physical health effects of traumatic exposure paula p. schnurr, ph.d. national center for ptsd...
TRANSCRIPT

Physical Health Effects of Traumatic Exposure
Paula P. Schnurr, Ph.D.National Center for PTSDExecutive Division, &Dartmouth Medical School

Presentation Goals
To increase understanding that:– trauma is related to poor health– a person’s reaction--PTSD especially--mediates the effect of exposure– there are plausible mechanisms through which PTSD could promote health
Premise: Good clinical practice is informed by research findings

Common Views About How Mental States Affect Health
• “It’s all in your head…”
• “You’re not really sick, it’s just stress…”
• “OK, you’re sick, but it’s only because you’re stressed…”

Example:How Depression (vs. Smoking) Affects Coronary Disease Onset
0
0.5
1
1.5
2
2.5
3
Risk
Smoking (US
Surgeon General)
Passive Smoking
(He et al., 1999)
Depression
(Wulsin et al., 2003)
All p < .05

What Are Health Outcomes?
Influence Due toMental Health Example
Self-reportsSymptoms +++ PILL, SCL-90Global status ++ SF-36Functioning ++ SF-36Conditions + “Has a doctor ever told
you that you have...?”
Utilization + Self-report, database
MorbidityPhysician exam (+) Review of systemsLaboratory tests 0 EKG
Mortality 0 Standardizedmortality ratio

Trauma in Relation to Illness and Injury
Direct– Survivor physically harmed
by trauma– Less common– Health problems related to
trauma– Medical problems part of
survivor identity
Indirect– Survivor not physically
harmed by trauma– More common– Health problems unrelated to
trauma

Findings on Trauma and Poor Health
Self-Report Utilization Morbidity Mortality
Military ++ + +/- +
Sexual ++ ++ +/- NA
Disaster ++ ++ + +/-
Other ++ NA + +
++ = clear association, + = probable association, +/- = inconsistent information, NA = insufficient information

Health Outcomes as a Function of Childhood Trauma

Health Risk Behaviors as a Function of Childhood Trauma

Wartime Stress and Coronary Artery Disease in Civilians (Sibai et al., 1989)
0
2
4
6
>2 war events >1 green-linecrossing/wk
Od
ds
Rat
io
Cases (³70%Stenosis) vs.Visitor Controls
Cases vs.Patient Controls
Cases more likely Cases more likely than controls to than controls to have high exposure have high exposure to war stressorsto war stressors

10-Year Mortality in War-Exposed Civilians (Sibai et al., 2001)
10
20
30
40
50
60
70
0 1-2 3-4 ³ 5
Number of War-Related Events
Rat
e P
er 1
000
Per
son
Yea
rs
Men: CVD
Men: All-Cause
Women:CVD
Women:All-Cause

Questions???
• How does traumatic exposure lead to poor health?
How Does Trauma Lead to Poor Health?The Role of Distress as a Mediator
DistressStressful
Event
PhysicalHealth
Outcome
Trauma PTSD Health

Higher WZE associated with a greater number of medical conditions(adjusted for age and education)
PTSD as a Mediator of the Relationship Between Warzone Exposure and Health in Female Veterans (Wolfe et al., 1994)
# Medical Conditions
WZ Exposure
.42**

PTSD as a Mediator of the Relationship Between Warzone Exposure and Health in Female Veterans (Wolfe et al., 1994)
Effect of WZE declined from .42** to .08 when PTSD added
PTSD Sxs
# MedicalConditions
# MedicalConditions
.42**
.08
WZExposure
WZExposure

Findings on PTSD and Poor Health
Self-Report Utilization Morbidity Mortality
Military ++ + + +
Sexual ++ + + NA
Disaster + + + NA
Other + + + NA
++ = clear association, + = probable association, NA = insufficient information

Odds of Self-Reported Medical Disorder Due to PTSD in Female Vietnam Veterans (Wolfe et al., 1994)
0 1 2 3 4 5
Dermatological*
Gastrointestinal*
Pain*
Gynecological*
Cardiovascular*
Respiratory
Liver
Weight changeOR indicates change associated w/1.0 SD in PTSD symptoms
Adjusted for age, education, and WZE
*p < .05
*
*
*
*
*

Adjusted Odds of Self-Reported Medical Disorder Due to PTSD in Vietnam Veterans (Boscarino, 1997)
0 0.5 1 1.5 2 2.5
Cancer
Circulatory
Digestive
Musculoskeletal
Genitourinary
Endocrine
Nervous system
Skin
Respiratory
Any disorder
*p < .05
*
*
*
*
*
*

