physician executive council - advisory · leadership team (vpma, cqo, cmio) and emerging physician...
TRANSCRIPT

Physician Executive Council
Regina Lohr Consultant [email protected] Sruti Nataraja Practice Manager [email protected] Allison Shimooka Managing Director [email protected]
Results of the 2012 CMO Survey
The Evolving Role of the CMO
2445 M Street NW | Washington DC 20037 | P 202.266.5600 | F 202.266.5700 | advisory.com

© 2013 THE ADVISORY BOARD COMPANY • 26414 2 ADVISORY.COM
Table of Contents Introduction ................................................................................................................ 5
Emergence of the Chief Physician Executive ......................................................... 6
An Expanding Set of CMO Responsibilities ........................................................... 7
Rightsizing the CMO Role ......................................................................................... 8
A New Generation of Physician Executives .......................................................... 10
Guiding Questions for a Rightsized CMO Role .................................................... 11
Appendix: 2012 Physician Executive Survey Results ......................................... 12

© 2013 THE ADVISORY BOARD COMPANY • 26414 3 ADVISORY.COM
Available Within Your Physician Executive Council Membership The Physician Executive Council is built on 15 years of research and experience—resulting in a wealth of resources available to address CMOs’ most pressing issues. Studies and tools, such as those outlined below, are available in unlimited quantities through your Physician Executive Council membership.
Strategic Guidance on Leading the Enterprise Toward Value-Based Care
The New Quality Compact Partnering with Physicians to Advance a New Performance Standard
Equipping medical staff leaders to support individual physician performance improvement (PI)
Ensuring a strong foundation for evidence-based practice
Aligning physician incentives to support performance goals
Extending physician PI across the care continuum
Delivering on Value Positioning Quality for Success in an Evolving Performance-Based Environment
Protecting revenue capture on reported metrics
Fostering a culture of physician partnership
Elevating patient experience performance
Developing an enterprise quality strategy
Leveraging health IT to enhance care quality
Implementation-Ready Tools and Best Practices
Physician Leadership Effectiveness Compendium Select Practices for Promoting Physician Leadership Success
Growing the leadership base
Advancing leadership development
Providing ongoing leadership support
Delivering structured performance reviews
Aligning compensation with performance goals
Leadership Self-Assessment on Physician Engagement A Guide for Evaluating Your Approach and Identifying Improvement Opportunities
Executive leadership
Use of performance data
Communication
Physician leadership
Teamwork
To order copies of these and other Physician Executive Council studies and tools,
please visit our website: advisory.com/Research/Physician-Executive-Council

© 2013 THE ADVISORY BOARD COMPANY • 26414 4 ADVISORY.COM
How the Advisory Board Is Helping You Meet the CMO’s Challenge As the health care system transforms, the CMO role is also evolving—and expanding. An Advisory Board survey of 70+ CMOs found a host of new responsibilities for physician executives, from quality improvement to health care informatics to physician leadership development. CMOs cited six main areas where more support is most urgently needed:
Comprehensive Portfolio of Services
Managing an Evolving Responsibility Set
Anticipating Future Needs
Cultivating the Next Generation of Leaders
Navigating the New Health Care Data Challenge
Fast-Tracking Implementation with House-wide Education
Creating a Culture That will Embrace Change
Physician Executive Council Research membership focused on supporting the CMO and team with best demonstrated practices, insights, tools, expert consultations, and networking opportunities
Resources
Research aimed at elevating performance management, transforming clinical care delivery, and minimizing care variation
Information, insight, and expert support for the evolving role of the CMO
Webconferences, tools, and publications for clinical leadership team (VPMA, CQO, CMIO) and emerging physician leaders
Physician Engagement Initiative Best-in-class survey platform with a suite of change management supports to advance physician engagement and equip physicians to pursue organizational strategic goals
Features
Targeted survey questions for employed, affiliated, and independent physicians
Year-round guidance on engagement strategies to advance revenue, strategy, and mission goals
User-friendly results site with prescriptive reports and unparalleled analytic flexibility
Specialty and practice site benchmarking capabilities
Physician Leadership Development Hands-on programs for business and leadership skill development of executives and staff members, including on-site interactive workshops and online learning resources
Offerings
Curriculum library of 40+ interactive workshops
Courses selected to reflect institution-specific initiatives
Local examples, priorities, and data embedded to maximize applicability of all teaching
Workshops offer clear, actionable frameworks and opportunities for practice to make lessons transferrable to physicians’ own real-life leadership work
Performance Technologies National peer collaboratives powered by web-based analytic platforms
Crimson Continuum of Care: Supports physician alignment on quality and efficiency initiatives
Crimson Care Registry: Provides clinical data analysis and evidence-based prompts at the point of care
Crimson Population Risk Management: Illuminates cost and quality opportunities for defined populations
Crimson Real Time Readmissions: Predicts readmission risk, prompts appropriate interventions at the point of care

