pitfalls in avoiding operation for autoimmune pancreatitis
TRANSCRIPT

Accepte
ReprintSan AntFt Sam
0039-60
Publishe
doi:10.1
968 S
Pitfalls in avoiding operation forautoimmune pancreatitisPeter A. Learn, MD,a Evan B. Grossman, MD,b Richard K. G. Do, MD, PhD,c Peter J. Allen, MD,d
Murray F. Brennan, MD,d Michael I. D’Angelica, MD,d Ronald P. DeMatteo, MD,d Yuman Fong, MD,d
David S. Klimstra, MD,e Mark A. Schattner, MD,f and William R. Jarnagin, MD,d Ft Sam Houston, TX,and Brooklyn and New York, NY
Background. Despite improved clinical characterization, autoimmune pancreatitis is often stilldiagnosed only after a major operative procedure. This study seeks to elucidate the circumstances thatcontribute to an inaccurate preoperative diagnosis.Methods. Two independent reviewers identified retrospectively an institutional cohort of 68 patients withadequate clinical data to support the diagnosis of autoimmune pancreatitis. Further data regardingpresentation, diagnostic studies, and clinical course was abstracted from medical records. Comparativeanalyses were performed between those patients who underwent major operative procedures and those whodid not.Results. Fifty-three patients underwent operative intervention as their initial treatment. Compared to the15 patients avoiding operation, these patients were less likely to have diffuse pancreatic enlargementidentified on pretreatment imaging (8% vs 80%) or to have pretreatment serum IgG4 level evaluations(11% vs 100%). Among the 21 patients in whom IgG4 levels were first checked postoperatively, only 12had increases of at least twice the upper limit of normal. Pretreatment fine needle aspirates wereinterpreted incorrectly as definite or suspicious for adenocarcinoma in 12 patients, of whom 10underwent operation. Clinically important postoperative disease recurrence was suspected or proven in13 patients.Conclusion. Pitfalls leading to major pancreatic resections in autoimmune pancreatitis includeunnecessarily high thresholds for initiating serum IgG4 evaluation, false positive cytologic evaluationsfor malignancy, and failure to recognize non-classic initial presentations, or recurrence of disease. Betterdiagnostic strategies are needed, but awareness of these specific findings should help to decrease thenumber of patients undergoing operation for unrecognized autoimmune pancreatitis. (Surgery2011;150:968-74.)
From the Department of Surgery,a San Antonio Military Medical Center, Ft Sam Houston, TX; Department ofMedicine,b SUNY Downstate Medical Center, Brooklyn, NY; Department of Radiology,c Department of Surgery,d
Department of Pathology,e and Department of Medicine,f Memorial Sloan-Kettering Cancer Center, New York, NY
SINCE AUTOIMMUNE PANCREATITIS (AIP) was first pro-posed as a clinical entity in 1995,1 investigatorshave improved the clinical characterization of thedisease, including serologic and radiologic find-ings, extrapancreatic manifestations, and responseto therapy.2-4 Despite these efforts, this rare clinicalentity all too frequently eludes preoperative diag-nosis, resulting in a major operative procedurefor a disease process that generally responds wellto medical therapy.5-7
d for publication June 15, 2011.
requests: Peter A. Learn, MD, Department of Surgery,onio Military Medical Center, 3851 Roger Brooke Dr,Houston, TX 78234. E-mail: [email protected].
60/$ - see front matter
d by Mosby, Inc.
016/j.surg.2011.06.015
URGERY
In 2003, we reported our institutional experi-ence with operative resection of lymphoplasma-cytic sclerosing pancreatitis (LPSP), the histologicrepresentation of AIP.8 That publication precededthe emergence of data regarding the utility of se-rum IgG4 and better clinical and radiographiccharacterization of AIP. Since that time, we haveidentified patients with AIP based on clinical find-ings, precluding a potential major operation andits attendant risks. Nevertheless, misdiagnosis stilloccurs in many patients, leading to unnecessaryoperations. Although greater awareness has nodoubt decreased the number of these cases, theclinical and radiographic features that distinguishAIP from pancreatic adenocarcinoma can be sub-tle and difficult to appreciate, even for experi-enced clinicians.
