pilomatrixoma in the differential diagnosis of pathologic calcification of the paraoral soft tissue
TRANSCRIPT
Int. J. Oral Surg. 1977: 6:283-286
(Key words; calci]ications, pathologic; tumors, skin)
Pilomatrixoma in the differential diagnosis of pathologic calcification of the paraoral soft tissue
I. VAN DER WAAL, G. BEEMSTER, H. A. KRAAIJENttAGEN AND W. A. M. VAN DER KWAST
Free University, Amsterdam
ABSa'mXCT - As an incidental finding a firm nodule was palpated in the skirt overlying the right angle o~' the mandibIe in a 78-year-oId female. The radiograph showed a dense calcification. Histologically the lesion proved to be a pilomatrixoma. A br/ef review of the literature of the pilomatrixoma is presented. Finally, some comments are made about calcification in the paraoral region, especially in the lateral aspect of the neck.
(Received [or publication 17 July, accepted 6 September 1976)
The pilomatrixoma is a tumor that was first described in 1880 by MALI-IERBE & CHE- NANTAIsS, who used the term "calcifying epithelioma of the sebaceous glands". They considered this lesion a benign neoplasm. In 1954 CASTmLIANO & RONtNaER1 de- scribed three patients of their own series and reviewed 243 reported in the literature between 1880 and 1950. About 80 % of all patients were under the age of 25, while only 5 % were above the age of 60. Both sexes proved to be equally affected. The duration of most cases varied from some months to 24 months. The skin of the head and neck was the most favored site. Clini- cally the lesions usually presented as asymp- tomatic, single, nodular, subcutaneous le- sions that occasionally showed ulceration
of the skin. The size varied from less than 2 cm to 7 cm. Recurrences after simple excision were extremely rare. In 1961 FoR- ms & HELWm 4 reported 228 cases from the flies of the Armed Forces Institute of Pathology. The majority, 97 %, occurred in white males and females. These authors strongly advocated the use of the term "pilomatrixoma", reflecting the concept that the cells of this lesion are derived from primitive epidermal germ cells which are differentiating toward hair matrix cells. They considered the lesion to be benign and found only one case report~ in which a malignant degeneration was sufficiently proven. In a total of 600 cases a multiple occurrence of pilomatrixoma was recorded in about 2 %tl.
284 VAN DER WAAL ET AL.
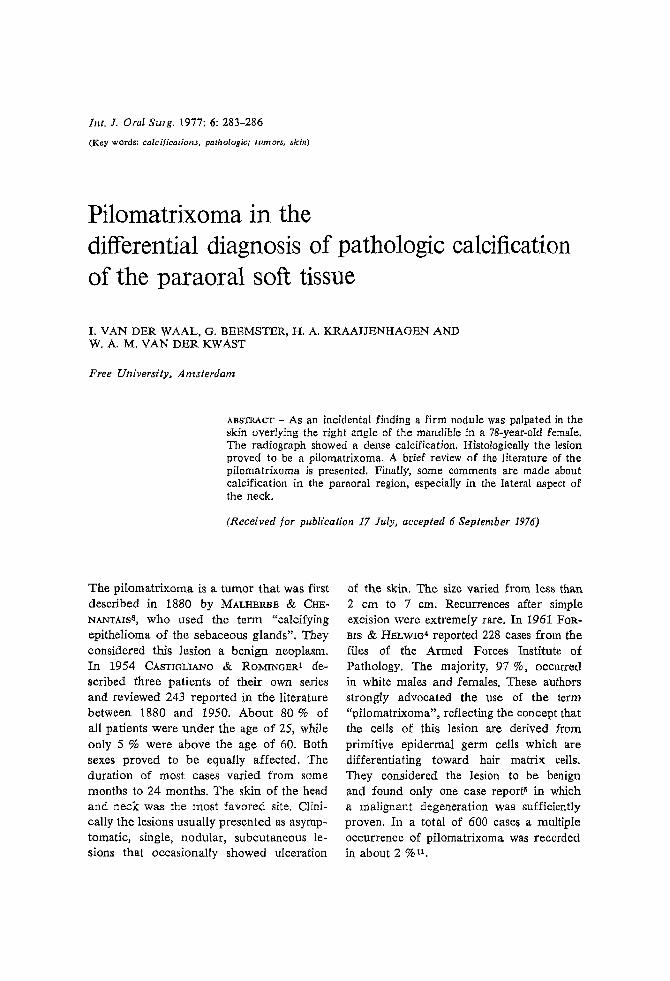
Fig. 1. Panoramic radiograph shows a circum- scribed radiopaque structure at the right angle of the mandible.
In 1972 HARPER a reported the associa- tion of the pilomatrixoma with myotonic muscular dystrophy. In his series of 167 patients with muscular dystrophy, seven were affected by a pilomatrixorna. Accord- ing to HARPER this association probably re- presents a further p[eiotropic effect of the myotonic dystrophy gene. In 1974, CAZERS, OKUN & PEARSON -~ reported 37 new cases, and in 1976, ROTHMAN, KENDALL & BALDI l0 reported a giant pilomatrixoma in the face of a 56-year-old woman.
In 1975 LEVER7 suggested that the rather common ossification in the pilomatrixoma probably results from metaplasia of fibro- blasts into osteoblasts. Calcium-rich "shad- ow" cells seem to act as an inducing factor in this process.
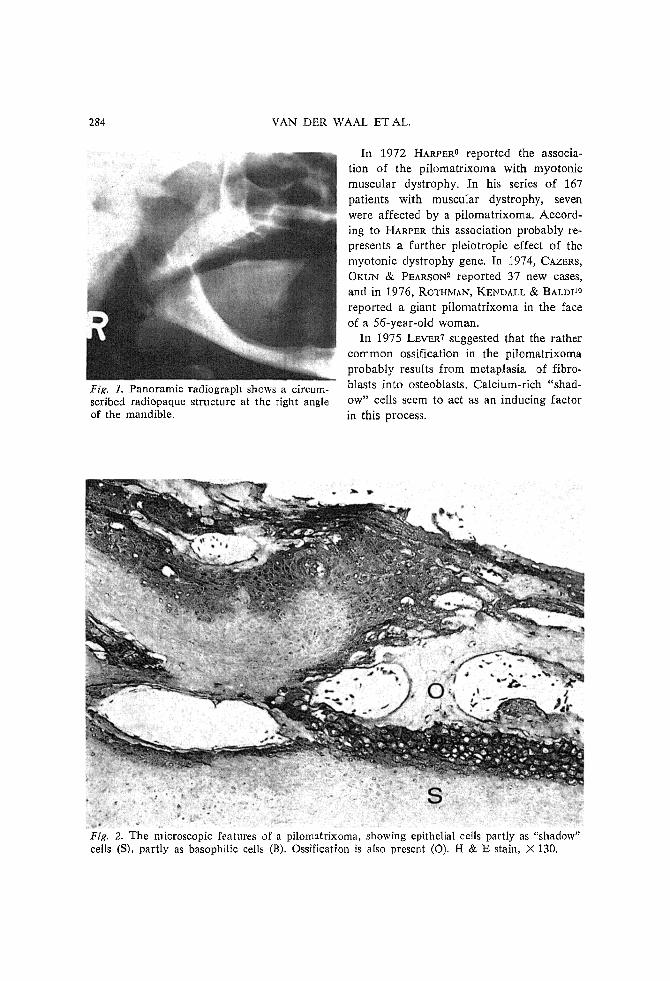
Fig. 2. The microscopic features of a pilomatrixoma, showing epithelial cells partly as "shadow" cells (S), partly as basophilic ceils (B). Ossification is also present (O). H & E stain, X 130.
PILOMATRIXOMA 285
Case report A 78-year-old white female was referred to the Department of Oral Surgery of the Free Uni- versity. On extraoral examination an indura- tion was palpated in the skin just above the right angle of the mandible, The lesion measured about 2 cm in diameter and could be moved freely over the underlying structures. The overlying skin did not show any abnorm- ality and seemed to be somewhat fixed to the lesion, The nodule could not be palpated bi- manually. No similar lesions were noticed else- where in the skin.
The extraoral examination did not show any abnormality. The flow from both the right submandibular gland and the parotkl gland was normal A panoramic radiograph showed an irregular, radiopaque structure at the right angle of the mandible (Fig. 1). The anteropos- tenor view distinctly showed the subcutaneous location of the mass. For academic reasons only, a sialogram of the right parotid gland was made. This clearly demonstrated the extragland- ular location of the lesion. The medical history was essentially negative. Values of routine blood examination were within normal limits, as were the serum calcium and phosphorus levels. The clinical diagnosis was osteoma cutis,
Using local anesthesia the lesion was excised. The healing of the skin wound was uneventful. There were no signs of recurrences 12 months postoperatively.
H I S T O P A T H O L O G Y The tissue was decalcified and stained routinely with hematoxylin-eosin stain. Microscopic examination showed the characteristic aspects of a pilomatrixoma with abundant calcification and ossification (Fig. 2). There were some in- f lammatory changes in the stromal tissue and a very few giant cells, arranged along the epith- elial structures.
Discussion Due to the inc reas ing use of p a n o r a m i c
r ad iog raphs the o ra l su rgeon quite of ten
becomes invo lved in the diagnosis of ab-
n o r m a l calcif ied s t ruc tu res in the upper
neck , especial ly n e a r the ang le o f the
mand ib le . T h e s e s t r u c t u r e s m o s t of ten are
a s y m p t o m a f i c and r ep re sen t ca lc i f ica t ions
in the deepe r l y m p h nodes . A h is tory of
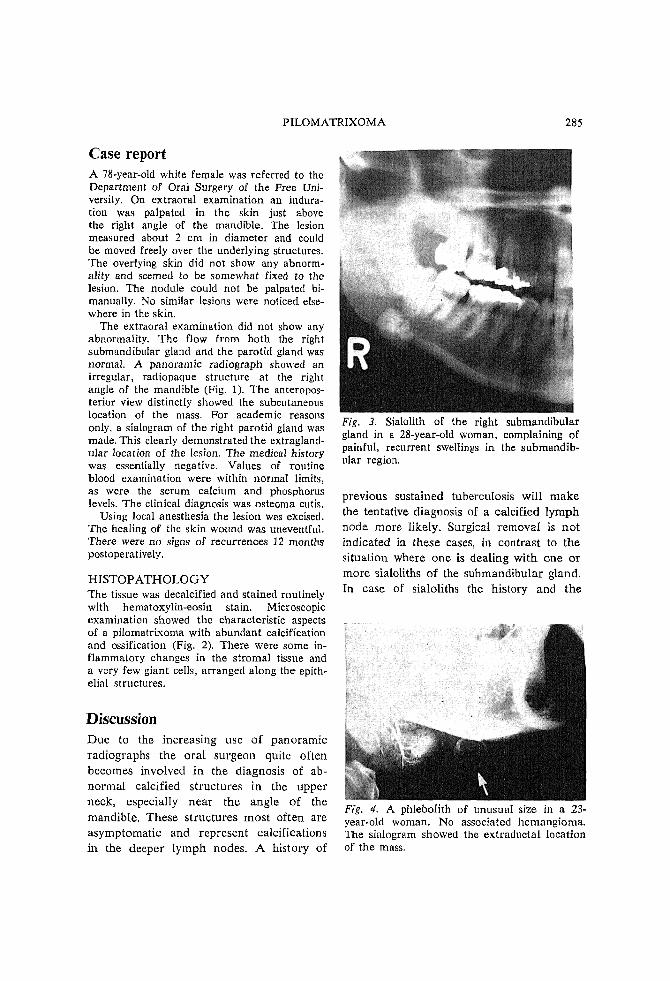
Fig. 3. Sialolith of the right submandibular gland in a 28-year-old woman, complaining of painful, recurrent swellings in the submandib- ular region.
p rev ious sustahaed tuberculos is wil l m a k e
the ten ta t ive d iagnosis of a ca lc i f ied l y m p h
node m o r e l ikely. Surgical r e m o v a l is n o t
ind ica ted in these eases, in con t r a s t to the
s i tua t ion where o n e is dea l ing w i t h one or
more sialoliths of the s u b m a n d i b u l a r gland.
In case of sialoli ths the h i s to ry and t h e
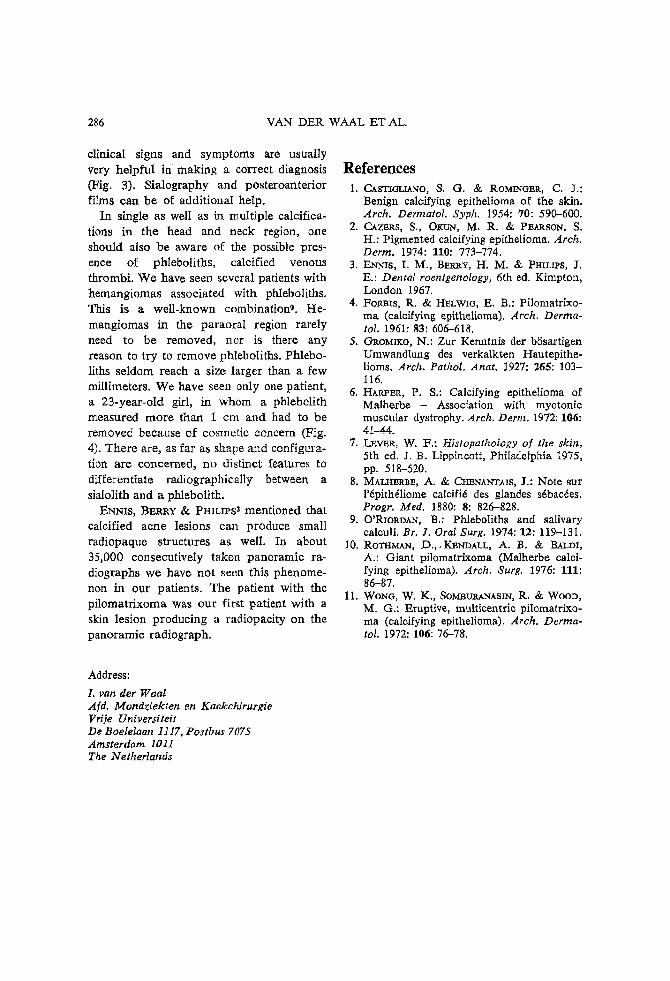
Fig. 4. A phlebolith of unusual size in a 23- year-old woman. No associated hemangioma. The sialogram showed the extraductal location of the mass.
286 VAN DER WAAL ET AL.
clinical signs and symptoms are usually very helpful i n making a correct diagnosis (Fig. 3). Sialography and posteroanterior films earl be of additional help.
In single as well as in multiple calcifica- tions in the head and neck region, one should also be aware of the possible pres- ence of phleboliths, calcified venous thrombi. We have seen several patients with hemangiomas associated with phleboliths. This is a well-known combinationS. He- mangiomas in the paraoral region rarely need to be removed, nor is there any reason to try to remove phleboliths. Phlebo- liths seldom reach a size larger than a few millimeters. We have seen only one patient, a 23-year-old girl, in whom a phlebolith measured more than 1 cm and had to be removed because of cosmetic concern (Fig. 4). There are, as far as shape and configura- tion are concerned, no distinct features to differentiate radiographically between a sialolith and a phlebolith.
~NNIS, BFALRY & PHI~/PS~ mentioned that calcified acne lesions can produce small radiopaque structures as well. In about 35,000 consecutively taken panoramic ra- diographs we have not seen this phenome- non in our patients. The patient with the pilomatfixoma was our first patient with a skin lesion producing a radiopacity on the panoramic radiograph.
References 1. ChSTIOLIANO, S. G. ~; ROMINO~R, C..)',:
Benign calcifying epithelioma of the skin. Arch. Dermatol. Syph. 1954: 70: 590--600.
2. ChZ~RS, S., O~uN, M. R. & PEArtS0N, S. H.: Pigmented calcifying epithelioma. Arch. Derm. 1974: 110: 773-774.
3. ENNIS, I. M., BERI~Y, H. M. & PHILIPS, J. E.: Dental roentgenology, 6th ed. Kimpton, London 1967.
4. Foams, R. & HELWm, E. B.: Pilomatrixo- ma (ealcifyiu~ epithelioma). Arch. Derma- tol. 1961: 83: 606-618.
5. C_mOMIKO, N.: Zur Kenntnis der bhsartigen Umwandlung des verkalkten Hautepithe- lioms. Arch. PathoI. Anat. 1927: 265: 103- 116.
6. HArteart, P. S.: Calcifying epithelioma of M a l h e r b e - Association with myotonic muscular dystrophy. Arch. Derm. 1972: 106: 41-44.
7. I .~v~, W. F.: Histopathotogy of the skin, 5th ed, L B. Lippincott, Philadelphia 1975, pp. 518-520.
8. MALHERBE, A. &; Ct~NANTMS, J.: NoCe sur l'6pithdliome ealcifid des glandes sdbaedes. Progr. Med. 1880: 8: 826-828.
9. O'RIortDAN, B.: Phleboliths and salivary calculi. Br. 1. Oral Surg. 1974: 12: 119-131.
10. I~OTHMAN, D.,. KENDALL, A. B. & BALDI, A.: Giant pilomatrixoma (Malherbe calci- fying epithelioma). Arch. Surg. 1976: 111: 86-87.
11. WoNG, W. K., SOMmraXNASm, R. & WOOD, M. G.: Eruptive, multicentrie pilomatrixo- ma (calcifying epithelioma). Arch. Derma- tol. 1972: 106: 7&78.
Address:
l. van der Waal A/d. Mondzfekten en Kaakchirurgie Vri}e Universiteit De Boelelaan 1117, Postbus 7075 Amsterdam 1011 The Netherlands