platelet function and blood coagulation system status in ... · platelet function and blood...
TRANSCRIPT

Full Terms & Conditions of access and use can be found athttps://www.tandfonline.com/action/journalInformation?journalCode=iplt20
Platelets
ISSN: 0953-7104 (Print) 1369-1635 (Online) Journal homepage: https://www.tandfonline.com/loi/iplt20
Platelet function and blood coagulation systemstatus in childhood essential thrombocythemia
Dmitrii M. Polokhov, Nikolay M. Ershov, Anastasia A. Ignatova, EvgeniyaA. Ponomarenko, Marina V. Gaskova, Pavel A. Zharkov, Daria V. Fedorova,Alexandr V. Poletaev, Elena A. Seregina, Galina A. Novichkova, Nataliya S.Smetanina & Mikhail A. Panteleev
To cite this article: Dmitrii M. Polokhov, Nikolay M. Ershov, Anastasia A. Ignatova, Evgeniya A.Ponomarenko, Marina V. Gaskova, Pavel A. Zharkov, Daria V. Fedorova, Alexandr V. Poletaev,Elena A. Seregina, Galina A. Novichkova, Nataliya S. Smetanina & Mikhail A. Panteleev (2019):Platelet function and blood coagulation system status in childhood essential thrombocythemia,Platelets, DOI: 10.1080/09537104.2019.1704710
To link to this article: https://doi.org/10.1080/09537104.2019.1704710
Published online: 19 Dec 2019.
Submit your article to this journal
View related articles
View Crossmark data

Platelet function and blood coagulation system status in childhoodessential thrombocythemia
Dmitrii M. Polokhov 1, Nikolay M. Ershov 1, Anastasia A. Ignatova 1, Evgeniya A. Ponomarenko 1,Marina V. Gaskova 1, Pavel A. Zharkov 1, Daria V. Fedorova 1, Alexandr V. Poletaev 1, Elena A. Seregina 1,Galina A. Novichkova 1, Nataliya S. Smetanina 1, & Mikhail A. Panteleev 1,2,3,4
1Oncology and Immunology, Federal Research and Clinical Centre of Pediatric Hematology, Moscow, Russian Federation, Russia, 2Center forTheoretical Problems of Physicochemical Pharmacology, Moscow, Russia, 3Faculty of Physics, Moscow State University, Moscow, Russia, and 4Facultyof Biological and Medical Physics, Moscow Institute of Physics and Technology, Dolgoprudny, Russia
Abstract
Childhood essential thrombocythemia (ET) is a rare chronic myeloproliferative disorder. Thequality of life of ET patients may decrease as a result of ischemic and hemorrhagic complica-tions of unclear origin. Our goal was to characterize the hemostatic system in children with ET.We genotyped and investigated blood samples from 20 children with ET in a prospective caseseries study using platelet aggregation, functional flow cytometry (FC) assay and standardclotting assays. Three children had a JAK2V617F mutation, 4 had mutations in CALR and 13were triple-negative. Myelofibrosis in stage 1-2 was detected in 3 children. Three patients hadbleeding episodes and seven had ischemic events. Aggregation in response to collagen,adenosine diphosphate, and ristomycin was decreased in all patients. In FC, significant changesin the whole patient group compared to the healthy children control group were decrease inthe resting forward scatter and PAC1 binding (activated GPIIb/IIIa) level. For the activatedplatelets, dense granules release (by mepacrine), PAC1, and GPIIb/IIIa levels were significantlydecreased. GPIb/V/IX, P-selectin, and phosphatidylserine levels manifested only moderatedifferences. Forward and side scatter changes in response to stimulation (representing shapechange) and dense granules release were significantly lower in the 3 patients with bleedingthan in the 17 patients without hemorrhage. Activated partial thromboplastin time was slightlyprolonged, prothrombin index was slightly shortened and thrombin time was normal, whilefibrinogen was mildly decreased in the ET patients. It could be concluded that the observedplatelet function defects could be related to bleeding in ET, and be potentially used asa marker.
Keywords
Blood coagulation tests, essential thrombo-cythemia, flow cytometry, plateletaggregation
History
Received 19 July 2019Revised 15 November 2019Accepted 8 December 2019Published online 21 December 2019
Introduction
Essential thrombocythemia (ET) is a chronic myeloproliferativedisorder (CMPD) characterized by an increase in the plateletcount of more than 450 thousands/μL and megakaryocytic hyper-plasia in bone marrow (BM). It can be accompanied by leukocy-tosis, spleno- and hepatomegaly, hemorrhage and thrombosis, andpossible transformation to myelofibrosis (MF) or acute leukemia(AL) [1]. The reported incidence of ET in childhood is approxi-mately 1 per 10.000.000, which is 60 times lower than in adults[1,2]. The leading hypothesis regarding the onset of ET is damageto the pluripotent hematopoietic stem cell genome. Emergingmutations in the JAK2, MPL or CALR genes trigger the activationmechanism of the JAK/STAT signaling pathway; however, thereare “triple-negative” patients with none of these genes affected[3–10]. There are no reliable data on the prevalence of mutationsin children [2–4,8]. Splenomegaly and hepatomegaly in children,
individually or in combination, can occur in approximately half ofthe patients [2].
Clinical manifestations of ET are mainly neurological (e.g.,dizziness, headache, syncope, and transient ischemic attack),microcirculatory (e.g., rodonalgia, acroparesthesia, ischemia ofthe fingers and visual impairment), gastrointestinal (e.g., nausea,vomiting and abdominal pain) and hemorrhagic (e.g., nasal bleed-ing, petechiae, ecchymosis and other). Thrombotic and hemor-rhagic complications are the main causes of mortality amongadult patients with ET [1,2,11]. The frequency of thromboticevents in children is 0-17% [2].