This study presents an update of our institutionalexperience with AIP, in particular focusing on how

SurgeryVolume 150, Number 5
Learn et al 969
some patients still proceed to operative explorationbecause of an inaccurate preoperative diagnosis.
METHODS
Data collection. This investigation was designedas a retrospective cohort study with approval fromthe MSKCC Institutional Review Board. Patientswere identified using 3 primary data sources: (1) asearch of the surgical pathology database for anyreports with any mention of lymphoplasmacyticinflammation (not confined to pancreatic speci-mens) or other findings suggestive of lymphoplas-macytic sclerosing pancreatitis; (2) a search of thelaboratory results database for IgG4 test results; and(3) inclusion of previously identified and reportedcases.8 Searches included results from 1985 throughJune 2009. The medical records of patients identi-fied from these searches were then reviewed to ex-clude patients without any evidence of pancreaticinvolvement. One hundred sixty-eight potentialcases were identified. Of these, 40 were outside pa-thology consultations for which clinical data was un-available and therefore were excluded.
Two investigators (P.A.L. and E.B.G.) reviewedindependently the records of the remaining 128patients to determine whether adequate historicdata supported the diagnosis of autoimmune pan-creatitis. For most patients, the diagnosis wasconfirmed pathologically. For those without a clearpathologic diagnosis, we aggregated informationfrom radiologic and serologic tests, response tomedical therapy, and non-hepatopancreatobiliarytract involvement, consistent with the criteria out-lined by Chari et al,4 to identify clinical cases of au-toimmune pancreatitis. This approach resulted ina cohort of 68 patients for whom further datawere collected.
Data were abstracted on patient demographics,presenting symptoms, radiologic, serologic, andendoscopic investigations, and therapeutic inter-ventions for the study cohort. A synopsis of radi-ologic and endoscopic reports based on key termsas delineated in the Results section was created.While the original radiologic reports offered someinsight into how imaging could have influenceddecision-making, we also pursued a formal reviewof available cross-sectional studies by a hepatopan-creatobiliary imaging specialist (R.K.G.D.) who wasblinded to the original read. This intent of thereview was to evaluate the accuracy of findings onthe prior report and to assess further for what arenow known to be important radiologic findings inAIP.9-11 Operative complications were recordedprospectively according to a previously describedand routinely used grading system.12
Statistical analysis. For tests of statistical signif-icance, we used the Mann-Whitney test for contin-uous variables and Fisher’s exact test fordichotomous variables as appropriate. We consid-ered 2-sided P values < .05 as the threshold of sig-nificance. We used Stata v8.0 SE (StataCorp LP,College Station, TX) for all analyses.
RESULTS
Demographics and clinical presentation for the68 patients are reported in Table I. Median follow-up for the entire cohort was 30 months. Medianfollow-up for patients diagnosed without histologicexamination (n = 13) was 10 months (range 6–129months). The majority of patients presented withjaundice, although 13 presented only with laboratoryor radiologic abnormalities in the absence of clearsymptoms. Operative intervention was performedon 53 patients (78%). Twenty-nine patients were re-ported in our previous experience prior to 2003, ofwhom 28 underwent operation. Of the 39 patientstreated since that report, 14 (36%) were diagnosedwith AIP prior to treatment and avoided operation.
Among patients undergoing operation prior todiagnosis with AIP/LPSP, a major resection (prox-imal, distal, or total pancreatectomy) was per-formed in 41, while 12 underwent a pancreaticbiopsy with or without a bypass procedure(Table II). In all cases, operation was undertakenfor a presumptive diagnosis of pancreatic cancerwith ‘‘curative intent,’’ although in many, the sur-geon recognized the possibility of LPSP as a diagno-sis intraoperatively. Postoperative clinical recurrenceof the disease process was suggested in 11, of whomfour received steroid therapy. Eight patients experi-enced a postoperative complication grade 3 orgreater (i.e., requiring invasive intervention or re-sulting in permanent organ injury or death), with1 patient dying from postoperative complicationsof pancreaticoduodenectomy.