© 2013 THE ADVISORY BOARD COMPANY • 26414 5 ADVISORY.COM
Introduction In response to market changes incentivizing cost reduction and quality outcomes, the health care enterprise is changing dramatically. Yesterday’s systems revolved around hospitals, which treated patients with acute illnesses; tomorrow’s systems encompass the full continuum of care, expanding beyond the hospital to provide patients with ongoing, comprehensive health management.
In this new environment of “systemness,” physicians are central to cost control and quality improvement efforts. The linchpin role of physicians in care planning, coordination, and delivery—value-added processes that define a system—makes them indispensable partners in the effort to generate value from these new systems.
As the physician role evolves, chief medical officers’ roles are changing in kind. Historically, CMOs served as the primary liaison between the hospital and medical staff. However, with newer market pressures affecting the hospital-physician dynamic, CMOs are being called upon to leverage their skill as “influencer in chief,” to engage and establish credibility with physicians. Simultaneously, organizations striving toward care transformation are increasingly dependent on the CMOs’ depth of expertise in quality management and performance improvement.
In October, November, and December 2012, the Physician Executive Council conducted an online survey of more than 90 CMOs1 to gather quantitative data about their changing responsibilities. We augmented this data with anecdotal information by interviewing more than 30 CMOs and fostering discussions on this topic at the inaugural CMO Forum in November 2012.
This white paper draws on the Physician Executive Council’s recent research to:
1) Examine the impact of health care transformation on the CMO role
2) Highlight strategies CMOs are using to successfully manage these changes
1 Includes respondents who self-identified as chief medical officer or similar positions, such as VP of medical affairs.
As the physician role evolves in response to health care transformation, CMO roles are changing in kind
Please see the appendix for additional findings and data from the 2012 Physician Executive Survey.

© 2013 THE ADVISORY BOARD COMPANY • 26414 6 ADVISORY.COM
Emergence of the Chief Physician Executive With the shift to risk-based payment models that increase accountability across the care continuum, many organizations are turning to a chief physician executive to provide unified clinical leadership over enterprise-wide initiatives. This new leader will oversee all physician strategy, including relationships with both employed and independently aligned physicians, and will also be responsible for coordinating care transformation efforts for all providers across the care continuum. The emergence of a centralized physician leader is poised to have a major impact on the CMO role.
Leadership of the Clinical Enterprise
There are numerous candidates for the chief physician executive role. At some organizations, CMOs are leveraging their expertise in quality improvement and credibility with physicians to take on this new role. However, they are not the only potential candidates; the president of the medical group or PHO, or the VP of clinical integration, can each bring critical experience and expertise to this strategically critical role.
Whoever takes on the chief physician executive role must have established credibility with physicians, a history of driving organizational change, and experience across the continuum, including in the ambulatory care setting, which has not fallen under the traditional purview of most CMOs. As one CMO for a large East Coast health care system said, “Right now we’re trying to decide who will have authority over the clinical integration network, and I’m not sure it will be the CMO. The traditional CMO’s inpatient experience may not provide the right skills needed to take on such an ambulatory focus.”
As the leadership team decides who will assume the chief physician executive role, CMOs should sit down with their CEO to discuss their organization’s leadership structure and the future shape of their role. Key questions should include:
What do you envision as the leadership structure over the broader physician enterprise?
What components of the broader health system strategy will I be leading?
What level of support can I expect in my future role?
Will I have a team to whom I can delegate some of my traditional responsibilities?
A new physician executive to oversee cross-continuum physician strategy and care coordination
CMOs need to sit down with their CEO to discuss the future shape of their role

