pilot pharmacy participant manual - cphm.ca iq/manual/training manual... · r e c t e et s u a v i...
TRANSCRIPT

Recte et Suavite
r
reporting learning improving
Safety
Pilot Pharmacy Participant ManualA Guide to Continuous Quality Improvement
Safety. Improvement. Quality.

2. College of Pharmacists of Manitoba - Safety IQ Training Manual
Table of ContentsDisclaimer 3
Introduction 4
Expectations: 5
Participants and the College 5
How to Use this Manual 6
Documents 7
Timeline for the Safety IQ Pilot 9
Frequently Asked Questions: 10
Safety IQ and CQI FAQ 10
Electronic Links: 12
CPhIR and MSSA 12
Appendix Practice Direction: Medication Incidents and Discrepancies or Near - Miss Events 13
The Apology Act 17
Canadian Disclosure Guidelines 18
Quarterly Meeting Agenda 20
Quarterly Meeting Report Forms 21
Quarterly Meeting Notes 22
Quarterly Meeting Action Plan 23
CQI Summarization 24
Annual MSSA Improvement Plan 26
Comprehensive Analysis (or Root Cause Analysis) Steps and Instructions 27
How to Create a Constellation Diagram 29
Constellation Diagram Example 34
Suggested Protocol for Handling Medication Incidents and Near-Misses 36

2. 3.College of Pharmacists of Manitoba - Safety IQ Training Manual
DisclaimerThe information contained in this guide was originally intended for use by Nova Scotia pharmacists as a reference for their continuous quality Improvement (CQI) program SafetyNET-Rx. It was also adapted for use by the Saskatchewan pharmacists for their CQI program COMPASS. The authors of the original document were as follows:
Authors:
Andrea Scobie, Dalhousie University
Neil MacKinnon, James L. Winkle College of Pharmacy, University of Cincinnati
Todd Boyle, St. Francis Xavier University
Bev Zwicker, Nova Scotia College of Pharmacists
Tom Mahaffey, St. Francis Xavier University
Funding for the original project was supplied by the Canadian Foundation for Pharmacy Innovation Fund.
The information in this reference manual has been adapted for the use by pharmacists participating in the Safety IQ (Safety Improvement in Quality) Pilot. The Safety IQ Pilot is a joint effort between the College of Pharmacists of Manitoba and ISMP Canada.

4. College of Pharmacists of Manitoba - Safety IQ Training Manual
IntroductionWelcome to the Safety IQ Pilot.
The College of Pharmacists of Manitoba (the College) would like to thank you for your commitment to advancing patient safety in Manitoba and congratulates you on being a part of this exciting new endeavour. By participating in Safety IQ, you are showing you value the importance of a safe medication system and are willing to take steps toward a culture of safety in Manitoba. Your willingness to volunteer your time and be open to working with the College and the Institute of Safe Medication Practices Canada (ISMP Canada) is remarkable.
The Safety IQ Pilot aims to evaluate the implementation of a continuous quality improvement (CQI) program in Manitoba community pharmacies. Medication safety and safe medication practices are important issues throughout the healthcare spectrum. The College recognizes the importance of ensuring community pharmacies not only recognize, resolve and learn from medication errors, but also review all their system processes to ensure patient safety.
The partners in the Safety IQ Pilot are the College and ISMP Canada, with SafetyNET-Rx (Nova Scotia CQI program) conducting some research for the project. COMPASS (Saskatchewan CQI program) will also serve as a valuable resource.
Promising research has been done in Nova Scotia through the SafetyNET-Rx program that shows which components need to be included in an effective community pharmacy CQI program. The SafetyNET-Rx project identified that a CQI program needs to be both proactive and reactive to be effective. Safety IQ will be modeled after the SafetyNET-Rx and COMPASS CQI projects, and will use the same tools and processes.
ISMP Canada will provide three online tools that will be used by volunteer pharmacies during the Pilot:
• Community Pharmacy Incident Reporting (CPhIR)
• Medication Safety Self-Assessment (MSSA)
• Quality Improvement tool
SafetyNET-Rx will conduct research and collect valuable information regarding the attitudes, barriers, supports, etc. of pharmacies reporting and participating in a CQI program.
The College is very excited to partner with ISMP Canada and SafetyNET-Rx and would like to thank them for their involvement in this very important project.
Thank you for your participation!

4. 5.College of Pharmacists of Manitoba - Safety IQ Training Manual
Throughout the Pilot, ISMP Canada will be providing monthly follow-ups with each Pilot site to ensure pharmacy staff are comfortable with the program tools and to identify any technical issues. ISMP Canada, via CPhIR, will collect the data on medication incidents from Pilot pharmacies and will provide the College with updates in an aggregate format. Medication incidents reported by Pilot pharmacies to ISMP Canada will be anonymous. The College will not receive any information regarding medication incidents reported in a format that will allow the College to identify any particular pharmacy.
SafetyNET-Rx will contact Pilot pharmacies periodically to collect research information for Safety IQ. SafetyNET-Rx will also ask Pilot pharmacies to participate in surveys at various times during the Pilot regarding barriers, supports, etc. to determine what enables or what prevents pharmacy staff from reporting medication incidents and near-misses, or from participating in a standardized CQI program.
Each Pilot pharmacy is expected to participate to the best of their ability in all elements of the Pilot and to use all the online tools provided to the Pilot sites, including:
• Completing the MSSA;
• Recording all medication incidents and near-misses; and
• Holding quarterly meetings to discuss medication incidents and developing an improvement plan.
In return for your commitment and dedication to the Safety IQ Pilot, your team will receive:
• Complimentary 1-year subscription to ISMP’s CPhIR and MSSA tools;
• Complimentary training on all of the tools;
• Support from the College throughout the project via monthly follow-up phone calls and/or visits to ensure your team is comfortable with all of the resources provided;
• A quarterly newsletter dedicated to Safety IQ updates and resources
• Website elements dedicated to Safety IQ including resources to mitigate medication incidents and near-misses; and
• Public resources to proudly display your pharmacy’s participation as a Safety IQ Champion.
Expectations:Participants and the College