SF-36 Scores in Mustard Gas Exposed Veterans (Schnurr et al., 2000)
0 20 40 60 80
PhysicalFunction
Role Impair-Physical
Fatigue
Pain
PTSD and partial PTSD < no PTSD
Full PTSD
PartialPTSDNo PTSD
NormativeSample

Predicted Physical Symptoms, Age 65 Retirement (Schnurr et al., 2005)
0
5
10
15
20
25
51 53 55 57 59 61 63 65 67 69 71 73 75 77 79
Noexposure
Traumaonly
PTSD

Adjusted Annual Cost Ratios in Female HMO Enrollees (Walker et al., 2003)
0
0.5
1
1.5
2
2.5
PC Specialty MH Total
Low v. Medium PTSD
Low v. High PTSD
PCL med = 30-44,high = 45+
*p < .05 adjusted for demographics, chronic disease, and mental health
**
*
*

PTSD and Hazard of Physician-Diagnosed Disease in Older Veterans (Schnurr, Spiro, & Paris, 2000)
0 0.2 0.4 0.6 0.8 1 1.2 1.4
Cancer
Endocrine
Hypertension
Ischemic
Other Cardio.
Arterial
Pulmonary
Upper GI
Lower GI
Urinary
Dermatologic
Musculoskeletal
Hazard is expressed per 10-pt increase in PTSD sxs and is adjusted for age, BMI, smoking, and alcohol consumption
*p < .05
*
*
*
*

PTSD and Arterial Disorder in Older Veterans (Schnurr et al., 2000)

Odds of Physician-Diagnosed Disorder as a Function of PTSD Diagnosis (Ouimette et al., 2004)
0
0.5
1
1.5
2
2.5
3
3.5
4
Odds Ratio
Circulatory
Musculosketal
Gastrointestinal
Dermatological
**
Gender did not moderate the effects of PTSD
*p < .05, adjusted for age, smoking, alcohol, BMI

Mortality Due to PTSD in Vietnam Veterans (Bullman & Kang, 1994)
0
0.5
1
1.5
2
2.5
All Causes Cancer Circulatory Digestive ExternalCauses
RR
**
*p < .05

Questions???
• How does traumatic exposure lead to poor health?
• Are the effects of PTSD unique from the effects of other psychiatric disorders?

Effects of PTSD and Depression on SF-36 Physical Component Scores in Female Veterans (Frayne et al., 2004)
-7
-6
-5
-4
-3
-2
-1
0
Depressionalone
PTSD alone
PTSD andDepression
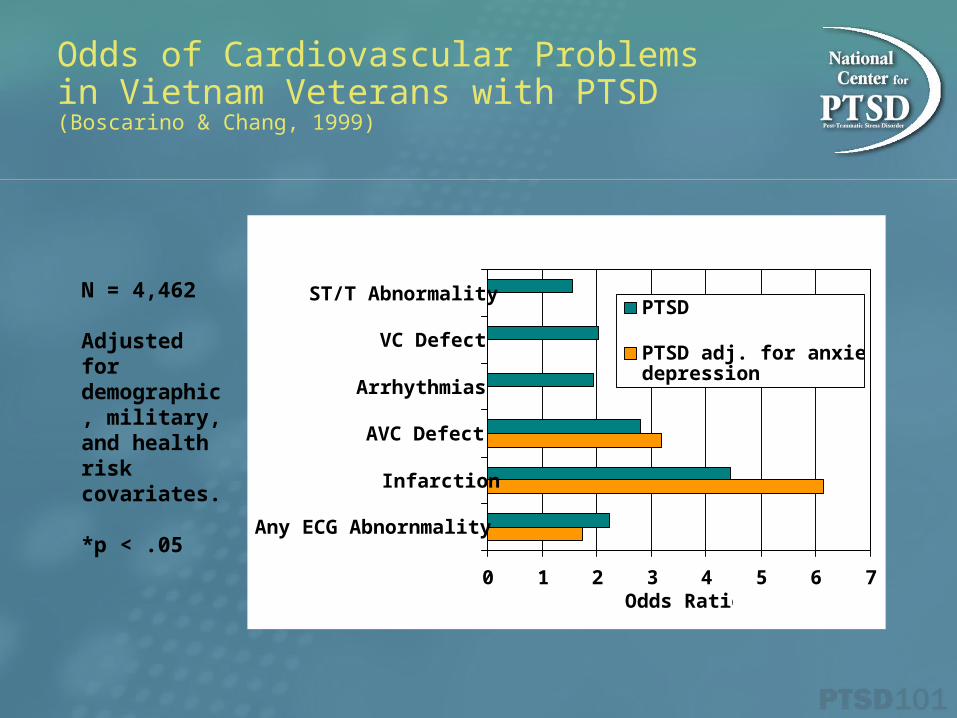
Odds of Cardiovascular Problems in Vietnam Veterans with PTSD (Boscarino & Chang, 1999)
0 1 2 3 4 5 6 7
Any ECG Abnornmality
Infarction
AVC Defect
Arrhythmias
VC Defect
ST/T Abnormality
Odds Ratio
PTSD
PTSD adj. for anxiety &depression
*
*
**
*
N = 4,462
Adjusted for demographic, military, and health risk covariates. *p < .05