© 2013 THE ADVISORY BOARD COMPANY • 26414 7 ADVISORY.COM
An Expanding Set of CMO Responsibilities Whether or not CMOs are appointed as the chief physician executive, their contributions to the leadership team will remain critical to advancing the organization’s enterprise vision. As such, CMOs must expect their roles to change moving forward. Many CMOs have already found their role expanding to include a host of emerging responsibilities.
Emerging priorities overtaking traditional CMO responsibilities
As recently as five years ago, the CMO role was primarily focused on improving quality within the four walls of the hospital, managing credentialing and peer review processes, and serving as a liaison between a hospital’s administration and its medical staff. With the market pushing organizations toward achieving value-based care in recent years, new responsibilities have emerged and are rapidly filling CMOs’ plates.
Analysis of our 2012 Physician Executive Survey showed that the responsibilities of quality improvement and medical staff affairs that were once standard are occupying less and less of a CMO’s time. In place of these traditional responsibilities, CMOs are spreading their attention across a host of new areas including health informatics, cross-continuum care coordination, and population health management.
Percentage of CMOs Identifying Selected Responsibilities as One of Their Most Time Consuming2
2012 Physician Executive Survey
n=75
A particular CMO’s involvement in these emerging responsibilities will vary based on a number of organizational and individual factors, including composition of the executive team and the CMO’s areas of experience.
2 Based on the survey question, “From the list below, please select the four responsibilities that consumed the largest portion of your time three years ago,” and “From the list below, please select the four responsibilities that you anticipate will consume the largest portion of your time three years from now.”
CMOs are taking on nontraditional responsibilities

© 2013 THE ADVISORY BOARD COMPANY • 26414 8 ADVISORY.COM
CMO oversight moving out of inpatient arena
Another dimension of the CMO role expansion is an increasing amount of time and attention spent on venues outside of the traditional inpatient space, including responsibilities related to hospital outpatient and physician network settings. The Physician Executive Council’s survey found that three years ago, CMOs spent approximately one-third of their time on management responsibilities in the ambulatory setting. Today, they spend half of their time in this arena, and they expect this trend to continue, estimating that three years from now they will be spending nearly two-thirds of their time focusing outside of the traditional inpatient space.
Average Percentage of Time CMOs Estimated Spending on Ambulatory Care Responsibilities3
2012 Physician Executive Survey
n=73
Rightsizing the CMO Role As CMOs are tapped to lead a broader array of tasks, they must shape their roles to enable focus on their most strategic responsibilities. Without taking proactive steps, CMOs will find that the increasing scope of their role can limit their effectiveness, as evidenced by the 37% of CMOs who indicate that they are not able to effectively prioritize their most strategic responsibilities amid their full portfolio of duties.
No standard job description exists for the “rightsized” CMO role. CMOs must individually evaluate their core competencies and determine how to most effectively leverage the position to achieve organizational goals. Some CMOs will spend a disproportionate amount of their attention on traditional duties and delegate newer initiatives to other physician leaders. Other CMOs may opt to concentrate on newer initiatives and will hand off many of their traditional duties. In either case, the vast expansion in job scope will require CMOs to re-sculpt their position by following a three-step framework:
1. Identify the responsibilities to prioritize
2. Define the responsibilities to delegate
3. Find recipients for delegated responsibilities
3 Based on the survey question, “Approximately what percentage of your time do you spend on management responsibilities related to each of the settings of care listed below: hospital inpatient, hospital outpatient, and physician network?” Graphic represents percentage for both hospital outpatient and physician network care.
CMOs now spend half their time on ambulatory care responsibilities
There is no standard job description for the rightsized CMO role