6. College of Pharmacists of Manitoba - Safety IQ Training Manual
Medication incident or near miss occurs.
Staff dispenses medication according to current legislation
and standards of practice.
Known medication incident that reaches the patient is managed with
best practices and in accordance with current standards of practice.
Medication incident or near miss is anonymously reported to ISMP Canada
using the Community Pharmacy Incident Reporting (CPhIR) Tool.
Pharmacy team identifies areas for improvement and develops a
plan to achieve their goals.
Pharmacy staff trained on Safety IQ, CPhIR tools, and MSSA.
Pharmacy staff complete MSSA.
CQI leader chairs quarterly meeting to review:1. Summary of CPhIR reports based on reported
incidents and near misses.2. Any other relevant ISMP Canada reports.
3. Progress with improvement plans.
How to Use this ManualWe recommend that you thoroughly familiarize yourself with the contents of this training manual. The documents included in this guide have been selected to help you better understand and develop CQI processes. Once you have read through the guide, we encourage you to sit down with staff members to review the documents and to discuss how to best implement the processes in your pharmacy.
The CQI cycle for community pharmacists (Figure 1) provides a visual description of the CQI process. Its purpose is to help you better understand when and how to use the forms included in this guide.
Figure 1: The CQI Cycle for Community Pharmacies.
6. 7.College of Pharmacists of Manitoba - Safety IQ Training Manual
DocumentsThe documents highlighted and included in this manual for your reference and use.
Safety IQ and CQI FAQ These have been provided as a quick reference on a number of topics related to the Safety IQ Pilot (pages 10 and 11 of this guide).
The College’s Medication Incidents and Near-Misses Practice DirectionThis Practice Direction outlines the current provincial legislation surrounding medications incidents and near-misses, and should be referred to for guidance. Section 3.2 and 3.3 discuss the responsibility of a pharmacist upon discovery of a medication incident. All members are expected to follow this practice direction, in addition to the steps required as a Safety IQ participant. A copy of this Practice Direction can also be found on pages 13-16 of this guide.
The Apology Act The Apology Act allows members of a health care team, including pharmacists, to apologize to patients who have been impacted by medical incidents that may or may not have resulted in harm. An apology can be made without fear of liability as it is not admissible in court, and is not an admission of fault. This gives pharmacists the ability to exercise empathy with their patients in times of distress. A copy of The Apology Act can be found on page 17 of this guide.
Canadian Disclosure Guidelines Compiled by the Canadian Patient Safety Institute (CPSI), the Canadian Disclosure Guidelines: Being Open with Patients and Families, provides guidance on how best to disclose medication incidents to patients. This document is meant as a guideline only, and pharmacies are encouraged to discuss the procedures in place in their pharmacy for disclosure to patients. An excerpt from this document can be found on pages 18 and 19 of this guide.
Community Pharmacy Incident Reporting (CPhIR) Program Instruction Guide and FAQ’s This resource will answer any questions you may have about the reporting process on the CPhIR tool, and a printable version is available online.
To access the online version, log in to CPhIR at www.cphir.ca using your pharmacy’s unique user name and password. Under “CE & Resources,” you will find the “CPhIR Training Guide” and FAQ’s.
CPhIR Report Form A full length CPhIR form showing all the components of the report has been included for your reference in the Safety IQ folder. As the Pilot moves forward, you and your team will become very familiar with all of its components.
To access the online version, log in to CPhIR at www.cphir.ca using your pharmacy’s unique user name and password. Under “Report an Incident,” you will find a link called “Print Blank Form” on the top right hand corner of the webpage.
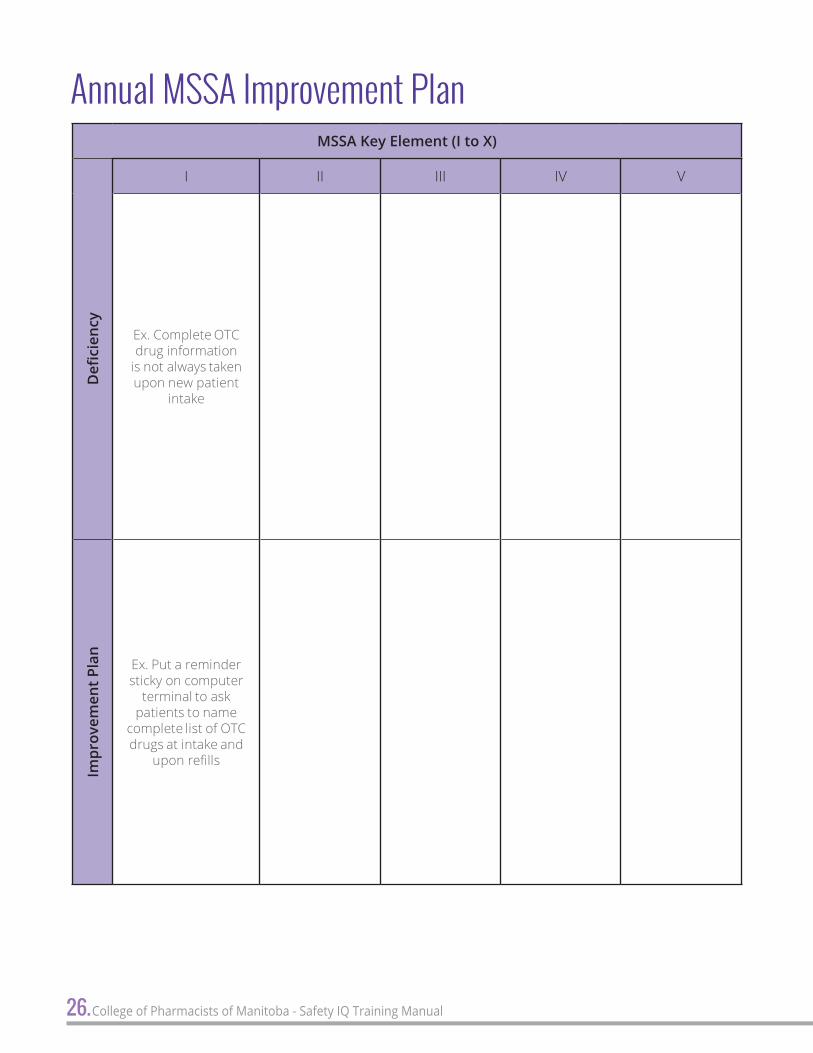
MSSA Instructional Guide The MSSA Instructional Guide will assist your team to understand and successfully complete the MSSA survey, which is a self-assessment tool that helps a pharmacy team to evaluate the level of safety in their practice. This instructional guide describes different ways you can display the answers submitted from your pharmacy team, providing an excellent way to facilitate discussions and come up with improvement plans. An sample Annual MSSA Improvement Plan is included on page 26 of this guide.
To access the online version, log in to CPhIR at www.cphir.ca using your pharmacy’s unique user name and password. Under “Your Account,” you will find a link to the “MSSA Instructional Guide” and the “MSSA Handbook.”
8. College of Pharmacists of Manitoba - Safety IQ Training Manual
Sample Quarterly Meeting Agenda This has been included to help pharmacy managers conduct quarterly staff meetings. By following a standard agenda, quarterly meetings should address the same content and provide staff members with a predictable, structured flow. Time is allocated for review of old business, review of new medication incidents, and announcements to staff. At the end of each meeting, a tentative date for the next meeting should be set by all in attendance. It is important that the improvement plan is reviewed and amended as needed at each meeting. A copy of this document can be found on page 20 of this guide
Quarterly Meeting Report and Action Plan FormsThis should be filled out for each quarterly meeting. The form encourages discussion and analysis of medication incidents based on a number of dimensions, including workflow, staffing and environment issues. The creation of action plans in each of these areas assist in the effort to reduce the likelihood of a medication incident or near-miss reoccurring. These forms also aide in the discussion of “old business” during quarterly meetings to ensure follow through on the action plans. Samples of these forms can be found on pages 21 - 23 of this guide.
To access the online version, log in to CPhIR at www.cphir.ca using your pharmacy’s unique user name and password. Under “Quality Improvement,” you will find a link called “Print Blank Meeting Form” on the top left hand corner of the webpage.
CQI Summarization Document This document provides a “self-audit” for pharmacies and it can be useful to fill this document out monthly, together with the use of the “Stats” and “Quality Improvement” features in CPhIR, to help keep track of the number of medication incidents and near-misses reported and when quarterly meetings take place. A copy of the summarization document can be found on pages 24 and 25 of this guide.
Comprehensive Analysis InstructionsThese instrucitons provides pharmacies with directions on how to employ comprehensive or root cause analysis techniques when analyzing medication incidents during quarterly and staff meetings. An outline of this process can be found on pages 27 and 28 of this guide.
Constellation DiagramConstellation diagramming is an analysis and problem-solving tool that offers a systematic way to analyze factors that contribute to medication incidents and near-misses. As a visual representation, constellation diagrams encourage teams to draw connections between contributing factors and bring clarity to problem-solving. Instructions to create a constellation diagram can be found on pages 29-33 of this guide. An example of a completed constellation diagram can be found on pages 34 and 35 of this guide.
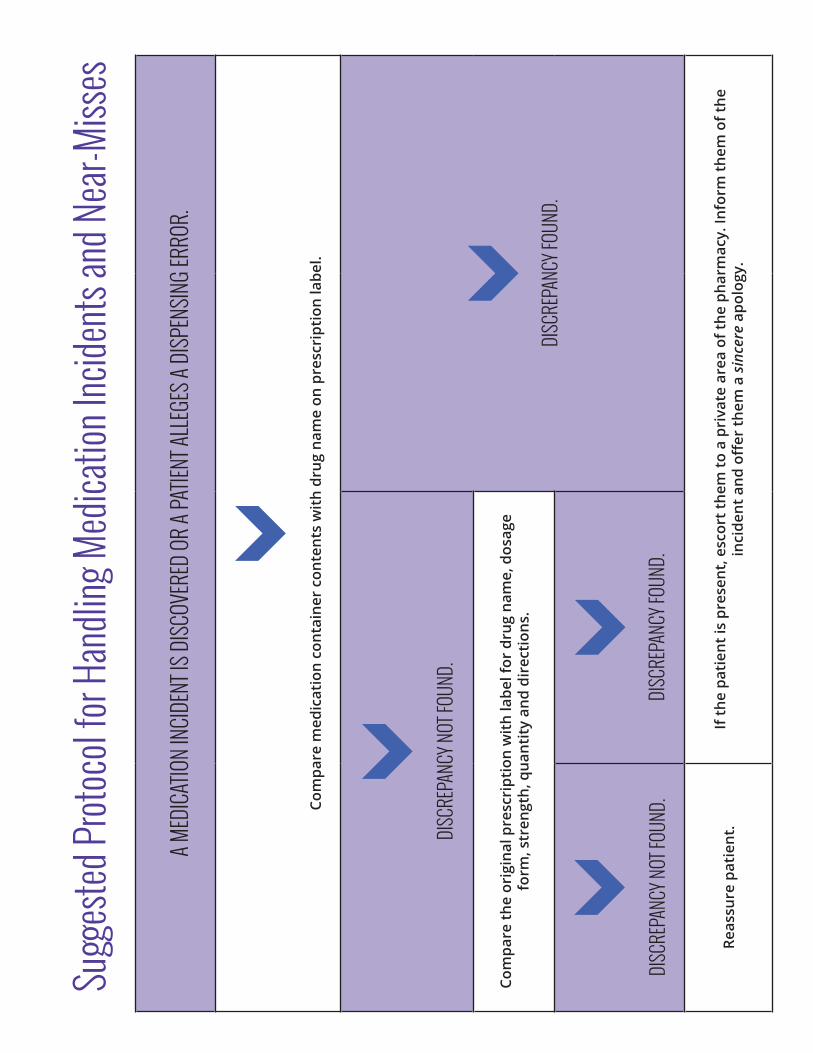
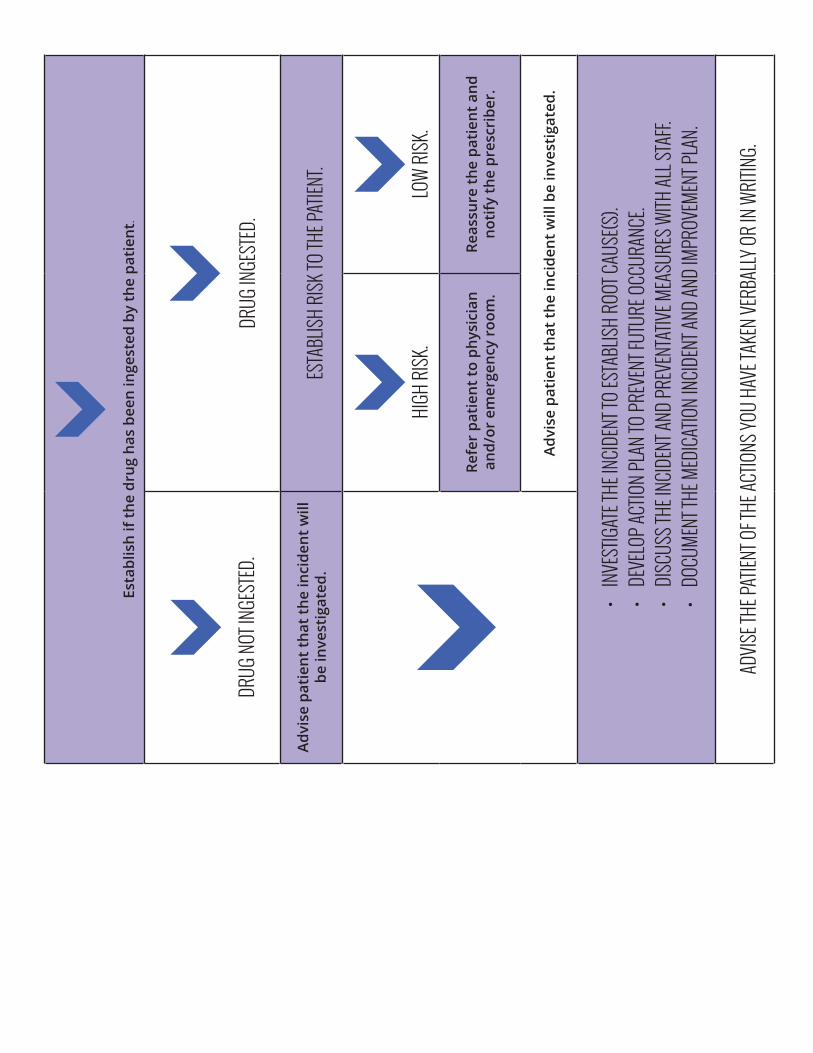
Suggested Protocol for Handling Medication Incidents and Near-Misses This provides an easy-to-follow policy when a medication incident that has reached the patient has occurred or is suspected to have occurred in the dispensary. The protocol is generic enough to use in all instances where a medication incident has reached a patient and provides direct advice on how to proceed. This protocol should be placed on a shared notice space for all pharmacy professionals (pharmacists, pharmacy technicians, pharmacy assistants, and locum staff, etc.) to view and reference.
A copy of this document can be found on pages 36 and 37 of this guide.
8. 9.College of Pharmacists of Manitoba - Safety IQ Training Manual
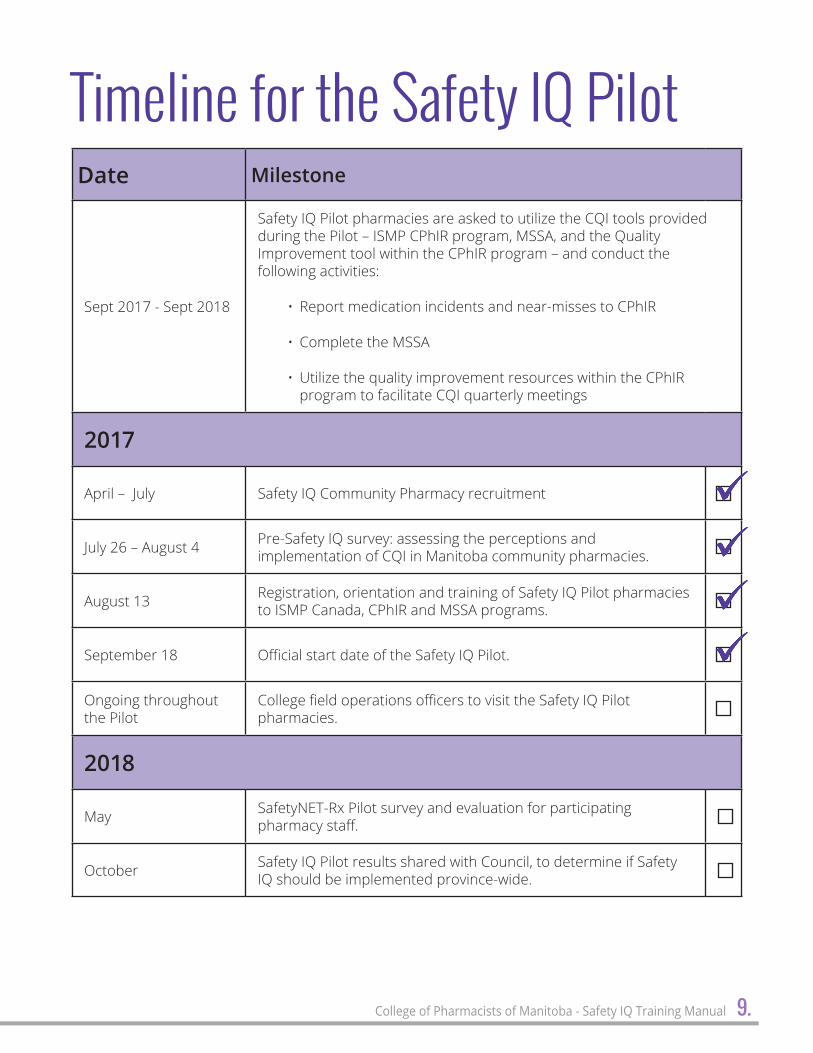
Timeline for the Safety IQ PilotDate Milestone
Sept 2017 - Sept 2018
Safety IQ Pilot pharmacies are asked to utilize the CQI tools provided during the Pilot – ISMP CPhIR program, MSSA, and the Quality Improvement tool within the CPhIR program – and conduct the following activities:
• Report medication incidents and near-misses to CPhIR
• Complete the MSSA
• Utilize the quality improvement resources within the CPhIR program to facilitate CQI quarterly meetings
2017
April – July Safety IQ Community Pharmacy recruitment
July 26 – August 4 Pre-Safety IQ survey: assessing the perceptions and implementation of CQI in Manitoba community pharmacies.
August 13 Registration, orientation and training of Safety IQ Pilot pharmacies to ISMP Canada, CPhIR and MSSA programs.
September 18 Official start date of the Safety IQ Pilot.
Ongoing throughout the Pilot
College field operations officers to visit the Safety IQ Pilot pharmacies.
2018
May SafetyNET-Rx Pilot survey and evaluation for participating pharmacy staff.
October Safety IQ Pilot results shared with Council, to determine if Safety IQ should be implemented province-wide.