We compared the results of the pretreatmentevaluation of patients who underwent operativeintervention prior to the diagnosis of AIP andthose who avoided operation (Table III). Multi-phase, contrast enhanced, high resolution mag-netic resonance imaging or computed tomography(CT) pancreas-directed imaging was performed innearly all patients presenting after 1998, and themajority were either obtained internally or were re-viewed preoperatively by a MSKCC radiologist. Areport of diffuse pancreatic enlargement by the ra-diologist was highly associated with avoidance ofoperation (P < .001), but this ‘‘classic’’ findingwas reported in only 15 patients in this series(22%). An identifiable mass or ‘‘suggestion’’ of a

Table I. Patient demographics and clinicalpresentation
Full cohort N = 68
Mean age at presentation (SD) 63 (14)Median follow-up duration in
months (IQR)30 (9–81)
Previously reported* 29 (43)Male gender* 45 (66)Racey
White, non-Hisp 53 (79)Asian 8 (12)White, Hisp 2 (3)Black, non-Hisp 2 (3)Other 2 (3)
Symptoms at presentationJaundice* 41 (60)Pain* 33 (49)Weight loss* 32 (45)Evaluation for abnormal lab* 8 (11)Incidental radiologic finding* 5 (7)
Comorbidities at presentationDiabetes* 22 (32)Non-hepatobiliary immune-
mediated disorder*5 (7)
Collagen vascular disorder 3Inflammatory bowel disease 2Grave’s disease 1Bell’s palsy 1
Non-hepatobiliary organ involvement* 7 (10)Sialadenitis 5Interstitial nephritis 1Epididymitis 1
Involvement of biliary tract* 7 (10)Initial therapeutic intervention
Operation* 53 (78)Medical (i.e., steroids)* 14 (21)Neither* 1 (7)
*Values are n (%).yTotal number of patients is less than total number of disorders because2 patients presented with multiple immune-mediated disorders.
SurgeryNovember 2011
970 Learn et al
mass was described in 30 (44%), while 62 (91%)were reported to have either common bile ductor pancreatic duct dilatation of varying degrees.
Of the 68 patients in the study, 37 had digitizedstudies available for review on our picture archiv-ing and communication system. For the remainingpatients, the original studies were no longerretained in archived records or the copies availablewere of inadequate quality for complete assess-ment (i.e., digitized copies of film). The specificradiologic findings assessed on review are summa-rized in Table IV. Among 21 patients in this subsetwho were originally reported to have a mass, sug-gestion of a mass, or mass-like enlargement, onlyone was found to have a hypodense mass on review.
Eight were found to have focal pancreatic enlarge-ment. Eleven of the remaining 12 had evidence ofbile duct enlargement without a discrete mass. Therecognition of pancreatic duct dilation (PDD, de-fined as duct diameter 4 mm and greater) washighly conserved: readings were concordant in 36(7 with PDD), while in 1 patient, the reviewer dis-agreed with the initial assessment that PDD waspresent. A greater rate of discordance was seen inthe assessment of diffuse pancreatic enlargement(DPE). Initial and review readings agreed on thepresence of DPE in 11 and absence in 19. Discor-dant results on the review reading were the ab-sence of DPE in 3 and the presence of DPE in 4.
Serum IgG4 levels were assessed in 42 patients,half of which were drawn prior to any treatment.Patients undergoing operation as initial treatmentwere much less likely to have had serum IgG4 levelsdrawn preoperatively. Among the 21 patients whoseserum IgG4 was first checked postoperatively, levelswere increased in 14, with 12 having values at least 2times the upper limit of normal (Figure). No pa-tient underwent operation with a preoperativelyknown IgG4 level that was increased.
