0
• Part of the feedback pathway that regulates weight
and food intake: thus hitting multiple receptors for
appetite regulation (Satiety and time to next feeding)
• Non-stimulating and in this author’s opinion useful in
the cardiovascular patient
• Titrate slowly as GI side effects are common
– Don’t be afraid to back titrate
• May not need top dose to get effective weight loss
• Drug of choice in the pre-diabetic and diabetic
• Patient that has already lost some weight on their
own
Multifaceted Approaches to Optimize Care for Patients with Obesity
© 2015 Vindico Medical Education
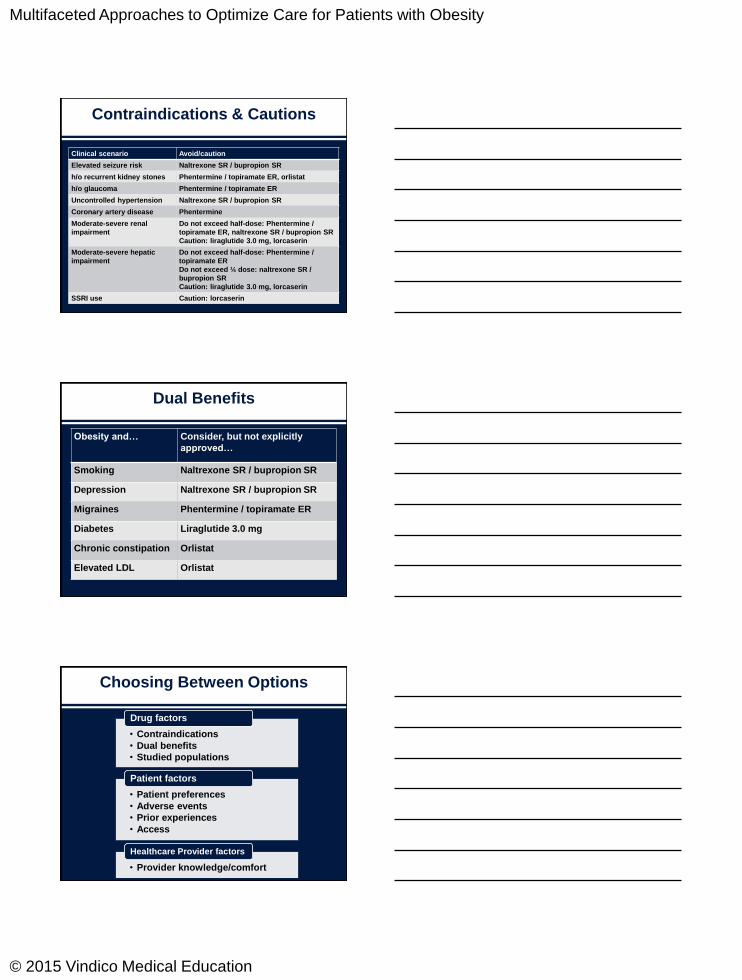
Contraindications & Cautions
Clinical scenario Avoid/caution
Elevated seizure risk Naltrexone SR / bupropion SR
h/o recurrent kidney stones Phentermine / topiramate ER, orlistat
h/o glaucoma Phentermine / topiramate ER
Uncontrolled hypertension Naltrexone SR / bupropion SR
Coronary artery disease Phentermine
Moderate-severe renal
impairment
Do not exceed half-dose: Phentermine /
topiramate ER, naltrexone SR / bupropion SR
Caution: liraglutide 3.0 mg, lorcaserin
Moderate-severe hepatic
impairment
Do not exceed half-dose: Phentermine /
topiramate ER
Do not exceed ¼ dose: naltrexone SR /
bupropion SR
Caution: liraglutide 3.0 mg, lorcaserin
SSRI use Caution: lorcaserin
Dual Benefits
Obesity and… Consider, but not explicitly
approved…
Smoking Naltrexone SR / bupropion SR
Depression Naltrexone SR / bupropion SR
Migraines Phentermine / topiramate ER
Diabetes Liraglutide 3.0 mg
Chronic constipation Orlistat
Elevated LDL Orlistat
Choosing Between Options
• Contraindications
• Dual benefits
• Studied populations
Drug factors
• Patient preferences
• Adverse events
• Prior experiences
• Access
Patient factors
• Provider knowledge/comfort
Healthcare Provider factors

Multifaceted Approaches to Optimize Care for Patients with Obesity
© 2015 Vindico Medical Education