© 2013 THE ADVISORY BOARD COMPANY • 26414 9 ADVISORY.COM
Delegation is a critical component of this framework. Not surprisingly, fully 86% of CMOs are already seeking to delegate some of their traditional responsibilities to other clinical leaders.
CMOs Seeking to Off-Load Responsibilities to Other Leaders4
2012 Physician Executive Survey n=72
Of course, a CMO’s ability to delegate is dependent on access to willing and capable clinical leaders. In some cases, CMOs audit existing roles to find available leaders within the organization, while elsewhere one or more new positions are created to take on the delegated responsibilities. The table below provides three representative examples of how CMOs are following this framework and identifying the appropriate leaders to absorb some of their tasks.
Three Rightsizing Strategies for CMOs
Strategy Process
Transform existing leadership roles
CMO prioritized emerging areas such as population health and leadership development
Delegated traditional responsibilities, including utilization review and patient safety
Transformed part-time medical director roles into positions including Chief Utilization Officer and Chief Patient Safety Officer to assume delegated responsibilities
Promote a key thought partner
CMO prioritized emerging responsibilities, including cross-continuum care coordination
Delegated quality improvement and medical staff affairs responsibilities Created a deputy CMO position, with CEO’s support, filled by an existing
physician leader who had long been an informal thought partner for clinical leadership decisions
Strengthen leadership in emerging areas
CMO prioritized building relationships with a growing network of affiliated physicians, educating physicians on population health strategies and garnering buy-in for system-wide quality initiatives
Delegated emerging priorities, including accountable care efforts Worked with CEO to create new medical director position for accountable
care responsibilities; recruited an experienced leader to strengthen the organization’s abilities in this area
Questions to guide the CMO through this three-step framework are included on page 11.
4 Based on the survey question, “Please indicate the extent to which you agree with the statement: I am seeking ways to delegate some of my traditional responsibilities to other clinical leaders in order to prioritize my most strategic responsibilities.” Graphic includes responses of strongly agree, agree, and tend to agree.
Some CMOs delegate tasks to existing leaders, while others create new positions to take on specific responsibilities

© 2013 THE ADVISORY BOARD COMPANY • 26414 10 ADVISORY.COM
A New Generation of Physician Executives When CMOs and their executive leadership teams decide that a new physician executive position is needed to absorb some of the CMO’s workload, the newly created roles vary widely. These positions are often uniquely designed based on the needs of the organization. Titles may be role-specific, such as associate CMO, or responsibility-specific, as with a medical director for post-acute care.
Emerging Responsibility-Specific Physician Executive Positions
With these new positions, organizations are establishing a new generation of physician executives. Such positions are often used as a succession-planning strategy to attract, promote, and retain top physician leadership talent within an organization.
Newly created positions are absorbing some of the CMO workload
© 2013 THE ADVISORY BOARD COMPANY • 26414 11 ADVISORY.COM
Guiding Questions for a Rightsized CMO Role Listed below are questions CMOs should ask as they apply the three-step rightsizing framework to their own role. These questions serve as a self-assessment tool to guide CMOs through the process of identifying responsibilities to prioritize, defining responsibilities to delegate, and finding recipients for the delegated responsibilities.
Step 1: Identify the responsibilities to prioritize
CMOs should first identify where they can be most effective at moving the organization toward achieving its mission and goals. Questions to consider include:
• Which responsibilities are you most uniquely qualified to execute because of your background and experience?
• Which responsibilities do you find most interesting and motivating to work on?
• Which responsibilities do you find yourself naturally prioritizing?
• Which responsibilities most closely align with your vision for the future of the organization?
Step 2: Define the responsibilities to delegate
The next step is determining which current CMO responsibilities will hinder prioritization of the responsibilities identified above; these are the responsibilities CMOs should delegate. Questions to consider include:
• Which responsibilities naturally fall off your “to-do” list on a regular basis?
• Which responsibilities are not well matched to your skills and interests?
• Which responsibilities do not align closely with your strategic priorities but consume a disproportionate amount of your time?
• Which responsibilities do not require your experienced judgment?
Step 3: Find recipients for delegated responsibilities
Finally, CMOs must identify appropriate individuals in the organization to take on the delegated responsibilities. Often, this means delegating to an existing physician leader, but CMOs may also find candidates outside of their medical staff. In instances where no appropriate individual exists within the organization, CMOs must evaluate whether financial resources exist to look outside the organization. Questions to consider include:
• Which individuals have proven strengths and experience relating to the delegated responsibilities?
• Which individuals have expressed interest in topics related to the responsibilities you are seeking to delegate?
• Which individuals are ready to expand their management and leadership skills?
For more guidance in rightsizing the CMO role, download the Role Maximization Toolkit at advisory.com/Research/Physician-Executive-Council/Resources/2013/Role-Maximization-Toolkit