With respect to preoperative endoscopic exam-inations, rates of endoscopic retrograde cholangi-opancreatography (ERCP) and stent placementwere not remarkably different between groups. Agreater percentage of patients avoiding operationunderwent endoscopic ultrasonography (EUS)(87% vs 30%, Table III). This finding reflects par-tially the introduction of EUS into the preopera-tive evaluation coinciding temporally with abetter recognition of the clinical entity of AIP.When evaluating only those patients who werenot reported previously, a time period in whichEUS was consistently available, EUS was stillperformed in only 14 of 27. Among all 29 patientssubmitted to EUS, a mass was identified sono-graphically in a greater fraction of patients who un-derwent operation (14 of 16) than those who didnot (7 of 13), (P = .09).
Pretreatment biopsy results appeared linked totreatment decisions. Thirty-seven patients under-went a biopsy prior to treatment (Table III). Of the23 patients undergoing operation after a preoper-ative biopsy, the biopsy specimens in 10 were inter-preted as either adenocarcinoma (2) or suspiciousfor adenocarcinoma (8). In contrast, among the 14patients who had a pretreatment biopsy withoutundergoing operation, only 2 were read as suspi-cious for adenocarcinoma. Of particular note,both patients submitted to core biopsies had patho-logic confirmation of LPSP or lymphoplasmacyticcells. No patients in this series were diagnosed

Table II. Outcomes of surgical treatment
Surgery N = 53
Type of initial operationMajor resection 41 (77%)Pancreatoduodenectomy 33Distal pancreatectomy 6Total pancreatectomy 2
Non-resection 12 (23%)Operative exploration/biopsy only 7Biopsy with biliary or enteric bypass* 5
Symptom recurrence 11 (21%)After major resection 10After biliary bypass 1
Steroid treatment after surgery 9Complications 18 (34%)
Grade 1 3Grade 2 7Grade 3 6Grade 4 1Grade 5 1
Patients undergoing major resection afterdiagnosis of AIP
2
FNA biopsy interpreted as carcinoma 1Other radiologic finding promptingoperation (cystic lesion)
1
*Performed in conjunction with biopsy.
SurgeryVolume 150, Number 5
Learn et al 971
with adenocarcinoma after resection or close clini-cal follow-up. The false positive rate of all pretreat-ment biopsies in patients with AIP, combiningspecimens interpreted either as definite (2) or sus-picious (10) for adenocarcinoma, was 32% (95%CI, 17–48%). Among the 27 patients with percuta-neous or endoscopic fine needle aspirate (FNA) cy-tology specimens, the false positive rate was 41%(95% CI, 22–61%); the 2 specimens interpreted asdefinite for adenocarcinoma were FNA samples.
Among patients submitted to operation, diseaserecurrence in the remnant pancreas or the hep-atobiliary tract was suggested clinically in 11 andconfirmed pathologically in 2. Evidence suspiciousfor recurrence was observed at a median follow-upof 113 months (interquartile range [IQR] 4–26months). Such recurrences resulted commonly inbiliary drainage procedures (2 by percutaneoustranshepatic cholangiography, 3 by ERCP). Onepatient with images that were concerning forintrahepatic cholangiocarcinoma underwent ma-jor hepatectomy for what was found to be lympho-plasmacytic sclerosing cholangitis on histologicexamination.
DISCUSSION
The results of this study point to several diag-nostic traps that may complicate the accurate
identification of AIP prior to operative interven-tion. The first apparent pitfall is inadequate aware-ness of the spectrum of clinical presentation,particularly as it pertains to radiologic findings.Without this understanding, the diagnosis willcontinue to be made in the wake of a majoroperation as occurred in our early experience.Only a minority of patients with AIP in our seriesdemonstrated the classic criteria of radiologicdiffuse enlargement and increased serum IgG4,even after radiologic review. The discordant assess-ments on diffuse pancreatic enlargement in 7 of 37reviewed images points to the subjective nature ofthis particular finding. Our review confirmed thatit is critically important for the radiologist to befamiliar with the extrapancreatic manifestations ofAIP, because these manifestations were notablyprevalent in our population, a point that hasbeen made clearly by other investigators.9,11 Wealso observed a surprising number of patientswith an objectively measurable degree of pancre-atic duct dilation, which is not described broadlyin this condition10 and could easily increase theconcern for malignancy when managing these pa-tients. Insensitivity to the full spectrum of presenta-tions of AIP contributed likely to the decision tooperate, often without obtaining additional diag-nostic studies.