Medical Service Utilization in Male Vietnam Veterans (Schnurr et al., 2000)
0
0.5
1
1.5
2
2.5
3
3.5
Od
ds
Rati
o
Recentoutpatient
Recentinpatient
Recent VAoutpatient
LifetimeVA
outpatient
LifetimeVA
inpatient
PTSDOther Axis ISubstance Abuse
**
* *
*
*
**
*p < .05

• How does traumatic exposure lead to poor health?
• Are the effects of PTSD unique from the effects of other psychiatric disorders?
• How does PTSD lead to poor health?
Questions???

Case-Control Study of High v. Low VA Healthcare Users(Deykin et al., 2001)
PTSD
Depression
MedicalConditions
Utilization
Effects of PTSD on number of medical conditions both direct
and mediated through depression
OR of PTSD in High v. Low
Users = 2.17

Effects of PTSD and Depression on Health Status in Peacekeepers(Asmundson et al., 2002)
*p < .01
PTSD
Depression
PoorHealth
AlcoholAlcoholUseUse
.24*
.81* .40*
.17*

Possible Ways PTSD Could Affect Health
PsychologicalDepression
HostilityCoping
BehavioralSmoking
DietExercise
BiologicalCardiovascular reactivityAutonomic hyperarousal
Disturbed sleep physiologyAdrenergic dysregulation
Enhanced thyroid functionAltered HPA a ctivity
Dynamic Regulation of Body Systems
• Homeostasis: body maintains constancy within a tight range (e.g., Cannon, 1929)
• Allostasis: body increases or decreases vital functions within an operating range, in response to environmental challenge (Sterling & Eyer, 1988)

A Unifying Mechanism: Allostatic Load
• “The strain on the body produced by repeated up and downs of physiologic response, as well as the elevated activity of physiologic systems under challenge, and the changes in metabolism and wear and tear on a number of organs and tissues”
– McEwen & Stellar, 1993

Allostasis and Allostatic Load
Allostatic Load
Allostasis

Effect of Allostatic Load on Incidence of Cardiovascular Disease (Seeman et al., 1997)
New Disease Over 2.5 Years (N = 736)
0%
5%
10%
15%
Allostatic Load Category
0
1-2
≥ 3

PTSD and Allostatic Load (Schnurr & Jankowski, 1999)
other risk factors
sympatheticactivation
self-medication(smoking & drinking)
stress due to drinkingconsequences
Allostatic Load
Thresholdfor illness

Multifactorial Model of Trauma, PTSD, & Health (Schnurr & Green, 2004)
PTSD
Exposure
BiologicalAlterations
PsychologicalAlterations
AttentionalProcesses
Health RiskBehaviors
IllnessBehavior
Disease

(1) Exposure affects health primarily through PTSD and other distress reactions
PTSD
Exposure
BiologicalAlterations
PsychologicalAlterations
AttentionalProcesses
Health RiskBehaviors
IllnessBehavior
Disease

(2) PTSD and distress reactions affect illness behavior by altering symptom perception
PTSD
Exposure
BiologicalAlterations
PsychologicalAlterations
AttentionalProcesses
Health RiskBehaviors
IllnessBehavior
Disease

(3) Effects of PTSD on disease are mediated through interdependent psychological, biological, and behavioral mechanisms
PTSD
Exposure
BiologicalAlterations
PsychologicalAlterations
AttentionalProcesses
Health RiskBehaviors
IllnessBehavior
Disease

Summary
• Traumatic exposure is related to poor health
• A person’s reaction–PTSD especially–mediates the effect of exposure
• There are plausible mechanisms through which PTSD could promote poor health

Treatment Issues: Two Scenarios
Trauma problems in medical patients
Medical problems in trauma patients
In either case, MH providers need to
address medical problems & work with
medical staff