© 2013 THE ADVISORY BOARD COMPANY • 26414 12 ADVISORY.COM
Appendix: 2012 Physician Executive Survey Results Methods for Data Collection and Analysis
From October through December 2012, The Advisory Board Company surveyed physician executives at hospitals and health systems around the country. This online survey sought to gather data about how top-level physician executives’ roles are changing and the challenges they are facing.
Survey results represent the experiences of 75 physician executives from approximately 35 health systems and 30 hospitals nationwide, including both Advisory Board members and nonmembers. Analysis of these results can be used to illuminate trends among physician executives, though sampling methods used do not allow for nationwide statistical estimates.
Respondent Characteristics
A majority of survey respondents described their position as chief medical officer (CMO), though responses from vice presidents of medical affairs, chief clinical officers, and associate CMOs are included in the data. We have reported the data separately for system-level physician executives and hospital-level physician executives.
Respondent Position Titles, by Percent of Physician Executives5 “Which of the following best describes your position?”
System-Level (n=40)
Hospital-Level (n=35)
Chief Medical Officer 78% 69%
Vice President of Medical Affairs 20% 37%
Chief Clinical Officer 0% 6%
Associate Chief Medical Officer 8% 0%
Survey respondents varied in their organization size and in how long they have held their current positions. The participating system-level physician executives represented health systems ranging in size from those comprising 2 hospitals to those with more than 50 affiliated hospitals. Participating hospital physician executives primarily represented community hospitals and teaching hospitals ranging in size from 40 beds to 1,000 beds. On average, physician executives who participated in the survey have been in their jobs for just under five years.
Survey Respondent Profile
System-Level (n=40)
System-Level (n=35)
Average Organization Size6 10 hospitals 300 beds
Average Tenure7 4.3 years 4.9 years
5 Multiple selections allowed. 6 Responses to the questions, “How many individual hospitals comprise your system?” and “What is your institution’s
approximate bed size?” 7 Responses to the question, “For how long have you held this position?”

© 2013 THE ADVISORY BOARD COMPANY • 26414 13 ADVISORY.COM
Divisions Reporting to the Physician Executive
CMO and VPMA roles have long been definied by their responsibilty for quality improvement and patient safety, and survey data indicate that these two divisions continue to be under the purview of most system and hospital physician executives. At least 50% of both system and hospital physician executives also have responsibility for infection prevention/control.
System and hospital physician executives diverge on their responsibility for other divisions. For example, more system physician executives than hospital physician executives report responsibility for areas such as continuing medical education and clinical integration programs. Conversely, hospital physician executives more commonly have responsibility for clinical divisions, risk management, and case management than system physician executives.
Responsibility for System and Hospital Divisions, by Percent of Physician Executives “Which of the following divisions (or equivalent) currently report up to you?”
System-Level (n=40)
Hospital-Level (n=34)
Quality/Performance Improvement 90% 82%
Patient Safety 60% 62%
Continuing Medical Education 60% 47%
Infection Prevention/Control 50% 59%
Clinical Integration Program 45% 27%
Utilization Review 43% 47%
Graduate Medical Education 40% 35%
Case Management 38% 56%
Clinical Divisions 38% 53%
Risk Management 38% 53%
Research 30% 24%
Patient Experience 30% 18%
Ambulatory Physician Network 30% 15%
Physician/Provider Recruitment 28% 32%
Clinical Informatics 25% 27%
Physician Hospital Organization 15% 15%
Accountable Care Organization 13% 9%

