physiotherapy in intensive care... an updated systematic review
TRANSCRIPT

CHEST Original ResearchCRITICAL CARE
journal.publications.chestnet.org CHEST / 144 / 3 / SEPTEMBER 2013 825
In most developed countries, physiotherapy is seen as an integral component of the multidisciplinary
management of patients in ICUs. The role of physio-therapy in the ICU and the treatment techniques used by physiotherapists in the ICU vary consider-
ably between units, depending on factors such as the country in which the ICU is located, local tradition, staffi ng levels, and expertise. In 2000, Stiller 1 published a literature review investigating the effectiveness of physiotherapy for adult, intubated patients on mechan-ical ventilation in the ICU, covering a broad range of physiotherapy practice. This concluded that there was only limited evidence concerning the effectiveness of physiotherapy in this setting and identifi ed an urgent need for further research to be conducted to justify the role of physiotherapy in the ICU. The review is frequently cited in articles concerning the role of physiotherapy in the ICU. Given that . 10 years have passed since its publication, what new evidence regard ing the role of physiotherapy in the ICU has emerged? Does this new evidence confi rm the role
Background: Although physiotherapy is frequently provided to patients in the ICU, its role has been questioned. The purpose of this systematic literature review, an update of one published in 2000, was to examine the evidence concerning the effectiveness of physiotherapy for adult, intu-bated patients who are mechanically ventilated in the ICU. Methods: The main literature search was undertaken on PubMed, with secondary searches of MEDLINE, CINAHL, Embase, the Cochrane Library, and the Physiotherapy Evidence Database. Only papers published from 1999 were included. No limitations were placed on study design, intervention type, or outcomes of clinical studies; nonsystematic reviews were excluded. Items were checked for relevance and data extracted from included studies. Marked heterogeneity of design precluded statistical pooling of results and led to a descriptive review. Results: Fifty-fi ve clinical and 30 nonclinical studies were reviewed. The evidence from random-ized controlled trials evaluating the effectiveness of routine multimodality respiratory physio-therapy is confl icting. Physiotherapy that comprises early progressive mobilization has been shown to be feasible and safe, with data from randomized controlled trials demonstrating that it can improve function and shorten ICU and hospital length of stay. Conclusions: Available new evidence, published since 1999, suggests that physiotherapy interven-tion that comprises early progressive mobilization is benefi cial for adult patients in the ICU in terms of its positive effect on functional ability and its potential to reduce ICU and hospital length of stay. These new fi ndings suggest that early progressive mobilization should be implemented as a matter of priority in all adult ICUs and an area of clinical focus for ICU physiotherapists. CHEST 2013; 144(3):825–847
Abbreviations: IMT 5 inspiratory muscle training; LOS 5 length of stay; MH 5 manual hyperinfl ation; NMES 5 neuro-muscular electrical stimulation; RCT 5 randomized controlled/comparative trial; VAP 5 ventilator-associated pneumonia; VH 5 ventilator hyperinfl ation
Physiotherapy in Intensive Care An Updated Systematic Review
Kathy Stiller , PhD
Manuscript received December 5, 2012; revision accepted May 2, 2013 . Affi liations: From the Physiotherapy Department, Royal Adelaide Hospital, Adelaide, SA, Australia. Funding/Support : The author has reported to CHEST that no funding was received for this study . Correspondence to: Kathy Stiller, PhD, Royal Adelaide Hospi-tal, Physiotherapy Department, North Terrace, Adelaide, SA, Australia, 5000; e-mail: [email protected] © 2013 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians. See online for more details. DOI: 10.1378/chest.12-2930
Downloaded From: http://journal.publications.chestnet.org/ by a University of Pittsburgh User on 10/14/2013

826 Original Research
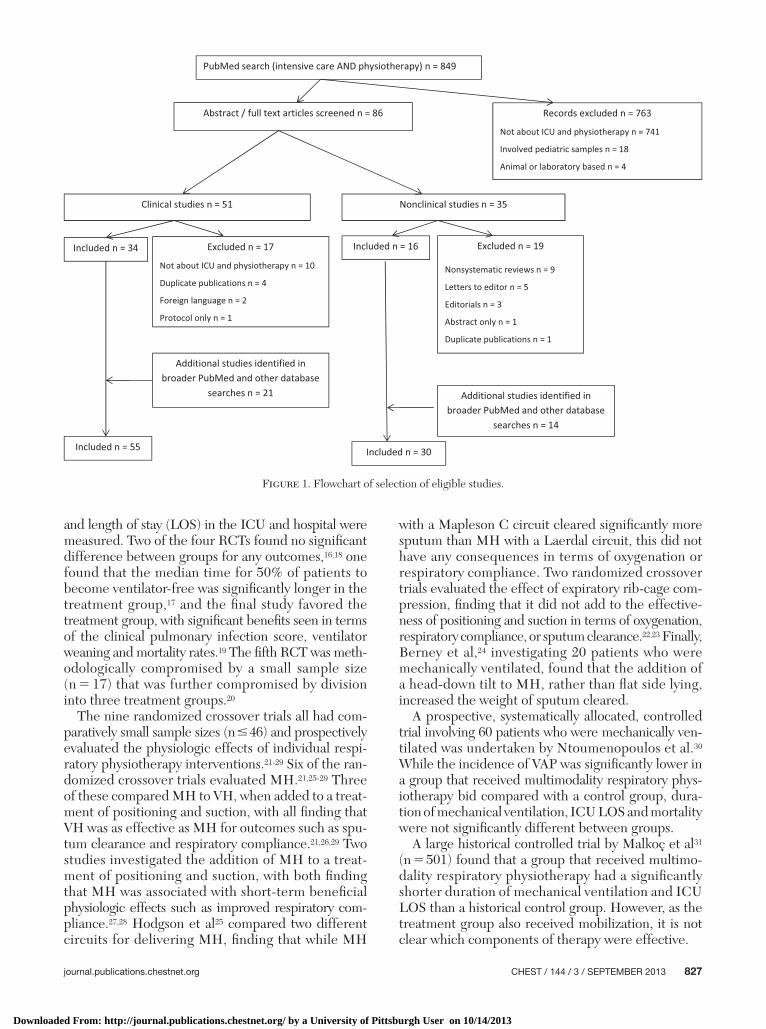
did not study the population and/or intervention of interest ( Fig 1 ).
Systematic Reviews
Twelve systematic literature reviews were identi-fi ed. Their characteristics, including a summary of their results and conclusions, are shown in Table 1 . 4-15 In contrast to the current review, which covers a wide range of ICU physiotherapy practices, these reviews focused on specifi c areas of physiotherapy practice in the ICU, with the most frequent topic being the early mobilization and rehabilitation of patients in the ICU. 4-10 Despite only limited data being available, most con-cluded that early mobilization and rehabilitation are safe and effective in the ICU setting, although further research is required to confi rm and extend its role. 4-10
Clinical Trials: Study and Patient Characteristics
The clinical trials reviewed evaluated a variety of physiotherapy interventions, including multimodality respiratory physiotherapy, mobilization, inspiratory muscle training (IMT), and neuromuscular electrical stimulation (NMES). For the sake of clarity, study fi ndings are presented according to the intervention evaluated.
Multimodality Respiratory Physiotherapy: Eighteen clinical trials were identifi ed that evaluated the effec-tiveness of multimodality respiratory physiotherapy, with the interventions studied including various com-binations of positioning, manual hyperinfl ation (MH), ventilator hyperinfl ation (VH), chest wall vibrations, and rib-cage compression. 16-33 The characteristics and main fi ndings of these 18 studies are shown in Table 2 (sorted according to methodological quality and sam-ple size). There were fi ve RCTs, 16-20 nine randomized crossover trials, 21-29 one systematically allocated con-trolled trial, 30 one historical controlled trial, 31 and two observational studies. 32,33
Four of the fi ve RCTs were well designed and involved samples of at least 101 patients. 16-19 Study populations comprised patients who were intubated and mechan-ically ventilated after cardiac surgery, 16 mechanically ventilated . 48 h, 17,19 or mechanically ventilated with acquired brain injury. 18 Patients were prospectively randomly allocated to a control group (usually receiving standard medical/nursing care) or a treatment group that received additional multimodality respiratory phys-iotherapy (comprising a combination of techniques such as positioning, MH, with or without chest wall vibrations). Frequency of this additional multimodality respiratory physiotherapy was as clinically indicated in two studies, 16,17 bid, 19 and six times a day. 18 Medium-term clinical outcomes such as duration of intubation, incidence of ventilator-associated pneumonia (VAP),
of physiotherapy in the ICU? Does it highlight areas of clinical practice where physiotherapy is most effective?
The objective of this systematic review was to update a summary of the evidence concerning the effective-ness of physiotherapy in the ICU. In keeping with Stiller, 1 this review only considers the management of adult, intubated patients on mechanical ventilation.
Materials and Methods
Search Strategy and Study Selection
The PICOS (population, intervention, comparison, outcome and study design) criteria used in this study were deliberately broad to capture all relevant articles, requiring only that the popu-lation comprised adult (aged � 18 years), intubated, mechanically ventilated patients being cared for in an ICU setting and that a physiotherapy intervention had been evaluated or discussed. No limitations were placed on study outcomes. All relevant clinical articles were included and systematic literature reviews, expert opinion papers, and surveys were also eligible for inclusion. The primary literature search was conducted using the PubMed data-base for articles published from January 1, 1999, to July 31, 2012, using the following search terms: “intensive care” AND “physio-therapy.” Additional searches were undertaken on PubMed using the terms “critical care” or “intensive care” AND “physical therapy,” “therapeutic exercise,” “functional training,” “exercise,” “exercise therapy,” “mobilisation,” “rehabilitation” or “ambulation.” Sec-ondary searches, using the same time limitations and search terms, were undertaken on MEDLINE, CINAHL, Embase, Cochrane Library, and the Physiotherapy Evidence Database. Titles and abstracts generated by the search strategy were assessed for eligi-bility and full-text copies of articles deemed to be potentially rel-evant were retrieved. Duplicate publications were excluded. If relevant articles could not be accessed via the Internet, authors were contacted directly. Given that this was a nonclinical study, institutional review board approval was not sought.
Methodological Quality and Analysis
The methodological quality of randomized controlled or com-parative trials (RCTs) was appraised with reference to the National Health and Medical Research Council Guidelines 2 and Consoli-dated Standards of Reporting Trials (CONSORT) statement . 3 All data were extracted by the author. Marked heterogeneity of study design and outcome measures precluded statistical pooling of results for meta-analysis, hence a descriptive summary of the fi nd-ings is presented.
Results
Literature Search
The initial PubMed literature search identifi ed 849 items published since 1999, with 50 relevant studies (34 clinical, 16 nonclinical) included in the review. An additional 35 relevant studies (21 clinical, 14 nonclinical) were retrieved in a broader PubMed search or from other databases. Thus, in total, 85 new studies (55 clinical, 30 nonclinical) were reviewed. Articles were most often excluded because they
Downloaded From: http://journal.publications.chestnet.org/ by a University of Pittsburgh User on 10/14/2013
journal.publications.chestnet.org CHEST / 144 / 3 / SEPTEMBER 2013 827
and length of stay (LOS) in the ICU and hospital were measured. Two of the four RCTs found no signifi cant difference between groups for any outcomes, 16,18 one found that the median time for 50% of patients to become ventilator-free was signifi cantly longer in the treatment group, 17 and the fi nal study favored the treatment group, with signifi cant benefi ts seen in terms of the clinical pulmonary infection score, ventilator weaning and mortality rates. 19 The fi fth RCT was meth-odologically compromised by a small sample size (n 5 17) that was further compromised by division into three treatment groups. 20
The nine randomized crossover trials all had com-paratively small sample sizes (n � 46) and prospectively evaluated the physiologic effects of individual respi-ratory physiotherapy interventions. 21-29 Six of the ran-domized crossover trials evaluated MH. 21,25-29 Three of these compared MH to VH, when added to a treat-ment of positioning and suction, with all fi nding that VH was as effective as MH for outcomes such as spu-tum clearance and respiratory compliance. 21,26,29 Two studies investigated the addition of MH to a treat-ment of positioning and suction, with both fi nding that MH was associated with short-term benefi cial physiologic effects such as improved respiratory com-pliance. 27,28 Hodgson et al 25 compared two different circuits for delivering MH, fi nding that while MH
with a Mapleson C circuit cleared signifi cantly more sputum than MH with a Laerdal circuit, this did not have any consequences in terms of oxygenation or respiratory compliance. Two randomized crossover trials evaluated the effect of expiratory rib-cage com-pression, fi nding that it did not add to the effective-ness of positioning and suction in terms of oxygenation, respiratory compliance, or sputum clearance. 22,23 Finally, Berney et al, 24 investigating 20 patients who were mechanically ventilated, found that the addition of a head-down tilt to MH, rather than fl at side lying, increased the weight of sputum cleared.
A prospective, systematically allocated, controlled trial involving 60 patients who were mechanically ven-tilated was undertaken by Ntoumenopoulos et al. 30 While the incidence of VAP was signifi cantly lower in a group that received multimodality respiratory phys-iotherapy bid compared with a control group, dura-tion of mechanical ventilation, ICU LOS and mortality were not signifi cantly different between groups.
A large historical controlled trial by Malkoç et al 31 (n 5 501) found that a group that received multimo-dality respiratory physiotherapy had a signifi cantly shorter duration of mechanical ventilation and ICU LOS than a historical control group. However, as the treatment group also received mobilization, it is not clear which components of therapy were effective.
Figure 1. Flowchart of selection of eligible studies.
Downloaded From: http://journal.publications.chestnet.org/ by a University of Pittsburgh User on 10/14/2013

828 Original Research
Tabl
e 1—
Cha
ract
eris
tics
of
Syst
emat
ic L
iter
atu
re R
evie
ws
Stud
yTo
pic
Stud
ies
Rev
iew
ed, N
o.Su
mm
ary
of R
esul
ts, A
utho
rs’ C
oncl
usio
ns
Mob
iliza
tion/
earl
y re
habi
litat
ion
A
dler
and
Mal
one 4
Mob
iliza
tion
of c
ritic
ally
ill p
atie
nts
with
an e
mph
asis
on
func
tiona
l out
com
es a
nd
patie
nt s
afet
y.
15E
vide
nce
from
the
limite
d nu
mbe
r of
stu
dies
that
hav
e ex
amin
ed th
e ea
rly
m
obili
zatio
n of
cri
tical
ly il
l pat
ient
s su
ppor
ts e
arly
mob
iliza
tion
as a
saf
e an
d ef
fect
ive
inte
rven
tion
that
can
hav
e a
sign
ifi ca
nt im
pact
on
func
tiona
l out
com
es.
A
mid
ei 5
Vari
able
s th
at h
ave
been
use
d to
eva
luat
e
phys
iolo
gic
resp
onse
s to
mob
iliza
tion.
17M
ost s
tudi
es th
at h
ave
inve
stig
ated
the
mob
iliza
tion
of c
ritic
ally
ill p
atie
nts
ev
alua
ted
card
iopu
lmon
ary
func
tion.
Fut
ure
stud
ies
eval
uatin
g th
e sa
fety
and
ef
fi cac
y of
mob
iliza
tion
in th
is s
ettin
g sh
ould
mea
sure
mul
tiple
phy
siol
ogic
va
riab
les,
incl
udin
g in
fl am
mat
ory
biom
arke
rs, a
nd o
ther
mea
sure
s of
ph
ysio
logi
c fu
nctio
n, s
uch
as p
ain,
com
fort
, anx
iety
, moo
d, a
nd s
leep
.
Am
idei
6 C
once
pt o
f mob
iliza
tion
in th
e cr
itica
l
care
set
ting.
61M
obili
zatio
n ca
n be
defi
ned
as
an in
terd
isci
plin
ary,
goa
l-dir
ecte
d th
erap
y ai
med
at fa
cilit
atin
g m
ovem
ent a
nd im
prov
ing
outc
omes
in c
ritic
ally
ill p
atie
nts.
The
co
ncep
t of m
obili
zatio
n ne
eds
furt
her
defi n
ition
with
res
pect
to fa
ctor
s su
ch a
s th
e ac
tiviti
es it
com
pris
es, t
heir
qua
ntity
, int
ensi
ty, d
urat
ion,
and
freq
uenc
y,
and
inte
rdis
cipl
inar
y ro
les.
C
hoi e
t al 7
Mob
ility
inte
rven
tions
to im
prov
e ou
tcom
es
in
pat
ient
s un
derg
oing
pro
long
ed
mec
hani
cal v
entil
atio
n.
10T
he s
tudi
es r
evie
wed
sup
port
the
abili
ty o
f mob
ility
inte
rven
tions
to im
prov
e th
e
outc
omes
of p
atie
nts
rece
ivin
g pr
olon
ged
mec
hani
cal v
entil
atio
n, b
ut th
ere
is
limite
d ev
iden
ce o
n ho
w to
bes
t acc
ompl
ish
this
goa
l.
O’C
onno
r an
d W
alsh
am 8
Wor
ldw
ide
avai
labi
lity
of m
obili
zatio
n
ther
apy
in I
CU
and
its
role
.94
a T
here
is m
arke
d va
riab
ility
bet
wee
n co
untr
ies
in th
e av
aila
bilit
y an
d pr
escr
iptio
n
of m
obili
zatio
n th
erap
y in
the
ICU
set
ting,
with
rou
tine
mob
iliza
tion
ther
apy
leas
t lik
ely
to b
e av
aila
ble
in th
e U
nite
d St
ates
. The
dat
a in
sup
port
of
mob
iliza
tion
ther
apy
for
criti
cally
ill p
atie
nts,
whi
le o
f a lo
w le
vel o
f evi
denc
e,
are
subs
tant
ial.
Thi
s ju
stifi
es a
par
adig
m s
hift
in a
ttitu
des
tow
ard
PT a
nd th
e pr
even
tion
of c
ritic
al il
lnes
s w
eakn
ess.
T
hom
as 9
Reh
abili
tatio
n of
the
patie
nt w
ith
cr
itica
l illn
ess.
33 a
The
evi
denc
e av
aila
ble
rega
rdin
g th
e ef
fect
iven
ess
of p
hysi
cal t
rain
ing
with
in
th
e IC
U e
nvir
onm
ent i
s lim
ited
to p
atie
nts
with
long
-ter
m r
espi
rato
ry fa
ilure
w
ho m
ay n
ot b
e re
pres
enta
tive
of a
gen
eral
cri
tical
ly il
l pop
ulat
ion.
T
hom
as 10
E
ffec
t of p
hysi
cal r
ehab
ilita
tion
com
men
ced
im
med
iate
ly o
n IC
U a
dmis
sion
com
pare
d w
ith d
elay
ed r
ehab
ilita
tion.
46 a
Whe
n th
e re
habi
litat
ion
of c
ritic
ally
ill p
atie
nts
is c
omm
ence
d ea
rly
duri
ng th
eir
IC
U a
dmis
sion
, it l
eads
to a
hig
her
rate
of P
T c
onsu
ltatio
n, a
nd p
atie
nt-r
elat
ed
bene
fi ts
are
seen
, suc
h as
dec
reas
ed ti
me
to a
chie
ve a
ctiv
ity m
ilest
ones
, im
prov
ed fu
nctio
nal o
utco
mes
at I
CU
and
hos
pita
l dis
char
ge, a
nd r
educ
ed d
irec
t pa
tient
cos
ts. E
arly
reh
abili
tatio
n of
the
criti
cally
ill p
atie
nt, l
ed b
y PT
s, h
as th
e po
tent
ial t
o dr
amat
ical
ly in
fl uen
ce r
ecov
ery
and
func
tiona
l out
com
es in
this
vu
lner
able
pat
ient
gro
up.
Res
pira
tory
tech
niqu
es
Clin
i and
Am
bros
ino 11
R
atio
nale
and
eff
ectiv
enes
s of
spe
cifi c
PT
inte
rven
tions
and
use
of w
eani
ng p
roto
cols
fo
r pa
tient
s in
a r
espi
rato
ry I
CU
.
81 a
Evi
denc
e su
ppor
ting
PT R
xs fo
r pa
tient
s in
the
ICU
is li
mite
d du
e to
the
lack
of lo
ng-t
erm
stu
dies
. Whi
le th
ere
is s
tron
g ev
iden
ce to
sup
port
the
use
of
ther
apis
t-dr
iven
wea
ning
pro
toco
ls, f
urth
er s
tudi
es w
ith la
rger
sam
ple
size
s ar
e ne
eded
to e
valu
ate
the
effe
ctiv
enes
s of
mos
t PT
tech
niqu
es in
the
ICU
. (Con
tinu
ed)
Downloaded From: http://journal.publications.chestnet.org/ by a University of Pittsburgh User on 10/14/2013