The second pitfall would be an excessively highthreshold for checking serum IgG4 levels. In prac-tice, the test is often sent only when radiologiccriteria are highly suggestive. If one assumes thatserum IgG4 measured in the acute postoperativeperiod correlates well with preoperative levels,then our results suggest that the threshold usedin this series is too high and fails to identify asubstantial number of patients. Recognizing thatfalse positive increases occur in pancreatic cancer,3
we would not endorse a policy of universally apply-ing the test as a screening mechanism. Consider-ing the test in any patient without a clear cancerdiagnosis and with equivocal radiologic findingsmay improve the pretest probability enough toavoid false positive results but requires more ro-bust evaluation.
The third important pitfall is the frequency withwhich FNA specimens have been interpreted assuspicious or even positive for adenocarcinoma. Inthis situation, it is not difficult to understand why asurgeon would recommend going forward withresection, even if radiographic evidence mightsuggest the possibility of AIP. Cytologic suspicionfor carcinoma on FNA should not necessarily over-ride solid, alternative clinical and/or radiographicevidence pointing toward AIP (i.e., suggestive
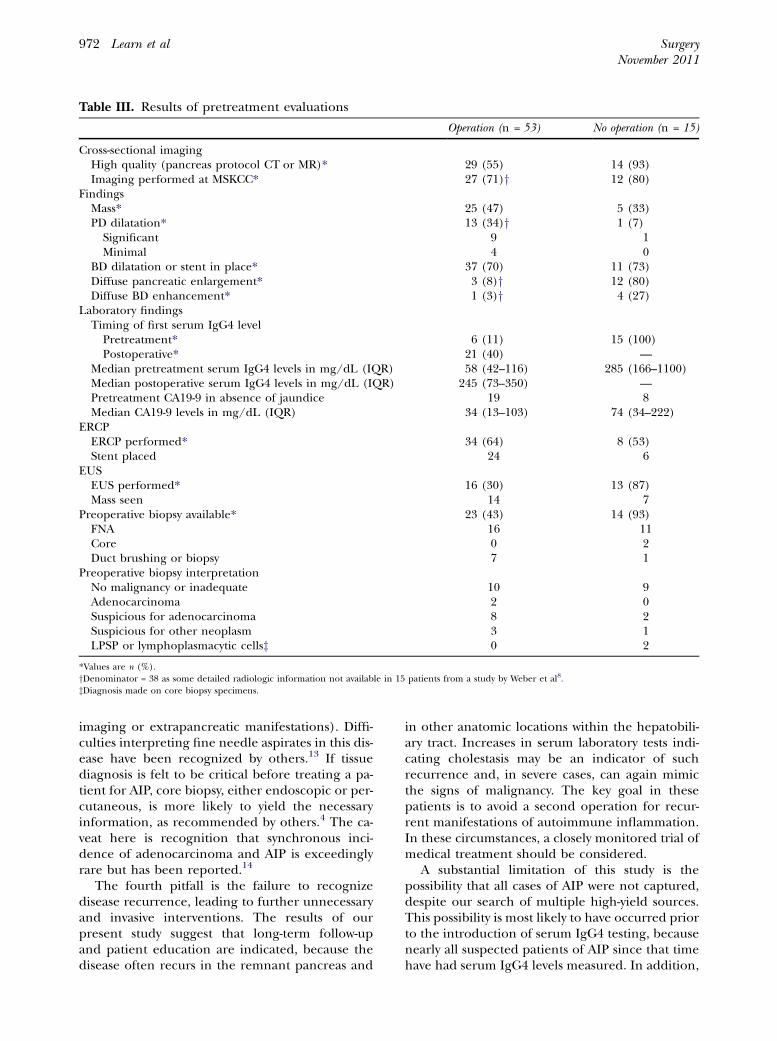
Table III. Results of pretreatment evaluations
Operation (n = 53) No operation (n = 15)
Cross-sectional imagingHigh quality (pancreas protocol CT or MR)* 29 (55) 14 (93)Imaging performed at MSKCC* 27 (71)y 12 (80)
FindingsMass* 25 (47) 5 (33)PD dilatation* 13 (34)y 1 (7)
Significant 9 1Minimal 4 0
BD dilatation or stent in place* 37 (70) 11 (73)Diffuse pancreatic enlargement* 3 (8)y 12 (80)Diffuse BD enhancement* 1 (3)y 4 (27)
Laboratory findingsTiming of first serum IgG4 levelPretreatment* 6 (11) 15 (100)Postoperative* 21 (40) —
Median pretreatment serum IgG4 levels in mg/dL (IQR) 58 (42–116) 285 (166–1100)Median postoperative serum IgG4 levels in mg/dL (IQR) 245 (73–350) —Pretreatment CA19-9 in absence of jaundice 19 8Median CA19-9 levels in mg/dL (IQR) 34 (13–103) 74 (34–222)
ERCPERCP performed* 34 (64) 8 (53)Stent placed 24 6
EUSEUS performed* 16 (30) 13 (87)Mass seen 14 7
Preoperative biopsy available* 23 (43) 14 (93)FNA 16 11Core 0 2Duct brushing or biopsy 7 1
Preoperative biopsy interpretationNo malignancy or inadequate 10 9Adenocarcinoma 2 0Suspicious for adenocarcinoma 8 2Suspicious for other neoplasm 3 1LPSP or lymphoplasmacytic cellsz 0 2