10. College of Pharmacists of Manitoba - Safety IQ Training Manual
Frequently Asked Questions:Safety IQ and CQIWhat is a medication incident or a near-miss event?The College’s Medication Incidents and Discrepancies or Near-miss Events Practice Direction states the following:
Medication incident – a preventable occurrence or circumstance that may cause or lead to inappropriate medication use or patient harm. Medication incidents may be related to professional practice, drug products, procedures, and systems, and include prescribing, order communication, product labelling/ packaging/nomenclature, compounding, dispensing, distribution, administration, education, monitoring, and use.
Discrepancy or Near-Miss Event – an event or circumstance that took place, and could have resulted in an unintended or undesired outcome(s), but was discovered before reaching the patient.
Do all medication incidents need to be reported?All medication errors that reach a patient must be recorded anonymously online, as well as fully and identifiably within readily retrievable records in the pharmacy.
As outlined in the Medication Incidents and Discrepancies or Near-miss Events Practice Direction, the extent to which intercepted errors are reported will be a professional judgment decision of the pharmacy manager in consideration of the nature of the intercepted error, its implication for patient safety, and the extent to which it is reoccurring.
What is a Safety IQ Champion?As part of the Safety IQ Pilot, each store will ideally select at least two in-store Champions, preferably one pharmacist and one pharmacy technician. These Safety IQ Champions are
responsible for training other staff by creating an open dialogue on medication discrepancies and near-miss events and introduce the Safety IQ project. These individuals are responsible for bringing their pharmacy team together annually to
• complete the Medication Safety Self-Assessment (MSSA) survey;
• training staff to use the Canadian Pharmacy Incident Reporting (CPhIR) tool; and
• scheduling and facilitating quarterly review meetings.
What is the Medication Safety Self-Assessment (MSSA) survey?The MSSA survey is an assessment tool that helps a pharmacy team to evaluate the level of safety in their practices. This assessment requires the pharmacy team to answer 89 questions on ten key elements. The tool will be completed by each participating pharmacy annually.
What is the Community Pharmacy Incident Reporting (CPhIR) tool?CPhIR is an online reporting program developed in a collaboration with the ISMP Canada, the Ontario Ministry of Health and Long-term Care (OMHLTC), and the participating pharmacies of the initial SafetyNET-Rx pilot. CPhIR allows pharmacies to anonymously and easily report a medication incident directly from their own computer terminals to an independent organization for population of a national aggregate database. Graphs can be generated instantaneously in order to assist pharmacy managers in presenting medication incident information to their staff for discussion at quarterly meetings and to identify trends over time.