journal.publications.chestnet.org CHEST / 144 / 3 / SEPTEMBER 2013 829
Stud
yTo
pic
Stud
ies
Rev
iew
ed, N
o.Su
mm
ary
of R
esul
ts, A
utho
rs’ C
oncl
usio
ns
Pa
ulus
et a
l 12
Ben
efi ts
and
ris
ks o
f MH
in c
ritic
ally
ill p
atie
nts.
19M
H r
esul
ts in
sho
rt-t
erm
ben
efi c
ial e
ffec
ts o
n ph
ysio
logi
c en
dpoi
nts
such
as
re
spir
ator
y co
mpl
ianc
e, o
xyge
natio
n, a
nd a
irw
ay c
lear
ance
. How
ever
, its
eff
ect
on b
road
er o
utco
mes
, suc
h as
dur
atio
n of
mec
hani
cal v
entil
atio
n an
d IC
U L
OS,
is
unk
now
n. M
H h
as b
een
asso
ciat
ed w
ith s
ide
effe
cts,
alb
eit i
nfre
quen
tly.
App
ropr
iate
ly p
ower
ed a
nd m
etho
dolo
gica
lly s
ound
stu
dies
are
nee
ded
befo
re
it ca
n be
rec
omm
ende
d fo
r ro
utin
e us
e.O
ther
topi
cs
Elli
ott e
t al 13
O
bser
vatio
nal a
nd fu
nctio
nal a
sses
smen
t
inst
rum
ents
use
d to
ass
ess
patie
nts
in th
e IC
U,
post
-IC
U, a
nd p
osth
ospi
taliz
atio
n.
107 a
Stud
ies
have
use
d m
any
diff
eren
t out
com
es to
mea
sure
the
func
tion
of
IC
U s
urvi
vors
, inc
ludi
ng m
uscl
e st
reng
th, f
unct
iona
l tes
ts, a
nd h
ealth
-rel
ated
qu
ality
of l
ife. I
n ge
nera
l, th
e se
nsiti
vity
and
val
idity
of t
hese
inst
rum
ents
for
use
with
sur
vivo
rs o
f a c
ritic
al il
lnes
s ha
s no
t yet
bee
n es
tabl
ishe
d.
Han
ekom
et a
l 14
Iden
tify
whi
ch o
utco
mes
sho
uld
be m
easu
red
in
the
adul
t cri
tical
car
e en
viro
nmen
t and
w
hich
out
com
es P
Ts a
re c
urre
ntly
incl
udin
g in
res
earc
h re
port
s.
35R
esea
rch
that
has
inve
stig
ated
the
effi c
acy
of P
T in
IC
U h
as p
rim
arily
mea
sure
d
phys
iolo
gic
vari
able
s or
pro
vide
d de
scri
ptio
ns o
f cur
rent
pra
ctic
e, w
ithou
t lin
king
thes
e to
bro
ader
out
com
es s
uch
as fu
nctio
nal s
tatu
s an
d he
alth
-rel
ated
qu
ality
of l
ife. F
urth
er w
ork
is n
eede
d to
dev
elop
and
refi
ne
patie
nt-c
ente
red
and
econ
omic
mea
sure
men
ts th
at w
ill b
e su
ffi ci
ently
sen
sitiv
e to
be
able
to
mea
sure
the
effe
ct o
f PT
ser
vice
pro
visi
on in
IC
U.
H
ellw
eg 15
E
ffec
tiven
ess
of P
T a
nd O
T fo
r pa
tient
s in
the
IC
U w
ith tr
aum
atic
bra
in in
jury
.34
a D
ata
conc
erni
ng th
e ef
fect
iven
ess
of P
T a
nd O
T fo
r pa
tient
s in
the
ICU
with
trau
mat
ic b
rain
inju
ry a
re v
ery
limite
d, m
akin
g it
impo
ssib
le to
off
er c
lear
, ev
iden
ce-b
ased
rec
omm
enda
tions
. Res
pira
tory
PT
has
not
bee
n sh
own
to b
e ef
fect
ive
for
the
prev
entio
n or
Rx
of V
AP.
The
effi
cacy
of o
ther
PT
and
OT
in
terv
entio
ns m
ust s
till b
e de
mon
stra
ted.
LO
S 5
leng
th o
f sta
y; M
H 5
man
ual h
yper
infl a
tion;
OT
5 o
ccup
atio
nal t
hera
py; P
T 5
phy
siot
hera
py o
r ph
ysic
al th
erap
y; R
x 5 tr
eatm
ent;
VAP
5 ve
ntila
tor-
asso
ciat
ed p
neum
onia
. a I
ndic
ates
the
num
ber
of a
rtic
les
in th
e re
fere
nce
list (
num
ber
of s
tudi
es in
clud
ed in
rev
iew
not
spe
cifi c
ally
sta
ted)
.
Tabl
e 1—
Con
tinu
ed
Downloaded From: http://journal.publications.chestnet.org/ by a University of Pittsburgh User on 10/14/2013

830 Original Research
Tabl
e 2—
Cha
ract
eris
tics
of
Stu
dies
Eva
luat
ing
Mu
ltim
odal
ity
Res
pira
tory
Phy
siot
hera
py
Stud
yPa
rtic
ipan
ts, N
o.,
Type
Inte
rven
tion
Out
com
esR
esul
tsSu
mm
ary
of A
utho
rs’ C
oncl
usio
ns
Pros
pect
ive,
rand
omiz
ed,
co
ntro
lled/
com
para
tive
tria
ls
Patm
an e
t al 16
21
0, in
tuba
ted,
m
echa
nica
lly
vent
ilate
d,
post
-car
diac
su
rger
y.
Con
trol
: sta
ndar
d m
edic
al/n
ursi
ng c
are.
Dur
atio
n of
intu
batio
n,
ICU
and
hos
pita
l LO
S,
inci
denc
e of
pos
tope
rativ
e pu
lmon
ary
com
plic
atio
ns.
No
sign
ifi ca
nt d
iffer
ence
bet
wee
n gr
oups
for
any
outc
ome.
For
rou
tine,
unc
ompl
icat
ed c
ardi
ac
surg
ery
subj
ects
, the
pro
visi
on o
f PT
in
terv
entio
ns d
urin
g th
e po
stop
erat
ive
intu
batio
n pe
riod
did
not
impr
ove
outc
omes
.
Rx:
as
for
cont
rol p
lus
PT
as in
dica
ted,
incl
udin
g po
sitio
ning
, MH
, suc
tion.
Te
mpl
eton
and
Pal
azzo
17
180,
intu
bate
d,
mec
hani
cally
ve
ntila
ted
. 4
8 h.
Con
trol
: sta
ndar
d m
edic
al/n
ursi
ng c
are.
Tim
e to
bec
ome
vent
ilato
r-fr
ee,
ICU
and
hos
pita
l mor
talit
y,
ICU
LO
S.
Med
ian
time
for
50%
to b
ecom
e ve
ntila
tor-
free
sig
nifi c
antly
long
er
in R
x gr
oup.
No
sign
ifi ca
nt
diff
eren
ce b
etw
een
grou
ps fo
r an
y ot
her
outc
ome.
Stan
dard
car
e is
at l
east
as
effe
ctiv
e as
ch
est P
T in
pat
ient
s re
quir
ing
mec
hani
cal v
entil
atio
n .
48
h.R
x: a
s fo
r co
ntro
l plu
s re
spir
ator
y PT
as
indi
cate
d,
incl
udin
g po
sitio
ning
, MH
, ch
est w
all v
ibra
tions
, suc
tion.
Pa
tman
et a
l 18
144,
intu
bate
d,
mec
hani
cally
ve
ntila
ted
. 2
4 h,
acq
uire
d br
ain
inju
ry.
Con
trol
: sta
ndar
d m
edic
al/n
ursi
ng c
are.
Inci
denc
e of
VA
P, d
urat
ion
of m
echa
nica
l ven
tilat
ion,
IC
U a
nd h
ospi
tal L
OS,
C
PIS
scor
es, P
a o 2 /F
io 2 .
No
sign
ifi ca
nt d
iffer
ence
bet
wee
n gr
oups
for
any
outc
ome.
A r
egul
ar r
espi
rato
ry P
T r
egim
en in
ad
ditio
n to
rou
tine
med
ical
/nur
sing
ca
re d
id n
ot s
igni
fi can
tly d
ecre
ase
the
inci
denc
e of
VA
P, d
urat
ion
of
mec
hani
cal v
entil
atio
n or
IC
U L
OS
in a
dults
with
acq
uire
d br
ain
inju
ry.
Rx:
as
for
cont
rol p
lus
resp
irat
ory
PT, i
nclu
ding
po
sitio
ning
, MH
, suc
tion,
6
times
/d.
Pa
ttans
hetty
and
Gau
de 19
101
, int
ubat
ed,
mec
hani
cally
ve
ntila
ted
. 4
8 h.
Con
trol
: MH
and
suc
tion
bid.
CPI
S sc
ore,
mor
talit
y,
wea
ning
suc
cess
, dur
atio
n of
intu
batio
n, I
CU
LO
S.
Red
uctio
n in
CPI
S sc
ore
sign
ifi ca
ntly
gr
eate
r in
Rx
grou
p. W
eani
ng s
ucce
ss
sign
ifi ca
ntly
hig
her
in R
x gr
oup.
M
orta
lity
sign
ifi ca
ntly
low
er in
Rx
grou
p. N
o si
gnifi
cant
diff
eren
ce
betw
een
grou
ps fo
r du
ratio
n of
in
tuba
tion
or I
CU
LO
S.
Mul
timod
ality
res
pira
tory
PT
bid
de
crea
sed
CPI
S sc
ores
, sug
gest
ing
a de
crea
se in
VA
P an
d m
orta
lity
rate
s.R
x: a
s fo
r co
ntro
l plu
s po
sitio
ning
, che
st w
all
vibr
atio
ns.
B
arke
r an
d A
dam
s 20
17, i
ntub
ated
, m
echa
nica
lly
vent
ilate
d, A
LI.
Gro
up 1
: sup
ine
30°
head
-up,
3-
min
pre
oxyg
enat
ion
(F io
2 5 1
), su
ctio
n.
Pa o
2 , Pa
co 2 ,
dyna
mic
re
spir
ator
y co
mpl
ianc
e,
peak
air
way
pre
ssur
e,
HR
, BP,
S vo
2 bef
ore
and
10-,
30-,
and
60-m
in
post
-Rx.
Sign
ifi ca
nt c
hang
es o
bser
ved
in P
a co
2 an
d co
mpl
ianc
e ov
er ti
me
for
all t
hree
gr
oups
(Pa c
o 2 i
ncre
ased
, com
plia
nce
decr
ease
d 10
-min
pos
t-R
x). P
a o 2 /F
io 2
and
S vo
2 did
not
sig
nifi c
antly
cha
nge
in a
ny g
roup
. S vo
2 was
sig
nifi c
antly
lo
wer
in g
roup
2. H
R a
nd B
P sh
owed
si
gnifi
cant
, but
not
clin
ical
ly im
port
ant,
chan
ges
over
tim
e.
Dis
conn
ectio
n of
pat
ient
s w
ith A
LI
from
m
echa
nica
l ven
tilat
ion
for
PT R
x ca
n re
sult
in s
igni
fi can
t der
ecru
itmen
t of t
he
lung
s an
d al
tere
d ph
ysio
logy
. The
use
of
MH
doe
s no
t app
ear
to o
verr
ide
the
loss
of P
EE
P an
d th
e de
recr
uitm
ent
effe
cts.
Gro
up 2
: as
for
grou
p 1,
then
po
sitio
ned
(L a
nd R
fl at
si
de ly
ing)
, suc
tion.
Gro
up 3
: as
for
grou
p 2,
pl
us M
H.
(Con
tinu
ed)
Downloaded From: http://journal.publications.chestnet.org/ by a University of Pittsburgh User on 10/14/2013