*Values are n (%).yDenominator = 38 as some detailed radiologic information not available in 15 patients from a study by Weber et al8.zDiagnosis made on core biopsy specimens.
SurgeryNovember 2011
972 Learn et al
imaging or extrapancreatic manifestations). Diffi-culties interpreting fine needle aspirates in this dis-ease have been recognized by others.13 If tissuediagnosis is felt to be critical before treating a pa-tient for AIP, core biopsy, either endoscopic or per-cutaneous, is more likely to yield the necessaryinformation, as recommended by others.4 The ca-veat here is recognition that synchronous inci-dence of adenocarcinoma and AIP is exceedinglyrare but has been reported.14
The fourth pitfall is the failure to recognizedisease recurrence, leading to further unnecessaryand invasive interventions. The results of ourpresent study suggest that long-term follow-upand patient education are indicated, because thedisease often recurs in the remnant pancreas and
in other anatomic locations within the hepatobili-ary tract. Increases in serum laboratory tests indi-cating cholestasis may be an indicator of suchrecurrence and, in severe cases, can again mimicthe signs of malignancy. The key goal in thesepatients is to avoid a second operation for recur-rent manifestations of autoimmune inflammation.In these circumstances, a closely monitored trial ofmedical treatment should be considered.
A substantial limitation of this study is thepossibility that all cases of AIP were not captured,despite our search of multiple high-yield sources.This possibility is most likely to have occurred priorto the introduction of serum IgG4 testing, becausenearly all suspected patients of AIP since that timehave had serum IgG4 levels measured. In addition,

Table IV. Results of review of available radiologic studies for 37 patients
Imaging finding Operation (n = 24) No operation (n = 13)
Hypodense mass 1 (4) 1 (8)Focal enlargement 8 (33) 3 (23)Diffuse enlargement 5 (21) 10 (77)Rim sign 4 (17) 9 (69)Pancreatic duct narrowing 7 (29) 5 (38)Pancreatic duct dilation 7 (29) 0Median diameter in mm (range) 5 (4–10)Intra- or extrahepatic biliary duct involvement 9 (38) 7 (54)Renal involvement 1 (4) 4 (31)Retroperitoneal fibrosis 0 1 (8)Retroperitoneal lymphadenopathy 0 0
Values are n (%) unless otherwise specified.