It was reported that platelets in adult patients with ET areabnormal. Various changes in the platelet phenotype include thenumber of CD62p (P-selectin), CD63 and GPIIb/IIIa (PAC1 bind-ing) receptors at rest and after activation of TRAP (thrombinreceptor-activating peptide) and CRP (collagen-related peptide)[12]. Immunophenotyping reveals a state of intravascular plateletactivation [10]. According to a study of platelet aggregation in 55adult patients with ET in platelet-rich plasm (PRP), aggregationwas impaired in 75% of them. However, these ex vivo tests do notdetect platelet hyperaggregability [10]. These changes in the reac-tivity of platelets have not been definitively identified as the causes
Correspondence: Mikhail Panteleev, Dmitry Rogachev National MedicalResearch Center of Pediatric Hematology, Oncology and Immunology, 1Samory Mashela str., Moscow 117997, Russian Federation.Email: [email protected]
http://www.tandfonline.com/ipltISSN: 0953-7104 (print), 1369-1635 (electronic)
Platelets, Early Online: 1–11© 2019 Taylor & Francis Group, LLC. DOI: https://doi.org/10.1080/09537104.2019.1704710

of thrombotic or hemorrhagic complications, with the exception oferythromelalgia and acquired von Willebrand syndrome [1]. In thepresent study, we attempted to gain insight into the mechanism ofhemostasis abnormalities in children with ET by carrying outlaboratory analysis of their hemostasis parameters.
Materials and Methods
Study Design and Recruitment of Patients
Study design is a prospective, case series investigation. Duringthe period from February 2015 to April 2019, we examined 20children with ET (Table I). The diagnosis of ET was establishedaccording to the diagnostic criteria of WHO [13]. The study wasapproved by the Independent Ethics Committee of the RogachevNational Medical Research Center of Pediatric Hematology,Oncology, and Immunology (protocol #8/2016 from18.10.2016). Written informed consent was obtained from allhealthy volunteers and patients, or from their officialrepresentatives.
Clinical and Laboratory Examination
The patients underwent clinical and laboratory examination,including routine studies, genetic and morphological studies ofbone marrow and platelets, examination of the liver and spleen,and functional tests of the hemostasis system. Genetic studieswere conducted by the Sanger sequencing method. The dimen-sions of the liver and spleen were assessed by ultrasound and/ormultislice computed tomography (MSCT)/magnetic resonanceimaging (MRI). For hemostasis analysis, blood was collected byvenipuncture into 3 ml vacuum citrate tubes (S-Monovette),which were delivered to the laboratory within 15 min. Samplepreparation and analysis required 1 h.
Blood Test
The peripheral blood test was performed on a hematologicalanalyzer Sysmex XS-1000i (Sysmex Corporation, Japan).
Genetic Studies
Genetic studies were conducted by Sanger’s sequencing methodon a genetic analyzer Applied Biosystem 3130xl (AppliedBiosystems, LLC, USA).
Morphology of the Bone Marrow
The trepanobioptate was stained with hematoxylin and eosin, fol-lowed by impregnation with silver. The sample was examined usingan ECLIPSE 80i microscope (Nikon Instruments Europe B.V.,Netherlands).
Radiation Methods
Visualization of the liver and spleen was performed usinga magnetic resonance imager Achieva 3.0Т, (Philips MedicalSystems, Nederland B.V., Netherlands), and a completely digitaluniversal ultrasound diagnostic apparatus of the expert classACUSON S2000 ultrasound system (Siemens MedicalSolution, USA).
Functional Activity of Platelets: Flow Cytometry
In a cytometric study, we analyzed the marker composition ofplatelets at rest and after activation in diluted blood witha mixture of TRAP (PAR-1 receptor agonist) and CRP (a glyco-protein VI agonist) as described previously [14–16]. AnnexinV-Alexa647 and antibodies against P-selectin (CD62p-Alexa647), GPIIb/IIIa (CD61-PE), its activation (PAC1-FITC),and glycoprotein I (CD42b-PE) were from Biolegend (SanDiego, CA, USA). CRP was kindly provided by Prof. R.W.Farndale (University of Cambridge, Cambridge, UK). All otherreagents were from Sigma-Aldrich (St Louis, MO, USA).Platelets were either left intact or loaded with mepacrine(1 mM) for 30 min at 37°C. Subsequently, they were either leftunstimulated or stimulated with CRP at 20 μg/μl and SFLLRN at12.5 μM for 10 min in the presence of 2.5 mM calcium chloride.Both resting and activated samples were incubated with antibo-dies against CD61, CD42b, CD62p, as well as PAC1 and annexinV for 10 min. Then, they were diluted 10-fold with buffer
Table I. Clinical and instrumental characteristics of patients.
№ SexAge atonset
PLT atonset** PLT** Hepatomegaly Splenomegaly Other symptoms
StageMF
1 F 13 1200 1184 no yes no 0-12 F 8 2000 1549 no no no 0-13 F 4 1496 1496 no no no 0-14 M 0.6 1600 1064 no no no 0-15 M 10 2500 1736 yes no no 0-16 M 10 1013 1439 no no no 0-17 F 7 1235 951 yes yes no 0-18 M 16 1550 1522 yes yes no 0-19 M 2 1000 1104 yes no no 0-110 M 5 2246 2303 no yes no 0-111 F 9 896 1562 no no Headaches 0-112* М 10 1594 862 yes yes Headaches 0-113 М 8 1044 989 no yes Headaches; numbness of the fingers; chest pain 0-114 М 12 1800 2172 yes no Headache 115 М 15 2932 2620 yes yes Headache; stomachache 1-216 М 11 1000 1869 yes yes Headache; numbness of the fingers 0-117 F 4 1258 770 no no Headache 0-118 F 6 2500 2744 no yes Ecchymosis; nasal bleeding; bleeding after tooth
extraction1
19* F 15 2000 780 yes yes Nasal bleeding 0-120* М 16 561 603 no no Nasal bleeding 0-1
*Patients on therapy; **Platelets count, thousand cells/μL.