journal.publications.chestnet.org CHEST / 144 / 3 / SEPTEMBER 2013 831
Tabl
e 2—
Con
tinu
ed
Stud
yPa
rtic
ipan
ts, N
o.,
Type
Inte
rven
tion
Out
com
esR
esul
tsSu
mm
ary
of A
utho
rs’ C
oncl
usio
ns
Pros
pect
ive,
rand
omiz
ed,
cros
sove
r tr
ials
D
enni
s et
al 21
46
, int
ubat
ed,
mec
hani
cally
ve
ntila
ted,
at
elec
tasi
s or
co
nsol
idat
ion
on C
XR
.
Con
trol
: pos
ition
ing,
VH
, ch
est-
wal
l vib
ratio
ns,
suct
ion.
Sput
um w
eigh
t, V t
, HR
, M
AP,
dyn
amic
res
pira
tory
co
mpl
ianc
e, a
irw
ay
pres
sure
, Pa o
2 /F io
2 bef
ore,
im
med
iate
ly a
nd 3
0-m
in
post
-Rx.
Sign
ifi ca
ntly
hig
her
airw
ay p
ress
ure
with
MH
than
VH
. No
sign
ifi ca
nt
diff
eren
ce b
etw
een
Rxs
for
othe
r ou
tcom
es.
VH
was
as
safe
and
eff
ectiv
e du
ring
re
spir
ator
y PT
Rx
as M
H, w
hen
appl
ied
with
the
sam
e pa
ram
eter
s and
pre
caut
ions
. V
H h
as p
oten
tial a
dvan
tage
s ov
er M
H,
the
bigg
est b
eing
that
no
vent
ilato
r circ
uit
disc
onne
ctio
n is
requ
ired.
Rx:
as
for
cont
rol e
xcep
t MH
no
t VH
.
U
noki
et a
l 22
31, i
ntub
ated
, lik
ely
to
requ
ire
mec
hani
cal
vent
ilatio
n .
48
h.
Con
trol
: pos
ition
ing,
suc
tion.
Pa o
2 /F io
2 , Pa
co 2 ,
dyna
mic
re
spir
ator
y co
mpl
ianc
e,
sput
um w
eigh
t bef
ore
and
25-m
in p
ost-
Rx.
No
sign
ifi ca
nt d
iffer
ence
bet
wee
n R
xs fo
r an
y ou
tcom
e. N
o si
gnifi
cant
di
ffer
ence
see
n fr
om p
re- t
o po
st-R
x fo
r an
y ou
tcom
e.
The
rou
tine
use
of r
ib-c
age
com
pres
sion
is
not
rec
omm
ende
d in
a g
ener
al
popu
latio
n of
mec
hani
cally
ven
tilat
ed
patie
nts.
Rx:
as
for
cont
rol p
lus
5-m
in e
xpir
ator
y ri
b-ca
ge
com
pres
sion
pre
suct
ion.
G
enc
et a
l 23
22, i
ntub
ated
, m
echa
nica
lly
vent
ilate
d.
Con
trol
: pos
ition
ing,
5-m
in
MH
, suc
tion.
Pa o
2 /F io
2 , Pa
co 2 ,
stat
ic
resp
irat
ory
com
plia
nce,
sp
utum
wei
ght,
V t , H
R,
MA
P be
fore
and
5- a
nd
20-m
in p
ost-
Rx.
No
sign
ifi ca
nt d
iffer
ence
bet
wee
n R
xs
for
any
outc
ome.
Com
plia
nce
and
V t s
igni
fi can
tly in
crea
sed
from
pr
e- to
pos
t-R
x. N
o si
gnifi
cant
ch
ange
in o
ther
out
com
es.
The
rou
tine
use
of r
ib-c
age
com
pres
sion
du
ring
MH
is n
ot r
ecom
men
ded
in
a ge
nera
l pop
ulat
ion
of m
echa
nica
lly
vent
ilate
d pa
tient
s.R
x: a
s fo
r co
ntro
l plu
s ex
pira
tory
rib
-cag
e co
mpr
essi
on d
urin
g M
H.
B
erne
y et
al 24
20
, int
ubat
ed,
mec
hani
cally
ve
ntila
ted.
Con
trol
: sid
e ly
ing
fl at,
MH
, su
ctio
n.Sp
utum
wei
ght,
PEF
R
duri
ng M
H, s
tatic
re
spir
ator
y co
mpl
ianc
e be
fore
and
imm
edia
tely
po
st-R
x.
Sign
ifi ca
ntly
mor
e sp
utum
and
hig
her
PEF
R d
urin
g R
x w
ith h
ead-
dow
n til
t. C
ompl
ianc
e si
gnifi
cant
ly
impr
oved
ove
r tim
e, n
o si
gnifi
cant
di
ffer
ence
bet
wee
n R
xs.
The
hea
d-do
wn
tilt p
ositi
on s
houl
d be
co
nsid
ered
whe
n th
e pr
imar
y ai
m
of R
x is
spu
tum
rem
oval
for
intu
bate
d,
mec
hani
cally
ven
tilat
ed p
atie
nts.
Rx:
as
for
cont
rol b
ut s
ide
lyin
g in
hea
d-do
wn
tilt.
H
odgs
on e
t al 25
20
, int
ubat
ed,
mec
hani
cally
ve
ntila
ted.
Rx
1: p
ositi
onin
g, M
H w
ith
Map
leso
n C
cir
cuit,
suc
tion.
Sput
um w
eigh
t, st
atic
re
spira
tory
com
plia
nce,
V t ,
Pa
o 2 /F
io 2 ,
Pa co
2 bef
ore,
30
-, an
d 60
-min
pos
t-R
x.
MH
with
Map
leso
n C
cir
cuit
clea
red
sign
ifi ca
ntly
mor
e sp
utum
. No
sign
ifi ca
nt d
iffer
ence
bet
wee
n R
xs
for
othe
r ou
tcom
es.
Mor
e se
cret
ions
wer
e cl
eare
d us
ing
the
Map
leso
n C
com
pare
d w
ith th
e L
aerd
al c
ircu
it; h
owev
er, t
his
had
no
cons
eque
nce
in te
rms
of o
xyge
natio
n.R
x 2:
as
for
Rx
1 ex
cept
MH
w
ith L
aerd
al c
ircu
it.
Ber
ney
and
Den
ehy 26
20
, int
ubat
ed,
mec
hani
cally
ve
ntila
ted.
Rx
1: p
ositi
onin
g, M
H,
suct
ion.
Sput
um w
eigh
t, st
atic
re
spir
ator
y co
mpl
ianc
e be
fore
, im
med
iate
ly
and
30-m
in p
ost-
Rx.
No
sign
ifi ca
nt d
iffer
ence
bet
wee
n R
xs
in s
putu
m w
eigh
t or
com
plia
nce.
C
ompl
ianc
e si
gnifi
cant
ly im
prov
ed
afte
r bo
th R
xs.
VH
was
as
effe
ctiv
e as
MH
in s
putu
m
clea
ranc
e an
d im
prov
ing
resp
irat
ory
com
plia
nce.
Rx
2: a
s fo
r R
x 1
exce
pt V
H.
H
odgs
on e
t al 27
18
, int
ubat
ed,
mec
hani
cally
ve
ntila
ted,
lung
co
llaps
e an
d/or
co
nsol
idat
ion
on C
XR
, Pa
o 2 /F io
2 , 35
0.
Con
trol
: pos
ition
ing,
suc
tion.
Stat
ic r
espi
rato
ry c
ompl
ianc
e,
Pa o
2 /F io
2 , Pa
co 2 ,
sput
um
wei
ght,
HR
, MA
P be
fore
, im
med
iate
ly a
nd 2
0-m
in
post
-Rx.
Sign
ifi ca
ntly
gre
ater
incr
ease
in
com
plia
nce
and
sput
um w
eigh
t for
M
H R
x. I
ncre
ase
in c
ompl
ianc
e se
en
imm
edia
tely
and
20-
min
pos
t-R
x. N
o si
gnifi
cant
diff
eren
ce b
etw
een
Rxs
fo
r ot
her
outc
omes
.
Res
pira
tory
com
plia
nce
and
sput
um
clea
ranc
e w
ere
impr
oved
by
the
addi
tion
of M
H to
a R
x of
pos
ition
ing
and
suct
ioni
ng w
ithou
t com
prom
ise
to
card
iova
scul
ar s
tabi
lity
or g
as e
xcha
nge.
Rx:
as
for
cont
rol p
lus
MH
.
(Con
tinu
ed)
Downloaded From: http://journal.publications.chestnet.org/ by a University of Pittsburgh User on 10/14/2013

832 Original Research
Stud
yPa
rtic
ipan
ts, N
o.,
Type
Inte
rven
tion
Out
com
esR
esul
tsSu
mm
ary
of A
utho
rs’ C
oncl
usio
ns
C
hoi a
nd J
ones
28
15, i
ntub
ated
, m
echa
nica
lly
vent
ilate
d, V
AP.
Con
trol
: sup
ine,
suc
tion.
Stat
ic r
espi
rato
ry c
ompl
ianc
e,
airw
ay r
esis
tanc
e be
fore
, im
med
iate
ly a
nd 3
0-m
in
post
-Rx.
Sign
ifi ca
ntly
gre
ater
incr
ease
in
com
plia
nce
for
MH
Rx.
Sig
nifi c
ant
decr
ease
in a
irw
ay r
esis
tanc
e 30
-min
po
st-M
H R
x bu
t not
con
trol
Rx.
Suct
ion
alon
e di
d no
t cau
se d
eter
iora
tion
in c
ompl
ianc
e an
d ai
rway
res
ista
nce
and
can
prob
ably
be
used
saf
ely
in p
atie
nts
with
VA
P. T
he a
dditi
on o
f MH
impr
oved
re
spir
ator
y m
echa
nics
com
pare
d w
ith
suct
ion
alon
e.
Rx:
as
for
cont
rol p
lus
MH
.
Sa
vian
et a
l 29
14, i
ntub
ated
, m
echa
nica
lly
vent
ilate
d.
Rx
1: p
ositi
onin
g, M
H,
suct
ion.
PEF
R, V
t , P
a o 2 /F
io 2 ,
stat
ic
resp
irato
ry c
ompl
ianc
e, H
R,
MA
P, s
putu
m w
eigh
t, c
o 2
befo
re, i
mm
edia
tely
and
30
-min
pos
t-R
x.
Sign
ifi ca
ntly
hig
her
PEF
R w
ith M
H.
Sign
ifi ca
ntly
hig
her
V t w
ith V
H.
co 2
sign
ifi ca
ntly
diff
eren
t bet
wee
n R
xs
(upw
ard
tren
d M
H, d
ownw
ard
tren
d V
H).
No
sign
ifi ca
nt d
iffer
ence
be
twee
n R
xs fo
r ot
her
outc
omes
.
VH
pro
mot
ed g
reat
er im
prov
emen
ts in
re
spira
tory
mec
hani
cs w
ith le
ss m
etab
olic
di
stur
banc
e th
an M
H. O
ther
var
iabl
es
such
as s
putu
m p
rodu
ctio
n, h
emod
ynam
ics
and
oxyg
enat
ion
wer
e af
fect
ed s
imila
rly
by b
oth
tech
niqu
es.
Rx
2: a
s fo
r R
x 1
exce
pt V
H.
Pros
pect
ive,
syst
emat
ical
ly
allo
cate
d,
cont
rolle
d tr
ial
N
toum
enop
oulo
s et a
l 30
60, i
ntub
ated
, m
echa
nica
lly
vent
ilate
d �
48
h.
Con
trol
: sid
e ly
ing,
suc
tion
as
requ
ired
.In
cide
nce
of V
AP,
CPI
S sc
ore,
du
ratio
n of
mec
hani
cal
vent
ilatio
n, I
CU
LO
S,
ICU
and
28-
d m
orta
lity.
Sign
ifi ca
ntly
low
er in
cide
nce
of V
AP
and
CPI
S sc
ore
in R
x gr
oup.
No
sign
ifi ca
nt d
iffer
ence
bet
wee
n gr
oups
for
othe
r ou
tcom
es.
Res
pira
tory
PT
was
inde
pend
ently
as
soci
ated
with
a r
educ
tion
in V
AP.
Rx:
pos
ition
ing,
exp
irato
ry
ches
t wal
l vib
ratio
ns,
suct
ion,
bid
.Pr
ospe
ctiv
e,
hi
stor
ical
co
ntro
lled
tria
l
Mal
koç
et a
l 31
510,
intu
bate
d,
mec
hani
cally
ve
ntila
ted.
Con
trol
(his
tori
cal):
sta
ndar
d nu
rsin
g ca
re.
Dur
atio
n of
mec
hani
cal
vent
ilatio
n, I
CU
LO
S.Si
gnifi
cant
ly s
hort
er d
urat
ion
of
mec
hani
cal v
entil
atio
n an
d IC
U
LO
S in
Rx
grou
p.
PT c
an r
educ
e th
e pe
riod
of R
x re
quir
ed
in I
CU
.R
x: p
ositi
onin
g, p
ercu
ssio
n,
vibr
atio
n, c
ough
ing,
dee
p br
eath
ing,
suc
tion,
bed
ex
erci
ses,
mob
iliza
tion
(not
des
crib
ed),
bid,
5
d/w
k.(C
onti
nued
)
Tabl
e 2—
Con
tinu
ed
Downloaded From: http://journal.publications.chestnet.org/ by a University of Pittsburgh User on 10/14/2013

journal.publications.chestnet.org CHEST / 144 / 3 / SEPTEMBER 2013 833
From the two prospective observational studies, Thomas et al 32 found that lateral positioning had no signifi cant effect on oxygenation of 34 patients on mechanical ventilation and Clarke et al, 33 studying 25 patients on mechanical ventilation, reported that manual hyperventilation can result in higher infl ation pressures in patients with susceptible lungs.
Mobilization: For the purposes of this review, the definition of mobilization provided by Stiller 1 has been used, whereby mobilization is a broad term that encompasses active limb exercises, actively moving or turning in bed, sitting on the edge of the bed, sitting out of bed in a chair (via mechanical lifting machines, slide board, or standing transfer), standing, and walking. Twenty-six clinical trials were identifi ed that evaluated the use of mobilization interventions. 34-59 Table 3 summarizes their characteristics. There were three RCTs, 34-36 fi ve nonrandomized controlled trials, 37-41 one historical controlled study, 42 and 17 observational studies. 43-59
The largest prospective RCT, by Schweickert et al, 34 involved 104 patients who had been mechanically ventilated for , 72 h and were likely to require venti-lation for a further 24 h. The patients were randomly allocated to receive daily sedative interruption fol-lowed by therapy that concentrated on mobilization activities (eg, range of motion exercises, functional tasks, sit/stand/walk) or daily sedative interruption and standard medical/nursing care. Compared with the control group, the treatment group demonstrated a signifi cantly shorter duration of delirium and mechan-ical ventilation, and signifi cantly more patients in the treatment group achieved an independent functional status at hospital discharge. The second prospective RCT, involving 90 patients whose ICU LOS was anticipated as being . 7 days, investigated the effec-tiveness of adding cycling exercise using a bedside cycle ergometer to a standard physiotherapy mobili-zation regimen (ie, limb exercises, walk). 35 While no signifi cant differences were found between groups at ICU discharge, the treatment group achieved sig-nifi cantly higher distances in the 6-min walk test than the control group at hospital discharge and their quadriceps strength improved signifi cantly between ICU and hospital discharge. The third RCT, by Chang et al, 36 prospectively investigated the effect of sitting out of bed (for at least 30 min, most often on a daily basis) on the respiratory muscle strength of 34 patients over a 6-day study period. The patients in the con-trol group were positioned supine or semirecumbent in bed. No signifi cant differences were seen between groups.
Two of the fi ve nonrandomized controlled stud ies pro-spectively allocated patients to a control group (standard medical/nursing care) or a treatment group (progressive St
udy
Part
icip
ants
, No.
, Ty
peIn
terv
entio
nO
utco
mes
Res
ults
Sum
mar
y of
Aut
hors
’ Con
clus
ions
Pros
pect
ive,
obse
rvat
iona
l stu
dies
T
hom
as e
t al 32
34
, int
ubat
ed,
mec
hani
cally
ve
ntila
ted
with
or
with
out
pulm
onar
y in
fi ltr
ates
on
CX
R.
90°
side
lyin
g.Pa
o 2 /F
io 2 ,
Pa co
2 , V t
, dy
nam
ic re
spira
tory
co
mpl
ianc
e, a
irway
pre
ssur
e,
MA
P, H
R, c
ardi
ac in
dex,
ad
vers
e ev
ents
bef
ore,
du
ring
, and
30-
and
12
0-m
in p
ost-
Rx.
No
sign
ifi ca
nt c
hang
e in
Pa o
2 /F io
2 , Pa
co 2 ,
MA
P, H
R.
The
resu
lts d
id n
ot su
ppor
t the
use
of l
ater
al
posi
tioni
ng to
impr
ove
oxyg
enat
ion
in
vent
ilate
d pa
tient
s w
ithou
t lun
g pa
thol
ogy
or w
ith p
ulm
onar
y in
fi ltr
ates
.C
ompl
ianc
e an
d V t
sig
nifi c
antly
de
crea
sed
duri
ng p
ositi
onin
g, c
ardi
ac
inde
x si
gnifi
cant
ly in
crea
sed
30-m
in
post
-Rx.
21%
inci
denc
e of
adv
erse
ev
ents
(min
or, t
rans
ient
).
Cla
rke
et a
l 33
25, s
edat
ed,
intu
bate
d,
mec
hani
cally
ve
ntila
ted.
Man
ual h
yper
vent
ilatio
n w
ith M
aple
son
C c
ircu
it.V t
, pea
k ai
rway
pre
ssur
e,
Pa o
2 , Pa
co 2 b
efor
e,
duri
ng, a
nd im
med
iate
ly
post
-Rx.
Sign
ifi ca
nt n
egat
ive
corr
elat
ion
betw
een
aver
age
V t a
nd lu
ng in
jury
sco
re.
Sign
ifi ca
nt p
ositi
ve c
orre
latio
n be
twee
n av
erag
e pe
ak a
irw
ay p
ress
ure
and
lung
in
jury
scor
e. P
a o 2 s
igni
fi can
tly im
prov
ed
from
pre
- to
imm
edia
tely
pos
t-R
x. N
o si
gnifi
cant
cha
nge
in P
a co
2 .
Man
ual h
yper
vent
ilatio
n ca
uses
hig
her
infl a
tion
pres
sure
s an
d sm
alle
r V t
s as
th
e lu
ng s
core
incr
ease
s, s
ugge
stin
g an
in
crea
sed
pote
ntia
l for
bar
otra
uma
or
volu
trau
ma
in s
usce
ptib
le lu
ngs.
AL
I 5 ac
ute
lung
inju
ry; C
PIS
5 cl
inic
al p
ulm
onar
y in
fect
ion
scor
e; C
XR
5 ch
est
radi
ogra
ph; H
R 5
hea
rt r
ate;
L 5
left
; MA
P 5
mea
n ar
teri
al B
P; P
EE
P 5
pos
itive
end
exp
irat
ory
pres
sure
; PE
FR
5 p
eak
expi
rato
ry fl
ow r
ate;
R 5
righ
t; S v
o 2 5
mix
ed v
enou
s ox
ygen
sat
urat
ion;
co
2 5 C
O 2 o
utpu
t; V
H 5
vent
ilato
r hy
peri
nfl a
tion;
V t
5 ti
dal v
olum
e. S
ee T
able
1 le
gend
for
expa
nsio
n of
oth
er a
bbre
viat
ions
.
Tabl
e 2—
Con
tinu
ed
Downloaded From: http://journal.publications.chestnet.org/ by a University of Pittsburgh User on 10/14/2013