050
010
0015
0020
00
Seru
m Ig
G4
Leve
l (m
g/dL
)
Pretreat, No Surgery Pretreat, Surgery Postsurgical Only
Timing of Serum IgG4 Testing
Figure. Comparison of the first recorded serum IgG4levels in each patient. Groups are defined according tothe timing of evaluation and treatment: prior to anytreatment in patients not undergoing operation (Pre-treat, No Surgery), prior to operation (Pretreat, Surgery),or after operation (Postsurgical Only). Dashed line repre-sents upper limit of normal (121 mg/dL).
SurgeryVolume 150, Number 5
Learn et al 973
the spectrum of disease seen at MSKCC, a NationalCancer Institute-designated comprehensive cancercenter, skews the patient population toward malig-nant diseases. Indeed, the substantial number ofpatients who demonstrated focal masses, pancre-atic duct dilation, and/or biliary obstruction, sug-gests referral patterns biased toward those with themost worrisome-appearing cross-sectional imaging.We recognize that data regarding extra-pancreaticmanifestations and recurrence are unavoidablyincomplete in this retrospective study. There mightalso be concern that a median follow-up time ofslightly greater than 10 months in the clinicallydiagnosed patients is an inadequate amount oftime to determine diagnostic error, although witha minimum follow-up of 5.6 months, we wouldexpect all but the most subtle cases of cancermisdiagnosed as AIP to have become apparent.
In light of continued difficulty distinguishingsome forms of AIP from pancreatic adenocarci-noma, what recommendations for improvementcan be made? Chari et al4 have provided a thought-ful diagnostic strategy that would have capturedmany but certainly not all patients in this cohort.While serum IgG4 testing has improved the abilityto rule in the diagnosis, it is not specific enough toexclude a cancer diagnosis. Furthermore, increas-ing clinicopathologic evidence supports distin-guishing between 2 subtypes of AIP: classic AIPand AIP with granulocytic epithelial lesions. Inthe latter entity, IgG4 is not increased typically, fur-ther placing limits on the utility of this test.15,16
When balancing the risks of a major pancreaticresection for benign disease against the risks ofallowing malignant disease to progress untreated,we favor avoiding the latter. If the surgeon wishesto explore a trial of steroid treatment, we agreewith other authors17,18 that response must be as-sessed with very close interval (2–4 week) radio-logic follow-up after initiation of therapy, whichmay include a repeat EUS and biopsy. Continuedefforts to simplify the diagnostic strategy for AIPare likely to depend either on enriching the popu-lation in which the positive predictive value ofIgG4 testing can be maximized or on defining aneven more accurate test.19 In the meantime, aware-ness of the pitfalls we have outlined should con-tribute toward the goal of avoiding unwarrantedmorbidity and mortality.
REFERENCES
1. Yoshida K, Toki F, Takeuchi T, Watanabe S, Shiratori K,Hayashi N. Chronic pancreatitis caused by an autoim-mune abnormality. Proposal of the concept of autoim-mune pancreatitis. Dig Dis Sci 1995;40:1561-8.
2. Hamano H, Kawa S, Horiuchi A, Unno H, Furuya N, Aka-matsu T, et al. High serum IgG4 concentrations in patientswith sclerosing pancreatitis. N Engl J Med 2001;344:732-8.

SurgeryNovember 2011
974 Learn et al
3. Ghazale A, Chari ST, Smyrk TC, Levy MJ, Topazian MD,Takahashi N, et al. Value of serum IgG4 in the diagnosisof autoimmune pancreatitis and in distinguishing it frompancreatic cancer. Am J Gastroenterol 2007;102:1646-53.
4. Chari ST, Takahashi N, Levy MJ, Smyrk TC, Clain JE,Pearson RK, et al. A diagnostic strategy to distinguish au-toimmune pancreatitis from pancreatic cancer. Clin Gas-troenterol Hepatol 2009;7:1097-103.