2 D. M. Polokhov et al. Platelets, Early Online: 1–11

A containing 2.5 mM calcium and analyzed using a Novocyteflow cytometer (Acea Bioscience, San Diego, CA, USA). Ascontrol groups for functional platelet activity assay, blood sampleswere collected from 72 healthy adults aged 18–50 years and 58healthy children (27 boys and 31 girls) with a median age of 10years (2–17 years).
Aggregometry
The study of platelet aggregation function in PRP was performedon the Biola aggregometer (Biola, Moscow, Russia) in accordancewith the Recommendations for the Standardization of LightTransmission Aggregometry (LTA): A Consensus of theWorking Party from the Platelet Physiology Subcommittee ofSSC/ISTH [17]. PRP was prepared by centrifuging blood samplesat 200 x g for 10 min. The volume of plasma PRP for the studywas 300 μl. The agonists used were: adenosine diphosphate(ADP), 5 μM (Sigma-Aldrich, St Louis, MO, USA), collagen,0.06 mg (NPO Renam, Russia), ristomycin, 0.45 mg (NPORenam, Russia). Aggregation curves were recorded for 10 min.As control blood samples were collected from 14 healthy adultswith a median age of 26.5 years (22–44 years) and 14 healthychildren with a median age of 10.5 years (5–17 years) were used.
Routine Coagulation Assays
The activated partial thromboplastin time (APTT) (normal range25.1–36.5 s), prothrombin index (PI) (normal range 9.4–13.7 s),thrombin time (TT) (normal range 15.8–24.9 s) and fibrinogenlevel (normal range 2–3.93 g/L) were determined using the ACLTOP 700 coagulation analyzer (Instrumentation Laboratory,Bedford, MA, USA) with assay kits provided by the manufacturer(Instrumentation Laboratory). To interpret the results, the refer-ence values of the manufacturer and the data obtained for thecontrol group of 62 healthy children with a median age of 9 years(1–17 years) were used. The activity of vWF (vWF: Rco) wasdetermined only for patients (normal range 48.2–201.9%).
Statistical Analysis
The analyses of significant differences were performed usinga nonparametric Mann-Whitney test with a significance level ofp < .05. For the correlation analysis, the Pearson correlationcoefficient was calculated.
Results
Patient Demographics and Characterization
The median age of the patients at the time of the laboratory exam-ination was 12.5 years (from 1.5 to 17 years). The median age ofdisease onset was 10 years (range 1.5–16 years). The gender com-position was 1.5:1 (12 boys and 8 girls, respectively). In 10 (50%)patients, the disease progressed without clinical symptoms(group 1). Seven (35%) had ischemic symptoms, including erythro-melalgia, chest pain, headaches, sometimes with nausea and vomit-ing (group 2). Thrombosis was not observed. In 3 (15%), ETmanifested according to the hemorrhagic type, including ecchymosisand/or nosebleeds of different severity (group 3). Instrumentallyidentified splenomegaly occurred in 10 (50%), hepatomegaly in 9(45%) and splenohepatomegaly in 6 cases (30%) (Table I). Out of 20children with ET examined, clonal markers were not revealed in 13(65%); these were marked as triple-negative ET. Three children(15%) had a JAK2V617F mutation, and four (20%) had a mutationin the CALR gene. Mutations in the MPL gene did not occur(Table II). ET in children has a low frequency of transformationinto post-ET MF or other malignant tumors [2]. Among the 20
children observed, MF-0-1 was detected histologically in 17 andMF-1-2 in 3 children with clinical symptoms (Table I). In trepano-bioptate, a free reticulin network was observed with many crossings,especially in perivascular regions.
Platelet Count and Status of Other Cells
The number of platelets in our study varied from 603 to 2744(normal range 204–356), with a median of 1468 thousand cells/μL. In group 1, there were 951 to 2303, with a median of 1468thousand cells/μL. In group 2, there were 770 to 2620, witha median of 1562 thousand cells/μL. In group 3, there were 603to 2744, with a median of 780 thousand cells/μL. Differencesbetween patient groups are not significant (p > .05) (Table I,Figure 1A). The mean platelet volume (MPV) ranged from 8.2 to11.8 fL, with a median of 9.15 (normal range 9–13 fL).
The leukocytes (WBC) ranged from 4.8 to 16.11 thousandcells/μL, with a median of 8.325 (normal range 6.05–9.85).WBC were increased in 7 (9.99 to 16.11 thousand of cells/μL,median 12.07) and decreased in 2 independently of their symp-toms. WBC in patients without symptoms was 4.8–13.27 thou-sand cells/μL, with a median 8.825. In those with clinicalsymptoms (ischemic and hemorrhagic), it was ranged from 5.85to 16.11 thousand cells/μL, with a median of 7.84. Median for allpatients was 8.325. Differences between groups were not signifi-cant (p > .05) (Figure 1B). The red blood cells (RBC) countranged from 3.91 to 5.45 million cells/μL with a median of 4.615(normal range 4.2–4.6) (data not shown).
Seventeen patients did not receive cytoreductive therapy for atleast 2 weeks before blood collection for the assays of hemostasisfunction. Three patients received cytoreductive therapy with ana-grelide or peg-interferon with effect (Table I).
Platelet Functional Activity: Flow Cytometry
Two groups of healthy volunteers were studied, healthy adults andhealthy children (fig. 2, 3). Adult control was used to distinguishbetween the age-dependent and age-independent changes in thepatient platelet functionality. At rest, the healthy children plateletshad significantly smaller side light scattering (SSC) (p < .001),
Table II. Genetic research results.