10. 11.College of Pharmacists of Manitoba - Safety IQ Training Manual
Having access to CPhIR has many advantages, including ISMP Canada’s established policies and processes that enable anonymous reporting that rigorously protect privacy, participants have comfort with using the program to submit sensitive information.
By submitting to a national database, pharmacies enable the identification of safety-related trends and patterns that can be communicated across the profession, not just in their own pharmacy.
Is there a paper form that can be used in place of the online form?Participants can choose to use paper forms to collect error reports if they prefer. In fact, using paper forms is one strategy that can help integrate medication incidents and near-miss events reporting into a pharmacy workflow. These forms can be found on your CPhIR account under the “Report an Incident” tab. On the right hand side of the page, there is an option to “Print Blank Page.” Filled paper forms can be collected in batches from staff and entered manually into the online reporting system at the end of every shift to ensure that all information is captured for the production of aggregated reports.
Is the information that is submitted to ISMP Canada confidential?Yes, the information submitted to ISMP Canada is completely confidential. Reports do not include identifiers for either the individual entering the data or the patient affected by the medication incident. This ensures anonymity of all individuals involved in the incident. The specific information submitted by individual pharmacies can only be viewed by that particular pharmacy by logging in using their username and password.
*Please remember to submit data as an open incident, to prevent lost information as CPhIR will automatically timeout after 24 minutes for confidentiality reasons.
Is there a fee for the use of ISMP Canada’s MSSA and the CPhIR tool?Participating Pilot pharmacies will receive a complimentary 1-year subscription to use ISMP Canada’s MSSA and CPhIR tools.
What is the purpose of quarterly meetings?At least once every quarter, teams within each pharmacy including pharmacy managers, staff pharmacists, pharmacy technicians and pharmacy assistants should meet to discuss the previous quarter’s medication incidents, and to formulate strategies to reduce the likelihood of them occurring in the future. Using the CPhIR tool, pharmacy managers can generate an internal report that analyzes and summarizes the medication incidents and near-miss events submitted to provide a discussion framework for the meeting. Depending on the frequency and severity of the medication incidents occurring at the pharmacy, the pharmacy manager may decide that such meetings should take place more frequently. Also, any areas for improvement as identified in the MSSA and any staff education requirements, etc should be discussed. CPhIR also has an online tool under the “Quality Improvement” tab that allows the pharmacy to record and keep track of quarterly meeting medication incidents, MSSA issues and plans for improvement, etc.
12. College of Pharmacists of Manitoba - Safety IQ Training Manual
Regulatory issues:
Ronda Eros, Practice Consultant College of Pharmacists of Manitoba [email protected]
Jill Hardy, Deputy Registrar College of Pharmacists of Manitoba [email protected]
Communications:
Rachel Carlson, Communications and Quality Assurance Coordinator College of Pharmacists of Manitoba [email protected]
Medication Safety Self-Assessment (MSSA):
Institute for Safe Medication Practices Canada (ISMP Canada) [email protected]
Community Pharmacy Incident Reporting (CPhIR):
Institute for Safe Medication Practices Canada (ISMP Canada) [email protected]
Where can I find the contact information for those involved in the Safety IQ Pilot?
Electronic Links:CPhIR and MSSA The website link to CPhIR and MSSA is:
http://www.cphir.ca
Using the pharmacy username and password provided by ISMP Canada, log into the CPhIR program.
For future reference you may enter the pharmacy information below;
Username: ____________________________
Password: ____________________________
The MSSA electronic link can be accessed once the above CPhIR login information is entered. On the “Home” page of CPhIR, you will see a link “Login to MSSA”.
12. 13.College of Pharmacists of Manitoba - Safety IQ Training Manual
AppendixPractice Direction: Medication Incidents and Discrepancies or Near - Miss Events