834 Original Research
Tabl
e 3—
Cha
ract
eris
tics
of
Stu
dies
Eva
luat
ing
Mob
iliz
atio
n
Stud
yPa
rtic
ipan
ts, N
o.,
Type
Inte
rven
tion
Out
com
esR
esul
tsSu
mm
ary
of A
utho
rs’ C
oncl
usio
ns
Pros
pect
ive,
ran
dom
ized
,
cont
rolle
d/co
mpa
rativ
e tr
ials
Sc
hwei
cker
t et a
l 34
104,
intu
bate
d,
mec
hani
cally
ve
ntila
ted
, 7
2 h,
lik
ely
to
cont
inue
� 2
4 h.
Con
trol
: dai
ly s
edat
ive
inte
rrup
tion
and
stan
dard
ca
re (i
nclu
ded
PT a
nd O
T
per
prim
ary
care
team
).
Ret
urn
to in
depe
nden
t fu
nctio
nal s
tatu
s at
hos
pita
l D
C, d
urat
ion
of d
elir
ium
an
d m
echa
nica
l ven
tilat
ion,
ve
ntila
tor-
free
day
s, I
CU
an
d ho
spita
l LO
S, a
dver
se
even
ts.
Ret
urn
to in
depe
nden
t fun
ctio
nal
stat
us a
t hos
pita
l DC
occ
urre
d in
si
gnifi
cant
ly m
ore
Rx
grou
p pa
tient
s.
Dur
atio
n of
del
iriu
m a
nd m
echa
nica
l ve
ntila
tion
sign
ifi ca
ntly
sho
rter
in R
x gr
oup.
Ven
tilat
or-f
ree
days
, and
IC
U
and
hosp
ital L
OS
not s
igni
fi can
tly
diff
eren
t bet
wee
n gr
oups
. Ser
ious
ad
vers
e ev
ents
: 0.2
%.
Seda
tion
inte
rrup
tion
and
PT/O
T
in th
e ea
rlie
st d
ays
of c
ritic
al
illne
ss w
as s
afe
and
wel
l to
lera
ted,
res
ulte
d in
bet
ter
func
tiona
l out
com
es a
t hos
pita
l D
C, s
hort
er d
urat
ion
of
delir
ium
, and
mor
e ve
ntila
tor-
free
day
s.
Rx:
dai
ly s
edat
ive
inte
rrup
tion
for
PT a
nd O
T (e
g, R
OM
ex
erci
ses,
bed
mob
ility
, fu
nctio
nal a
nd A
DL
task
s,
sit/s
tand
/wal
k).
B
urtin
et a
l 35
90, c
ritic
ally
ill,
antic
ipat
ed
ICU
LO
S .
7 d
po
stre
crui
tmen
t.
Con
trol
: sta
ndar
d PT
m
obili
zatio
n (li
mb
exer
cise
s,
wal
k), 5
d/w
k.
6MW
D a
t hos
pita
l DC
, qu
adri
ceps
forc
e, fu
nctio
nal
stat
us (s
it-to
-sta
nd [B
BS]
an
d ph
ysic
al fu
nctio
ning
[S
F-3
6]) a
t IC
U a
nd h
ospi
tal
DC
, adv
erse
eve
nts.
6MW
D a
nd S
F-3
6 su
bsco
re
sign
ifi ca
ntly
hig
her
in R
x gr
oup
at h
ospi
tal D
C. Q
uadr
icep
s for
ce
impr
oved
sign
ifi ca
ntly
mor
e be
twee
n IC
U a
nd h
ospi
tal D
C in
Rx
grou
p.
Abi
lity
to s
tand
inde
pend
ently
(B
BS
� 2
) not
sig
nifi c
antly
di
ffer
ent b
etw
een
grou
ps.
Seri
ous
adve
rse
even
ts: 0
%.
Whe
n in
stitu
ted
earl
y in
IC
U
surv
ivor
s w
ith a
pro
long
ed
stay
, exe
rcis
e tr
aini
ng m
ay
enha
nce
reco
very
of
func
tiona
l exe
rcis
e ca
paci
ty,
func
tiona
l sta
tus,
and
qu
adri
ceps
forc
e at
ho
spita
l DC
.
Rx:
as
for
cont
rol p
lus
cycl
ing
exer
cise
(bed
side
cyc
le
ergo
met
er),
20 m
in, 5
d/w
k.
C
hang
et a
l 36
34, m
echa
nica
lly
vent
ilate
d �
72
h,
able
to tr
ansf
er to
ch
air
with
two
nurs
es.
Con
trol
: pos
ition
ed s
upin
e to
se
mi-r
ecum
bent
, no
PT.
Rap
id s
hallo
w b
reat
hing
inde
x,
V t , r
espi
rato
ry m
uscl
e st
reng
th b
efor
e an
d 30
-min
po
stin
terv
entio
n ov
er 6
-d
tria
l per
iod.
No
sign
ifi ca
nt d
iffer
ence
s be
twee
n gr
oups
for
any
outc
ome
over
6-
d tr
ial p
erio
d.
6 d
of c
hair
sitt
ing
was
inef
fect
ive
at im
prov
ing
resp
irat
ory
mus
cle
func
tion
in
mec
hani
cally
ven
tilat
ed
patie
nts
in th
e IC
U.
Rx:
sit
in c
hair,
30-
120
min
, at
leas
t 3 d
/wk.
Pros
pect
ive,
nonr
ando
miz
ed,
cont
rolle
d tr
ials
M
orri
s et
al 37
33
0, in
tuba
ted,
m
echa
nica
lly
vent
ilate
d, a
cute
re
spir
ator
y fa
ilure
.
Con
trol
: sta
ndar
d m
edic
al/n
ursi
ng c
are.
Prop
ortio
n re
ceiv
ing
ICU
PT,
da
ys u
ntil
fi rst
out
of b
ed,
vent
ilato
r da
ys, I
CU
and
ho
spita
l LO
S, a
dver
se
even
ts.
ICU
PT
pro
vide
d to
sig
nifi c
antly
m
ore
patie
nts
in R
x gr
oup.
R
x gr
oup
fi rst
out
of b
ed
sign
ifi ca
ntly
ear
lier.
ICU
and
ho
spita
l LO
S si
gnifi
cant
ly s
hort
er
in R
x gr
oup.
Ven
tilat
or d
ays
not
sign
ifi ca
ntly
diff
eren
t bet
wee
n gr
oups
. Ser
ious
adv
erse
eve
nts:
0%.
Impl
emen
tatio
n of
an
earl
y m
obili
ty p
roto
col b
y a
mob
ility
te
am r
esul
ted
in m
ore
PT
sess
ions
and
was
ass
ocia
ted
with
a s
hort
er L
OS
for
hosp
ital
surv
ivor
s.
Rx:
pro
gres
sive
mob
iliza
tion
(eg,
RO
M e
xerc
ises,
func
tiona
l ta
sks,
sit/
stan
d/w
alk)
from
a
mob
ility
team
, 7 d
/wk.
(Con
tinu
ed)
Downloaded From: http://journal.publications.chestnet.org/ by a University of Pittsburgh User on 10/14/2013

journal.publications.chestnet.org CHEST / 144 / 3 / SEPTEMBER 2013 835
Stud
yPa
rtic
ipan
ts, N
o.,
Type
Inte
rven
tion
Out
com
esR
esul
tsSu
mm
ary
of A
utho
rs’ C
oncl
usio
ns
Ya
ng e
t al 38
12
6, m
echa
nica
lly
vent
ilate
d .
14
d.C
ontr
ol: r
outin
e pa
ssiv
e jo
int
exer
cise
s by
nur
ses
5-10
min
, bi
d.
Rap
id s
hallo
w b
reat
hing
in
dex,
BI,
wea
ning
suc
cess
. Ti
min
g no
t cle
ar.
Rap
id s
hallo
w b
reat
hing
inde
x di
d no
t sig
nifi c
antly
cha
nge.
BI
sign
ifi ca
ntly
impr
oved
ove
r tim
e in
Rx
grou
p (n
ot c
lear
wha
t ha
ppen
ed to
con
trol
). W
eani
ng
succ
ess
rate
hig
her
in R
x gr
oup
(sig
nifi c
ance
not
sta
ted)
.
Not
sta
ted.
Rx:
bre
athi
ng tr
aini
ng, p
rogr
essiv
e m
obili
zatio
n (e
g, p
assi
ve/a
ctiv
e R
OM
exe
rcis
es, s
it/st
and/
wal
k),
30 m
in, d
aily
, 5 ti
mes
/wk.
W
inke
lman
et a
l 39
75, m
echa
nica
lly
vent
ilate
d .
48
h, li
kely
to
con
tinue
� 2
4 h.
Con
trol
pha
se: s
tand
ard
med
ical
/nur
sing
car
e.In
fl am
mat
ory
biom
arke
rs,
HR
, RR
, sys
tolic
BP,
Sp o
2 , ad
vers
e ev
ents
ove
r 7-
d tr
ial p
erio
d. D
urat
ion
of
mec
hani
cal v
entil
atio
n,
ICU
LO
S.
Dai
ly e
xerc
ise
linke
d to
incr
ease
d IL
-10.
HR
, RR
, sys
tolic
BP,
Sp o
2 no
t sig
nifi c
antly
diff
eren
t bet
wee
n co
ntro
l and
Rx
phas
es. S
erio
us
adve
rse
even
ts: ,
5%
. Dur
atio
n of
ve
ntila
tion
not s
igni
fi can
tly d
iffer
ent
betw
een
phas
es. I
CU
LO
S sig
nifi c
antly
shor
ter d
urin
g R
x ph
ase.
The
res
ults
sho
uld
enco
urag
e cl
inic
ians
to a
dd m
obili
ty
prot
ocol
s to
the
care
of
patie
nts
in th
e IC
U.
Rx
phas
e: p
rogr
essi
ve
mob
iliza
tion
(per
Mor
ris e
t al 37
), 20
min
, dai
ly, 2
-7 d
.
N
eedh
am e
t al 40
57
, mec
hani
cally
ve
ntila
ted
. 4
d.
Con
trol
pha
se: s
tand
ard
med
ical
/nur
sing
car
e.Pr
eval
ence
of d
eep
seda
tion
and
delir
ium
, fun
ctio
nal
mob
ility
, IC
U a
nd h
ospi
tal
LO
S, a
dver
se e
vent
s.
Prev
alen
ce o
f dee
p se
datio
n an
d de
liriu
m si
gnifi
cant
ly lo
wer
dur
ing
Rx
phas
e. F
unct
iona
l mob
ility
sig
nifi c
antly
bet
ter d
urin
g R
x ph
ase.
Si
gnifi
cant
ly sh
orte
r IC
U a
nd
hosp
ital L
OS
durin
g R
x ph
ase
com
pare
d w
ith p
rior
yea
r. Se
riou
s ad
vers
e ev
ents
: 0%
.
Red
ucin
g de
ep s
edat
ion
and
incr
easi
ng e
arly
mob
iliza
tion
resu
lted
in s
ubst
antia
l im
prov
emen
ts in
IC
U d
elir
ium
an
d fu
nctio
nal m
obili
ty, w
ith
a de
crea
se in
IC
U a
nd
hosp
ital L
OS.
Rx
phas
e: r
educ
ed s
edat
ion,
ea
rly
prog
ress
ive
mob
iliza
tion
(eg,
sit/
stan
d/w
alk)
.
C
hian
g et
al 41
32
, mec
hani
cally
ve
ntila
ted
. 1
4 d.
Con
trol
: sta
ndar
d m
edic
al/n
ursin
g ca
re in
clud
ing
prom
otio
n of
m
obili
zatio
n (e
g, e
xerc
ises
, w
alk)
.
Res
pira
tory
mus
cle
stre
ngth
, up
per
and
low
er li
mb
stre
ngth
, BI,
FIM
, ve
ntila
tor-
free
tim
e at
3
and
6 w
k.
Res
pira
tory
mus
cle
and
limb
stre
ngth
sig
nifi c
antly
incr
ease
d at
3
and
6 w
k in
Rx
grou
p bu
t not
co
ntro
l gro
up. B
I and
FIM
scor
es
signi
fi can
tly h
ighe
r in
Rx
grou
p th
an
cont
rol g
roup
at 3
and
6 w
k.
Vent
ilato
r-fr
ee ti
me
incr
ease
d si
gnifi
cant
ly in
Rx
grou
p bu
t not
con
trol
gro
up a
t 6 w
k.
A 6
-wk
phys
ical
trai
ning
pro
gram
m
ay im
prov
e lim
b m
uscl
e st
reng
th a
nd v
entil
ator
-fre
e tim
e an
d im
prov
e fu
nctio
nal
outc
omes
in p
atie
nts
requ
irin
g pr
olon
ged
mec
hani
cal
vent
ilatio
n.
Rx:
pro
gres
sive
mob
iliza
tion
(eg,
str
engt
heni
ng a
nd
RO
M e
xerc
ises,
sit/s
tand
/wal
k),
5 tim
es/w
k fo
r 6
wk.
Pros
pect
ive,
his
tori
cal
co
ntro
lled
tria
l
Bas
sett
et a
l 42
260,
not
sta
ted.
Con
trol
: his
tori
cal c
ontr
ol.
Vent
ilato
r da
ys,
vent
ilato
r-fr
ee d
ays,
IC
U
and
hosp
ital m
orta
lity,
IC
U
and
hosp
ital L
OS,
day
s to
st
andi
ng a
nd a
mbu
latin
g.
No
sign
ifi ca
nt d
iffer
ence
s be
twee
n gr
oups
for
any
outc
omes
.A
n ea
rly
mob
ility
pro
gram
im
prov
ed I
CU
team
focu
s on
th
e pr
oces
s of
ear
ly m
obili
ty,
but n
o si
gnifi
cant
diff
eren
ces
wer
e se
en in
qua
ntita
tive
outc
omes
.
Rx:
pro
gres
sive
mob
iliza
tion
(eg,
RO
M e
xerc
ises,
func
tiona
l ta
sks,
sit/
stan
d/w
alk)
.
(Con
tinu
ed)
Tabl
e 3—
Con
tinu
ed
Downloaded From: http://journal.publications.chestnet.org/ by a University of Pittsburgh User on 10/14/2013

836 Original Research
Stud
yPa
rtic
ipan
ts, N
o.,
Type
Inte
rven
tion
Out
com
esR
esul
tsSu
mm
ary
of A
utho
rs’ C
oncl
usio
ns
Pros
pect
ive,
obs
erva
tiona
l
stud
ies
L
edits
chke
et a
l 43
106,
all
patie
nts
in I
CU
.U
sual
pra
ctic
e.F
requ
ency
of m
obili
zatio
n (s
it/st
and/
wal
k), a
dver
se
even
ts, b
arri
ers
to
mob
iliza
tion.
Patie
nts
wer
e m
obili
zed
on 5
4% o
f da
ys a
udite
d. A
dver
se e
vent
s: 1
%.
Avo
idab
le b
arri
ers
incl
uded
lo
catio
n of
vas
cula
r ac
cess
line
s,
sche
dulin
g of
mob
iliza
tion,
seda
tion.
Cri
tical
ly il
l pat
ient
s ca
n be
saf
ely
mob
ilize
d.
T
hom
sen
et a
l 44
104,
tran
sfer
red
from
gen
eral
IC
U to
a sp
ecifi
c re
spira
tory
IC
U,
mec
hani
cally
ve
ntila
ted
. 4
d,
resp
irat
ory
failu
re.
Ear
ly p
rogr
essi
ve
mob
iliza
tion
(eg,
sit/
wal
k)
follo
win
g tr
ansf
er.
Fre
quen
cy o
f am
bula
tion.
Prob
abili
ty o
f am
bula
tion
sign
ifi ca
ntly
in
crea
sed
afte
r tr
ansf
er to
the
resp
irat
ory
ICU
. Aft
er 2
d, n
umbe
r of
pat
ient
s am
bula
ting
incr
ease
d th
reef
old
com
pare
d w
ith
pret
rans
fer.
The
IC
U e
nvir
onm
ent m
ay
cont
ribu
te to
the
unne
cess
ary
imm
obili
zatio
n of
pat
ient
s w
ith
acut
e re
spir
ator
y fa
ilure
.
B
aile
y et
al 45
10
3, m
echa
nica
lly
vent
ilate
d .
4 d
, re
spir
ator
y fa
ilure
.
Ear
ly p
rogr
essi
ve
mob
iliza
tion
(eg,
sit/
wal
k).
Fea
sibi
lity,
adv
erse
eve
nts.
Tota
l of 1
,449
ear
ly m
obili
zatio
n ac
tiviti
es. A
dver
se e
vent
s: ,
1%
.E
arly
mob
iliza
tion
is fe
asib
le a
nd
safe
in r
espi
rato
ry fa
ilure
pa
tient
s.
Clin
i et a
l 46
77, t
rach
eost
omiz
ed,
diffi
cult
to w
ean.
Ear
ly r
ehab
ilita
tion
incl
udin
g pr
ogre
ssiv
e m
obili
zatio
n (e
g,
limb
exer
cise
s, sit
/sta
nd/w
alk)
, w
eani
ng p
roto
col,
nutr
ition
al
supp
ort.
Mor
talit
y, w
eani
ng s
ucce
ss,
BA
DL
sco
re a
t bas
elin
e an
d IC
U D
C, a
dver
se
even
ts.
Hos
pita
l mor
talit
y: 8
7%. W
eani
ng
succ
ess:
74%
. BA
DL
sco
re
impr
oved
. Adv
erse
eve
nts:
0%
.
Ear
ly r
ehab
ilita
tion
cont
ribu
tes
to B
AD
L re
cove
ry in
di
ffi cu
lt-to
-wea
n pa
tient
s.
G
arzo
n-Se
rran
o et
al 47
63
, all
patie
nts
in I
CU
.M
obili
zatio
n (e
g, li
mb
exer
cise
s,
bed
mob
ility
, sit/
stan
d/w
alk)
by
nur
sing
or
PT s
taff
.
Lev
el o
f mob
iliza
tion
achi
eved
, adv
erse
eve
nts.
PTs
mob
ilize
d pa
tient
s to
a
sign
ifi ca
ntly
hig
her
leve
l of
mob
ility
than
nur
sing
sta
ff.
Adv
erse
eve
nts:
0%
.
Rou
tine
invo
lvem
ent o
f PTs
in
dire
ctin
g m
obili
zatio
n R
x m
ay
prom
ote
earl
y m
obili
zatio
n of
cr
itica
lly il
l pat
ient
s.
Zann
i et a
l 48
32, m
echa
nica
lly
vent
ilate
d .
4 d
.M
obili
zatio
n (e
g, li
mb
exer
cise
s,
bala
nce,
func
tiona
l act
iviti
es,
sit/s
tand
/wal
k).
HR
, BP,
Sp o
2 bef
ore
and
post
sess
ion,
RO
M,
mus
cle
stre
ngth
, fu
nctio
nal o
utco
mes
, ad
vers
e ev
ents
.
HR
, BP,
Sp o
2 : m
inim
al c
hang
es
duri
ng s
essi
ons.
Low
er-li
mb
join
t co
ntra
ctur
es fr
eque
nt, d
id n
ot
impr
ove
duri
ng h
ospi
taliz
atio
n.
Lim
b w
eakn
ess
com
mon
, im
prov
ed d
urin
g ho
spita
lizat
ion.
A
dver
se e
vent
s: 0
%.
Reh
abili
tatio
n th
erap
y ap
pear
ed
safe
with
out s
igni
fi can
t ph
ysio
logi
c ch
ange
s or
adv
erse
ef
fect
s, b
ut w
as o
nly
prov
ided
in
freq
uent
ly.
St
iller
et a
l 49
31, a
ny p
atie
nt in
IC
U
bein
g m
obili
zed
by P
Ts.
Mob
iliza
tion
(eg,
sit/
stan
d/w
alk)
.H
R, B
P, S
p o 2 b
efor
e,
duri
ng a
nd im
med
iate
ly
post
sess
ion,
adv
erse
ev
ents
.
HR
and
BP
incr
ease
d si
gnifi
cant
ly
duri
ng s
essi
ons.
No
sign
ifi ca
nt
chan
ge in
Sp o
2 . A
dver
se
even
ts: 4
% (m
inor
, tra
nsie
nt).
Acu
tely
ill p
atie
nts
in th
e IC
U
can
be s
afel
y m
obili
zed
with
out m
ajor
det
erio
ratio
n in
thei
r cl
inic
al s
tatu
s.
Bah
adur
et a
l 50
30, t
rach
eost
omiz
ed,
mec
hani
cally
ve
ntila
ted.
Usu
al c
are,
incl
udin
g si
ttin
g.F
requ
ency
of s
ittin
g ou
t of
bed
.63
% s
at o
ut o
f bed
on
a m
edia
n of
two
occa
sion
s.D
espi
te a
cul
ture
of e
arly
m
obili
zatio
n, s
ome
patie
nts
wer
e co
nsid
ered
too
unw
ell
for
it to
occ
ur.
(Con
tinu
ed)
Tabl
e 3—
Con
tinu
ed
Downloaded From: http://journal.publications.chestnet.org/ by a University of Pittsburgh User on 10/14/2013