№ JAK2 ex. 12,14,15,19MPL
ex. 1-12 CALR ex. 9
1 WT WT BP2 WT WT WT3 WT BP BP4 WT WT c.1135delG; p.E379fs*405 WT WT WT6 WT WT WT7 WT WT WT8 WT WT c.1099-1150del52; p.L367fs*469 c.1849G>T; p.Val617Phe WT WT10 WT WT WT11 WT WT WT12 WT WT WT13 c.1849G>T;p.Val617Phe WT WT14 WT WT WT15 WT WT WT16 WT WT WT17 c.1849G>T;p.Val617Phe WT WT18 BP WT c.1149-
1154_delGGACAAinsTCCTTGTC;p.Glu383AspfsTer48
19 WT WT WT20 WT WT c.1154_1155insTTGTC p.K385fs*47
BP, benign polymorphism; WT, wild type.
DOI: https://doi.org/10.1080/09537104.2019.1704710 Hemostasis in childhood essential thrombocythemia 3
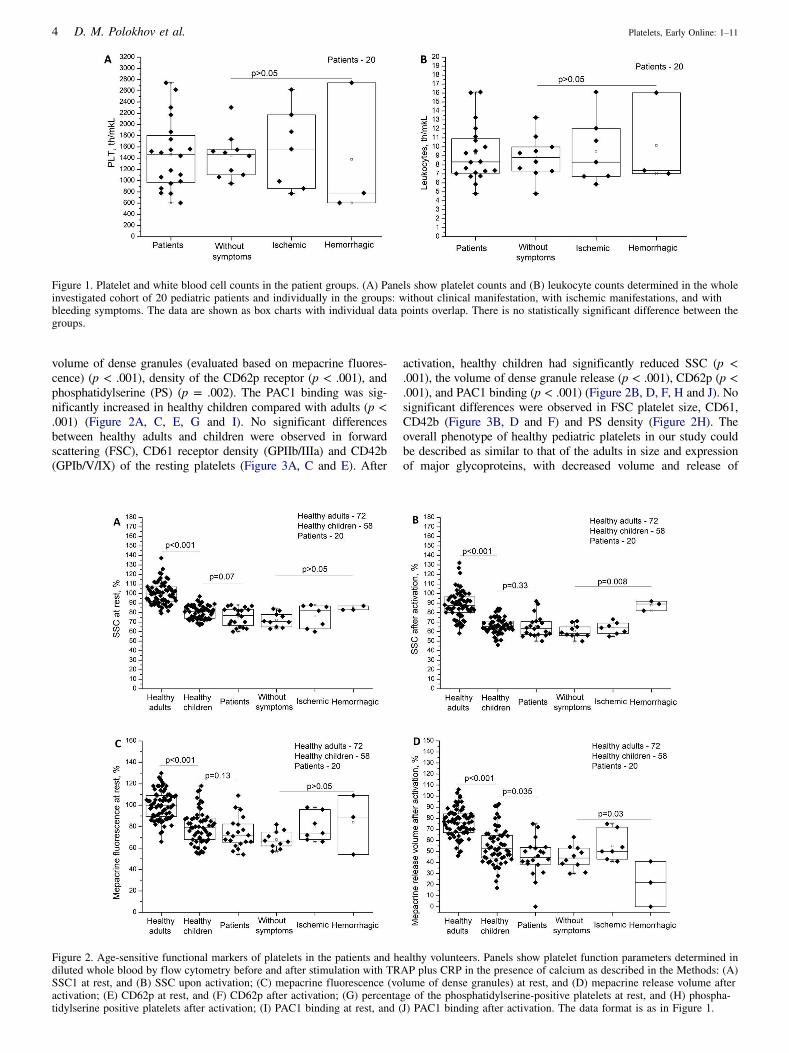
volume of dense granules (evaluated based on mepacrine fluores-cence) (p < .001), density of the CD62p receptor (p < .001), andphosphatidylserine (PS) (p = .002). The PAC1 binding was sig-nificantly increased in healthy children compared with adults (p <.001) (Figure 2A, C, E, G and I). No significant differencesbetween healthy adults and children were observed in forwardscattering (FSC), CD61 receptor density (GPIIb/IIIa) and CD42b(GPIb/V/IX) of the resting platelets (Figure 3A, C and E). After
activation, healthy children had significantly reduced SSC (p <.001), the volume of dense granule release (p < .001), CD62p (p <.001), and PAC1 binding (p < .001) (Figure 2B, D, F, H and J). Nosignificant differences were observed in FSC platelet size, CD61,CD42b (Figure 3B, D and F) and PS density (Figure 2H). Theoverall phenotype of healthy pediatric platelets in our study couldbe described as similar to that of the adults in size and expressionof major glycoproteins, with decreased volume and release of
Figure 1. Platelet and white blood cell counts in the patient groups. (A) Panels show platelet counts and (B) leukocyte counts determined in the wholeinvestigated cohort of 20 pediatric patients and individually in the groups: without clinical manifestation, with ischemic manifestations, and withbleeding symptoms. The data are shown as box charts with individual data points overlap. There is no statistically significant difference between thegroups.
Figure 2. Age-sensitive functional markers of platelets in the patients and healthy volunteers. Panels show platelet function parameters determined indiluted whole blood by flow cytometry before and after stimulation with TRAP plus CRP in the presence of calcium as described in the Methods: (A)SSC1 at rest, and (B) SSC upon activation; (C) mepacrine fluorescence (volume of dense granules) at rest, and (D) mepacrine release volume afteractivation; (E) CD62p at rest, and (F) CD62p after activation; (G) percentage of the phosphatidylserine-positive platelets at rest, and (H) phospha-tidylserine positive platelets after activation; (I) PAC1 binding at rest, and (J) PAC1 binding after activation. The data format is as in Figure 1.
4 D. M. Polokhov et al. Platelets, Early Online: 1–11

alpha- and dense granules, and with decreased level of procoagu-lant platelets and increased level of activated integrins at rest (thesetwo differences disappear upon activation).