14. College of Pharmacists of Manitoba - Safety IQ Training Manual

14. 15.College of Pharmacists of Manitoba - Safety IQ Training Manual
16. 17.College of Pharmacists of Manitoba - Safety IQ Training Manual
The Apology ActHER MAJESTY, by and with the advice and consent of the Legislative Assembly of Manitoba, enacts as follows:
Definitions1 The following definitions apply in this Act.
“apology” means an expression of sympathy or regret, a statement that one is sorry or any other words or actions indicating contrition or commiseration, whether or not the words or actions admit or imply an admission of fault in connection with the matter to which the words or actions relate. («excuses»)
“court” includes a tribunal, an arbitrator and any other person who is acting in a judicial or quasi-judicial capacity. («tribunal»)
Effect of apology on liability2(1) An apology made by or on behalf of a person in connection with a matter
(a) does not constitute an express or implied admission of fault or liability by the person in connection with the matter;
(b) does not, despite any wording to the contrary in a contract of insurance and despite any other enactment, void, impair or otherwise affect insurance coverage that
(i) is available, or
(ii) would, but for the apology, be available, to the person in connection with the matter; and
(c) must not be taken into account in determining fault or liability in connection with the matter.
Evidence of apology not admissible in court2(2) Despite any other enactment, evidence of an apology made by or on behalf of a person in connection with any matter is not admissible in a court as evidence of the fault or liability of the person in connection with the matter.
Coming into force3 This Act comes into force 90 days after the day it receives royal assent.
18. College of Pharmacists of Manitoba - Safety IQ Training Manual
Canadian Disclosure GuidelinesThe Canadian Patient Safety Institute (CPSI) developed the Canadian Disclosure Guidelines (Guidelines) to help organizations be open and honest with patients and families about patient safety incidents. The objectives of the Guidelines are as follows:
Facilitate patient/healthcare provider communications that respect and address the needs of patients and strengthen relationships.
1. Promote a clear and consistent approach to disclosure.
2. Promote interdisciplinary teamwork.
3. Support learning from patient safety incidents.
The following checklist was adapted from the Guidelines for the purposes of the Safety IQ Pilot:
Disclosure Process Plan � Gather existing facts.
� Establish who will present and who will lead the discussion.
� Set when the initial disclosure will occur.
� Formulate what will be said and how effective disclosure will be accomplished.
� Locate a private area to hold disclosure meeting, free of interruptions.
� Be aware of your emotions and seek support if necessary.
� Anticipate patient’s emotions and ensure support is available including who the patient chooses to be part of the discussion such as family, friends, etc.
Initial Disclosure � Introduce the participants to the patient, functions and reasons for attending the meeting.
� Use language and terminology that is appropriate for the patient, being sensitive of cultural and language needs.
� Describe the facts of the adverse event and its outcome known at the time.
� Describe the steps that were and will be taken in the care of the patient.
� Avoid speculation or blame.
� Express regret.
� Inform the patient of the process for analysis of the event and what the patient can expect to learn from the analysis, with appropriate timelines.
18. 19.College of Pharmacists of Manitoba - Safety IQ Training Manual
� Provide time for questions and clarify whether the information is understood.
� Offer to arrange subsequent meetings along with sharing key contact information.
� Offer practical and emotional support such as spiritual care services, counselling and social work, as needed.
� Facilitate further investigation and treatment if required.
Subsequent and Post-Analysis Disclosure � Continue practical and emotional support as required.
� Further factual information as it becomes available.
� Describe any actions that are taken as a result of internal analyses such as system improvements.
Document the disclosure discussions as per organizational practices and include: � The time, place, and date of disclosure.
� The names and relationships of all attendees.
� The facts presented.
� Offers of assistance and the response.
� Questions raised and the answers given.
� Plans for follow-up with key contact information for the organization.
Source: Canadian Patient Safety Institute (CPSI). Canadian Disclosure Guidelines. 2011. Available: http://www.patientsafetyinstitute.ca/en/toolsResources/disclosure/Pages/default.aspx.
20.College of Pharmacists of Manitoba - Safety IQ Training Manual
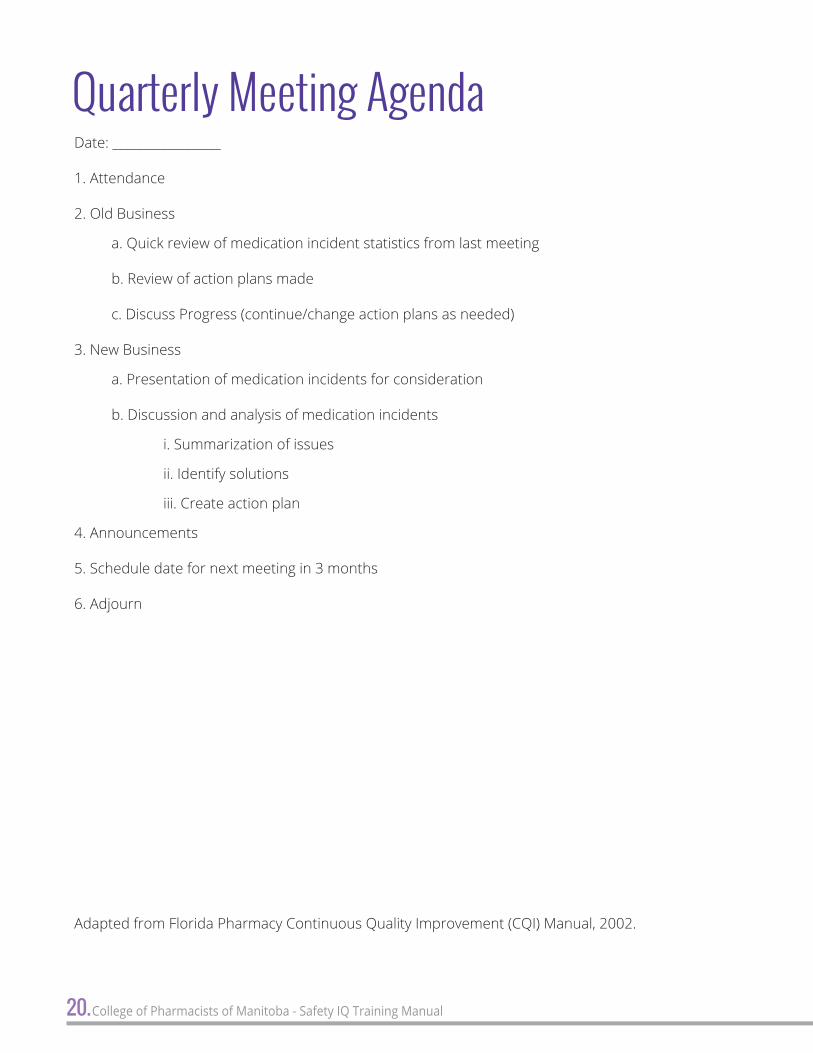
Quarterly Meeting AgendaDate: __________________
1. Attendance
2. Old Business
a. Quick review of medication incident statistics from last meeting
b. Review of action plans made
c. Discuss Progress (continue/change action plans as needed)
3. New Business
a. Presentation of medication incidents for consideration
b. Discussion and analysis of medication incidents
i. Summarization of issues
ii. Identify solutions
iii. Create action plan
4. Announcements
5. Schedule date for next meeting in 3 months
6. Adjourn
Adapted from Florida Pharmacy Continuous Quality Improvement (CQI) Manual, 2002.
20. 21.College of Pharmacists of Manitoba - Safety IQ Training Manual
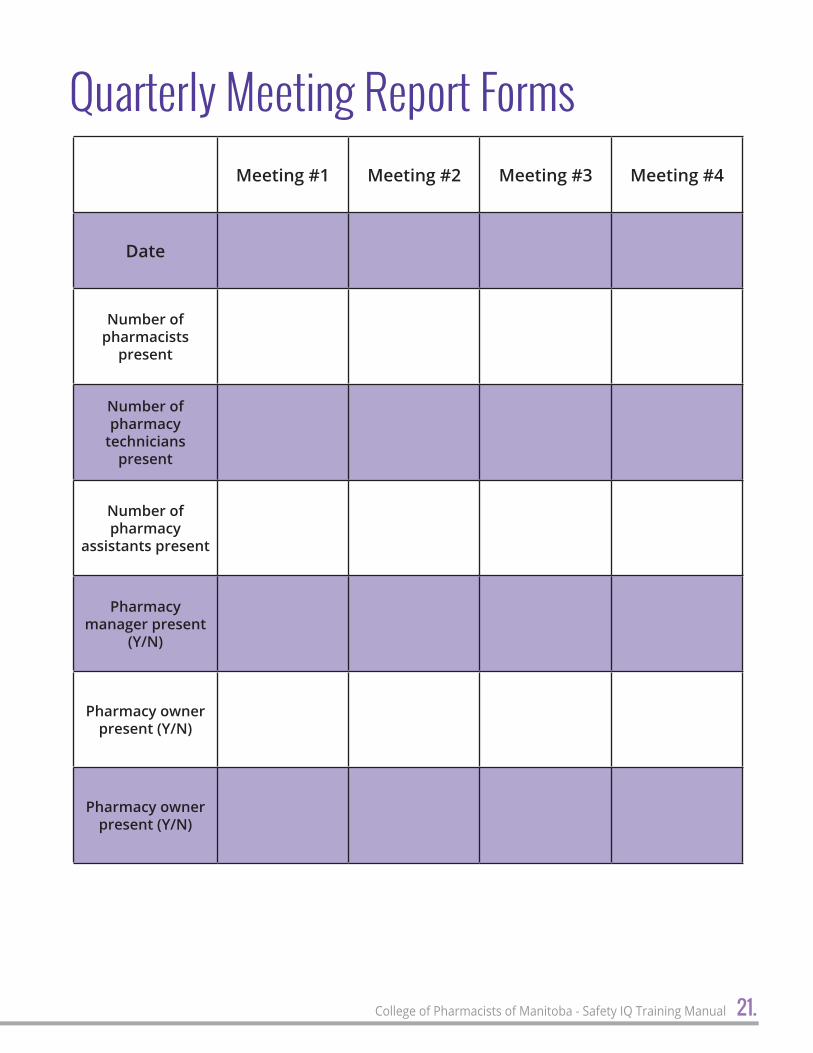
Quarterly Meeting Report FormsMeeting #1 Meeting #2 Meeting #3 Meeting #4
Date
Number of pharmacists
present
Number of pharmacy
technicians present
Number of pharmacy
assistants present
Pharmacy manager present
(Y/N)
Pharmacy owner present (Y/N)
Pharmacy owner present (Y/N)

22. College of Pharmacists of Manitoba - Safety IQ Training Manual
Meeting #1 Notes
Meeting #2 Notes
Meeting #3 Notes
Meeting #2 Notes
Quarterly Meeting Notes

22. 23.College of Pharmacists of Manitoba - Safety IQ Training Manual
Quarterly Meeting Action PlanPlanned Action
Meeting #1 (date & discussion)
Follow Up
Example: Place Rx’s to be picked up in red basket
September 15, 2017
Confusion surrounding which Rx’s to be picked up vs. waited for.
Will use colour-coded baskets.
December 15, 2017
Not adopted by all staff. Discussed again to ensure
everyone is on same page.
March 15, 2017
Working well. Less confusion
and reduced near misses.
June 15, 2018
Trained new staff on procedure. Still
working well.