journal.publications.chestnet.org CHEST / 144 / 3 / SEPTEMBER 2013 837
Stud
yPa
rtic
ipan
ts, N
o.,
Type
Inte
rven
tion
Out
com
esR
esul
tsSu
mm
ary
of A
utho
rs’ C
oncl
usio
ns
B
ourd
in e
t al 51
20
, mec
hani
cally
ve
ntila
ted
� 2
d,
ICU
sta
y �
7 d
.
Ear
ly p
rogr
essi
ve m
obili
zatio
n (e
g, s
it/til
t tab
le/w
alk)
.F
easi
bilit
y, H
R, R
R, M
AP,
Sp
o 2 b
efor
e an
d po
stse
ssio
n,
adve
rse
even
ts.
Cha
ir s
ittin
g si
gnifi
cant
ly d
ecre
ased
H
R a
nd R
R. H
R a
nd R
R
sign
ifi ca
ntly
incr
ease
d w
ith
tiltin
g-up
and
wal
king
. Sp o
2 si
gnifi
cant
ly d
ecre
ased
with
w
alki
ng. A
dver
se e
vent
s: 3
%
(min
or).
Ear
ly m
obili
zatio
n is
feas
ible
and
sa
fe fo
r pa
tient
s in
IC
U
for
. 7
d.
N
ordo
n-C
raft
et a
l 52
19, m
echa
nica
lly
vent
ilate
d �
7 d
, IC
U a
cqui
red
wea
knes
s.
Prog
ress
ive
mob
iliza
tion
(eg,
lim
b ex
erci
ses,
si
t/sta
nd/w
alk)
, 30
min
, 5
d/w
k.
Adv
erse
eve
nts,
feas
ibili
ty,
mus
cle
stre
ngth
, fu
nctio
nal o
utco
mes
.
Adv
erse
eve
nts:
0%
. 170
ses
sion
s pr
ovid
ed. P
atie
nts
DC
hom
e ha
d hi
gher
str
engt
h an
d fu
nctio
nal s
core
s.
Ear
ly m
obili
zatio
n an
d PT
wer
e sa
fe a
nd fe
asib
le fo
r pa
tient
s w
ith I
CU
acq
uire
d w
eakn
ess.
N
orre
nber
g et
al 53
16
, pat
ient
s in
IC
U.
Pass
ive
limb
mov
emen
ts.
o 2 ,
CIX
, O 2 E
R b
efor
e an
d du
ring
inte
rven
tion.
o 2 s
igni
fi can
tly in
crea
sed
duri
ng
inte
rven
tion:
ach
ieve
d by
incr
ease
in
O 2 E
R in
pat
ient
s w
ith c
ardi
ac
dysf
unct
ion,
by
incr
ease
in C
IX in
pa
tient
s with
out c
ardi
ac d
ysfu
nctio
n.
Sim
ple
man
euve
rs li
ke p
assi
ve
limb
mov
emen
ts c
an in
fl uen
ce
the
hem
odyn
amic
sta
tus
of
patie
nts
in I
CU
.
C
hang
et a
l 54
15, i
ntub
ated
, m
echa
nica
lly
vent
ilate
d .
5 d
.
Stan
ding
on
a til
t tab
le
(70°
from
hor
izon
tal),
5
min
.
e , V
t , R
R, P
a o 2 ,
Pa co
2 be
fore
, dur
ing,
im
med
iate
ly a
nd 2
0-m
in
post
inte
rven
tion.
e , R
R, a
nd V
t si
gnifi
cant
ly
incr
ease
d du
ring
and
imm
edia
tely
po
st-t
ilt, n
ot s
igni
fi can
t by
20 m
in
post
-tilt
. Pa o
2 and
Pa c
o 2 :
no
sign
ifi ca
nt c
hang
e.
Stan
ding
on
a til
t tab
le p
rodu
ced
a tr
ansi
ent i
ncre
ase
in
vent
ilatio
n in
cri
tical
ly il
l pa
tient
s.
Za
fi rop
oulo
s et
al 55
15
, int
ubat
ed,
mec
hani
cally
ve
ntila
ted,
el
ectiv
e m
ajor
ab
dom
inal
su
rger
y.
Ear
ly m
obili
zatio
n (e
g, s
it/st
and/
wal
k) w
hile
sp
onta
neou
sly
brea
thin
g on
F io
2 5 1
.0.
Rib
cag
e an
d ab
dom
en
disp
lace
men
t, V t
, RR
, e
, HR
, BP,
Sp o
2, P
a o 2 ,
Pa co
2 bef
ore,
dur
ing,
an
d 20
-min
po
stin
terv
entio
n.
Stan
ding
sig
nifi c
antly
incr
ease
d ri
b ca
ge d
ispl
acem
ent,
V t , R
R, a
nd
e .
No
furt
her
sign
ifi ca
nt c
hang
es s
een
with
wal
king
. BP
and
HR
si
gnifi
cant
ly in
crea
sed
whe
n th
e pa
tient
s sa
t on
edge
of b
ed. P
a o 2
and
Pa co
2 : no
sig
nifi c
ant c
hang
e.
Cha
nges
in V
t , R
R, a
nd
e du
ring
m
obili
zatio
n w
ere
larg
ely
due
to p
ositi
onal
cha
nge
from
su
pine
to s
tand
ing.
Sk
inne
r et
al 56
12
, tra
cheo
stom
ized
, m
echa
nica
lly
vent
ilate
d.
Prog
ress
ive
mob
iliza
tion
(eg,
lim
b ex
erci
ses,
si
t/sta
nd/w
alk)
.
Res
pons
iven
ess
and
relia
bilit
y of
the
phys
ical
fu
nctio
n IC
U te
st,
adve
rse
even
ts.
The
test
was
eas
y to
per
form
, re
spon
sive
and
rel
iabl
e. A
dver
se
even
ts: 0
%.
Thi
s te
st m
ay b
e us
ed to
pre
scri
be
and
eval
uate
exe
rcis
e fo
r w
eak,
de
bilit
ated
pat
ient
s in
IC
U.
T
hela
nder
sson
et a
l 57
12, m
echa
nica
lly
vent
ilate
d, u
nabl
e to
act
ivel
y m
ove,
se
vere
hea
d in
jury
.
Pass
ive
RO
M e
xerc
ises
upp
er
and
low
er li
mbs
.IC
P, C
PP, C
BF
V, P
I, B
P,
and
HR
bef
ore,
du
ring
, and
10
min
po
stin
terv
entio
n.
ICP
sign
ifi ca
ntly
dec
reas
ed
post
inte
rven
tion.
No
sign
ifi ca
nt
chan
ge in
oth
er o
utco
mes
.
Pass
ive
RO
M e
xerc
ises
can
be
used
saf
ely
in c
ritic
ally
ill
neur
osur
gica
l pat
ient
s in
IC
U.
(Con
tinu
ed)
Tabl
e 3—
Con
tinu
ed
Downloaded From: http://journal.publications.chestnet.org/ by a University of Pittsburgh User on 10/14/2013
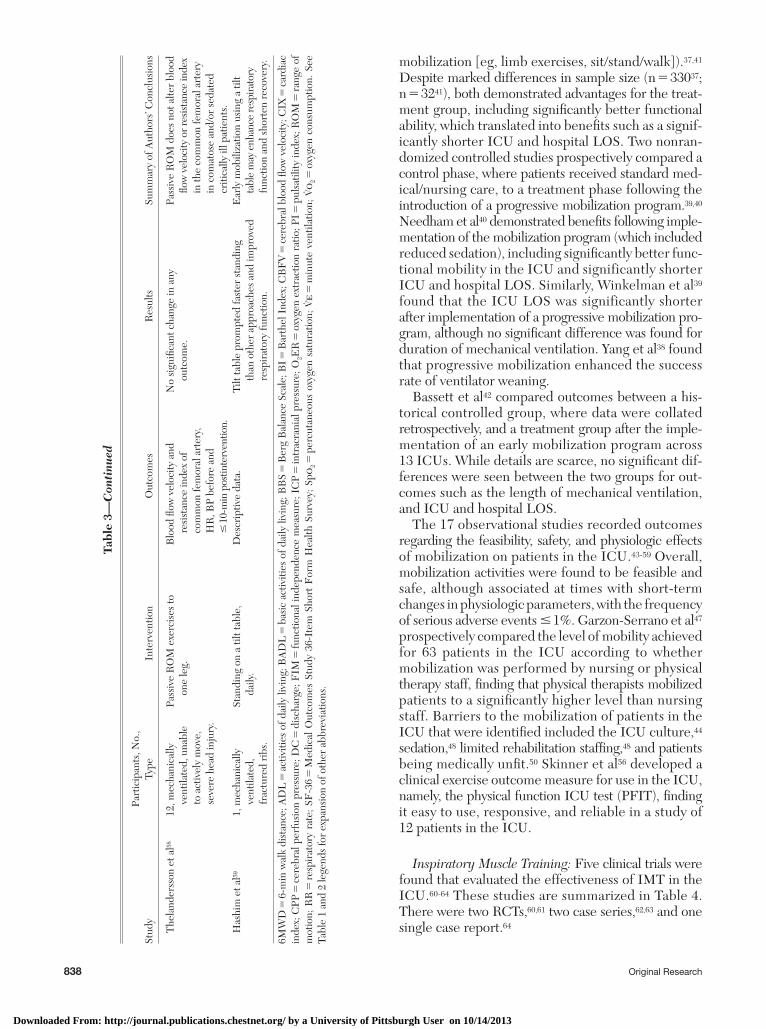
838 Original Research
mobilization [eg, limb exercises, sit/stand/walk]). 37,41 Despite marked differences in sam ple size (n 5 330 37 ; n 5 32 41 ), both demonstrated advantages for the treat-ment group, including signifi cantly better functional ability, which translated into benefi ts such as a signif-icantly shorter ICU and hospital LOS. Two nonran-domized controlled studies prospectively compared a control phase, where patients received standard med-ical/nursing care, to a treatment phase follow ing the introduction of a progressive mobilization program. 39,40 Needham et al 40 demonstrated benefi ts following imple-mentation of the mobilization program (which included reduced sedation), including signifi cantly better func-tional mobility in the ICU and significantly shorter ICU and hospital LOS. Similarly, Winkelman et al 39 found that the ICU LOS was significantly shorter after implementation of a progressive mobilization pro-gram, although no signifi cant difference was found for duration of mechanical ventilation. Yang et al 38 found that progressive mobilization enhanced the success rate of ventilator weaning.
Bassett et al 42 compared outcomes between a his-torical controlled group, where data were collated retrospectively, and a treatment group after the imple-mentation of an early mobilization program across 13 ICUs. While details are scarce, no signifi cant dif-ferences were seen between the two groups for out-comes such as the length of mechanical ventilation, and ICU and hospital LOS.
The 17 observational studies recorded outcomes regarding the feasibility, safety, and physiologic effects of mobilization on patients in the ICU. 43-59 Overall, mobilization activities were found to be feasible and safe, although associated at times with short-term changes in physiologic parameters, with the frequency of serious adverse events � 1%. Garzon-Serrano et al 47 prospectively compared the level of mobility achieved for 63 patients in the ICU according to whether mobilization was performed by nursing or physical therapy staff, fi nding that physical therapists mobilized patients to a signifi cantly higher level than nursing staff. Barriers to the mobilization of patients in the ICU that were identifi ed included the ICU culture, 44 sedation, 48 limited rehabilitation staffi ng, 48 and patients being medically unfi t. 50 Skinner et al 56 developed a clinical exercise outcome measure for use in the ICU, namely, the physical function ICU test (PFIT), fi nding it easy to use, responsive, and reliable in a study of 12 patients in the ICU.
Inspiratory Muscle Training: Five clinical trials were found that evaluated the effectiveness of IMT in the ICU. 60-64 These studies are summarized in Table 4 . There were two RCTs, 60,61 two case series, 62,63 and one single case report. 64
Stud
yPa
rtic
ipan
ts, N
o.,
Type
Inte
rven
tion
Out
com
esR
esul
tsSu
mm
ary
of A
utho
rs’ C
oncl
usio
ns
T
hela
nder
sson
et a
l 58
12, m
echa
nica
lly
vent
ilate
d, u
nabl
e to
act
ivel
y m
ove,
se
vere
hea
d in
jury
.
Pass
ive
RO
M e
xerc
ises
to
one
leg.
Blo
od fl
ow v
eloc
ity a
nd
resi
stan
ce in
dex
of
com
mon
fem
oral
art
ery,
H
R, B
P be
fore
and
�
10-m
in p
ostin
terv
entio
n.
No
sign
ifi ca
nt c
hang
e in
any
ou
tcom
e.Pa
ssiv
e R
OM
doe
s no
t alte
r bl
ood
fl ow
vel
ocity
or r
esis
tanc
e in
dex
in th
e co
mm
on fe
mor
al a
rter
y in
com
atos
e an
d/or
sed
ated
cr
itica
lly il
l pat
ient
s.
Has
him
et a
l 59
1, m
echa
nica
lly
vent
ilate
d,
frac
ture
d ri
bs.
Stan
ding
on
a til
t tab
le,
daily
.D
escr
iptiv
e da
ta.
Tilt
tabl
e pr
ompt
ed fa
ster
sta
ndin
g th
an o
ther
app
roac
hes
and
impr
oved
re
spir
ator
y fu
nctio
n.
Ear
ly m
obili
zatio
n us
ing
a til
t ta
ble
may
enh
ance
resp
irato
ry
func
tion
and
shor
ten
reco
very
.
6MW
D 5
6-m
in w
alk
dist
ance
; AD
L 5
activ
ities
of d
aily
livi
ng; B
AD
L 5
bas
ic a
ctiv
ities
of d
aily
livi
ng; B
BS
5 B
erg
Bal
ance
Sca
le; B
I 5 B
arth
el I
ndex
; CB
FV
5 ce
rebr
al b
lood
fl ow
vel
ocity
; CIX
5 ca
rdia
c in
dex;
CPP
5 ce
rebr
al p
erfu
sion
pre
ssur
e; D
C 5
dis
char
ge; F
IM 5
func
tiona
l ind
epen
denc
e m
easu
re; I
CP
5 in
trac
rani
al p
ress
ure;
O 2 E
R 5
oxy
gen
extr
actio
n ra
tio; P
I 5 p
ulsa
tility
inde
x; R
OM
5 ra
nge
of
mot
ion;
RR
5 re
spir
ator
y ra
te; S
F-3
6 5
Med
ical
Out
com
es S
tudy
36-
Item
Sho
rt F
orm
Hea
lth S
urve
y; S
p o 2 5
per
cuta
neou
s ox
ygen
sat
urat
ion;
e
5 m
inut
e ve
ntila
tion;
o
2 5 o
xyge
n co
nsum
ptio
n. S
ee
Tabl
e 1
and
2 le
gend
s fo
r ex
pans
ion
of o
ther
abb
revi
atio
ns.
Tabl
e 3—
Con
tinu
ed
Downloaded From: http://journal.publications.chestnet.org/ by a University of Pittsburgh User on 10/14/2013