In the cohort of patients compared with healthy children,there was a significant decrease in platelet size in FSC in theresting state (p < .001) (Figure 3A), and a decrease in PAC1binding (p = .005) (Figure 2I). Significant differences werenot observed in the SSC, volume of dense granules, the levelof CD62p, PS (Figure 2A, C, E and G) and CD61, CD42b(Figure 3C, E). After activation, the patients had significantlyreduced FSC (p = .008) (Figure 3B), volume of dense gran-ules release (p = .035) (Figure 2D), the density of CD61(p < .001) (Figure 3D) and the binding of PAC1 (p = .03)(Figure 2J). No significant differences were observed in SSCgranularity, CD62p (Figure 2B, F) and CD42b receptor den-sity (Figure 3F). One can summarize that the overall
phenotype of the ET patient platelets is that of a smallersize, decreased dense granule release and integrin expres-sion/activation.
Flow cytometry parameters of the platelets in 3 patients withhemorrhagic symptoms did not differ significantly from 17 patientswithout hemorrhages at rest. However, after activation, they did notdemonstrate a characteristic decrease in FSC (p = .008) (Figure3B) and SSC (p = .008) (Figure 2B) suggesting shape changedefects. When comparing the ratio of FSC and SSC before andafter activation, this difference remained (Figure 3F, H). Thevolume of dense granule release was significantly reduced (p =.03) (Figure 2D) and the density of CD42b receptor was increased(p = .02) (Figure 3F) in the patients with hemorrhage, but nosignificant differences were observed in the CD62p alpha granules,PS, binding of PAC1 (Figure 2F, H and J) and CD61 (Figure 3D).
Figure 2. (Continued).
DOI: https://doi.org/10.1080/09537104.2019.1704710 Hemostasis in childhood essential thrombocythemia 5

Patients with ischemic symptoms did not significantly differ frompatients with asymptomatic ET.
We examined differences in platelet phenotype depending on thegenetic markers of the disease. Patients with a triple-negative formof the disease (n = 13) and having a mutation in the JAK2 or CALRgene (n = 7) were compared. In patients with mutations, platelet sizewas significantly increased (Figure 6A, B, p = .03), CD62p was
significantly increased after activation (Figure 6C, p = .03) and thevolume of dense granules release was reduced (Figure 6D, p = .047).
Platelet Aggregation
Platelet aggregation in response to ADP, collagen, and ristomycinin patients revealed a significant impairment (p < .05) compared
Figure 3. Age-independent markers of platelet function. Panels show platelet function parameters determined by flow cytometry under the sameconditions as in Figure 2: (A) FSC at rest, and (B) FSC upon activation; (C) CD61 at rest, and (D) CD61 after activation; (E) CD42b at rest, and (F)CD42b after activation; ratios of (G) SSC and (H) FSC for resting platelets and activated ones. The data format is as in Figure 1.
6 D. M. Polokhov et al. Platelets, Early Online: 1–11

with the adult and pediatric control groups. Interestingly, nosignificant differences were observed between healthy childrenand adults. Likewise, there were no significant differences inaggregation between groups of patients with different clinicalmanifestations (Figure 4A–C). However, the mean values ofaggregation degree were several-fold smaller for patients withbleeding suggesting that the difference could become significantwith more patients.
Blood Coagulation Assays
In the cohort of patients compared with healthy children, fibrino-gen level was decreased (p = .005), while TT did not differsignificantly in patients compared with the control group. APTTwas prolonged (p < .001), and PI was decreased (p = .016). ThevWF: Rco was measured in 19 patients, and it was decreased in14 of them. There were no significant differences between patientgroups in these tests (p > .05) (Figure 5A-E). The activity of vonWillebrand factor was reduced to 0% in 2 children with clinicalsymptoms and a platelet count more 2600 thousand cells/μL. Inthe 10 children without clinical symptoms median of vWF Rcowas 34%. In the nine children with clinical manifestations, themedian of vWF Rco was 14.3%.
The number of platelets and leukocytes, the results of LTA andclotting assays did not significantly differ between patients witha triple-negative form of ET and having mutations in the CALRand JAK2 genes (date not shown).
A marked negative correlation (Cpearson = −0.64) between theplatelet count and von Willebrand factor activity was revealed in thestudyof the Pearson correlations between the tests (Figure 5F).Aweaknegative correlation (Cpearson =−0.3, p = .2) was observed between
the activity of vonWillebrand factor and agglutinationwith ristomycin(Figure 4D).We did not observe a correlation between CD42b densityand agglutination with ristomycin (Cpearson = −0.06), correlationbetween PAC1 binding after activation and aggregation with ADP orcollagen was also weak (Cpearson = −0.16 and −0.13, respectively)(data not shown).
Discussion
The main goal of our work was to study the characteristics of thehemostasis system in pediatric patients with ET and their poten-tial associations with the relevant symptoms of the disease. Themain conclusions are:
(1) Patients’ platelets are smaller in size compared with healthyvolunteers; the volume of the release of dense granules, thelevel of CD61 and PAC1 binding are reduced after activation;
(2) In the three patients with bleeding, the platelets did not showa reduction in FSC size and SSC granularity after activationthat was characteristic of others; these morphologicalabnormalities were combined with a decrease in dense gran-ule release and decreased CD42b loss;
(3) Despite the pronounced thrombocytosis and clinical manifes-tations, no significant increase in markers of intravascularactivation (PAC1 binding, CD62p, and PS) was detected onnon-stimulated platelets;
(4) The marker composition of platelets in healthy adults issomewhat different from healthy children, which makes itinappropriate to use references for adults to pediatric patients.
An important point for the interpretation of these results is theproblem of “healthy childhood hemostasis”. The reference ranges
Figure 4. The results of light-transmission aggregometry in healthy volunteers and patients. Panels show the maximal degree of platelet aggregationinduced by (A) ADP, (B) collagen, and (C) ristomycin. Panel (D) shows the correlation between the activity of von Willebrand factor and aggregationwith ristomycin.
DOI: https://doi.org/10.1080/09537104.2019.1704710 Hemostasis in childhood essential thrombocythemia 7

for platelet-dependent and blood coagulation assays in children ofdifferent ages are sorely lacking. In particular, there are reportsthat platelet function could be either significantly decreased[16,18,19] or increased [20] in children compared to adults.Therefore, we included not only healthy adult, but also matchedchildren control groups for all hemostasis assays of the presentstudy. This turned out not to be critical for aggregation, where weobserved no difference between healthy adults and children, butan impaired response for all children patients compared withhealthy children. However, this had a critical impact on the con-clusions from the flow cytometry part of the study, where healthychildren had less reactive platelets (thus more in line with[16,18,19]). Like in aggregation, patients as a group differedfrom healthy children by decreased integrin activation and dense
granule release. However, cytometry was able to observe differ-ences between bleeding and non-bleeding patients to the best ofour knowledge, there were no previous reports on this possibility.Interestingly, hemorrhage were mostly related to light scatterchanges and impaired mobilization of dense granules. Theseresults could be important for a better understanding of the natureof platelet function in children and its relationship to bleeding,although additional research and larger age-dependent cohorts areneeded for definitive conclusions.
According to Soyer N, among 708 adult patients with CMPD,ET patients accounted for more than half (390 patients). Whendiagnosed, thrombosis was observed in 15.12% of patients andbleeding occurred in 9% [11]. For comparison, among our 20pediatric patients, ischemic symptoms were observed in 35%, and
Figure 5. Coagulogram results in healthy volunteers and patients. Panels show coagulation assays with (A) fibrinogen concentration, (B) thrombintime, (C) APTT, (D) prothrombin index, (E) activity of von Willebrand factor for healthy donors and patient groups. Panel (F) shows a correlationbetween platelet count and the activity of von Willebrand factor.
8 D. M. Polokhov et al. Platelets, Early Online: 1–11

hemorrhagic in 15%. It is worth noting that we did not findsignificant differences in any of the tests for patients withischemic symptoms compared with asymptomatic ET and to thebest of our knowledge, there were no previous reports about thesediffernces. This could mean that, even if these symptoms arerelated to hemostasis, the mechanisms could be beyond the plate-let functionality.
The general decrease of activated integrins on platelets of thepatients may be important as a mechanism of their decreasedaggregation. Still, correlation analysis showed a poor correlationof the degree of aggregation of platelets with ADP and collagenwith PAC1 binding after platelet activation by a mixture of CRP+ TRAP in patients and healthy children (data not shown) and tothe best of our knowledge, there were no previous reports on thispossibility. This result clearly illustrates the need to understandthe characteristics of the nature of platelet activation in responseto various agonists and their combinations to interpret the results.
The platelet differences in size and characteristics of dense andalpha granules observed between patients with mutations andtriple-negative forms of ET require further study. We have notseen such observations in the literature. Likewise, a larger groupof patients is needed to ascertain whether increased P-selectin isassociated with an increase in the number of leukocyte-plateletaggregates, and a decrease in the release of dense granules isassociated with the increased manifestation of bleeding.
It was previously reported that, in adult patients, CD42b andCD41 (GPIIb/IIIa) levels at rest were significantly reduced com-pared with a control group of healthy volunteers [21]. Binding ofPAC1 [12], CD63 of dense granules [22] and CD62p [12,21,22]was higher, which is sign of intravascular platelet activation.After stimulation, CD41, CD62p [21] and CD63 [12,21] weredecreased compared with the normal values, which agrees with
the suggestion of intravascular platelet activation and suggestsimpaired platelet function. PAC1 after activation was not signifi-cantly different from healthy volunteers [12]. Severe intravascularactivation in adult patients with ET compared with childrenresulted from a large number of age-related risk factors, especiallythe presence of cardiovascular diseases [10,12,21,22]. These datawith adult patients differ from those obtained by us with children(we observed impaired PAC1 and not signs of pre-activation atrest), but also point toward the generally impaired plateletfunction.
In the analysis of 657 cases of ET, with the age of patientsfrom 8 to 93 years, a median of 52 years, it was shown that anincreased number of leukocytes (from 3.28 to 35 thousand cells/μL, median 8.73) is associated with a threefold increase in the riskof thrombosis [23]. It has also been reported that, in patients withpolycythemia vera and ET, an increased WBC count is associatedwith an increased incidence of thrombotic or hemorrhagic events[24]. In our study, the median number of leukocytes in patientswith clinical symptoms was lower than without symptoms, whichdiffers the previously cited data and requires further study.
It is known that ET, in adult and children, with platelet countsin excess of 500–1000 thousand cells/μL is often associated withan acquired von Willebrand syndrome (aVWS). Such patientshave reduced vWF activity due to a decrease or absence oflarge forms of plasma vWF multimers [25–28]. In clonal andreactive thrombocytosis, the basic mechanisms appear to be thesame: vWF multimers with a high molecular weight in plasmatemporarily bind to an increased mass of circulating platelets andare primarily degraded by ADAMTS13 [29]. Thus, in both cases,aVWS can explain the obvious paradox of why thrombocytosiscan be associated with bleeding. Our study demonstrated anaVWS in patients and indicates the possible connection between
Figure 6. Significant differences in the platelet phenotype of patients were observed depending on the genetic characteristics of the disease. Panelsshow the relationship between the disease genotype and platelet phenotype in patients with triple-negative forms of ET and with gene mutations (JAK2and CALR): (A) FSC at rest and (B) FSC upon activation, (C) CD62p after activation and (D) mepacrine release volume after activation.
DOI: https://doi.org/10.1080/09537104.2019.1704710 Hemostasis in childhood essential thrombocythemia 9

the degree of thrombocytosis, von Willebrand factor activity andthe nature of the clinical manifestations (Table I, Figure 5E, F), inagreement with the existing concepts about aVWS.