24.College of Pharmacists of Manitoba - Safety IQ Training Manual
General Information
Pharmacy Name: License/Accreditation/Permit No.:
Address: Phone/Fax No.:
Email:
Time Period of report (mm/yyyy – mm/yyyy):
Medication Safety Self-Assessment
Date of last completed self-assessment: (dd/mm/yyyy):
Number of individuals who participated in the completion of the self-assessment:
Dates of follow-up discussion with staff:
Was the analysis of the self-assessment results completed? (Y/N) ________
If Yes, when? __________
Medication Incident Reporting
Number of medication incidents reported each month:
Jan _____ Feb _____ Mar ______ Apr _____ May _____ Jun _____ Jul _____ Aug _____ Sep _____ Oct _____ Nov _____ Dec _____
Who primarily enters medication incident data?
Person who discovers medication incidents
Pharmacist Pharmacy Technician Pharmacy Assistant Student
Quarterly Meetings
Q1 Q2 Q3 Q4
Date of meeting (dd/mm/yyyy)
CQI Summarization
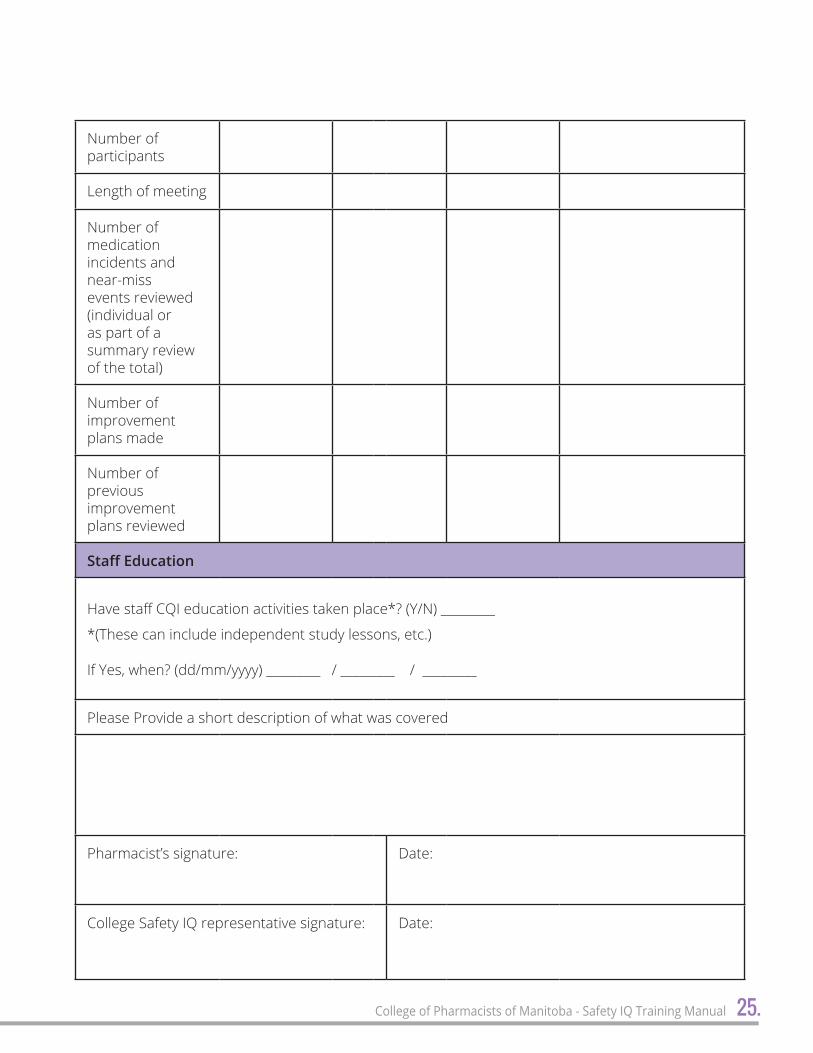
24. 25.College of Pharmacists of Manitoba - Safety IQ Training Manual
Number of participants
Length of meeting
Number of medication incidents and near-miss events reviewed (individual or as part of a summary review of the total)
Number of improvement plans made
Number of previous improvement plans reviewed
Staff Education
Have staff CQI education activities taken place*? (Y/N) _________
*(These can include independent study lessons, etc.)
If Yes, when? (dd/mm/yyyy) _________ / _________ / _________
Please Provide a short description of what was covered
Pharmacist’s signature: Date:
College Safety IQ representative signature: Date:
26.College of Pharmacists of Manitoba - Safety IQ Training Manual
Annual MSSA Improvement PlanMSSA Key Element (I to X)
Defi
cien
cy
I II III IV V
Ex. Complete OTC drug information
is not always taken upon new patient
intake
Impr
ovem
ent P
lan
Ex. Put a reminder sticky on computer
terminal to ask patients to name
complete list of OTC drugs at intake and
upon refills
26. 27.College of Pharmacists of Manitoba - Safety IQ Training Manual
Comprehensive Analysis (or Root Cause Analysis) Steps and InstructionsComprehensive Analysis or Root Cause Analysis is a method of problem solving techniques with a purpose of determining the “root cause” of a medication incident in order to prevent the medication incident from occurring again in the future. A Comprehensive Analysis or Root Cause Analysis views every medication incident as an opportunity to learn and improve a process by determining the “root cause” of a medication incident so that the issue can be addressed in order to take appropriate action in your community pharmacy to improve the overall process. When determining the “root cause” of a medication incident, it can be helpful to use a constellation diagram with your pharmacy staff for brainstorming purposes. The constellation diagram will list various possibilities to where the “root cause” of the medication incident lies.
The steps to Comprehensive Analysis or Root Cause Analysis can be described as follows:
What Happened?Step 1: Define and describe the medication incident that occurred in your community pharmacy.
When defining the medication incident that occurred in your pharmacy it is important to be specific about the incident that occurred (e.g. what drugs were involved). You may also want to categorize the medication incident that occurred in your pharmacy as well during this step (e.g. wrong dose; wrong drug).
Step 2: Detail as much information about the medication incident as possible. Gather as much detail about the situation as possible on your own and from pharmacy staff who were working at the time of the medication incident. Asking questions such as “when did the medication incident happen?” and “what else was going on in the community pharmacy at the time?” are some examples. You may want experienced staff who may be knowledgeable
of why exactly the medication incident happened to speak at your brainstorming session for determining the root cause of the problem.
How and Why did it Happened?Step 3: Determine all possible causes of the medication incident using the
Constellation Diagram (see below) and sort based on the categories of causes in the diagram.
During your brainstorming session with your pharmacy staff, start out by using the Constellation Diagram on a white board or where everyone can see it and contribute. Fill in the medication incident defined in Step 1 in the centre of the constellation where it says incident and the outcome of the incident. The Constellation Diagram contains categories where causes of the medication incident may lie. Brainstorm with your staff all the possible causes of the medication incident and document them under the appropriate categories. The categories listed in the diagram are only a suggestion, so feel free to add any categories that you feel are appropriate for your pharmacy. Also, it is not important to fill in all of the categories, it is only important for you and your staff to do a thorough brainstorming session here and to consider all of the categories on the Constellation Diagram so that no potential causes of the medication incident are missed.
Step 4: Define relationships between the potential causes of the medication incident identified in Step 3 by asking why repeatedly.
Now that your Constellation Diagram is filled out, look at each of the causes of the \medication incident that you’ve listed under the categories individually. For each cause ask the team to brainstorm why it happened. For example, if you’ve determined that the