5. Deshpande V, Mino-Kenudson M, Brugge W, Lauwers GY.Autoimmune pancreatitis: more than just a pancreatic dis-ease? A contemporary review of its pathology. Arch PatholLab Med 2005;129:1148-54.
6. Frulloni L, Scattolini C, Falconi M, Zamboni G, Capelli P,Manfredi R, et al. Autoimmune pancreatitis: differences be-tween the focal and diffuse forms in 87 patients. Am J Gas-troenterol 2009;104:2288-94.
7. de Castro SM, de Nes LC, Nio CY, Velseboer DC, ten KateFJ, Busch OR, et al. Incidence and characteristics of chronicand lymphoplasmacytic sclerosing pancreatitis in patientsscheduled to undergo a pancreatoduodenectomy. HPB(Oxford) 2010;12:15-21.
8. Weber SM, Cubukcu-Dimopulo O, Palesty JA, SuriawinataA, Klimstra D, Brennan MF, et al. Lymphoplasmacytic scle-rosing pancreatitis: inflammatory mimic of pancreatic carci-noma. J Gastrointest Surg 2003;7:129-37.
9. Bodily KD, Takahashi N, Fletcher JG, Fidler JL, Hough DM,Kawashima A, et al. Autoimmune pancreatitis: pancreaticand extrapancreatic imaging findings. AJR Am J Roent-genol 2009;192:431-7.
10. Nakazawa T, Ohara H, Sano H, Ando T, Imai H, Takada H,et al. Difficulty in diagnosing autoimmune pancreatitis byimaging findings. Gastrointest Endosc 2007;65:99-108.
11. Suzuki K, Itoh S, Nagasaka T, Ogawa H, Ota T, Naganawa S.CT findings in autoimmune pancreatitis: assessment using
multiphase contrast-enhanced multisection CT. Clin Radiol2010;65:735-43.
12. Grobmyer SR, Pieracci FM, Allen PJ, Brennan MF, JaquesDP. Defining morbidity after pancreaticoduodenectomy:use of a prospective complication grading system. J AmColl Surg 2007;204:356-64.
13. Deshpande V, Mino-Kenudson M, Brugge WR, Pitman MB,Fernandez-del Castillo C, Warshaw AL, et al. Endoscopic ul-trasound guided fine needle aspiration biopsy of autoim-mune pancreatitis: diagnostic criteria and pitfalls. Am JSurg Pathol 2005;29:1464-71.
14. Witkiewicz AK, Kennedy EP, Kennyon L, Yeo CJ, HrubanRH. Synchronous autoimmune pancreatitis and infiltratingpancreatic ductal adenocarcinoma: case report and reviewof the literature. Hum Pathol 2008;39:1548-51.
15. Dhall D, Suriawinata AA, Tang LH, Shia J, Klimstra DS. Useof immunohistochemistry for IgG4 in the distinction of au-toimmune pancreatitis from peritumoral pancreatitis. HumPathol 2010;41:643-52.
16. Sah RP, Chari ST, Pannala R, Sugumar A, Clain JE, Levy MJ,et al. Differences in clinical profile and relapse rate of type1 versus type 2 autoimmune pancreatitis. Gastroenterology2010;139:140-8.
17. Gardner TB, Levy MJ, Takahashi N, Smyrk TC, Chari ST.Misdiagnosis of autoimmune pancreatitis: a caution to clini-cians. Am J Gastroenterol 2009;104:1620-3.
18. Moon SH, Kim MH, Park DH, Hwang CY, Park SJ, Lee SS,et al. Is a 2-week steroid trial after initial negative investiga-tion for malignancy useful in differentiating autoimmunepancreatitis from pancreatic cancer? A prospective outcomestudy. Gut 2008;57:1704-12.
19. Frulloni L, Lunardi C, Simone R, Dolcino M, Scattolini C, Fal-coni M, et al. Identification of a novel antibody associated withautoimmune pancreatitis. N Engl J Med 2009;361:2135-42.