© 2013 THE ADVISORY BOARD COMPANY • 26414 14 ADVISORY.COM
Involvement in IT and Informatics Issues
Nearly all physician executives have undertaken one or more roles to support the development and adoption of health IT (HIT) within their institutions. Physician executives most commonly play a role in the planning and strategic design of HIT and also utilize HIT data and informatics to drive quality within their organizations.
Roles in Support of Health IT, by Percent of Physician Executives “In supporting health information technology in your organization,
which of the following roles have you undertaken?”
System-Level (n=40)
Hospital-Level (n=34)
Planning/strategic design of HIT 78% 65%
Utilizing data and informatics from HIT systems to drive quality 73% 71%
Explaining HIT to physicians, such as training physicians or discussing HIT decisions with physicians
70% 65%
Ongoing optimization of HIT systems, such as by ensuring an intuitive and user-friendly physician interface
63% 56%
Overseeing implementation of HIT, including electronic health records 55% 56%
A small percentage of physician executives support HIT by serving as the chief medical information officer (CMIO), in addition to their other duties. More commonly, physician executives work closely with the CMIO to achieve HIT goals.
Relationship with the CMIO, by Percent of Physician Executives “Which statement best characterizes your relationship with your organization’s CMIO?”
System-Level (n=40)
Hospital-Level (n=35)
Direct reporting relationships (i.e., CMIO reports directly to me) 18% 9%
Shared reporting relationships (i.e., CMIO reports directly to me as well as another position, such as the CIO)
13% 0%
No reporting relationship, but we communicate frequently 40% 43%
No reporting relationship, and we communicate infrequently 10% 14%
Organization does not have a CMIO 13% 20%
I also serve as the CMIO 5% 11%

© 2013 THE ADVISORY BOARD COMPANY • 26414 15 ADVISORY.COM
Responsibilities Across Settings of Care
Physician executives reported that they are spending a decreasing percentage of their time on management responsibilities in the hospital inpatient setting and an increasing percentage of their time in the hospital outpatient setting and physician network setting.
System physician executives reported spending an average of 53% of their time in the hospital inpatient setting three years ago, and hospital physician executives reported spending an average of 70% of their time in this setting three years ago. Looking to the future, both groups of physician executives expect this time to decrease, with system physician executives expecting to spend 32% of their time in the inpatient setting three years from now and hospital physician executives spending 44% of their time in that setting.
Responsibilities Across Care Settings: System-Level, by Percent of Time Spent8
“Approximately what percentage of your time did you spend (or do you anticipate spending) on management responsibilities related to each of the
following settings of care three years ago, today, and three years from now?”
n=40
Three Years Ago Today
Three Years from Now
Hospital Inpatient 53% 43% 32%
Hospital Outpatient 21% 24% 28%
Physician Network 26% 33% 41%
Responsibilities Across Care Settings: Hospital-Level, by Percent of Time Spent8
“Approximately what percentage of your time did you spend (or do you
anticipate spending) on management responsibilities related to each of the following settings of care three years ago, today, and three years from now?”
n=35
Three Years
Ago Today Three Years from Now
Hospital Inpatient 70% 57% 44%
Hospital Outpatient 16% 23% 29%
Physician Network 13% 19% 27%
8 Due to rounding, responses may not sum to 100%.

© 2013 THE ADVISORY BOARD COMPANY • 26414 16 ADVISORY.COM
Most Time-Consuming Responsibilities
Both system and hospital physician executives are currently in the midst of a shift in their top responsibilites—those responsibilities that consume the most time. Whereas three years ago most physician executives agreed that quality management, medical staff affairs, and administration/medical staff liaison were among their most time-consuming responsibilities, there is no such agreement today. Less than half of physician executives anticipate that these traditional responsibilities will still be at the top three years from now, and a variety of emerging responsibilities are expected to take their place.
The biggest changes for system physician executives has been the emergence of physician leadership development and population health management. In addition, leadership within the chief executive team (C-suite) is emerging as the most commonly identified top responsibility among system physician executives.
Most Time Consuming Responsibilities: System-Level, by Percent of Physician Executives “From the list below, please select the four responsibilities that consumed (or that you anticipate will
consume) the largest portion of your time three years ago (or three years from now).”
n=40
Three Years
Ago Three Years
from Now Percentage-
Point Change9
Physician Leadership Development 18% 48% 30
Population Health Management 8% 35% 27
Leadership Within the Chief Executive Team (C-Suite) 50% 70% 20
Care Coordination 15% 30% 15
Clinical Standardization 23% 30% 7
Health IT and Informatics 15% 18% 3
Developing Physician Contracts and Partnership Models10 15% 13% (3)
Clinical Operations Leadership 23% 15% (8)
Regulatory Functions (e.g., The Joint Commission, CMS) 25% 8% (17)
Liaison Between Administration and Medical Staff11 58% 35% (23)
Medical Staff Affairs 58% 23% (35)
Quality Management / Performance Improvement 80% 43% (37)
9 Physician executives were also asked about the responsibilities that currently consume the largest portion of their
time, and these responses generally corresponded with the trends shown. 10 For example, co-management and professional services agreements. 11 Including physician alignment and collaborating with independent physicians.

© 2013 THE ADVISORY BOARD COMPANY • 26414 17 ADVISORY.COM
Among hospital physician executives, the responsibilities that physician executives reported were increading the most were care coordination, developing physician contracts and partnership models, and population health management. Leadership within the chief executive team (C-suite) is most commonly anticipated to be a top responsibility among hospital physician executives, as well.
Most Time Consuming Responsibilities: Hospital-Level, by Percent of Physician Executives “From the list below, please select the four responsibilities that consumed (or that you anticipate will
consume) the largest portion of your time three years ago (or three years from now).”
n=35
Three Years
Ago Three Years From Now
Percentage-Point
Change12
Care Coordination 9% 26% 17
Developing Physician Contracts and Partnership Models13 9% 26% 17
Population Health Management 3% 20% 17
Patient Experience Management 6% 20% 14
Physician Leadership Development 11% 23% 12
Clinical Standardization 14% 23% 9
Health IT and Informatics 17% 26% 9
Leadership Within the Chief Executive Team (C-Suite) 46% 51% 5
Clinical Operations Leadership 17% 14% (3)
Liaison Between Administration and Medical Staff14 57% 43% (14)
Regulatory Functions (e.g. The Joint Commission, CMS) 43% 20% (17)
Quality Management / Performance Improvement 80% 49% (31)
Medical Staff Affairs 77% 43% (34)
12 Physician executives were also asked about the responsibilities that currently consume the largest portion of their
time, and these responses generally corresponded with the trends shown. 13 For example, co-management and professional services agreements. 14 Including physician alignment and collaborating with independent physicians.

© 2013 THE ADVISORY BOARD COMPANY • 26414 18 ADVISORY.COM
Strategically Important Responsibilities
The largest portion of physician executives identified physician leadership development and leadership within the chief executive team as the most strategically important responsibilities for them to focus on now in order to move their organizations forward. Sixty percent of system physician executives and 51% of hospital physician executives selected each of these two responsibilities. At least one-third of system and hospital physician executive respondents also selected quality management/performance improvement and liaison between administration and medical staff as most strategically important.
Most Strategically Important Responsibilities, by Percent of Physician Executives “From the list below, please select the four responsibilities that are most strategically important
for you to focus on now in order to move your organization forward.”
System-Level (n=40)
Hospital-Level (n=35)
Physician Leadership Development 60% 51%
Leadership Within the Chief Executive Team (C-Suite) 60% 51%
Quality Management / Performance Improvement 40% 49%
Liaison Between Administration and Medical Staff 38% 43%
Population Health Management 38% 29%
Health IT And Informatics 18% 37%
Clinical Standardization 33% 34%
Care Coordination 33% 31%
In order to prioritize these strategically important responsibilities, most physician executives are seeking ways to delegate some of their traditional responsibilities to other clinical leaders. Ninety-two percent of system physician executives and 79% of hospital physician executives strongly agreed, agreed, or tended to agree with the statement, “I am seeking ways to delegate traditional responsibilites to other clinical leaders in order to prioritize my most strategic responsibilities.”
Physician Executives Seeking to Delegate Responsibilities to Other Leaders15 “I am seeking ways to delegate traditional responsibilities to other
clinical leaders in order to prioritize my most strategic responsibilities.”
15 Due to rounding, responses may not sum to 100%.
© 2013 THE ADVISORY BOARD COMPANY • 26414 19 ADVISORY.COM
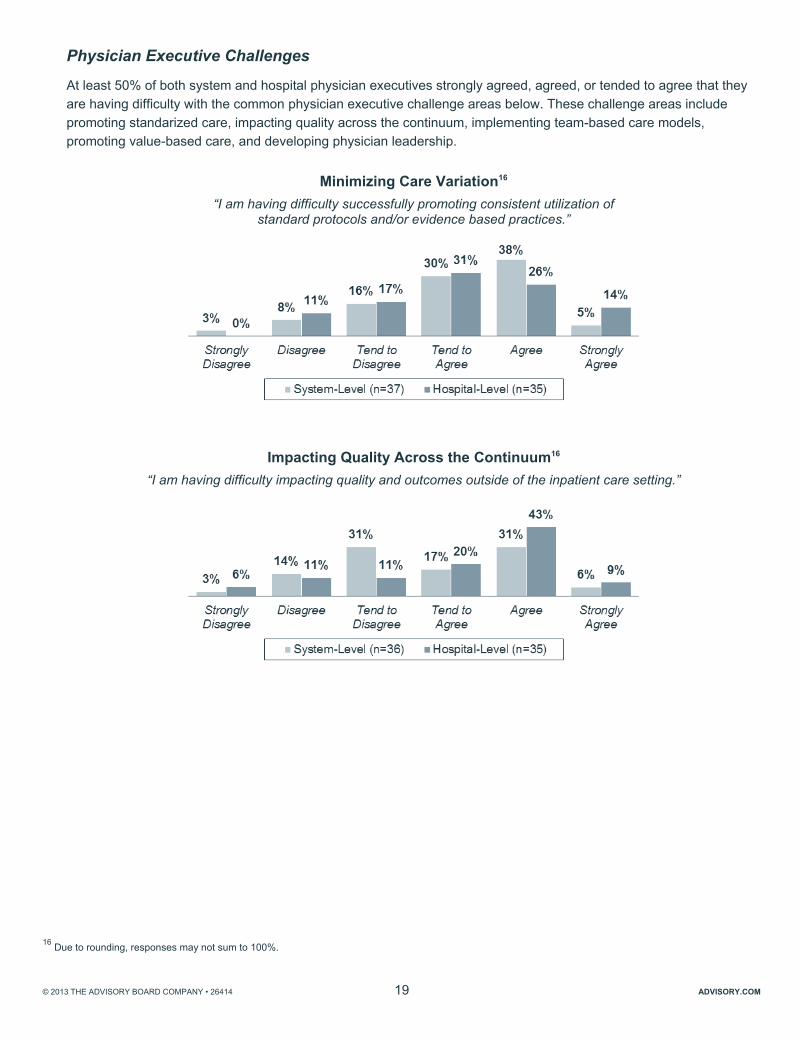
Physician Executive Challenges
At least 50% of both system and hospital physician executives strongly agreed, agreed, or tended to agree that they are having difficulty with the common physician executive challenge areas below. These challenge areas include promoting standarized care, impacting quality across the continuum, implementing team-based care models, promoting value-based care, and developing physician leadership.
Minimizing Care Variation16 “I am having difficulty successfully promoting consistent utilization of
standard protocols and/or evidence based practices.”
Impacting Quality Across the Continuum16 “I am having difficulty impacting quality and outcomes outside of the inpatient care setting.”
16 Due to rounding, responses may not sum to 100%.

© 2013 THE ADVISORY BOARD COMPANY • 26414 20 ADVISORY.COM
Implementing Team-Based Care Models17 “I am having difficulty engaging and influencing physicians to adopt
team-based care models and/or care redesign.”
Promoting Value-Based Care17 “I am having difficulty influencing the medical team to embrace value-based care.”
Developing Physician Leadership17
“I am having difficulty developing the necessary competencies (e.g., project management, conflict resolution, etc.) within my staff in order to broaden the physician leadership bench.”
17 Due to rounding, responses may not sum to 100%.