28. College of Pharmacists of Manitoba - Safety IQ Training Manual
medication incident was that the wrong medication was given out and one potential cause was that the staff member was not trained correctly, ask why. When you’ve determined the potential cause of the staff member not being trained correctly ask why again and keep going with this process until the question why cannot be answered. Continue this process for each of the potential causes that you have listed in your Constellation Diagram.
What can be Done to Reduce the Likelihood of Recurrence?Step 5: Brainstorm which potential cause would eliminate the medication incident in the community pharmacy if it was fixed and identify potential solutions to eliminate the potential cause.
When brainstorming possible solutions to eliminate the cause of the medication incident the solution must meet three important criteria. First, the solution to eliminate the cause of the medication incident must eliminate the medication incident if it is implemented. Second, if eliminated, the root solution cannot result in more medication incidents within the pharmacy. Third, the solution must also be possible within the pharmacy. When conducting the brainstorming session there should be discussion among the pharmacy staff why a potential strategy for the removal of the cause of the medication incident does or does not meet the specified criteria. This process could leave you with only one possible solution or several.
Step 6: Rank solutions that will best eliminate the medication incident in the pharmacy.
If Step 5 leaves you with only one possible solution then there is no need to determine the best solution as there is only one choice. If instead there are several possible solutions from Step 5 then the team should be asked to rank each solution based on effectiveness of eliminating the medication incident and feasibility of the solution. The averages of the two scores should be calculated and the solution with the best score should be chosen for implementation.
Step 7: Implement the solutions determined in Step 6 into your pharmacy’s process and monitor to ensure the solutions have been effective.
Upon implementation of the chosen solution it is important to monitor to ensure the solution has had the desired effectiveness. If the solution has not resulted in the desired effectiveness, it could be because the “root cause” of the medication incident was incorrect or because the best possible solution to remove the “root cause” was not chosen.
Step 8: If the medication incident continues to occur, repeat the Comprehensive Analysis or Root Cause Analysis process.
If you determine that the solution implemented has not had the desired effectiveness it may be necessary to complete the Comprehensive Analysis or Root Cause Analysis again to determine a different “root cause” to the medication incident that may have been incorrectly defined previously, or to brainstorm a better solution to remove the “root cause” from the process. Because it may be necessary to repeat the process in your pharmacy for the same medication incident if the solution is not effective, it is important to keep all notes and information gathered about the medication incident until the solution has been deemed to be a success.
Adapted from: Incident Analysis Collaborating Parties. Canadian Incident Analysis Framework.Edmonton, AB: Canadian Patient Safety Institute; 2012.

28. 29.College of Pharmacists of Manitoba - Safety IQ Training Manual
Constellation diagramming is an analysis and problem-solving tool developed in the Canadian Incident Analysis Framework. A constellation diagram offers a systematic way to analyze factors that contribute to medication incidents and near-misses at the system level. As a visual representation, constellation diagrams encourage teams to draw connections between contributing factors and bring clarity to problem-solving.
There are five steps to creating a constellation diagram:
Step 1: Describe the incident or near-miss.
Step 2: Identify potential contributing factors.
Step 3: Define inter-relationships between and among potential contributing factors.
Step 4: Identify the findings.
Step 5: Confirm the findings with the team.
Step 1: Describe the Incident
Briefly summarize the incident and harm/potential harm in the centre of the diagram (typically less than ten words):
It is crucial for the team to clearly define the starting point for analysis. This can be a harmful outcome that the team wants to prevent (a near-miss event), or this can be a medication incident in which a medication error was made and the medication was dispensed to the patient (no-harm, mild-harm, severe-harm, or death).
INCIDENT:
OUTCOME:
Figure 1: Describe the Incident
Step 2: Identify Potential Contributing Factors
a. Add the contributing factors categories to the diagram (task, equipment, work environment, patient, care team, organization, etc.) (See Figure 2).
b. Identify the potential contributing factors to each category. Asking questions about each category can help your team brainstorm as many possible contributing factors that you can. Use sticky notes to add the factors (see Figure 3).
TASK
EQUIPMENT
WORKENVIRONMENT
PATIENT
CARE TEAM
ORGANIZATION
INCIDENT:
OUTCOME:
Figure 2: Add contributing factor categories
How to Create a Constellation Diagram

30.College of Pharmacists of Manitoba - Safety IQ Training Manual
IDENTIFYING CONTRIBUTING FACTORS
When identifying contributing factors it is important to throughly interrogate the issue. Your team may want to consider the following questions to build your constellation diagram (this is not an exhaustive list, but rather, a starting-off-point for your brainstorming ):
TASK (care/work process):
Were there previous or predicted failures for this task?
Were specialized skills required to perform the task?
Was a fixed process or sequence of steps required (e.g. order sets, checklists)? Did it exist and was is followed?
Was the information required to make care decisions available and up-to-date?
Were there constraints or pressures (e.g. time, resources) when performing the task?
EQUIPMENT (including information and communication systems):
Were the warning labels, reference guide and safety mechanisms functional and readily visible/accessible?
Was the equipment standardized?
Would the users describe this equipment as ‘easy to use’?
WORK ENVIRONMENT:
Did noise levels interfere with communication?
Was lighting adequate for the task?
Was the work area adequate for the task(s) being performed (e.g. enough space, appropriate layout, accessible resource, etc)?
PATIENT(S) CHARACTERISTICS:
Did the patient(s) have the information to assist avoiding the incident? If not, what would have supported the patient in assisting their care team?
Did factors like age, sex, medications, allergies, diagnosis, other medical conditions, contribute to the incident? How did they contribute?
Did any social or cultural factors contribute to the incident? What factors? In which way?
CARE TEAM:
Was there a clear understanding of roles and responsibilities?
Was the quality and quantity of communication (verbal/written) between team members appropriate (clear, accurate, free of jargon, relevant, complete, timely)?
Were there regular team briefings/debriefings about important care issues?
Was team morale good? Do team members support one another?
ORGANIZATION:
Were relevant polices and procedure available, known, accessible, and did they meet the needs of users?
Were there any workarounds to the documented policy/procedure?
Was everyone (patients, clinicians, other staff) comfortable to speak-up about safety concerns?
Was communication between staff and management supportive of day-to-day safe patient care?
Did scheduling influence the staffing level, or cause stress or fatigue?

30. 31.College of Pharmacists of Manitoba - Safety IQ Training Manual
Step 3: Define Inter-relationships between and among contributing factors
Once your team has identified the potential contributing factors in Step 2, the second phase of analysis begins. Your team should be asking questions such as, what was this influenced by? What else influenced the circumstances?
The team then expands the constellation diagram to include ‘relational chains’ of contributing factors (see Figure 4). This questioning process continues until there are no more questions, knowledge becomes limited, or until issues identified fall outside the scope of the analysis.
It is important to recognize that sometimes the relationships between the factors are a key part of the problem.
Step 4: Identify the Findings
The next step in the analysis is to identify the findings that are central to the incident (see Figure 5). The team can expect more than one key finding as there is seldom, if ever, only a single reason why an incident occurred.
Finding will be identified in three categories:
• Factors that, if corrected, would likely have prevented the incident or mitigated the harm — these will be the basis for developing recommended actions.
TASK
EQUIPMENT
WORKENVIRONMENT
PATIENT
CARE TEAM
ORGANIZATION
INCIDENT:
OUTCOME:
FACTOR
FACTOR
FACTORFACTOR
FACTORFACTOR
FACTORFACTOR
FACTOR
FACTOR
Figure 3: Add contributing factors
FACTOR

32. College of Pharmacists of Manitoba - Safety IQ Training Manual
TASK
EQUIPMENT
WORKENVIRONMENT
PATIENT
CARE TEAM
ORGANIZATION
INCIDENT:
OUTCOME:
FACTOR
FACTOR
FACTORFACTOR
FACTORFACTOR
FACTORFACTOR
FACTOR
FACTOR
Figure 4: Define relationships between potential contributing factors
• Factors that, if corrected, would not have prevented the incident or mitigated the harm, but are important for patient/staff safety or safe patient care in general. These issues should be included in the team’s findings and brought to the attention of appropriate individuals for follow-up and documents in the analysis report.
• Mitigating factors — factors that didn’t allow the incident to have more serious consequences and represent solid safeguards that should be kept in place.
Step 5: Confirm the Findings with the Team
Ensure consensus and support for the development of recommended actions.
The team should agree on the findings before moving forward to develop recommended actions. If there is a lack of immediate agreement, it is important to discuss and work through any disagreements to strive for consensus before proceeding.
For an example of an incident analysis using a constellation diagram, see page 38 of this manual.
FACTOR