journal.publications.chestnet.org CHEST / 144 / 3 / SEPTEMBER 2013 839
with joint contractures in the ICU had a signifi cantly longer ICU LOS and lower ambulatory level at the time of hospital discharge than those without joint contractures.
Nonclinical Studies: Study and Sample Characteristics
Expert Opinion: Three articles, summarized in Table 5 , provided expert opinions regarding the role of physiotherapy in the ICU. 71-73 Gosselink et al 71 sum-marized the fi ndings of the European Respiratory Society and European Society of Intensive Care Medi-cine Task Force on the effectiveness of physiotherapy for acute and chronic critically ill patients. Despite noting a lack of high-level evidence, they identifi ed the following evidence-based targets for physiother-apy: deconditioning, muscle weakness, joint stiffness, impaired airway clearance, atelectasis, intubation avoidance, and weaning failure. The two studies by Hanekom et al 72,73 used a Delphi process to develop evidence-based clinical management algorithms for the prevention, identifi cation, and management of pulmonary dysfunction in intubated patients in the ICU and for the early physical activity and mobiliza-tion of critically ill patients.
Surveys: A total of 15 surveys ( Table 5 ) were iden-tifi ed that evaluated physiotherapy interventions in the ICU. 74-88 Sample sizes ranged from 32 88 to 482; 74 most samples comprised physiotherapists alone, 74-76,78-81,84-86,88 two included physiotherapists and nursing staff, 82,83 one study included ICU directors and physiothera-pists, 77 and the last included patients in the ICU. 87 All studies used purpose-designed surveys. Topics surveyed were general physiotherapy service provision, 74,79,80,82,85 use of passive movements, 75,86 rehabilitation and exer-cise prescription, 78 positioning, 83 VH, 76,84 MH, 88 use of tilt tables, 81 ICU directors’ perceptions of their physiotherapy service, 77 and patient satisfaction with the ICU physiotherapy service. 87 The fi ndings of each study are summarized in Table 5 .
Discussion
This systematic review updates a summary of the research evidence concerning the effectiveness of phys-iotherapy in the ICU published in 2000. A total of 85 new studies (55 clinical and 30 nonclinical) were reviewed.
The most striking change in the evidence base since the review published by Stiller in 2000 1 has been the advent and growth of research, particularly in the last 5 years, evaluating the use of early progressive mobi-lization. In contrast to 2000, when no studies were
Cader et al, 60 in a well-designed prospective RCT involving 41 elderly patients who were mechanically ventilated for . 48 h due to type 1 respiratory failure, found that daily progressive IMT using a thresh-old training device was associated with signifi cant benefi ts (eg, shorter weaning time) compared with a control group. In contrast, the prospective RCT by Caruso et al, 61 whose study sample comprised 25 patients likely to require mechanical ventilation . 72 h, found that IMT using the trigger sensitivity on the venti-lator did not have signifi cant benefi ts in terms of weaning duration or rate of reintubation.
Threshold IMT was found to be effective in terms of weaning ventilator-dependent patients in the case series by Sprague and Hopkins 63 involving six patients, and a single case study by Bissett and Leditschke. 64 Bissett et al, 62 in another case series, evaluated the safety of IMT, with no deleterious effects on physio-logic parameters or clinically important adverse effects recorded.
Neuromuscular Electrical Stimulation: Three clin-ical studies, summarized in Table 4 , were identifi ed that evaluated the effectiveness of NMES. 65-67 There were two prospective, stratifi ed RCTs 65,66 and one within-subject RCT. 67
The RCT by Routsi et al 65 involved 52 critically ill patients, stratifi ed according to age and sex, and evaluated the effect of daily NMES to the quadriceps and peroneous longus muscles. They demonstrated a signifi cantly lower incidence of critical-illness poly-neuromyopathy and reduced weaning time in the treatment group. The stratifi ed RCT by Gruther et al 66 allocated 33 patients to a daily session of NMES to the quadriceps muscle or a sham treatment, with the sample stratifi ed according to ICU LOS. While no signifi cant difference was seen between the treatment and sham groups for short-stay patients ( , 7 days), longer-term patients ( . 14 days) who received NMES had a signif-icant increase in muscle thickness at 4 weeks, whereas the sham group had no signifi cant change in muscle thickness. The within-subject RCT by Poulsen et al, 67 involving eight male patients in the ICU with septic shock, found no signifi cant difference in quadriceps muscle volume between patients’ control and treat-ment sides after 7 days.
Other Clinical Trials: Three other clinical trials that investigated physiotherapy interventions in the ICU are summarized in Table 4 . 68-70 Zeppos et al 68 documented a low incidence of adverse physiologic effects associated with all physiotherapy interven-tions in the ICU; De Freitas 69 found that patients who received physiotherapy were predominantly male, elderly, nonsurgical, and with high disease severity and mortality; and Clavet et al 70 reported that patients
Downloaded From: http://journal.publications.chestnet.org/ by a University of Pittsburgh User on 10/14/2013

840 Original Research
Tabl
e 4—
Cha
ract
eris
tics
of
Stu
dies
Eva
luat
ing
Insp
irat
ory
Mu
scle
Tra
inin
g, N
euro
mu
scu
lar
Ele
ctri
cal
Stim
ula
tion
, and
Oth
er I
nter
vent
ions
Stud
ySt
udy
Des
ign
Part
icip
ants
, No.
, Typ
eIn
terv
entio
nO
utco
mes
Res
ults
Sum
mar
y of
Aut
hors
’ Con
clus
ions
Insp
irat
ory
m
uscl
e tr
aini
ng
Cad
er e
t al 60
Pr
ospe
ctiv
e,
ra
ndom
ized
, co
ntro
lled
tria
l.
41, i
ntub
ated
,
mec
hani
cally
ve
ntila
ted
. 4
8 h,
.
70
y ol
d, ty
pe 1
re
spir
ator
y fa
ilure
.
Con
trol
: usu
al c
are.
MIP
, Ind
ex o
f Tob
in
(R
R/V
t du
ring
a
1-m
in s
pont
aneo
us
brea
thin
g tr
ial)
befo
re a
nd p
ostw
eani
ng,
wea
ning
tim
e.
MIP
incr
ease
d si
gnifi
cant
ly m
ore
in
Rx
grou
p. I
ndex
of T
obin
w
orse
ned
in b
oth
grou
ps, b
ut
sign
ifi ca
ntly
less
so
in R
x gr
oup.
W
eani
ng ti
me
sign
ifi ca
ntly
sh
orte
r in
Rx
grou
p.
In in
tuba
ted
olde
r pe
ople
,
IMT
impr
oves
MIP
and
the
Inde
x of
Tob
in, w
ith a
re
duce
d w
eani
ng ti
me
in
som
e pa
tient
s.
Rx:
IM
T (t
hres
hold
devi
ce, p
rogr
essi
ve
resi
stan
ce),
5 m
in
bid,
7 d
/wk.
C
arus
o et
al 61
Pr
ospe
ctiv
e,
ra
ndom
ized
, co
ntro
lled
tria
l.
25, l
ikel
y to
req
uire
mec
hani
cal
vent
ilatio
n .
72
h.
Con
trol
: usu
al c
are.
MIP
dai
ly u
ntil
wea
ned,
wea
ning
dur
atio
n,
rein
tuba
tion
rate
.
No
sign
ifi ca
nt d
iffer
ence
bet
wee
n
grou
ps fo
r an
y ou
tcom
e.IM
T fr
om th
e be
ginn
ing
of
m
echa
nica
l ven
tilat
ion
did
not s
hort
en w
eani
ng d
urat
ion
or d
ecre
ase
rein
tuba
tion
rate
.
Rx:
IM
T (i
nspi
rato
ry
tr
igge
r se
nsiti
vity
on
ven
tilat
or,
prog
ress
ive
resi
stan
ce),
up to
30
min
per
se
ssio
n bi
d.
Bis
sett
et a
l 62
Cas
e se
ries
10, t
rach
eost
omiz
ed,
ve
ntila
tor
depe
nden
t.
IMT
(thr
esho
ld
de
vice
, pro
gres
sive
re
sist
ance
), da
ily,
5-6
d/w
k.
HR
, MA
P, S
p o 2 ,
RR
befo
re a
nd p
ost-
sess
ions
un
til w
eane
d, a
dver
se
even
ts.
HR
, MA
P, S
p o 2 ,
RR
: no
si
gnifi
cant
cha
nge.
Adv
erse
ev
ents
: 0%
.
Thr
esho
ld I
MT
can
be
de
liver
ed s
afel
y in
se
lect
ed v
entil
ator
-dep
ende
nt
patie
nts.
Sp
ragu
e an
d H
opki
ns 63
C
ase
seri
es.
6, tr
ache
osto
miz
ed,
ve
ntila
tor
depe
nden
t.
IMT
(thr
esho
ld
de
vice
, pro
gres
sive
re
sist
ance
), 30
-50
min
pe
r se
ssio
n, d
aily
, 6-
7 d/
wk.
Wea
ning
suc
cess
,
trai
ning
pre
ssur
es,
MIP
.
All
patie
nts
wer
e w
eane
d fr
om
th
e ve
ntila
tor
afte
r in
itiat
ion
of I
MT.
Mea
n tr
aini
ng p
ress
ures
an
d M
IP in
crea
sed
over
tim
e.
IMT
may
pro
mot
e w
eani
ng
in
pat
ient
s w
ho a
re
vent
ilato
r-de
pend
ent.
B
isset
t and
Led
itsch
ke 64
Si
ngle
case
stu
dy.
1, tr
ache
osto
miz
ed,
ve
ntila
tor
depe
nden
t.
IMT
(thr
esho
ld
de
vice
, pro
gres
sive
re
sist
ance
), up
to
30 m
in p
er s
essi
on,
daily
, 7 d
/wk.
Wea
ning
suc
cess
.W
eane
d of
f mec
hani
cal v
entil
atio
n
afte
r in
itiat
ion
of I
MT.
IMT
sho
uld
be c
onsi
dere
d as
a th
erap
eutic
str
ateg
y fo
r ve
ntila
tor-
depe
nden
t pat
ient
s.
Neu
rom
uscu
lar
el
ectr
ical
stim
ulat
ion
R
outs
i et a
l 65
Pros
pect
ive,
stra
tifi e
d,
rand
omiz
ed,
cont
rolle
d tr
ial.
52, m
echa
nica
lly
ve
ntila
ted,
A
PAC
HE
II
scor
e �
13.
Str
atifi
ed
acco
rdin
g to
age
an
d se
x.
Con
trol
:
no in
terv
entio
n.M
RC
mus
cle
stre
ngth
,
freq
uenc
y of
cr
itica
l illn
ess
poly
neur
omyo
path
y,
wea
ning
per
iod,
du
ratio
n of
mec
hani
cal
vent
ilatio
n, I
CU
LO
S.
MR
C s
core
sig
nifi c
antly
hig
her
in
Rx
grou
p. I
ncid
ence
of
poly
neur
omyo
path
y si
gnifi
cant
ly
low
er in
Rx
grou
p. W
eani
ng
peri
od s
igni
fi can
tly s
hort
er in
R
x gr
oup.
No
sign
ifi ca
nt
diff
eren
ce b
etw
een
grou
ps
for
othe
r ou
tcom
es.
Dai
ly N
ME
S ca
n pr
even
t cri
tical
illne
ss p
olyn
euro
myo
path
y in
cri
tical
ly il
l pat
ient
s an
d ca
n sh
orte
n th
e du
ratio
n of
wea
ning
.R
x: N
ME
S to
quad
rice
ps a
nd
pero
neou
s lo
ngus
bi
late
rally
, 55
min
dai
ly.
(Con
tinu
ed)
Downloaded From: http://journal.publications.chestnet.org/ by a University of Pittsburgh User on 10/14/2013

journal.publications.chestnet.org CHEST / 144 / 3 / SEPTEMBER 2013 841
Stud
ySt
udy
Des
ign
Part
icip
ants
, No.
, Typ
eIn
terv
entio
nO
utco
mes
Res
ults
Sum
mar
y of
Aut
hors
’ Con
clus
ions
G
ruth
er e
t al 66
Pr
ospe
ctiv
e,
st
ratifi
ed,
ra
ndom
ized
, co
ntro
lled
tria
l.
33, s
trat
ifi ed
acco
rdin
g to
IC
U L
OS:
acu
te
subg
roup
: IC
U
LO
S ,
7 d
; lo
ng-t
erm
su
bgro
up: I
CU
L
OS
. 1
4 d.
Con
trol
: sha
m
st
imul
atio
n.Q
uadr
icep
s m
uscl
e
laye
r th
ickn
ess
(ultr
ason
ogra
phy)
at
base
line
and
4 w
k.
Acu
te s
ubgr
oup:
mus
cle
th
ickn
ess
sign
ifi ca
ntly
de
crea
sed
over
tim
e in
bot
h gr
oups
, no
sign
ifi ca
nt d
iffer
ence
be
twee
n gr
oups
. Lon
g-te
rm
subg
roup
: mus
cle
thic
knes
s si
gnifi
cant
ly in
crea
sed
over
tim
e in
Rx
grou
p bu
t not
con
trol
gr
oup,
thic
knes
s si
gnifi
cant
ly
grea
ter
in R
x gr
oup
at 4
wk.
NM
ES
coul
d be
an
effe
ctiv
e
adju
nct i
n IC
U to
rev
erse
m
uscl
e w
astin
g in
lo
ng-t
erm
pat
ient
s.R
x: N
ME
S to
quad
rice
ps, d
aily
, 5
d/w
k fo
r 4
wk.
Po
ulse
n et
al 67
W
ithin
-sub
ject
,
rand
omiz
ed,
cont
rolle
d tr
ial.
8, m
echa
nica
lly
ve
ntila
ted,
sep
tic
shoc
k, p
redi
cted
IC
U L
OS
� 7
d.
Con
trol
sid
e: n
o
inte
rven
tion.
Qua
dric
eps
mus
cle
vo
lum
e (C
T im
age)
at
day
s 1
and
7.
Mus
cle
volu
me
sign
ifi ca
ntly
decr
ease
d ov
er ti
me.
N
o si
gnifi
cant
diff
eren
ce
betw
een
grou
ps.
Los
s of
mus
cle
mas
s in
pat
ient
s
with
sep
tic s
hock
was
una
ffec
ted
by N
ME
S.R
x si
de: N
ME
S to
quad
rice
ps, 6
0 m
in,
daily
for
7 d.
Oth
er in
terv
entio
ns
Zepp
os e
t al 68
Pr
ospe
ctiv
e,
ob
serv
atio
nal
stud
y.
Any
pat
ient
in th
e
ICU
rec
eivi
ng P
T
inte
rven
tion.
Any
PT
inte
rven
tion.
Adv
erse
eve
nts.
12,2
81 in
terv
entio
ns p
rovi
ded.
Adv
erse
eve
nts:
0.2
%.
PT in
terv
entio
n in
IC
U is
saf
e.
D
e F
reita
s 69
Pros
pect
ive,
obse
rvat
iona
l st
udy.
146,
any
pat
ient
s in
the
ICU
rec
eivi
ng
PT in
terv
entio
n.
Not
sta
ted.
APA
CH
E I
I in
dex.
APA
CH
E I
I in
dex
scor
es
re
fl ect
ed s
ever
e di
seas
e in
pa
tient
s re
ceiv
ing
PT.
Prov
ided
des
crip
tive
data
for
pa
tient
s in
IC
U r
ecei
ving
PT.
C
lave
t et a
l 70
Ret
rosp
ectiv
e,
ch
art r
evie
w.
155,
IC
U
L
OS
� 1
4 d.
Not
app
licab
le.
Am
bula
tory
sta
tus
at
ho
spita
l DC
acc
ordi
ng
to p
rese
nce/
abse
nce
of jo
int c
ontr
actu
res
in I
CU
, IC
U L
OS.
Sign
ifi ca
ntly
mor
e pa
tient
s w
ith
co
ntra
ctur
es in
IC
U h
ad a
low
am
bula
tory
leve
l at h
ospi
tal
DC
than
thos
e w
ithou
t co
ntra
ctur
es. I
CU
LO
S si
gnifi
cant
ly lo
nger
in th
ose
with
con
trac
ture
s.
The
dev
elop
men
t of j
oint
cont
ract
ures
in I
CU
adv
erse
ly
affe
cted
am
bula
tory
sta
tus
at D
C fr
om h
ospi
tal.
APA
CH
E 5
Acu
te P
hysi
olog
ic a
nd C
hron
ic H
ealth
Eva
luat
ion;
IM
T 5
insp
irat
ory
mus
cle
trai
ning
; M
IP 5
max
imal
ins
pira
tory
pre
ssur
e; M
RC
5 M
edic
al R
esea
rch
Cou
ncil;
NM
ES
5 n
euro
mus
cula
r el
ectr
ical
stim
ulat
ion.
See
Tab
le 1
-3 le
gend
s fo
r ex
pans
ion
of o
ther
abb
revi
atio
ns.
Tabl
e 4—
Con
tinu
ed
Downloaded From: http://journal.publications.chestnet.org/ by a University of Pittsburgh User on 10/14/2013

842 Original Research
Tabl
e 5—
Cha
ract
eris
tics
of
Non
clin
ical
Stu
dies
Stud
yPa
rtic
ipan
ts, N
o., T
ype
Topi
cSu
mm
ary
of R
esul
ts
Exp
ert o
pini
on
Gos
selin
k et
al 71
10
, ER
S an
d E
SIC
M ta
skfo
rce.
PT fo
r cr
itica
lly il
l pat
ient
s.D
espi
te a
lack
of h
igh-
leve
l evi
denc
e, th
e fo
llow
ing
evid
ence
-bas
ed ta
rget
s fo
r
PT w
ere
iden
tifi e
d: d
econ
ditio
ning
, mus
cle
wea
knes
s, jo
int s
tiffn
ess,
impa
ired
ai
rway
cle
aran
ce, a
tele
ctas
is, i
ntub
atio
n av
oida
nce,
and
wea
ning
failu
re.
H
anek
om e
t al 72
7,
Del
phi p
anel
ists
.C
linic
al m
anag
emen
t alg
orith
m fo
r
the
prev
entio
n, id
entifi
cat
ion,
and
m
anag
emen
t of p
ulm
onar
y dy
sfun
ctio
n in
pat
ient
s in
the
ICU
.
The
pan
elis
ts a
gree
d on
a s
erie
s of
sta
tem
ents
con
cern
ing
the
indi
catio
ns,
te
chni
que
and
dosa
ge o
f PT
Rxs
for
man
agin
g pu
lmon
ary
dysf
unct
ion
in
intu
bate
d pa
tient
s in
IC
U.
H
anek
om e
t al 73
7,
Del
phi p
anel
ists
.C
linic
al m
anag
emen
t alg
orith
m fo
r
the
earl
y m
obili
zatio
n of
cri
tical
ly
ill p
atie
nts.
The
pan
elis
ts c
oncl
uded
that
an
indi
vidu
al m
obili
zatio
n pl
an m
ust b
e de
velo
ped
fo
r ea
ch p
atie
nt a
dmitt
ed to
an
ICU
, and
mad
e a
case
that
ear
ly p
hysi
cal a
ctiv
ity
and
mob
iliza
tion
shou
ld b
e th
e fo
unda
tion
pilla
rs o
f PT
man
agem
ent i
n IC
U.
Surv
eys
H
odgi
n et
al 74
48
2, U
S PT
s w
orki
ng w
ith c
ritic
ally
ill p
atie
nts.
Cur
rent
PT
pra
ctic
es fo
r pa
tient
s
reco
veri
ng fr
om c
ritic
al il
lnes
s in
th
e U
S.
PT w
as c
omm
only
adm
inis
tere
d to
pat
ient
s in
the
ICU
dur
ing
thei
r re
cove
ry.
89
% r
equi
red
med
ical
ref
erra
l to
initi
ate
PT. T
he fr
eque
ncy
and
type
of
inte
rven
tion
vari
ed b
ased
on
hosp
ital t
ype
and
the
clin
ical
sce
nari
o.
Stoc
kley
et a
l 75
165,
PTs
wor
king
in U
K I
CU
s.C
urre
nt u
se o
f pas
sive
mov
emen
ts
in
UK
IC
Us.
92%
rou
tinel
y tr
eate
d ve
ntila
ted,
sed
ated
pat
ient
s in
IC
Us.
Of t
hese
, 99%
use
d
pass
ive
mov
emen
ts r
outin
ely
and
78%
per
form
ed p
assi
ve m
ovem
ents
dai
ly.
Join
ts m
ost c
omm
only
trea
ted
wer
e th
e sh
ould
er, h
ip, k
nee,
elb
ow, a
nd a
nkle
, fo
r a
med
ian
of 5
tim
es p
er a
rea,
and
join
ts w
ere
take
n to
the
end
of R
OM
. 78
% m
onito
red
the
effe
cts
of p
assi
ve m
ovem
ents
, with
HR
and
BP
mos
t fr
eque
ntly
mon
itore
d.
Hay
es e
t al 76
16
5, s
enio
r PT
s w
orki
ng in
Aus
tral
ian
or
NZ
ICU
s.C
urre
nt P
T p
ract
ice
with
res
pect
to
V
H, b
arri
ers
to it
s us
e, d
escr
iptio
n of
its
tech
niqu
e in
Aus
tral
ia a
nd N
Z.
Onl
y 21
% u
sed
VH
. Lac
k of
trai
ning
and
med
ical
app
rova
l wer
e th
e m
ain
barr
iers
to it
s us
e. W
hen
VH
was
use
d, it
s ap
plic
atio
n va
ried
con
side
rabl
y be
twee
n re
spon
dent
s.
Jone
s 77
54 d
irec
tors
and
103
sen
ior
PT
s in
Aus
tral
ian,
UK
, Can
adia
n,
Hon
g K
ong,
and
So
uth
Afr
ican
IC
Us.
ICU
dir
ecto
rs’ p
erce
ptio
n of
thei
r
PT s
ervi
ce. S
enio
r PT
s’ qu
alifi
catio
ns,
expe
rien
ce, r
esea
rch,
teac
hing
, and
jo
b ov
erla
p.
79%
of I
CU
dir
ecto
rs th
ough
t the
PT
ser
vice
was
out
stan
ding
or
very
goo
d.
Se
cret
ion
rem
oval
was
see
n as
the
PTs’
mai
n ro
le. 6
0% b
elie
ved
the
PTs’
wor
k co
uld
be c
over
ed b
y ot
her
disc
iplin
es.
40%
of P
Ts w
ere
awar
e of
mer
ging
pro
fess
iona
l bou
ndar
ies.
Sk
inne
r et
al 78
11
1, P
Ts w
orki
ng in
Aus
tral
ian
ICU
s.E
xerc
ise
pres
crip
tion
by P
Ts fo
r
patie
nts
in th
e IC
U in
Aus
tral
ia.
94%
pre
scri
bed
exer
cise
rou
tinel
y fo
r pa
tient
s in
IC
U, w
ith a
ctiv
e,
ac
tive-
assi
sted
exe
rcis
es, a
nd m
obili
zatio
n (e
g, s
it to
sta
nd, s
it on
edg
e of
bed
) m
ost c
omm
only
pre
scri
bed.
34%
rou
tinel
y us
ed o
utco
me
mea
sure
s to
mon
itor
exer
cise
pre
scri
ptio
n, in
clud
ing
Sp o
2 , R
R, a
nd fu
nctio
nal t
ests
.
Nor
renb
urg
and
Vinc
ent 79
10
2, P
Ts w
orki
ng in
Eur
opea
n IC
Us.
Profi
le a
nd r
ole
of P
Ts in
Eur
opea
n IC
Us.
The
pro
fi le
and
role
of P
Ts in
IC
U v
arie
d ac
ross
Eur
ope.
100
% r
epor
ted
that
PTs
wer
e in
volv
ed in
the
prov
isio
n of
res
pira
tory
ther
apy,
pos
ition
ing,
and
m
obili
zatio
n.
Kum
ar e
t al 80
89
, PTs
wor
king
in I
ndia
n IC
Us.
Rol
e of
PTs
in I
ndia
n IC
Us.
55%
req
uire
d m
edic
al r
efer
ral t
o in
itiat
e th
e pr
ovis
ion
of P
T. 9
1% w
ere
in
volv
ed in
the
prov
isio
n of
res
pira
tory
ther
apy
and
100%
in th
e pr
ovis
ion
of
mob
iliza
tion.
C
hang
et a
l 81
86, s
enio
r PT
s w
orki
ng in
Aus
tral
ian
ICU
s.U
se o
f tilt
tabl
es in
the
PT m
anag
emen
t
of p
atie
nts
in th
e IC
U in
Aus
tral
ia.
67%
use
d til
t tab
les
to a
ssis
t sta
ndin
g an
d m
obili
zatio
n. T
ilt ta
bles
wer
e m
ost
fr
eque
ntly
use
d to
faci
litat
e w
eigh
t bea
ring
, pre
vent
mus
cle
cont
ract
ures
, im
prov
e lo
wer
lim
b st
reng
th, a
nd in
crea
se a
rous
al. T
itle
tabl
es m
ost f
requ
ently
ap
plie
d to
pat
ient
s w
ith n
euro
logi
c co
nditi
ons
or p
rolo
nged
IC
U L
OS.
(Con
tinu
ed)
Downloaded From: http://journal.publications.chestnet.org/ by a University of Pittsburgh User on 10/14/2013

journal.publications.chestnet.org CHEST / 144 / 3 / SEPTEMBER 2013 843
Stud
yPa
rtic
ipan
ts, N
o., T
ype
Topi
cSu
mm
ary
of R
esul
ts
C
habo
yer
et a
l 82
71 n
urse
man
ager
s, 6
PTs
wor
king
in A
ustr
alia
n IC
Us.
Ava
ilabi
lity
of P
T s
ervi
ces
in I
CU
s an
d
role
of P
Ts a
nd n
ursi
ng s
taff
in p
rovi
sion
of
“ch
est P
T”
in A
ustr
alia
.
87%
had
wee
kday
PT
cov
er, 6
6% h
ad w
eeke
nd P
T c
over
, , 1
0% h
ad e
veni
ng
PT
cov
er. N
urse
s w
ere
invo
lved
in a
ll as
pect
s of
“ch
est P
T.”
PTs
wer
e m
ost
freq
uent
ly in
volv
ed in
the
prov
isio
n of
mob
iliza
tion,
che
st w
all v
ibra
tions
, po
sitio
ning
, per
cuss
ion,
and
suc
tion.
T
hom
as e
t al 83
71
, PTs
and
nur
ses
wor
king
in
A
ustr
alia
n IC
Us.
Use
of p
ositi
onin
g in
Aus
tral
ian
ICU
s.86
% b
elie
ved
patie
nts
shou
ld b
e tu
rned
eve
ry 2
h. P
ositi
ons
mos
t fre
quen
tly
us
ed o
n a
daily
bas
is w
ere
a qu
arte
r tu
rn fr
om s
upin
e, s
upin
e w
ith th
e he
ad o
f be
d el
evat
ed 3
0°, a
nd s
ittin
g ou
t of b
ed.
D
enni
s et
al 84
64
, PTs
wor
king
in A
ustr
alia
n IC
Us.
Prev
alen
ce o
f usi
ng V
H d
urin
g PT
Rxs
in A
ustr
alia
n IC
Us.
39%
use
d V
H d
urin
g PT
Rxs
. VH
mos
t fre
quen
tly u
sed
in th
e se
ttin
g of
spu
tum
rete
ntio
n an
d re
spir
ator
y in
fect
ion.
M
atila
inen
and
Ols
eni 85
57
, PTs
wor
king
in S
wed
ish
ICU
s.Pr
ofes
sion
al r
ole
and
educ
atio
nal
pr
efer
ence
s of
Sw
edis
h IC
U P
Ts.
89%
of I
CU
PTs
als
o w
orke
d in
oth
er c
linic
al a
reas
. Tim
e sp
ent i
n IC
U r
ange
d
from
5-4
0 h/
wk.
100
% w
ere
invo
lved
in th
e pr
ovis
ion
of r
espi
rato
ry th
erap
y,
mob
iliza
tion,
and
lim
b ex
erci
ses.
W
iles
and
Still
er 86
51
, PTs
wor
king
in A
ustr
alia
n IC
Us.
Use
of p
assi
ve m
ovem
ents
in
A
ustr
alia
n IC
Us.
35%
rou
tinel
y as
sess
ed p
assi
ve li
mb
RO
M o
f all
patie
nts
in th
e IC
U. 1
4%
ro
utin
ely
prov
ided
pas
sive
lim
b ex
erci
ses
as a
Rx
for
all p
atie
nts
in th
e IC
U.
Pres
crip
tion
of p
assi
ve li
mb
RO
M e
xerc
ises
was
var
iabl
e be
twee
n re
spon
dent
s.
Still
er a
nd W
iles 87
35
, pat
ient
s in
the
ICU
.Pa
tient
sat
isfa
ctio
n w
ith P
T s
ervi
ce in
an I
CU
.T
here
was
a h
igh
degr
ee o
f sat
isfa
ctio
n w
ith th
e pe
rson
al c
hara
cter
istic
s of
the
PTs
seen
and
the
PT s
ervi
ce p
rovi
ded
in I
CU
.
Hod
gson
et a
l 88
32, P
Ts w
orki
ng in
Aus
tral
ian
ICU
s.U
se o
f MH
by
PTs
in A
ustr
alia
n IC
Us.
91%
use
d M
H a
s a
Rx
tech
niqu
e. 7
6% u
sed
MH
as
a ro
utin
e R
x fo
r ve
ntila
ted
pa
tient
s. T
here
was
str
ong
agre
emen
t bet
wee
n re
spon
dent
s on
the
com
pone
nts
of M
H, p
refe
rred
Rx
posi
tions
, con
trai
ndic
atio
ns, a
nd p
erce
ived
be
nefi t
s. T
here
was
con
side
rabl
e va
riat
ion
betw
een
resp
onde
nts
in th
e du
ratio
n, n
umbe
r of
bre
aths
, and
cir
cuits
use
d w
hen
perf
orm
ing
MH
.
ER
S 5
Eur
opea
n R
espi
rato
ry S
ocie
ty; E
SIC
M 5
Eur
opea
n So
ciet
y of
Int
ensi
ve C
are
Med
icin
e; N
Z 5
New
Zea
land
; UK
5 U
nite
d K
ingd
om; U
S 5
Uni
ted
Stat
esct
. See
Tab
le 1
-4 le
gend
s fo
r ex
pans
ion
of
othe
r ab
brev
iatio
ns.
Tabl
e 5—
Con
tinu
ed
Downloaded From: http://journal.publications.chestnet.org/ by a University of Pittsburgh User on 10/14/2013

844 Original Research
Limitations of this systematic review included the variable methodological quality of the studies. The diverse range of study samples and study methodology precluded pooling of results and statistical analysis. The interventions that were provided usually com-prised numerous components, making it impossible to determine the effectiveness of individual treatment components.
A strength of this literature review was the inclu-sion of all clinical studies that have evaluated physio-therapy for adult patients in the ICU, irrespective of study design. Additionally, by reviewing the evidence concerning a broad range of physiotherapy practice, rather than focusing on one specifi c type of interven-tion (eg, multimodality respiratory physiotherapy or mobilization alone), it has been possible to highlight the emerging evidence concerning the benefi cial effects of early progressive mobilization compared with other physiotherapy interventions.
Conclusions
In summary, the evidence concerning the effi cacy of routine multimodality respiratory physiotherapy for adult, intubated patients receiving mechanical venti-lation remains unclear. There is strong, albeit limited, evidence published since the review in 2000 showing that physiotherapy intervention focusing on early pro-gressive mobilization is feasible and safe, and results in signifi cant functional benefi ts, which may translate into a reduced ICU and hospital LOS. This emerging evidence confi rms the role of the physiotherapist in ICU and highlights that early progressive mobiliza-tion is an effective area of physiotherapy clinical prac-tice for adult, intubated, mechanically ventilated patients. Further research to confi rm the effi cacy of early progressive mobilization is required, in partic-ular to determine the optimal “dosage” in terms of its most effective components, intensity, duration, and frequency.
Acknowledgments Author contributions: Dr Stiller had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Dr Stiller: contributed to the literature search, identifi cation of relevant studies, data extraction, analysis of the results, and writ-ing of the paper. Financial/nonfi nancial disclosures: The author has reported to CHEST that no potential confl icts of interest exist with any com-panies/organizations whose products or services may be discussed in this article . Other contributions: The author would like to thank Alisia Jedrzejczak, BPhysio (Hons), and Kate Roberts, BAppSc (Physio), BSc, for their helpful comments regarding this paper.
References 1 . Stiller K . Physiotherapy in intensive care: towards an evidence-
based practice . Chest . 2000 ; 118 ( 6 ): 1801 - 1813 .
identifi ed, the current review included 26 clinical studies on this topic and, while study quality was var-iable, statistically signifi cant and clinically important benefi ts resulting from early mobilization were dem-onstrated. These new clinical studies have shown that early progressive mobilization is feasible and safe, and results in signifi cant functional benefi ts that may trans-late into positive effects on the ICU and hospital LOS. Stiller 1 noted that the role of physiotherapy in the ICU would continue to be questioned until physio-therapy has been shown to have a favorable impact on broader outcomes of patients in the ICU. The new evidence demonstrating the benefi cial effects of mobilization on broader outcomes such as the ICU and hospital LOS confi rms an unquestionable role for physiotherapy in the ICU. Given that the demand for physiotherapy services often outstrips the resources available, and the new evidence demonstrating the effectiveness of physiotherapy interventions aimed at early mobilization, ICU physiotherapists should give priority to interventions aimed at early progres-sive mobilization. To be successful, implementation of early progressive mobilization relies on an ICU culture that considers mobilization an essential part of multidisciplinary care. Safety guidelines and pro-tocols for progressive mobilization of patients in the ICU are available. 34,37,42,47,89
Eighteen new clinical trials were identifi ed that eval-uated the effectiveness of multimodality respiratory physiotherapy for adult, intubated, mechanically ven-tilated patients in the ICU. The results of these trials support and extend the conclusions made by Stiller in 2000, 1 namely, that multimodality respiratory phys-iotherapy may result in short-term improvements in pulmonary function. While there is some new evidence from RCTs that the provision of routine multimodal-ity respiratory physiotherapy can impact positively on outcomes such as duration of intubation and the ICU LOS, there is, however, a similar amount of new high-quality evidence suggesting that it may not. In terms of specifi c respiratory physiotherapy interven-tions, there is limited evidence from new randomized crossover trials suggesting that expiratory rib-cage compression is ineffective and that MH may have benefi cial short-term effects on respiratory compli-ance, concurring with the conclusions made in the 2000 review. 1 New evidence has emerged demon-strating that VH is as effective as MH. There is new high-quality evidence concerning the effectiveness of IMT for patients in the ICU; however, this evidence is scarce, hence the routine or selective use of IMT for patients in the ICU cannot be recommended at present. Similarly, the evidence that has been published since 1999 concerning the effectiveness of NMES is limited and, thus, clinical recommendations regarding its use in ICU cannot be made.
Downloaded From: http://journal.publications.chestnet.org/ by a University of Pittsburgh User on 10/14/2013

journal.publications.chestnet.org CHEST / 144 / 3 / SEPTEMBER 2013 845
23 . Genc A , Akan M , Gunerli A . The effects of manual hyperin-fl ation with or without rib-cage compression in mechanically ventilated patients . Ital J Physiother. 2011 ; 1 ( 2 ): 48 - 54 .
24 . Berney S , Denehy L , Pretto J . Head-down tilt and manual hyperinfl ation enhance sputum clearance in patients who are intubated and ventilated . Aust J Physiother . 2004 ; 50 ( 1 ): 9 - 14 .
25 . Hodgson C , Ntoumenopoulos G , Dawson H , Paratz J . The Mapleson C circuit clears more secretions than the Laerdal circuit during manual hyperinfl ation in mechanically-ventilated patients: a randomised cross-over trial . Aust J Physiother . 2007 ; 53 ( 1 ): 33 - 38 .
26 . Berney S , Denehy L . A comparison of the effects of manual and ventilator hyperinfl ation on static lung compliance and sputum production in intubated and ventilated intensive care patients . Physiother Res Int . 2002 ; 7 ( 2 ): 100 - 108 .
27 . Hodgson C , Denehy L , Ntoumenopoulos G , Santamaria J , Carroll S . An investigation of the early effects of manual lung hyperinfl ation in critically ill patients . Anaesth Intensive Care . 2000 ; 28 ( 3 ): 255 - 261 .
28 . Choi JS-P , Jones AY-M . Effects of manual hyperinfl ation and suctioning in respiratory mechanics in mechanically ven-tilated patients with ventilator-associated pneumonia . Aust J Physiother . 2005 ; 51 ( 1 ): 25 - 30 .
29 . Savian C , Paratz J , Davies A . Comparison of the effectiveness of manual and ventilator hyperinfl ation at different levels of positive end-expiratory pressure in artifi cially ventilated and intubated intensive care patients . Heart Lung . 2006 ; 35 ( 5 ): 334 - 341 .
30 . Ntoumenopoulos G , Presneill JJ , McElholum M , Cade JF . Chest physiotherapy for the prevention of ventilator-associated pneumonia . Intensive Care Med . 2002 ; 28 ( 7 ): 850 - 856 .
31 . Malkoç M , Karadibak D , Yildirim Y . The effect of physio-therapy on ventilatory dependency and the length of stay in an intensive care unit . Int J Rehabil Res . 2009 ; 32 ( 1 ): 85 - 88 .
32 . Thomas PJ , Paratz JD , Lipman J , Stanton WR . Lateral posi-tioning of ventilated intensive care patients: a study of oxy-genation, respiratory mechanics, hemodynamics, and adverse events . Heart Lung . 2007 ; 36 ( 4 ): 277 - 286 .
33 . Clarke RCN , Kelly BE , Convery PN , Fee JPH . Ventilatory char-acteristics in mechanically ventilated patients during manual hyperventilation for chest physiotherapy . Anaesthesia . 1999 ; 54 ( 10 ): 936 - 940 .
34 . Schweickert WD , Pohlman MC , Pohlman AS , et al. Early physical and occupational therapy in mechanically ventilated, critically ill patients: a randomised controlled trial . Lancet . 2009 ; 373 ( 9678 ): 1874 - 1882 .
35 . Burtin C , Clerckx B , Robbeets C , et al . Early exercise in criti-cally ill patients enhances short-term functional recovery . Crit Care Med . 2009 ; 37 ( 9 ): 2499 - 2505 .
36 . Chang M-Y , Chang L-Y , Huang Y-C , Lin K-M , Cheng C-H . Chair-sitting exercise intervention does not improve respira-tory muscle function in mechanically ventilated intensive care unit patients . Respir Care . 2011 ; 56 ( 10 ): 1533 - 1538 .
37 . Morris PE , Goad A , Thompson C , et al . Early intensive care unit mobility therapy in the treatment of acute respiratory failure . Crit Care Med . 2008 ; 36 ( 8 ): 2238 - 2243 .
38 . Yang P-H , Wang C-S , Wang Y-C , et al . Outcome of physical therapy intervention on ventilator weaning and functional status . Kaohsiung J Med Sci . 2010 ; 26 ( 7 ): 366 - 372 .
39 . Winkelman C , Johnson KD , Hejal R , et al . Examining the positive effects of exercise in intubated adults in ICU: a pro-spective repeated measures clinical study . Intensive Crit Care Nurs . 2012 ; 28 ( 6 ): 307 - 318 .
40 . Needham DM , Korupolu R , Zanni JM , et al . Early physical medicine and rehabilitation for patients with acute respira-tory failure: a quality improvement project . Arch Phys Med Rehabil . 2010 ; 91 ( 4 ): 536 - 542 .
2 . National Health and Medical Research Council . How to use the evidence: assessment and application of scientifi c evidence. 2000 . National Health and Medical Research Council website. http://www.nhmrc.gov.au/_fi les_nhmrc/publications/attachments/cp69.pdf . Accessed October 1, 2012.
3 . Schulz KF , Altman DG , Moher D ; CONSORT Group . CONSORT 2010 statement: updated guidelines for report-ing parallel group randomized trials . Ann Intern Med . 2010 ; 152 ( 11 ): 726 - 732 .
4 . Adler J , Malone D . Early mobilization in the intensive care unit: a systematic review . Cardiopulm Phys Ther J . 2012 ; 23 ( 1 ): 5 - 13 .
5 . Amidei C . Measurement of physiologic responses to mobili-sation in critically ill adults . Intensive Crit Care Nurs . 2012 ; 28 ( 2 ): 58 - 72 .
6 . Amidei C . Mobilisation in critical care: a concept analysis . Intensive Crit Care Nurs . 2012 ; 28 ( 2 ): 73 - 81 .
7 . Choi J , Tasota FJ , Hoffman LA . Mobility interventions to improve outcomes in patients undergoing prolonged mechan-ical ventilation: a review of the literature . Biol Res Nurs . 2008 ; 10 ( 1 ): 21 - 33 .
8 . O’Connor ED , Walsham J . Should we mobilise critically ill patients? A review . Crit Care Resusc . 2009 ; 11 ( 4 ): 290 - 300 .
9 . Thomas AJ . Exercise intervention in the critical care unit - what is the evidence? Phys Ther Rev . 2009 ; 14 ( 1 ): 50 - 59 .
10 . Thomas AJ . Physiotherapy led early rehabilitation of the patient with critical illness . Phys Ther Rev . 2011 ; 16 ( 1 ): 46 - 57 .
11 . Clini E , Ambrosino N . Early physiotherapy in the respiratory intensive care unit . Respir Med . 2005 ; 99 ( 9 ): 1096 - 1104 .
12 . Paulus F , Binnekade JM , Vroom MB , Schultz MJ . Benefi ts and risks of manual hyperinfl ation in intubated and mechani-cally ventilated intensive care unit patients: a systematic review . Crit Care . 2012 ; 16 ( 4 ): R145 .
13 . Elliott D , Denehy L , Berney S , Alison JA . Assessing physical function and activity for survivors of a critical illness: a review of instruments . Aust Crit Care . 2011 ; 24 ( 3 ): 155 - 166 .
14 . Hanekom SD , Faure M , Coetzee A . Outcomes research in the ICU: an aid in defi ning the role of physiotherapy . Physiother Theory Pract . 2007 ; 23 ( 3 ): 125 - 135 .
15 . Hellweg S . Effectiveness of physiotherapy and occupational therapy after traumatic brain injury in the intensive care unit . Crit Care Res Pract . 2012 ; 2012 : 768456 .
16 . Patman S , Sanderson D , Blackmore M . Physiotherapy follow-ing cardiac surgery: is it necessary during the intubation period? Aust J Physiother . 2001 ; 47 ( 1 ): 7 - 16 .
17 . Templeton M , Palazzo MGA . Chest physiotherapy pro-longs duration of ventilation in the critically ill ventilated for more than 48 hours . Intensive Care Med . 2007 ; 33 ( 11 ): 1938 - 1945 .
18 . Patman S , Jenkins S , Stiller K . Physiotherapy does not prevent, or hasten recovery from, ventilator-associated pneumonia in patients with acquired brain injury . Intensive Care Med . 2009 ; 35 ( 2 ): 258 - 265 .
19 . Pattanshetty RB , Gaude GS . Effect of multimodality chest phys-iotherapy in prevention of ventilator-associated pneumonia: A randomized clinical trial . Indian J Crit Care Med . 2010 ; 14 ( 2 ): 70 - 76 .
20 . Barker M , Adams S . An evaluation of a single chest phys-iotherapy treatment on mechanically ventilated patients with acute lung injury . Physiother Res Int . 2002 ; 7 ( 3 ): 157 - 169 .
21 . Dennis D , Jacob W , Budgeon C . Ventilator versus manual hyperinfl ation in clearing sputum in ventilated intensive care unit patients . Anaesth Intensive Care . 2012 ; 40 ( 1 ): 142 - 149 .
22 . Unoki T , Kawasaki Y , Mizutani T , et al . Effects of expiratory rib-cage compression on oxygenation, ventilation, and airway-secretion removal in patients receiving mechanical ventila-tion . Respir Care . 2005 ; 50 ( 11 ): 1430 - 1437 .
Downloaded From: http://journal.publications.chestnet.org/ by a University of Pittsburgh User on 10/14/2013

846 Original Research
60 . Cader SA , Vale RG , Castro JC , et al . Inspiratory muscle training improves maximal inspiratory pressure and may assist weaning in older intubated patients: a randomised trial . J Physiother . 2010 ; 56 ( 3 ): 171 - 177 .
61 . Caruso P , Denari SDC , Ruiz SAL , et al . Inspiratory muscle training is ineffective in mechanically ventilated critically ill patients . Clinics (Sao Paulo) . 2005 ; 60 ( 6 ): 479 - 484 .
62 . Bissett B , Leditschke IA , Green M . Specifi c inspiratory mus-cle training is safe in selected patients who are ventilator-dependent: a case series . Intensive Crit Care Nurs . 2012 ; 28 ( 2 ): 98 - 104 .
63 . Sprague SS , Hopkins PD . Use of inspiratory strength training to wean six patients who were ventilator-dependent . Phys Ther . 2003 ; 83 ( 2 ): 171 - 181 .
64 . Bissett B , Leditschke IA . Inspiratory muscle training to enhance weaning from mechanical ventilation . Anaesth Intensive Care . 2007 ; 35 ( 5 ): 776 - 779 .
65 . Routsi C , Gerovasili V , Vasileiadis I , et al . Electrical muscle stimulation prevents critical illness polyneuromyopathy: a randomized parallel intervention trial . Crit Care . 2010 ; 14 ( 2 ): R74 .
66 . Gruther W , Kainberger F , Fialka-Moser V , et al . Effects of neuromuscular electrical stimulation on muscle layer thick-ness of knee extensor muscles in intensive care unit patients: a pilot study . J Rehabil Med . 2010 ; 42 ( 6 ): 593 - 597 .
67 . Poulsen JB , Møller K , Jensen CV , Weisdorf S , Kehlet H , Perner A . Effect of transcutaneous electrical muscle stimu-lation on muscle volume in patients with septic shock . Crit Care Med . 2011 ; 39 ( 3 ): 456 - 461 .
68 . Zeppos L , Patman S , Berney S , Adsett JA , Bridson JM , Paratz JD . Physiotherapy in intensive care is safe: an observational study . Aust J Physiother . 2007 ; 53 ( 4 ): 279 - 283 .
69 . De Freitas ERFS . Profi le and severity of the patients of intensive care units: prospective application of the APACHE II index . Rev Lat Am Enfermagem . 2010 ; 18 ( 3 ): 317 - 323 .
70 . Clavet H , Hébert PC , Fergusson DA , Doucette S , Trudel G . Joint contractures in the intensive care unit: association with resource utilization and ambulatory status at discharge . Disabil Rehabil . 2011 ; 33 ( 2 ): 105 - 112 .
71 . Gosselink R , Bott J , Johnson M , et al . Physiotherapy for adult patients with critical illness: recommendations of the Euro-pean Respiratory Society and European Society of Intensive Care Medicine Task Force on physiotherapy for critically ill patients . Intensive Care Med . 2008 ; 34 ( 7 ): 1188 - 1199 .
72 . Hanekom S , Berney S , Morrow B , et al . The validation of a clinical algorithm for the prevention and management of pul-monary dysfunction in intubated adults—a synthesis of evi-dence and expert opinion . J Eval Clin Pract . 2011 ; 17 ( 4 ): 801 - 810 .
73 . Hanekom S , Gosselink R , Dean E , et al . The development of a clinical management algorithm for early physical activity and mobilization of critically ill patients: synthesis of evidence and expert opinion and its translation into practice . Clin Rehabil . 2011 ; 25 ( 9 ): 771 - 787 .
74 . Hodgin KE , Nordon-Craft A , McFann KK , Mealer ML , Moss M . Physical therapy utilization in intensive care units: results from a national survey . Crit Care Med . 2009 ; 37 ( 2 ): 561 - 566.
75 . Stockley RC , Hughes J , Morrison J , Rooney J . An investiga-tion of the use of passive movements in intensive care by UK physiotherapists . Physiotherapy . 2010 ; 96 ( 3 ): 228 - 233 .
76 . Hayes K , Seller D , Webb M , Hodgson CL , Holland AE . Ventilator hyperinfl ation: a survey of current physiotherapy practice in Australia and New Zealand . New Zealand Journal of Physiotherapy. 2011 ; 39 ( 3 ): 124 - 130 .
77 . Jones AY-M . Intensive care physiotherapy–medical staff per-ceptions . Hong Kong Physiotherapy Journal. 2001 ; 19 ( 1 ): 9 - 16 .
41 . Chiang L-L , Wang L-Y , Wu C-P , Wu H-D , Wu Y-T . Effects of physical training on functional status in patients with prolonged mechanical ventilation . Phys Ther . 2006 ; 86 ( 9 ): 1271 - 1281 .
42 . Bassett RD , Vollman KM , Brandwene L , Murray T . Integrating a multidisciplinary mobility programme into intensive care practice (IMMPTP): a multicentre collaborative . Intensive Crit Care Nurs . 2012 ; 28 ( 2 ): 88 - 97 .
43 . Leditschke IA , Green M , Irvine J , Bissett B , Mitchell IA . What are the barriers to mobilizing intensive care patients? Cardiopulm Phys Ther J . 2012 ; 23 ( 1 ): 26 - 29 .
44 . Thomsen GE , Snow GL , Rodriguez L , Hopkins RO . Patients with respiratory failure increase ambulation after transfer to an intensive care unit where early activity is a priority . Crit Care Med . 2008 ; 36 ( 4 ): 1119 - 1124 .
45 . Bailey P , Thomsen GE , Spuhler VJ , et al . Early activity is fea-sible and safe in respiratory failure patients . Crit Care Med . 2007 ; 35 ( 1 ): 139 - 145 .
46 . Clini EM , Crisafulli E , Antoni FD , et al . Functional recovery following physical training in tracheotomized and chronically ventilated patients . Respir Care . 2011 ; 56 ( 3 ): 306 - 313 .
47 . Garzon-Serrano J , Ryan C , Waak K , et al . Early mobilization in critically ill patients: patients’ mobilization level depends on health care provider’s profession . PM R . 2011 ; 3 ( 4 ): 307 - 313 .
48 . Zanni JM , Korupolu R , Fan E , et al . Rehabilitation therapy and outcomes in acute respiratory failure: an observational pilot project . J Crit Care . 2010 ; 25 ( 2 ): 254 - 262 .
49 . Stiller K , Phillips AC , Lambert P . The safety of mobilisation and its effect on haemodynamic and respiratory status of inten sive care patients . Physiother Theory Pract . 2004 ; 20 ( 3 ): 175 - 185 .
50 . Bahadur K , Jones G , Ntoumenopoulos G . An observational study of sitting out of bed in tracheostomised patients in the intensive care unit . Physiother. 2008 ; 94 ( 4 ): 300 - 305 .
51 . Bourdin G , Barbier J , Burle J-F , et al . The feasibility of early physical activity in intensive care unit patients: a prospec-tive observational one-center study . Respir Care . 2010 ; 55 ( 4 ): 400 - 407 .
52 . Nordon-Craft A , Schenkman M , Ridgeway K , Benson A , Moss M . Physical therapy management and patient outcomes following ICU-acquired weakness: a case series . J Neurol Phys Ther . 2011 ; 35 ( 3 ): 133 - 140 .
53 . Norrenberg M , De Backer D , Freidman G , Moraine J-J , Vincent J-L . Cardiovascular response to passive leg movement in critically ill patients . Clin Intensive Care . 1999 ; 10 ( 1 ): 1 - 6 .
54 . Chang AT , Boots RJ , Hodges PW , Thomas PJ , Paratz JD . Standing with the assistance of a tilt table improves minute ventilation in chronic critically ill patients . Arch Phys Med Rehabil . 2004 ; 85 ( 12 ): 1972 - 1976 .
55 . Zafi ropoulos B , Alison JA , McCarren B . Physiological responses to the early mobilisation of the intubated, ventilated abdom-inal surgery patient . Aust J Physiother . 2004 ; 50 ( 2 ): 95 - 100 .
56 . Skinner EH , Berney S , Warrillow S , Denehy L . Development of a physical function outcome measure (PFIT) and a pilot exercise training protocol for use in intensive care . Crit Care Resusc . 2009 ; 11 ( 2 ): 110 - 115 .
57 . Thelandersson A , Cider A , Volkmann R . Cerebrovascular and systemic haemodynamic parameters during passive exercise . Advances in Physiotherapy. 2010 ; 12 ( 1 ): 58 - 63 .
58 . Thelandersson A , Volkmann R , Cider A . Blood fl ow velocity and vascular resistance during passive leg exercise in the critically ill patient . Clin Physiol Funct Imaging . 2012 ; 32 ( 5 ): 338 - 342 .
59 . Hashim AM , Joseph LH , Embong J , Kasim Z , Mohan V . Tilt table practice improved ventilation in a patient with pro-longed artifi cial ventilation support in intensive care unit . Iran J Med Sci . 2012 ; 37 ( 1 ): 54 - 57 .
Downloaded From: http://journal.publications.chestnet.org/ by a University of Pittsburgh User on 10/14/2013

journal.publications.chestnet.org CHEST / 144 / 3 / SEPTEMBER 2013 847
84 . Dennis DM , Jacob WJ , Samuel FD . A survey of the use of ventilator hyperinfl ation in Australian tertiary intensive care units . Crit Care Resusc . 2010 ; 12 ( 4 ): 262 - 268 .
85 . Matilainen T , Olseni L . Physiotherapists in general intensive care units in Sweden–professional role, educational preferences and opinion about specialist certifi cation . Nordisk Fysioterapi. 2005 ; 9 ( 2 ): 74 - 81 .
86 . Wiles L , Stiller K . Passive limb movements for patients in an intensive care unit: a survey of physiotherapy practice in Australia . J Crit Care . 2010 ; 25 ( 3 ): 501 - 508 .
87 . Stiller K , Wiles L . Patient satisfaction with the physiotherapy service in an intensive care unit . South African Journal of Physiotherapy. 2008 ; 64 ( 1 ): 1 - 5 .
88 . Hodgson C , Carroll S , Denehy L . A survey of manual hyperin-fl ation in Australian hospitals . Aust J Physiother . 1999 ; 45 ( 3 ): 185 - 193 .
89 . Stiller K . Safety issues that should be considered when mobilizing critically ill patients . Crit Care Clin . 2007 ; 23 ( 1 ): 35 - 53 .
78 . Skinner EH , Berney S , Warrillow S , Denehy L . Rehabilitation and exercise prescription in Australian intensive care units . Physiother. 2008 ; 94 ( 3 ): 220 - 229 .
79 . Norrenberg M , Vincent J-L ; European Society of Intensive Care Medicine . A profi le of European intensive care unit physiotherapists . Intensive Care Med . 2000 ; 26 ( 7 ): 988 - 994 .
80 . Kumar JA , Maiya AG , Pereira D . Role of physiotherapists in intensive care units of India: a multicenter survey . Indian J Crit Care Med. 2007 ; 11 ( 4 ): 198 - 203 .
81 . Chang AT , Boots R , Hodges PW , Paratz J . Standing with assis-tance of a tilt table in intensive care: a survey of Australian physiotherapy practice . Aust J Physiother . 2004 ; 50 ( 1 ): 51 - 54 .
82 . Chaboyer W , Gass E , Foster M . Patterns of chest physiotherapy in Australian intensive care units . J Crit Care . 2004 ; 19 ( 3 ): 145 - 151 .
83 . Thomas PJ , Paratz JD , Stanton WR , Deans R , Lipman J . Positioning practices for ventilated intensive care patients: current practice, indications and contraindications . Aust Crit Care . 2006 ; 19 ( 4 ): 122 - 126 . , 128, 130-132.
Downloaded From: http://journal.publications.chestnet.org/ by a University of Pittsburgh User on 10/14/2013