Summarizing the results of the study, we show that plateletfunctions is generally impaired in ET, in particular, adhesion(decries vWf Rco, disruption of aggregation with ristomycin),integrin activation and dense granule release (as observed byaggregation assay and flow cytometry), while platelet shapechange and dense granule release seem to be specifically impairedin the patients with bleeding. These results suggest the possibilityof using these tools to evaluate the risks of complications.
Acknowledgements
The authors thank the patients and healthy volunteers who participated inthe study and colleges who supported our work: Dmitry S. Abramov forbone marrow morphology, Yuliya V. Olshanskaya for genetic analysis,Svetlana A. Plyasunova for blood tests, Fazoil I. Ataullakhanov forimportant discussions. The authors were supported by a grant from theendowment foundation «Doctors, innovations, science for children», andby the Russian Foundation for Basic Research grants 17-04-01309, 17-00-00140 and 18-34-20026. This research was supported by the charita-ble “Grant life” foundation.
Addendum
Dmitrii M. Polokhov designed the study, performed experiment, analyzeddata, and wrote the manuscript. Nicolay M. Ershov, Pavel A. Zharkov andNataliya S. Smetanina recruited patients and critically revised the manu-script. Daria V. Fedorova recruited patients. Anastasia A. Ignatova,Evgeniya A. Ponomarenco, Alexander V. Poletaev, Elena A. Sereginaperformed experiments and analyzed data. Marina V. Gaskova performedexperiments and edited the manuscript. Galina A. Novichkova andMikhail A. Panteleev edited the manuscript.
Disclosure of Conflict of Interests
All authors state that they have no conflict of interest.
ORCID
Dmitrii M. Polokhov http://orcid.org/0000-0001-6905-2878Nikolay M. Ershov http://orcid.org/0000-0003-2677-367XAnastasia A. Ignatova http://orcid.org/0000-0002-5217-3937Evgeniya A. Ponomarenko http://orcid.org/0000-0002-8697-7570Marina V. Gaskova http://orcid.org/0000-0002-3277-9018Pavel A. Zharkov http://orcid.org/0000-0003-4384-6754Daria V. Fedorova http://orcid.org/0000-0003-4567-1871Alexandr V. Poletaev http://orcid.org/0000-0001-5209-2099Elena A. Seregina http://orcid.org/0000-0002-7534-3863Galina A. Novichkova http://orcid.org/0000-0002-2322-5734Nataliya S. Smetanina http://orcid.org/0000-0002-8805-1499Mikhail A. Panteleev http://orcid.org/0000-0002-8128-7757
References
1. Hoffman R. 2012. Hematology: Basic principles andpractice. Essential thrombocythemia. Philadelphia, PA: ChurchillLivingstone.
2. Fu R, Zhang L, Yang R. Paediatric essential thrombocythaemia:clinical and molecular features, diagnosis and treatment. BrJ Haematol 2013;163:295–302. doi:10.1111/bjh.2013.163.issue-3
3. Sekiya Y, Okuno Y, Muramatsu H, Ismael O, Kawashima N,Narita A, Wang X, Xu Y, Hama A, Fujisaki H, et al. JAK2, MPL,and CALR mutations in children with essential thrombocythemia.Int J Hematol 2016;104:266–267. doi:10.1007/s12185-016-2022-2
4. Teer JK, Painter JS, Maciejewski JP. To the editor : CALR muta-tions in patients with essential thrombocythemia diagnosed inchildhood. Blood 2014;123:3677–3680.
5. Imai M, Araki M, Komatsu N. Somatic mutations of calreticulin inmyeloproliferative neoplasms. Int J Hematol 2017;105:743–747.doi:10.1007/s12185-017-2246-9
6. Rotunno G, Mannarelli C, Guglielmelli P, Pacilli A, Pancrazzi A,Pieri L, Fanelli T, Bosi A, Vannucchi AM. Impact of calreticulinmutations on clinical and hematological phenotype and outcome inessential thrombocythemia. Blood 2014;123:1552–1555.doi:10.1182/blood-2013-11-538983
7. Rumi E, Pietra D, Ferretti V, Klampfl T, HarutyunyanAS,Milosevic JD,ThemNCC, Berg T, Elena C, Casetti IC, et al. JAK2 or CALRmutationstatus defines subtypes of essential thrombocythemia with substantiallydifferent clinical course and outcomes. Blood 2014;123:1544–1551.doi:10.1182/blood-2013-11-539098
8. Giona F, Teofili L, Moleti ML, Martini M, Palumbo G,Amendola A, Mazzucconi MG, Testi AM, Pignoloni P,Orlando SM, et al. Thrombocythemia and polycythemia in patientsyounger than 20 years at diagnosis: clinical and biologic features,treatment, and long-term outcome. Blood 2012;119:2219–2227.doi:10.1182/blood-2011-08-371328
9. Kucine N, Chastain KM, Mahler MB, Bussel JB. Primary thrombo-cytosis in children. Haematologica 2014;99:620–628. doi:10.3324/haematol.2013.092684
10. Koprivnikar J, Kessler CM. Thrombocytosis: essential thrombo-cythemia and reactive causes. Fourth Edi. Consult hemost thromb.Third. 2013. Philadelphia, PA: Elsevier.doi:10.1016/B978-1-4557-2296-9.00019-1
11. Soyer N, Haznedaroğlu İC, Cömert M, Çekdemir D, Yılmaz M,Ünal A, Çağlıyan G, Bilgir O, İlhan O, Özdemirkıran F, et al.Multicenter retrospective analysis of turkish patients with chronicmyeloproliferative neoplasms. Turk J Hematol 2017;34:27–33.doi:10.4274/tjh
12. Connor DE, Ma DDF, Joseph JE. Flow cytometry demonstratesdifferences in platelet reactivity and microparticle formation insubjects with thrombocytopenia or thrombocytosis due to primaryhaematological disorders. Thromb Res 2013;132:572–577.doi:10.1016/j.thromres.2013.09.009
13. Arber DA, Orazi A, Hasserjian R, Borowitz MJ, Le Beau MM,Bloomfield CD, Cazzola M, Vardiman JW. The 2016 revision to theWorld Health Organization classification of myeloid neoplasms andacute leukemia. Blood 2016;127:2391–2406. doi:10.1182/blood-2016-03-643544
14. Suntsova EV, Demina IM, Ignatova AA, Ershov NM, Trubina NM,Dobrynina J, Serkova IV, Supik ZS, Orekhova EV, Hachatryan LA,et al. Bleeding tendency and platelet function during treatment withromiplostim in children with severe immune thrombocytopenicpurpura. Int J Hematol 2017;105:841–848. doi:10.1007/s12185-017-2207-3
15. Ignatova AA, Karpova OV, Trakhtman PE, Rumiantsev SA,Panteleev MA. Functional characteristics and clinical effectivenessof platelet concentrates treated with riboflavin and ultraviolet lightin plasma and in platelet additive solution. Vox Sang2016;110:244–252. doi:10.1111/vox.2016.110.issue-3
16. Ignatova AA, Ponomarenko EA, Polokhov DM, Suntsova EV,Zharkov PA, Fedorova DV, Balashova EN, Rudneva AE, PtushkinVV, Nikitin EA, et al. Flow Cytometry for Pediatric Platelets.Platelets 2018;00:1–10.
17. Cattaneo M, Cerletti C, Harrison P, Hayward CPM, Kenny D,Nugent D, Nurden P, Rao AK, Schmaier AH, Watson SP, et al.Recommendations for the standardization of light transmissionaggregometry: A consensus of the working party from the plateletphysiology subcommittee of SSC/ISTH. J Thromb Haemost2013;11:1183–1189. doi:10.1111/jth.2013.11.issue-6
18. Koltsova EM, Balashova EN, Ignatova AA, Poletaev AV, PolokhovDM, Kuprash AD, Ionov OV, Kirtbaya AR, Lenyushkina AA,Timofeeva LA, et al. Impaired platelet activity and hypercoagulationin healthy term and moderately preterm newborns during the earlyneonatal period. Pediatr Res 2018. doi:10.1038/s41390-018-0184-8
19. Hézard N, Potron G, Schlegel N, Amory C, Leroux B, Nguyen P.Platelets and Blood Cells Unexpected persistence of platelet hypor-eactivity beyond the neonatal period : a flow cytometric study inneonates, infants and older children. Thromb Haemost2003;90:116–123.
20. Yip C, Linden MD, Attard C, Monagle P, Ignjatovic V. Plateletsfrom children are hyper-responsive to activation by thrombin recep-tor activator peptide and adenosine diphosphate compared to plate-lets from adults. Br J Haematol 2003:168(4):526–532.
10 D. M. Polokhov et al. Platelets, Early Online: 1–11

21. Falanga A, Marchetti M, Vignoli A, Balducci D, Russo L,Guerini V, Barbui T. V617F JAK-2 mutation in patients with essen-tial thrombocythemia: relation to platelet, granulocyte, and plasmahemostatic and inflammatory molecules. Exp Hematol2007;35:702–711. doi:10.1016/j.exphem.2007.01.053
22. Karakantza M, Giannakoulas NC, Zikos P, Sakellaropoulos G,Kouraklis A, Aktypi A, Metallinos IC, Theodori E,Zoumbos NC, Maniatis A. Markers of endothelial and in vivoplatelet activation in patients with essential thrombocythemia andpolycythemia vera. Int J Hematol 2004;79:253–259. doi:10.1532/IJH97.E0316
23. Carobbio A, Antonioli E, Guglielmelli P, Vannucchi AM, Delaini F,Guerini V, Finazzi G, Rambaldi A, Barbui T. Leukocytosis and riskstratification assessment in essential thrombocythemia. J Clin Oncol2008;26:2732–2736. doi:10.1200/JCO.2007.15.3569
24. Lim Y, Lee JO, Kim SH, Kim JW, Kim YJ, Lee KW, Lee JS,Bang SM. Prediction of thrombotic and hemorrhagic events duringpolycythemia vera or essential thrombocythemia based on leukocyteburden. Thromb Res 2015;135:846–851. doi:10.1016/j.thromres.2015.02.023
25. Schneider C, Stutz-Grunder E, Lüer S, Keller P, Kremer Hovinga J,Ammann R, Karow A. Fulminant essential thrombocythemia asso-ciated with acquired von willebrand syndrome and bleeding epi-sodes in a 14-year-old Girl. Hamostaseologie 2019. doi:10.1055/s-0039-1679929
26. Mohri H. Acquired von Willebrand syndrome: its pathophysiology,laboratory features and management. J Thromb Thrombolysis2003;15:141–149. doi:10.1023/B:THRO.0000011369.70824.e6
27. Mital A, Prejzner W, Bieniaszewska M, Hellmann A. Prevalence ofacquired von Willebrand syndrome during essential thrombocythe-mia: A retrospective analysis of 170 consecutive patients. Pol ArchMed Wewn 2015;125:914–920. doi:10.20452/pamw.3211
28. Budde U, Scharf RE, Franke P, Hartmann-Budde K, Dent J,Ruggeri ZM. Elevated platelet count as a cause of abnormal vonWillebrand factor multimer distribution in plasma. Blood1993;82:1749–1757. doi:10.1182/blood.V82.6.1749.1749
29. Shim K, Anderson PJ, Tuley EA, Wiswall E, Sadler JE. Platelet-VWF complexes are preferred substrates of ADAMTS13 underfluid shear stress. Blood 2008;111:651–657. doi:10.1182/blood-2007-05-093021
DOI: https://doi.org/10.1080/09537104.2019.1704710 Hemostasis in childhood essential thrombocythemia 11