32. 33.College of Pharmacists of Manitoba - Safety IQ Training Manual
Adapted from: Incident Analysis Collaborating Parties. Canadian Incident Analysis Framework. Edmonton, AB: Canadian Patient Safety Institute; 2012.
TASK
EQUIPMENT
WORKENVIRONMENT
PATIENT
CARE TEAM
ORGANIZATION
INCIDENT:
OUTCOME:
FACTOR
FACTOR
FACTORFACTOR
FACTORFACTOR
FACTORFACTOR
FACTOR
FACTOR
Figure 5: Completed Constellation Diagram
FINDING
FINDING
FINDINGFINDING
FINDING
FINDING
FINDING
FACTOR

34.College of Pharmacists of Manitoba - Safety IQ Training Manual
Constellation Diagram ExampleAn Insulin Mix-up IncidentIncident Description: A patient with insulin-dependent diabetes had a prescription for Novolin®ge 30/70 Penfill® and was self-administering the drug every morning and every evening by insulin pen (Novolin-Pen®). The patient had recently obtained from the community pharmacy a refill of the cartridge prescription, receiving several boxes of 5 cartridges each. On the morning of the incident, the patient had inserted a new cartridge, taken from one of the new boxes, into the insulin pen. A short time after self-injecting the prescribed morning dose, the patient was found in a diaphoretic state, with pupils dilated and with a decreased level of consciousness. Fortunately, the symptoms were recognized as signs of hypoglycemia,
and the patient was given sugar followed by additional food. Shortly thereafter, the patient’s blood glucose level, measured with a glucometer, was approximately 2.5 mmol/L. Because of the unexplained hypoglycemia, the insulin supply was checked. It was discovered that one box of NovoRapid® insulin had been given to the patient, along with several boxes of the correct Novolin®ge 30/70.
Reference: Patient Report of Insulin Mix-Up Shared. ISMP Canada Safety Bulletin 2007; 7(6): 1-2. Available from: https://www.ismp-canada.org/download/safetyBulletins/ISMPCSB2007-06InsulinMixUp.pdf
Constellation Diagram of Insulin Mix-Up Incident

34. 35.College of Pharmacists of Manitoba - Safety IQ Training Manual
Recommended Actions Table for an Insulin Mix-up IncidentCausal Statement #1: Pharmaceutical “branding” through look-alike packaging increased the likelihood of incorrect product selection, dispensing and administration of the incorrect insulin, and the resulting acute hypoglycemia.
Causal Statement #2: Repeated scanning of only one of the multiple items selected decreased the likelihood that an incorrect product selection would be detected, leading to the dispensing and administration of the incorrect insulin and the resulting acute hypoglycemia.
Action # Description Hierarchy of
effectivenessType of
action
Staff member(s) responsible for/ involved in implementation
1A
Apply warning labels to all look-alike insulin products in refrigerator.
Control Immediate
Pharmacy manager – Oversee
Pharmacy technician – Implement action
1B
Segregate short, intermediate and long-acting insulins in the refrigerator
Control Immediate Pharmacy manager
– Oversee and implement
Simplification & Standardization
Simplification & Standardization
Action # Description Hierarchy of
effectivenessType of
action
Staff member(s) responsible for/ involved in implementation
2A
Require that each item be scanned during the dispensing process to maximize the value of the check process
Control Immediate
Pharmacy manager – Oversee
Pharmacy technician, staff pharmacists – Implement action
Rules & Policies
Timeframe for Implementation
Timeframe for Implementation
36.College of Pharmacists of Manitoba - Safety IQ Training Manual
A MED
ICATIO
N IN
CIDEN
T IS D
ISCOV
ERED
OR A
PATIE
NT AL
LEGE
S A D
ISPEN
SING
ERRO
R.
Com
pare
med
icat
ion
cont
aine
r co
nten
ts w
ith
drug
nam
e on
pre
scri
ptio
n la
bel.
DISC
REPA
NCY N
OT FO
UND.
DISC
REPA
NCY F
OUND
.
Com
pare
the
orig
inal
pre
scri
ptio
n w
ith
labe
l for
dru
g na
me,
dos
age
form
, str
engt
h, q
uant
ity
and
dire
ctio
ns.
DISC
REPA
NCY N
OT FO
UND.
DISC
REPA
NCY F
OUND
.
Reas
sure
pat
ient
.If
the
pati
ent i
s pr
esen
t, es
cort
them
to a
pri
vate
are
a of
the
phar
mac
y. In
form
them
of t
he
inci
dent
and
off
er th
em a
sin
cere
apo
logy
.
Esta
blis
h if
the
drug
has
bee
n in
gest
ed b
y th
e pa
tien
t.
DRUG
NOT
INGE
STED
.DR
UG IN
GEST
ED.
Advi
se p
atie
nt th
at th
e in
cide
nt w
ill
be in
vest
igat
ed.
ESTA
BLISH
RISK
TO TH
E PAT
IENT.
HIGH
RISK
.LO
W RI
SK.
Refe
r pa
tien
t to
phys
icia
n an
d/or
em
erge
ncy
room
.Re
assu
re th
e pa
tien
t and
no
tify
the
pres
crib
er.
Advi
se p
atie
nt th
at th
e in
cide
nt w
ill b
e in
vest
igat
ed.
• IN
VEST
IGAT
E THE
INCID
ENT T
O ES
TABL
ISH RO
OT CA
USE(S
).•
DEVE
LOP A
CTIO
N PL
AN TO
PREV
ENT F
UTUR
E OCC
URAN
CE.
• DI
SCUS
S THE
INCID
ENT A
ND PR
EVEN
TATIV
E MEA
SURE
S WITH
ALL S
TAFF.
• DO
CUME
NT TH
E MED
ICATIO
N IN
CIDEN
T AND
AND
IMPR
OVEM
ENT P
LAN.
ADVIS
E THE
PATIE
NT O
F THE
ACTIO
NS YO
U HA
VE TA
KEN
VERB
ALLY
OR I
N WR
ITING
.
Sugg
ested
Proto
col fo
r Han
dling
Med
icatio
n Inc
idents
and N
ear-M
isses
36. 37.College of Pharmacists of Manitoba - Safety IQ Training Manual
A MED
ICATIO
N IN
CIDEN
T IS D
ISCOV
ERED
OR A
PATIE
NT AL
LEGE
S A D
ISPEN
SING
ERRO
R.
Com
pare
med
icat
ion
cont
aine
r co
nten
ts w
ith
drug
nam
e on
pre
scri
ptio
n la
bel.
DISC
REPA
NCY N
OT FO
UND.
DISC
REPA
NCY F
OUND
.
Com
pare
the
orig
inal
pre
scri
ptio
n w
ith
labe
l for
dru
g na
me,
dos
age
form
, str
engt
h, q
uant
ity
and
dire
ctio
ns.
DISC
REPA
NCY N
OT FO
UND.
DISC
REPA
NCY F
OUND
.
Reas
sure
pat
ient
.If
the
pati
ent i
s pr
esen
t, es
cort
them
to a
pri
vate
are
a of
the
phar
mac
y. In
form
them
of t
he
inci
dent
and
off
er th
em a
sin
cere
apo
logy
.
Esta
blis
h if
the
drug
has
bee
n in
gest
ed b
y th
e pa
tien
t.
DRUG
NOT
INGE
STED
.DR
UG IN
GEST
ED.
Advi
se p
atie
nt th
at th
e in
cide
nt w
ill
be in
vest
igat
ed.
ESTA
BLISH
RISK
TO TH
E PAT
IENT.
HIGH
RISK
.LO
W RI
SK.
Refe
r pa
tien
t to
phys
icia
n an
d/or
em
erge
ncy
room
.Re
assu
re th
e pa
tien
t and
no
tify
the
pres
crib
er.
Advi
se p
atie
nt th
at th
e in
cide
nt w
ill b
e in
vest
igat
ed.
• IN
VEST
IGAT
E THE
INCID
ENT T
O ES
TABL
ISH RO
OT CA
USE(S
).•
DEVE
LOP A
CTIO
N PL
AN TO
PREV
ENT F
UTUR
E OCC
URAN
CE.
• DI
SCUS
S THE
INCID
ENT A
ND PR
EVEN
TATIV
E MEA
SURE
S WITH
ALL S
TAFF.
• DO
CUME
NT TH
E MED
ICATIO
N IN
CIDEN
T AND
AND
IMPR
OVEM
ENT P
LAN.
ADVIS
E THE
PATIE
NT O
F THE
ACTIO
NS YO
U HA
VE TA
KEN
VERB
ALLY
OR I
N WR
ITING
.

38.College of Pharmacists of Manitoba - Safety IQ Training Manual
Notes:

38. 39.College of Pharmacists of Manitoba - Safety IQ Training Manual
Notes:
