phd dissertation - menighedsfakultetetep.teologi.dk/diverseopen/2013phdfroelundpedersenheidi... ·...
TRANSCRIPT
PHD Dissertation
Religiosity and coping in a secular society:
Prevalence, characteristics, and associations to quality-of-life among Danes
facing life-threatening lung disease and other stressful life events
Heidi Frølund Pedersen
Unit for Psycho-oncology and Health Psychology Research
Department of Psychology and Behavioural Sciences
Aarhus University
July 2013
___________________________________________
ii
Religiosity and coping in a secular society: Prevalence, characteristics, and associations to
quality-of-life among Danes facing life threatening lung disease and other stressful life events
© Heidi Frølund Pedersen
Department of Psychology and Behavioural Sciences
School of Business and Social Sciences
Aarhus University
Bartholins Allé 9
DK – 8000 Aarhus C
Supervisor:
Robert Zachariae, professor affiliated at Unit for Psycho-oncology and Health Psychology, Aarhus
University Hospital and Aarhus University, Denmark
Co-supervisors:
Jan Tønnesvang, professor affiliated at Department of Psychology, Aarhus University, Denmark
Christina Gundgaard Pedersen, post. doc. affiliated at Unit for Psycho-oncology and Health
Psychology, Aarhus University Hospital and Aarhus University, Denmark
Cover design: Arne Hougaard Pedersen
Illustration: Elin Karlsnes. Trykt med tilladelse af Tidsskrift for Den Norske Legeforening, der
først bragte illustrationen 21. januar 2011 i volume 131 (2): 138-140

___________________________________________
iii
The cords of death entangled me;
the torrents of destruction overwhelmed me.
The cords of the grave coiled around me;
the snares of death confronted me.
In my distress I called to the LORD;
I cried to my God for help.
From his temple he heard my voice;
my cry came before him, into his ears.
…
He reached down from on high and took hold of me;
he drew me out of deep waters.
He rescued me from my powerful enemy,
from my foes, who were too strong for me.
(Phalms, 18, verses 4-6, 16-17)
To my father!
You faced the entanglement of death and torrents of destruction.
___________________________________________
iv
Contents
Original papers ................................................................................................................................................................... vi
Acknowledgements ........................................................................................................................................................ vii
Preface .................................................................................................................................................................................... ix
List of abbreviations ......................................................................................................................................................... 1
English summary ................................................................................................................................................................ 2
Dansk resumé (Danish summary) ............................................................................................................................. 6
Introduction ....................................................................................................................................................................... 10
The Danish context ......................................................................................................................................................... 11
The concepts of religion and spirituality in a secular society.................................................................... 12
A conceptual framework ............................................................................................................................................. 13
Religious coping ............................................................................................................................................................... 14
Measurement of religious coping ....................................................................................................................... 15
Empirical findings ...................................................................................................................................................... 16
Negative religious coping .................................................................................................................................... 17
Positive religious coping ...................................................................................................................................... 17
Longitudinal studies .............................................................................................................................................. 18
Predictors of religious coping ............................................................................................................................ 18
The application of religious coping theory among Danes ........................................................................... 19
Empirical findings on religiosity during stressful events in Denmark .................................................. 20
Aim of this present thesis ............................................................................................................................................ 22
Study design .................................................................................................................................................................. 22
Summary of the four studies ................................................................................................................................. 24
Study 1: Religious coping and quality of life among severely ill lung patients in a secular
society .......................................................................................................................................................................... 24
Study 2: Coping without religion? Religious coping, quality of life and existential well-being
among lung disease patients and matched controls in a secular society ....................................... 25
Study 3: Psycho-social factors associated with religious struggles during negative life events
in a secular society ................................................................................................................................................. 26
Study 4: Studying religious and spiritual coping in a secular culture: A question of validty . 26
___________________________________________
v
Discussion ........................................................................................................................................................................... 27
Prevalence of religious beliefs and religious coping among Danish lung disease patients .... 27
Increased relevance of religiosity and religious coping during illness? .......................................... 28
Religious, spiritual, and existential concerns among lung disease patients .................................. 29
Addressing religious, spiritual, and existential concerns ....................................................................... 30
Associations between religious coping and QoL ......................................................................................... 31
Negative religious coping......................................................................................................................................... 31
Positive religious coping ...................................................................................................................................... 32
Individual characteristics associated with religious struggles ............................................................ 33
Negative events ........................................................................................................................................................ 33
The impact of individual differences............................................................................................................... 34
Religious characteristics ...................................................................................................................................... 35
Methodological considerations and limitations ............................................................................................... 37
The validity of Brief RCOPE in a secular society .......................................................................................... 37
A critical comment on the theoretical and empirical work on religious coping .......................... 39
Integrating a hermeneutical approach to religious coping? .................................................................. 42
Generalizabilty ............................................................................................................................................................. 43
Conclusion: A soda-analogy? ..................................................................................................................................... 45
Perspectives and future studies ............................................................................................................................... 48
Clinical implications .................................................................................................................................................. 48
Research implications .............................................................................................................................................. 49
References .......................................................................................................................................................................... 51
Appendix ............................................................................................................................................................................. 64
Paper 1
Paper 2
Paper 3
Paper 4
___________________________________________
vi
Original papers
This thesis is based on the following original papers presented in the order in which they were
written:
1. Pedersen, H.F., Pargament, K.I., Pedersen, C.G., & Zachariae, R. (2013). Religious Coping
and Quality of Life among Severely Ill Lung Patients in a Secular Society. International
Journal for the Psychology of Religion, 23: 188-203
2. Pedersen, H.F., Pedersen, C.G., Pargament, K.I., & Zachariae, R. (2013). Coping without
religion? Religious coping, quality of life, and existential well-being among lung disease
patients and matched controls in a secular society. Research in the Social Scientific Study of
Religion, 24: 163-192
3. Pedersen, H.F., Pedersen, C.G., & Zachariae, R. Psycho-social factors associated with
religious struggles during negative life events in a secular society (submitted for The
Psychology of Religion and Spirituality)
4. Pedersen, H.F. & Tønnesvang, J. Studying religious and spiritual coping in a secular culture:
A question of validity (submitted for Mental Health, Religion, and Culture)
The present volume includes an introduction to the field of research, original papers, discussion of
the study results, and conclusions of the work presented in study 1-4 as well as suggestions for
future research and clinical implications

___________________________________________
vii
Acknowledgements
This Ph.D. thesis was carried out in collaboration with Unit for Psycho-oncology and Health
Psychology Research, Aarhus University and Aarhus University Hospital, the respiratory medical
clinics in Aarhus, Aalborg, Holstebro, Randers, and Rønne, and Statistics Denmark. I greatly
acknowledge the financial support provided by: Aarhus University, The Danish Cancer Society,
Danish Knowledge and Research Centre of Complementary and Alternative Medicine (ViFAB) in
collaboration with Center for Cross-Scientific Evaluation Studies on Complementary and
Alternative Medicine (CCESCAM) at University of Southern Denmark and Aarhus University,
Lykfeldts Legat, Max og Inger Wørzners Mindelegat, and Fritz, Georg og Marie Gluds Legat.
Many individuals have been involved in the different studies and provided guidance and support
during the 6 years that I have been working on this present thesis. I wish to thank the following:
First of all I want to thank all the participants included in the studies, especially the lung disease
patients who despite difficult circumstances spend time and energy responding to long
questionnaires, and the ten lung cancer patients who let me come close to their experience of illness
and existential concerns in individual interviews. Half a year after these interviews had been
conducted eight patients were not alive anymore, which reminded me about the gravity of their
situations and hopefully this thesis gives voice to some of their experiences of facing life’s ultimate
challenge.
I want to thank my supervisor professor Robert Zachariae, for giving me the opportunity to go into
research on a rather controversial topic and for his support during the process. He has sharpened my
critical sense in research on psychology of religion and health and was always efficient and
supportive in his guidance and contributions to study design and the single papers included in this
thesis. Furthermore he has created a fruitful research environment on psycho-oncology and health
psychology and my thanks are also directed at every single colleague at Unit for Psycho-oncology
and Health Psychology Research for encouragement, practical and statistical help, and vivid
discussions at our research meetings.For good and thought provoking discussions I thank Jan
Tønnesvang, my co-supervisor, who first awakened my interest in the psychology of religion and
for always insisting on taking a theoretical approach to the rather complex phenomena of religion.
___________________________________________
viii
I want to thank Christina G. Pedersen, my co-supervisor and mentor, for giving me the opportunity
to work together with her on the lung disease project. Her positive and careful attitude has been an
important support to me, and her skills in project managing and statistics have helped me carry this
thesis through.
For being an encouraging and inspiring mentor, I wish to thank Kenneth I. Pargament. During my
visit at Bowling Green State University, Ohio, in 2011 he willingly shared his passion and wide
knowledge in the psychology of religion, as well as his personal qualities as a mentor. He is one of
the main reasons why I carried through with this project.
To Peter la Cour I direct my deepest appreciations for being the spearhead of the psychology of
religion in Denmark, and for taking a differentiated and critical focus on theories and methodology
in this field. His friendly personality and strong integrity has been a personal inspiration to me.
For making the way for the Interdisciplinary Research Network on Faith and Health in Denmark
and Scandinavia and for encouragements to go into research, I thank Niels Christian Hvidt.
For sharing ups and down, victories and worries on the journey of the Ph.D. study I wish to thank
Berit Kjærside Nielsen, Dorthe Toudal Viftrup, Hanne Fentz Nørr, and Yoon Lia Keci Frederiksen,
You have all in Your unique ways made work life a little funnier.
To my family: my mother, Erik, my sister and three brothers and their families, my father in-law,
Elly, and the rest of my family in-law, and my cousin, Anitta Callesen and her family: Thank you
for being good company, for solicitude, for practical help, for encouragements and genuine interest
in this project.
To my three beautiful daughters, Gry, Liv, and Sif: You all arrived during the Ph.D. period and
have been a great blessing to me. I thank you reminding me about the important things in life and
how to prioritize these, and for being loving and forgiving, when I did not succeed.
Many more deserves to be mentioned, but my absolute greatest acknowledgments and thanks are
directed at my husband, Arne, who has supported me unconditionally, encouraged me and loved
me, and patiently laid ear to major and minor concerns of mine about this thesis during six years.
You truly have proven that you want to “walk all the way and back again” with me!
___________________________________________
ix
Preface
I am often asked the question: “Why did you choose to get into research on faith and health?” It
would seem that you need a particular reason for doing that, because this kind of research is still
rather controversial in Denmark. My personal motivation was fired by a curiosity about whether
and how some of the deepest feelings and considerations on existential and religious matters
become important when adjusting to stressful life circumstances in a society where religion is not
exactly the first topic to be discussed at a dinner party! My own frame of reference is Christianity,
in which I was born and raised. To me, belief in God has always been an important and integrated
part of my life. Especially during life-changing experiences belief in a transcendent reality has been
a source of comfort, challenge, joy, gratitude, and hope. I have witnessed how belief offered a
reference of interpretation and support to family members and friends who suffered from life
threatening disease such as cancer, and how they in their religious interpretation, miraculously lived
longer than expected or even survived a severe diagnosis. To others, traumatic events became a
stumbling block that threw them into doubts and struggles which changed their beliefs and relations
to others radically. However, I know that “to be a believer” means a lot of different things to Danes
today, and that these beliefs may be hard to express – even for people who can be characterized as
having traditional religious beliefs. Given my personal background, I do have my pre-assumptions
which may have influenced the course of the project and the choices of methodology and measures.
Trying to be open and critical about my own potential biases, I also consider my background as a
Christian to have guided me to be sensitive towards this controversial topic – especially during
qualitative interviews with patients to whom existential and religious questions were very present
and for some a heavy burden. I also consider this project as a “case of learning by doing”. Situated
in a quantitative oriented research unit I may have been methodologically biased in approaching the
research topic at hand with tools of systematic literature reviews to guide my choice of methods and
measures. Furthermore, taking a functional approach to the study of religion, focus has been
directed towards what “religion does” to people in crisis, rather than “what it is”, and thereby
looking for effects instead of unfolding the phenomenology of beliefs among Danes during major
negative life events. Because this present study is one of the first on religious coping in Denmark, it
was decided to rely on theoretical work and measures developed in the United States because no
validated measures on religious coping existed at the time of preparing the studies underlying this
___________________________________________
x
thesis (2007). However, as the project proceeded other methods were needed to shed new light on
the research questions and methods used. As such, this thesis also reflects some of the decision-
making processes and assumptions underlying much research but seldom made entirely explicit.
Heidi Frølund Pedersen
Aarhus, July 2013

___________________________________________
xi
List of abbreviations
BDI Becks Depression Inventory
Brief RCOPE Brief Religious Coping Scale
Brief SCOPE Brief Spiritual Coping Scale
CAM Conventional and Alternative Treatment
CBI The Cancer Behavior Inventory
CCI Charlson Co Morbidity Index
COPD Chronic obstructive pulmonary disease
FACIT The Functional Assessment of Cancer Illness Therapy Scale
FACIT-Sp The Functional Assessment of Chronic Illness Therapy - Spiritual Well-
being Scale
LDP Lung disease patients
LRE List of Recent Event
NEO-FFI NEO Five Factor Inventory
PSS Perceived Stress Scale
RAAS Revised Adult Attachment Scale
RCOPE Religious Coping Scale
QoL Quality of life
___________________________________________
2
English summary
The assumption that people turn to religion when faced with major negative life events – especially
during life threatening disease - has received increased attention in research on faith and health
during the last 15 years. It is suggested that religion can represent a coping resource to the
individual during adjustment to negative life events. Empirical studies have mainly found religious
coping to be associated with positive outcomes such as higher well-being and lower levels of
distress, although some contradictory results have been found. In recent years the measurement of
religious coping has been refined, and studies have revealed that some forms of religious coping
reflecting religious doubts, feelings of spiritual abandonment and thoughts about Gods punishments
(negative religious coping) appears to be burden in adjustment and have been associated with lower
well-being, higher amount of distress, and increased mortality among medically ill patients.
However, the majority of empirical work has been conducted in the United States, which is
characterized as the most religious of the modern, Western societies. Less is known about the role
of religion during major negative life events in more secularized societies like Scandinavia. In this
present thesis the main aim was to investigate to which degree newly diagnosed Danish lung
disease patients (LDP) turn to religion as a coping recourse when compared to healthy individuals
of whom some reported negative life events. Furthermore, it was explored to which degree religious
coping was associated with quality of life (QoL) and whether individual psychosocial
characteristics were associated with negative religious coping (religious struggles). Finally, it was
explored to which degree measures on religious coping developed in the United States are valid and
applicable in a secular context.
With the aim of providing novel data on religious coping in secular societies, four independent
empirical studies was conducted including a group of newly diagnosed LDPs (mainly lung cancer
and chronic obstructive pulmonary disease (COPD) and an age- and gender matched control group.
The two samples responded to questionnaires on socio-demographic information, religious coping
measured by Brief religious coping scale (Brief RCOPE), religious, spiritual, and existential
concerns, QoL, existential well-being, and personality factors such as personality traits and
attachment style. The healthy control group was asked to report if they had experienced negative
life events within the last 12 months. Furthermore a qualitative study was conducted among three
___________________________________________
3
focus groups of healthy Danes, and ten individual interviews with lung cancer patients. Participants
were asked to respond to a questionnaire on religious (Brief RCOPE) and spiritual coping and
reflect on the content and relevance of the questionnaire when adjusting to negative life events.
In study 1 it was found that LDPs did report to engage religious coping strategies during illness
adjustment to some degree. Positive religious coping was more prevalent than negative religious
coping strategies. However, the level of religious coping was considerably lower than that found in
studies from the U.S. Patients characterized as believing or spiritual reported more positive
religious coping than non-believing patients, but no differences were found between believing,
spiritual, or non-believing patients regarding negative religious coping. Positive religious coping
was not found to be significantly associated with QoL, however negative religious coping was
significantly associated with lower QoL among LDPs. Furthermore it was found that a small part of
the patients reported to have more existential, spiritual, and religious concerns following the lung
disease, and a minority expressed a need to talk to a health care professional about existential or
spiritual concerns, whereas no one wished to talk about their religious concerns with a health care
professional.
In study 2, LDPs was found to report significantly more positive religious coping, especially
positive religious meaning-making and asking forgiveness, when compared to a group of healthy
Danes of whom some reported negative life events. Positive religious coping was not found to be
associated with QoL or existential well-being in any of the participating samples, however negative
religious coping was found to be associated with lower QoL among LDPs only. Furthermore,
reporting to receive support from one’s congregation was associated with higher QoL and
existential well-being among the healthy control participant who did not report negative life events.
In study 3 it was investigated whether different psychosocial factors was associated with reporting
religious struggles in a group of middle-aged- and elderly Danes of whom some reported negative
life events. Initial analyses suggested the that impact of event on QoL, lower income, higher levels
of neuroticism, insecure attachment, higher frequency of church attendance and reporting
congregational support was associated with reporting religious struggles. However, in a final
regression model testing the significant variables from the initial analyses, it was found that higher
levels of the personality trait neuroticism and reporting congregational support were the only
statistical significant variables associated with religious struggles.

___________________________________________
4
In study 4 it was examined to which degree a measure on religious coping developed in the U.S
(Brief religious coping scale, Brief RCOPE) and a newly developed scale on spiritual coping were
applicable and valid among a group of healthy middle-aged and elderly Danes and Danish lung
cancer patients. In an exploratory thematic analysis three themes in relation to validity emerged: 1)
The importance of the available language and “religious capital” of the individual and 2) the
influence of the specific context of the individual when asked to respond to questions about
religious coping. Furthermore 3) the question of whether religion and spirituality should be
understood as a universal or context-specific phenomenon that is measurable and comparable across
cultures was found to be a crucial theme, and discussed in relation to the methods applied in the
psychology of religion.
It is concluded that religious coping as measured by the Brief RCOPE was to some degree prevalent
among Danes facing major life events, and especially among LDPs, partly supporting the
hypothesis that life threatening disease is likely to make people turn to religion, even among
individuals living in a highly secular society. However, as such, religious coping as operationalised
in the measure of Brief RCOPE did not appear to be a central phenomenon among the participating
individuals, because it assumes a mainly theistic perception of the sacred. Although nearly 65% of
the LDPs and healthy participants reported to believe in God or a spiritual being, sociological
studies suggest that the character of belief in God have changed from concrete beliefs in a personal
and active God to more ill-defined and impersonal concepts of a higher being. The qualitative study
suggested that religious beliefs and experience was a private and often ‘tacit’ issue to the
participants suggesting that quantitative measures may be problematic to apply in especially secular
societies, because participants may face difficulties in accessing their beliefs at a solely cognitive
level. Furthermore, signs of other religious and spiritual strategies of meaning-making in adjustment
to major negative life events that were not captured by the Brief RCOPE were found suggesting that
religious and spiritual beliefs may become important, even to individuals who do not perceive
themselves as very religious, and new measures and methods are called for. Narrative methodology
may allow the individual to come closer to how personal beliefs have formed, what they contain,
and how they become important in interpretation and meaning-making during negative events.
However, as found in this thesis, expressing religious doubts, thoughts about God’s punishment and
feelings of spiritual abandonment during lung disease were associated with lower levels of QoL,
indicating the individual to experience tension and despair in association to illness. Health care

___________________________________________
5
personnel should take serious this potential threat to the health and well-being of the individual
facing lung disease and be attentive to potential struggles among patients. However, more
knowledge is needed regarding the prevalence of religious, but also spiritual and existential
struggles among different medical samples in secular societies before any interventions can be
suggested, and future studies should pay attentions to the impact of individual differences in the
development of religious, spiritual, or existential struggles.
___________________________________________
6
Dansk resumé (Danish summary)
Antagelsen at mennesker vender sig til religion, når de bliver konfronteret med større negative
livsbegivenheder – særligt i forbindelse med livstruende sygdom - har fået større opmærksomhed i
tro og helbred forskningen igennem de sidste 15 år. Det er foreslået, at religion kan optræde som en
’coping’ ressource for individet i forbindelse med håndteringen af negative livsbegivenheder.
Empiriske undersøgelser har overvejende fundet at religiøs coping er forbundet med positive udfald
så som større velbefindende samt lavere forekomst af sorg og lidelse (’distress’), om end
resultaterne har været modstridende. De senere år er målingen af religiøs coping blevet forfinet, og
studier har fundet at visse former for religiøs coping, der afspejler religiøs tvivl, følelse af åndelig
forladthed, og tanker om Guds straf (også kaldet ’negativ religiøs coping’), synes at udgøre en
byrde i individets tilpasning, og er blevet associeret med lavere velbefindende, større forekomst af
sorg og lidelse, samt forøget dødelighedsrisiko blandt medicinsk syge patienter. Dog er størstedelen
af de empiriske studier gennemført i USA, der er blevet betegnet som det mest religiøse af de
moderne, vestlige samfund. Vi ved meget lidt om religionens rolle i forbindelse med større negative
livsbegivenheder i mere sekulariserede samfund som de skandinaviske. I nærværende afhandling
var hovedformålet at undersøge, i hvilken grad nydiagnosticerede danske lungepatienter vender sig
til religion som en coping ressource i sammenligning med raske danskere, hvoraf nogle angav
negative livsbegivenheder. Derudover blev det undersøgt, i hvilken grad religiøs coping var
forbundet med livskvalitet, og om individuelle psykosociale karakteristika var forbundet med
negativ religiøs coping (også kaldet ’religiøs anfægtelse’). Slutteligt blev det undersøgt hvorvidt
spørgeskemaer om religiøs coping udviklet i USA er valide og anvendelige i en sekulær kontekst.
Med henblik på at tilvejebringe ny viden om religiøs coping i sekulære samfund blev fire
uafhængige empiriske undersøgelser gennemført, og inkluderede en gruppe nydiagnosticerede
lungepatienter (hovedsageligt patienter med lungekræft og kronisk obstruktiv lungesygdom) samt
en rask kontrolgruppe matchet til lungepatientgruppen på baggrund af alder og køn. De to grupper
svarede på spørgsmål om socio-demografiske forhold, religiøs coping målt med spørgeskemaet
’Brief religious coping scale’ (Bief RCOPE), religiøse, spirituelle, og eksistentielle overvejelser,
livskvalitet, eksistentielt velvære, og personlighedsfaktorer såsom personlighedstræk og
tilknytningsstil. Den raske kontrolgruppe blev bedt om at angive, om de havde oplevet negative

___________________________________________
7
livsbegivenheder indenfor de sidste 12 måneder. Endvidere blev en kvalitativ undersøgelse
gennemført blandt tre fokusgrupper bestående af raske danskere, samt 10 individuelle interviews
med lungekræftpatienter. Deltagerne blev bedt om at respondere på spørgeskemaet om religiøs
coping (Brief RCOPE) og et nyt skema om spiritual coping, og reflektere over indholdet og
relevansen af spørgeskemaet i forbindelse med håndteringen af negative livsbegivenheder.
I undersøgelse 1 blev det fundet at lungepatienter i nogen grad angav at anvende religiøse coping
strategier i forbindelse med sygdomshåndtering. Positiv religiøs coping forekom oftere end negative
religiøse coping strategier. Dog var forekomsten af religiøs coping betydeligt lavere end niveauet
fundet i studier fra USA. Patienter, der anså sig selv som troende eller spirituelle, angav mere
positiv religiøs coping end ikke-troende patienter, men ingen forskelle blev fundet i forekomsten af
negativ religiøs coping mellem troende, spirituelle og ikke-troende patienter. Positiv religiøs coping
var ikke signifikant forbundet med livskvalitet, mens negativ religiøs coping viste sig at være
signifikant forbundet med lavere livskvalitet blandt lungepatienter. Derudover viste resultaterne at
en mindre andel af lungepatienterne angav at have haft flere religiøse, spirituelle, og eksistentielle
overvejelser som følge af deres sygdom, og mens en minoritet angav at have et behov for at tale
med sundhedspersonalet om eksistentielle og spirituelle overvejelser, ønskede ingen at tale med
sundhedspersonalet om deres religiøse overvejelser.
Undersøgelse 2 viste, at lungepatienter angav signifikant mere positiv religiøs coping, særligt
positiv religiøs mening og behov for tilgivelse, i sammenligning med en gruppe af raske danskere,
hvoraf nogle angav negative livsbegivenheder. Positiv religiøs coping var ikke signifikant associeret
med livskvalitet eller eksistentielt velbefindende i nogen af de deltagende grupper. Derimod viste
negativ religiøs coping sig at være signifikant forbundet med lavere livskvalitet udelukkende blandt
lungepatienter. Ydermere blev det fundet at raske kontrolpersoner, der ikke angav negative
livsbegivenheder og som rapporterede at modtage støtte fra deres trosfæller, havde en højere
livskvalitet og eksistentielt velvære.
I undersøgelse 3 blev det udforsket, hvorvidt forskellige psykosociale faktorer var forbundet med
det at opleve religiøse anfægtelser (negativ religiøs coping) blandt midaldrende og ældre danskere,
hvoraf nogle angav negative livsbegivenheder. I de indledende analyser blev det foreslået, at
indflydelsen af en negativ livsbegivenhed på livskvalitet, lavere indkomst, højere niveauer af
personlighedstrækket neuroticisme, usikker tilknytning, højere frekvens af kirkegang, samt at

___________________________________________
8
angive støtte fra ens trosfæller var forbundet med det at opleve religiøse anfægtelser. Dog viste den
endelige regressionsanalyse indeholdende de signifikante variable fra de indledende analyser, at
neuroticisme og det at modtage støtte fra ens trosfæller var de eneste signifikante variable forbundet
med det at opleve religiøse anfægtelser.
Undersøgelse 4 havde til formål at efterprøve, hvorvidt et spørgeskema om religiøs coping udviklet
i USA (Brief RCOPE) og et nyligt udviklet spørgeskema om spirituel coping var anvendelige og
valide blandt en gruppe af raske midaldrende og ældre danskere samt danske lungekræftpatienter. I
en eksplorativ tematisk analyse fremkom tre temaer med relation til validitet: 1) Betydningen af
individets tilgængelige sprog og ”religiøse kapital” og 2) betydningen af den konkrete kontekst som
individet er situeret i, når vedkommende bliver adspurgt om religiøs coping. Derudover blev temaet
om 3) hvorvidt religion og spiritualitet skal anskues som et universelt eller et kontekst-specifikt
fænomen, der er målbart og sammenligneligt på tværs af kulturer, fundet at være afgørende i
forhold til validitet, og blev diskuteret i relation til de anvendte metoder indenfor
religionspsykologien.
På baggrund af de fire undersøgelser, kan det konkluderes, at religiøs coping som målt ved hjælp af
Brief RCOPE i nogen grad var forekommende blandt danskere, som var konfronteret med større
negative livsbegivenheder, særligt blandt lungepatienter. Dette støtter til dels hypotesen, at
livstruende sygdom kan få folk til at vende sig til religion, selv blandt mennesker der generelt
opfattes som meget sekulariserede. Dog, som sådan kan religiøs coping operationaliseret ved hjælp
af Brief RCOPE ikke siges at have været et centralt fænomen blandt de deltagende personer, fordi
dette spørgeskema forudsætter en teistisk forståelse af ”det hellige” (opfattelsen af en konkret og
handlende Gud). Selvom næsten 65% af lungepatienterne og de raske kontrolpersoner angav at tro
på Gud eller en spirituel kraft, viser sociologiske undersøgelser, at karakteren af gudstro har ændret
sig fra konkret tro på en personlig og aktiv Gud til mere udefinerbare og upersonlige begreber om et
højere væsen. Den kvalitative undersøgelse viste, at religiøs tro og religiøs oplevelse for mange
deltagere var privat og ofte med karakter af ’tavs viden’, hvilket indikerer at kvantitative
måleredskaber kan vise sig at være problematiske at anvende, særligt i sekulære kulturer, fordi
deltagerne kan opleve vanskeligheder ved at skulle tilgå deres personlige tro eller overbevisning på
et rent kognitivt plan. Ydermere fandt den kvalitative undersøgelse tegn på forekomsten af andre
religiøse og spirituelle meningsdannelsesstrategier i håndteringen af negative livsbegivenheder, som

___________________________________________
9
ikke blev indfanget af Brief RCOPE. Dette antyder at religiøs og spirituel tro er vigtigt, selv blandt
personer der ikke anser sig selv for meget religiøse, men at nye måleredskaber og metoder er
nødvendige i fremtidige studier. Narrativ metode kan måske i højere grad give den enkelte
mulighed for at komme i kontakt med, hvordan personlig tro er blevet udformet, hvad den rummer,
og hvordan den bliver betydningsfuld i tolkningen og meningsdannelsen i forbindelse med negative
livsbegivenheder. Imidlertid, som fundet i denne afhandling, så er det at udtrykke religiøs tvivl,
tanker om Guds straf og følelsen af åndelig forladthed i forbindelse med lungesygdom forbundet
med lavere livskvalitet, hvilket antyder at patienten oplever stor anspændthed og fortvivlelse i
forbindelse med lungesygdommen. Sundhedspersonalet bør derfor tage denne potentielle trussel
mod helbred og velvære alvorligt og være opmærksom på ”religiøs anfægtelse” blandt
lungepatienter. Dog er der brug for mere viden om forekomsten af religiøs, men også spirituel
anfægtelse og eksistentiel fortvivlelse, blandt forskellige medicinske grupper i sekulære samfund
inden forslag til intervention eller forebyggelse kan foreslås. Fremtidige studier kan med fordel rette
opmærksomhed mod den potentielle indflydelse af individuelle forskelle i udviklingen af religiøse
og spirituelle anfægtelser, og eksistentiel fortvivlelse.
___________________________________________
10
Introduction
In March 2007 the Danish Nursing Journal (Sygeplejersken) published a special issue on “faith and
health” and the main article was titled: “Hospitals disregard patients’ spiritual needs” (Søndergaard
& Christensen, 2007). At that time very little was written or spoken on issues regarding faith and
health in Denmark, and the reluctance to talk with patients about religiosity, spirituality, and
existential issues in the health care system may also have hindered research interest or possibilities
in this field. Internationally, research has found spirituality and religiosity to impact decision-
making, course of illness, and quality of life (QoL) during severe illness such as cancer (Koenig,
King, & Larson, 2012). Furthermore, spiritual or existential needs have been found to be just as
important to address as psycho-social needs (Puchalski et al. 2009), and recently the
implementation of a bio-psychosocial-spiritual model of health in research and health care has been
suggested (Dyer, 2011). However, the majority of studies on faith and health have been conducted
in Northern America, which is far more religiously oriented than Northern Europe where the
relevance of implementing spirituality in research and health care in more secular societies has been
questioned (Salander, 2006). In practice, personnel employed in Danish health care institutions
hesitate in offering spiritual care because the spirituality or religiosity of the patient is considered a
private matter (Christensen & Turner, 2008; Dam, Johansen, Jørgensen, Winck, 2006).
Additionally, a recent study suggests that only 16% of the general population in Denmark expects
the Danish health care system to be able to provide spiritual care during life threatening illness
(PAVI, 2013). Yet, little is known about the actual religious, spiritual, and existential needs and
resources among Danes facing severe illness, or whether religiosity or spirituality impacts the QoL
of the patient. It is argued that due to secularization coherent world views may be lacking among
people living in secular societies, and result in difficulties in coming to terms with major life events
potentially impacting adjustment negatively (Stålhandske, Ekstrand, Tyden, 2011). In 2008, a
Swedish psychologist of religion encouraged the psychology of religion in Scandinavia to take
responsibility for identifying and assessing categories of function and dysfunction for an existential
public health and, in pace with the increased focus on well-being in public health, to provide models
and interventions for enhancing existential well-being (DeMarinis, 2008). Furthermore, a ‘Research
Network on Faith and Health’ was established first in Denmark in 2007 and since extended to
include Scandinavia in 2012 (see: www.faith-health.org), thus enhancing research in this area. The

___________________________________________
11
main aim of this thesis therefore is to explore, in a Danish context, the prevalence, characteristics
associated with, and influence of religious coping on QoL during severe illness and negative life
events.
The Danish context
The reluctance shown particularly towards religious and spiritual issues in Denmark calls for an
explanation, and in the following a short description of the characteristics of Danish society and
attitudes towards religion is given. Denmark has been named the most secularized society in the
world (Zuckerman, 2008). According to theories of secularization, a society becomes secularized as
a consequence of modernity, and ultimately religion disappears (Andersen & Lüchau, 2008). Due to
the industrial revolution and modernity following this development, Denmark is now one of the
richest societies in the world, having a strong welfare system which allows its inhabitants to enjoy a
relatively high standard of living and security, a well-established democracy, and a high degree of
individual freedom. However, there is a low commitment to religious institutions, while religion as
such has decreased in importance in Denmark. Following interviews with 150 Danes and Swedes,
Zuckerman (2008) arrived at a picture of Danes as ‘cultural Christians’, for whom religion (the
Christian heritage) was mostly about food, culture, and social events that were drained of all
religious content and basically a non-issue. According to the European Value Survey (2008), Danes
seem to prefer a “belonging without believing” relationship to the church. Approximately 80% of
the population are members of the Evangelical Lutheran Church (Den Danske Folkekirke), but only
10% attend church services regularly (e.g. once a month). Furthermore, traditional religious ideas
are declining: Only 36% believe in life after death, 21% in sin, and 9% in Hell. Moreover, the
picture of God has changed during the last 50 years from concrete, personal conceptions into more
ill-defined and vague ideas of an impersonal God (Lüchau, 2005). Despite the limited support for
traditional religious ideas, very few (7%) are willing to characterize themselves as atheists
(European Value Survey, 2008). Neither very religious, nor confessed atheists, 7 out of 10
characterize themselves as “believers”, and the majority of Danes state that they are “Christians in
their own way” (Iversen, 2006). Thus, even though traditional religion has lost its impact and
support, as the original theories of secularization predicted, it has not disappeared, but rather
changed into individualized and privatized forms (Andersen & Lüchau, 2008). Hence, researchers
call for new concepts of religion to capture the changes we are experiencing (Rosen, 2009).

___________________________________________
12
The concepts of religion and spirituality in a secular society
According to Rosen (2009) the previous conceptualization of religion assumed a system of ideas,
institutions and practices that shared the same core, a so-called “packed religion”. However,
religion in Denmark (and other societies influenced by secularization, individualization, and the
privatizing of religion) may be conceptualized rather as “unpacked religion” with several distinct
aspects not sharing a common core. In this new conceptualization, religion as “unpacked” can be
understood as consisting of five independent aspects: as personal beliefs that are actualized ad-hoc
in respect to context; as routinized religion, which refers to the religious institution to which one
can belong; as practices and traditions like passage rites and religious fests that for the majority of
people are devoid of religious content but upheld for social reasons; and, finally religion-as-
heritage, which has no religious content either, but signifies the cultural history, the shared norms
and values, of those whose heritage lies in a given church or religious tradition (Rosen, 2009:9).
The concept of spirituality is not explicitly a part of this definition, but calls for clarification since it
has made its entrance into theoretical and empirical research on faith and health in Scandinavia
(Stifoss-Hansen, 1999). Some have argued that the entry of the concept of spirituality covers a trend
towards individualized beliefs disconnected from organized religion, and is exemplified in the
phrase “being a believer, but not religious”, meaning that the individual relates to something beyond
human life but does not subscribe to traditional religion except for passage rites and feasts (Rosen,
2009; Stifoss-Hansen, 1999). However, internationally, the concept of spirituality is fenced in
conceptual confusion covering state of well-being, belief in a transcendent reality, and existential
concerns (Salander, 2006), and this also seems to be the case in Denmark. In a study among 514
adult Danes, la Cour, Ausker, & Hvidt (2012) found that six distinct understandings of the concept
‘spirituality’ exists: (1) positive dimensions in human life and well-being; (2) New Age ideology;
(3) an integrated part of established religious life; (4) a vague striving, opposed to religion; (5)
selfishness; and (6) ordinary inspiration in human activities. Thus, when operating with the concept
in research projects it is recommended to define “in a few words” what is meant by spirituality. In
this thesis, spirituality is understood as something deeply involved in the personal beliefs and
practices of the individual, hence not stemming from religion-as-heritage − the latter presupposes a
shared cultural heritage from the dominating church or religious tradition, which in Denmark is
Christianity − but represents beliefs influenced by other traditions, such as Eastern religions or other
untraditional beliefs in the transcendent.

___________________________________________
13
Alongside the religious and spiritual views of life among Danes are the secular, existential
orientations inspired by philosophy, humanism, and existential psychology not centered on a belief
in a transcendent reality. However, the religious, spiritual, and secular existential orientations share
some common features like offering interpretations of meaning, freedom, personal values and value
of life, and may often be present at the same time to the individual facing challenging life situations
(la Cour & Hvidt, 2010). Hence, research on faith and health among people in secularized societies
calls for conceptual clarity and sensitivity to different approaches to meaning-making and
adjustment during severe illness or stressful events.
A conceptual framework
Researchers from Scandinavia have argued that the conceptual umbrella embracing research on
faith and health in secularized areas should be defined as existential health (DeMarinis, 2008), and
a conceptual framework has been developed as a guide for mapping the issue of interest in
secularized societies to be more distinct about what is meant when investigating existential health.
la Cour & Hvidt (2010) proposes to distinguish between religious orientation, spiritual orientation,
and secular existential orientation, although acknowledging that they have common features.
Furthermore for all three meaning-making orientations, three dimensions underlie the nature of
these orientations: knowing (the specific content), doing (any given practice), and being (the
importance to the individual). This thesis mainly focuses on the prevalence and importance of the
religious orientation during life threatening and stressful situations among Danes. However as will
be presented during this thesis, secular existential and spiritual meaning-making orientations are
present and important aspects to investigate in terms of existential health in secular societies too, yet
not the main focus of this thesis. It is argued that Danes hold a “religion in crisis” (la Cour, 2005).
This statement has two senses: That traditional “packed” religion among Danes is in crisis because
it is disappearing. The second sense: That religion among Danes is most likely activated and
becomes important during important life transitions and major negative events such as life
threatening disease. In the definition of religion as unpacked (Rosen, 2009) it is highlighted that
personal beliefs are actualized and developed cognitively ad-hoc through life experiences such as
major negative life events. However, very little theoretical and empirical research has been
conducted in Denmark to highlight how religious orientation develops or unfolds in the three
dimensions of knowing, doing, and being during crisis, and whether religious orientations represent

___________________________________________
14
a resource in adjustment to crisis among Danes. The theory of religious coping developed by
Kenneth I. Pargament (1997) offers a framework for investigating the content, practice, and
importance of religious beliefs in coping with crisis and may also apply in investigating religious
orientation among Danes.
Religious coping
Research on religious coping has received increased attention since Pargament (1997) formulated
his transactional theory on religious coping. The theory is embedded in a functional approach to
religion focusing on how religion and spirituality is involved in the process of coping during times
of distress. The theory builds on the core assumptions of Lazarus and Folkman’s (1984) functional
transactional theory of coping. Basically, coping is understood as the cognitive and behavioral
processes engaged by the individual to reduce stress and regain psychic equilibrium during
incidences of threat, challenge, or loss. Central to the theory of religious coping is the concept of an
orienting system, which is mainly cognitively based and consists of values, habits, relationships,
generalized beliefs, and personality. The orienting system determines how a given stressor is
appraised, which resources will be activated and which coping strategies are likely to be
implemented (Gall & Guirguis-Younger, 2013). It is assumed that religious beliefs may engender a
sense of optimism, control, and meaning that affects whether a given stressor is appraised as
stressful and thereby affect the level of stress and potentially health (Dull & Skokan, 1995).
However, religious coping is not solely cognitive in nature, but multidimensional (e.g., cognitive,
behavioural, affective, relational), it serves multiple purposes (e.g., meaning-making, intimacy,
control, comfort, closeness with God), and is multi-valent (i.e., potentially helpful or harmful). The
transactional model of religious coping has been criticised for being too static as it does not take
into account the possible changes, developments, or declines of religious beliefs. Therefore,
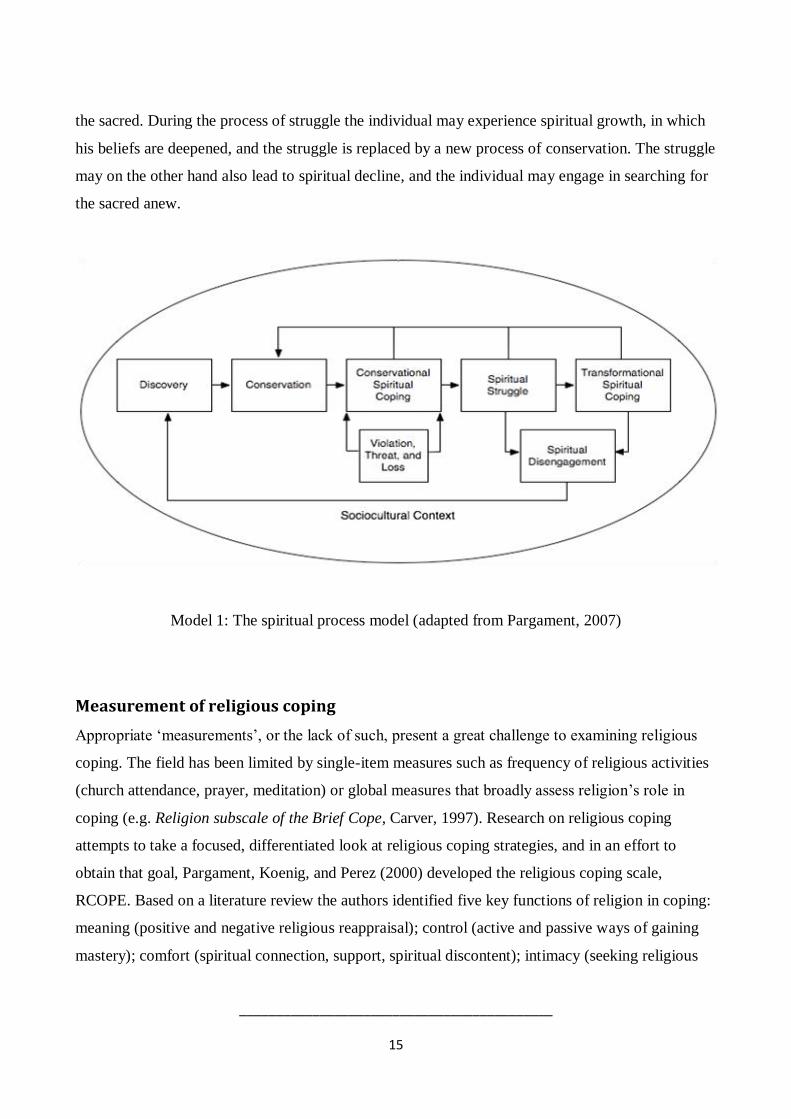
Pargament (2007) developed the spiritual process model (see model 1). In this model the process of
searching for the sacred, conserving the sacred and transforming the sacred are core concepts. The
sacred is understood as the ‘ultimate concern’ of the individual, and may be secular in nature, such
as family and friends, but becomes spiritual when it is related to divine aspects of life. When the
sacred has been discovered the individual engages in consolidating his beliefs through strategies of
conservation. However, when struck by a major negative life event religious struggle is likely to
occur, and the individual engages in coping strategies to transform and hold on to his beliefs about
___________________________________________
15
the sacred. During the process of struggle the individual may experience spiritual growth, in which
his beliefs are deepened, and the struggle is replaced by a new process of conservation. The struggle
may on the other hand also lead to spiritual decline, and the individual may engage in searching for
the sacred anew.
Model 1: The spiritual process model (adapted from Pargament, 2007)
Measurement of religious coping
Appropriate ‘measurements’, or the lack of such, present a great challenge to examining religious
coping. The field has been limited by single-item measures such as frequency of religious activities
(church attendance, prayer, meditation) or global measures that broadly assess religion’s role in
coping (e.g. Religion subscale of the Brief Cope, Carver, 1997). Research on religious coping
attempts to take a focused, differentiated look at religious coping strategies, and in an effort to
obtain that goal, Pargament, Koenig, and Perez (2000) developed the religious coping scale,
RCOPE. Based on a literature review the authors identified five key functions of religion in coping:
meaning (positive and negative religious reappraisal); control (active and passive ways of gaining
mastery); comfort (spiritual connection, support, spiritual discontent); intimacy (seeking religious
___________________________________________
16
support from others; interpersonal spiritual discontent); and life transformation (religious direction,
conversion) (Gall & Guirguis, 2013). These core functions served as the theoretical underpinning of
the measure, and 21 different coping strategies were developed resulting in a 105 item
questionnaire. The measure has been tested and validated, but because of the rather lengthy
questionnaire, a shorter version, Brief RCOPE, was developed including 14 items (Pargament,
Smith, Koenig, & Perez, 1998). This questionnaire includes positive religious coping, referring to a
positive connection with the transcendent, with others, and a vision of the world as good, and
negative religious coping, which involves religious struggles primarily with the transcendent and
others. The Brief RCOPE is the most widely used measurement on religious coping and has shown
good psychometric qualities in several different samples in North America. Furthermore, is has
been revised for use among other religious traditions such as Judaism (Rosmarin, Pargament, &
Mahoney, 2009), Islam (Khan & Watson, 2006), and Hinduism (Tarakeshwar, Pargament, &
Mahoney, 2003), and it is now being translated into several different languages.
Empirical findings
Comprehensive reviews on empirical findings of religious and spiritual coping during illness and
negative events have recently been conducted (Exline, 2013; Gall & Guirguis, 2013; Lavery & Hay,
2010). The following is a short outline based on some of the main findings in this research area. In
general, religious coping resources have been associated with beneficial outcomes on health and
well-being among medically ill patients and participants reporting stressful events such as
bereavement (Gall & Guirguis, 2013). Contradictory findings have nonetheless been found, but as
previous studies mainly relied on uni-dimensional measures of public religious activity as an
expression of religious coping during illness, explaining these findings was made difficult (Thuné-
Boyle, Stygall, Keshtgar, & Newman, 2006). However, since the development of multidimensional
measures like the Brief RCOPE more studies have encompassed these and have been able to
differentiate religious coping strategies to a higher degree (Lavera & O’Hay, 2010). The distinction
between positive and negative strategies of religious coping seems to be able to explain some of the
diversity in findings, and the most consistent results have been found on negative religious coping
also referred to as ‘religious struggle’.

___________________________________________
17
Negative religious coping
A meta-analysis conducted by Ano & Vasconcelles (2005) on religious coping strategies and
psychological adjustment during stressful events suggests negative religious coping to be associated
with higher levels of depression, anxiety, and distress. Furthermore, in a systematic review of
studies on cancer populations (Thuné-Boyle, Stygall, Kesthgar, & Newman, 2006) 3 out of 17
studies found negative effects between religious coping and adjustment, 7 found some positive
effects, and 7 found no effect. However, the different measures applied did not all distinguish
between positive and negative forms of religious coping. Recent studies applying the Brief RCOPE
have found negative religious coping to be associated with higher levels of depression and anxiety
among breast cancer patients (Thuné-Boyle, Stygall, Keshtgar, Davidson, & Newman, 2013), and
lower QoL among a group of cancer patients (Tarakeshwar and colleagues (2006). Furthermore
Cole (2005), Fitchett and colleagues (2004), and Zwingmann and colleagues (2008) found negative
religious coping to be associated with poorer adjustment to illness in terms of pain frequency,
poorer overall physical functioning, and emotional distresss among groups of congestive heart
failure patients, cancer patients, and diabetes patients.
Positive religious coping
Results on positive religious coping still remain unclear. The meta-analysis conducted by Ano &
Vasconcelles (2005) suggested a moderate positive association between positive religious coping
and outcomes like spiritual growth, positive affect, higher self-esteem, and well-being, but a
negative association between positive religious coping and higher levels of depression and anxiety,
which signify that positive religious coping serves some adaptive functions. However, other studies
have found non-significant associations between positive religious coping and adjustment (Herbert
et al. 2009; Sherman et al. 2005, 2009). Methodological issues are at stake such as time of
measurement – especially among medically ill patients where stage of illness is considered to be
crucial. Furthermore, cross-sectional studies may blur the picture, as positive religious coping is
suggested to affect spiritual growth and thereby over time have a positive effect. Complicating
matters, studies have found positive and negative coping strategies to be positively correlated
indicating that patients may use positive and negative religious coping at the same time
(Zwingmann et al. 2006).
___________________________________________
18
Longitudinal studies
Sherman and colleagues (2005) argue that the reason why negative religious coping has a higher
impact on adjustment to cancer or other negative events may be that religious struggles are more
likely to represent a change in response to a negative event, whereas positive religious coping may
express maintenance of typical coping response. It is suggested that religious struggles can be
associated with spiritual growth in line with the spiritual process model (Pargament, Desai, &
McConnell, 2006; Pargament, 2007), however, the majority of empirical studies suggest that they
have more severe impact on adjustment, well-being, and physical health if they are maintained over
time. Sherman and colleagues (2009) found that among myeloma patients going through a
transplant operation, negative religious coping at baseline was associated with higher levels of
anxiety, depression and lower levels of well-being six months after the transplant operation.
Furthermore, Exline, Park, Smyth, & Carey (2011) found, on the basis of samples of cancer patients
and bereaved individuals, that religious struggles that lasted longer than a year were at risk of
turning chronic and have even more devastating consequences for the individual in terms of well-
being, and Pargament, Koenig, Tarakeshwar, & Hahn, (2001) found that negative religious coping
at baseline and at two-year follow-up was associated with higher mortality among elderly medically
ill patients. Although studies have found that positive religious coping strategies are far more
prevalent than negative religious coping strategies (Pargament, Koenig, & Perez, 2000), religious
struggle may be a “red flag” to be aware of to prevent harmful effects (Pargament et al., 2003).
Predictors of religious coping
Some studies have investigated the socio-demographic characteristics associated with religious
coping, and it is suggested that mainly elderly, lower educated, poorer people, women, and
minorities engage in religious coping strategies (Pargament, 1997). One explanation states that
people with limited access to secular resources seek spiritual resources to cope with stressful events.
Not surprisingly, studies also find that highly religious people engage in religious coping (Bell-
Meisenhelder & Marcum, 2004), although religious coping strategies may also become relevant to
less religious people facing traumatic events, e.g. bereaved parents (Brotherson & Soderquist, 2002)
and family members of homicide victims (Thompson & Vardaman, 1997). Another study on
spiritual struggles suggests that atheists and agnostics also engage in anger towards a hypothetical
God (Exline, Park, Smyth, & Carey, 2011). In recent years studies have investigated individual
psychological characteristics associated with religious coping. It has been argued that religious
___________________________________________
19
struggles may represent general poor psychological functioning and stem from multiple factors
(Lavera & O’Hay, 2010; Ano & Pargament, 2012). In a study, Ano & Pargament (2012) explored a
range of psychosocial predictors of spiritual/religious struggles, and suggested that a more negative
appraisal of stressful events, an insecure attachment to God, and neuroticism significantly predicted
spiritual struggles. Similarly, Exline and colleagues (2011) found that social cognitions of holding
God responsible for a traumatic event, perceiving the event as having a high degree of negative
impact to the individual, difficulties finding a meaning with a negative event, and seeing oneself as
a victim predicted spiritual struggles. Finally, Schottenbauer et al. (2006b) also found negative
religious coping to be associated with insecure attachment and viewing events as uncontrollable.
The application of religious coping theory among Danes
The majority of studies on religious and spiritual coping have been conducted in the context of the
United States, which has been characterized as the most religious of the industrialized societies in
the West (Schoenig, 2012). Due to increased fragmentation, deinstitutionalization, and privatization
of experience in the Western world (Bellah, Madsen, Sullivan, Swidler & Tipton, 1985; Gergen,
1991) the prevalence and impact of religious and spiritual orientations are also changing in the U.S.
Knowledge about the prevalence of religious resources in coping and how they affect adjustment
and QoL during stressful events in a far more secular culture like Denmark may potentially add
important knowledge to the U.S. and the rest of the international research in faith and health.
The theory of religious coping suggests that if religious beliefs are coherent and integrated in the
orienting system and supported by the society as an acceptable coping strategy, it is more likely that
religious resources will be activated and involved in coping during major life events (Pargament,
2007; Park, 2005). However, it is also suggested that even though religious ideas only make up a
minor part of the orienting system it may become an important part of the coping process
(Pargament, 1997). This could apply to Danes, who although not very religious, are not totally
removed from religious expressions. The ‘terror management theory’ also suggests that reminders
of one’s mortality such as life threatening disease is likely to activate religious responses to protect
self-esteem and bolster anxiety (Vail et al. 2010). However, less developed and integrated religious
beliefs may also be more easily shattered and incapable of functioning as a resource in crisis
(Pargament, 2007). It has been suggested that people influenced by secularization may to a higher

___________________________________________
20
degree lack coherent world views and when confronted with major life events such as loss, serious
illness, and accidents, their interpretations of the events and meaning-making becomes a difficult
task (la Cour, 2008; Stålhandske, Ekstrand, & Tyden, 2011). Thus, major life events are likely to
reveal fundamental frailty and shatter the worldview of the individual (Janoff-Bulman, 1992) and
thereby − among Danes − may also involve struggles in coming to terms with a traumatic event.
Empirical findings on religiosity during stressful events in Denmark
Studies on religious belief and health in Denmark are sparse, but a few studies conducted among
Danish samples give tentative support for the assumption that religious resources become more
relevant during stressful or life-threatening events. In a study among 480 hospitalized Danes
(Ausker, la Cour, Busch, Nabe-Nielsen, & Pedersen, 2008), it was found that religious, spiritual,
and existential practices correlated positively with illness severity, indicating that patients became
more religiously and spiritually engaged as the severity of the illness increased. Correlations were
strongest among the younger patients (>36 years). Furthermore, a study including 3,128 breast
cancer patients (Pedersen, Christensen, Jensen, & Zachariae, 2012) suggested that breast cancer
patients are more likely to be religiously oriented than the general population. In all, 83% of the
breast cancer patients reported to believe in God or a higher being, compared to the normal Danish
population of which approximately 65% report to believe in God or a higher being (The Danish
Value Survey, 2008). A recent twin study on religious coping during negative life events included
3,000 Danish participants, of whom approximately 1,830 had experienced a crisis that led to
increased reflection on religious matters. Even though the level of religious coping was lower
among the Danish participants than levels found in American studies, the tendency was clear:
participants, who had experienced a crisis, reported using both positive and negative strategies of
religious coping to a higher degree than the general sample, and losing a child or a partner led to the
highest score (Hvidtjørn, Hjelmborg, Skytthe, Christensen, & Hvidt, 2013). A qualitative study
among 12 terminally ill patients at hospice holding different views of life suggested that both
positive and negative religious coping strategies were engaged by some of the patients and that
eleven out of twelve prayed or meditated. Furthermore patients found it important and helpful to
talk about their different views of ‘life after death’ with a nurse (Nielsen, 2005). However, a
qualitative, longitudinal study among 21 younger (18-40 years) newly diagnosed cancer patients
suggested that younger Danes do not suddenly become very religious as a consequence of illness, if
___________________________________________
21
religion was not a part of their orienting system all ready. Instead, the worldview of the individual
was scaled up and engaged in meaning-making and adjustment to illness among both religious and
non-religious patients (Ausker, 2012). Studies on links between religiosity, spirituality, and
psychological outcomes such as QoL and depression following severe illness or stressful events are
still very limited in a Danish context, however a few studies have been conducted among medical
samples. A study on 460 breast cancer patients participating in a study on expressive writing found
that 77% reported to believe in God or a higher being, and 60% believed in the positive effect of
faith on their QoL. However, only 38% believed their faith to have any positive influence on the
course of cancer disease (Jensen-Johansen et al. 2012). Another study on faith and religious coping
among 97 heart attack patients suggested that there were no associations between religious coping
or belief in God/a higher being and depressive symptoms at baseline and at 6 month follow-up after
the heart attack. However, about one-fifth of the patients reported that, to some extent, they found
comfort in religion or spirituality, and one-fourth of the patients reported to have prayed or
meditated when faced with stressful events (Bekke-Hansen et al., 2013).
Although more studies on religion, spirituality and health in a secular context like Denmark have
begun to emerge during the last five years, much has yet to be explored. The extent to which
religious coping has been examined is still limited, and few studies have incorporated
multidimensional research measures but have relied on single-items. Studies are particularly needed
on links between religious beliefs, religious coping, and psychological outcomes, such as QoL
following negative events. Regrettably, at the time of writing, these studies are almost absent in a
Danish context. Furthermore, few international studies (Ano & Pargament, 2012), and none in a
Danish context so far, have examined associations between individual psychosocial characteristics,
such as personality traits and attachment style, and religious coping.

___________________________________________
22
Aim of this present thesis
In light of the growing interest in faith and health internationally, and recently in more secular
societies as Denmark, the main aim of this present thesis is to explore religious coping and
associations to psychological measures such as QoL and individual characteristics in Denmark. The
following questions were investigated based on two survey studies including:
1) newly diagnosed LDPs; and 2), a group of healthy Danes (of whom some had reported negative
life events); as well as a qualitative study among healthy Danes and lung cancer patients:
1. How prevalent is religious belief and religious coping among Danes facing severe lung
disease?
2. Is religious coping more prevalent among Danes facing severe lung disease and specific
negative life events than Danes coping with general, everyday challenges?
3. Do Danish LDPs report increased religious, spiritual, and/or existential concerns following
their diagnosis, and do they report a need to discuss these concerns with a health care
professional?
4. Is religious coping associated with QoL and existential well-being among Danes coping
with severe lung disease and specific negative life events?
5. Is religious struggle associated with individual psychosocial characteristics?
6. Are measures on religious coping developed in the United States applicable in a secular
context?
This present thesis is based on four independent papers. Before summarizing the results however, a
few remarks on the design and course of the studies on which this thesis is built should be
mentioned.
Study design
In 2007, a larger project on complementary alternative treatment and faith among newly diagnosed
Danish lung cancer patients and chronic obstructive LDPs was being prepared by Christina
Gundgaard Pedersen as a part of her PhD, and the principal investigator of this present thesis (Heidi
Frølund Pedersen) was responsible for the research questions and measures on faith and religious
coping as well as some of the measures of personality dispositions. Furthermore, she was

___________________________________________
23
responsible for establishing a control group matched on age, gender, education, and region to be
compared with the LDPs. Christina G. Pedersen was in charge of the recruitment procedures, and
the lung disease study was launched in the autumn of 2008. The lung disease study was planned to
be a longitudinal nationwide study with 6 month follow-up, and it was expected that, potentially,
1,500 LDPs would participate in the study. However, only five out of twenty-five possible
respiratory medicine clinics in Denmark (four on the main peninsula of Jutland and one on an island
in the eastern part of Denmark) chose to participate in the study, which resulted in an extended
recruitment period. During autumn 2009, the principle investigator of this present thesis took over
the responsibility of the recruitment of LDPs and contacted the five respiratory medicine clinics and
urged them to continue recruiting LDPs for the study for another year, as only 86 out of 337
questionnaires had been returned after one year of data collection. In this process the health
personnel reported that LDPs considered the number of questions to be overwhelming and,
furthermore, that some patients showed a certain reluctance towards the subject of the study,
namely, complementary alternative treatment and faith. Searching through some of the returned
questionnaires by hand, it became obvious that the questionnaires on religiosity and religious
coping suffered from a relatively high degree of missing responses. This led the principal
investigator of this present thesis to conduct a qualitative study among lung cancer patients and
three groups of healthy Danes to test the face validity of the questionnaire on religious coping. The
qualitative study led to insights on the validity of the questionnaires on religiosity and religious
coping, which is presented and discussed in Paper 4. However, since one of the aims of this present
thesis was to compare LDPs with a healthy control group it was not possible to make any
substantial changes in the questionnaires on religious coping in the study of the control group
(presented in Paper 2). The control group was established during spring 2010, and in October 2010
the recruitment of the LDPs ended, including 120 returned questionnaires at baseline, of which 9
were excluded due to a high amount of missing responses. This present thesis includes data from
the baseline study among LDPs, the age- and gender matched control group, and the qualitative
interviews among lung cancer patients and healthy Danes. An outline of the data collection periods
and sample characteristics in the individual studies is presented in Table 1. The content of the 3
baseline questionnaire packages and the specific measures used in the analyses of the four papers
are presented in the Appendix.
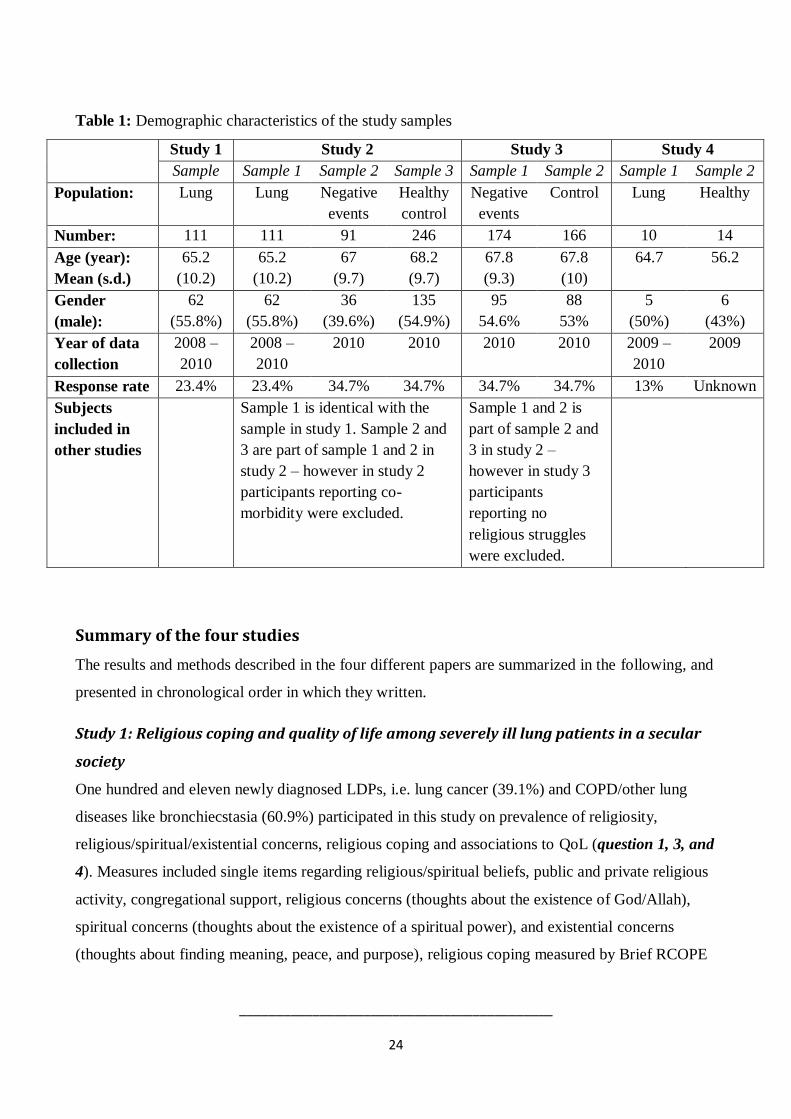
___________________________________________
24
Table 1: Demographic characteristics of the study samples
Study 1 Study 2 Study 3 Study 4
Sample Sample 1 Sample 2 Sample 3 Sample 1 Sample 2 Sample 1 Sample 2
Population: Lung Lung Negative
events
Healthy
control
Negative
events
Control Lung Healthy
Number: 111 111 91 246 174 166 10 14
Age (year):
Mean (s.d.)
65.2
(10.2)
65.2
(10.2)
67
(9.7)
68.2
(9.7)
67.8
(9.3)
67.8
(10)
64.7 56.2
Gender
(male):
62
(55.8%)
62
(55.8%)
36
(39.6%)
135
(54.9%)
95
54.6%
88
53%
5
(50%)
6
(43%)
Year of data
collection
2008 –
2010
2008 –
2010
2010 2010 2010 2010 2009 –
2010
2009
Response rate 23.4% 23.4% 34.7% 34.7% 34.7% 34.7% 13% Unknown
Subjects
included in
other studies
Sample 1 is identical with the
sample in study 1. Sample 2 and
3 are part of sample 1 and 2 in
study 2 – however in study 2
participants reporting co-
morbidity were excluded.
Sample 1 and 2 is
part of sample 2 and
3 in study 2 –
however in study 3
participants
reporting no
religious struggles
were excluded.
Summary of the four studies
The results and methods described in the four different papers are summarized in the following, and
presented in chronological order in which they written.
Study 1: Religious coping and quality of life among severely ill lung patients in a secular
society
One hundred and eleven newly diagnosed LDPs, i.e. lung cancer (39.1%) and COPD/other lung
diseases like bronchiecstasia (60.9%) participated in this study on prevalence of religiosity,
religious/spiritual/existential concerns, religious coping and associations to QoL (question 1, 3, and
4). Measures included single items regarding religious/spiritual beliefs, public and private religious
activity, congregational support, religious concerns (thoughts about the existence of God/Allah),
spiritual concerns (thoughts about the existence of a spiritual power), and existential concerns
(thoughts about finding meaning, peace, and purpose), religious coping measured by Brief RCOPE
___________________________________________
25
(Pargament et al. 1998) and QoL (Cella et al. 1993; Peterman, Fitchett, Brady, Pharm, & Cella,
2002). Results suggested that the number of LDPs reporting to believe in God or a spiritual power
was comparable with the general population in Denmark (65%). Furthermore, a minor proportion
reported to have experienced increased existential, spiritual, and/or religious concerns since their
diagnosis, but very few reported a need to discuss existential or spiritual issues with a health
professional, and none reported a need to discuss religious issues. Oneway ANOVA analysis
suggested that patients reporting to believe in God only, or God and a spiritual power, reported a
higher QoL than patients reporting to believe in a spiritual power only. Although positive religious
coping was prevalent, the level was lower than levels found in studies from the U.S. No association
was found between positive religious coping and QoL. Negative religious coping was not as
prevalent as positive religious coping, but hierarchical regression analysis suggested negative
religious coping to be associated with a lower QoL when controlling for socio-demographic and
religious factors.
Study 2: Coping without religion? Religious coping, quality of life and existential well-
being among lung disease patients and matched controls in a secular society
Aiming at examining whether religious coping is mobilized among people coping with severe
illness and stressful events compared to a control group (question 2), and whether religious coping
is associated with QoL and existential well-being (question 4), this survey study included 111
newly diagnosed LDPs and a group of 91 healthy Danes reporting stressful life events compared to
a healthy control group matched on age, gender, education, and region (n= 246). Measures included
single items about general religious activity, congregational support, religious coping measured by
the Brief RCOPE (Pargament, 1998), QoL (Cella et al. 1993), existential well-being (Peterman,
Fitchett, Brady, Pharm, & Cella, 2002) and among the two groups of healthy Danes, a revised
version of the List of Recent Events (LRE, Henderson, Byrne, & Duncan-Jones, 1981). Although
no differences in general religious activity was found between the three groups, positive religious
coping was more prevalent among LDPs than the control group, especially with regard to asking for
forgiveness and religious meaning-making. Hierarchical regression analyses suggested that negative
religious coping was associated with a lower QoL among LDPs only, whereas congregational
support was found to be associated with a higher QoL and existential well-being in the control
group. No associations were found between positive religious coping and QoL or existential well-
being in any of the three groups.

___________________________________________
26
Study 3: Psycho-social factors associated with religious struggles during negative life
events in a secular society
Examining the associations between religious struggle and individual characteristics (question 5),
this study included 340 Danes of whom some reported a specific negative life event. Measures
included negative religious coping (Brief RCOPE, Pargament et al, 1998), religious beliefs, general
religious activity measured as public and private religious activity, congregational support, social
support (subscale of FACIT, Cella et al. 1993), personality traits (NEO-FFI, Costa & MaCray,
1992), attachment style (RAAS, Fraley, Waller, & Brennan, 2000), and socio-demographic
information. Between 9% and 24 % of the participants reported negative religious coping to some
degree, e.g. religious struggles. Initial analyses suggested that participants rating the specific
negative events as having low impact on QoL were less likely to report religious struggles, whereas
marginally significant results suggested participants rating the event as having high negative impact
on Q L to be more likely to report religious struggles. Furthermore, participants having a lower
income, having higher levels of neuroticism, attending church, and receiving congregational support
were more likely to report religious struggles. The final logistic regression model found higher
levels of neuroticism and reporting congregational support to be associated with reporting religious
struggles.
Study 4: Studying religious and spiritual coping in a secular culture: A question of validty
To test the face validity of a U.S. developed measure on religious coping (question 6), three focus
groups of healthy Danes (n=14) and 10 individual interviews with lung cancer patients were
conducted. Participants were asked to respond to a revised version of the Brief RCOPE and a scale
called Brief SCOPE measuring whether the respondent turned to God or to a spiritual power when
coping with major negative life events or lung cancer. Participants were asked about their
understandings of the terms “God” and “spiritual power”, their understandings of the items in the
two questionnaires and the relevance of religious coping in their life situations. Exploratory
thematic analysis revealed three themes in relation to validity: The importance of language and the
“religious capital” of the participant when responding to measures about religiousness in secular
society, the influence of the situation-specific context when asked about religious coping, and the
question of universality versus context-specificity in the measurement of religious and spiritual
phenomena such as religious coping.

___________________________________________
27
Discussion
The primary aim of this present thesis was to investigate the following questions:
1. How prevalent is religious belief and religious coping among Danes facing severe lung
disease?
2. Is religious coping more prevalent among Danes facing severe lung disease and specific
negative life events than Danes coping with general, everyday challenges?
3. Do Danish LDPs report increased religious, spiritual, and/or existential concerns following
their diagnosis, and do they report a need to discuss these concerns with a health care
professional?
4. Is religious coping associated with QoL and existential well-being among Danes coping
with severe lung disease and specific negative life events?
5. Is religious struggle associated with individual psychosocial characteristics?
6. Are measures on religious coping developed in the U.S. applicable in a secular context?
In the following, results from Studies 1-3 will be discussed in light of the existing theory and
empirical studies presented in the introduction, and Study 4 will be discussed taking into account
the methodology and limitations of this present thesis.
Prevalence of religious beliefs and religious coping among Danish lung disease
patients
Study 1 suggested that belief in God or a spiritual power was widespread among LDPs, however
not exceeding the level of the general Danish population as found in previous studies from
Denmark including breast cancer patients (Jensen-Johansen et al. 2012; Pedersen, Christensen,
Jensen, & Zachariae, 2012). Studies have found women to be more religiously oriented than men
(Hvidtjørn, Hjelmborg, Skytthe, Christensen, & Hvidt,2013; Paloutzian, 1996) and this may to
some extent explain the findings from the breast cancer studies. The lung disease group included
more men (56%) than women and is more comparable with the general Danish population. Positive
religious coping was prevalent, however the level (mean=3.1) was considerably lower than the level
found among medically ill patients from the U.S. (mean=14.8) (Pargament, Koenig, Tarakeshwar,
___________________________________________
28
& Hahn, 2004). Strategies for seeking God’s love and care, religious transformation, and asking
forgiveness for one’s sins were most prevalent and reported by between 29% and 37% of the total
sample of LDPs (note: discrepancies between the amount of LDPs reporting the individual religious
coping strategies in Study 1 and Study 2 are explained by the fact that in Study 1 the percentage of
the entire patient group is reported including missing responses (N=111), whereas the valid
percentage is reported in Study 2 (N=96)). Not surprisingly, patients who considered themselves to
be a ‘believing’ or ‘spiritual’ person reported more positive religious coping than non-believers.
Still, some non-responders reported on seeking God’s love and care, which may reflect that
religious coping can be mobilized during severe illness, even among patients who do not usually
engage in religious beliefs. Overall, the level of negative religious coping (mean=1.5) was low, but
closer to the level found in the U.S. sample (mean=2.3) established by Pargament and colleagues
(2004). Demonic reappraisal was one of the least reported strategies and confirms the findings of
the European Value Survey (2008) that traditional religious beliefs, including the concept of the
devil, have decreased. Feeling abandoned by one’s religious community was the least reported
strategy (less than 2%) and may be explained by the low commitment to the Evangelical Lutheran
Church in Denmark. However, feelings of abandonment and punishing reappraisal were the most
prevalent strategies reported by between 10% and 16%, and also reported by non-believers. This
supports the finding that religious struggles may appear among atheists and agnostics as well
(Exline, Park, Smyth, & Carey, 2011), and analyses suggested that there were no differences
between believing, spiritual, or non-believing patients regarding negative religious coping
strategies.
Increased relevance of religiosity and religious coping during illness?
Question 2 aimed at testing the generalizability of a finding from U.S. studies that reminders of
mortality and human frailty, such as life threatening disease, are associated with greater
religiousness and religious coping when compared to individuals reporting no negative life events.
Study 2 found no differences in general religiousness − measured by church attendance and
prayer/meditation/scripture reading − between LDPs, individuals reporting negative events
(negative events group), and a healthy control group. Thus, stressful events did not result in
increased religious practice. Overall positive religious coping was more prevalent among LDPs
when compared to the control group reporting no negative events. No differences were found in
overall positive religious coping among LDPs and the negative events group. However the single

___________________________________________
29
coping strategies of asking forgiveness for one’s sins, which was reported by one-third of the LDPs,
and positive religious meaning-making, which was reported by 60.4% of the LDPs, were more
prevalent than among both the negative events group and the control group. It is suggested that due
to life style related factors like smoking in the etiology of a lung disease, patients diagnosed with
lung cancer report greater self-blame (Chapple, Ziebland, & McPherson, 2004). Thus, LDPs
participating in this present study may have felt a greater need to be reconciled with close relatives,
themselves, and ultimately God, by asking forgiveness for an unhealthy life style (De Guzman et al.
2010). Furthermore, receiving a life-threatening disease may increase the need for finding meaning,
and LDPs participating in this present study may have expressed a hope or a trust in a higher, divine
meaning. No differences in negative religious coping strategies were found between the three
groups. Contrary to expectations, no differences in religious coping were found between the control
group and the negative events group. This may be due to methodological limitations. In some
instances the negative events reported in the present study involved a close relative, and negative
events may thereby have been less serious than lung disease. This finding would support the theory
of terror management, namely, that reminders of one’s own personal mortality are more likely to
trigger religiosity than more mundane life events.
Religious, spiritual, and existential concerns among lung disease patients
Question 3 aimed at examining the existential, spiritual, and religious concerns and needs among
LDPs, and it was found that patients expressed relatively low levels of increased religious, spiritual,
and existential concerns following their diagnosis. Between 10.2% and 16.2% of the patients
responded positively that they had more thoughts on existential, spiritual, and religious issues. This
finding came as a surprise given the relative severity of the patients’ diagnosis and the time of
measurement. Studies among lung cancer patients and mixed groups of cancer patients have found
existential and spiritual concerns to be elevated at the time of diagnosis and at the point in time
when death is perceived as unavoidable (Ausker, la Cour, Busch, Nabe-Nielsen, & Pedersen, 2008;
Moadel et al. 1999; Murray, Kendall, Boyd, Worth, & Benton, 2004). The point of measurement
(immediately after diagnosis) was chosen because it was hypothesized that existential, religious,
and spiritual concerns would be elevated and thereby relatively prevalent. As found in Study 2, it
was suggested that almost two thirds of the LDPs sought positive religious meaning-making, which
makes the low prevalence of existential, spiritual, and religious concerns puzzling. One explanation
may be that the questions were not differentiated enough. The question about existential concerns

___________________________________________
30
was clustered and covered “thoughts about finding peace, meaning, and purpose”. Existential
concerns may also cover fears of death and dying, fear of losing control, feelings of loneliness, and
concerns about relationships (Moadel et al., 1999; Murray et al, 2004; Yalom, 1980), and more
differentiated and comprehensive measures of existential concerns could have revealed a more
nuanced picture. It may also be argued that a single question about elevated thoughts about
existential matters is too abstract, and a formulation such as “Behind all this I think God has a
meaning after all”, which was used in Study 2, could have induced more concrete reflections among
the patients. Conversely, it is suggested that secular worldviews may be associated with existential
indifference characterized as a state of low meaningfulness and yet not a crisis of meaning (Schnell,
2010). Thus, due to secularization Danes may be less concerned about existential issues in general,
and findings from the World Value Surveys (1997) give tentative support for this hypothesis, as it
was found that only 29% of Danes report to reflect much upon the meaning of life compared to 34%
in the United Kingdom, 37% in Finland, and 48% in the U.S (la Cour, 2005). The lack of
engagement in existential, spiritual, and religious issues can be positive in the sense that Danes may
be less vulnerable to crisis of meaning. However the present study only measured religious,
spiritual, and existential concerns at the time of diagnosis, and future studies may reveal if levels of
concerns increase with the severity and stage of illness.
Addressing religious, spiritual, and existential concerns
Study 1 also found that only a minor group of LDPs reported a need to discuss spiritual (0.9%) and
existential considerations (3.9%) with a health care professional and none wanted to discuss their
religious concerns. These results indicate that Danes are very private about their existential and
spiritual considerations, and that religion may be a non-topic as suggested by Zuckerman (2008) –
at least in the conversation with health care professionals. A study from the U.S. including ethnic
diverse samples suggests that between 28% and 43% of cancer patients report a need to talk to
someone about existential concerns like finding peace of mind and meaning in life (Moadel et al.
1999), and another U.S. study found that 62% of severely ill patients find it important that the
physician attends to the spiritual concerns of the patient. However, the same study also found that
62% did not think that is was the physician’s job to talk with patients about spiritual concerns
(Holmes, Rabow, & Dibble, 2006). The same attitude may be present among Danes. As suggested
in the study of Danes’ expectations towards the Danish health care system’s ability to provide
palliative care, it was found that: whereas 96% expected to receive medical care, only 16% reported
___________________________________________
31
that they expected to receive spiritual care at the end-of-life (PAVI 2013). Thus, Danes may not
perceive the discussion of religious, spiritual, and existential concerns with health care personnel as
necessary, appropriate, or something to be demanded. Rather, it may be the hospital chaplain who is
expected to take care of the patients’ spiritual and existential needs. However in everyday life some
patients are reluctant to talk to a pastor, particularly if they do not consider themselves very
religious or have another spiritual orientation than Christianity. Therefore it may be crucial that the
physicians and nurses are attentive to the potential existential, spiritual, and religious concerns of
the patient, especially as results from this thesis suggest that religious concerns and struggles can
affect the patient’s QoL.
Associations between religious coping and QoL
Negative religious coping
Question 4 aimed at investigating the possible associations between religious coping and the QoL
among LDPs and Danes reporting negative life events. Although less prevalent than positive
religious coping, Study 1 suggested that negative religious coping had a significant negative impact
on QoL among LDPs, while Study 2 found this to be true among LDPs only. Negative religious
coping among the negative events group and the healthy control group was not associated with
QoL. Several studies have suggested that the associations between religious coping and measures of
well-being and QoL are stronger when coping with major life stressors such as medical illness
(Cummings & Pargament, 2010), and frequency of pain and poorer physical functioning have been
associated with greater levels of negative religious coping among cancer patients (Cole, 2005; Hills
et al. 2005; Sherman et al. 2005). Thus, the severity of the LDPs’ situation is likely to have resulted
in the links between religious struggles and lower QoL. However, due to the cross-sectional design
it is not possible to conclude whether low QoL resulted in religious struggles or vice versa. It may
also be argued that due to less integrated and fragmentized religious beliefs the LDPs experienced
frustration instead of comfort when trying to mobilize religious resources. According to Pargament
(2007) less integrated religious world views may more easily be shattered when the individual is
exposed to turmoil and distress, and could result in religious struggles. If personal beliefs in secular
societies are actualized ad hoc as suggested by Rosen (2009), Danes may not be able to actualize
these beliefs effectively during major life stressors as the cognitive content of these beliefs is not
sufficiently explicated and developed before a crisis strikes. According to Dull & Skokan (1995)
___________________________________________
32
one of the mechanisms behind the positive link between religious coping and stress is that religious
beliefs engender a sense of optimism, control, and meaning, that effect whether a given negative
event is appraised as stressful at all. The question is whether Danes in general are poorly equipped
to profit by their beliefs when struck by major events?
Positive religious coping
The hypothesis that Danes lack fully functioning religious beliefs that are able to function as a
buffer against distress may be supported by the finding that positive religious coping was not
associated with QoL or existential well-being among LDPs or the negative events group. According
to Pargament and colleagues (2001), lack of associations between positive religious coping and
measures like QoL can be explained by the argument that: “religion has more significant effects for
those whose roles and identities are more closely tied to religion” (p. 510), and this has been
confirmed in empirical studies since (Jonas & Fischer, 2006). In a study among deeply religious
participants from the Netherlands, which is also a society characterized by secularization, positive
religious coping was found to be associated with higher levels of existential well-being and less
anxiety (Pieper, de Vries-Schot, & van Uden, 2012). Future studies among deeply religious Danes
may reveal whether religious beliefs function as a resource affecting health and well-being, or
whether secularization has impacted the ability of religious beliefs to offer comfort, meaning, and
hope even among the most religiously oriented during major life events. The non-significant links
between positive religious coping and QoL could also be explained by the religious coping
mobilization effect (Pargament, 1997). Religious coping could have been mobilized during severe
distress. However, severe distress may also have caused low QoL, and the two effects could
hypothetically have neutralized each other. Longitudinal studies are needed to clear up this
hypothesis.
Whereas no associations were found between positive religious coping and QoL, Study 1 suggested
that LDPs reporting to believe in God only, or God and a spiritual power, reported higher levels of
QoL than patients believing in a spiritual power only. Analyses suggested that patients believing in
a spiritual power only reported less public and private religious activity and low support from
fellow believers, indicating a non-traditional belief without organized social engagement in
religious communities. Study 2 suggested that congregational support was associated with higher
levels of QoL and existential well-being in the control group only. These independent findings
___________________________________________
33
suggest that Danes holding religious beliefs that involve a social engagement in a church or another
religious fellowship may more likely benefit from their religious orientations in terms of social
support, which is suggested to function as a buffer against stress (Cohen & Wills, 1985), affect QoL
among cancer patients (Allart, Soubeyran, & Cousson-Gélie, 2013), and ultimately result in
decreased mortality (la Cour, Avlund, & Schultz-Larsen, 2006; McCullough, Hoyt, Larson, Koenig,
& Thoreson, 2000).
Individual characteristics associated with religious struggles
Question 5 aimed at studying different psycho-social factors and their associations to religious
struggles in a group of participants reporting negative events, and is described in Paper 3. Results
revealed remarkably few significant associations between religious struggles and socio-
demographic factors, personality dispositions, religious factors, social factors, and situational
factors. In fact, only two variables, neuroticism and congregational support, were statistically
significant when testing the final logistic regression model, including all variables associated with
religious struggles in a series of initial analyses. A couple of explanations for this finding are
suggested.
Negative events
Initial analyses suggested that participants rating the negative event as having little or no negative
impact on QoL were less likely to report religious struggles, indicating that the gravity of negative
events is important to consider in predicting religious struggle. This has also been found in studies
from the U.S. (Exline, Park, Smyth, & Carey, 2011; Ano & Pargament, 2012) and a recent Danish
twin study suggest that traumatic events like losing a child or a spouse are more likely to elicit
negative religious coping responses than more mundane events (Hvidtjørn, Hjelmborg, Skytthe,
Christensen, & Hvidt, 2013). This may be explained by the theory of core assumptions put forward
by Janoff-Bulman (1992), that humans live with the assumption that the world is good and
meaningful. When faced with traumatic events this assumption is easily shattered and the individual
may experience great confusion and despair trying to reconstruct his assumptions about the world.
Under these circumstances, religious struggles are likely to occur. The theory of religious coping
also suggests that more severe events are likely to elicit religious coping responses. However,
nearly half of the sample in this present study did not rate the impact of events on QoL and did not
specify the nature of the event when responding to the negative subscale of Brief RCOPE. Thus, it
___________________________________________
34
was not possible to determine whether the gravity of negative events was significantly associated
with the presence of religious struggles in the final regression model, and a type 2 error is likely to
have occurred. That is when an effect is truly present but not found statistically significant due to
lack of power (Field, 2009). Future studies should be careful to register the nature of negative
events and the subjectively perceived gravity of these events. Furthermore, it may also be argued
that situational factors could potentially have mediated or moderated the associations between
individual differences and religious struggles. Hence, future studies could benefit by applying more
sophisticated models of analyses like structural equation modeling to investigate possible mediators
and moderators of religious struggles, situational factors, and individual differences.
The impact of individual differences
An explanation for the relatively few significant results may be based on the finding that
neuroticism was relatively highly correlated with negative religious coping. Personality traits as
measured by the Big Five have in general been found to be strong predictors of a wide range of
individual, interpersonal, and social outcomes (Ozer & Benet-Martinéz, 2006). Neuroticism in
particular has been found to be the strongest predictor compared to other personality dispositions on
psychological outcomes like negative affect and QoL (Steel, Smith, & Shulz, 2008). Furthermore,
personality traits have been associated with certain patterns of coping behaviour, suggesting that
personality traits to a great extent determine how the individual adjusts to different circumstances
(Costa, Somerfield, and McCray, 1996), and some even argue that “coping is personality in action
under stress” (Bolger 1990, p. 525). For example, neuroticism has been associated with the
tendency to blame oneself and others (Costa, Somerfield, and McCray, 1996), which is also
represented in the negative subscale of Brief RCOPE covering thoughts of being punished by God.
According to the general transactional coping theory it is assumed that the individual has a high
degree of freedom to choose his appraisal of a stressor and how to adjust, and little attention is paid
to the influence of individual differences possibly influencing the coping process. Pargament (1997)
implements the concept of an orienting system in his theory on religious coping, consisting of
personality dispositions, religious dispositions, and social dispositions, and thereby acknowledging
that the freedom to choose one’s coping strategies is to some degree limited by basic dispositions
and previous experiences. However, this point has not been clearly underscored in the earliest
studies on religious coping. Recent studies seem to investigate the influence of basic personality
dispositions to a higher degree and have also found neuroticism to be associated with negative

___________________________________________
35
religious coping styles (Ano & Pargament, 2012; Wood et al. 2010). Yet, longitudinal studies
including personality traits as predictors of religious struggles are lacking. It may be suggested that
continuous religious struggles highly correlated with neuroticism represent a trait-like rather than
state- like construct. If this is the case, it may also explain why religious struggles have been found
to have a devastating impact on health over time (Exline, Park, Smyth, & Carey, 2011; Pargament,
Koenig, Tarekeshwar, & Hahn, 2001), as studies have found neuroticism to be associated with
increased mortality (Shipley, Weiss, Der, Taylor, & Deary, 2007). Furthermore, if the tendency to
engage in negative religious coping is determined by neuroticism, this may also explain why
relatively few studies have found negative religious coping to be associated with spiritual growth
(Exline, 2013). Neuroticism has been found to be negatively associated with open, mature
spirituality (Saroglou, 2002), and is therefore likely to complicate the possibilities for spiritual
growth. Future studies should pay closer attention to the influence of individual differences like
personality traits in adjustment to major negative life events, and more longitudinal studies are
needed to clarify whether continuous religious struggles are more trait-like than state- like.
Furthermore, it was expected that insecure attachment would be significantly associated with
religious struggle. Studies have found insecure attachment style to be associated with negative
religious coping (Schottenbauer et al. 2006b), and especially disorganized attachment style is
suggested to be associated with viewing God as aberrant and frightening (Granqvist, Hagekull, &
Ivarsson, 2012). However, this association could not be confirmed in the final regression model,
and could be ascribed to the type of attachment measure applied. It is argued that the individual’s
relationship to God “bears striking resemblance to the child’s attachment to caregivers, and seems
to meet important criteria for defining attachment relationships” (Granqvist, 2005:36; Kirkpatrick,
1999). Therefore a measure of parental attachment style may be more appropriate to apply when
studying attachment in relation to religious coping.
Religious characteristics
No clear conclusions could be drawn regarding the association between religious beliefs, religious
activity, and religious struggles. Previous studies have found that religious struggles are also
prevalent among atheists and agnostics (Exline, Park, Smyth, & Carey, 2011), but religious beliefs
did not turn out to be significant in the final regression model, although the initial analyses
suggested secular believers to report less religious struggles. Instead, congregational support was
found to be associated with religious struggles, and it was hypothesized that individuals facing
___________________________________________
36
stressful events turned to their congregation for social support. However it may also be argued that
congregational support is an indicator of traditional religiousness, since very few Danes are engaged
in their church or congregation. Future studies should apply more precise measures of religious and
spiritual engagement as well as different religious, spiritual, and secular-existential orientations to
better predict whether religious struggles occur among the religiously oriented only. The hypothesis
that individuals living in secular societies are more prone to struggles of a religious, spiritual or
existential character during traumatic events because they lack coherent worldviews (DeMarinis,
2008) could not be confirmed since the only measure of struggle or negative coping style was
religious in nature. This means, therefore, that future studies should apply measures of existential
and spiritual struggles and this point leads on to methodological reflections on the validity of theory
and measures used in this thesis.
___________________________________________
37
Methodological considerations and limitations
In proposing models and methods for investigating how religion affects the coping process and
well-being of the individual during crisis, the theory of religious coping has contributed greatly to
the field of psychology of religion. As such, Kenneth I. Pargament deserves acknowledgement for
his seminal work giving insights as to how religion functions during crisis. In this present thesis the
theory and methods developed by Pargament (1997; 2007) and colleagues (1998; 2000) was
adopted and applied in a Danish context to test the generalizability of findings from a U.S. context
in a far more secular society. However, taking a critical stance, the coping perspective of religion
and the mainly quantitative methodology used in this research field has its limitations and will be
discussed in this section on methodological considerations.
The validity of Brief RCOPE in a secular society
As presented in Study 4, much is up for discussion regarding the applicability and validity of the
chosen religious coping measure, Brief RCOPE. Three themes in relation to the validity of
measuring religious and spiritual coping in a secular society emerged. First of all it was found that
the religious and/or spiritual language and concepts available to the individual determined to which
degree the participants were able to decode and respond adequately to the questionnaires. A
potential problem was detected among non-believers and non-theists of whom some refused to
respond because the language and underlying conception of religious beliefs were perceived to
reflect old-fashioned and traditional Christianity. Especially non-believers missed other response
options such as “Not relevant”, and in its absence some chose to mark negative religious coping on
items like “Questioned the power of God” with “Very much” to express their disbeliefs. As a
consequence this particular item was omitted from the analyses in Studies 1-3; and in Studies 1 and
2 non-believers were omitted from the regression analyses testing associations between religious
coping and QoL. However, even though the individual responding to the questionnaire held the
appropriate religious concepts and language to decode the different religious coping items,
participants with a theistic belief pinpointed that the language offered to them was too limited to
describe their experience of beliefs. The second theme highlighted the importance of the concrete
situation of the individual when measuring religious coping. Participants who were asked to recall a
negative event had great difficulty responding to the questions retrospectively if the negative was

___________________________________________
38
not severe enough or fresh in memory. Being situated in a stressful circumstance like having lung
cancer or being able to recall a recent negative life event was more likely to give rise to religious
interpretations of the event, even among participants who did not view themselves as very religious.
As such the questionnaire of Brief RCOPE did tap into ways of applying religious beliefs in coping
during major negative life events, although with varying precision. However, the third theme
questioned whether religious and spiritual phenomena can and should be measured as a universal or
a context-specific phenomenon. One of the underlying assumptions in the Brief RCOPE is that the
individual engages with a personal and active God. However, theistic beliefs (beliefs in a personal
and active God) have decreased in Denmark, and changed into more ill-defined and vague concepts
of an impersonal transcendent being (Lüchau, 2005). A new scale on spiritual coping which had
been developed for this project was found to be an important contribution – especially to
participants who did not believe in God. However, results suggested that the underlying construct
came too close to the Brief RCOPE’s conception of an active and involved spiritual being.
Furthermore the negative formulated items in the spiritual scale were not found adequate, since
participants believing in a spiritual power rather than God, described this spiritual being as solely
positive in nature. Thus, as a consequence it was determined only to include the Brief RCOPE in
the analyses conducted in study 1 to 3. Furthermore, fragments of what could be characterized as
religious and spiritual meaning-making strategies in adjusting to major negative events were found
among patients and healthy participants, however not presented in the Brief RCOPE neither the new
spiritual scale, because they did not necessary include the concept of a personal and active God.
Therefore, the results from Studies 1 to 3 are most likely to have ignored other religious, spiritual
and existential coping and meaning-making processes during adjustment that are important for
people living in secularized societies. Ganzevoort (2004) states it very clearly: “If religion is taking
new shapes (as is the case in Scandinavia), we need new concepts and measures as well” (p. 119),
and this is the natural conclusion of Study 4. Hall, Meador and Koenig (2008) elaborate on ways to
use questionnaires of religiosity in general and still ensure context-sensitivity. They recommend
using measures that enable the individual to read his own religious or spiritual view of life into the
questionnaires. Furthermore, it would be worthwhile studying religious or spiritual homogenous
groups, or, if studying mixed groups, employing ways of distinguishing groups that share
theologically similar perspectives to obtain more meaningful findings. However, this method still
requires shared understandings of faith traditions, and this may be problematic in societies like
___________________________________________
39
Scandinavia where religion is highly individualized and fragmentized. Furthermore, this approach
assumes that religious beliefs have universal, context-free characteristics that are stable and can be
measured objectively. Although very prevalent in the psychology of religion this assumption is to
opt for critique as it has far-reaching consequences for how we are able to understand religious and
spiritual phenomena. This leads on to critical reflections on the theoretical and empirical work of
religious coping.
A critical comment on the theoretical and empirical work on religious coping
In a recent paper on the history of the Western psychology of religion, Nelson (2012) describes the
development of the discipline with regard to three scientific paradigms: the hermeneutical-
phenomenological, positivistic naturalism, and religious integration, highlighting the underlying
research assumptions and preferred methods, and discussing their advantages and disadvantages. In
line with the tradition of critical psychology as represented by Wulff (1997), Nelson criticizes the
dominance of the positivistic naturalism paradigm in the psychology of religion, although it has
helped the discipline to be established as a legitimate part of mainstream psychology (Emmons &
Paloutzian, 2003; Pargament, Mahoney, Exline, Jones, & Shafranske, 2013). The positivistic
naturalism paradigm relies on the methodological assumptions that “operationalization is the key to
methodology”, and often “reliability in measurement has some degree of priority over validity”,
and “quantitative methods are assumed to be the best way of testing the operationalised
propositions”. Furthermore, the epistemology of the positivistic naturalism assumes true knowledge
to “consist of abstract propositions about universal causal laws”, and regarding ethical assumptions
“simplicity is privileged over completeness in models and explanations”. Finally, the ontology of
positivistic naturalism assumes the human person as “essentially a self-contained individual and any
cultural or relational context is secondary to this individual essence” (Nelson, 2012, pp. 693-694).
When applied in research disciplines like natural science this paradigm has its many advantages, but
in the psychology of religion some disadvantages are inevitable. With regard to the theoretical and
empirical work on religious coping a couple of disadvantages will be presented:
First of all, in religious coping theory it is assumed that crisis is likely to evoke religious responses
and therefore, Pargament (1997) states that there is no better place to study religion than in “the
___________________________________________
40
laboratory of times of crisis and coping” (p. 5). However as in all “experimental” research, it is
important to consider the ecological validity of the design (Bronfenbrenner, 1979) and the
generalizability of results. Taking a crisis coping perspective on religion, focus is directed at the
individual and is at risk of arriving at a one-dimensional “here and now” image of how religion
functions under unusual circumstances, not taking into account a range of potential dimensions
inflicted before, during, and after a crisis. Past experiences, individual differences, social relations,
and the surrounding milieu plays a great role in how religious beliefs are shaped and expressed
(Ganzevoort, 1998), and whether they become involved during crisis or not. The concept of the
orienting system as introduced by Pargament (1997) attempts at accounting for individual and
social factors in a multidimensional model of religion. However the orienting system and its
different elements are diffusely described, and according to Ganzevoort (1998) seen as “external
independent variables rather than influencing and being influenced by the coping process and
religion of the individual” (p. 262). Furthermore, even though Pargament (1997; 2007) makes an
effort to describe religiosity and spirituality as multidimensional and continuous process, the
applied quantitative measures makes it difficult to uncover this complex picture, and unfortunately
often end up by portraying religion and coping in a simplistic manner. For example in the measure
Brief RCOPE, religious and spiritual beliefs are operationalised as if they were a stable and fixed
part of the orienting system, almost like a tool that functions in more or less desirable ways when
applied in individual problem solving (Ausker, 2012). As mentioned by some of the participants in
Study 4, the questionnaire was perceived as rigid and not applicable in all situations. Furthermore,
several participants protested against either single items or the whole idea of measuring religious
belief by paper and pencil, because they could not read their own experience of religious beliefs
into the questionnaire. Thus, as a consequence of the underlying positivistic approach in the theory
and measure of religious coping, religious beliefs are easily understood as simple, static, universal,
and context-free phenomena that can be measured objectively and replicated in other settings.
However, religious and spiritual beliefs may rather be seen as changeable and situational, which
develop and unfold ad hoc as suggested by Rosen (2009) and closely connected to the language,
narratives, and characteristics of the individual and his surroundings.
According to recent sociological studies (European Value Survey, 2008) religion and spirituality do
not seem to disappear, but are changing, in secular societies, and recent studies from a Danish

___________________________________________
41
context suggest that medical illness is likely to increase religious, spiritual, and existential concerns,
beliefs and practices (Ausker, la Cour, Busch, Nabe-Nielsen, & Pedersen, 2008). However, it is
questionable to what degree the coping perspective is successful at uncovering the influence and
impact of religion during adjustment to illness and other major negative life events. Being a part of
the cognitive tradition in psychology, general coping theory relies on the assumption that coping is
a mainly conscious process in which the individual more or less rationally appraises the nature of a
given stressor and which coping resources to apply. But as found in Study 4, the nature of religion
appeared undefined and tacit to many participants, and very difficult to access at a solely cognitive
level when trying to explain how it became important during negative events in meaning-making
and adjustment. Furthermore, given the private nature of religion to individuals in secular societies,
a questionnaire may not be the appropriate way to access this sensitive topic. The majority of Danes
may not be used to expressing themselves in very manifest ways about religion and their personal
beliefs. Some of the interviewees even stated that they became suspicious as to whether the research
team had a hidden agenda to missionize through the Brief RCOPE because it was so explicit about
religious matters. As such, religious coping as operationalized in the Brief RCOPE must be
understood as a contextual phenomenon in the U.S. but not very central to individuals in secular
societies. It is likely that the Brief RCOPE may cause trouble for some individuals in the U.S. too,
as individualization and privatization of beliefs is becoming more commonplace there as well.
Finally, the theory of coping emphasizes the importance of the individual being active in problem
solving. However, in some incidents it may be de-motivating to engage in active problem solving
like suffering from chronic pain, grieving over the loss of a child, or being terminally ill, because
the problem cannot be solved! It may be impossible to gain control or there may be little meaning to
make. In these incidences the individual is likely to score high on “religious struggles”. Thus, the
coping functions of religious coping presumes the individual will succeed if he engages actively in
positive coping strategies of meaning-making, gaining control, seeking support and intimacy or
transforms spiritually. But, he copes negatively if he bargains with God, cannot make sense of his
situation or does not grow spiritually. As such, the theory of religious coping could be perceived as
normative prescribing the ‘good way’ of coping. Sometimes, however, ‘none’-coping may be the
best strategy, like accepting the lack of control or ceasing to try to make sense of a trauma are not
necessarily negative in nature. As suggested by Schottenbauer, Rodgriguez, Glass, and Arnkoff

___________________________________________
42
(2006) in situations with a high amount of control it may indeed be viewed as maladaptive to
engage in passive religious deferral (handing over the control to God), but in situations with low
control it may just be the exact right thing to do for people whose beliefs rely on God. The
dichotomized way of describing religious coping functions (good versus bad coping) may result
from an interest in evaluating the effect of coping in terms of outcome, rather than revealing the
process of religious coping. Revealing the process of religious coping, however, calls for an
increased focus on the social and cultural context in which the individual is situated. As such the
theory on religious coping must also be understood as a “child of its time” developed in the
cognitive wave of the psychology in which social and cultural influence was mainly seen as an
external influence on internal processes (Klaassen, Graham, & Young, 2009). As stated by Belzen
(2010): “Ideas never come out of the blue…different cultures lead to different theories, and so do
different periods of time within the same culture” (p. 18). Although the religious coping theory
provides a useful framework for studying religion, it is one perspective of many on how religion
may become involved during major negative life events.
Integrating a hermeneutical approach to religious coping?
There is much more to say and learn about the complex processes of religious beliefs, individual
differences, social relations, adjustment, and well-being than can be revealed by taking a positivistic
perspective applying mainly quantitative methods. As stated by Gorsuch, measurement has been
both a “boon and a bane” to the psychology of religion, because it has helped the discipline to
become more legitimate in mainstream psychology, but at the expense of a true explanation of
religion (Gorsuch, 1984; Hood, 1999). Historically the psychology of religion has been separated
into functional and substantive approaches to religion (Wulff, 1997; Nelson, 2012). That is,
researchers have distinguished between “what religion is” (the substance) and “what religion does”
(the function) resulting in very different approaches and methodologies applied. The substantive
approach has mainly relied on qualitative, hermeneutical methodology, whereas the functional
approach has mainly applied quantitative methodology (Hood, 1999). However, this distinction is
counter-productive as it overlooks potential causal explanations of how and why religion becomes
involved and potentially helpful or harmful under certain circumstances to different individuals. It
seems as fairly reasonable to assume that the substance of religious and spiritual beliefs is crucial
for the function in terms of adjustment and well-being, and that the substance of religious and

___________________________________________
43
spiritual beliefs is affected by the individual’s dispositions, social relations, and surrounding
narratives and language available in the culture. Future empirical and theoretical work could benefit
from taking a hermeneutical-phenomenological approach applying narrative, qualitative methods in
investigating religion and coping as multifaceted processes unfolding in the concrete life story of
the individual and his surroundings (Ganzevoort, 1998; Nelson, 2012). McGuire (2008) proposes to
examine and understand religion as much more than pure cognitive content, but the daily practices
of body, mind, emotion, and spirit, a so-called “lived religion”, and calls for anthropological
methodology to come closer to the content and importance of religious experience. Others have
called for a cultural psychology of religion aiming at highlighting the cultural embedment of
religion even more and moving away from an individual focus (Belzen, 2010; Hood, 2010).
Contextual action theory has also been proposed as an integrative framework for studying religion
and spirituality taking into account human emotional, cognitive, behavioral, and relational processes
and drawing on hermeneutics, phenomenology, and narrative studies (Klaassen, Graham, & Young,
2009). Although this kind of research has limited generalizability in a positivistic manner, the
psychology of religion may generate more genuine and useful theories and empirical work for the
involved individuals, and may also benefit from integrating perspectives from theology, philosophy
and the sociology of religion. However, acknowledging the favor of quantitative methodology in
the psychology of religion, future studies should aim at developing context-specific measures
reflecting the language, narratives, and concepts available to the population one wants to study.
This could be done by applying qualitative methodology to generate concepts and categories of
religious and spiritual beliefs and functions in a particular setting. Moreover, the most important
point in research is to acknowledge that, what can be said about a specific phenomenon is limited to
the perspective and methodology used, and that a specific operationalization of a given phenomena
is just one aspect of the complexity of the real world that may be inflicted by the researcher’s pre-
assumptions and biases.
Generalizabilty
As such, the scope of the results presented in this thesis is admittedly also limited due to the
methodology and instruments applied. With regard to the “knowing” dimension, the Brief RCOPE
does not totally cover the often tacit content of religious orientations among Danes and needs to be
extended or reformulated to cover new forms of religious and spiritual beliefs. In relation to “doing”
___________________________________________
44
and “being”, the measure of Brief RCOPE is likely to draw a skewed picture of how religiosity is
involved in coping when asking people to reflect on a rather complex issue on command, and
because it does not take into account the process of religious coping. Although longitudinal studies
may come closer to revealing the process of religious coping, other methodologies could be applied
too. Furthermore, the coping perspective operationalised through questionnaires is considered too
narrow a focus to take if one wants to explore how and why religion becomes involved during
major life events, because these processes are often unconscious and not directly accessible to the
individual. Moreover, due to the socio-demographic characteristics of the samples included in this
present thesis the generalizability of the results is limited to elderly, relative low-SES individuals
living in secularized societies. Since this present thesis only included lung disease patients results
may not apply to other patient groups. The relative low response rate of especially the lung disease
sample calls for caution when interpreting the results, as selection bias may have occurred; it is
likely that mainly lung patients in better physical condition did participate. The focus on religious
issues is likely to have caused some patients and control participants to decline from participating,
and the samples may have an overrepresentation of religiously oriented Danes. Finally, due to the
cross-sectional design it was not possible to examine any causal associations between religious
coping, individual characteristics, negative events, or QoL.
___________________________________________
45
Conclusion: A soda-analogy?
This summer (2013) a soda- company is running a campaign, selling their product with different,
individual names tagged on the front of each soda. It is therefore possible to go into any given shop
and find a product directed personally to you almost anywhere in the world. Funny idea – and
certainly successful in obtaining what the company wants – to sell more of their products. In
quantitative research we as researchers are successful if we gain a high respondent rate and are able
establish evidence to support (or reject) our hypotheses. To obtain that goal we do our best to direct
the form of our product to our target group. In studying religion and health we should, as suggested
by Hall, Koenig, and Meador (2008), make scales on religion in such a way that the individual is
able to read his own religious beliefs into the questionnaire (the personal label). As with the soda,
we assume the product to contain the same key features (sugar, carbon dioxide, water and some
kind of flavor additive) making it comparable all over the world. Likewise with religious coping
scales, we expect them to contain some kind of relationship to the sacred. Furthermore, we assume
that certain circumstances, for example hot weather or social gatherings make people more likely to
buy a soda. In the analogy with religious coping, we assume that highly stressful, challenging,
and/or life- threatening situations make people turn to religion as a coping resource. Finally, we
assume that the product is able to serve different purposes under different circumstances – the soda
is able to quench thirst, add “a little something” to the social gathering, make the individual look
prestigious when choosing this particular brand etc. In the analogy with religious coping, we
assume religious coping to serve the functions of gaining control, finding meaning, feeling intimacy
and support, and obtaining spiritual transcendence during negative events. However, we are only
successful in selling our product if we address it towards individuals living in societies where
buying a soda is legitimate, makes sense, and fulfills the needs of the individual. But what if the
society does not approve of this given product? Or what if the consumer does not prefer exactly this
product – what if he buys another product? Or he would like to mix it himself? Maybe some of the
key features are the same – but the relationship between them differs. What can we then say about
the content? Or why he prefers this taste? Or what function it serves? And what about the
experience? Or the effect of the product? If the “homemade” version contains less sugar maybe the
costumer gains less weight, but due to the amount of caffeine it may have some other side effects?

___________________________________________
46
Are we able to detect these differences in experience or effect if we assume the form, the content,
and the function of our product to be the same all over the world?
In this present study, a “product” (Brief RCOPE), which was developed in the U.S. was applied
with a couple of changes to direct it more personally to the target group with the assumption that
people in need would “consume” or respond positively to the form (the questionnaire) reflecting the
given content (religion as coping strategy). Results suggested that some consumed the product and
that some effects were detectable. Positive religious coping, although not as prevalent as found in
U.S studies, was more prevalent than negative religious coping. Furthermore, LDPs were found to
report more positive religious coping than participants dealing with less severe negative life events,
partially supporting the hypothesis that people in need may turn to religion. No effects were found
between positive religious coping and QoL, whereas negative religious coping was found to have a
negative impact on QoL among LDPs only. Moreover, it was detected that reporting negative
religious coping was associated with higher levels of neuroticism and congregational support.
However, a qualitative study suggested that the form and content of the Brief RCOPE was not a
perfect match to the target group. Some chose not to respond because it was not perceived as
directed to them, others tried to communicate their non-belief or dissatisfaction with the
questionnaire by responding in an inadequate way. A few were able to answer adequately, while
others were unable to explain why they had responded as they had because their beliefs were not
very explicit. Ways of engaging in religious and spiritual beliefs that were not covered by the Brief
RCOPE were found, suggesting that the phenomenon of religious coping as found in the United
States is context specific and not comparable with more secular societies when applying the Brief
RCOPE. Furthermore, it is questionable whether the theory of coping operationalized through
quantitative methods is the appropriate way of investigating how beliefs become important and
potentially protective or harmful to the individual facing major life challenges in general – and in
secular societies in particular. The theory of coping assumes a rather conscious way of relating to
beliefs and adjustment during crisis. However, as suggested by Rosen (2009) and found in Study 4,
in a society dominated by privatization and individualization of experience, personal beliefs are
often tacit and applied and developed ad hoc. Therefore it may be difficult to measure beliefs and
detect true effects at a solely cognitive level by questionnaires. Furthermore, few individuals in
secular societies may think they involve religion actively in coping, as is the underlying assumption
of Brief RCOPE. Religion could be approached as “lived” as suggested by McGuire (2008).

___________________________________________
47
Therefore, narrative methodology is relevant as a way to detect patterns of functions and
dysfunctions in meaning-making and ascertain how it becomes important to the individual in terms
of adjustment, and could potentially give rise to new context-specific measures of religion and
spirituality in secular society.
___________________________________________
48
Perspectives and future studies
Clinical implications
Although many things are up for discussion regarding methods and measures chosen in this present
thesis, it was found that some forms of religious coping were negatively associated with QoL
among medically ill LDPs. This finding is in line with a range of international studies, and must be
taken seriously, because something is at stake for patients experiencing religious struggles, and
most likely also struggles of a spiritual and existential kind. The results are relevant to health care
personnel, especially nurses, who are obligated to provide spiritual care among patients. An
ongoing but quiet debate about spiritual care among Danish nurses indicates that many nurses
express uncertainty about how to provide this, although it is recognized as an important topic
(www.aandeligomsorg.dk). International as well as Danish studies suggest that this may be due to
lack of time and skills, lack of vocabulary, personal issues surrounding death and dying, as well as a
misunderstood consideration of the patient’s privacy (Abbas & Dein, 2011; Christensen & Turner,
2008; Dam, Johansen, Jørgensen, & Winck, 2006). However, international studies suggest that it is
important to approach the individual’s relation to spirituality or religion in order to be in a better
position to prevent or intervene on potential spiritual struggles. A growing body of intervention
studies is emerging (see Pargament, Mahoney, & Shafranske, 2013 for a comprehensible overview
of the field). The relevance of examining the question: “For whom do religious and spiritual beliefs
become a potential burden?” should be taken seriously by Scandinavian health care systems too,
and methods for discovering the “red flags” of potential spiritual distress are needed. However,
results from this present thesis should be interpreted as preliminary regarding the ability for
deducing clinical implications. More research on religious, spiritual, and existential needs and
resources among different medical samples are needed from secular societies, and it is too early to
suggest specific screening tools for religious or spiritual struggles or applying spirituality-integrated
interventions in Denmark. The question about who is best suited to approach the religious, spiritual,
and/or existential needs remains unanswered. The bio-medical model of health care seems to
dominate the Danish health care system as very few Danes expect to receive spiritual care during
end-of-life care (PAVI, 2013). As suggested in Study 1, only a minority called for the opportunity
to talk to a health care professional about existential and spiritual concerns. This finding is
supported by a study conducted by Ausker, la Cour, Busch, Nabe-Nielsen, & Pedersen (2008)
among 480 hospitalized Danes, where only 1% of the patients indicated that they would like to talk

___________________________________________
49
to a doctor and 11% would like to talk to a nurse about existential or religious concerns. However,
according to the study conducted by PAVI (2013) younger Danes are more likely to expect the
Danish health care system to address spiritual needs, and in the future patients may place higher
demands on a holistic approach to the individual. Ausker, la Cour, Busch, Nabe-Nielsen, &
Pedersen (2008) also found that younger patients (<36 years) were more likely to have had a
conversation about existential or religious topics after their hospitalization (34%) compared to 13%
of the oldest (>56 years) patients. This may of course reflect that more existential issues are at stake
for younger patients. However, the study also found younger patients to report more religious
activity and religious/spiritual beliefs than older patients, indicating that future generations may be
in need of increased focus on existential health. Furthermore, a qualitative study conducted among
12 terminally ill patients receiving end-of-life care at hospice suggested that especially patients
having difficulties expressing themselves about religious or spiritual matters experienced a need for
the nurse to attend to spiritual issues to come to terms with unresolved conflicts of personal beliefs
(Nielsen, 2005). Courses directed at nurses and doctors on communication skills and touching
difficult existential issues are becoming more commonplace in Denmark and represent one way to
enable health personnel to better detect possible religious, spiritual, and existential needs and
struggles. However, there may be a particular need to work with the reluctance to touch spiritual or
religious issues among nurses and doctors. Often local or hospital chaplains, rabbis or imams are
referred to if the question at stake exceeds the competence and resources of the health care
personnel and, as such, represents an important resource in the health care system. Given the
changing religious and spiritual beliefs among people in secular societies, however, it is important
to have other competences to refer to, like a conversational partner with a philosophic or secular
humanistic background, a spiritual coach, or psychologists to accommodate individuals with secular
or spiritual views of life.
Research implications
The findings of this thesis touches the surface of how religious and spiritual orientations become
involved in and affect adjustment and well-being among Danes facing lung disease and other major
life events. However, much more waits to be explored! Hopefully this thesis it gives rise to other
studies aiming at revealing more of the complex picture of how religious, spiritual, and secular-
existential worldviews are involved in and impact the lives of individuals facing major and minor

___________________________________________
50
life events. Future studies should include younger participants to investigate whether religious,
spiritual, and existential struggles are becoming more commonplace, affecting health and well-
being in line with the hypothesis that due to increased secularization coherent worldviews are
lacking and may affect the ability to adjust adequately to major life events (DeMarinis, 2008; la
Cour, 2008). Furthermore, studies should develop and apply measures that are sensitive to the
specific worldview of the individual and be careful not to enforce certain ideas and concepts of
religious, spiritual, and secular existential orientation on the research participant (la Cour & Hvidt,
2010). Qualitative methods or mixed methods design are called for, since they may reveal more in-
depth information about the complicated processes of meaning-making, adjustment, and well-being
during major negative events and prevent simplistic conclusions on the associations between life
orientation and health. Furthermore, studies should take into account the impact of individual
differences in the adjustment to major negative life events, and apply more sophisticated statistical
analyses to test possible moderators and mediators of religious and spiritual coping. Finally, studies
in Denmark should investigate different medical samples, at different stages of illness progression,
and follow them over time to generate more genuine results of the impact of religious, spiritual, and
existential concerns among people living in secular societies during illness.
___________________________________________
51
References
Abbas, S.Q. & Dein, S. (2011). The difficulties assessing spiritual distress in palliative care
patients: a qualitative study. Mental Health, Religion, & Culture, 14 (4): 341-352.
Allart, P., Soubeyran, P., & Cousson-Gélie, F. (2013). Are psychosocial factors associated with
quality of life in patients with haematological cancer? A critical review of the literature.
Psychooncology, 22(2): 241-249. doi: 10.1002/pon.3026.
Andersen, P.B., & Lüchau, P. (2008). Individualisering og aftraditionalisering af danskernes
religiøse værdier. (English: ”Individualization and detraditionalization of Danes’ religious
values”) I: Gundelach, P (Ed.). Små og store forandringer. Danskernes værdier siden 1981.
Hans Reitzels Forlag.
Ano, G.G., & Pargament, K.I. (2012). Predictors of spiritual struggles: an exploratory study. Mental
Health, Religion, and Culture. Advance online publication.
Ano, G. G., & Vasconcelles, E. B. (2005). Religious coping and psychological adjustment to stress:
A meta-analysis. Journal of Clinical Psychology, 61(4), 461-480. doi:10.1002/jclp.20049.
Ausker, N.H., la Cour, P., Busch, C., Nabe-Nielsen, H., & Pedersen, L.M. (2008). Danske patienter
intensiverer eksistentielle tanker og religiøst liv. (English: ”Danish patients’ intensity
existential thoughts and religious life”). Ugeskrift for Læger, 170 (21): 1828-1833.
Ausker, N. H. (2012). Time for change? Negotiations of religious continuity, change, and
comsumption among cancer patients in Denmark. (Original titel in Danish: ”Tid til
forandring? Forhandlinger af religiøs kontinuitet, forandring, og forbrug blandt
kræftpatienter i Danmark”). Ph.D. thesis, Department of Cross-cultural and Regional
Studies, Copenhagen University.
Beck, A.T., Steer, R.A., & Brown, G.B. (1996). Manual for Beck Depression Inventory - II. San
Antonio, TX Psychological Corporation.
Bekke-Hansen, S., Pedersen, C.G., Thygesen, K., Christensen, S., Waelde, L.C., & Zachariae, R.
(2013). The role of religious faith, spirituality and existential considerations among heart

___________________________________________
52
patients in a secular society: Relation to depressive symptoms 6 months post acute coronary
syndrome. Journal of Health Psychology. E-pub ahead of print. doi:
10.1177/1359105313479625.
Bellah, R.N., Madsen, R., Sullivan, W.M., Swidler, A., & Tipton, S.M. (1985). Habit of heart:
Individualism and commitment in American life. New York, NY: Harper & Row.
Bell-Meisenhelder, J. & Marcum, J.P. (2004). Responses of clergy to 9/11: Posttraumatic stress,
coping, and religious outcomes. Journal for the Scientific Study of Religion, 43: 545–554.
doi: 10.1111/j.1468-5906.2004.00255.x.
Belzen, J.A. (2010). Towards cultural psychology of religion: principles, approaches and
applications. New York, NY, US: Springer Science + Business Media. doi: 10.1007/978-
90-481-3491-5.
Bolger, N. (1990). Coping as a personality process: A prospective Study. Journal of Personality
and Social Psychology, 59 (3): 525-537.
Bronfenbrenner, U. (1979): Toward an experimental ecology of human development. American
Psychologist, 32 (7): 513-531.
Brotherson, E.J., Evon, D.M., Sedway, J.A., & Egan, T. (2004). Coping with a child’s death:
Spiritual issues and therapeutic implications. Journal of Family Psychotherapy, 13: 53-86.
doi: 10.1300/J085v13n01_04.
Carver, C.S. (1997). You want to measure coping but your protocol’s too long: Consider the Brief
COPE. International Journal of Behavioral Medicine, 4: 92-100. doi:
10.1207/s15327558ijbm0401_6.
Cella, D.F., Tulsky, D.S., Gray, G., Sarafian, B., Linn, E., Bonomi, A., Silberman, M., Yellen, S.B.,
Winicour, P., Brannon, J. et al. (1993). The functional assessment of cancer therapy scale:
Development and validation of the general measure. Journal of Clinical Oncology, 11 (3),
570-579.
Charlson, M.E., Pompei, P., Ales, K.L., & MacKenzie, C.R. (1987). A new method of classifying
prognostic comorbidity in longitudinal studies: Development and validation. Journal of
Chronic Diseases, 40 (5), 373-383.

___________________________________________
53
Chapple, A., Ziebland, S., & McPherson, A. (2004). Stigma, shame, and blame experienced by
patients with lung cancer: Qualitative study. British Medical Journal, 328 (7454):1470
Christensen, K.H. & Turner, S. (2008). Spiritual care perspectives of Danish registered nurses.
Journal of Holistic Nursing, 26(7): 7-14.
Cohen, S. & Williamson, G.M. (1988). Perceived stress in a probability sample of the United
States. In: S. Spaacan & S. Oskamp (Eds). The Social Psychology of Health. Sage
Publications Inc, California.
Cohen, S. & Wills, T.A. (1985). Stress, social support, and the buffering hypothesis. Psychological
Bulletin, 98 (2): 310-357. doi: http://dx.doi.org.ez.statsbiblioteket.dk:2048/10.1037/0033-
2909.98.2.310.
Cole, B.S. (2005). Spiritually-focused psychotherapy for people diagnosed with cancer: A pilot
study outcome. Mental Health, Religion, and Culture, 8 (3): 217-226. doi:
10.1080/13694670500138916.
Costa, P.T., & McCrae, R.R. (1992). Normal personality assessment in clinical practice: The NEO
Personality Inventory. Psychologival Assessment, 4 (1): 5-13.
Costa, P. T., Somerfield, M. R., McCrae, R. R. (1996). Personality and Coping: A
Reconceptualization. In: M. Zeidner & N. Endler (Ed.). Handbook of Coping: Theory,
Research, Applications. John Wiley & Sons, Inc: New York.
Crowne, D, & Marlowe, D. (1964). The Approval Motive Studies in Evaluative Dependence. John
Wiley & Sons: New York.
Cummings, J.P., & Pargament, K.I. (2010). Medicine for the spirit: Religious coping in individuals
with medical conditions. Religions, 1, 28–53. http://www.mdpi.com/2077-1444/1/1/28.
Dam, E., Johansen, L., Jørgensen, B.H., & Winck, O. (2006). Åndelig omsorg bør have mere plads i
sygeplejen. (English: ”Spiritual care ought to have more space in nursing”).
Sygeplejersken, 106 (5): 54-57.
De Guzman, A.B., Sindac, L.A.G., Sioson, J.J.T., Sison, K.J.B., Socia, J.K,M., Solidum,
R.F., . . . & Suaberon, L.C.D.C. (2010). Looking through a window: The guilt and remorse
space of a lung cancer patient. Journal of Cancer Education, 25, 663–665. doi:10.1007/
s13187-010-0127-5.

___________________________________________
54
DeMarinis, V. (2008). The Impact of Postmodernization on Existential Health in Sweden:
Psychology of Religion’s Function in Existential Public Health Analysis. Archieve for the
Psychology of Religion, 30: 57-74.
Dull, V.T. & Skokan, L.A. (1995). A cognitive model of religion’s influence on health. Journal of
Social Issues, 51:49-64. doi: 10.1111/j.1540-4560.1995.tb01323.x.
Dyer, A.R. (2011). The need for a new “New Medical Model”: A bio-psychosocial-spiritual model.
Southern Medical Journal, 14 (4): 297-298. doi: 10.1097/SMJ.0b013e318208767b.
Emmons, R.A. & Paloutzian, R. (2003). The Psychology of Religion. Annual Review of
Psychology; 54:377-402.
Exline, J. (2013). Religious and spiritual struggles. In: K.I. Pargament, Exline, J., & Jones, J.W.
(Eds). APA Handbook of Psychology, Religion, and Spirituality. Volume 1. Context,
Theory, and Research. American Psychological Association. Washington D.C.
Exline, J.J., Park, C.L., Smyth, J.M., & Carey, M.P. (2011). Anger toward God: Social-cognitive
predictors, prevalence, and links with adjustment to bereavement and cancer. Journal of
Personality and Social Psychology, 100(1), 129-148. doi:10.1037/a0021716.
Field, A. (2009). Discovering statistics using SPSS, 3rd
ediction. Sage Publications Ltd.
Fitchett, G., Murphy, P.E., Kim, J., Gibbons, J., Cameron, J.R., & Davis, J.A. (2004). Religious
struggle: Prevalence, correlates and mental health risks in diabetic, congestive heart failure,
and oncology patients. International Journal of Psychiatry in Medicine, 34, (2), 179-196.
Fraley, R.C., Waller, N.G., & Brennan, K.A (2000). An item response theory analysis of self-report
measures of adult attachment. Journal of Personality and Social Psychology, 78(2):350-
365.
Gall, T.L. & Guirguis-Younger, M. (2013). Religious and spiritual coping: Current theory and
research. In: Pargament, K.I. (Ed.): APA Handbook of Psychology, Religion, and
Spirituality, Volume 1. Context, Theory, and Research. American Psychological
Association, Washington, D.C. doi: 10.1037/14045-000.
Ganzevoort, R.R. (1998). Religious coping reconsidered. Part One: an integrated approach. Journal
of Psychology and Theology, 26 (3): 260-275.

___________________________________________
55
Ganzevoort, R.R. (2004). Receptivity and the nature of religion. Journal of Empirical Theology, 17
(1): 115-125.
Gergen, K.J. (1991). The saturated self: Dilemmas of identity in contemporary life. New York:
Basic Books.
Gorsuch, R.L. (1984). The bone and bane of investigating religion. American Psychologist, 39: 228
– 236.
Granqvist, P. (2005). Building a bridge between attachment and religious coping: tests of
moderators and mediators. Mental Health, Religion, and Culture, 8 (1): 35-47. doi:
10.1080/13674670410001666598.
Granqvist, P., Hagekull, B., & Ivarsson, T. (2012). Disorganized attachment promotes mystical
experiences via a propensity for alterations in consciousness (absorbtion). The International
Journal for the Psychology of Religion, 22: 130-197. doi: 10.1080/10508619.2012.670012
Hall, D.E., Koenig, H.G., & Meador, K.G. (2008). Measuring Religiousness in Health Research:
Review and Critique. Journal of Religion and Health, 47:134-163. doi: 10.1007/s10943-
008-9165-2.
Henderson, S., Byrne, D.G, & Duncan-Jones, P. (1981). Neurosis and the social environment.
Sydney: Academic Press.
Herbert, R., Bozena, Z., Schulz, R., & Scheier, M. (2009). Positive and negative religious coping
and well-being in women with breast cancer. Journal of Palliative Medicine, 12 (6): 537-
545. doi: 10.1089=jpm.2008.0250.
Hills, J., Paice, A., Cameron, J.R., & Shott, S. (2005). Spirituality and distress in palliative care
consultation. Journal of Palliative Medicine, 8 (4), 782-788.
Holmes, S.M., Rabow, M.W., & Dibble, S.L. (2006). Screening the soul: Communication regarding
spiritual concerns among primary care physicians and seriously ill patients approaching the
end of life. American Journal of Hospice & Palliative Care, 23: 25-33. doi:
10.1177/104990910602300105.
Hoge, D.R. (1972). A validated instrinsic religious motivation scale. Journal of the Scientific Study
of Religion, 11: 369-376.
Hood, R.W. (1999). American Psychology of Religion and the Journal of the Scientific Study on
Religion. Journal for the Scientific Study on Religion, 39 (4): 531-543.
___________________________________________
56
Hood, R. (2010). “Towards cultural psychology of religion: principles, approaches, and
applications”: an appreciative response to Belzen's invitation. Mental Health, Religion &
Culture, 13 (4): 397-406.
Hvidtjørn, D., Hjelmborg, J., Skytthe, A., Christensen, K., & Hvidt, N.C. (2013). Religiousness and
Religious Coping in a Secular Society: The Gender Perspective. Journal of Religion and
Health, doi: 10.1007/s10943-013-9724-z.
Iversen, H.R. (2006). Secular Religion and Religious Secularism: A profile of the religious
development in Denmark since 1968. Nordic Journal of Religion and Society, 19 (2), pp.
75-92.
Janoff-Bulman, R. (1992). Shattered assumptions: Towards a new psychology of trauma. New
York, NY: Free Press.
Jensen-Johansen, M.B., Christensen, S., Valdimarsdottir, H., Zakowsky, S., Jensen, A.B., Bovbjerg,
D.H., & Zachariae, R. (2012). Effects of an expressive writing intervention on cancer-
related distress in Danish breast cancer survivors – results from a nationwide randomized
clinical trial. Psychooncology. E-pub ahead of print. doi: 10.1002/pon.3193.
Jonas, E., & Fischer, P. (2006). Terror management and religion: Evidence that intrinsic
religiousness mitigates worldview defense following mortality salience. Journal of
Personality and Social Psychology, 91 (3), 553–567. doi:10.1037/0022-3514.91.3.553.
Kahn, Z.H. & Watson, P.J. (2006). Construction of the Pakistani religious coping practices scale:
Correlations with religious coping, religious orientation, and reactions to stress among
Muslim university students. The International Journal for the Psychology of Religion, 16:
101-112. doi: 10.1207/s15327582ijpr1602_2.
Klaassen, D.W., Graham, M.D., Young, R.A. (2009). Spiritual/religious coping as intentional
activity: An action theoretical perspective. Archieve for the Psychology of Religion, 31: 3-
33. doi: 10.1163/157361209X371456
Kirkpatrick, L. A. (1999). Attachment and religious representations and behavior. In Handbook of
attachment theory and research, J. Cassidy, & P. R. Shaver (Eds), pp. 803–822. NY:
Guilford.
___________________________________________
57
Koenig, H.G., King, D., and Carson, V.B. (Eds.) (2012). Handbook of Religion and Health. Oxford
University Press, New York.
La Cour, P. (2005). Danskernes Gud i krise. (English: ”Danes’ God in crisis”). In M.T. Højsgaard
& H.R. Iversen (Eds.), Gudstro i Danmark (pp. 59 – 82). København: Anis.
La Cour, P., Avlund, K., & Schultz-Larsen, K. (2006). Religion and survival in a secular region. A
twenty year follow-up of 734 Danish adults born in 1914. Social Science and Medicine, 62:
157-164. doi: 10.1016/j.socscimed.2005.05.029.
La Cour, P. (2008). Existential and religious issues when admitted to hospital in a secular society:
Patterns of change. Mental Health, Religion and Culture, 11 (8): 769-782. doi:
10.1080/13674670802024107.
La Cour, P., & Hvidt, N.C. (2010). Research on meaning-making and health in secular society:
Secular, spiritual, and religious existential orientations. Social Science and Medicine, 71
(7): 1292-99. doi: 10.1016/j.socscimed.2010.06.024
la Cour, P. Ausker, N.H., Hvidt, N.C. (2012). Six understandings of the word 'spirituality' in a
secular country. Archiv für Religionspsychologie / Archive for the Psychology of Religions.
34 (1): 63-81.
Lavera, M.E. & O’Hea, E.L. (2010). Religious/spiritual coping and adjustment in individuals with
cancer: Unanswered questions, important trends, and future directions. Mental Health,
Religion, and Culture, 13(1): 55-65. doi: 10.1080/13674670903131850
Lazarus, R.S. & Folkman, S. (1984). Stress, appraisal, and coping. New York: Springer
Lüchau, P. (2005). Danskernes gudstro siden 1940’erne. (English: ”The godbelief of Danes since
1940es”). In M.T. Højsgaard & H.R. Iversen (Eds.), Gudstro i Danmark (pp. 31-58).
København: Anis.
McCullough, M.E., Hoyt, W.T., Larson, D.B., Koenig, H.G., Thoresen, C. (2000). Religious
involvement and mortality: A meta-analytic review. Health Psychology, 19 (3): 211-222.
McGuire, M.B. (2008). Lived Religion. Faith and Practice in Everyday Life. Oxford University
Press Inc.
Merluzzi, T.V., Nairn, R.C., Hegde, K., Martinez, Sanchez, M.A., & Dunn, L. (2001). Self-efficacy
for coping with cancer: Revision of the cancer behavior inventory (version 2.0). Psycho-
Oncology, 10(3): 206-17.
___________________________________________
58
Moadel, A., Morgan, C., Fatone, A., Grennan, J., Carter, J., Laruffa, G., Skummy, A., & Dutcher, J.
(1999). Seeking meaning and hope: Self-reported spiritual and existential needs among an
ethnically-diverse cancer patient population. Psycho-oncology, 8, 378-385.
Murray, S.A., Kendal, M., Worth, A., & Benton, T.F. (2004). Exploring the spiritual needs of
people dying from lung cancer or heart failure: A prospective qualitative interview study of
patients and their carers. Palliative Medicine, 18, 39-45.
Nelson, J.M. (2012). A history of psychology of religion in the West: Implications for theory and
method. Pastoral Psychology, 61: 685-710. doi: 10.1007/s11089-011-0407-y.
Nielsen, R. (2005). At være sig selv – at blive sig selv. Den åndelige dimension hos døende
mennesker. (English: “Being one self – becoming one self. The spiritual dimension among
dying people”). Unitas Forlag
Ozer, D.J. & Benet-Martinéz, V. (2006). Personality and the prediction of consequential outcomes.
Annual Review of Psychology, 57: 401-421. doi:10.1146/annurev.psych.57.102904.190127
Paloutzian, R. (1996). Invitation to the Psychology of Religion. Needham Heights, MA: Allyn &
Bacon, 2nd
ed.
Pargament, K.I. (1997). The psychology of religion and coping. Theory, research, practice. New
York: Guildford.
Pargament, K. I. (2007). Spiritually integrated psychotherapy. Understanding and addressing the
sacred. New York: Guildford.
Pargament, K.I., Desai, K.M., & McConnell, K.M. (2006). Spirituality: A pathway to post-
traumatic growth or decline? In: L.G. Calhoun & R.G. Tedeschi (Eds.), Handbook of post-
traumatic growth: Research and practice: 121-37. Mahwah, N.J.: Erlbaum.
Pargament, K.I., Mahoney, A., Exline, J.J., Jones, J.W., & Shafranske, E.P. (2013). Envisioning an
integrative paradigm for the psychology of religion and spirituality. In: Pargament, K.I.,
Exline, J.J., & Jones, J.W. (Ed). APA Handbook of Psychology, Religion, and Spirituality,
Volume 1. Context, Theory, and Research: 3- 19. American Psychological Association,
Washington D.C. doi: 10.1037/14045-000.
Pargament, K.I., Koenig, H.G., & Perez, L.M. (2000). The many methods of religious coping:
Development and initial validation of the RCOPE. Journal of Clinical Psychology, 56
(4):519-43.
___________________________________________
59
Pargament, K.I., Koenig, H.G., Tarakeswar, N., & Hahn, J. (2001). Religious struggle as a predictor
of mortality among medically ill elderly patients: A two year longitudinal study. Archives of
Internal Medicine, 161, 1881-85. doi:10-1001/pubs.Arch Intern Med.-ISSN-0003-9926-161-
15-ioi00736.
Pargament, K.I., Koenig, H.G., Tarakeswar, N., & Hahn, J. (2004). Religious coping methods as
predictors psychological, physical, and spiritual outcomes among medically ill elderly
patients: A 2 year longitudinal study. Journal of Health Psychology, 9, 713-730. doi:
10.1177/1359105304045366.
Pargament, K.I., Mahoney, A., & Shafranske, E.P. (Ed) (2013). APA Handbook of Psychology,
Religion, and Spirituality, Volume 2. An Applied Psychology of Religion and Spirituality.
American Psychological Association, Washington D.C. doi: 10.1017/14046-000.
Pargament, K.I., Smith, B.W., Koenig, H.G., & Perez, L. (1998). Patterns of positive and negative
religious coping with major life stressors. Journal of the Scientific Study of Religion, 37 (4),
710-724.
Pargament, K.I., Zinnbauer, B.J., Scott, A.B., Butter, E.M., Zerowin, J., & Stanic, P. (2003). Red
flags and religious coping: Identifying some religious warning signs among people in crisis.
Journal of Clinical Psychology, 59 (12): 1335-1348.
Park, C. (2005). Religion and meaning. In R. F. Paloutzian & C. L. Park (Eds.), Handbook of the
Psychology of Religion and Spirituality: 295-314. New York: Guilford Press.
Parker, D.A., Taylor, G.J., & Bagby, R.M. (2003). The 20-item Toronto Alexithymia Scale III.
Reliability and factorial validity in a community population. Journal of Psychosomatic
Research, 55 (3): 269-275. doi: 10.1016/S0022-3999(02)00578-0.
PAVI (Palliative Research Center, 2013). Danskerne om livet med sygdom og død. (English: Danes
about the life with illness and death”). www.pavi.dk.
Pedersen, C.G., Christensen, S., Jensen, A.B., & Zachariae, R. (2012). In God and CAM we trust.
Religious faith and alternative medicine (CAM) in a nationwide cohort of women treated
for early breast cancer. Journal of Religion and Health. E-pub ahead of print. doi:
10.1007/s10943-012-9569-x.
___________________________________________
60
Peterman, A.H., Fitchett, G., Brady, M.J., Pharm, L.H., & Cella, D. (2002). Measuring spiritual
well-being in patients with cancer: The functional assessment of chronic illness therapy –
spiritual well-being scale (FACIT-Sp). Annals of Behavioral Medicine, 24 (1), 49-58. Doi:
http://dx.doi.org.ez.statsbiblioteket.dk:2048/10.1207/S15324796ABM2401_06.
Pieper, J.Z.T., de Vries-Schot, M.R., & van Uden, M.H.F. (2012). Religious and receptive coping
importance for the well-being of Christian outpatients and parishioners. Archieve for the
Psychology of Religion, 34: 173-189.
Puchalski, C., Ferrell, B., Virani, R., Otis-Green, S., Baird, P., Bull, J….Sulmasy, D. (2009).
Improving the quality of life of spiritual care as a dimension of palliative care: The report
of the consensus conference. Journal of Palliative Medicine, 12 (10): 885-908.
Rosen, I. (2009). I’m a believer, but I’ll be damned if I’m religious. Belief and religion in the
Greater Copenhagen Area – a focus group study. Ph.D. Thesis. Lund’s University.
Rosmarin, D.H., Pargament, K.I., & Flannelly, K.L. (2007). Religious coping among Jews:
Development and initial validation of the JCOPE. Journal of Clinical Psychology, 65: 670-
683. doi: 10.1002/jclp.20574.
Salander, P. (2006). Who needs the concept of spirituality? Psycho-oncology, 15(7), 647-649
Saroglou, V. (2002). Religion and the five factors of personality: A meta-analytic review.
Personality and Individual Differences, 32, 15–25.
Schaefer, C.A. & Gorsuch, R.L. (1992). Dimensionality of religion: Belief and motivation as
predictors of behavior. Journal of Psychology and Christianity, 11(3): 244-254.
Schnell, T. (2010). Existential indifference: Another quality of meaning in life. Journal of
Humanistic Psychology, 50 (3): 351-373. doi: 10.1177/0022167809360259.
Schottenbauer, M.A., Rodgriguez, B.F., Glass, C.R., and Arnkoff, D.B. (2006). Religious coping
research and contemporary personality theory: An exploration of Endler’s (1997) integrative
personality theory. British Journal of Psychology, 97: 499-519. doi:
10.1348/000712606X97840.
Schottenbauer, M.A., Klimes-Dougan, B., Rodriguez, B.F., Arnkoff, D.B., Glass, C.R., Lasalle,
V.H. (2006b). Attachment and affective resolution following a stressful event: General and
religious coping as mediators. Mental Health, Religion, and Culture, 9 (5): 448-471. doi:
10.1080/13694670500440684.
___________________________________________
61
Schoenig, R. (2012). “World Religions: Facts, Comments, and Questions”. Talk presented at the
International Education Week, Nov. 15. http://www.theranger.org/u-s-most-religious-
country-in-industrialized-world-professor-says-1.2800927#.UcS7oTu_KSo.
Sherman, A.C., Plante, T.G., Simonton, S., Latif, U., Anaissie, E.J. (2009). Prospective study of
religious coping among patients undergoing autologous stem transplantation. Journal of
Behavioural Medicine, 32: 118-128. doi: 10.1007/s10865-008-9179-y.
Sherman, A.C., Simonton, S., Latif, U., Spohn, R., & Tricot, G. (2005). Religious struggle and
religious comfort in response to illness: Health outcomes among stem cell transplant
patients. Journal of Behavioral Medicine, 28 (4), 359-367.
Shipley, B.A., Weiss, A., Dear, G., Taylor, M.D., & Deary, I.J. (2007). Neuroticism, extraversion,
and mortality in the UK Health and Lifestyle Survey: A 21-Year prospective cohort study.
Psychosomatic Medicine, 69 (9): 923-931. doi: 10.1097/PSY.0b013e31815abf83.
Steel, P., Schmidt, J., & Shultz, J. (2008). Refining the relationship between personality and
subjective well-being. Psychological Bulletin, 134 (1): 138-161. doi: 10.1037/0033-
2909.134.1.138.
Stifoss-Hanssen, H. (1999). Religion and sprituality: What a European ear hears. The international
Journal for the Psychology of Religion, 9, 25-33.
Stålhandske, M.L., Ekstrand, M, & Tyden, T. (2011). Existential experiences and strategies in
relation to induced abortion: An interview study with 24 Swedish women. Archive for the
Psychology of Religion, 33 (3): 345-370.
Søndergaard, B. & Christensen, K.B. (2007). Sygehuse svigter patienternes åndelige behov.
(English: ”Hospitals disregard patients’ spiritual needs”). Sygeplejersken, 107 (5): 14-16.
Tarakeshwar, N., Pargament, K.I., & Mahoney, A. (2003). Initial development of a measure of
coping among Hindus. Journal of Community Psychology, 31: 607-628. doi:
10.1002/jcop.10071.
Tarakeshwar, N., Vanderwerker, L.C., Paulk, E., Pearce, M.J., Kasl, S.V., Prigerson, H.G. (2006).
Religious coping is associated with the quality of life of patients with advanced cancer.
Journal of Palliative Care, 9 (3): 646-657.
Tellegen, A. & Atkinson, G. (1974). Openness to Absorbing and Self-Altering Experiences
(Absorption), A Trait Related to Hypnotic-Susceptibility. Journal of Abnormal
Psychology, 83(3): 268-77.
___________________________________________
62
The European Value Survey, 2008. Data from Denmark. Originally conducted by prof. Peter
Gundelach. Data was made available by the Danish Data Archive (archive number DDA-
21432).
Thompson, M.P. & Vardaman, P.J. (1997). The role of religion in coping with the loss of a family
member to homicide. Journal for the Scientific Study of Religion, 36: 44-51. doi:
10.2307/1387881.
Thuné-Boyle, I.C., Stygall, J.A., Keshtgar, M.R., & Newman, S.P. (2006). Do religious/spiritual
coping strategies affect illness adjustment in patients with cancer? A systematic review of
the literature. Social Science and Medicine, 63: 151-164.
Thuné-Boyle, I.C., Stygall, J.A., Keshtgar, M.R., Davidson, T., & Newman, S.P. (2013).
Religious/spiritual coping resources and their relationship with adjustment in patients
newly diagnosed with breast cancer in the UK. Psycho-Oncology, 22: 646-658. doi:
10.1002/pon.3048.
Tomich, P.L. & Helgeson, V.S. (2004). Is finding something good in the bad always good? Health
Psychology, 23: 16-23.
Vail, K.E., III, Rothschild, Z.K., Weise, D.R., Solomon, S., Pyszczynski, T., & Greenberg, J.
(2010). A terror management analysis of the psychological functions of religion.
Personality and Social Psychology Review, 14, 84–94. doi:10.1177/1088868309351165.
Wood, B.T., Worthington Jr, E.L., Exline, J.J., Yali, A.M., Aten, J.D., & McMinn, M.R. (2010).
Development, refinement, and psychometric properties of the Attitudes Toward God Scale
(ATGS-9). Psychology of Religion and Spirituality, 2, 148–167. doi: 10.1037/a0018753
Wulff, D.M. (1997). Psychology of Religion. Classic and Contemporary. John Wiley & Sons, Inc.
www.aandeligomsorg.dk
www.faith-health.org
Zachariae R, Pedersen, C.G., Jensen, A.B., Ehrnrooth, E., Rossen, P.B., & von der Maase, H.
(2003). Association of perceived physician communication style with patient satisfaction,
distress, cancer-related self-efficacy, and perceived control over the disease. British
Journal of Cancer, 88(5): 658-65.
Zuckerman, P. (2008). Society without God. What the least religious nations can tell us about
contentment. New York, NY: NYU Press.

___________________________________________
63
Zwingmann, C., Müller, C., Körber, J., & Murken, S. (2008). Religious commitment, religious
coping and anxiety: a study in German patients with breast cancer. European Journal of
Cancer Care, 17: 361-370. doi: 10.1111/j.1365-2354.2007.00867.x
Yalom, I. D. (1980). Existential psychotherapy. New York: Basic Books.
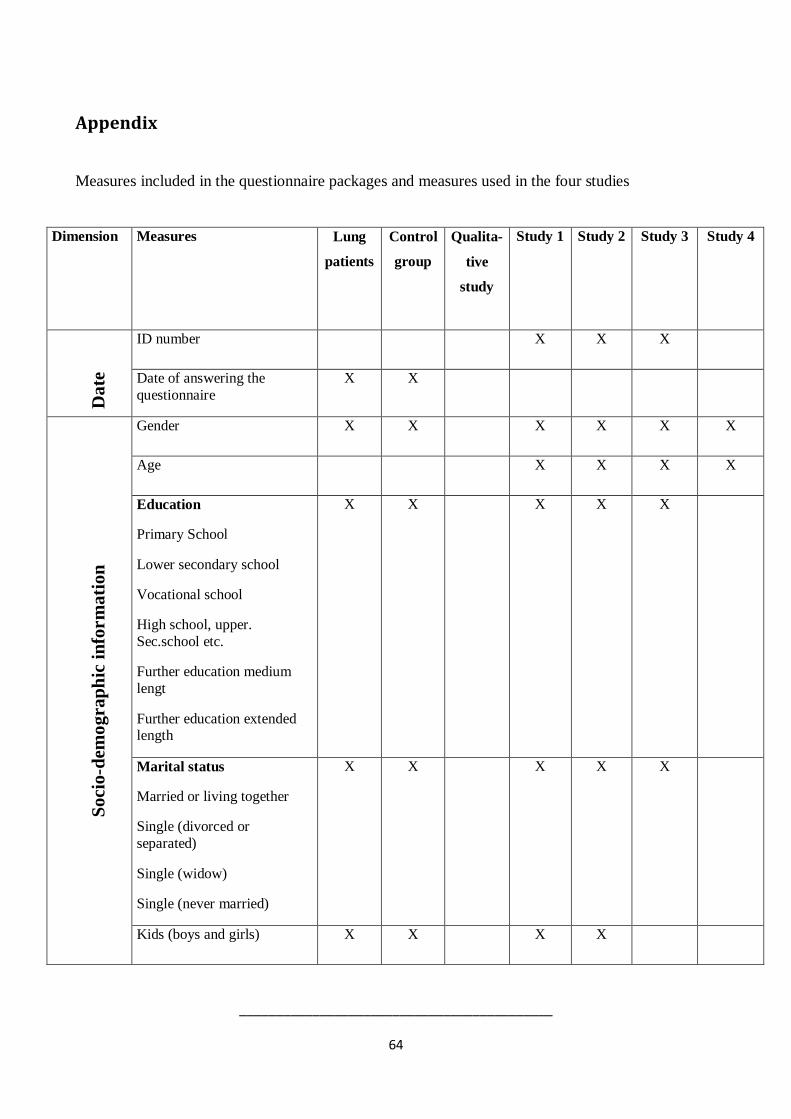
___________________________________________
64
Appendix
Measures included in the questionnaire packages and measures used in the four studies
Dimension Measures Lung
patients
Control
group
Qualita-
tive
study
Study 1 Study 2 Study 3 Study 4
Da
te
ID number X X X
Date of answering the
questionnaire
X X
So
cio
-dem
ograp
hic
in
form
ati
on
Gender X X X X X X
Age X X X X
Education
Primary School
Lower secondary school
Vocational school
High school, upper.
Sec.school etc.
Further education medium
lengt
Further education extended length
X X X X X
Marital status
Married or living together
Single (divorced or
separated)
Single (widow)
Single (never married)
X X X X X
Kids (boys and girls) X X X X

___________________________________________
65
Dimension Measures Lung
patients
Control
group
Qualita-
tive
study
Study 1 Study 2 Study 3 Study 4
Kids living at home (boys
and girls)
X X
Work situation before
illness
Self-employed
Full-time
Part-time
Umemployed (involuntary)
Umemployed (voluntary)
Pensioned/early retirement
Sick leave
X
Current work situation
Self-employed
Full-time
Part-time
Umemployed (involuntary)
Umemployed (voluntary)
Pensioned/early retirement
Sick leave
X X X X X
Annual income (household
and your own)
<200.000
2-300.000
3-400.000
4-500.000
5-600.000
X X X X X

___________________________________________
66
Dimension Measures Lung
patients
Control
group
Qualita-
tive
study
Study 1 Study 2 Study 3 Study 4
6-700.000
Volunteer work during the
last 12 months (relief work,
member of boards etc.)
X (2
items)
X (1
item)
X X
Dairy over the course of the
illness
X
Smoking X
Dela
y
Patient-delay og system-
delay (9 items)
X
Illn
ess
an
d c
o
morb
idit
y
Type of lung disease (COPD; cancer, other)
X X X
Treatment (Operation, chemo, other, don’t know)
X
Purpose of the treatment
(improve QOL, healing, life-sustaining)
X
CCI (Physical co morbidity) (Charlson et al., 1987)
X X X X
Qu
ali
ty o
f li
fe
FACT-G, 30 items
(physically, social, emotional, functional well-being) 21
items in control version
(Cella et al., 1993)
X X X X
FACIT Sp, 12 items
(Existential well-being) 10
items in control version (Peterman et al., 2002)
X X X X
Co
pin
g CBI-14 items (self-efficacy)
10 items in control version
(Merluzzi et al. 2001)
X X
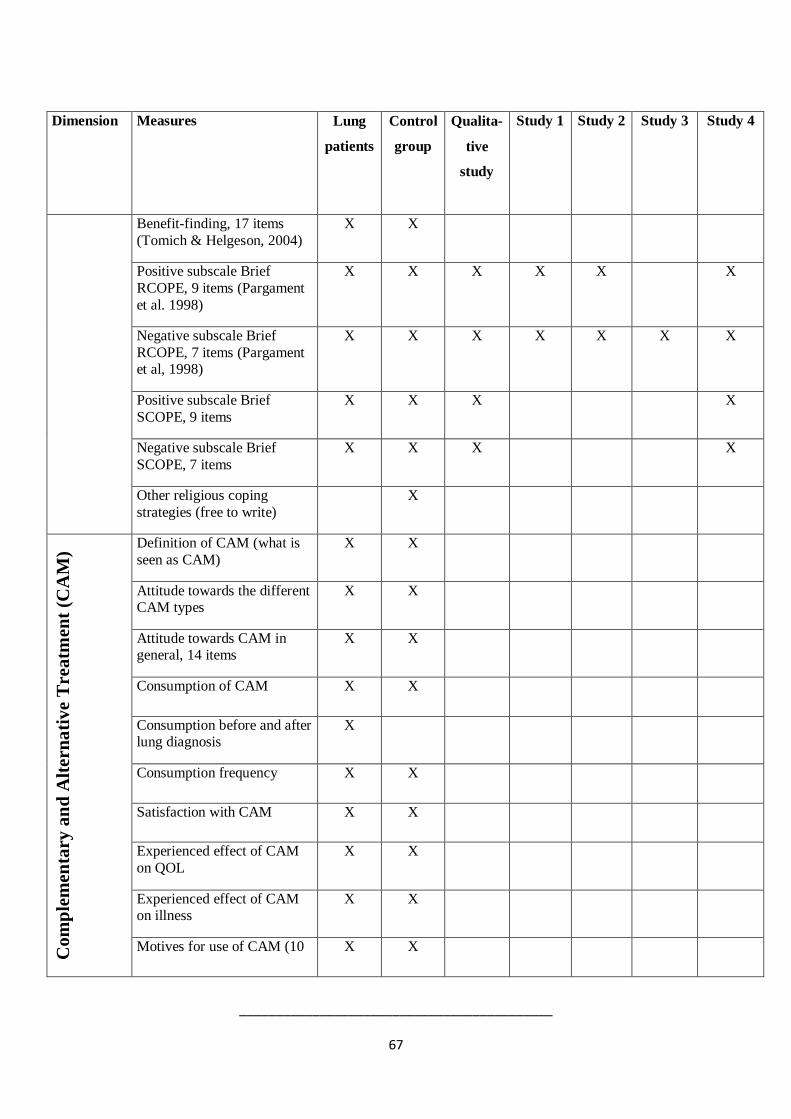
___________________________________________
67
Dimension Measures Lung
patients
Control
group
Qualita-
tive
study
Study 1 Study 2 Study 3 Study 4
Benefit-finding, 17 items
(Tomich & Helgeson, 2004)
X X
Positive subscale Brief
RCOPE, 9 items (Pargament
et al. 1998)
X X X X X X
Negative subscale Brief
RCOPE, 7 items (Pargament et al, 1998)
X X X X X X X
Positive subscale Brief
SCOPE, 9 items
X X X X
Negative subscale Brief
SCOPE, 7 items
X X X X
Other religious coping
strategies (free to write)
X
Co
mp
lem
en
tary
an
d A
ltern
ati
ve
Treatm
en
t (C
AM
)
Definition of CAM (what is
seen as CAM)
X X
Attitude towards the different CAM types
X X
Attitude towards CAM in general, 14 items
X X
Consumption of CAM X X
Consumption before and after lung diagnosis
X
Consumption frequency X X
Satisfaction with CAM X X
Experienced effect of CAM
on QOL
X X
Experienced effect of CAM on illness
X X
Motives for use of CAM (10 X X
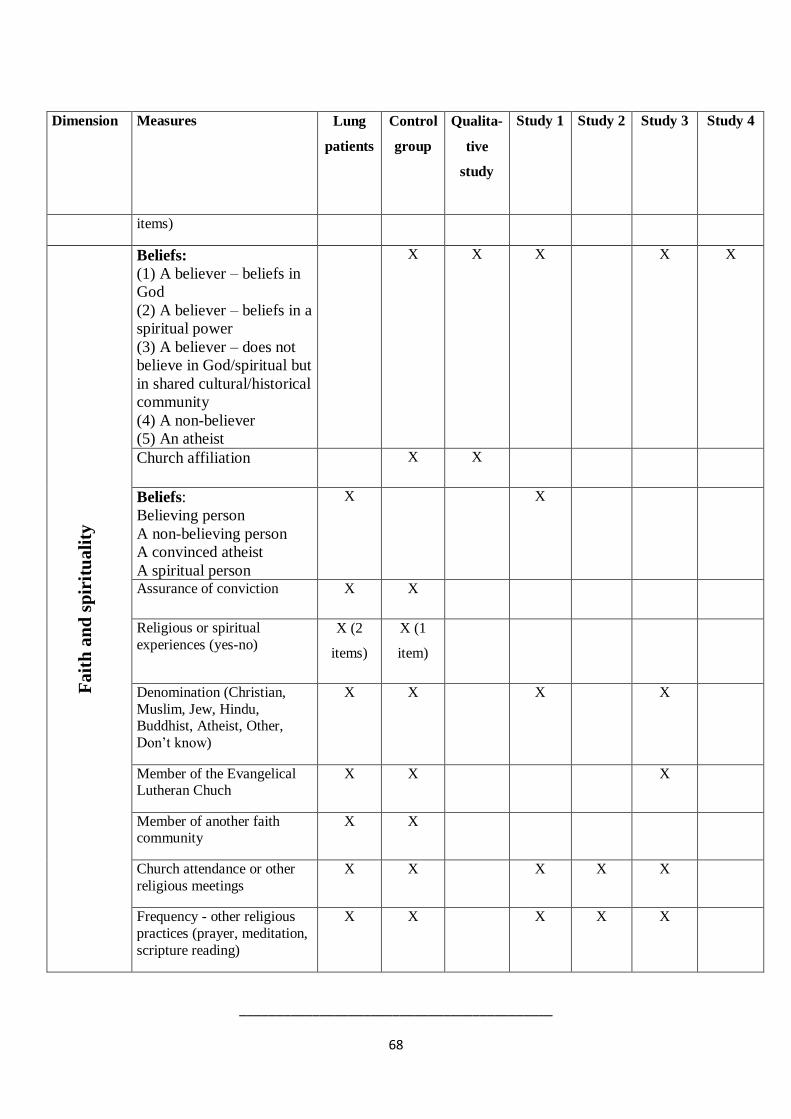
___________________________________________
68
Dimension Measures Lung
patients
Control
group
Qualita-
tive
study
Study 1 Study 2 Study 3 Study 4
items)
Fait
h a
nd
sp
irit
uali
ty
Beliefs:
(1) A believer – beliefs in
God
(2) A believer – beliefs in a
spiritual power
(3) A believer – does not
believe in God/spiritual but
in shared cultural/historical
community
(4) A non-believer
(5) An atheist
X X X X X
Church affiliation X X
Beliefs:
Believing person
A non-believing person
A convinced atheist
A spiritual person
X X
Assurance of conviction X X
Religious or spiritual
experiences (yes-no) X (2
items)
X (1
item)
Denomination (Christian,
Muslim, Jew, Hindu, Buddhist, Atheist, Other,
Don’t know)
X X X X
Member of the Evangelical Lutheran Chuch
X X X
Member of another faith community
X X
Church attendance or other
religious meetings
X X X X X
Frequency - other religious
practices (prayer, meditation,
scripture reading)
X X X X X
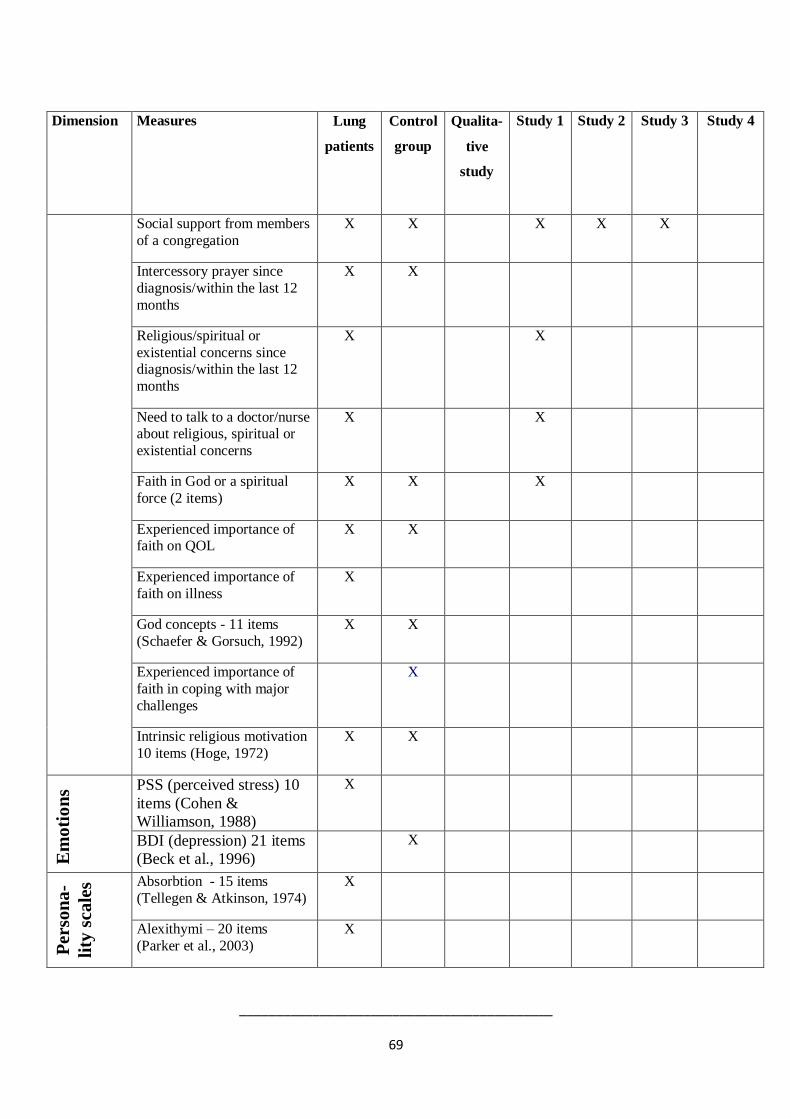
___________________________________________
69
Dimension Measures Lung
patients
Control
group
Qualita-
tive
study
Study 1 Study 2 Study 3 Study 4
Social support from members
of a congregation
X X X X X
Intercessory prayer since
diagnosis/within the last 12
months
X X
Religious/spiritual or
existential concerns since diagnosis/within the last 12
months
X X
Need to talk to a doctor/nurse about religious, spiritual or
existential concerns
X X
Faith in God or a spiritual
force (2 items)
X X X
Experienced importance of faith on QOL
X X
Experienced importance of
faith on illness
X
God concepts - 11 items
(Schaefer & Gorsuch, 1992)
X X
Experienced importance of
faith in coping with major
challenges
X
Intrinsic religious motivation
10 items (Hoge, 1972)
X X
Em
oti
on
s PSS (perceived stress) 10
items (Cohen &
Williamson, 1988)
X
BDI (depression) 21 items
(Beck et al., 1996)
X
Perso
na
-
lity
sca
les Absorbtion - 15 items
(Tellegen & Atkinson, 1974)
X
Alexithymi – 20 items
(Parker et al., 2003)
X
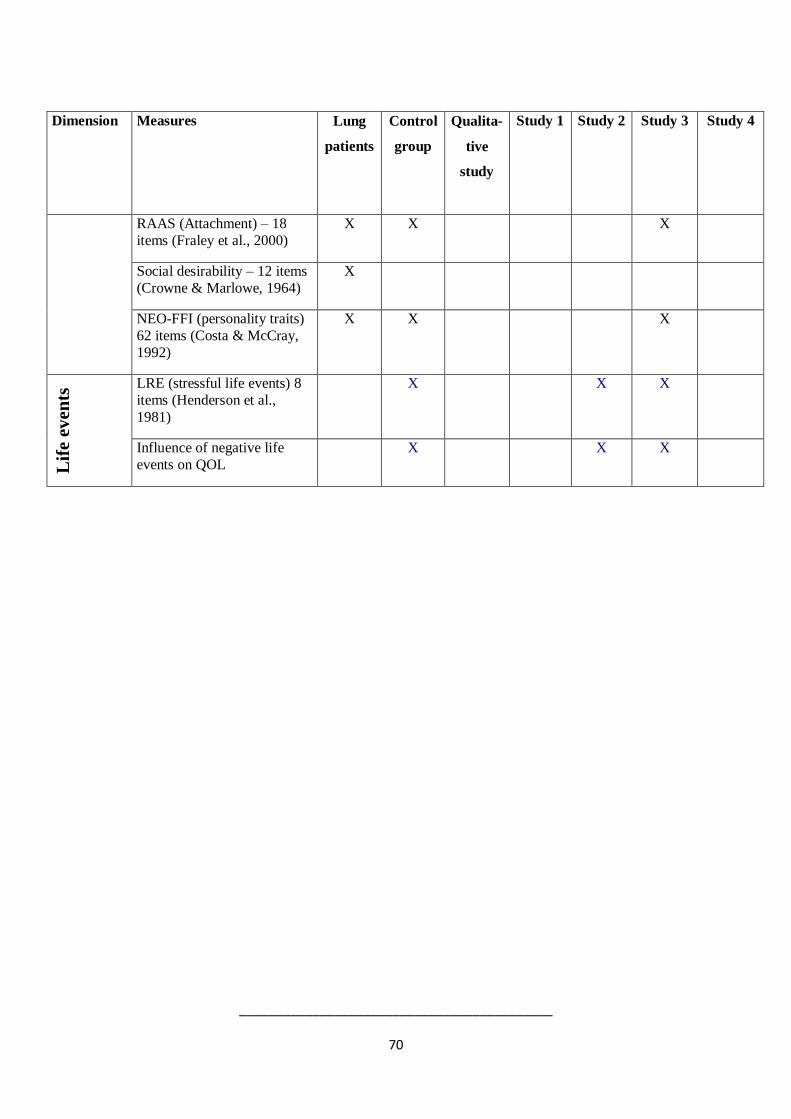
___________________________________________
70
Dimension Measures Lung
patients
Control
group
Qualita-
tive
study
Study 1 Study 2 Study 3 Study 4
RAAS (Attachment) – 18
items (Fraley et al., 2000)
X X X
Social desirability – 12 items
(Crowne & Marlowe, 1964)
X
NEO-FFI (personality traits)
62 items (Costa & McCray,
1992)
X X X
Lif
e e
ven
ts LRE (stressful life events) 8
items (Henderson et al.,
1981)
X X X
Influence of negative life
events on QOL
X X X

Paper 1

The International Journal for the Psychology of Religion, 23:188–203, 2013
Copyright © Taylor & Francis Group, LLC
ISSN: 1050-8619 print/1532-7582 online
DOI: 10.1080/10508619.2012.728068
Religious Coping and Quality of Life AmongSeverely Ill Lung Patients in a Secular Society
Heidi F. PedersenDepartment of Psychology
Aarhus University, Denmark
Kenneth I. PargamentDepartment of Psychology
Bowling Green State University
Christina G. PedersenDepartment of Psychology
Aarhus University, Denmark
Robert ZachariaeDepartment of Oncology
Aarhus University Hospital, Denmark
This survey study investigated the prevalence of religious beliefs and religious coping and possible
associations between religious factors and quality of life (QoL) among a group of severely ill lung
patients (lung cancer and chronic obstructive pulmonary disease) in Denmark (N D 111). Almost
two thirds (64.8%) reported having some belief in God and/or a spiritual power. Patients who
reported believing in God and patients who believed in God and a spiritual power reported better
QoL than patients who reported that they believed in a spiritual power only. Religious coping was
prevalent; for positive religious coping strategies, those used from least to most often, respectively,
were invoked 15% to 37% of the time; for negative religious coping strategies the percentages
were 3% to 16%. Negative religious coping was associated with lower QoL (ˇ D �0.320, p <
.006), whereas no associations were found between positive religious coping and QoL. Results are
discussed in relation to the cultural context of secularized societies like the Scandinavian countries.
Spirituality and religion have received increased attention in health research (Cobb, Puchalski,
& Rumbold, 2012; Masters & Hooker, 2013). A number of studies have linked religion andspirituality with the development and course of a variety of diseases (Koenig, King, & Carson,
Correspondence should be sent to Heidi Frølund Pedersen, Department of Psychology, Aarhus University, 8000
Aarhus C, Denmark. E-mail: [email protected]
188
COPING AND QUALITY OF LIFE FOR LUNG PATIENTS 189
2012). In addition, indices of religiousness have been found associated with lower mortality
(McCullough, Hoyt, Larson, Koenig, & Thoresen, 2000) as well as with various measuresof well-being and quality of life (QoL) (Krupski et al., 2006; Mytko & Knight, 1999). In
general, religion and spirituality appear to be associated with improved health, although some
studies have found ambiguous results indicating at least some negative effects of religion and
spirituality on well-being and health (for a comprehensive review, see Cobb et al., 2012).
Research in this domain has so far been limited in some important respects. Perhaps mostimportant, there are problems of measurement. Religion and spirituality have most often been
assessed with global one-dimensional constructs, for example, frequency of church attendance
(Hill, 2013; Hill & Pargament, 2003). Such measures are unable to pinpoint the possible “active
ingredients” in religion and spirituality that promote or impair health and well-being, because
religion is multidimensional (Stefanek, McDonald, & Hess, 2005).
Researchers have therefore called for more specific, theory-based approaches to investigatingand measuring religiousness and spirituality (Paloutzian & Park, 2013; Park & Paloutzian,
2013). Some advances have been made, particularly in the area of religious coping research.
Growing out of the transactional coping theory of Lazarus and Folkman (1984), studies of
religious coping focus on the variety of ways in which religion and spirituality are expressed
in the efforts of people to understand and deal with major life stressors. Pargament (1997) de-scribed religious coping as multidimensional (e.g., cognitive, behavioural, affective, relational),
multipurpose (e.g., meaning making, intimacy, control, comfort, closeness with God), and
multivalent (i.e., potentially helpful or harmful). Research on religious coping attempts to take a
focused, differentiated look at religious coping strategies, which include both positive religious
coping (e.g., seeking spiritual support) and negative religious coping or religious struggles(e.g., anger at God). Empirical studies have shown that positive religious coping methods are
generally related to more favourable health outcomes among patients with severe illnesses, such
as cancer, heart disease, and HIV/AIDS (Ano & Vasconcelles, 2005), although there have been
some exceptions to this pattern of findings (Hills, Paice, Cameron, & Shott, 2005). Conversely,
negative religious coping have been found associated with increased distress, lower well-being,
and higher mortality among severely ill patients (Pargament, Koenig, Tarakeswar, & Hahn,2001; Sherman, Simonton, Latif, Spohn, & Tricot, 2005; Zwingmann, Wirtz, Müller, Körber,
& Murken, 2006).
A key limitation to these studies is that the majority of research has been conducted within
the theistic context of North America and with largely Christian participants. It is unclear how
well the research paradigms and methods developed in research with North American Christiansapply to other, less religious contexts. Some researchers have, for example, argued that this type
of research cannot be generalized to secularized countries (e.g., European societies; Salander,
2006). The present study examined the prevalence of religiousness among people dealing
with significant medical illness in Denmark and considers the degree to which indices of
religiousness and religious coping are predictive of the patients’ QoL.
SECULARIZATION?
Sociologists continue to debate whether “secularization” adequately describes the changing role
of religion in Europe, as religion in European countries displays different patterns of change.

190 PEDERSEN ET AL.
Furthermore, empirical studies suggest that about 42% of the European population may fall
into the category of “fuzzy fidelity,” that is, people who are neither traditionally religious norcompletely secularized (Voas, 2009). Denmark has been named one of the most secularized
countries in the world (Zuckerman, 2008). Approximately 51.8% of Danes are estimated to
be “fuzzies,” 28.7% secular, and only 19.5% very religious (Storm, 2009). This finding is
supported by other sociological studies suggesting that although more than 80% of Danes are
members of the National Church, only 2% attend church services regularly (Højsgaard & RavnIversen, 2005). Through interviews with 150 Danes and Swedes, Zuckerman (2008) arrived at
a picture of Danes as Cultural Christians, who attend church for social events a few times a
year and fail to hold or practice any traditional Christian beliefs. In fact, Zuckerman suggested
that religion is simply a nonissue to Danes.
RELIGIOSITY AND HEALTH IN DENMARK
But is religiousness largely irrelevant to Danes? A few studies have provided indirect evidence
to suggest that this may not be the case, especially when illness strikes. In a survey of
a cohort of 3,128 Danish women treated for primary breast cancer, 83% reported havingeither unambiguous or at least a little faith in “God or a higher spiritual being,” which
is somewhat larger than what one finds in the general Danish population (65%) (Pedersen,
2009). In another study of 480 hospitalized Danish patients, those with severe illnesses also
reported more existential, spiritual, and religious practice activity; this tendency was higher for
younger patients (<36 years) (la Cour, 2008). These results suggest that a medical crisis mayelicit religious and spiritual beliefs and practices even among people in the most secularized
societies. Such findings have been explained by the “religious coping mobilization” effect
(Koenig, Pargament, & Nielsen, 1998; Pargament, 1997). That is, the crisis of illness prompts
greater reliance on religious resources or greater religious struggle as individuals are faced with
new challenges.
Elaborating on this process of religious coping mobilization, Pargament (1997) noted thatpeople appear to have different orienting systems, that is, cognitive schematas shaped by
previous experiences that help them navigate and make sense of the world. Major life crises,
such as severe illness, may be more likely to activate religious beliefs and practices as a way of
coping with stressful events, even if religion makes up only a minor part of the orienting system.
This theoretical perspective may also apply to Danes who, although not very religious, are nottotally removed from religious expression. Studies describing the prevalence and influence of
belief in God in Denmark indicate that the number of Danes believing in a deity is similar to
the level reported 50 years ago, although it has been argued that beliefs have shifted from a
traditional view of an active and involved God to more ill-defined images of a distant, divine
entity (Lüchau, 2005). It is important to recognize, however, that people who are either nottraditionally religious or totally secular (i.e., fuzzies) may also find it more difficult to mobilize
religious or spiritual beliefs and practices because they lack the foundation of a strong religious
belief system or context to support these beliefs.
Religious orienting systems that lack integration and coherence may also be more easily
shaken by major crises, leading to religious struggles and poorer adjustment in turn (Exline
& Rose, 2013; Gall, Kristjansson, Charbonneau, & Florrack, 2009; Pargament, 2007). Among

COPING AND QUALITY OF LIFE FOR LUNG PATIENTS 191
Danes manifesting lower levels of consistent, integrated religious and spiritual beliefs, illness
could therefore be particularly likely to trigger existential, spiritual, and religious strugglesand subsequent distress. On the other hand, it could also be argued that groups not bound to
specific religious systems of belief and practice (i.e., “fuzzies”) may be able to adapt more
flexibly than religious individuals to stressful situations (la Cour, 2005).
OBJECTIVES
The present study was designed to explore the assertion that religiousness is largely irrelevant to
the lives of people in secularized societies. More specifically, we investigated the prevalence ofreligiousness and positive and negative religious coping among a group of patients from a highly
secularized country (Denmark) with severe, chronic lung diseases (i.e., lung cancer and chronic
obstructive pulmonary disease [COPD]). We hypothesized that because of the serious nature
of these lung diseases, a substantial proportion of patients with lung disease would manifest
signs of religiousness and make use of religious coping methods. We also hypothesized thatthe outcomes on measures of religiosity, spirituality, and religious coping would be associated
with QoL. It was predicted that positive religious coping would be associated with better QoL
and that negative religious coping would be associated with poorer QoL.
METHODS
Participants
The sample included 62 men and 49 women between the ages 26 and 105 years (M D 65.2,SD D 10.2) newly diagnosed with chronic lung diseases, that is, lung cancer (39.1%) and
COPD/other lung diseases like bronchiecstasia (60.9%). More than two thirds (68.5%) of the
patients had less than 11 years of education, 72.7% were married, 67% were retired, and
39.4% reported an annual income below USD$35,700, which according to the Organisation
for Economic Co-operation and Development (OECD) standards is perceived as relative povertyin Denmark (OECD, 2009). Thus, this sample was considered relatively low socioeconomic
status (SES).1
Procedure
Five respiratory medicine clinics (four on the main peninsula of Jutland and one at an island inthe eastern part of Denmark) participated in the project. From October 2008 to October 2010,
patients being diagnosed with a severe chronic lung disease were informed about the study by
the medical staff and asked to give their informed consent to participate. Patients were asked
to complete the questionnaire shortly after their diagnosis and return it to the research team by
mail. Those who did not return the questionnaire within 2 weeks received a single reminder. In
1Detailed sociodemographic data were collected and are available from the author, but analyses indicated that these
data did not affect the outcomes on the key dependent measures and are therefore not subsequently referred to.

192 PEDERSEN ET AL.
all, 514 received the questionnaire and 120 responded (response rate D 23.4%). Nine patients
were excluded because of insufficient data, resulting in a final sample of 111 patients. Theproject was evaluated by the Committee on Biomedical Research Ethics in Denmark.
Measures
The present study was part of a larger study on QoL, complementary alternative treatment,
and religiosity among severely ill chronic lung disease patients in Denmark, and measures
in the questionnaire package included medical information, information on psychosocial vari-
ables such as self-efficacy, QoL, personality traits, religious measures, and information about
complementary and alternative treatment. In the present study, the following measures wereused.
Sociodemographic information. Sociodemographic information included age, gender,
marital status (dichotomized into married/cohabiting and widowed/divorced/single), number
of children, highest education level (dichotomized into “Low education” D 7–10 years and
“High education” >10 years), current work situation (dummy coded into “Part-time/sick leave,”
“Retired,” and “Full time”) and SES.
Medical information. Information about the patients’ medical condition was retrievedfrom the Danish Lung Cancer Registry and from the records of the participating respiratory
medical clinics. The variables included diagnosis and date of diagnosis. Self-reported comor-
bidity was assessed with an adapted version of the Charlson Co-morbidity Index (Charlson,
Pompei, Ales, & MacKenzie, 1987; Christensen et al., 2009).
Health-related QoL and existential well-being. A Danish version of the Functional
Assessment of Cancer Therapy Scale (Cella et al., 1993) was used to measure overall QoL.This scale is a standardized questionnaire developed for cancer research and contains 30 items
covering the patients’ physical, emotional, social, and functional well-being. Responses are
given on a 5-point Likert scale ranging from not at all to a lot. In addition, existential well-
being was measured using the FACIT-Sp (Peterman, Fitchett, Brady, Pharm, & Cella, 2002), a
12-item questionnaire covering the patients’ sense of meaning, purpose and peace in life, andability to find comfort in spiritual convictions during illness. In the present sample, the internal
consistency (Cronbach’s alpha) of the total QoL score was 0.95 and ranged from 0.77 to 0.90
for the subscales.
Beliefs and religious identifiers. Patients were asked two questions concerning their
religious beliefs: whether they believed in “God” and whether they believed in a “Spiritual
power,” each with the response options of “yes, “maybe,” or “no.” Participants with no belief ineither God or a spiritual power were coded as “Non-believers.” Participants having unambiguous
or little faith (Yes C Maybe) in a spiritual power only were coded as “spiritual believers.”
Participants having unambiguous or a little faith (Yes C Maybe) in God only C God and a
spiritual power were coded as “God-believers.” Patients were also asked to identify themselves
as either “a believing person,” “a spiritual person,” “a nonbelieving person,” and “a convinced
atheist.” “Nonbelieving” patients and “Atheists” were coded as “nonbelieving patients.”

COPING AND QUALITY OF LIFE FOR LUNG PATIENTS 193
Religious behavior, thoughts and needs. Public religious behavior was measured by
a single item about church attendance and/or attendance at other religious meetings. Privatereligious behavior was measured by a single item about the frequency of prayer, meditation,
and/or scripture readings. Response options to these measures were 5-point Likert scales
ranging from never to every day. Participants were also asked if they since their diagnosis
had experienced more frequent religious thoughts (e.g., thoughts about the existence of God),
spiritual thoughts (e.g., thoughts about the existence of a spiritual power), and/or existentialthoughts (e.g., thoughts about finding meaning, purpose and peace), and whether they had
experienced the need to consult a professional about these religious, spiritual, and/or existential
thoughts. Response options to these measures were “yes” or “no.”
Congregational support. This construct was measured by a single item: “To what degree
do you receive support from your fellow believers” on a 5-point Likert scale with response
options ranging from not at all to a great deal.
Religious coping. Positive and negative religious coping was measured by the Brief
RCOPE (Pargament, Smith, Koenig, & Perez, 1998), a 14-item measure with two subscales:
Positive Religious Coping and Negative Religious Coping. Positive Religious Coping measures
the degree to which the patients cope with illness by looking to God for comfort and support,
and Negative Religious Coping measures to which degree the patients interpret their illness asa punishment or abandonment by God. The response format is a 4-point Likert scale ranging
0 (not at all), 1 (to some degree), 2 (a lot), and 3 (a great deal). The questionnaire was
translated into Danish by three independent translators, and the translations were discussed until
agreement was obtained. A preliminary qualitative pilot study conducted by the research team
(unpublished) revealed potential problems with using the scales among Danish nonbelievers.
Results indicated that nonbelievers may score higher on negative religious coping as a way toexpress their disbelief rather than religious struggle. For example, an item like “Questioned the
power of God” may be answered with “a great deal” by a nonbeliever, not because he or she
has religious doubts but simply because the person does not believe in God’s powers. Thus,
the item “Questioned the power of God” was omitted, and furthermore nonbelievers were
left out of the analyses concerning associations between religious coping on QoL. Internalconsistencies (Cronbach’s alpha) were 0.93 for the Positive Religious Coping subscale and
0.60 for the Negative Religious Coping subscale in the present sample. Among “believing”
and “spiritual” patients, Cronbach’s alphas were 0.92 for Positive Religious Coping and 0.71
for Negative Religious Coping.
Statistical Analysis
Mean substitution was used to handle missing data on continuous variables in accordance withSchafer and Graham (2002). This procedure is adequate and preferable to procedures such
as listwise deleting or scale mean substitution. Means and standard deviations of religious
coping were explored. Religious coping was positively skewed, and nonparametric as well
as parametric tests were applied when appropriate. Kruskal–Wallis tests were conducted to
determine possible differences in religious coping between “believing,” “spiritual,” and “non-
believing” patients. Bivariate, unadjusted regressions and one-way analyses of variance were

194 PEDERSEN ET AL.
conducted to explore associations between demographic factors, medical factors, religiousness,
religious coping, and overall QoL. Finally, hierarchal regression analyses were conducted todetermine the associations between religious coping and QoL while adjusting for demographic,
medical, and religious factors. Prior to testing a final model, three independent regression
models were conducted to determine which variables should be included in the final regression
in order to prevent overfitting. The first model consisted of demographic variables: marital
status, education, annual house income, and current work situation. To prevent underfitting,the significance level in the first three independent regression models was set at p < .10, and
variables that were significant at this level were carried forward to the next model testing the
medical factors: Diagnosis and Charlson Co-morbidity Index scores. The statistically significant
variables in the second model were carried forward to the third model testing religious factors:
congregational support, religious coping, and church attendance. In the final model, all variables
that were significant at level p < .10 in the previous three independent models were included.The level of significance for the final model was set at p < .05.
RESULTS
Prevalence of Religiousness and Existential Needs
The sample consisted of 83.6% Christians, and 54.9% reported unambiguous faith or a little
faith in God, 9.9% had unambiguous faith or a little faith in a spiritual power only, and 35.1%
reported no belief in either God or a spiritual power. A total of 14.6% reported that they
attended church regularly (more than once a month) and 23.1% reported praying more than
once during the week. Since the time of diagnosis, between 10.2% and 16.2% reported havingmore religious, spiritual, or existential thoughts. Although none reported having a need to
discuss religious thoughts with a professional, a minor proportion (0.9–3.6%) reported having
experienced a need to talk about spiritual or existential thoughts with a professional.
Prevalence of Religious and Spiritual Coping
Table 1 displays means and standard deviations on the religious coping subscales and the
percentages of patients indicating that they use the respective coping strategies to some extent
or more. The most frequently reported positive religious coping strategies were “Seeking God’slove and care” (seeking spiritual support), “Trying to see how God might strengthen me in this
situation” (religious transformation), and “Asking forgiveness for my sins (religious purifica-
tion).” Negative strategies like “Deciding the devil made this happen (demonic reappraisal)”
and “Wondering whether my religious community had abandoned me” (interpersonal religious
discontent) were less frequent.Kruskal–Wallis tests were used to test possible significant differences in religious coping
between patients considering themselves to be “a believing person,” “a spiritual person,” and “a
nonbelieving person.” The difference was statistically significant for Positive Religious Coping
�2(90) D 14.37, p D .001, and no statistical differences were found for Negative Religious
Coping. Mann–Whitney tests were used to run post hoc analyses applying a Bonferroni
correction of the alpha value (p < .017). Results indicated that “believers” scored significantly

COPING AND QUALITY OF LIFE FOR LUNG PATIENTS 195
TABLE 1
Percentages of Patients Indicating That They Use Religious Coping to ‘‘Some Degree’’ or More
Type of Patient
Total
% (N)a
Believing
% (N)b
Spiritual
% (N)c
Nonbelieving
% (N)d P
Positive religious coping (“Some degree” or more)
1. Looking for a stronger connection with God 26.1 (96) 40.3 (62) 36.4 (11) 0.0 (18) .005
2. Seek Gods love and care 36.9 (96) 54.8 (62) 36.4 (11) 11.1 (18) .004
3. Seek Gods help to let go of my anger 19.8 (96) 29.0 (62) 18.2 (11) 5.6 (18) .105
4. Try to put my plans into action together with God 22.5 (96) 32.3 (62) 27.3 (11) 5.6 (18) .077
5. Try to see how God might try to strengthen me
in this situation
32.2 (97) 50.8 (63) 18.2 (11) 5.6 (18) .001
6. Ask forgiveness for my sins 28.8 (97) 41.3 (63) 36.4 (11) 5.6 (18) .018
7. Focus on my religion to stop worrying about my
problems
15.3 (97) 22.2 (63) 18.2 (11) 5.6 (18) .275
Positive religious coping MEAN and
(standard deviation)
3.1 (4.5) 4.1 (4.8) 2.9 (4.6) 0.04 (1.4) .001
Negative religious coping (“Some degree”–“A great deal”)
8. Feel that God has abandoned me 6.3 (17) 8.2 (61) 0.0 (10) 11.1 (18) .570
9. Feel that I am being punished by God 5.4 (95) 8.1 (62) 0.0 (10) 5.6 (18) .624
10. Wonder what I did since God is punishing me 9.9 (96) 12.9 (62) 0.0 (11) 11.0 (18) .451
11. Questioned Gods love for me 16.2 (97) 15.9 (63) 9.1 (11) 27.8 (18) .372
12. Wonder whether my religious community has
abandoned me
1.8(101) 3.2 (63) 0.0 (15) 0.0 (18) .586
13. Decided that an evil power (like the Devil) made
this happen
2.7 (97) 4.8 (63) 0.0 (11) 0.0 (18) .490
Negative religious coping MEAN and
(standard deviation)
1.5 (2.1) 1.2 (2) 0.7 (1.6) 2.8 (2.3) .343
aN D 111. bN D 68. cN D 17. dN D 19.
higher on Positive Religious Coping (z D �3.764, p D .001) than nonbelievers. “Spiritual”
patients scored significantly higher than nonbelievers on positive religious coping (z D �2.186,
p D .029). There were no significant differences between believers and spiritual patients onthe Positive Religious Coping scale.
Religious and Spiritual Beliefs Associated QoL
One-way analyses of variance were conducted to test the associations between overall QoLand beliefs in God and/or a spiritual power. The results suggested that “God-believing” pa-
tients (patients believing in God and patients believing in God and a spiritual power) had
a higher overall QoL compared to patients having no belief or belief in a spiritual power
only, F(2, 102) D 4.451, p D .014. Post hoc analyses (Bonferroni tests, adjusting for multiple
comparisons) indicated that “spiritual believing” patients (believing in a spiritual power only),
had a significantly (p < .05) lower QoL than God-believing patients. The difference between
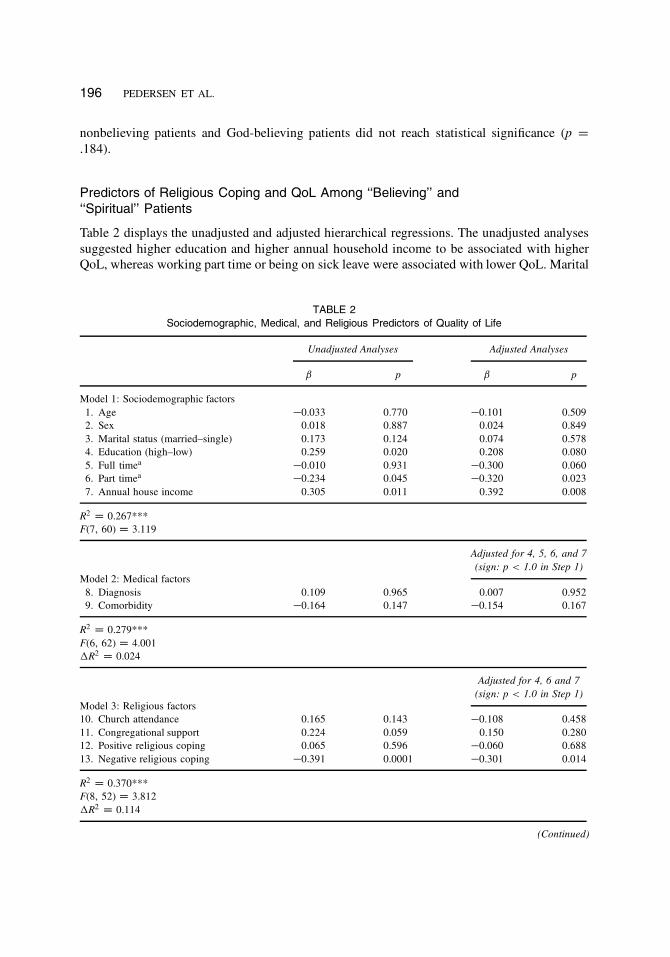
196 PEDERSEN ET AL.
nonbelieving patients and God-believing patients did not reach statistical significance (p D
.184).
Predictors of Religious Coping and QoL Among ‘‘Believing’’ and
‘‘Spiritual’’ Patients
Table 2 displays the unadjusted and adjusted hierarchical regressions. The unadjusted analyses
suggested higher education and higher annual household income to be associated with higherQoL, whereas working part time or being on sick leave were associated with lower QoL. Marital
TABLE 2
Sociodemographic, Medical, and Religious Predictors of Quality of Life
Unadjusted Analyses Adjusted Analyses
ˇ p ˇ p
Model 1: Sociodemographic factors
1. Age �0.033 0.770 �0.101 0.509
2. Sex 0.018 0.887 0.024 0.849
3. Marital status (married–single) 0.173 0.124 0.074 0.578
4. Education (high–low) 0.259 0.020 0.208 0.080
5. Full timea�0.010 0.931 �0.300 0.060
6. Part timea�0.234 0.045 �0.320 0.023
7. Annual house income 0.305 0.011 0.392 0.008
R2D 0.267***
F(7, 60) D 3.119
Adjusted for 4, 5, 6, and 7
(sign: p < 1.0 in Step 1)
Model 2: Medical factors
8. Diagnosis 0.109 0.965 0.007 0.952
9. Comorbidity �0.164 0.147 �0.154 0.167
R2D 0.279***
F(6, 62) D 4.001
�R2D 0.024
Adjusted for 4, 6 and 7
(sign: p < 1.0 in Step 1)
Model 3: Religious factors
10. Church attendance 0.165 0.143 �0.108 0.458
11. Congregational support 0.224 0.059 0.150 0.280
12. Positive religious coping 0.065 0.596 �0.060 0.688
13. Negative religious coping �0.391 0.0001 �0.301 0.014
R2D 0.370***
F(8, 52) D 3.812
�R2D 0.114
(Continued)
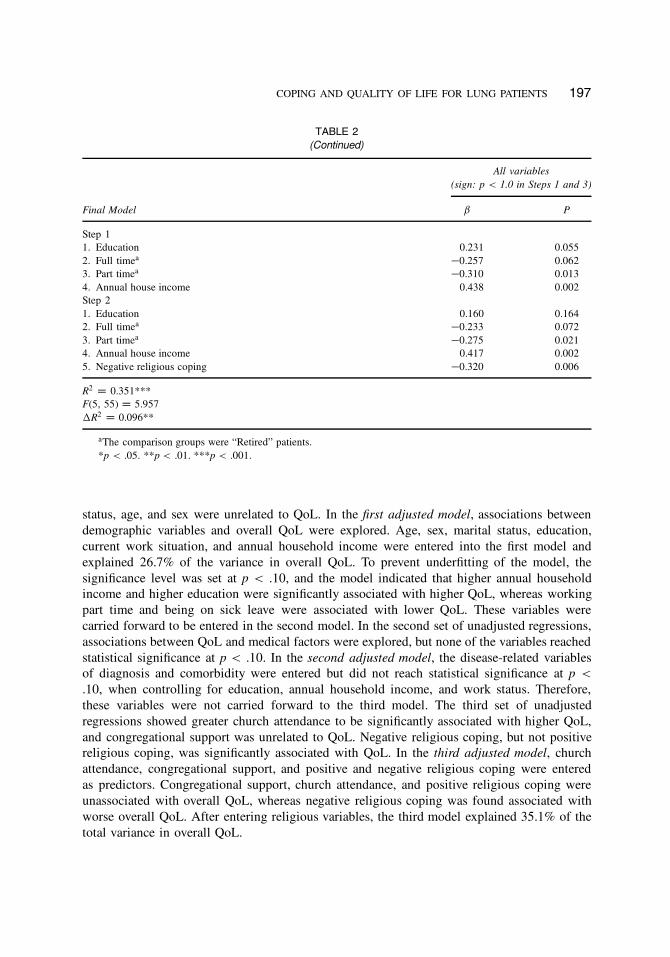
COPING AND QUALITY OF LIFE FOR LUNG PATIENTS 197
TABLE 2
(Continued)
All variables
(sign: p < 1.0 in Steps 1 and 3)
Final Model ˇ P
Step 1
1. Education 0.231 0.055
2. Full timea�0.257 0.062
3. Part timea�0.310 0.013
4. Annual house income 0.438 0.002
Step 2
1. Education 0.160 0.164
2. Full timea�0.233 0.072
3. Part timea�0.275 0.021
4. Annual house income 0.417 0.002
5. Negative religious coping �0.320 0.006
R2D 0.351***
F(5, 55) D 5.957
�R2D 0.096**
aThe comparison groups were “Retired” patients.
*p < .05. **p < .01. ***p < .001.
status, age, and sex were unrelated to QoL. In the first adjusted model, associations between
demographic variables and overall QoL were explored. Age, sex, marital status, education,
current work situation, and annual household income were entered into the first model and
explained 26.7% of the variance in overall QoL. To prevent underfitting of the model, the
significance level was set at p < .10, and the model indicated that higher annual householdincome and higher education were significantly associated with higher QoL, whereas working
part time and being on sick leave were associated with lower QoL. These variables were
carried forward to be entered in the second model. In the second set of unadjusted regressions,
associations between QoL and medical factors were explored, but none of the variables reached
statistical significance at p < .10. In the second adjusted model, the disease-related variablesof diagnosis and comorbidity were entered but did not reach statistical significance at p <
.10, when controlling for education, annual household income, and work status. Therefore,
these variables were not carried forward to the third model. The third set of unadjusted
regressions showed greater church attendance to be significantly associated with higher QoL,
and congregational support was unrelated to QoL. Negative religious coping, but not positivereligious coping, was significantly associated with QoL. In the third adjusted model, church
attendance, congregational support, and positive and negative religious coping were entered
as predictors. Congregational support, church attendance, and positive religious coping were
unassociated with overall QoL, whereas negative religious coping was found associated with
worse overall QoL. After entering religious variables, the third model explained 35.1% of the
total variance in overall QoL.

198 PEDERSEN ET AL.
The final model included variables significant at p < .10 in the previous adjusted regressions.
The significance level in the final model was set at p < .05. In the final model, threevariables reached statistical significance, with working part time/being on sick leave, annual
household income, and using negative religious all being significantly associated with poorer
QoL.
DISCUSSION
It has been argued that religiousness may be largely irrelevant to people in secular societies
like Denmark (Zuckerman, 2008). However, religiosity has so far been assessed in very generalterms and has not been studied in detail, such as in terms of specific coping strategies.
Our findings among a sample of low-SES Danish patients who had recently been diagnosed
with chronic lung disease suggest, contrary to the findings from sociological studies, that
religiosity and spirituality is a relevant factor to Danes facing a serious health-related problem.
Beliefs in God or a spiritual power were prevalent in the present sample of patients and were
shown to be associated with QoL. Furthermore, religious coping strategies were prevalent,with negative religious coping being significantly associated with lower QoL after controlling
for sociodemographic variables associated with QoL. A small group reported having more
existential, spiritual, and religious thoughts after diagnosis, but very few were interested in
discussing existential or spiritual thoughts with a professional, and none were interested in
talking about religious thoughts with a professional. This result suggests the private characterof religion to Danes (Andersen & Riis, 2002). In the remaining part of the discussion, we
consider these findings in more detail.
Religious Beliefs
Beliefs in a transcendent power were prevalent, with more than half of the patients reportingbelief in God or a spiritual power. The present study differs from several previous studies by
distinguishing between belief in a personal God and belief in a spiritual power, showing that
whereas approximately one tenth of the patients reported a belief in a spiritual power only, more
patients (31.5%) reported a belief in a personal God. Some patients reported beliefs in both a
personal God and a spiritual power (23.4%). In the World Value Surveys 1999–2001, more thanone third (38.1%) of Danes reported to believe in a “spirit or life force” and 24.9% believed in a
“personal God.” One reason for the difference found between these results and the results from
our sample could be related to the age of the present sample. The mean age of our sample was
65 years compared to 45.8 years in the Value Surveys, and traditional theistic beliefs (beliefs
in an active, involved God) may be more prevalent among elderly people (Andersen, Ausker,& la Cour, 2011). Another reason could be that the concepts of “a personal God” and “spiritual
power” are not mutually exclusive. In contrast to the Value Surveys, patients in our study were
not forced to choose between the two constructs, and a significant group reported belief in
both. This finding suggests that Danes may hold more fuzzy concepts of the transcendent than
previously (Lüchau, 2005).

COPING AND QUALITY OF LIFE FOR LUNG PATIENTS 199
Existential Needs
The finding that only a minor proportion reported having a need to discuss existential and
spiritual thoughts with a professional, and none reported a need to discuss religious thoughts
with a professional, suggests that religion is considered a private matter among Danes. In
contrast, studies show that between 25% and 51% of Americans are willing to talk about reli-
gious, spiritual, and existential thoughts (Miller, Pittman, & Strong, 2003; Moadel et al., 1999)
and find it helpful to share their thoughts and feelings with professionals such as physicians(Kristeller, Rhodes, Cripe, & Sheets, 2005). The private nature of Danish religiousness may
leave those experiencing religious, spiritual, or existential struggles isolated with their thoughts.
Although the nature of our study did not allow for exploring this aspect further, it would be
interesting in future studies to investigate whether this has any bearing on patients’ illness
adjustment and QoL.
Religious Coping
The relatively high percentage of patients that reportedly used religious coping at least to some
degree challenges the assertion that religious beliefs are not salient among people from secular
societies and is more consistent with the hypothesis that crisis may “mobilize” religious coping
strategies. Although less prevalent than positive religious coping, the key question here is why
Danes express religious struggles, if religion is a nonissue for them as suggested by Zuckerman(2008). We suggest, given the age of the present sample, that a large proportion could have
experienced some kind of religious socialization through baptism and confirmation as children
and that they therefore hold some traditional religious beliefs. However, these beliefs may
not have been differentiated, elaborated, and refined over their lifespan, partly because of the
secularization taking place in Danish society. Faced with a life-threatening crisis, these patientsmay have tried to mobilize religious resources that remained undeveloped. As a result, their
religion may have become a source of struggle rather than a source of support and comfort. In
any case, it appears that religious issues are not irrelevant in this secular society; in contrast
they appear to remain salient to Danes in times of great urgency.
Religious Coping and Quality of Life
Previous studies have shown that elderly people, women, and people who lack secular resourcessuch as money and education are especially likely to use religious coping and gain benefits from
it (Pargament, 1997). Consistent with these findings, we hypothesized that positive religious
coping would be associated with better QoL in this sample of elderly, low-SES patients.
However, positive religious coping did not explain any of the variance in QoL. There are a few
possible explanations for this finding. First, the level of positive religious coping in this samplewas lower than that of medical patients in the United States (Pargament, Koenig, Tarakeshwar,
& Hahn, 2004). Danish patients may not rely on religious resources to the same extent that
Americans do, perhaps because most Danes enjoy a relatively high living standard. Second, as
previously noted, it is also possible that the positive religious coping methods are less effective
because they are less deeply grounded in the individual’s repertoire of resources and orientation

200 PEDERSEN ET AL.
to the world. Finally, the lack of links between positive religious coping and QoL could reflect
the religious coping mobilization effect (Pargament, 1997). That is, in cross-sectional studies,the positive effect of religion on QoL could be counterbalanced and washed out by mobilization
of religious coping by the distress associated with a poorer QoL. Longitudinal studies are
needed to identify whether religious coping mobilization is taking place.
In contrast to the findings involving positive religious coping, negative religious coping was,
as predicted, associated with lower QoL. The findings suggest that religious struggles, thoughnot as prevalent as positive religious coping, may still have implications for well-being even
among people in highly secularized societies. Multiple comparison analyses suggested that
especially patients believing only in a spiritual power scored significantly lower on QoL than
people believing in God. Furthermore, there was a tendency for this group to score higher on
negative religious coping than God-believing patients. We do not know the nature of the beliefs
of those who believed only in a spiritual power, but apparently these beliefs are associatedwith nontraditional spiritual beliefs and behaviors as this group showed lower levels of private
religious activity (such as prayer), showed lower levels of public religious activity (such as
church attendance), and received little support from fellow believers (congregational members)
when compared to patients with belief in God. It is likely that when crisis strikes, these beliefs
are challenged, resulting in spiritual struggles that may be causing lower QoL. People holdingnontraditional spiritual beliefs and not receiving social support from fellow believers may be
left to fend for themselves in their efforts to resolve their existential and spiritual struggles.
If Danish society does indeed become more secularized, it is possible that spiritual struggles
will increasingly become commonplace among patients dealing with life-threatening diseases as
their religious belief systems becomes more fragmentized, less integrated, and less helpful. Asreligious upbringing becomes less common among younger generations (Ausker & Mørk, 2007)
younger patients in secular societies may become more vulnerable to spiritual struggles because
they lack concepts and language to deal with existential, religious, and spiritual questions
(la Cour, 2008) and as a result grasp for whatever existential, spiritual, or religious meaning-
making systems (Park, 2005) they believe may help them cope. The question is whether they
will succeed in constructing a new system of religious or spiritual meaning or whether theirstruggles will lead to frustration, confusion, and despair. The topic of spiritual struggles seems
ripe for further empirical study. Health professionals should also consider how they might assist
in the prevention and resolution of existential, spiritual or religious struggles.
Limitations
This study is one of the first to explore religious coping among medical samples in Denmark.
However, a number of limitations should be noted. First, the sample represents elderly, low-SES
lung disease patients from Denmark. It is unclear whether the findings will generalize to other
patient groups, Danish or otherwise. Second, the study had a low response rate, likely due atleast in part to the severity of the illness these patients were experiencing. Unfortunately, it was
not possible to explore this further, as information about the health condition of nonresponders
was not available to us. The low response rate could also reflect the reluctance among many
Danes to discuss religious issues. Therefore, the sample might have an overrepresentation
of religiously oriented patients. Third, the study used a cross-sectional design. As a result,
important questions about causal relationships cannot be determined. Fourth, the Brief RCOPE
COPING AND QUALITY OF LIFE FOR LUNG PATIENTS 201
seemed to apply to subgroups of patients identifying themselves as “believing” and “spiritual.”
However, it is likely that other spiritual and existential coping strategies are also prevalentamong Danish patients. It could be important, especially among younger patient groups, to
consider other scales or develop new items covering more spiritual and existential ways of
coping (Ahmadi, 2006).
Conclusions
Despite the limitations noted previously, the results of the present study challenge the notionthat religion and spirituality are unimportant to patients in secular societies. The sample
reported widespread beliefs in God or a spiritual power, which in turn were associated with
QoL. Furthermore, religious coping appeared to be prevalent. Negative religious coping, in
particular, was found associated with poorer QoL. These findings underscore the potential
risk of religious struggles for the QoL of patients, particularly those holding nontraditionalspiritual beliefs. Although the majority of patients were not interested in talking about reli-
gious, spiritual, or existential thoughts with professionals, patients—especially those undergoing
religious struggles—could perhaps benefit from increased attention to these matters from health
professionals.
ACKNOWLEDGMENTS
The project was supported by the Danish Knowledge and Research Centre of Complementary
and Alternative Medicine (ViFAB) in collaboration with Center for Cross-Scientific Evaluation
Studies on Complementary and Alternative Medicine (CCESCAM) at University of SouthernDenmark and Aarhus University as well as a stipend from Aarhus University.
REFERENCES
Ahmadi, F. (2006). Culture, religion and spirituality in coping. The example of cancer patients in Sweden. Uppsala:
Acta Universitatis Upsaliensis.
Andersen, P. B., Ausker, N. H., & la Cour, P. (2011). Går fanden i kloster, når han bliver gammel? In P. Gundelach
(Ed.), Små og store forandringer. Danskernes værdier siden 1981 (pp. 97–113). Copenhagen,Denmark: Hans Reitzels
Forlag.
Andersen, P. B., & Riis, O. (2002). Religionen bliver privat. In P. Gundelach (Ed.), Danskernes værdier 1981–1999
(pp. 76–98). Copenhagen, Denmark: Hans Reitzels Forlag.
Ano, G. G., & Vasconcelles, E. B. (2005). Religious coping and psychological adjustment to stress: A meta-analysis.
Journal of Clinical Psychology, 61, 461–480.
Ausker, N. H., & Mørk, L. (2007). Trosfaktoren—Hvad siger patienterne? Tidsskrift for Sjelesorg, 2, 126–139.
Cella, D. F., Tulsky, D. S., Gray, G., Sarafian, B., Linn, E., Bonomi, A., : : : Brannon, J. (1993). The functional
assessment of cancer therapy scale: Development and validation of the general measure. Journal of Clinical Oncology,
11, 570–579.
Charlson, M. E., Pompei, P., Ales, K. L., & MacKenzie, C. R. (1987). A new method of classifying prognostic
comorbidity in longitudinal studies: Development and validation. Journal of Chronic Diseases, 40, 373–383.
Christensen, S., Zachariae, R., Jensen, A., Vaeth, M., Møller, S., Ravnsbaek, J., & von der Maase, H. (2009). Prevalence
and risk of depressive symptoms 3–4 months post-surgery in a nationwide cohort study of Danish women treated
for early stage breast-cancer. Breast Cancer Research and Treatment, 113, 339–355.
202 PEDERSEN ET AL.
Cobb, M., Puchalski, C., & Rumbold, B. (Eds.). (2012). Oxford textbook of spirituality in healthcare. Oxford, UK:
Oxford University Press.
Exline, J. J., & Rose, E. D. (2013). Religious and spiritual struggles. In R. F. Paloutzian & C. L. Park (Eds.), Handbook
of the psychology of religion and spirituality, 2nd ed. (pp. 380–398). New York, NY: Guilford.
Gall, T. L., Kristjansson, E., Charbonneau, C., & Florack, P. (2009). A longitudinal study on the role of spirituality in
response to the diagnosis and treatment of breast cancer. Journal of Behavioral Medicine, 32, 174–186.
Hill, P. C. (2013). Measurement assessment and issues in the psychology of religion and spirituality. In R. F. Paloutzian
& C. L. Park (Eds.), Handbook of the psychology of religion and spirituality, 2nd ed. (pp. 48–74). New York, NY:
Guilford.
Hills, J., Paice, A., Cameron, J. R., & Shott, S. (2005). Spirituality and distress in palliative care consultation. Journal
of Palliative Medicine, 8, 782–788.
Hill, P. C., & Pargament, K. I. (2003). Advances in the conceptualization and measurement of religion and spirituality.
Implications for physical and mental health research. American Psychologist, 51, 64–74.
Højsgaard, M. T., & Ravn Iversen, H. (2005). Gudstro i Danmark [Godbelief in Denmark]. Frederiksberg, Denmark:
Anis.
Koenig, H. G., King, D. E., & Carson, V. B. (2012). Handbook of religion and health (2nd ed.) New York, NY: Oxford
University Press.
Koenig, H., Pargament, K. I., & Nielsen, J. (1998). Religious coping and health status in medically ill hospitalized
older adults. The Journal of Nervous and Mental Disease, 186, 513–521.
Kristeller, J. L., Rhodes, M., Cripe, L. D., & Sheets, V. (2005). Oncologist assisted spiritual interventions study
(OASIS): Patient acceptability and initial evidence of effects. International Journal of Psychiatry in Medicine, 35,
329–347.
Krupski, T. L., Kwan, L., Arlene, F., Sonn, G. A., Malinski, S., & Litwin, M. S. (2006). Spirituality influences health
related quality of life in men with prostate cancer. Psycho-oncology, 15, 121–131.
la Cour, P. (2005). Danskernes Gud i krise [The Danes’ God in crisis]. In M. T. Højsgaard & H. R. Iversen (Eds.),
Gudstro i Danmark [Godbelief in Denmark]. (pp. 59–82). Copenhagen, Denmark: Anis.
la Cour, P. (2008). Existential and religious issues when admitted to hospital in a secular society: Patterns of change.
Mental Health, Religion and Culture, 11, 769–782.
Lazarus, R. S., & Folkman, S. (1984). Stress, appraisal, and coping. New York, NY: Springer.
Lüchau, P. (2005). Danskernes gudstro siden 1940’erne [Godbelief among Danes since 1940]. In M. T. Højsgaard &
H. R. Iversen (Eds.), Gudstro i Danmark [Godbelief in Denmark]. (pp. 31–58). Copenhagen, Denmark: Anis.
Masters, K. S., & Hooker, S. A. (2013). Religion, spirituality, and health. In R. F. Paloutzian & C. L. Park (Eds.),
Handbook of the psychology of religion and spirituality, 2nd ed. (pp. 519–539). New York, NY: Guilford.
McCullough, M. E., Hoyt, W. T., Larson, D. B., Koenig, H. G., & Thoresen, C. (2002). Religious involvement and
mortality: A meta-analytic review. Health Psychology, 19, 211–222.
Miller, B. E., Pittman, B., & Strong, C. (2003). Gynecologic cancer patients’ psychosocial needs and their views on
the physician’s role in meeting those needs. International Journal of Gynecologic Cancer, 13, 111–119.
Moadel, A., Morgan, C., Fatone, A., Grennan, J., Carter, J., Laruffa, G., : : : Dutcher, J. (1999). Seeking meaning and
hope: Self-reported spiritual and existential needs among an ethnically-diverse cancer patient population. Psycho-
oncology, 8, 378–385.
Mytko, J. J., & Knight, S. J. (1999). Body, mind and spirit: Towards the integration of religiosity and spirituality in
cancer quality of life research. Psycho-oncology, 8, 439–450.
Organisation for Economic Co-operation and Development. (2009). Poverty. In OECD, Society at a Glance 2009:
OECD Social Indicators. Paris, France: OECD Publishing. doi:10.1787/soc_glance-2008-17-en
Paloutzian, R. F., & Park, C. L. (2013). Recent progress and core issues in the science of the psychology of religion
and spirituality. In R. F. Paloutzian & C. L. Park (Eds.), Handbook of the psychology of religion and spirituality,
2nd ed. (pp. 3–22). New York, NY: Guilford.
Pargament, K. I. (1997). The psychology of religion and coping. Theory, research, practice. New York, NY: Guilford.
Pargament, K. I. (2007). Spiritually integrated psychotherapy. Understanding and addressing the sacred. New York,
NY: Guilford.
Pargament, K. I., Koenig, H. G., Tarakeswar, N., & Hahn, J. (2001). Religious struggle as a predictor of mortality
among medically ill elderly patients: A two year longitudinal study. Archives of Internal Medicine, 161, 1881–1885.
Pargament, K. I., Koenig, H. G., Tarakeswar, N., & Hahn, J. (2004). Religious coping methods as predictors of
psychological, physical and spiritual outcomes among medically ill elderly patients: A two-year longitudinal study.
Journal of Health Psychology, 9, 713–730.

COPING AND QUALITY OF LIFE FOR LUNG PATIENTS 203
Pargament, K. I., Smith, B. W., Koenig, H. G., & Perez, L. (1998). Patterns of positive and negative religious coping
with major life stressors. Journal of the Scientific Study of Religion, 37, 710–724.
Park, C. L. (2005). Religion and meaning. In R. F. Paloutzian & C. L. Park (Eds.), Handbook of the psychology of
religion and spirituality (pp. 295–314). New York, NY: Guilford.
Park, C. L., & Paloutzian, R. F. (2013). Directions for the future of the psychology of religion and spirituality: Research
advances in methodology and meaning systems. In R. F. Paloutzian & C. L. Park (Eds.), Handbook of the psychology
of religion and spirituality, 2nd ed. (pp. 651–665). New York, NY: Guilford.
Pedersen (2009). Complementary and alternative medicine among cancer patients. Prevalence, user characteristics,
and effectiveness for well-being. Ph.D. dissertation, Aarhus University.
Peterman, A. H., Fitchett, G., Brady, M. J., Pharm, L. H., & Cella, D. (2002). Measuring spiritual well-being in patients
with cancer: The functional assessment of chronic illness therapy–spiritual well-being scale (FACIT-Sp). Annals of
Behavioral Medicine, 24, 49–58.
Salander, P. (2006). Who needs the concept of spirituality? Psycho-oncology, 15, 647–649.
Schafer, J. L., & Graham, J. W. (2002). Missing data: Our view of the state of the art. Psychological Methods, 7,
147–177.
Sherman, A. C., Simonton, S., Latif, U., Spohn, R., & Tricot, G. (2005). Religious struggle and religious comfort
in response to illness: Health outcomes among stem cell transplant patients. Journal of Behavioral Medicine, 28,
359–367.
Stefanek, M., McDonald, P. G., & Hess, S. A. (2005). Religion, spirituality and cancer: Current status and method-
ological challenges. Psycho-oncology, 14, 450–463.
Storm, I. (2009). Halfway to heaven: Four types of fuzzy fidelity in Europe. Journal for the Scientific Study of Religion,
48, 702–718.
Voas, D. (2009). The rise and fall of fuzzy fidelity in Europe. European Sociological Review, 25, 155–168.
World Value Surveys 1999–2001. Data were available by the Danish Data Archive (archive number DD-214332)
Zuckerman, P. (2008). Society without God. What the least religious nations can tell us about contentment. New York,
NY: NYU Press.
Zwingmann, C., Wirtz, M., Müller, C., Körber, J., & Murken, S. (2006). Positive and negative religious coping in
German breast cancer patients. Journal of Behavioral Medicine, 29, 533–547.
Paper 2

© 2013 Koninklijke Brill NV ISBN 978-90-04-25205-9
Research in the SocialScientifijic Study of Religion
Volume 24
Edited by
Ralph L. PiedmontLoyola University Maryland
andAndrew Village
York St. John University, UK
LEIDEN •• BOSTON2013

© 2013 Koninklijke Brill NV ISBN 978-90-04-25205-9
CONTENTS
Preface ................................................................................................................ viiAcknowledgements ........................................................................................ ixManuscript Invitation .................................................................................... xi
The Revised Faith Development Scale: An Option for a More Reliable Self-Report Measurement of Postconventional Religious Reasoning ................................................................................. 1
J. Irene Harris and Gary K. Leak
Spirituality’s Unique Role in Positive Afffect, Satisfaction with Life, and Forgiveness over and above Personality and Individualism-Collectivism ............................................................. 15
Inna Reddy Edara
SPECIAL SECTION
RESTORING THE TEMPLE: RELIGIOUSNESS, SPIRITUALITY, AND HEALTH
Restoring the Temple: Religiousness, Spirituality, and Health .......... 45 Gina Magyar-Russell
Forgiveness, Religiousness, Spirituality, and Health in People with Physical Challenges: A Review and a Model ........................... 53
Caroline R. Lavelock, Brandon J. Grifffijin, and Everett L. Worthington, Jr.
Religious and Spiritual Appraisals and Coping Strategies among Patients in Medical Rehabilitation ....................................................... 93
Gina Magyar-Russell, Kenneth I. Pargament, Kelly M. Trevino, and Jack E. Sherman
The Relationship of Spirituality, Benefijit Finding, and Other Psychosocial Variables to the Hormone Oxytocin in HIV/AIDS ................................................................................................. 137
Courtney B. Kelsch, Gail Ironson, Angela Szeto, Heidemarie Kremer, Neil Schneiderman, and Armando J. Mendez

© 2013 Koninklijke Brill NV ISBN 978-90-04-25205-9
contents iii
Coping Without Religion? Religious Coping, Quality of Life, and Existential Well-Being among Lung Disease Patients and Matched Controls in a Secular Society ....................................... 163
Heidi Frølund Pedersen, Christina G. Pedersen, Kenneth I. Pargament, and Robert Zachariae
Magic and Jinn among Bangladeshis in the United Kingdom Sufffering from Physical and Mental Health Problems: Controlling the Uncontrollable ............................................................. 193
Simon Dein
Spirituality, Faith, and Mild Alzheimer’s Disease ................................. 221 Jocelyn Shealy McGee, Dennis R. Myers, Holly Carlson,
Angela Pool Funai, and Paul A. Barclay
Spiritual Struggles, Health-Related Quality of Life, and Mental Health Outcomes in Urban Adolescents with Asthma .................. 259
Sian Cotton, Kenneth I. Pargament, Jerren C. Weekes, Meghan E. McGrady, Daniel Grossoehme, Christina M. Luberto, Anthony C. Leonard, and George Fitchett
Testing the Validity of a Protocol to Screen for Spiritual Struggle among Parents of Children with Cystic Fibrosis .............................. 281
Daniel H. Grossoehme and George Fitchett
Winding Road: Preliminary Support for a Spiritually Integrated Intervention Addressing College Students’ Spiritual Struggles ... 309
Carmen K. Oemig Dworsky, Kenneth I. Pargament, Meryl Reist Gibbel, Elizabeth J. Krumrei, Carol Ann Faigin, Maria R. Gear Haugen, Kavita M. Desai, Shauna K. Lauricella, Quinten Lynn, and Heidi L. Warner
Authors’ Biographies ...................................................................................... 341Manuscript Reviewers ................................................................................... 351Subject Index .................................................................................................... 353Author Index .................................................................................................... 358

© 2013 Koninklijke Brill NV ISBN 978-90-04-25205-9
Research in the Social Scientifijic Study of Religion, Volume 24© Koninklijke Brill NV, Leiden, 2013
COPING WITHOUT RELIGION? RELIGIOUS COPING, QUALITY OF LIFE, AND EXISTENTIAL WELL-BEING AMONG LUNG DISEASE PATIENTS AND MATCHED CONTROLS IN A SECULAR SOCIETY
Heidi Frølund Pedersen, Christina G. Pedersen, Kenneth I. Pargament, and Robert Zachariae*
Abstract
The present study examined religious coping following negative life events among three groups of participants in Denmark: severely ill lung disease patients (n = 111), individuals facing other negative life events (n = 91), and a healthy control group (n = 246) matched on age, gender, education, and region. The aims of the study were to explore the degree to which major life stressors mobilize greater levels of religiousness in a secular society like Denmark, the types of religious behaviors and coping strategies employed (if any), and the associations between religious coping and well-being among the participant groups. While we found no diffferences in the level of general religious activities between groups, lung disease patients reported greater use of positive religious coping than the control group, especially asking forgiveness and religious meaning-making. Hierarchical regression analy-ses indicated that negative religious coping was signifijicantly associated with poorer overall quality of life (QoL) among lung disease patients (β = .19, p < 0.01), whereas congregational support was associated with better QoL (β = .20, p < 0.01) and existential well-being (β = .19, p < 0.01) in the control group. Positive religious coping was not associated with well-being measures in any of the groups. The results suggest that despite secularization, religion continues to be a relevant factor among Danes, particularly for those facing severe illness. The practical implications of these fijindings for health care are considered.
Keywords: Lung disease, negative life events, religiousness, religious coping, quality of life, existential well-being, secular
* Authors Note: Heidi F. Pedersen, Unit for Psycho-Oncology and Health Psychology, Department of Psychology, Aarhus University; Christina G. Pedersen, Unit for Psycho-Oncology and Health Psychology, Department of Psychology, Aarhus University; Kenneth I. Pargament, Bowling Green State University; Robert Zachariae, Unit for Psycho-Oncology and Health Psychology, and Department of Oncology, Aarhus University Hospital.
The project was supported by the Danish Knowledge and Research Centre of Com-plementary and Alternative Medicine (ViFAB) in collaboration with Center for Cross-Scientifijic Evaluation Studies on Complementary and Alternative Medicine (CCESCAM) at University of Southern Denmark and Aarhus University as well as a stipend from Aarhus University.
Correspondence concerning this article should be addressed to Heidi Frølund Pedersen, Department of Psychology, Aarhus University, 8000 Aarhus C, Denmark. E-mail: [email protected]

164 heidi frølund pedersen et al.
© 2013 Koninklijke Brill NV ISBN 978-90-04-25205-9
The idea that negative life events such as life threatening illness, accidents, or bereavement elicit religiosity or faith in something greater than man-kind is well-known and reflected in the famous saying: “There are no athe-ists in foxholes.” Although this maxim may be overstated, studies in the United States (US) have shown higher levels of religiousness among peo-ple facing life and death situations (Pargament, 1997). Life crises appear to mobilize religious and spiritual resources, and psychological theories sug-gest that this phenomenon may stem from a need to reduce death anxiety by afffording a sense of psychological security and the hope of immortal-ity (Vail et al., 2010). Specifijically, according to terror management theory (Greenberg, Pyszczynski, & Solomon, 1986), reminders of human mortal-ity make people engage in their own cultural world views and values to enhance self-esteem and deal with existential concerns. Religious and spiritual ideas are more appealing in this situation because they affford lit-eral immortality, as opposed to secular ideas of symbolic immortality like making major contributions to the cultural society that will persist after one’s demise or, more modestly, living on through the next generation. Experimental psychology has provided some evidence that religion may be more appealing when reminded about death, even among non-religious people. In a study by Jong, Halberstadt, and Bluemke (2012), explicit mea-sures (questionnaires) as well as implicit measures (single-target Implicit Association Test) were applied to test how thoughts of death influence belief in supernatural agents. Participants were instructed to categorize a series of nouns as real or imaginary (including religious concepts as God, Angel, Heaven) as quickly as possible. Hesitations in categorizing religious concepts as imaginary among non-believers in the death priming condi-tion were interpreted as signs of implicit religiosity caused by mortality salience. The study showed that participants explicitly defended their own worldviews; religious participants were more confijident that supernatural beings exist, whereas non-religious participants were more confijident that they do not. However, when measured implicitly, death priming increased beliefs in religious supernatural entities among all participants, regardless of their prior religious or non-religious worldviews.
Religion may serve other important functions in times of stress besides being a bufffer against death anxiety. In this vein, Pargament (1997) sug-gested that religion may serve multiple purposes among people cop-ing with major life events, including fijinding comfort and support from a higher being and obtaining social support from a religious or spiritual community. Religion can also function as a way of gaining control, either

coping without religion? 165
© 2013 Koninklijke Brill NV ISBN 978-90-04-25205-9
by attributing the responsibility for a stressful event to a higher being or asking for strength to handle a situation. In addition, religion can func-tion as a source of personal transformation; non-religious people may convert to religion and change their lives, and religious people may refijine and expand their religious beliefs. Finally, religion may offfer a framework for meaning-making. These functions may become especially signifijicant when people confront stressful events that shatter their worldviews and reveal their fundamental frailty, such as loss, serious illness, or accidents (Janofff-Bulman, 1992). Questions remain, however, about the generaliz-ability of this theory and research to other contexts.
Scandinavian societies like Denmark are considered to be among the most secularized in the world (Zuckerman, 2008). Although nearly 80% of Danes are members of the National Lutheran Church (Statistics Denmark, 2012), only 2% attend church on a weekly basis (Højsgaard & Iversen, 2005) as opposed to 43.1% of Americans (Gallup Daily Tracking, 2008–2010), and some have suggested that religion is a non-issue among Danes (Zuckerman, 2008). A few studies have explored the prevalence of religiosity among medically ill patients in Denmark, and their results indi-cate that medical patients are more religiously oriented than the general population (Andersen, Ausker, & la Cour, 2011; Ausker, la Cour, Busch, Nabe-Nielsen, Pedersen, 2008; Pedersen, 2009). The frame of reference in these studies, however, was the general population as a whole; the samples were not specifijically matched with respect to demographic factors such as age and gender, which have been found to be signifijicant predictors of religiosity (The Danish Value Survey, 2008; Pew Research Center, 2008).
Given this background, we explored whether individuals reporting a wide range of major negative events and life-threatened individuals, namely lung disease patients, are more likely to report religious coping when compared to a healthy control group matched on age, gender, and education level reporting no negative events. The aim was to test the hypothesis that negative life events, such as receiving a diagnosis of lung disease or grieving the death of a loved one, are more likely to elicit reli-gious activity and religious coping when compared to the coping activi-ties of individuals not confronted with major life events. Additionally, whether possible links between religion and well-being vary as a function of stressor type; that is, whether possible efffects of religious coping on well-being will be stronger among individuals reporting severe illness or negative events, were also explored.

166 heidi frølund pedersen et al.
© 2013 Koninklijke Brill NV ISBN 978-90-04-25205-9
Positive and Negative Methods of Religious Coping
Although religion is most often thought of in positive terms as afffording comfort and hope, anthropological studies have also suggested that reli-gion may often be far from comforting. One example is the Calvinist belief that God pre-determines souls to salvation or damnation (Thuesen, 2009). Thus, religion may be a double-edged sword depending on the religious worldviews available to the individual (Schaie, Krause, & Booth, 2004). Accordingly, research has identifijied both positive and negative religious coping strategies (Pargament, Koenig, & Perez, 2000). Positive religious coping can be viewed as reflecting a secure relationship with God, a spir-itual connectedness with others, and a belief in life as being generally meaningful. In contrast, negative religious coping, or religious or spiri-tual struggle, is defijined as an expression of spiritual conflicts and doubts in one’s religious beliefs, relation with the divine, and connections with other people (Pargament, Murray-Swank, Magyar, & Ano, 2005). Studies of negative religious coping suggest that people are more likely to experi-ence anger towards God when their worldview is shattered and when God is held responsible for a negative event (Exline, Park, Smyth, & Carey, 2011). Furthermore, it is argued that religious beliefs that are not coherent and well-integrated in a person’s belief system may be more easily shat-tered and become a potential source of struggle (Pargament, 2007). Much of the research showing that religiousness is mobilized in stressful times has focused on positive forms of religious coping. Less clear is whether stressful situations are more likely to produce negative religious coping or religious struggles.
Religious Coping and Well-Being
Studies of religious coping and health suggest that positive and negative religious coping strategies impact well-being and adjustment diffferently. Positive religious coping has generally been associated with positive out-comes in terms of better quality of life (QoL), existential well-being, and better adjustment among a variety of diseases (Ano & Vasconcelles, 2005). It is here important to note that some studies fijind limited or no associa-tions (Hebert, Zdaniuk, Schulz, & Scheier, 2009; Schreiber & Brockopp, 2012) and others have found negative associations (Hills, Paice, Cameron, & Shott, 2005). Conversely, negative religious coping, although less preva-lent than positive religious coping (Meisenhelder & Marcum, 2004), has

coping without religion? 167
© 2013 Koninklijke Brill NV ISBN 978-90-04-25205-9
been robustly tied to poorer physical and mental health in many popula-tions (Ano & Vasconcelles, 2005), including lower levels of quality of life and existential well-being among cancer patients (Delgado-Guay et al., 2011; Tarakeshwar et al., 2006) and poorer emotional regulation among the bereaved (Lee, Roberts, & Gibbons, 2012). Furthermore, longitudinal studies have found associations between chronic religious struggles and increased distress (Hebert et al., 2009; Sherman, Plante, Simonton, Latif, & Anaissie, 2009) and mortality among severely ill patients (Pargament, Koenig, Tarakeshwar, & Hahn, 2001).
Furthermore, several studies have suggested that the relationships between religiousness and indices of well-being and distress are stronger among people dealing with major life stressors, such as medical illness (see Cummings & Pargament, 2010). For example, in a national survey of adults in the US, reports of spiritual struggles were found to be associated with a variety of indicators of psychopathology, and these relationships were signifijicantly stronger among people facing medical illnesses (McCo-nnell, Pargament, Ellison, & Flannelly, 2006).
The Present Study
The studies reviewed above have largely been conducted in societies that are generally thought to be more religiously oriented than the Scandi-navian counties, such as the United States (Zuckerman, 2008). Little is therefore known about associations between religious coping and QoL and existential well-being in more secular societies such as Denmark. Perhaps religion is not a source of spiritual support or a framework for meaning-making in secular societies. On the other hand, religion may continue to be a positive resource, and sometimes a source of existen-tial and religious struggle, when people encounter signifijicant stressors, even in more secularized countries. The present study, therefore, focused on three questions: (a) Do major life stressors mobilize greater levels of religiousness in a secular society like Denmark? (b) What types of reli-gious coping strategies do Danes facing major negative life events employ, if any, and do these strategies difffer from those used by people who do not face negative life challenges? (c) Is religiousness associated with well-being, particularly in times of stress, among people in Denmark?
Specifijically, in the present study, we compared the prevalence of religiosity and religious coping in: (a) a group of lung disease patients, (b) a matched group of participants who reported a negative life event(s)

168 heidi frølund pedersen et al.
© 2013 Koninklijke Brill NV ISBN 978-90-04-25205-9
during the last 12 months (the negative events group), and (c) a control group of participants who did not report a negative life event during the past 12 months (the control group). We also explored whether the associa-tions between positive and negative religious coping and QoL and exis-tential well-being varied as a function of the stressor.
It was hypothesized that severely ill lung disease patients and the nega-tive events group would report higher levels of public and private religious activity as well as both more positive and negative religious coping than the control group. In addition, based on theory and previous fijindings, we hypothesized that higher levels of positive religious coping would be asso-ciated with higher overall QoL and existential well-being among patients and participants dealing with negative life events, in comparison to those reporting no negative life events. We also hypothesized that higher levels of negative religious coping would be associated with lower levels of over-all QoL and existential well-being.
Methods
Procedure
The lung disease participant group was recruited from fijive respiratory medicine clinics (four on the main peninsula of Jutland and one at an island in the eastern part of Denmark). From October 2008 to Octo-ber 2010, patients diagnosed with severe and chronic lung disease were informed about the study by the medical stafff and asked to give their informed consent to participate. Patients were asked to complete the questionnaire shortly after their diagnosis and return it to the research team by mail. Those who did not return the questionnaire within 2 weeks received a single reminder. In all, 514 received the questionnaire, and 120 responded (response rate: 23.4%). Nine patients were excluded because of insufffijicient data, resulting in a fijinal sample of 111 lung disease patients. The project was evaluated by the Committee on Biomedical Research Ethics in Denmark.
The control group was established by Statistics Denmark, a government agency that has access to a range of national registries such as the Cen-tral Person Registry (CPR). All Danish residents are given a CPR number, enabling retrieval of information for research purposes. In all, 11 individu-als per patient matched on age, gender, education level, and region were selected from the CPR. The resulting group of 1,437 potential participants received a questionnaire during March 2010 and was asked to complete

coping without religion? 169
© 2013 Koninklijke Brill NV ISBN 978-90-04-25205-9
and return the questionnaire. Those who did not return the question-naire within 2 weeks were mailed a single reminder. In all, 498 responded (response rate = 34.7%). Of these, 45 were excluded due to insufffijicient data, 116 were excluded due to reporting serious illness such as heart dis-ease, cancer, AIDS, diabetes, liver, and lung diseases, resulting in a fijinal sample of 337 matched control participants.
The present study was part of a larger study focusing on the use of complementary and alternative medicine (CAM) and religiosity among Danish chronically ill lung disease patients.
Measures
Socio-demographic informationSocio-demographic information included: age, gender, marital status (dichotomized into married/cohabiting and widowed/ divorced/ single), number of children, highest education level (dichotomized into Low edu-cation = 7–10 years and High education = > 10 years), current work situ-ation (dummy coded into Unemployed/sick leave, Retired, and Working part- or full-time), and socio-economical status (annual house income).
Medical informationAn adapted version of the Charlson Co-morbidity Index (Charlson, Pom-pei, Ales & MacKenzei, 1987; Christensen et al., 2009) was used to assess self-reported co-morbidity in the patient and control groups. Information on lung disease patients’ diagnosis was retrieved from the Danish Lung Cancer Registry (www.lungecancer.dk) and from the records of the par-ticipating respiratory medical clinics.
Negative life eventsAn adjusted version of the List of Recent Events (LRE) (Henderson, Byrne, & Duncan-Jones, 1981) was used to access the presence and psychological impact of major life events during the last 12 months among control par-ticipants covering: (a) illness, injury, and accident, (b) bereavement, (c) pregnancy or abortion, (d) changes in relationships, (e) living conditions, (f) education, (g) employment, and (h) fijinances and legal difffijiculties. We excluded the category of pregnancy or abortion, as this item did not seem relevant to this sample due to the mean age of the participants. The response format on the question “Have you within the past 12 months experienced [event]?” was Yes or No for each event. For the items “Illness, injury, and accident” and “Bereavement,” the question was formulated:

170 heidi frølund pedersen et al.
© 2013 Koninklijke Brill NV ISBN 978-90-04-25205-9
“Have you or one of your closest relatives experienced [event]?” For each event, participants were asked to indicate to what degree this event had a negative influence on their QoL on a 5-point Likert scale from 1: (Not at all) to 5: (Very much). Events that were rated higher than 2 were catego-rized as “Negative events.”
Health related quality-of-life (QoL)A Danish version of the Functional Assessment of Cancer Therapy Scale, FACT-G (Cella et al., 1993) was used to measure overall health-related QoL among lung disease patients. The FACT-G is a standardized ques-tionnaire developed for cancer research and consists of 30 items cover-ing the patients’ physical, emotional, social, and functional well-being (“I feel sick,” “I feel nervous,” “I sleep well”). The wording was changed from “cancer” to the broader term “lung disease.” Responses are given on a 5-point Likert scale ranging from 0 (Not at all) to 4 (Very much). The four subscales are computed into one total score. In the present samples, the internal consistency (Cronbach’s alpha) of the overall QoL score among lung disease patients was 0.92 and ranged from 0.77 to 0.90 for the sub-scales. For control participants, the overall QoL score was 0.87 and ranged from 0.74 to 0.86 for the subscales.
Existential well-beingExistential well-being was measured using the FACIT-Sp (Peterman, Fitch-ett, Brady, Pharm, & Cella, 2002), a 12-item questionnaire covering the patients’ sense of meaning, purpose, and peace in life and ability to fijind comfort in spiritual convictions during illness (“I feel peace,” “I fijind com-fort in my spiritual beliefs”). Responses are given on a 5-point Likert scale ranging from 0 (Not at all) to 4 (Very Much). A total score is calculated by summing the scores of each item. The internal consistency for existential well-being was 0.86 among lung disease patients and 0.82 for control par-ticipants. Participants in the control group were given an adjusted version of the FACT-G and the FACIT-Sp without items referring to lung disease, and total scores were calculated in accordance with scoring guidelines from the FACT-G in order to be able to compare the scores of the two independent groups (Brucker, Yost, Cashy, Webster, & Cella, 2005).
Religious behaviorPublic religious behavior was measured by a single item about church attendance and/or attendance at other religious meetings: “How often do you attend church or other religious services?” Private religious behavior

coping without religion? 171
© 2013 Koninklijke Brill NV ISBN 978-90-04-25205-9
was measured by a single item about the frequency of prayer, meditation, and/or Scripture readings: “How often do you engage in religious activi-ties like prayer, meditation, or Scripture reading?” Response options to these two measures were 5-point Likert scales ranging from 1 (Never) to 5 (Every day).
Congregational supportCongregational support was measured by a single item: “To what degree do you receive support from your fellow believers” on a 5-point Likert scale with response options ranging from 1 (Not at all) to 5 (A great deal) for lung disease patients, and the format 2 (Yes), 1 (No), or 0 (Not relevant) for control participants. The score was then dichotomized into 1 (Congre-gational support; 2–5 among the lung disease group, and 2 among negative events group and the control group) and 0 (No support; 1 for lung disease group, and 1 and 0 for negative events group and the control group).
Religious copingPositive and negative religious coping was measured by a revised version of the Brief RCOPE (Pargament, Smith, Koenig & Perez, 1998), a 14-item measure with two subscales: Positive religious coping which measures the degree to which the patients cope with illness by looking to God for com-fort and support (“Looked for a stronger connection with God”) and Nega-tive religious coping which measures the degree individuals interpret their illness as a punishment or abandonment by God (“Wondered whether God had abandoned me”). The latter subscale is often referred to as reli-gious or spiritual struggle, because it reflects a religious system in tension or turmoil (Pargament et al., 2005). The response format is a 4-point Likert scale ranging from 0 (Not at all) to 3 (A great deal), and a total score is calculated for each subscale. The original Brief RCOPE assesses religious meaning-making only in the negative subscale (such as “Wonder why God is punishing me”). Thus, a new item was developed covering positive reli-gious meaning-making in the present study: “Thought God had a meaning with my illness/situation after all,” and another variable covering spiritual support was added: “God granted me the strength to handle my illness/situation.” Internal consistencies (Cronbach’s alpha) were 0.94 for the positive and 0.60 for the negative religious coping subscale in the present sample. Deleting the item “Questioned the power of God” resulted in a Cronbach’s alpha of 0.71 for negative religious coping which was done in the following analyses. An unpublished qualitative validation study of the Brief RCOPE conducted by the fijirst author suggested that non-religious

172 heidi frølund pedersen et al.
© 2013 Koninklijke Brill NV ISBN 978-90-04-25205-9
people and atheists often answer this last item “Questioned the power of God” with “Very much.” Not because they have religious struggles but simply because they want to declare their disbelief in God. On this back-ground, we chose to delete this item, although this particular item has been found to be one of the most commonly endorsed religious strug-gles among cardiac patients with symptoms of acute coronary syndrome (Magyar-Russell et al., submitted for publication) and among diabetic, congestive heart failure, and oncology patients (Fitchett et al., 2004) in the United States.
Thus, the fijinal measure consisted of 15 items covering positive and negative religious coping strategies. When answering the religious cop-ing items, the negative events group and the control group were asked to think of the most negative life event they reported and the lung disease group was asked to think about how their illness afffected them.
Statistical Analysis
Mean substitution was used to handle missing data on continuous vari-ables as suggested by Schafer and Graham (2002). This procedure is adequate and preferable to procedures such as list-wise deleting or scale mean substitution. One-way ANOVAs and Chi-square tests were applied to test any diffferences in socio-demographic information between the lung disease group, negative events group, and control group. Religious coping was positively skewed, and non-parametric as well as parametric tests were applied when appropriate. Kruskal Wallis and Chi-square tests were applied to test diffferences in religious coping between the lung dis-ease group, negative events group, and control group. Finally, hierarchal regression analyses were conducted to determine the associations between religious coping, overall QoL, and existential well-being, while adjusting for demographic, medical, and religious factors. To reduce the risk of over-fijitting, three independent regression models were conducted in order to determine which variables should be included in the fijinal regression. The fijirst model consisted of demographic variables: sex, age, marital status, number of kids, education, annual house income, current work situa-tion, and volunteer work. In order to reduce the risk of under-fijitting, the signifijicance level in the fijirst three independent regression models was set at p < 0.10, and variables statistically signifijicant at this level were car-ried forward to the next model testing influence of the following medi-cal factors: diagnosis and Charlson Co-morbidity Index scores and group membership (i.e., lung disease, negative events, or a control individual reporting no negative events). The statistically signifijicant variables in the

coping without religion? 173
© 2013 Koninklijke Brill NV ISBN 978-90-04-25205-9
second model were carried forward to the third model testing the role of religious factors: church attendance, prayer/meditation/Scripture read-ing, congregational support, and positive and negative religious coping. In the fijinal model, all variables that were signifijicant at level p < 0.10 in the previous three independent models were included. Furthermore, an interaction term was added testing possible interactions between group membership and the religious variables by centering the data and multi-plying group membership with the signifijicant religious variables from the previous regression models. The signifijicance level for the fijinal model was set at p < 0.05. All analyses were conducted using SPSS 19.
Results
Sample
The lung disease participant sample included 55.9% males between the ages 26 and 105 years (M = 65.2, SD = 10.2) newly diagnosed with chronic lung diseases; that is, lung cancer (39.1%) and COPD/other lung diseases like bronchiecstasia (60.9%). More than two thirds (68.5%) of the patients had less than 11 years of education, 72.7% were married, 67% were retired, and 39.4% reported an annual income below 35.700 USD, which accord-ing to Organisation for Economic Co-operation and Development (OECD) standards is perceived as relative poverty in Denmark (OECD, 2009).
The matched control sample (N = 337) included 50.7% males. Partici-pants were between 42 and 96 years of age (M = 67.6, SD = 9.7). Almost three quarters (74.2%) of the participants had fewer than 11 years of edu-cation, 78% were married, 70.9% were retired, and 21.5% reported an annual income below 35.700 USD, which according to OECD standards is perceived as relative poverty in Denmark (OECD, 2009). Thus, both sam-ples were considered relatively low socioeconomic status (SES). Detailed socio-demographic data were collected and are available from the author, but analyses indicated that these data did not relate to the outcomes on the key dependent measures and are not described further here.
Ninety-one control participants reported negative events (negative events group), with 47% of these reporting to have experienced seri-ous accidents or illness of a close relative, 17% reporting a loss, and 36% reporting negative events in relations to work, fijinances, close relation-ships, or other events. A total of 246 control participants (control group) reported no negative events. The 111 lung disease patients were therefore compared separately to the 91 participants in the negative events group and the 246 participants in the control group.
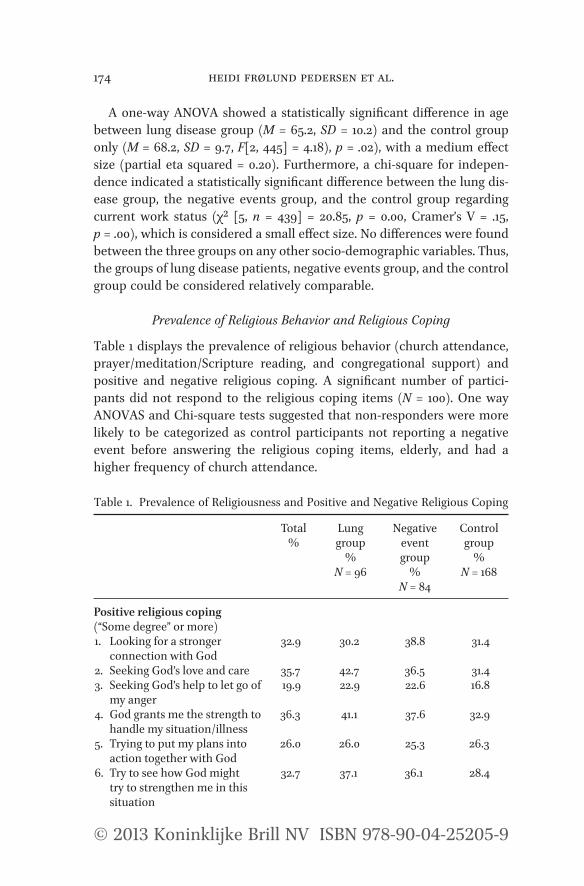
174 heidi frølund pedersen et al.
© 2013 Koninklijke Brill NV ISBN 978-90-04-25205-9
A one-way ANOVA showed a statistically signifijicant diffference in age between lung disease group (M = 65.2, SD = 10.2) and the control group only (M = 68.2, SD = 9.7, F[2, 445] = 4.18), p = .02), with a medium efffect size (partial eta squared = 0.20). Furthermore, a chi-square for indepen-dence indicated a statistically signifijicant diffference between the lung dis-ease group, the negative events group, and the control group regarding current work status (χ² [5, n = 439] = 20.85, p = 0.00, Cramer’s V = .15, p = .00), which is considered a small efffect size. No diffferences were found between the three groups on any other socio-demographic variables. Thus, the groups of lung disease patients, negative events group, and the control group could be considered relatively comparable.
Prevalence of Religious Behavior and Religious Coping
Table 1 displays the prevalence of religious behavior (church attendance, prayer/meditation/Scripture reading, and congregational support) and positive and negative religious coping. A signifijicant number of partici-pants did not respond to the religious coping items (N = 100). One way ANOVAS and Chi-square tests suggested that non-responders were more likely to be categorized as control participants not reporting a negative event before answering the religious coping items, elderly, and had a higher frequency of church attendance.
Table 1. Prevalence of Religiousness and Positive and Negative Religious Coping
Total%
Lunggroup
%N = 96
Negative eventgroup
%N = 84
Controlgroup
%N = 168
Positive religious coping (“Some degree” or more)1. Looking for a stronger
connection with God32.9 30.2 38.8 31.4
2. Seeking God’s love and care 35.7 42.7 36.5 31.43. Seeking God’s help to let go of
my anger19.9 22.9 22.6 16.8
4. God grants me the strength to handle my situation/illness
36.3 41.1 37.6 32.9
5. Trying to put my plans into action together with God
26.0 26.0 25.3 26.3
6. Try to see how God might try to strengthen me in this situation
32.7 37.1 36.1 28.4
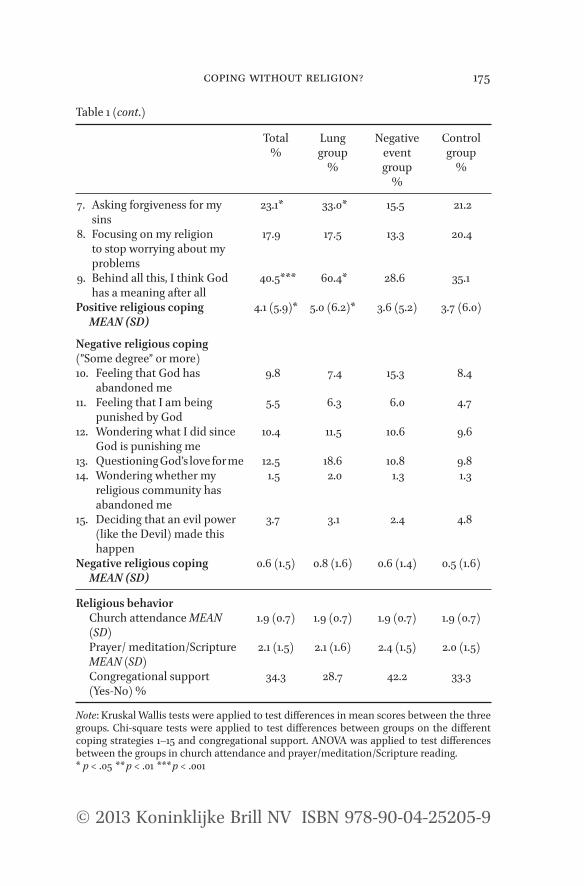
coping without religion? 175
© 2013 Koninklijke Brill NV ISBN 978-90-04-25205-9
Total%
Lunggroup
%
Negative eventgroup
%
Controlgroup
%
7. Asking forgiveness for my sins
23.1* 33.0* 15.5 21.2
8. Focusing on my religion to stop worrying about my problems
17.9 17.5 13.3 20.4
9. Behind all this, I think God has a meaning after all
40.5*** 60.4* 28.6 35.1
Positive religious coping MEAN (SD)
4.1 (5.9)* 5.0 (6.2)* 3.6 (5.2) 3.7 (6.0)
Negative religious coping (”Some degree” or more)10. Feeling that God has
abandoned me9.8 7.4 15.3 8.4
11. Feeling that I am being punished by God
5.5 6.3 6.0 4.7
12. Wondering what I did since God is punishing me
10.4 11.5 10.6 9.6
13. Questioning God’s love for me 12.5 18.6 10.8 9.814. Wondering whether my
religious community has abandoned me
1.5 2.0 1.3 1.3
15. Deciding that an evil power (like the Devil) made this happen
3.7 3.1 2.4 4.8
Negative religious coping MEAN (SD)
0.6 (1.5) 0.8 (1.6) 0.6 (1.4) 0.5 (1.6)
Religious behaviorChurch attendance MEAN (SD)
1.9 (0.7) 1.9 (0.7) 1.9 (0.7) 1.9 (0.7)
Prayer/ meditation/Scripture MEAN (SD)
2.1 (1.5) 2.1 (1.6) 2.4 (1.5) 2.0 (1.5)
Congregational support (Yes-No) %
34.3 28.7 42.2 33.3
Note: Kruskal Wallis tests were applied to test diffferences in mean scores between the three groups. Chi-square tests were applied to test diffferences between groups on the diffferent coping strategies 1–15 and congregational support. ANOVA was applied to test diffferences between the groups in church attendance and prayer/meditation/Scripture reading.* p < .05 ** p < .01 *** p < .001
Table 1 (cont.)

176 heidi frølund pedersen et al.
© 2013 Koninklijke Brill NV ISBN 978-90-04-25205-9
Chi-square tests showed no signifijicant diffferences between the lung disease group, the negative events group, and control group in church attendance, private religious practice, or congregational support. Overall, positive religious coping strategies were more frequently reported than negative strategies across all three groups. Kruskal Wallis and Chi-square tests showed no statistically signifijicant diffferences in overall negative religious coping and the separate negative religious coping strategies between the three groups. A Kruskal Wallis test indicated that the lung disease group reported more overall positive religious coping than both the negative events group and the control group (χ2 [2, n = 348] = 8.17, p = 0.02). Mann Whitney tests were applied as post hoc tests using a Bonferonni correction of the alpha value to 0.02 and suggested only the lung disease group and the control group difffered signifijicantly in overall positive religious coping, (U = 6470.5, z = –2.82, p = 0.01, r = –0.20), cor-responding to a medium efffect size. Specifijically, Chi square analyses indi-cated a statistically signifijicant diffference in the prevalence of the positive religious coping strategies of religious purifijication (“Asked forgiveness for my sins”) and positive religious meaning-making (“Thought God had a meaning after all”) between the three groups. Post-hoc analyses using the standardized residuals suggested lung disease patients reported greater religious purifijication (z = 2.00, α = 1.96) and religious meaning-making (z = 3.10, α = 1.96) than the negative events group and the control group.
Religious Coping and Overall Quality of Life
Table 2 displays the unadjusted and adjusted hierarchical regressions examining associations between socio-demographic and religious factors, religious coping, and overall quality of life and existential well-being.
The unadjusted analyses showed that higher annual household income was associated with higher overall QoL. In the fijirst adjusted model, asso-ciations between demographic variables and overall QoL were explored. Age, sex, marital status, number of children, education level, current work situation, and annual household income were entered into the fijirst model and explained 5.8% of the variance in overall QoL. In order to reduce the risk of under-fijitting of the model, the signifijicance level was set at p < 0.10, and the model indicated that higher education and higher annual house-hold income were signifijicantly associated with higher QoL. These variables were carried forward to be entered in the second model. In the second set of unadjusted regressions, associations between QoL and medical factors were explored, and the unadjusted analyses indicated that being a patient
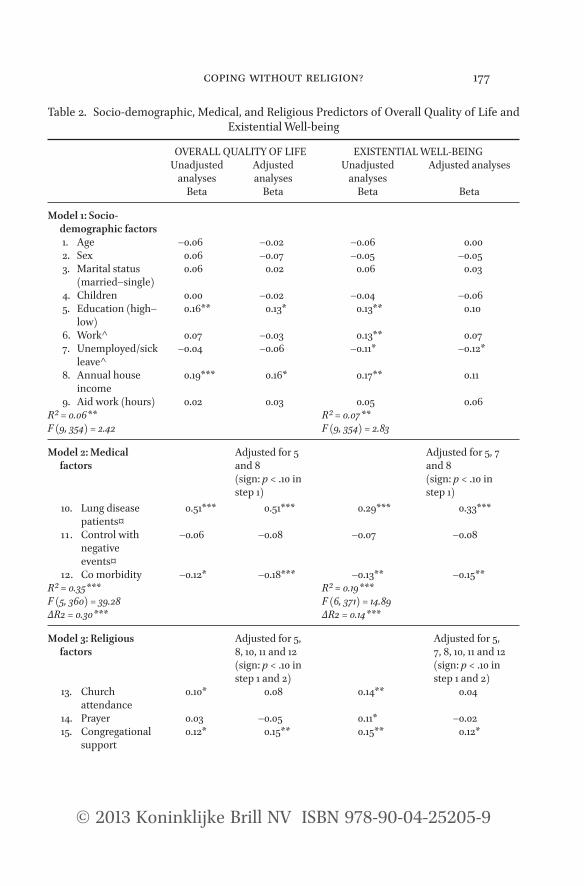
coping without religion? 177
© 2013 Koninklijke Brill NV ISBN 978-90-04-25205-9
Table 2. Socio-demographic, Medical, and Religious Predictors of Overall Quality of Life and Existential Well-being
OVERALL QUALITY OF LIFE EXISTENTIAL WELL-BEINGUnadjusted
analysesAdjusted analyses
Unadjusted analyses
Adjusted analyses
Beta Beta Beta Beta
Model 1: Socio- demographic factors
1. Age –0.06 –0.02 –0.06 0.002. Sex 0.06 –0.07 –0.05 –0.053. Marital status
(married–single)0.06 0.02 0.06 0.03
4. Children 0.00 –0.02 –0.04 –0.065. Education (high–
low)0.16** 0.13* 0.13** 0.10
6. Work^ 0.07 –0.03 0.13** 0.077. Unemployed/sick
leave^–0.04 –0.06 –0.11* –0.12*
8. Annual house income
0.19*** 0.16* 0.17** 0.11
9. Aid work (hours) 0.02 0.03 0.05 0.06R² = 0.06** R² = 0.07**F (9, 354) = 2.42 F (9, 354) = 2.83
Model 2: Medical factors
Adjusted for 5 and 8(sign: p < .10 in step 1)
Adjusted for 5, 7 and 8(sign: p < .10 in step 1)
10. Lung disease patients¤
0.51*** 0.51*** 0.29*** 0.33***
11 . Control with negative events¤
–0.06 –0.08 –0.07 –0.08
12. Co morbidity –0.12* –0.18*** –0.13** –0.15**R² = 0.35*** R² = 0.19***
F (6, 371) = 14.89ΔR2 = 0.14***
F (5, 360) = 39.28ΔR2 = 0.30***
Model 3: Religious factors
Adjusted for 5, 8, 10, 11 and 12 (sign: p < .10 in step 1 and 2)
Adjusted for 5, 7, 8, 10, 11 and 12 (sign: p < .10 in step 1 and 2)
13. Church attendance
0.10* 0.08 0.14** 0.04
14. Prayer 0.03 –0.05 0.11* –0.0215. Congregational
support0.12* 0.15** 0.15** 0.12*

178 heidi frølund pedersen et al.
© 2013 Koninklijke Brill NV ISBN 978-90-04-25205-9
16. Positive religious coping
0.11* 0.01 0.20*** 0.11
17. Negative religious coping
–0.12* –0.14** –0.06 –0.06
R² = 0.40*** R² = 0.24***F (10, 286) = 18.94 F (11, 285) = 8.05ΔR2 = 0.05** ΔR2 = 0.04**
Final modelStep 1
All variables (sign: p < .10 in step 1, 2, and 3)
Final modelStep 1
All variables (sign: p < .10 in step 1, 2, and 3)
Beta Beta1. Education 0.12* 1. Education 0.08
2. Unemployed/sick leave
–0.20***
2. Annual house income
0.13* 3. Annual house income
0.14**
3. Co morbidity –0.18*** 4. Co morbidity –0.15**4. Patient¤ 0.51*** 5. Patient 0.33***5. Control with
negative events¤–0.08 6. Control with
negative events¤–0.08
R² = 0.35*** R² = 0.19***F(5, 291) = 31.75 F(6, 352) = 14.13
Step 2 Step 21. Education 0.06 1. Education 0.08
2. Unemployed/sick leave
–0.20***
2. Annual house income
0.12 3. Annual house income
0.14**
3. Co morbidity –0.17*** 4. Co morbidity –0.15**4. Patient¤ 0.53*** 5. Patient¤ 0.34***5. Control with
negative events¤–0.09 6. Control without
negative events¤–0.09
6. Congregational support
0.17*** 7. Congregational support
0.17***
7. Negative religious coping
–0.14**
R² = 0.39*** R² = 0.22***F(7, 289) = 26.84 F(7, 351) = 14.34ΔR2 = 0.04*** ΔR2 = 0.03***
Table 2 (cont.)
OVERALL QUALITY OF LIFE EXISTENTIAL WELL-BEINGUnadjusted
analysesAdjusted analyses
Unadjusted analyses
Adjusted analyses
Beta Beta Beta Beta

coping without religion? 179
© 2013 Koninklijke Brill NV ISBN 978-90-04-25205-9
Table 2 (cont.)
OVERALL QUALITY OF LIFE EXISTENTIAL WELL-BEINGUnadjusted
analysesAdjusted analyses
Unadjusted analyses
Adjusted analyses
Beta Beta Beta Beta
Step 31. Education 0.09 1. Education 0.082. Annual house
income0.14** 2. Unemployed/
sick leave–0.19***
3. Co morbidity –0.17*** 3. Annual house income
0.14**
4. Patient¤ –0.53*** 4. Co morbidity –0.15**5. Control with
negative events¤–0.09 5. Patient¤ 0.34***
6. Congregational support
0.22** 6. Control without negative events¤
–0.08
7. Negative religious coping
–0.02 7. Congregational support
0.22**
8. Patient X congregational support¤
–0.09 8. Patient X congregational support¤
–0.03
9. Control with negative events X congregational support¤
–0.07 9. Control with negative events X congregational support¤
–0.07
10. Patient X negative religious coping¤
–0.19**
11. Control with negative events X negative religious coping¤
–0.05
R² = 0.42*** R² = 0.23***F(9,349) = 11.34ΔR2 = 0.00
F(11, 285) = 18.85ΔR2 = 0.03**
Note. Predictors, signifijicant at p < .10, were carried forward to the next models. P-value was set at .05 in the fijinal model^ The comparison groups were “Retired” participants¤ The comparison was controls without negative events* p < .05 ** p < .01 *** p < .001 ΔR2 = R square change
was associated with higher overall QoL, whereas comorbidity was associ-ated with lower overall QoL. In the second adjusted model, the disease-related variables of comorbidity and group membership were entered, and the analyses showed that the lung disease group reported a signifiji-cantly higher overall QoL than the negative events group and the control group, and comorbidity was signifijicantly associated with lower overall QoL, when controlling education level and annual household incomes.

180 heidi frølund pedersen et al.
© 2013 Koninklijke Brill NV ISBN 978-90-04-25205-9
After entering medical variables, the second model explained 35.3% of the total variance in overall QoL. The variables reaching signifijicance at level p < 0.10 were carried forward to the third model. According to the third set of unadjusted regressions, church attendance, congregational support, and positive religious coping were associated with higher overall QoL, whereas negative religious coping was associated with poorer overall QoL. In the third adjusted model, church attendance, prayer/meditation/Scripture reading, and positive religious coping were unassociated with overall QoL when controlling for demographic and medical variables, whereas congregational support was tied to better overall QoL, and nega-tive religious coping was linked with poorer overall QoL. After entering religious variables, the third model explained 39.8% of the total variance in overall QoL.
The fijinal model included variables signifijicant at p < 0.10 in the pre-vious adjusted regressions and four interaction terms testing possible interactions between group membership and congregational support and group membership and negative religious coping. The signifijicance level in the fijinal model was set at p < 0.05. In the fijinal model, fijive variables reached statistical signifijicance: Annual household income, being a lung disease patient, and receiving congregational support were signifijicantly associated with higher overall QoL, whereas comorbidity was signifijicantly associated with poorer QoL. The interaction term indicated that negative religious coping was signifijicantly associated with lower QoL among the lung disease group only and that congregational support was benefijicial for the control group only. The fijinal model accounted for 42.1% of the variance, the religious variables added 4.1% to the model over and above the demographic and medical factors, and the interaction terms added 2.7%, p < 0.01.
Religious Coping and Existential Well-Being
Exploring associations between existential well-being and diffferent pre-dictors, the fijirst set of unadjusted analyses showed that higher education, working full time or part time, and annual house income was associated with higher level of existential well-being, while being unemployed or at sick leave were associated with lower level of existential well-being. According to the fijirst set of adjusted analyses, being unemployed or on sick leave were associated with lower existential well-being, whereas higher annual house income was associated with better existential well-

coping without religion? 181
© 2013 Koninklijke Brill NV ISBN 978-90-04-25205-9
being. In the second set of unadjusted analyses, being a lung disease patient was associated with higher levels of existential well-being, while reporting co morbidity was associated with lower level of existential well-being. In the second set of adjusted analyses, controlling for demographic variables that were signifijicant in the fijirst adjusted model at p < 0.10, con-trols reporting negative events and participants reporting co-morbidity had lower level of existential well-being, while the lung disease group reported higher level of existential well-being. In the third set of unad-justed analyses, exploring associations between existential well-being and religious factors, church attendance, prayer/meditation/Scripture reading, congregational support, and positive religious coping were all associated with higher levels of existential well-being, while negative religious coping was not associated with existential well-being. In the third adjusted model controlling for demographic and medical factors that were signifijicant in model 1 and 2, congregational support reached statistical signifijicance and was carried forward to the last model.
The fijinal model included variables signifijicant at p < 0.10 in the previous adjusted regressions. Furthermore, interactions terms testing the possible interaction between group membership and congregational support were added. The signifijicance level in the fijinal model was set at p < 0.05. In the fijinal model, fijive variables reached statistical signifijicance: higher annual household income, being a lung disease patient, and reporting congrega-tional support were signifijicantly associated with higher levels of overall existential well-being, while comorbidity and being unemployed or on sick leave were signifijicantly associated with poorer existential well-being. The interaction efffect revealed that only the control group benefijitted from congregational support, but the interaction term did not add signifijicantly to the model over and above demographic, medical, and religious factors. The fijinal model accounted for 22.6 % of the variance, with congregational support adding 2.5% over and above demographic and medical factors.
Discussion
The present study was designed to test the generalizability of two fijindings that have emerged from research conducted in the US: (a) Reminders of mortality and human frailty, such as life threatening disease or negative life events, are associated with greater religiousness and religious coping when compared to individuals reporting no negative events, and (b) the

182 heidi frølund pedersen et al.
© 2013 Koninklijke Brill NV ISBN 978-90-04-25205-9
associations between religiousness and well-being are stronger among people facing major life events. More specifijically, higher levels of positive religious coping are tied to greater QoL and existential well-being among those dealing with negative life events, and higher levels of negative religious coping are tied to lower QoL and existential well-being among people facing major life events. The results of the present study offfered partial support for these predictions. Religious activities did not difffer between people facing life threatening illness and other negative events when compared to a healthy control group, but some forms of positive religious coping were more prevalent among life threatened individuals (lung disease patients) than those who were not dealing with negative life events (control group). Furthermore, negative religious coping was associ-ated with lower QoL among lung disease patients only. In contrast to our predictions, social support from one’s congregation was associated with better overall QoL and existential well-being only for the control group.
Religiosity and Prevalence of Religious Coping
The samples did not difffer signifijicantly in terms of religious behavior such as church attendance and prayer/meditation/Scripture reading, indicating that negative life events did not afffect either public or private religious behaviors signifijicantly. Our samples reported more frequent church atten-dance than usually reported for the general Danish population. Only 7% reportedly attend church monthly in the general population (The Danish Value Survey, 2008) in contrast to almost 15% in the present study. One reason for this diffference could be the relatively high mean age of our participants, which is supported by previous studies showing that elderly generations are more religiously oriented than younger ones. A Danish study by Andersen et al. (2011) using data from the Danish Value Survey 1990–2008 found that levels of religiosity were associated with the cohort the individuals belonged to; that is, elderly people were in general more religiously oriented than younger generations. However, the study did not support the idea that a person becomes more religious with age. The diffference between generations was mainly explained by declines in reli-gious socialization during childhood among the younger generations.
Religious coping strategies in the present study were prevalent among all three groups. Positive religious coping was reported more frequently than negative religious coping strategies, which is in accordance with results from previous studies (Bjorck & Thurman, 2007). The results suggest that lung disease patients report more overall positive religious

coping without religion? 183
© 2013 Koninklijke Brill NV ISBN 978-90-04-25205-9
coping when compared to the control group, but signifijicant diffferences were not found between lung disease patients and the negative events group or between the negative events group and the control group. The strategies of asking for forgiveness and positive religious meaning-making were especially prevalent in the lung disease group. Earlier studies have found that, due to life style-related factors like smoking in the etiol-ogy of lung disease, lung disease patients often report greater self-blame (Chapple, Ziebland, & McPherson, 2004). It could be that the lung disease patients in our study may have experienced a need to ask forgiveness for an unhealthy life style and could be seeking reconciliation with family or friends (and ultimately God) while there was still time (De Guzman et al., 2010). Furthermore, receiving a life threatening diagnosis like lung cancer or COPD may increase the need for fijinding meaning in the midst of major life challenges. In a study of the existential and spiritual needs among cancer patients, Moadel and colleagues (1999) found that 40% reported to have a need for fijinding meaning. In our sample, almost two thirds of the lung disease group (60%) reported using religious meaning-making to some degree or more, compared to approximately one third of both the negative events group and the control group. Patients may benefijit from increased focus on (religious) meaning-making, and health professionals or hospital chaplains may be able to support this positively. Caution is called for here, however. It may be premature to suggest specifijic inter-vention programs because research in this area in Denmark is only in its infancy, and more studies on religious, spiritual, and existential needs and practices during severe illness are needed.
Contrary to expectations, we found no diffferences in religious coping between the negative events group and the control group. Reasons for this fijinding may be that the negative events reported in the present study were less serious than lung disease and in some instances involved a close relative versus oneself. Therefore, it seems religion was not widely mobi-lized as a coping strategy by this group. This fijinding would support the theory of terror management, namely, that reminders of one’s own per-sonal mortality are more likely to trigger religiosity than more mundane life events.
Religious Coping and Overall QoL
While the unadjusted analyses suggested a positive association between positive religious coping and QoL, the adjusted model did not support the hypothesis that positive religious coping afffects well-being. It has been

184 heidi frølund pedersen et al.
© 2013 Koninklijke Brill NV ISBN 978-90-04-25205-9
suggested that due to the relatively high standard of living among Danes, religious coping strategies may not contribute signifijicantly to adjustment among Danes (Pedersen, Pedersen, Pargament, & Zachariae, in press) as seen in American studies among individuals with fewer economic and secular resources (Pargament, 1997). Another explanation could be that our results reflect the efffect of secularization. From this perspective, reli-gion no longer provides a framework for meaning, comfort, and control; it is only mobilized during times of distress but has little efffect on adjust-ment. Finally, the non-signifijicant associations between positive religious coping and QoL could be the result of what has been called a religious cop-ing mobilization efffect (Pargament, 1997). This efffect occurs in cross-sec-tional studies and involves two offfsetting or counterbalancing forces: (a) the positive efffect of religious coping on distress or well-being (i.e., QoL); and (b) the mobilizing efffect of distress or lower well-being (i.e., QoL) on religious coping. While the fijirst efffect would create a positive correla-tion between religious coping and QoL, the second efffect would create a negative correlation between religious coping and QoL. In theory, the two efffects could wash each other out, resulting in a non-signifijicant correla-tion between positive religious coping and distress/well-being. Longitu-dinal designs are needed to tease out these efffects.
In contrast, congregational support was found to be signifijicantly asso-ciated with better overall QoL. The control group benefijitted most by this type of support. Receiving social support from the members of one’s con-gregation or fellow believers may be perceived as interpersonal religious coping, which is represented in the Brief RCOPE by only one item (Ano & Pargament, 2012). A meta-analysis of 38 studies found that social sup-port from members of religious communities is one of the most-reported predictors of mental health (Larson et al., 1992) and appears to influence well-being more than private aspects of religiosity, such as prayer (Lim & Putnam, 2010). Social support in general has been found to be a stress-bufffering factor (Antonovsky, 1979). The present study, however, did not include specifijic measures of other types of non-religious social support (family, friends, neighbors, colleagues, self-help groups, or others). Thus, we do not know whether congregational support contributed to better QoL among Danes above and beyond the efffects of other forms of social support. It may, however, be argued that people engaged in religious communities may have easier access to social networks and therefore a fijirmer background of social support. This could also apply to Danes who are involved in religious communities.

coping without religion? 185
© 2013 Koninklijke Brill NV ISBN 978-90-04-25205-9
Although not as prevalent as positive religious coping, negative reli-gious coping was associated with lower overall QoL among lung disease patients, thereby confijirming previous results from a range of studies (Ano & Vasconcelles, 2005). Our results contribute to the literature by demon-strating that negative religious coping seems to afffect QoL in a negative direction even in a highly secularized society such as Denmark, in con-trast to the idea that religious beliefs are irrelevant to Danes (Zuckerman, 2008). There could be several possible explanations for this fijinding. First, lung disease patients report more internal causal illness attributions (e.g. smoking), which, in turn, have been associated with poorer adjustment in terms of higher anxiety and more depressive symptoms (Else-Quest, LoConte, Schiller, & Hyde, 2009). Thus, blaming oneself for an unhealthy life style leading to the development of illness may also be tied to religious struggles, such as thoughts of “getting what you deserve” as a punishment from God. One study by Webb (1995) found that self-blame among people who reported abuse experiences was tied to beliefs in a punitive God. Such fijindings may be explained by the just-world-theory (Lerner & Miller, 1978), which states that people are motivated to maintain their beliefs that the world is just (Hafer & Bégue, 2005). Patients facing severe illness may also pose the question “Why me?” and feel that their just world views have been violated (Janofff-Bulman, 1992). This could potentially lead to strategies of holding God responsible for an event, seeing oneself as a vic-tim (Exline et al., 2011), or perceiving an event as unfair and uncontrol-lable (Ano & Pargament, 2012), thereby resulting in religious struggles and poorer well-being.
Second, it is possible that other factors that were not measured are responsible for the associations between religious struggle and lower QoL. In a recent study of 309 undergraduate students coping with negative events, Ano and Pargament (2012) found that personality factors such as neuroticism and ambivalent attachment to God were signifijicant predic-tors of religious struggles. Due to the cross-sectional design of the pres-ent study, we are unable to determine whether negative religious coping caused low QoL or vice versa, and additional unknown variables could be contributing to both. Longitudinal studies that assess possible moderating or mediating factors are needed to explore such causal explanations.
Finally, in line with terror management theory, some studies have found that only well-developed religious beliefs function as a bufffer against death anxiety and result in higher well-being (Jonas & Fischer, 2006). As we have argued previously (Pedersen et al., in press), it is therefore possible

186 heidi frølund pedersen et al.
© 2013 Koninklijke Brill NV ISBN 978-90-04-25205-9
that religious struggle was prevalent among the lung disease group because their religious beliefs were not fully functioning and integrated due to secularization. When trying to mobilize their religious beliefs, lung disease patients may have experienced that their religious beliefs repre-sented a source of doubts and frustration instead of a source of comfort and hope, thereby resulting in poorer QoL. The present study found that lung disease patients may be especially vulnerable to the efffects of nega-tive religious coping on well-being, perhaps because of the profound and disturbing struggles that may be tied to lung disease as compared to other major life events.
Religious Coping and Existential Well-Being
Associations between existential well-being and positive and negative reli-gious coping did not reach statistical signifijicance in the adjusted regres-sions. Existential well-being represents the extent to which an individual experiences meaning and purpose in life and fijinds comfort in religious and spiritual beliefs. It has been suggested that one of the core functions of religion is meaning-making (Park, 2005). While previous studies have found positive associations between positive religious coping and exis-tential well-being (Arnette, Mascaro, Santana, Davis, & Kaslow, 2007; Holt et al., 2011), the present study failed to reveal associations between posi-tive religious coping strategies and existential well-being in the adjusted model. Negative religious coping was not associated with existential well-being either, which is somewhat surprising given the links between nega-tive religious coping and overall QoL.
The lack of statistically signifijicant associations between positive reli-gious coping and QoL and existential well-being in the adjusted regressions could also be explained by another fijinding. The hierarchical regressions indicated that the lung disease group scored signifijicantly higher on all subscales of overall QoL and existential well-being than the negative events group and the control group, which by itself was an unexpected fijinding. This fijinding could be due to several factors. First, normative data on the FACT-G comparing cancer patients with healthy controls suggest that patients may score higher on social well-being than the general popu-lation perhaps because they receive high levels of social support for their illness (Brucker et al., 2005). It may be argued that higher social support is associated with better emotional well-being, thereby causing a higher score in overall QoL as reported in the present study. Second, the dif-ferences in scores on well-being measures between patients and healthy

coping without religion? 187
© 2013 Koninklijke Brill NV ISBN 978-90-04-25205-9
controls may reflect avoidant coping strategies among the lung disease group; that is, patients may report higher levels of well-being as a way of minimizing the gravity of their situation. Finally, the fijinding could be influenced by selection bias in recruiting the patient sample. Due to the severity of lung disease, only the higher functioning patients may have participated. Thus, diffferences in QoL and existential well-being scores between the lung disease group, the negative events group, and the con-trol group could explain why no associations were found between posi-tive religious coping and QoL and existential well-being in the adjusted regression model. More studies investigating diffferent patient groups are needed to clarify the impact of religiosity among severely ill patients in secular societies like Denmark.
Limitations and Future Directions
The present study is among the fijirst to investigate the prevalence of reli-gious coping and associations to QoL and existential well-being in a secu-lar country such as Denmark. Some limitations of the study should be noted. Among the key limitations is the issue of the low response rate among lung disease patients and the subsequent limited representative-ness of this sample with respect to the population of lung disease patients as a whole. In general, the samples represented elderly individuals, and religious issues may be perceived very diffferently among younger gen-erations. One previous Danish study found that religious, spiritual, and existential concerns were signifijicantly more prevalent among younger (< 36 years) hospitalized patients (Ausker et al., 2008). Because religious upbringing has become less common over time in Denmark, it is important to identify those resources that become important in coping and mean-ing-making during challenging life events among younger Danes. Second, the cross-sectional design of the present study limits our ability to draw conclusions about causality. Although more recent longitudinal studies have yielded valuable insights into the mechanisms of religious coping in association with well-being, studies are needed in secular societies too. One area of potential interest is the question of possible associations between negative religious coping and post-traumatic growth, which so far has only been scantily explored in the literature (Pargament, Desai, & McConnell, 2006). Questions about this issue may be present in secular societies where existential and religious struggles may develop diffferently than in religious societies such as the US. It has been argued that ben-efijit fijinding or positive thinking may be more commonplace as a cultural

188 heidi frølund pedersen et al.
© 2013 Koninklijke Brill NV ISBN 978-90-04-25205-9
construction in the US than in European countries (Ehrenreich, 2009), but whether this has any influence on how negative events are dealt with in terms of religious coping among Europeans is unclear. Finally, the cop-ing and support assessments used in the present study were limited to religious coping and support. The rather large amount of non- responders on the religious coping items calls for reflection. Analyses suggested that especially control participants did not answer the religious coping items. This fijinding may be due to methodological issues. Control participants may have misinterpreted the instruction (that they were to think of how they usually cope with major challenges when answering the Brief RCOPE), and instead skipped the whole questionnaire, because they did not specify a negative event. Another explanation could be that the religious coping items did not apply to the non-responders. It could be important to exam-ine other secular and spiritual existential coping strategies of meaning-making and social support in further research (la Cour & Hvidt, 2010).
Despite these limitations, the present study yields relevant insights into the prevalence of religious coping and associations with well-being among Danes. Support was found for the hypothesis that life threatening situations like a lung disease may be tied to religious coping, even among individuals from societies who in general are not thought to be very religious. Support was also found for the hypothesis that negative religious coping (religious struggle) is associated with lower QoL among lung disease patients. These results indicate that although religion may not play a central role in the lives of the majority of the Danes, religious coping strategies may become relevant in life threatening situations such as severe illness. Health profes-sionals, as well as hospital chaplains, imams, and rabbis should consider a detailed religious or spiritual assessment (see Grossoehme & Fitchett, 2013 [this volume]) for patients who may be at risk of developing religious struggles, as this may be tied to poorer adjustment among Danes.
References
Andersen, P.B., Ausker, N.H., & la Cour, P. (2011). Går fanden i kloster, når han bliver gammel? In P. Gundelach (Ed.), Små og store forandringer. Danskernes værdier siden 1981 (pp. 97–113). København, Danmark: Hans Reitzels Forlag.
Ano, G.G., & Pargament, K.I. (2012). Predictors of spiritual struggles: an exploratory study. Mental Health, Religion, and Culture. Advance online publication. doi:10.1080/13674676.2012.680434
Ano, G.G., & Vasconcelles, E.B. (2005). Religious coping and psychological adjustment to stress: A meta-analysis. Journal of Clinical Psychology, 61(4), 461–480. doi:10.1002/jclp.20049
coping without religion? 189
© 2013 Koninklijke Brill NV ISBN 978-90-04-25205-9
Antonovsky, A. (1979). Health, stress, and coping. San Francisco, CA: Jossey-Bass.Arnette, N.C., Mascaro, N., Santana, M.C., Davis, S., & Kaslow, N.J. (2007). Enhancing spiri-
tual well‐being among suicidal African American female survivors of intimate partner violence. Journal of clinical psychology, 63(10), 909–924. doi:10.1002/jclp.20403
Ausker, N., la Cour, P., Busch, C., Nabe-Nielsen, H., & Pedersen, L.M. (2008). Danske patienter intensiverer eksistentielle tanker og religiøst liv [Existential thoughts and religious life of Danish Patients]. Ugeskrift for Læger, 170, 1828–1833.
Bjorck, J.P., & Thurman, J.W. (2007). Negative life events, patterns of positive and nega-tive religious coping, and psychological functioning. Journal for the Scientifijic Study of Religion, 46(2), 159–167. doi:10.1111/j.1468-5906.2007.00348.x
Brucker, P.S., Yost, K., Cashy, J., Webster, K., & Cella, D. (2005). General population and can-cer patient norms for the Functional Assessment of Cancer Therapy-General (Fact-G). Evaluation and Health Professions, 28(2), 192–211. doi:10.1177/0163278705275341
Cella, D.F., Tulsky, D.S., Gray, G., Sarafijian, B., Linn, E., Bonomi, A., & . . . Brannon, J. (1993). The functional assessment of cancer therapy scale: Development and validation of the general measure. Journal of Clinical Oncology, 11(3), 570–579. http://jco.ascopubs.org/
Chapple, A., Ziebland, S., & McPherson, A. (2004). Stigma, shame, and blame experienced by patients with lung cancer: Qualitative study. British Medical Journal, 328(7454), 1470. doi:10.1136/bmj.38111.639734.7C
Charlson, M.E., Pompei, P., Ales, K.L., & MacKenzie, C.R. (1987). A new method of classify-ing prognostic comorbidity in longitudinal studies: Development and validation. Journal of Chronic Diseases, 40(5), 373–383. doi:10.1016/0021-9681
Christensen, S., Zachariae, R., Jensen, A., Vaeth, M., Møller, S., Ravnsbaek, J., & von der Maase, H. (2009). Prevalence and risk of depressive symptoms 3–4 months post-surgery in a nationwide cohort study of Danish women treated for early stage breast-cancer. Breast Cancer Research and Treatment, 113(2), 339–355. doi:10.1007/s10549-008-9920-9
Cummings, J.P., & Pargament, K.I. (2010). Medicine for the spirit: Religious coping in indi-viduals with medical conditions. Religions, 1, 28–53. http://www.mdpi.com/2077-1444/1/1/28
——. The Danish Lung Cancer Registry. Retrieved from http://www.lungecancer.dk.——. The Danish Value Survey. (2008). Originally conducted by Prof. Peter Gundelach.
Data were made available by the Danish Data Archive (archive number DDA-21432).De Guzman, A.B., Sindac, L.A.G., Sioson, J.J.T., Sison, K.J.B., Socia, J.K,M., Solidum,
R.F., . . . & Suaberon, L.C.D.C. (2010). Looking through a window: The guilt and remorse space of a lung cancer patient. Journal of Cancer Education, 25, 663–665. doi:10.1007/s13187-010-0127-5
Delgado-Guay, M.O., Hui, D., Parsons, H.A., Govan, K., De la Crux, M., Thorney, S., & Bruera, E. (2011). Spirituality, religiosity, and spiritual pain in advanced cancer patients. Journal of Symptom and Pain Management, 41(6): 986–994. doi:10.1016/j.jpainsymman.2010.09.017
Ehrenreich, B. (2009). Smile or die. How positive thinking fooled America and the world. Lon-don, UK: MPG Books Group.
Else-Quest, N.M., LoConte, N.K., Schiller, J.H., & Hyde, J.S. (2009). Perceived stigma, self-blame, and adjustment among lung, breast and prostate cancer patients. Psychology & Health, 24(8), 949–964. doi:10.1080/08870440802074664
Exline, J.J., Park, C.L., Smyth, J.M., & Carey, M.P. (2011). Anger toward God: Social-cognitive predictors, prevalence, and links with adjustment to bereavement and cancer. Journal of Personality and Social Psychology, 100(1), 129–148. doi:10.1037/a0021716
Fitchett, G., Murphy, P.E., Kim, J., Gibbons, J., Cameron, J.R., & Davis, J.A. (2004). Religious struggle: Prevalence, correlates, and mental health risks in diabetic, congestive heart failure, and oncology patients. International Journal of Psychiatry in Medicine, 34(2), 179–196. doi:10.2190/UCJ9-DP4M-9C0X-835M
Gallup Daily Tracking. (2008–2010). Retrieved from http://www.gallup.com/poll/141044/Americans-Church-Attendance-Inches-2010.aspx#1.

190 heidi frølund pedersen et al.
© 2013 Koninklijke Brill NV ISBN 978-90-04-25205-9
Greenberg, J., Pyszczynski, T., & Solomon, S. (1986). The causes and consequences of a need for self-esteem: A terror management theory. In R.F. Baumeister (Ed.) Public self and private self (pp. 189–212). New York, NY: Springer. doi:10.1007/978-1-4613-9564-5_10
Grossoehme, D.H., & Fitchett, G. (2013). Testing the validity of a protocol to screen for spiritual struggle among parents of children with cystic fijibrosis. Research in the Social Scien-tifijic Study of Religion (24), http://www.brill.com/publications/research-social-scientifijic-study-religion.
Hafer, C.L., & Bégue, L. (2005). Experimental research on just-world-theory: Problems, developments, and future challenges. Psychological Bulletin, 131(1), 128–167. doi:10.1037/0033-2909.131.1.128
Hebert, R., Zdaniuk, B., Schulz, R., & Scheier, M. (2009). Positive and negative religious coping and well-being in women with breast cancer. Journal of Palliative Medicine, 12(6), 538–545. doi:10.1089=jpm.2008.0250
Henderson, S., Byrne, D.G., & Duncan-Jones, P. (1981). Neurosis and the social environment. Sydney, Australia: Academic Press.
Hills, J., Paice, A., Cameron, J.R., & Shott, S. (2005). Spirituality and distress in palliative care consultation. Journal of Palliative Medicine, 8(4), 782–788. doi:10.1089/jpm.2005.8.782
Højsgaard, M.T., & Ravn Iversen, H. (2005). Gudstro i Danmark. Frederiksberg, Danmark: Anis.
Holt, C.L., Wang, M.Q., Caplan, L., Schulz, E., Blake, V., & Southward, V.L. (2011). Role of religious involvement and spirituality in functioning among African Americans with cancer: testing a mediational model. Journal of Behavioral Medicine, 34, 437–448. doi: 10.1007/s10865-010-9310-8
Janofff-Bulman, R. (1992). Shattered assumptions: Towards a new psychology of trauma. New York, NY: Free Press.
Jonas, E., & Fischer, P. (2006). Terror management and religion: Evidence that intrinsic religiousness mitigates worldview defense following mortality salience. Journal of Per-sonality and Social Psychology, 91(3), 553–567. doi:10.1037/0022-3514.91.3.553
Jong, J., Halberstadt, J., & Bluemke, M. (2012). Foxhole atheism, revisited: The efffects of mortality salience and implicit religious belief. Journal of Experimental Social Psychol-ogy, 48, 983–989. doi:10.1016/j.jesp.2012.03.005
La Cour, P., & Hvidt, N.C. (2010). Research on meaning-making and health in secular soci-ety: Secular, spiritual, and religious existential orientations. Social Science and Medicine, 71(7), 1292–1299. doi:10.1016/j.socscimed.2010.06.024
Larson, D.B., Sherrill, K.A., Lyons, J.S., Craigie, F.C., Thielman, S.B., Greenwold, M.B. & Larson, S.S. (1992). Associations between dimensions of religious commitment and mental health reported in The American Journal of Psychiatry and Archives of General Psychiatry: 1978–1989. The American Journal of Psychiatry, 149(4), 557–559. http://ajp.psychiatryonline.org/journal.aspx?journalid=13
Lee., S.A., Roberts, L.B., & Gibbons, J.A. (2012). When religion makes grief worse: Negative religious coping as associated with maladaptive emotional responding patterns. Mental Health, Religion and Culture. doi:10.1080/13674676.2012.659242
Lerner, M.J., & Miller, D.T. (1978). Just world research and the attribution process: Looking back and ahead. Psychological Bulletin, 85(5), 1030–1051. doi:10.1037/0033-2909.85.5.1030
Lim, C., & Putnam, R.D. (2010). Religion, social networks, and life satisfaction. American Sociological Review, 75(6), 914–933. doi:10.1177/0003122410386686
Magyar-Russell, G., Brown, I.T., Idara, I., Smith, M.T., Marine, J.E. & Ziegelstein, R.C. In search of serenity: Religious struggle among patients hospitalized for acute coronary syn-drome. Manuscript submitted for publication.
McConnell, K., Pargament, K.I., Ellison, C.G., & Flannelly, K.J. (2006). Examining the links between spiritual struggles and symptoms of psychopathology in a national sample. Journal of Clinical Psychology, 62, 1469–1484. doi:10.1002/jclp.20325
Meisenhelder, J.B., & Marcum, J.P. (2004). Responses of clergy to 9/11: Posttraumatic stress, coping, and religious outcomes. Journal for the Scientifijic Study of Religion, 43(4), 547–554. doi:10.1111/j.1468-5906.2004.00255.x

coping without religion? 191
© 2013 Koninklijke Brill NV ISBN 978-90-04-25205-9
Moadel, A., Morgan, C., Fatone, A., Grennan, J., Carter, J., Larufffa, G., . . . & Dutcher, J. (1999). Seeking meaning and hope: Self-reported spiritual and existential needs among an ethnically-diverse cancer patient population. Psycho-oncology, 8, 378–385. doi:10.1002/(SICI)1099-1611(199909/10)8:5<378::AID-PON406>3.0.CO;2-A
Organisation for Economic Co-operation and Development. (2009). Poverty. In OECD Soci-ety at a glance 2009: OECD social indicators, (pp. 90–91). OECD Publishing. doi: 10.1787/soc_glance-2008-17-en
Pargament, K.I. (1997). The psychology of religion and coping. Theory, research, practice. New York, NY: Guildford.
——. (2007). Spiritually integrated psychotherapy. Understanding and addressing the sacred. New York, NY: Guildford.
Pargament, K.I., Desai, K.M., & McConnell, K.M. (2006). Spirituality: A pathway to post-traumatic growth or decline? In: L.G. Calhoun & R.G. Tedeschi (Eds.), The handbook of post-traumatic growth: Research and practice, (pp. 121–137). Mahwah, NJ: Erlbaum.
Pargament, K.I., Koenig, H.G., & Perez, L.M. (2000). The many methods of religious coping: Development and initial validation of the RCOPE. Journal of Clinical Psychology, 56(4), 519–543. doi:10.1002/(SICI)1097-4679(200004)56:4<519::AID-JCLP6>3.0.CO;2-1
Pargament, K.I., Koenig, H.G., Tarakeshwar, N., & Hahn, J. (2001). Religious struggle as a predictor of mortality among medically ill elderly patients: A 2 year longitudinal study. Archives of Internal Medicine, 161, 1881–1885. doi:10.1001/archinte.161.15.1881
Pargament, K.I., Murray-Swank, N.A, Magyar, G.M., & Ano, G.G. (2005). Spiritual strug-gle: A phenomenon of interest to psychology and religion. In W.R. Miller and H.D. Delaney (Eds.) Judeo-Christian perspectives on psychology: Human nature, motiva-tion and change, (pp. 245–68). Washington, DC: American Psychological Association. doi:10.1037/10859-013
Pargament, K.I., Smith, B.W., Koenig, H.G., & Perez, L. (1998). Patterns of positive and negative religious coping with major life stressors. Journal of the Scientifijic Study of Reli-gion, 37(4), 710–724. doi:10.2307/1388152
Park, C.L. (2005). Religion as a meaning-making framework in coping with life stress. Jour-nal of Social Issues, 61(4), 707–729. doi:10.1111/j.1540-4560.2005.00428.x
Pedersen, C.G. (2009). Complementary and alternative medicine among cancer patients. Prevalence, user characteristics, and efffectiveness for well-being. Doctoral dissertation, Aarhus University, Denmark.
Pedersen, H.F., Pedersen, C.G., Pargament, K.I., & Zachariae (in press). Religious coping among severely ill lung patients in a secular society. International Journal for the Psy-chology of Religion. doi:10.1080/10508619.2012.728068
Peterman, A.H., Fitchett, G., Brady, M.J., Pharm, L.H., & Cella, D. (2002). Measuring spiri-tual well-being in patients with cancer: The functional assessment of chronic illness therapy—spiritual well-being scale (FACIT-Sp). Annals of Behavioral Medicine, 24(1), 49–58. doi:10.1207/S15324796ABM2401_06
Pew Research Center (2008): U.S. Religious Landscape Survey. Retrieved from http://religions.pewforum.org/reports.
Schafer, J.L., & Graham, J.W. (2002). Missing data: our view of the state of the art. Psycho-logical Methods, 7, 147–177. doi:10.1037/1082-989X.7.2.147
Schaie, K.W., Krause, N., & Booth, A. (2004). Health and well-being in elderly. New York, NY: Springer Publishing Company, Inc.
Schreiber, J.A., & Brockopp, D.Y. (2012). Twenty-fijive years later—what do we know about religion/spirituality and psychological well-being among breast cancer survivors? A sys-tematic review. Journal of Cancer Survival, 6, 82–94. doi:10.1007/s11764-011-0193-7
Sherman, A.C., Plante, T.G., Simonton, S., Latif, U., & Anaissie, E.J. (2009). Prospective study of religious coping among patients undergoing autologous stem cell transplanta-tion. Journal of Behavioral Medicine, 32, 118–128. doi:10.1007/s10865-008-9179-y
Statistics Denmark. (2012). Retrieved from http://www.dst.dk/da/Statistik/emner/folkekirken/medlemmer-af-folkekirken.aspx?tab=nog

192 heidi frølund pedersen et al.
© 2013 Koninklijke Brill NV ISBN 978-90-04-25205-9
Tarakeshwar, N., Vanderwerker, L.C., Paulk, E., Pearce, M.J., Kasl, S.V., & Prigerson, H.G. (2006). Religious coping is associated with the quality of life of patients with advanced cancer. Journal of Palliative Care, 9(3), 646–657. doi:10.1089/jpm.2006.9.646
Thuesen, P.J. (2009). Predestination: The American career of a contentious doctrine. Oxford, UK: Oxford University Press.
Vail, K.E., III, Rothschild, Z.K., Weise, D.R., Solomon, S., Pyszczynski, T., & Greenberg, J. (2010). A terror management analysis of the psychological functions of religion. Person-ality and Social Psychology Review, 14, 84–94. doi:10.1177/1088868309351165
Webb, M.L. (1995). The religious beliefs about sufffering scale: Factor analysis, construct validity, and relationship to history of abuse. Doctoral dissertation, Fuller Theological Seminary.
Zuckerman, P. (2008). Society without God. What the least religious nations can tell us about contentment. New York, NY: NYU Press.
Paper 3
1
Psycho-social factors associated with religious struggles during
negative life events in a secular society
Heidi F. Pedersen, Christina G. Pedersen, & Robert Zachariae
Unit for Psycho-Oncology and Health Psychology, Department of Psychology, Aarhus University
and Department of Oncology, Aarhus University Hospital, Aarhus, Denmark
Submitted for Psychology of Religion and Spirituality (Spring 2013)
Author note
Heidi F. Pedersen, Unit for Psycho-Oncology and Health Psychology, Department of Psychology,
Aarhus University; Christina G. Pedersen, Unit for Psycho-Oncology and Health Psychology,
Department of Psychology, Aarhus University; Robert Zachariae, Unit for Psycho-Oncology and
Health Psychology, and Department of Oncology, Aarhus University Hospital
The project was supported by the Danish Knowledge and Research Centre of Complementary and
Alternative Medicine (ViFAB) in collaboration with Center for Cross-Scientific Evaluation Studies
on Complementary and Alternative Medicine (CCESCAM) at University of Southern Denmark and
Aarhus University as well as a stipend from Aarhus University.
Correspondence concerning this article should be addressed to Heidi Frølund Pedersen, Department
of Psychology, Aarhus University, 8000 Aarhus C, Denmark. E-mail: [email protected]
2
Abstract
Negative religious coping, e.g. religious struggles, has been associated with deleterious effects on
health and well-being. Yet, few studies have examined the possible psycho-social factors associated
with religious struggles. In this present study we examined the associations between the presence of
religious struggle and personal dispositions (personality traits and adult attachment style), religious
factors (religious beliefs, church attendance, and private religious activities), social factors (social
support and congregational support), situational factors (negative events and impact of event on
quality of life), and socio-demographic factors (age, gender, education, marital status, and income)
in a group of middle-aged and elderly community dwelling Danes exposed to major negative life
events. Results suggested that between 9% and 24% of the total sample reported religious struggle
to some degree. Multiple logistic regressions indicated that the presence of religious struggle was
associated with: higher levels of neuroticism (OR: 1.08, 95% CI: 1.04-1.12, p < 0.01) and reporting
higher levels of congregational support (OR: 2.7, 95% CI: 1.45-6.02, p < 0.01). The results are
discussed in relation to the secular culture of Denmark.
Keywords: Religious struggle, negative life event, neuroticism, god concept, secular

3
Several studies have explored the associations between spirituality and health, and in general the
results indicate beneficial effects of spirituality on physical and mental health (Koenig, King, and
Carson, 2012). However, spirituality may also be a source of problems. In recent years, measures of
spirituality have been refined especially in the area of religious coping (Pargament, Smith, Koenig,
& Perez, 1998), and several studies across diverse populations have revealed potential harmful
effects of engaging in negative religious coping, e.g. religious or spiritual struggles (hereafter
referred to as religious struggles) (Exline, 2013). Religious struggles are defined as questions,
tensions, and conflict about religious and spiritual issues concerning one’s God, interpersonal
relationships, and oneself (Pargament, Murray-Swank, Magyar, & Ano, 2005). The construct of
religious struggles has been examined using the negative subscale of the Brief RCOPE, a religious
coping measure developed by Pargament and collegues (1998), which mainly covers divine
struggles such as thoughts of being punished by God and feelings of abandonment, but also
interpersonal struggles covering concerns about abandonment from one’s congregation. Overall, it
has been found that religious struggles are negatively associated with physical and mental health. In
a meta analysis on 49 studies, modest but significant associations (effect size of 0.22) were found
between religious struggles and higher levels of psychological distress during negative events (Ano
& Vasconcelles, 2005). Literature reviews of studies among cancer patients also suggest measures
of negative religious coping to be associated with lower levels of quality of life (QoL) and greater
emotional distress (Lavera & O’Hea, 2010; Thuné-Boyle, Stygall, Keshtar, & Newman, 2006). It
has been argued that religious struggles is not harmful per se, but can also be a source of post
traumatic and spiritual growth (Gerber, Boals, & Schuettler, 2011), but studies are few and results
are contradicting (Exline, 2013). Furthermore, studies suggests that prolonged religious struggles
are at risk of turning chronic and have even more devastating impact on health in terms of poorer
adjustment to cancer over time (Exline, Park, Smyth, Carey, 2011) and increased mortality among

4
medically ill patients (Pargament, Koenig, Tarakeshwar, & Hahn, 2001). Thus, it is important to
look into which factors are associated with the development and presence of religious struggles in
order to better understand the phenomenon and possible prevent the struggles to grow into a more
chronic states.
Predictors of religious struggles
A growing number of studies encompass potential risk factors for developing religious
struggles, and theoretical models have been developed and tested to better understand which factors
may be associated with religious struggles. According to Pargament (1997), particular coping
strategies are chosen if they are available and compelling to the individual. Our general orienting
system, which covers personal elements (such as personality traits and attachment style), religious
elements (such as religiousness and perceptions of the Sacred), and social elements (such as
interpersonal relationships and access to social support), determines to which degree coping
strategies are available and compelling to us. Religious struggles may stem from an orienting
system characterized by conflict, strain and weakness, but could also be activated during severe
negative life events threatening core beliefs (Ano & Pargament, 2012; Bjorck & Thurman, 2007;
Pargament, 1997). It is suggested that religious struggle should be viewed as a multidimensional
phenomenon including personality, religious factors, social factors, situational factors, and socio-
demographic factors. Studies have found religious struggles to be associated with several different
sources like individual characteristics such as neuroticism (Ano & Pargament, 2012), and insecure
attachment style (Belavich & Pargament, 2002; Schottenbauer et al., 2006). It is argued that the
individual’s relationship to God “bears striking resemblance to the child’s attachment to caregivers”
(Granqvist, 2005: 36; Kirkpatrick, 1999), and insecure attachment style may therefore be a crucial
predictor of maladaptive adjustment such as religious struggles during negative life events. In terms

5
of social predictors, religious struggle has been found among people with poor social support
(McConnell et al. 2006). Furthermore situational factors such as negative events and evaluating this
life event as uncontrollable and shaking up an individual’s life have also been linked with religious
struggles (Ano & Pargament, 2012; Exline, Park, Smyth, Carey, 2011; Schottenbauer et al. 2006).
Finally, studies including socio-demographic factors suggest that being young (Exline et al., 2011),
male (Hvidtjørn, Hjelmborg, Skytthe, Christensen, & Hvidt, 2013), and unmarried (McConnell,
Pargament, & Ellison, 2006) is associated with greater religious struggles. However, relatively few
studies are currently available on psycho-social factors associated with religious struggles in more
secular contexts.
A universal or culture-specific phenomenon?
So far, the majority of studies on spirituality and health have been conducted in North
America, which has been characterized as being far more religiously oriented than, for instance,
Denmark (Zuckerman, 2008). In Denmark, religion is characterized as fragmentized and highly
individualized (Iversen, 2006), but it is unclear whether religious struggles are prevalent among
Danes. It is argued that secular individuals may to a higher degree be challenged when adjusting to
stressful life events because they lack coherent and functional world views (Stålhandske, Ekstrand,
& Tyden, 2011). On the other hand, they may not experience struggles in relation to religious issues
if they do not embrace religion as important in everyday life (la Cour, 2005). Researchers have
argued that aspects of religious struggles such as feeling abandoned by God or a higher power may
represent a universal existential void occurring during deep crisis and depression (Braam, et al.,
2010). In their study of a multi-ethnical sample (including Muslims and more secular Dutch
citizens), Braam and colleagues found that the strongest predictor of depression, independently of
the participants’ religious background, was the negative coping strategy of “feeling abandoned by

6
God”. Studies from the U.S. indicate that religious struggle may also appear among less religious
individuals (Exline, Park, Smyth, Carey, 2011) and recent research on spirituality and health in
Denmark (Pedersen, Pargament, Pedersen, Zachariae, 2013; Pedersen, Pedersen, Pargament, &
Zachariae, 2013), suggests that religious struggles are prevalent among Danes when dealing with
negative life events such as severe lung disease or bereavement, and that religious struggles may
pose a threat to well-being as negative religious coping was associated with lower quality of life
among lung disease patients. Due to increased individualization and fragmentation of religion in
Western world (Bellah, Madsen, Sullivan, Swidler, & Tipton, 1985; Pargament, Mahoney, Exline,
Jones, & Shafranske, 2013) information about what predicts religious struggles in a more secular
society like Denmark may add important information to international research on the phenomenon
of religious struggles.
In the present study we wanted to test the model suggested by Ano & Pargament (2012),
adding socio-demographic factors to the model, and explore which factors are associated with
religious struggles among people living in secular societies. The aim of the present study was to
explore the association between different psycho-social factors and religious struggles (negative
religious coping) during times of distress in a sample of middle-aged and elderly Danes. It was
hypothesized that a negative religious coping style would be associated with religious factors, i.e.
general religiousness, personality factors, i.e. insecure adult attachment style and neuroticism, social
factors, i.e. low social and congregational support, and situational factors, i.e. negative events and
the impact of negative events on QoL.
Method
Procedure
The present study was part of a larger study focusing on the use of complementary and
alternative medicine (CAM) and religiosity among Danish chronically ill lung disease patients. The
7
sample used in the present study was established as a control group socio-demographically matched
with a sample of chronically ill lung patients. The sample was established by Statistics Denmark, a
government agency with access to a wide range of national registries, including the Central Person
Registry (CPR). All Danish residents are given a CPR number, enabling retrieval of information
for research purposes. In all, 11 individuals per patient in the original study matched on age,
gender, education level, and region were selected from the CPR-registry. The resulting 1.437
potential participants were mailed a questionnaire during March 2010 and asked to complete and
return the questionnaire. Those who did not return the questionnaire within 2 weeks were mailed a
single reminder. In all, 498 responded (response rate = 34.7%). Of these, 45 were excluded due to
insufficient data, resulting in a total sample of 453 respondents.
Measures
Negative life events. An adjusted version of the List of Recent Events (LRE) (Henderson,
Byrne, & Duncan-Jones, 1981) was used to access the presence and psychological impact of major
life events during the last 12 months among the participants. The listed events included: (a) illness,
injury, and accident, (b) bereavement, (c) pregnancy or abortion, (d) changes in relationships, (e)
living conditions, (f) education, (g) employment, and (h) finances and legal difficulties. The
category of pregnancy or abortion was excluded, as this item did not seem relevant to the present
sample due to their mean age (mean 67.9, SD 9.7). The response format of the question “Have you
within the past 12 months experienced [event]?” was Yes or No for each event. For the items
“Illness, injury, and accident” and “Bereavement,” the questions were worded: “Have you or one of
your closest relatives experienced [event]?” For each event, participants were asked to indicate to
what degree this event had a negative influence on their QoL on a 5-point Likert scale from 1: (Not
at all) to 5: (Very much), resulting in an impact of event score. A categorical variable called

8
“negative events group” was created to distinguish between participants reporting a negative event
with high negative impact on QoL, participants reporting a negative event with low negative impact
on QoL, and participants not specifying a negative event: Participants scoring above 2 on the impact
of events score were categorized as the high impact group (value=3), participants scoring below 3
on the impact of event scores were categorized as the low impact group (value = 2), and participants
not specifying an event was categorized as the non-specified event group (value=1).
Religious struggles. Negative religious coping was measured using the negative subscale
of the Brief RCOPE (Pargament, Smith, Koenig & Perez, 1998), a 7-item measure of the degree to
which individuals interpret their situation as a punishment or abandonment by God (“Wondered
whether God had abandoned me”). This scale is often referred to as a religious or spiritual struggle
scale, because it is taken to reflect a religious system in tension or turmoil (Pargament et al., 2005).
The response format is a 4-point Likert scale ranging from 0 (Not at all) to 3 (A great deal), and a
total score is calculated. Internal consistency (Cronbach’s alpha) was 0.60 for the negative religious
coping scale in the present sample. Omitting item 7“Questioned the power of God” increased
Cronbach’s alpha to 0.71. An unpublished qualitative validation study of the Brief RCOPE
conducted by the first author suggested that non-religious people and atheists often answer this last
item “Questioned the power of God” with “Very much.” Not because they have religious struggles,
but simply because they want to declare their disbelief in God. On this background, we chose to
omit this item from the analysis, although this particular item has previously been found to be one
of the most commonly endorsed religious struggles among cardiac patients with symptoms of acute
coronary syndrome (Magyar-Russell et al., submitted for publication) and among diabetic,
congestive heart failure, and oncology patients (Fitchett et al., 2004) in the United States.
Thus, the final measure consisted of 6 items covering negative religious coping strategies.
When answering the religious coping items, participants were asked to think of the most negative

9
life event they reported. Those who did not specify a negative event were asked to answer how they
usually cope with major challenges. The data were positively skewed and we therefore chose to
dichotomize the scale into: 1: Religious struggle = all values above 0, and 0: No religious struggle
= 0.
Socio-demographic factors.
Socio-demographic information included: age, gender, marital status (dichotomized into
married/cohabiting and widowed/ divorced/ single), highest education level (dichotomized into Low
education = 7-10 years and High education = > 10 years), and socio-economical status (annual
house income).
Personality factors
Personality traits. Personality traits were measured by the NEO Five Factor Inventory including 62
items (NEO-FFI, Costa & MaCray, 1992), which covers the five-factor model of personality traits.
The NEO FFI consists of 5 subscales covering: Conscientiousness (“I am well known for my
judgment and common sense”), Agreeableness (“I would rather corporate than compete”),
Openness to experience (“I like to concentrate on a fantasy or daydream and let it grow and
develop”), Extroversion (“I am a happy and cheerful person”), and Neuroticism (“I often feel tense
and jittery”). Respondents indicated the degree to which they agreed with each statement on a five-
point Likert scale ranging from 1 = strongly disagree to 5 = strongly agree. A total score was
calculated for each subscale by summing the responses. In the present sample, the internal
consistency (Cronbach’s alpha) was: 0.74 for conscientiousness, 0.72 for agreeableness, 0.67 for
openness to experience, 0.81 for extroversion, and 0.84 for neuroticism respectively.
Adult attachment. Adult attachment was measured by a Danish version of the Revised
Adult Attachment Scale (RAAS), an 18-item self-report scale measuring how the participants
function and feel in a relationship with a partner, someone close, and people in general, (“I feel
10
good being dependent by others”, “I think it is difficult to trust others fully”). Each statement is
rated in a five-point Likert scale from 1 (not at all characteristic) to 5 (very characteristic). The
scale is two-dimensional: 1) items assessing closeness and dependency are merged into one
dimension (α= 0.65) (O’Connor & Elklit, 2008) and 2) an anxious attachment dimension (α= 0.76).
Based on the RAAS, attachment styles corresponding to Ainsworth’s three original attachment
patterns (secure, anxious-ambivalent, and avoidant) can be generated (Collins & Read, 1990; Stein,
Jacobs, Ferguson, Allen, & Fonagy, 1998; O’Connor & Elklit, 2008). A fourth attachment pattern
corresponding to a fearful style was also calculated (Collins & Feeney, 2004). The categorical
attachment styles are categorized using the values on the dimensions of “close-dependency” and
anxious attachment; e.g., secure attached are defined as scoring high on the close-dependency
dimension and low on the anxious dimension. High is defined as being above the midpoint on the 5-
point scale, and low as below the midpoint. Thus, cut off values for the respective attachments
styles were as follow: Secure attachment style = total close-dependency > 36 + total anxious
attachment style < 18. Preoccuppied attachment style = total close-dependency > 36 + total anxious
attachment style > 18. Dismissive attachment style = total close-dependency < 36 + total anxious
attachment style < 18. Fearful attachment style = total close-dependency < 36 + total anxious
attachment style > 18. In the present study 78.6% (n= 312) were determined as exhibiting a secure
attachment style, 4% (n= 16) a preoccupied attachment style, 14.1% (n=56) a dismissive attachment
style, and 3.3% (n=13) a fearful attachment style. Due to small numbers in two of the groups, we
chose to collapse the insecure attachment styles (preoccupied, dismissive, and fearful) into one
category (0 = Insecure) to be compared with the securely attached (1= Secure).
Religious factors
General religiousness. Public religious activity was assessed by a single item asking about
church attendance and/or attendance at other religious meetings: “How often do you attend church
11
or other religious services?” Private religious activity was measured by a single item about the
frequency of prayer, meditation, and/or scripture readings: “How often do you engage in religious
activities like prayer, meditation, or scripture reading?” Response options to both measures were
5-point Likert scales ranging from 1 (Never), 2 (A couple of times year), 3 (A couple of times a
month), 4 (Weekly), and 5 (Every day).
Religious beliefs. According to the European Value Survey (2008) seven out of ten Danes
characterize themselves as a believing person, however only 22% believe in a personal God and
35% believe in a higher spiritual power. We therefore developed five distinct items in the attempt of
accommodating people who neither believe in God or spiritual power. Participants were asked to
categorize themselves into one of five categories: 1) “I consider myself a believer. I believe in
God”, 2) “I consider myself a believer. I believe in a higher, spiritual being”, 3) “I consider myself
a believer. My beliefs concerns being part of a cultural/historical community, and I do not believe
in God or a higher, spiritual being”, 4) “I consider myself a non-believer, but would not reject the
possibility that a god or a higher, spiritual being exists”, and finally 5) “I consider myself an
atheist”.
Social factors. Social support. Social support was measured by the Social Well-being
subscale from a revised version of the FACT-G (Cella, Tulsky, Gray, Sarafian, Linn, Bonomi,
Silberman, Yellen, Winicour, Brannon et al., 1993) (“I feel close to my friends”, “I get emotional
support from my family/my nearest”, “I get support from my friends”, and “I feel close to my
partner (or the person that is my best support)”. Responses are given on a 5-point Likert scale
ranging from 1 = Not at all to 5 = Very much.
Congregational support. Congregational support was measured by a single item: “To what
degree do you receive support from your fellow believers” using the format: 2 = Yes, 1 = No, or 0 =
12
Not relevant. The score was then dichotomized into 1 = Congregational support and 0 = No
support.
Statistical analysis
Mean substitution was used to handle missing data on continuous variables as suggested by
Schafer and Graham (2002). This procedure is adequate and preferable to procedures such as list-
wise deleting or scale mean substitution. Chi square tests were conducted for the categorical
variables (gender, education, marital status, attachment, religious beliefs, congregational support,
and negative life events) possibly associated with the dependent variable: negative religious coping.
Spearman correlations were run for continuous variables (age, income, the five personality factors,
church attendance, private religious activity, and social support) possibly associated with negative
religious coping. The variables that were significant in the initial Chi-square tests and correlation
analyses were tested in five independent unadjusted regressions testing socio-demographic factors,
personality factors, religious factors, social factors, and situational factors. Variables that were
statistical significant at p < 0.1 in the five independent regression models were tested in a final
logistic regression, and the significance level was set at p < 0.05.
Results
Sample
Of the 453 participants, 113 did not answer the religious coping items and were excluded
from the analyses. One-way ANOVAS and chi square tests suggested non-responders to be mostly
people who did not specify a negative event, were older, had lower income, and went to church
more often than responders. A total of 340 participants were included in the analyses. The majority
was male (53.8%), and the mean age of the participants was 67.8 years (range 42 – 90 years, SD
13
9.6). The majority were married (79.5%), had fewer than 11 years of education (72.4%), and the
average annual house income was $52.000-$70.000. In terms of religious factors most (87.8%)
identified themselves as Christians and 91.8% were members of the National Church. When asked
about their beliefs, 52.1% of the sample considered themselves to believe in God (theists), 12.4%
considered themselves to believe in a higher, spiritual being (spiritual), 8.5% considered themselves
believers, but not believing in God or a higher, spiritual being (secular believer), 20.3% considered
themselves to be non-believers (non-believers), and 5.3% considered themselves to be atheists
(atheists), while the remaining 1.5% did not specify their belief. Only 3% attended church weekly,
10.9% attended church once or more a month, 60.1% a couple of times a year, while 26% of the
sample answered that they never attended church.
Negative events and religious struggles
In all, 174 referred to a specific negative event when answering the religious coping items
with 51.7% reporting this event to be an illness or accident, 15.5% bereavement, and 32.6% other
negative events, e.g. divorce or financial problems. Of the 174 reporting a specific event, 119
characterized the specified negative event to have a high negative impact on their quality of life and
is referred to as the high impact group, whereas 55 reported the event to have low or no impact on
their quality of life and is referred to as the low impact group. A total of 166 did not specify any
negative event or the impact of event, when answering the religious coping items and is referred to
as the non-specified event group. In the high impact group, 24.4% reported to experience religious
struggle in relation to the event to some degree (mean=0.75, SD=1.78). In the low impact group,
9.1% expressed religious struggles in relation to the event to some degree (mean=0.13, SD=0.47),
and in the non specified event group, 22.9% reported religious struggles to some degree
(mean=0.69, SD=1.67).
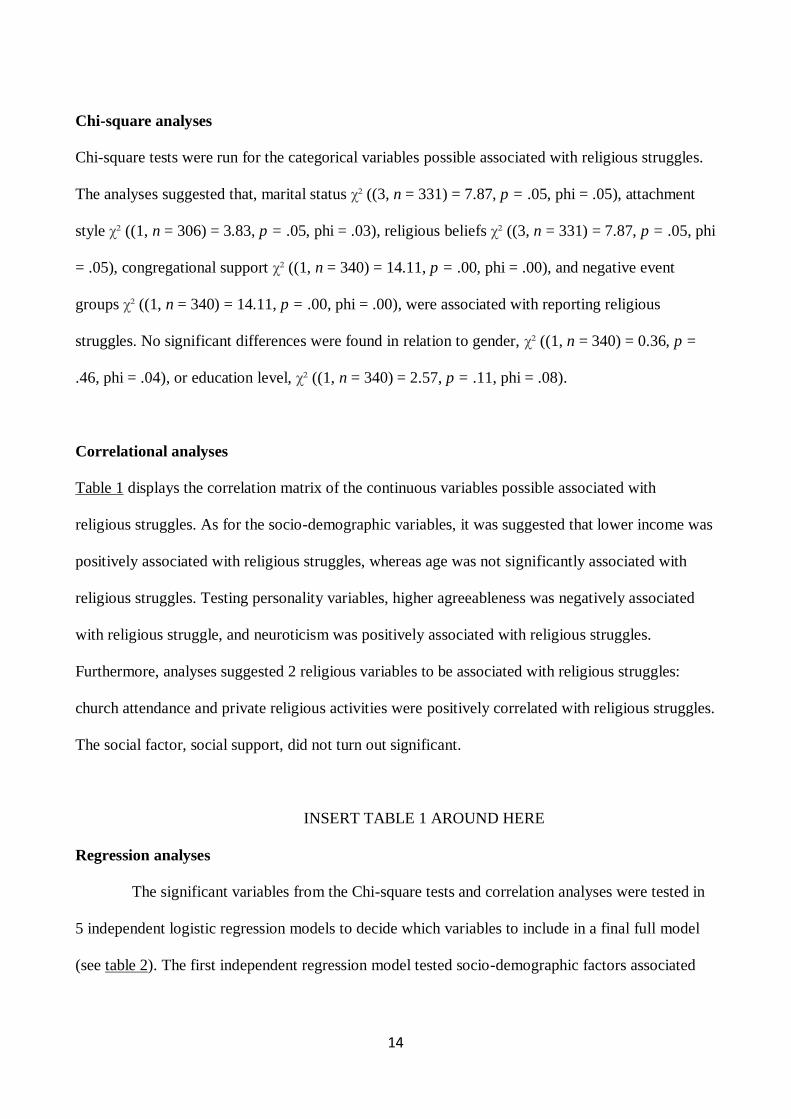
14
Chi-square analyses
Chi-square tests were run for the categorical variables possible associated with religious struggles.
The analyses suggested that, marital status χ² ((3, n = 331) = 7.87, p = .05, phi = .05), attachment
style χ² ((1, n = 306) = 3.83, p = .05, phi = .03), religious beliefs χ² ((3, n = 331) = 7.87, p = .05, phi
= .05), congregational support χ² ((1, n = 340) = 14.11, p = .00, phi = .00), and negative event
groups χ² ((1, n = 340) = 14.11, p = .00, phi = .00), were associated with reporting religious
struggles. No significant differences were found in relation to gender, χ² ((1, n = 340) = 0.36, p =
.46, phi = .04), or education level, χ² ((1, n = 340) = 2.57, p = .11, phi = .08).
Correlational analyses
Table 1 displays the correlation matrix of the continuous variables possible associated with
religious struggles. As for the socio-demographic variables, it was suggested that lower income was
positively associated with religious struggles, whereas age was not significantly associated with
religious struggles. Testing personality variables, higher agreeableness was negatively associated
with religious struggle, and neuroticism was positively associated with religious struggles.
Furthermore, analyses suggested 2 religious variables to be associated with religious struggles:
church attendance and private religious activities were positively correlated with religious struggles.
The social factor, social support, did not turn out significant.
INSERT TABLE 1 AROUND HERE
Regression analyses
The significant variables from the Chi-square tests and correlation analyses were tested in
5 independent logistic regression models to decide which variables to include in a final full model
(see table 2). The first independent regression model tested socio-demographic factors associated
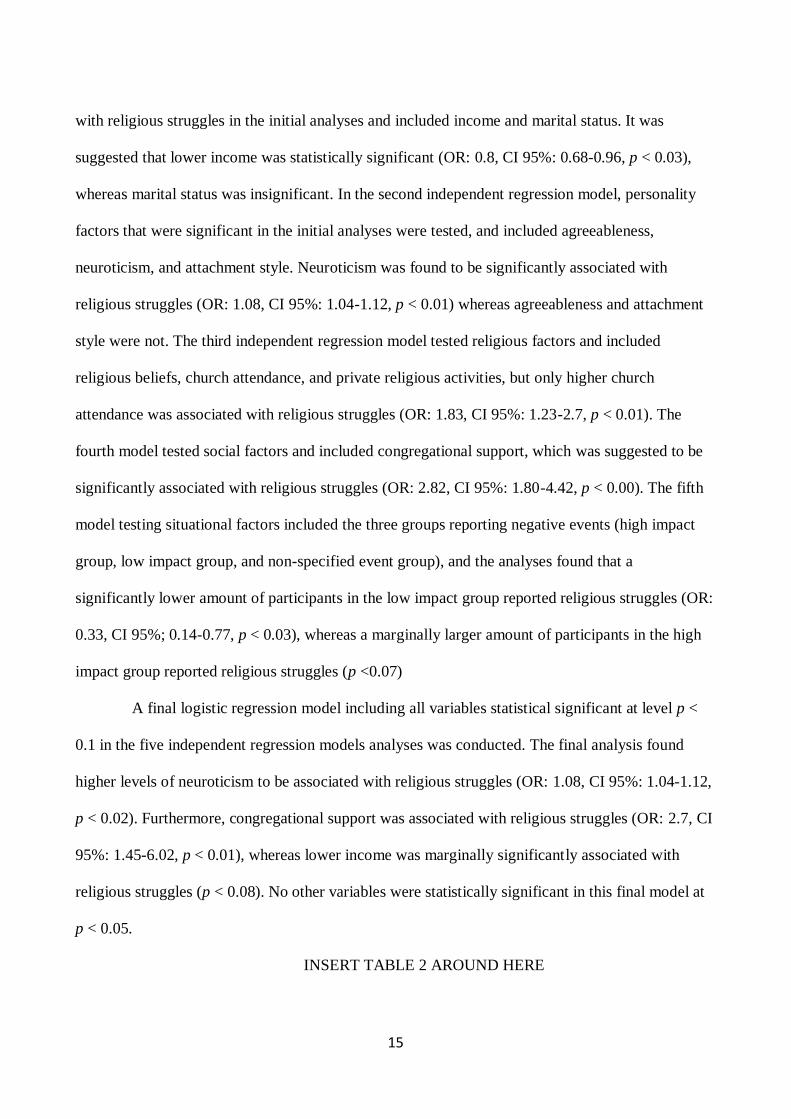
15
with religious struggles in the initial analyses and included income and marital status. It was
suggested that lower income was statistically significant (OR: 0.8, CI 95%: 0.68-0.96, p < 0.03),
whereas marital status was insignificant. In the second independent regression model, personality
factors that were significant in the initial analyses were tested, and included agreeableness,
neuroticism, and attachment style. Neuroticism was found to be significantly associated with
religious struggles (OR: 1.08, CI 95%: 1.04-1.12, p < 0.01) whereas agreeableness and attachment
style were not. The third independent regression model tested religious factors and included
religious beliefs, church attendance, and private religious activities, but only higher church
attendance was associated with religious struggles (OR: 1.83, CI 95%: 1.23-2.7, p < 0.01). The
fourth model tested social factors and included congregational support, which was suggested to be
significantly associated with religious struggles (OR: 2.82, CI 95%: 1.80-4.42, p < 0.00). The fifth
model testing situational factors included the three groups reporting negative events (high impact
group, low impact group, and non-specified event group), and the analyses found that a
significantly lower amount of participants in the low impact group reported religious struggles (OR:
0.33, CI 95%; 0.14-0.77, p < 0.03), whereas a marginally larger amount of participants in the high
impact group reported religious struggles (p <0.07)
A final logistic regression model including all variables statistical significant at level p <
0.1 in the five independent regression models analyses was conducted. The final analysis found
higher levels of neuroticism to be associated with religious struggles (OR: 1.08, CI 95%: 1.04-1.12,
p < 0.02). Furthermore, congregational support was associated with religious struggles (OR: 2.7, CI
95%: 1.45-6.02, p < 0.01), whereas lower income was marginally significantly associated with
religious struggles (p < 0.08). No other variables were statistically significant in this final model at
p < 0.05.
INSERT TABLE 2 AROUND HERE
16
Discussion
This present study explored the prevalence of religious struggles in a group of middle-aged
and elderly community-dwelling people living in a secular society, and tested a multidimensional
model of possible psycho-social factors associated with religious struggles, which included socio-
demographic variables, personality variables, religious variables, social variables, and situational
variables. The results suggested that the question of religious struggles is not trivial, even among
people who live in what has been characterized as the most secular society in the world
(Zuckerman, 2008). Between 9% and 24% of the sample reported that they engaged in one or more
of the negative religious coping styles, e.i. religious struggles. In addition, the model established by
Ano & Pargament (2012) appeared useful as a framework for exploring different psycho-social
factors associated with religious struggles, although remarkably few variables stood out as
predictors of religious struggles in the final multidimensional model. In the initial analyses it
appeared that participants having fewer secular resources (low income), fewer psychological
resources (neuroticism and insecure attachment style), being more religious active (high frequency
of church attendance and private religious practice), receiving support from their congregation, and
experiencing highly negative events expressed more religious struggles. In the final model only
neuroticism and receiving congregational support significantly predicted religious struggles,
whereas lower income was marginally significant. Several explanations may be suggested for the
role of lower income, neuroticism, and congregational support.
Socio-demographic factors
The only socio-demographic predictor that reached marginal significance in the final model
was lower income, and it may tentatively be suggested in line with other studies (McConnell,
Pargament, Ellison, & Flannelly, 2006) that people having fewer secular resources are more
vulnerable when faced with major life events and prone to religious struggles. However, no other
17
socio-demographic factors were associated with religious struggles. A Danish study suggests
religiously oriented men to report more negative religious coping (Hvidtjørn et al, 2013), whereas
another study suggests women to lose interest in religion when illness grow worse, which could
indicate religious struggles (la Cour, 2008). Neither of these contradictory patterns were confirmed
in this present study and more studies are needed to clear out possible gender differences during
different circumstances.
Personality characteristics
Neuroticism was one of two significant predictors of religious struggles in the final model
and suggests that religious struggles reflect an orienting system in tension and strain. Neuroticism
may affect how ones religiosity is expressed; that is the neurotic disposition may cause one’s
religious beliefs to become a source of religious struggle instead of a source of comfort and support,
and a previous meta-analysis (Saroglou, 2002) found neuroticism to be associated with lower levels
of open, mature spirituality. Neuroticism was also found to be a predictor of religious struggles in
the study of Ano & Pargament (2012) among college students dealing with negative life events, and
another study found that neuroticism was associated with greater disappointment and anger at God
(Wood et al. 2010). Thus, several studies link neuroticism to negative forms of religiosity during
distress and suggest that personality traits is a crucial factor to include when examining the
efficiency of religious beliefs in adjustment. In fact, researchers in trait psychology criticize
researchers engaging in studies on stress and coping for not taking individual differences more into
account when explaining associations between stressors and different coping strategies (Costa,
Somerfield, & McCrae, 1996). It is argued that personality traits affect thoughts, feelings, and
actions far more than any other personality disposition and according to Bolger’s (1990) “coping is
personality in action under stress” (p. 525). A study by Costa, Somerfield, & McCrae (1996) found
people high in neuroticism to react badly to stress and engage in blaming themselves and others.
18
This may also be the case among people engaging in religious struggles who interpret a negative
event as God’s punishment. Furthermore, a review of meta-analyses on personality traits studies
suggests that personality traits like neuroticism are far stronger predictors of psychological
outcomes than any other individual characteristics (Steel, Smith, & Shulz, 2008). This may explain
the few significant associations tested in regression model. Furthermore, since the negative subscale
of Brief RCOPE reflects a mainly insecure relationship to God, it was expected that attachment
style would be a fairly strong predictor of religious struggles. Other studies have found the insecure
attachment style to be associated with negative religious coping (Schottenbauer et al. 2006), and
recently Granqvist, Hagekull, and Ivarsson (2012) suggested that especially disorganized
attachment style may be associated with viewing God as aberrant and frightening. However, the
applied measure of attachment relied on adult attachment style, and it may be argued that a measure
of parental attachment style is more appropriate to apply when studying attachment in relation to
religious coping as was the case in a study by Granqvist (2005).
Religious and social predictors
In the initial analyses religious beliefs, church attendance, and prayer were associated with
religious struggles, indicating that the more religiously oriented engage in these coping strategies.
In the final regression none of the religious identifiers were associated with religious struggles,
However, the final model also included congregational support, which was significantly associated
with religious struggles, and may to a high degree be correlated by church attendance; a variable
included in the final model but did not turn out significant. This finding suggests that the
participants experiencing religious struggles turned to their fellow believers for support during
times of distress. However, since relatively few Danes engage themselves in church attendance and
their congregation, congregational support could also be interpreted as a religious indicator. More
studies are needed to clarify this.

19
Situational factors
It was predicted that perceiving a negative event as having a highly negative impact on
QoL would be associated with religious struggles. Studies have found that the more an event is
perceived as shaking up one’s world, the more likely it is that struggle occurs (Ano & Pargament,
2012), and a recent Danish study suggests that more traumatic events such as losing a child or a
spouse is associated with higher levels of negative religious coping (Hvidtjørn, Hjelmborg,
Skytthe, Christensen, & Hvidt, 2013). The initial analyses suggested this to be somewhat true, as
the low impact event group was less likely to report religious struggles. However, nearly half of
the sample (N=166) did not choose a specific event when responding to the negative religious
coping questionnaire, and thereby they did not rate the impact of event. Thus, it was not possible
to determine the gravity of the non-specified negative events. It is likely that the participants in the
non-specified event group thought of events that did not lie within the frame of the last 12 months
as instructed. These events may have been perceived as having a highly negative impact on QoL,
but yet not rated in the questionnaire. To be able to use the information on the impact of event
among the participants who specified a negative event, and include the participants not specifying
an event, it was decided to create a category that distinguished between high impact events, low
impact events, and non-specified events. Thus, a lot of information was missing for the non-
specified event group and a type 2 error is possible to have occurred – that is, had they specified
an event, an effect might truly be present, but is not found significant in the statistical analysis due
to the missing information. It may also be argued, that the non-specified event group did not pick
a severe event but thought of how they usually handle major challenges when responding to the
items about religious coping. Thus, they may not have experienced religious struggles when
thinking about everyday challenges. However, the mean value of negative religious coping was
relative close to the high impact group, indicating that they did not differ significantly. Future

20
studies should be careful to measure more precisely the negative events that are recalled and use
indicators of the subjectively perceived gravidity of the event to decide whether the severity of
events predicts religious struggles. Furthermore, it may also be argued that situational factors
could potentially have mediated or moderated the associations between individual differences and
religious struggles: For example it is likely that the perceived impact of event on QoL could have
mediated the association between personality dispositions such as neuroticism or attachment style
and religious struggles (Schottenbauer et al, 2006a), and future studies could benefit by applying
more sophisticated models of analyses like structural equation modeling to investigate possible
mediators and moderators of religious struggles.
Limitations
This present study was conducted among a group of middle-aged and elderly Danes, and
the question of generalizability of results to younger generations is relevant. It has been argued that
especially elderly people are more likely to be more religious (Andersen, Ausker & la Cour, 2011)
and religious beliefs may also be more traditionalistic among elderly people. Thus, we do not know
whether major negative life events evoke religious struggles among younger individuals where
religious upbringing becomes more seldom (Mørk & Ausker, 2007). It may be argued that lack of
religious concepts and language leave the individual to fend for himself to find meaning and way
through crisis (DeMarinis, 2008). On the other hand, if religion is not a part of one’s orienting
system, it may not suddenly turn up during crisis and become the object of doubt and struggle.
Future studies will explore these topics. Furthermore, this present study used a cross-sectional
design and thereby causal relationships cannot be explored, and longitudinal studies are called for.
Despite limitations this present study adds to the empirical research about the psycho-social factors

21
associated with religious struggles with information from a more secular region and suggests that
especially personality factors are important to pay attention to in future studies.

22
References
Allingham, S. (2006). http://www.religion.dk/artikel/29955:Guide--Hvad-er-en-kulturkristen, 1st of
August
Ano, G. G., & Vasconcelles, E. B. (2005). Religious coping and psychological adjustment to stress:
A meta-analysis. Journal of Clinical Psychology, 61(4), 461-480. doi:10.1002/jclp.20049
Ano, G.G., & Pargament, K.I. (2012). Predictors of spiritual struggles: an exploratory study. Mental
Health, Religion, and Culture. Advance online publication.
doi:10.1080/13674676.2012.680434
Belavich, T.G. & Pargament, K.I. (2002). The Role of Attachment in Predicting Spiritual
Coping With a Loved One in Surgery. Journal of Adult Development, 9, (1): 13-29
Bellah, R.N., Madsen, R., Sullivan, W.M., Swidler, A., & Tipton, S.M. (1985). Habit of heart:
Individualism and commitment in American life. New York, NY: Harper & Row
Bjorck, J.P., & Thurman, J.W. (2007). Negative life events, patterns of positive and negative
religious coping, and psychological functioning. Journal for the Scientific Study of Religion,
46 (2), 159-167. Doi:
http://dx.doi.org.ez.statsbiblioteket.dk:2048/10.1111/j.1468-5906.2007.00348.x
Bolger, N. (1990). Coping as a personality process: A prospective Study. Journal of Personality
and Social Psychology, 59 (3): 525-537
Braam, A.W, Schrier, A.C., Tuinebreijer, W.C., Beekman, A.T.F., Dekker, J.J.M. & de Wit, M.A.S,
(2010). Religious coping and depression in multicultural Amsterdam: A comparison
between native Dutch citizens and Turkish, Maroccan and Surinamese/Antillean migrants.
Journal of Affective Disorders, 125, pp. 269-278
23
Cella, D.F., Tulsky, D.S., Gray, G., Sarafian, B., Linn, E., Bonomi, A., & Brannon, J. (1993). The
functional assessment of cancer therapy scale: Development and validation of the general
measure. Journal of Clinical Oncology, 11(3), 570-579. http://jco.ascopubs.org/
Collins, N.L. & Feeney, B.C. (2004). Working models of attachment shape perceptions of social
support: Evidence from experimental and observational studies. Journal of Personality &
Social Psychology, 87: 363-383
Collins, N.L. & Read, S.J. (1990). Adult attachment, working models, and relationship quality in
dating couples. Journal of Personality and Social Psychology, 58: 644-663
Costa, P.T., & McCrae, R.R. (1992). Normal personality assessment in clinical practice: The NEO
Personality Inventory. Psychologival Assessment, 4 (1): 5-13
Costa, P. T., Somerfield, M. R., McCrae, R. R. (1996). Personality and Coping: A
Reconceptualization. In: M. Zeidner & N. Endler (Ed.), Handbook of Coping: Theory,
Research, Applications. John Wiley & Sons, Inc: New York.
DeMarinis, V. (2008). The Impact of Postmodernization on Existential Health in Sweden:
Psychology of Religion’s Function in Existential Public Health Analysis. Archieve for the
Psychology of Religion, 30: 57-74
Exline, J.J., Park, C.L., Smyth, J.M., & Carey, M.P. (2011). Anger toward God: Social-cognitive
predictors, prevalence, and links with adjustment to bereavement and cancer. Journal of
Personality and Social Psychology, 100 (1), 129-148. doi:10.1037/a0021716
Exline, J. (2013). Religious and spiritual struggles. In: K.I. Pargament, Exline, J., & Jones, J.W.
(Eds). APA Handbook of Psychology, Religion, and Spirituality. Volume 1. American
Psychological Association. Washington D.C.

24
Fitchett, G., Murphy, P.E., Kim, J., Gibbons, J., Cameron, J.R., & Davis, J.A. (2004). Religious
struggle: Prevalence, correlates and mental health risks in diabetic, congestive heart failure,
and oncology patients. International Journal of Psychiatry in Medicine, 34, (2), 179-196
Granqvist, P. (2005). Building a bridge between attachment and religious coping: tests of
moderators and mediators. Mental Health, Religion, and Culture, 8 (1): 35-47. doi:
10.1080/13674670410001666598.
Granqvist, P., Hagekull, B., & Ivarsson, T. (2012). Disorganized attachment promotes mystical
experiences via a propensity for alterations in consciousness (absorbtion). The International
Journal for the Psychology of Religion, 22: 130-197. doi: 10.1080/10508619.2012.670012
Gerber, M.M., Boals, A., & Schuettler, D. (2011). The unique contributions of positive and
negative religious coping to posttraumatic growth and PTSD. Psychology of Religion and
Spirituality, 3(4) pp. 298-307. doi: 10.1037/a0023016
Henderson, S., Byrne, D.G, & Duncan-Jones, P. (1981). Neurosis and the social environment.
Sydney: Academic Press.
Hvidtjørn, D., Hjelmborg, J., Skytthe, A., Christensen, K., & Hvidt, N.C. (2013). Religiousness and
Religious Coping in a Secular Society: The Gender Perspective. Journal of Religion and
Health, doi: 10.1007/s10943-013-9724-z
Iversen, H.R. (2006). Secular Religion and Religious Secularism: A profile of the religious
development in Denmark since 1968. Nordic Journal of Religion and Society, 19 (2), pp.
75-92
Kirkpatrick, L. A. (1999). Attachment and religious representations and behavior. In Handbook of
attachment theory and research, J. Cassidy, & P. R. Shaver (Eds), pp. 803–822. NY:
Guilford.
25
Koenig, H.G., King, D., and Carson, V.B. (eds.) (2012). Handbook of Religion and Health. Oxford
University Press, New York
La Cour, P. (2005). Danskernes Gud i krise. In M.T. Højsgaard & H.R. Iversen (Eds.), Gudstro i
Danmark (pp. 59 – 82). København: Anis.
Lavera, M.E. & O’Hea, E.L. (2010). Religious/spiritual coping and adjustment in individuals with
cancer: Unanswered questions, important trends, and future directions. Mental Health,
Religion, and Culture, 13(1): 55-65
Magyar-Russell, G., Brown, I.T., Idara, I., Smith, M.T., Marine, J.E. & Ziegelstein, R.C. In Search
of Serenity: Religious Struggle among Patients Hospitalized for Acute Coronary Syndrome.
Manuscript submitted for publication
McConnell, K.M., Pargament, K.I., & Ellison, C.G., Flannelly, K.J. (2006). Examining links
between spiritual struggles and symptoms of psychopathology in a national sample.
Journal of Clinical Psychology, 62: 1469-1484. doi: 10.1002/jclp.20325
O’Connor, M. & Elklit, A. (2008). Attachment styles, traumatic events, and PTSD: a cross-
sectional investigation of adult attachment and trauma. Attachment & Human
Development, 10 (1): 59-71. doi: 10.1080/14616730701868597
Pargament, K.I. (1997). The psychology of religion and coping. Theory, research, practice. New
York, NY: Guildford.
Pargament, K.I., Desai, K.M., & McConnell, K.M. (2006). Spirituality: A pathway to post-
traumatic growth or decline? In: L.G. Calhoun & R.G. Tedeschi (Eds.), The handbook of
post-traumatic growth: Research and practice, (pp. 121-137). Mahwah, NJ: Erlbaum.
Pargament, K.I., Koenig, H.G., Tarakeswar, N., & Hahn, J. (2001). Religious struggle as a predictor
of mortality among medically ill elderly patients: A 2 year longitudinal study. Archives of

26
Internal Medicine, 161, 1881-1885. doi:10-1001/pubs.Arch Intern Med.-ISSN-0003-9926-
161-15-ioi00736
Pargament, K.I., Koenig, H.G., Tarakeswar, N., & Hahn, J. (2004). Religious coping methods as
predictors psychological, physical, and spiritual outcomes among medically ill elderly
patients: A 2 year longitudinal study. Journal of Health Psychology, 9, 713-730. doi:
10.1177/1359105304045366
Pargament, K.I., Mahoney, A., Exline, J., Jones, J.W., & Shafranske, E.P. (2013). Envisioning an
integrative paradigm for the psychology of religion and spirituality. In: K.I. Pargament,
Exline, J., & Jones, J.W. (Eds). APA Handbook of Psychology, Religion, and Spirituality.
Volume 1. American Psychological Association. Washington D.C.
Pargament, K I., Murray-Swank, N.A, Magyar, G.M., & Ano, G.G. (2005). Spiritual struggle: A
phenomenon of interest to psychology and religion. In W.R. Miller and H.D. Delaney (Eds.)
Judeo-Christian perspectives on psychology: Human nature, motivation and change, (pp.
245-68). Washington, DC: American Psychological Association. doi:10.1037/10859-013
Pargament, K.I., Smith, B.W., Koenig, H.G., & Perez, L. (1998). Patterns of positive and negative
religious coping with major life stressors. Journal of the Scientific Study of Religion, 37(4),
710-724. doi:10.2307/1388152
Pedersen, H.F., Pargament, K.I., Pedersen, C.G., & Zachariae (2013). Religious coping among
severely ill lung patients in a secular society. International Journal for the Psychology of
Religion. . International Journal for the Psychology of Religion, 23: 188-203. doi:
10.1080/10508619.2012.728068
Pedersen, H.F., Pedersen, C.G., Pargament, K.I., & Zachariae, R. (2013). Coping without religion?
Religious coping, quality of life, and existential well-being among lung disease patients and
27
matched controls in a secular society. Research in the Social Scientific Study of Religion, 24:
163-192.
Saroglou, V. (2002). Religion and the five factors of personality: A meta-analytic review.
Personality and Individual Differences, 32, 15–25
Schafer, J.L., & Graham, J.W. (2002). Missing data: our view of the state of the art. Psychological
Methods, 7, 147-177. doi:10.1037/1082-989X.7.2.147
Schottenbauer, M.A., Klimes-Dougan, B., Rodgiguez, B.F., Arnkoff, D.B., Glass, C.R., Lasalle,
V.H. (2006). Attachment and affective resolution following a stressful event: General and
religious coping as mediators. Mental Health, Religion, and Culture, 9 (5): 448-471. doi:
10.1080/13694670500440684
Steel, P., Schmidt, J., & Shultz, J. (2008). Refining the relationship between personality and
subjective well-being. Psychological Bulletin, 134 (1): 138-161. doi: 10.1037/0033-
2909.134.1.138
Stein, H., Jacobs, N.J., Ferguson, K.S., Allen, J.G., & Fonagy, P. (1998). What do adult attachment
scales measure ? Bulletin of the Menninger Clinic, 33-82
Stålhandske, M.L., Ekstrand, M, & Tyden, T. (2011). Existential experiences and strategies in
relation to induced abortion: An interview study with 24 Swedish women. Archive for the
Psychology of Religion, 33 (3): 345-370
The Danish Value Survey, 2008. Originally conducted by prof. Peter Gundelach. Data was made
available by the Danish Data Archive (archive number DDA-21432)
Thuné-Boyle, I.C., Stygall, J.A., Keshtgar, M.R., & Newman, S.P. (2006). Do religious/spiritual
coping strategies affect illness adjustment in patients with cancer? A systematic review of
the literature. Social Science and Medicine, 63: 151-164
Wood, B.T., Worthington Jr, E.L., Exline, J.J., Yali, A.M., Aten, J.D., & McMinn, M.R. (2010).
28
Development, refinement, and psychometric properties of the Attitudes Toward God Scale
(ATGS-9). Psychology of Religion and Spirituality, 2, 148–167
Zuckerman, P. (2008). Society without God. What the least religious nations can tell us about
contentment. New York, NY: NYU Press.

29
Table 1: Correlations between psycho-social variables and religious struggles
Variables 2 3 4 5 6 7 8 9 10 11
Socio-demographic factors
1. Age -.50** -.18** -.03 -.04 -0.7 -.08 .14* .18** 0.01 0.7
2. Income - .21** -.03 .25** -.16** .14* -.02 -.12* .07 -.14*
Personality factors
3. Contentiousness - .33* .09 -.62 .44 .01 -.04 .21** -.04
4. Agreeableness - -.09 -.33** .04 -.02 .10 .22** -.11*
5. Openness - -.11* .33** .05 .12* .12* -.06
6. Neuroticism - -.45** .10 .11 -.23** .26**
7. Extroversion - .04 -.04 .29** -.09
Religious factors
8. Church attendance - .51** .14* .20**
9. Private religious
activities
- .13* .15**
Social factors
10. Social support - -.08
Criterion variable
11. Negative religious
coping
-
Notes: *p < 0.05; **p < 0.01
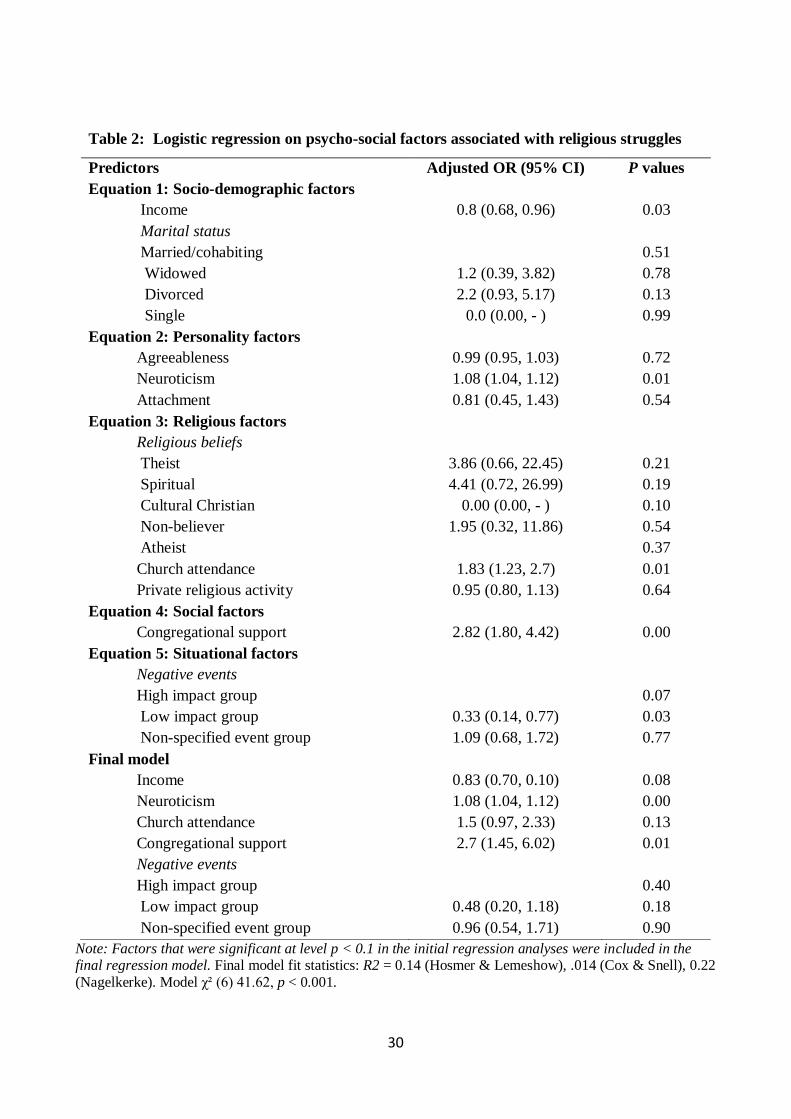
30
Note: Factors that were significant at level p < 0.1 in the initial regression analyses were included in the final regression model. Final model fit statistics: R2 = 0.14 (Hosmer & Lemeshow), .014 (Cox & Snell), 0.22
(Nagelkerke). Model χ² (6) 41.62, p < 0.001.
Table 2: Logistic regression on psycho-social factors associated with religious struggles
Predictors Adjusted OR (95% CI) P values
Equation 1: Socio-demographic factors
Income 0.8 (0.68, 0.96) 0.03
Marital status
Married/cohabiting 0.51
Widowed 1.2 (0.39, 3.82) 0.78
Divorced 2.2 (0.93, 5.17) 0.13
Single 0.0 (0.00, - ) 0.99
Equation 2: Personality factors
Agreeableness 0.99 (0.95, 1.03) 0.72
Neuroticism 1.08 (1.04, 1.12) 0.01
Attachment 0.81 (0.45, 1.43) 0.54
Equation 3: Religious factors
Religious beliefs
Theist 3.86 (0.66, 22.45) 0.21
Spiritual 4.41 (0.72, 26.99) 0.19
Cultural Christian 0.00 (0.00, - ) 0.10
Non-believer 1.95 (0.32, 11.86) 0.54
Atheist 0.37
Church attendance 1.83 (1.23, 2.7) 0.01
Private religious activity 0.95 (0.80, 1.13) 0.64
Equation 4: Social factors
Congregational support 2.82 (1.80, 4.42) 0.00
Equation 5: Situational factors
Negative events
High impact group 0.07
Low impact group 0.33 (0.14, 0.77) 0.03
Non-specified event group 1.09 (0.68, 1.72) 0.77
Final model
Income 0.83 (0.70, 0.10) 0.08
Neuroticism 1.08 (1.04, 1.12) 0.00
Church attendance 1.5 (0.97, 2.33) 0.13
Congregational support 2.7 (1.45, 6.02) 0.01
Negative events
High impact group 0.40
Low impact group 0.48 (0.20, 1.18) 0.18
Non-specified event group 0.96 (0.54, 1.71) 0.90

31

Paper 4

1
Studying religious and spiritual coping in a secular culture: A question of validity
Heidi Frølund Pedersen & Jan Tønnesvang
Department of Psychology, Aarhus University, Denmark
Submitted for Mental Health, Religion, and Culture (Summer 2013)
Author note
Heidi F. Pedersen (corresponding author), Department of Psychology, Aarhus University,
Bartholins Allé 9, 8000 Aarhus Denmark, e-mail: [email protected], telephone: 0045-87165307;
Jan Tønnesvang, Department of Psychology, Aarhus University, Bartholins Allé 9, 8000 Aarhus,
Denmark, e-mail: [email protected], telephone: 0045-87165795
2
Abstract
The present paper discuss methodological challenges when investigating religious and spiritual
phenomena like religious/spiritual coping in secular society like Denmark and adopting theoretical
concepts and measures developed in more religiously oriented societies like the U.S. The study is
based on 3 focus groups interviews (n=14) with healthy Danes and individual interviews with
Danish lung cancer patients (n=10) responding to the religious coping questionnaire, Brief RCOPE,
and a newly developed scale on spiritual coping, Brief SCOPE, and through an exploratory thematic
analysis three themes in relation to validity was found: The importance of language and the
“religious capital” of the participant when responding to measures about religiousness in secular
society, the influence of the situation-specific context when asked about religious coping, and the
question of universality versus context-specificity in the measurement of religious and spiritual
phenomena such as religious coping.
Keywords: Religious coping, secular, questionnaire, validity, qualitative
3
Historically, psychology as a scientific discipline has had an ambivalent relationship to religion.
Striving to cut loose the strings to philosophy and theology with which it shared the interest of
describing human experience, the young discipline of psychology distanced itself from these
disciplines during the first half of the 20th century (Paloutzian, 1996). Adopting a positivistic
approach to the study of the human experience, the objective methods of quantitative research let
psychology to be established as a legitimate science while distancing itself further to religion
(Emmons & Paloutzian, 2003). The psychology of religion had difficult times until the late 1960s,
because it was perceived as “unscientific” to be associated with religion, other than offering
reductive naturalistic explanations of its claim (Coon, 1992; Spilka & McIntosh, 1999), and as an
example psychology textbooks hardly included “religion” in their indexes until the 1970es (Spilka,
1981). During the last 40 years the psychology of religion has expanded, although Hood (1999)
argued that psychology of religion would never be a fully integrated part of mainstream psychology
in America, because only a few key researchers sustained the field. Furthermore, he argued that it
had little application to other cultures outside America. However, in 2003 APA published a special
issue on the psychology of religion (see for example Miller & Thoreson, 2003), which among other
things marked the turning point for the psychology of religion in America to become an integrated
part of the mainstream psychology, which uses the theoretical framework and methodology of
mainstream psychology to examine religious sentiment and behaviour (Selvam, 2011). In 2013
APA launched two handbooks on the psychology of religion (Pargament, 2013 vol. I and II)
cementing the legitimacy of the field. Part of this success may be caused by the dominating
quantitative approach for both models and methods in the psychology of religion (Gorsuch, 1984).
Especially studies on links between spirituality, religion, health, and well-being have increased
since the beginning of this century (Miller & Thoreson, 2003) and expanded to other cultures such
4
as Northern Europe (see www.faith-health.org). The area of religious and spiritual coping has
received great attention in faith and health research since Kenneth I. Pargament (1997) formulated
his transactional theory of religious coping. Studies on religious coping are almost solely
quantitatively founded, and the measure of Brief RCOPE (Pargament, Smith, Koenig & Perez,
1998) has become the religious coping measure of choice. It has a strong theoretical base, strong
psychometric properties, it links with a variety of adjustment indexes, and has been used among a
variety of samples representing different groups of medically ill patients, college students coping
with different negative life events, and different minorities (Hill & Edwards, 2013). Furthermore, it
has been revised into Jewish, Hindu, and Muslim versions and translated into different languages
such as Polish, Spanish, German, and Urdu, thereby also making this field open to cross-cultural
comparisons. Despite the apparent validity and psychometric solid base of this questionnaire,
cultural aspects of spiritual and religious experiences need to be considered carefully when adopting
measures from one culture to another (Belzen, 2010; Hood, 2010). In this present paper we discuss
the validity of measures on religion and spirituality when adapted from one culture to another based
on a qualitative study on spiritual and religious coping measured by Brief RCOPE among Danes
suffering from lung cancer and a control group of healthy Danes.
Preparing a study on religious coping – the case of learning by doing
This present study is a case of learning by doing in research humbly acknowledging that the scope
of research results is limited to the knowledge and measures available of a given time as well as the
assumptions and biases of the researcher. In 2007 a study on alternative and complementary
treatment and faith among newly diagnosed Danish lung patients (mainly lung cancer and chronic
obstructive pulmonary disease, COPD) was being prepared. At that time no validated measures of
religious coping was available in Danish. Relying on a quantitative approach, the literature was
5
reviewed systematically focusing on studies using questionnaires to investigate the associations
between religion, coping, well-being and quality of life among cancer patients. The literature
flooded with studies using all kinds of different instruments and studying all kinds of associations
between spirituality, religion, coping, and health among cancer patients. Reviews at that time
(Plante & Sherman, 2001; Thuné-Boyle, Stygall, Keshtar, & Newman, 2006) recommended using
multi-dimensional and problem specific measures to capture the research topic at hand. It became
evident that the theoretical framework developed by Pargament (1997) and the measure Brief
Religious Coping (Brief RCOPE) was widely used and recognized measure. Studies suggest that
religious coping is most likely to be prevalent and have a positive effect on well-being among
people in which religious belief is an integrated part of their living (Krageloh, Chai, Shepherd, &
Billington, 2010; Maynard, Gorsuch, & Bjorck, 2001), but it is also suggested that religious beliefs
may become important during stressful events even among people who do not characterize
themselves as very religious (Pargament, 1997; Vail et al., 2010). Denmark is characterized as a
secular society (Zuckerman, 2008), however 80% are members of the National Church, 72%
characterize themselves as believers, and only 7% characterize themselves as atheists (Danish
Value Survey, 2008). Although the majority of Danes cannot be characterized as traditionally
religious going to church regularly (only 10 % attend church once a month or more) they may not
be totally removed from religious expressions. Furthermore, studies suggest that the elderly
generations in Denmark are more religiously oriented than the younger generations (Andersen,
Ausker & la Cour, 2011), and given that the target group of the study was primarily middleaged-
and elderly patients, we expected them to be more religiously than the normal population. Thus, it
was decided to apply the Brief RCOPE in a Danish context with minor changes guided by the
example of a German and Swedish study that had applied the RCOPE among cancer patients
(Ahmadi, 2006; Zwingmann, Wirtz, Müller, Körber, & Murken, 2006).

6
Measures
Religious coping, Brief RCOPE. The Brief RCOPE is a shortened version of the Religious Coping
Scale (RCOPE) developed by Pargament, Koenig, and Perez (2000), which covers five core
functions of religion in coping: meaning (positive and negative religious reappraisal), control
(active and passive ways of gaining mastery), comfort (spiritual connection, support, spiritual
discontent), intimacy (seeking religious support from others, interpersonal spiritual discontent), and
life transformation (religious direction, conversion). These core functions has served as the
theoretical underpinning of the measure, and 21 different coping strategies has been developed
resulting in a 105 item questionnaire in the original RCOPE. The Brief RCOPE consists of two
subscales with 7 items each measuring positive religious coping (seeking spiritual support and
control) and negative religious coping (religious struggle such as anger at God or feelings of
abandonment). The response format is 0 = “Not at all” to 3 “A great deal”. The questionnaire was
translated into Danish by 3 independent researchers, and discussed until agreement was obtained.
The item about demonic reappraisal was modified into the formulation “a negative power (like the
Devil)”, and 2 items more were developed, one about spiritual support (“God granted me the
strength to handle my illness/situation”), and one about positive religious meaning-making
(“Thought God had a meaning with my illness/situation after all”) as the original Brief RCOPE only
taps into negative religious meaning-making (like interpreting a negative event as Gods
punishment).
Spiritual coping, Brief SCOPE
Sociological studies suggests that only 24.9% of Danes believes in a personal God whereas 38.1%
believes in “a spirit or life force” (Inglehardt et al., 2004), and in order to accommodate participants
who did not believe in God, we developed a scale called Brief SCOPE in which the concept “God”
7
was replaced with “Spiritual power” or “my spiritual faith/conviction”. In the introduction we asked
participants to answer the scale which used the concept they preferred (either RCOPE or SCOPE).
Furthermore, according to the study by Ahmadi (2006), Swedish cancer patients have more
individualized and spiritually oriented ways of coping with illness than Americans, like feeling an
inner spiritual strength and seeking meaning related to the spiritual. Therefore we added two new
strategies of “finding inner spiritual power and strength to help me cope with my illness/situation”
and “finding spiritual meaning with my illness/situation” (see table 1).
The study among lung cancer patients and COPD patients was launched in Fall 2008 and a
study among an age- and gender matched control group of healthy Danes was planned to be
launched when recruitment of the patient group was completed. Unfortunately, recruitment on the
first study went slowly and the response rate was relatively low (23.1%). Some of the returned
questionnaires had a relatively high percentage of missing responses – especially the religious
items. This finding could not solely be explained by the severe diagnosis of our target group. To
investigate this further, the first author conducted a qualitative study among lung cancer patients
and healthy control participants. The purpose of this study was to test the face validity of the
religious and spiritual coping measure among Danish lung cancer patients and healthy Danes.
Method
Participants and procedures
Focus groups
Three focus groups of healthy middle-aged and elderly Danes were established during
October and November 2009. Focus groups were chosen to get a variety of responses and highlight
potential disagreements on the content (Greenbaum, 2000; Halkier, 2006). We aimed at recruiting a
range of people representing different religious and spiritual views, and participants in the first
8
focus group were recruited by a snowball-sampling (Johnson, 1990), and consisted of 3 women and
4 men. They represented mainly non-believers and secular Christians (people who have been
baptized and belong to the state church, but to whom the Christian belief is more about cultural
tradition and not religious belief) and one Christian believer. In order to include people with
religious or spiritual back ground, a second group was recruited from a religious organization called
the Church Association for the Inner Mission in Denmark (Dansk Indre Mission), and consisted of
two women and one man, whom all identified themselves as believing Christians and associated
with the evangelical Lutheran church of Denmark, the state church. A third group was recruited
from a spiritualistic church in Aarhus, and consisted of 2 women and 2 men. They all identified
themselves as spiritualists believing in a spiritual entity or power. Participants were between 40 and
75 years old (mean age: 56.2). The questionnaires were sent to the participants to be completed a
couple of days before the interview, and informed consent was obtained from the participants.
Participants were asked to think of a negative event when answering the questionnaires regarding
religious and spiritual coping. Two of the focus group interviews took place at the Department of
Psychology in Aarhus, and one interview took place in the church facilities of the spiritual group.
The interviews lasted 2 hours, and participants were asked to discuss their understandings of the
terms “God” and “spiritual power”, and interviewed about the relevance and understandings of the
single items in the questionnaires. Interviews were conducted by the first author.
Single interviews
In order to get in-depth information on the content of the questionnaires semi-structured
interviews were conducted (Silverman, 2010) with lung cancer patients recruited from the
respiratory clinic at Aarhus University Hospital in the period of December 2009 to March 2010.
The lung cancer patients were informed about the study by the medical staff and interested patients
were contacted by telephone by the researcher for more information about the project before giving

9
their informed consent to participate. Approximately 100 patients were informed by the staff about
the project, and 13 patients accepted to be contacted by the researcher and agreed to participate. The
questionnaire was send by mail to the 13 participants to be completed a couple of days before the
interview, and 3 participants chose to withdraw when they received the questionnaire. One of these
patients explained that he thought the questions were too intimidating. 10 interviews were
conducted and informed consent was obtained before the interviews took place. Participants were 5
women and 5 men between 43 and 81 years (mean 64.7). The interviews were all but one conducted
in the home of the patient, and one interview took place at a hospital. The interviews lasted between
20 and 75 minutes (mean: 43 minutes). Participants were asked to explain what they understood by
the terms “God” and “spiritual power”, what relevance the questionnaires had to them, and how (if
relevant) their religious or spiritual views impacted their ways of adjusting to their illness. To
reduce the potential burden of participating in an interview, 5 patients were asked specifically about
their understandings of half of the items in the questionnaires, and the other 5 patients were asked
about the other items. All interviews are conducted by the first author
Analysis
Interviews were transcribed verbatim, and analyzed using an interactive model in which
data collection, reduction, display, and conclusion-drawing constitutes a iterate process (Miles &
Huberman 1994). First each interview was analyzed to get an in-depth understanding of how the
participant(s) related to the questionnaire as a whole and to the single items. In this process, two
researchers analyzed and discussed the content of each interview using a deductive thematic
analysis (Boyatzis, 1998; Braun & Clarke, 2006; Hayes, 1997) in which the core functions of
religious coping (seeking meaning, control, spiritual support, relational support and transformation)
served as the theoretical frame. Participants’ statements about the single items were condensed and
displayed into a table with five themes covering the five functions of religious coping. The

10
participants were divided into three groups based on their perceptions and beliefs (or non-beliefs) in
God or a higher being, and statements about the single items were further reduced and ordered in
accordance with the three groups. These units of analyses were presented elsewhere (Pedersen,
Pedersen, Sinclair, & Zachariae, 2010). However, the deductive strategy was insufficient to cover
important new themes on the validity of the religious and spiritual coping measures as well as new
coping strategies that emerged from the data material. Therefore, an explorative, inductive thematic
analysis (Frith & Gleeson, 2004) was conducted by the first author and verified by an independent
researcher to investigate new themes emerging from the data material. This is the central unit of
analysis presented in this present article. Three core themes on the validity of measures on
religiosity and spirituality emerged and shed light on the response patterns found among patients,
healthy controls, and the three different belief groups respectively, which will be presented in the
remainder of the paper.
Results
Participants were divided into three groups depending on their beliefs and view of life. Participants
who held a belief in a personal God, characterized as either a father-figure or personalized entity
who intervenes in peoples’ lives were categorized as theists. Participants, who did not believe in a
personalized God but still held a belief in a spiritual being described as positive energy or
“something more“ were characterized as non-theists. Finally, people who did neither believe in God
or a spiritual being were characterized as non-believers. The term “atheist” is not used, as some of
the non-believers although not claiming to believe in anything transcendent, still valued the
Christian culture and characterized themselves as Christians. Furthermore, some of the non-
believers were reluctant to reject the idea of something transcendent permanently.
11
A private matter, or lack of common language?
Religion is said to be a private matter to Danes, and some claim that it may even be a greater taboo
than sex. This was already presented by Gordon Allport in 1950. There may be some truth in this
statement, but the first theme emerging from the data suggested that it might also be associated with
lack of common concepts and language about religious and spiritual issues, which increases the
demands to constructing appropriate instructions and response formats in measures. Across the
three groups of theist, non-theist and non-believers there were great differences in the level of
reflections on religious and spiritual matters and ability to verbalize thoughts on these matters. A
male participant belonging to the non-believer group said:
”Well, I don’t know, it’s like… it’s… I don’t think… it is something, but still nothing and…it is airy,
right? And… there is too much air… I can’t really explain, I lack the words to explain. But it is air
– it is nothing… Try to fill it out as best as one can…”
Concepts like “God” and “spiritual power” were difficult to explain and especially distinguish to
some of the participants, to whom belief in something transcendent was mostly described as a
childhood belief in “something more” or “something above us”. When asked about their
understandings of the items in Brief RCOPE and Brief SCOPE and why they responded as they did,
they were unable to elaborate further. An 81-year old male patient from the theist group said:
“You need to be theologian to answer this questionnaire…when you never have reflected on this
your whole life it is very difficult to answer”.
Others had very reflected and articulated beliefs or non-beliefs, but especially non-theists did not
accept the formulations offered to them in the questionnaires. A woman from the non-theist group
said:
12
“…that thing about [believing in] a personal God. Already at that point I get offended, a personal
God, what is that? Maybe I am totally behind, but I actually went to the library and made them
search for “a personal god”. It is not an expression that we used in my home”
She and others from the non-theist group felt offended by the items in Brief RCOPE
mentioning sin, devil and God’s punishment, because they perceived the items to reflect old-
fashioned and conservative Christian ideas, and responding to the items would be the same as
confessing this type of Christian belief. It was even suggested by some of non-theists that the
research team had a hidden agenda of missionizing by handing out questionnaires that were very
explicit about religious matters. A female patient belonging to the non-theist group said:
“It is like you have already decided that people should be (Christian) believers…because
God is mentioned in almost every item”
The problem of the response format; that participants felt like agreeing on the content
when they did not want to, was also found among non-believers, who emphasized, that if they
marked items like “Questioned the power of God” and “Questioned God’s love for me” with “Not
at all”, it could be interpreted as an implicit declaration of a belief in God. The response format
“Not relevant” was called for, and in its absence some chose to mark the highest score “Very
much”; not as a sign of religious or spiritual struggle, which was the original intent of these items,
but as a way of declaring their non-belief. The opposite was found among theists; that even though
the particular coping strategies were not prevalent in the particular situation, they felt like
dismissing their beliefs if they responded items like “Sought Gods love and care” with “Not at all”.
A healthy male from the theist group stated that:
13
“…my experience of God is what no eye has seen, and no ear has heard… But still it is a reality
that goes beyond everything. And then you make a questionnaire in our three-dimensional
world…you can’t do that”.
To this participant, the questionnaires were too limited and not fully capable of grasping the
experience of religious belief. Even though this particular participant had a more refined and
articulated belief system than some of the other participants and may have been better capable of
answering the questions adequately, he ultimately objected to the idea of measuring religious
experience by paper and pencil, and called for in-depth methods to maintain the complexity of the
religious experience. Furthermore, it was found that having an alternative to RCOPE was very
important to some of the non-theists, because they could better associate with the term “spiritual
power” than “God”. However, several of the items did not apply to their conceptions of a spiritual
power, especially the negative subscale, as a spiritual power was associated with something purely
positive, not possessing the capacity to intervene in peoples’ lives directly by punishments.
Increased relevance of religion and spirituality during critical life situations?
The second theme emerging was the importance of the life situation in which one is situated when
asked to respond to a questionnaire on religious and spiritual coping. According to the theory of
religious coping, life threatening situations like severe illness or bereavement may more likely
trigger religious or spiritual responses in coping, and this was found to be an underlying assumption
across the healthy participants as well as the patients. Theists, to whom religious belief was an
integrated part of their life, were able to elaborate in great detail what they understood by the
questions, but especially healthy participants holding beliefs in a personal God reported difficulties
responding to the questionnaires. Even though they were asked to think of a negative life event
within the last 12 months, this appeared difficult and it was outlined that the questionnaire was
14
more relevant in critical situations like severe illness, accident or loss. A healthy female participant
characterized as theist stated:
“It seems a little rigid. It does not apply in every situation”
Especially the item of feeling anger at God or a spiritual power made some of the healthy
participants conclude that the questionnaires was aimed at people experiencing life threatening
events. Despite non-believers’ rejection of the existence of something transcendent, it was found
that particular situations which the participants referred to in the interview were linked to thoughts
on religious issues. A male participant, who did not perceive himself as a believer told about his
friend, who were very close to retiring and looked forward to enjoying a more quiet life with his
wife and family. A couple of months before his retirement, this man was run over by a truck and
killed on the same road that he had been bicycling to work every day for 30 years. The interviewee
said:
”When I saw that, I doubted (God’s powers)… He (God) could have spared him. He could have
given him a little more time”
Paradoxically, even though this interviewee did not believe in God, God as a concept was still
present in the interpretation of this particular situation. The importance of the particular context in
which one is situated was confirmed by the finding that patients who did not view themselves as
very religiously minded, were more open to discuss and reflect on the importance of religion and
spirituality in relation to their illness, than healthy non-believing participants. To cancer patients,
the situation of being severely ill was a present reality and thereby patients may have been more
open to discuss the relevance of religious or spiritual coping. A male patient belonging to the non-
believer group reported that the interview had been thought provoking in a positive sense, because
he usually did not think much about religious or spiritual issues. He said:
15
“Well, it has been fine (the questionnaire) because it gives food for thought, you know, and makes
me think about things differently than I used to.”
Furthermore, it was also found that some patients having more or less articulated beliefs in God
thought that the items applied to them – both positive and negative questions depending on their
interpretations of having cancer. A woman who did not characterize herself as awfully religious, but
still holding on to her childhood beliefs had several thoughts about why God was punishing her. To
her lung cancer was interpreted as an unfair punishment stealing a lot of her time and resources. She
perceived herself to be a good person involved in aid work knitting for the Red Cross, and therefore
it was incomprehensible to her why God was punishing her. She said:
“I don’t think He has the right to punish me like that and give me a serious illness to fight with,
when I am so involved in helping others”
To her even positive religious coping items like “Looked for a stronger connection with God” were
interpreted negatively, because she thought God should have supported her more. A male patient
who was a former alcoholic and now a strong believer stated that his belief was an integrated part of
his life and that it had rescued him from dying of his alcohol abuse. Now he experienced that God
or a higher being helped him to get through his illness and through other people guided him to take
decisions regarding his illness. He said:
“…I also got help making the decision to receive chemo, because when I received the diagnosis I
thought I was already dead. Then someone told me that chemo treatment had already been booked
for me and I just needed to say “yes” or “no”. But I just got even more confused and shattered and
I could not make that decision. Then I said “God help me, I can’t get any further here”…over 2
days everything changed because I sought help from people who knew something about it (chemo),

16
and then I accepted my situation and decided to receive chemo… my thoughts about death turned
into thoughts about life”.
A universal or context-specific phenomenon?
The third theme incorporated the other two themes of language and context and concerns the
question of how well universal instruments like questionnaires are at capturing the particular
experience of the individual. The questionnaires did tap into some features of religious and spiritual
coping with varying precision depending on the context, vocabulary at hand, and history of the
individual. However, new religious and spiritual coping strategies that were not covered in the
questionnaires emerged during the interviews. A cancer patient, who had been spiritually seeking
throughout her life, but now characterized herself as too rational to believe in God, said that there
were no items covering her way of believing. She was convinced that there is “something more”
than meets the eye, but expressed a strong belief in herself and her capability to cope and said:
“I am my own God Almighty”
She and others called for items covering the phenomenon of personal or spiritual growth when
faced with life threatening situations. Others referred to the idea of fate or a pre-destined course of
life that gave a sense of meaning, and some called for items covering the importance of social
support in difficult situations, which to some extend was understood as a spiritual connection
between humans – also to deceased family members. A female patient characterized as non-theist
explained that she often talked to her deceased brother about her worries when looking at a picture
of him. She said:
“I really feel that he sits next to me and that it, well, helps…that it gives you a little extra energy”
17
Despite declared non-belief, some of the non-believing participants held beliefs about the
afterlife and hopes of being reunited with deceased relatives. A female patient characterizing herself
as a non-believer said:
“…at one point I have this naïve faith that when I die, then my grandmother, whom I cared
much about, and my father are waiting for me. I don’t know where this belief derived from, and it is
not something that has developed further, but they just stand somewhere telling me to go that way
and it’s a kind of comfort”
Others underscored the importance of the Evangelical Lutheran Church (Den Danske Folkekirke) as
a cultural institution offering a frame of rituals in connection to life transitions. A non-believing
male patient said:
“I am not a believer, but still I think it is important that we have the church, right, because I think it
can help in the situations when one gets married, or dies and needs to be buried…I don’t know if
that can be characterized as faith, but it is there back in one’s mind, that you’ve got the church to
rely on and the fellowship there.”
Thus, fragments of what could be characterized as religious or spiritual beliefs and hopes were
present among people who did not see themselves as traditional religious, but this was not covered
fully in the questionnaires at hand. A female patient from the non-theist group said:
“You have all the different religions, right, Buddhism, Islam, Judaism, Christianity and the Greek
Orthodox … they are all available to you depending on what task you perform any given
day…today you may chose this belief, tomorrow another…it may not necessarily be a belief written
in a book”.

18
To her a few items in the questionnaires applied, however as described above, every context and
situation called for different religious or spiritual interpretations and therefore the religious ideas
and concepts presented in the Brief RCOPE and Brief SCOPE were too narrow to describe her
rather context-specific and eclectic beliefs.
Discussion
In recent years discussions on methodology and validity have increased in the psychology of
religion recognizing the limitations of the dominating positivistic approach to studying complex
phenomena like religious and spiritual experience (Belzen, 2010; Emmons & Paloutzian, 2003;
Nelson, 2012; Williamson & Ahmad, 2007). The original intent of this present study was to
evaluate the face validity of a widely used instrument covering religious coping, Brief RCOPE, and
a newly developed scale measuring spiritual coping, Brief SCOPE, among Danes. However, an
explorative thematic analysis revealed three themes related to validity that is important to consider
when investigating religious and spiritual phenomena. It is suggested that cross-cultural validity is
not only a matter of taking cross-national differences into account, but just as well as being aware of
context specific differences within a given culture between people holding different views of life
regarding religious and spiritual issues, and the importance of the situation in which the individual
is stated. At first glance, the impression of the participants’ response patterns suggested that theists
having articulated beliefs in God responded adequately to the Brief RCOPE and had higher scores
on this measure than did non-theists and non-believers. As such, the findings seemed to be
supporting the hypothesis suggested by Pargament (1997; 2007), that the more integrated a
religious belief system is, the more likely it is involved in coping strategies. However, the
explorative thematic analysis revealed that the finding could just as well exemplify the importance
of holding the appropriate “religious capital” (Bourdieu, 1986) or language to be able to understand
and respond to a given question adequately, but not necessarily reflect validity of the questionnaire
19
or religious coping in the particular situation. The average Cultural Christian Dane may not possess
the conceptual codes that are needed to answer instruments like Brief RCOPE in an adequate and
valid way because it is characterized by theistic belief which to a high degree is decreasing due to
secularization Danes (Lüchau 2005). However, since 72% of Danes consider themselves to be
believers (The Danish Value Survey, 2008) religious or spiritual beliefs may not be disappearing.
Instead, the concept of “religion” is changing and may be characterized as “unpacked” – meaning
that religion can no longer be described as system of ideas, institutions and practices that shares the
same core, a so called “packed religion”, but instead as several distinct aspects not sharing a
common core (Rosen, 2009). One of these aspects is personal beliefs which are defined as:
“…beliefs emerge as highly personal emotions and reflections that reside in the inner life of each
individual and are developed cognitively through life experiences. Such beliefs are difficult to
express not only due to lack of language, but also for the reason that they are usually tacit, seldom
systematized and usually actualized ad-hoc in respect to context (Rosen, 2009:8)
Some have argued that the Western world is becoming religious “illiterate” (Smith & Denton,
2005), because of a general neglect of religious and spiritual issues that follows secularization
(Pargament, Mahoney, Exline, Jones & Shafranske, 2013). Whether or not one calls it religious
illiteracy or tacit knowledge as in the above mentioned definition, results from this present study
suggests that it may be problematic to individuals living in secularized societies to decode a
questionnaire like Brief RCOPE because their beliefs are not made very explicit and cannot be
assumed to represent a coherent worldview. Especially patients, who held on to a childhood belief
or the sense of “something more”, had great difficulties expressing what this meant to them.
The theme on the importance of the context one is situated in is crucial to consider when
asking participants to respond to questions about religious and spiritual coping. In accordance with
the theory of religion as unpacked in Denmark (Rosen, 2009) it was found that personal beliefs
20
were actualized ad hoc in very specific contexts of for example negative life events that called for
explanations, comfort or hope – also among participants who did not view themselves as believers.
Furthermore, part of the critiques of the questionnaire may stem from methodological difficulties of
relating to a traumatic event on command and to report religious coping strategies retrospectively as
the healthy participants were asked to do (Fowler 1995).
The third theme encompassing the other two underscored the challenge of developing a
methodology that is sensitive to the individual’s religious, spiritual or secular existential view of life
and the context one is situated in, and at the same time being able to identify general patterns of
religious and spiritual ways of coping with crisis. This may be an even harder task as individualism
and secularism erodes the common cultural heritage that used to be adopted more or less
automatically through traditions and narratives rooted in philosophy and religion which shaped
identity and social life (Gergen, 1991). In a postmodern world, everything is individually
constructed and the individual may be more critical towards attempts of defining and measuring
human experience because he demands full autonomy to define his own unique experience (Iversen,
2006). This was reflected in the participants’ reluctance towards being categorized within a certain
religious category without further discussion and several participants argued that their views of the
Sacred or “something more” was not presented in the questionnaires at hand. From a social
constructionist perspective it is argued that the attempt of measuring a given phenomenon is a lost
cause, because we will never be able to determine whether we are talking about the same constructs.
However, trying to avoid the two extremes of positivism and constructionism, researchers still aim
at developing methodologies to observe and register human experience which are designed to make
participants able to express their experiences in such a way, that it may be generalized, because it is
assumed that there are phenomena in the real world that have common features and which can be
compared across individuals, contexts and cultures. In the psychology of religion it is even more

21
important to be sensitive to the phenomenon at hand because the structure and functions of beliefs
are closely tied to the contents of beliefs, which is highly influenced by the given culture and the
experiences of the individual, and measures should be developed with sensitivity to time, context,
and language of the individual. Thus, we do not argue for or against one methodology or another,
but recognize quantitative and qualitative methods as complementary. The most important point is
to acknowledge that what can be said about a specific phenomenon may be limited, and that a
specific operationalization of a given phenomena is just one aspect of the complexity of the real
world, that may be inflicted by the researchers pre-assumptions and biases.
Limitations and future directions
Some limitations should be highlighted in this present study. Given the methodology of qualitative
interviews and relatively few participants, cautions should be made in generalizing the results to
other contexts. In general, the focus group participants were more critical toward the questionnaires
than the patients, and besides the points about the importance of context (being severely ill or
healthy), this finding may be related to methodological differences too. Focus groups may be
subject to polarizing effects, with individuals taking more extreme positions than they would in
private, and this might especially have been the case in the focus group of the mixed group of non-
believers and Cultural Christians. The opposite might have been the case in the religious and
spiritual groups which may have been subject to the creation of consensus opinion (Morgan, 1997).
However, this present study suggests that studying religious and spiritual phenomena
in general, and in cross-cultural studies in particular, requires thoughtful reflections on the
importance of contexts and language when constructing or translating measures keeping in mind the
limitations of different methodologies. By using standardized questionnaires the ability to compare
across cultures is maintained, but will be limited by the instrument’s conceptual frame, and opt to
22
ignoring important information about other forms or functions of religious and spiritual coping
strategies as was the case in this present study. Qualitative methods are called for to avoid naïve
realism and postmodern anti-realism, and help remain within the framework of critical realism
(McGrath 2004:195). Qualitative, inductive methods may be a starting point for developing
concepts of religious, spiritual, and existential coping that are sensitive to a particular culture.
Despite the limited cross-cultural generalizability of qualitative studies, they may give a richer
understanding of a particular culture’s concepts and metaphors that are present when humans try to
come to terms with some of life’s most critical and vulnerable situations. Regarding the measure
Brief RCOPE, future studies are recommended to apply new, culture-sensitive measures of
religious, spiritual, and secular existential meaning-making processes if the psychology of religion
is to grasp the complexity of how different worldviews may function or dysfunction during times of
distress among people living in highly secular societies (DeMarinis, 2008).
Acknowledgements
We wish to thank Robert Zachariae, Unit for Psychooncology and Health Psychology, Aarhus
University Hospital and Aarhus University for critical comments. Furthermore we wish to thank
Charlotte Jonassen, Department of Psychology, Aarhus University, for fruitful discussions on
methodology and the topic at hand
23
References
Ahmadi, F. (2006). Culture, religion and spirituality in coping. Dissertation. University of Uppsala.
Allport, G. (1950). The individual and his religion: a psychological interpretation. New York:
Macmillan
Andersen, P.B., Ausker, N.H., & la Cour. (2011). P. Går fanden i kloster, når han bliver
gammel? In P. Gundelach (Ed.), Små og store forandringer. Danskernes værdier siden
1981 (pp. 97–113). København, Danmark: Hans Reitzels Forlag.
Belzen, J.A. (2010). Towards cultural psychology of religion: principles, approaches and
applications. New York, NY, US: Springer Science + Business Media
Bourdieu, P. (1986). The forms of capital. In J. Richardson (Ed.) Handbook of Theory and Research
for the Sociology of Education (New York, Greenwood): 241-258.
Boyatzis, R.E. (1998). Transforming qualitative information: thematic analysis and code
development. Sage
Braun, V. & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in
Psychology, 3: 77-101
Coon, D.J. (1992). Testing the limits of sense and science: American experimental psychologists
combat spiritualism 1880 - 1920. American Psychology, 47:143-151
DeMarinis, V. (2008). The Impact of Postmodernization on Existential Health in Sweden:
Psychology of Religion’s Function in Existential Public Health Analysis. Archieve for the
Psychology of Religion, 30: 57-74
Emmons, R.A. & Paloutzian, R. (2003). The Psychology of Religion. Annual Review of
Psychology; 54:377-402
Fowler, F.J. (1995). Improving Survey Questions: Design and Evaluation. Thousand Oaks, CA, US:
Sage Publications, Inc.
24
Frith, H. & Gleeson, K. (2004). Clothing and embodiment: men managing body image and
appearance. Psychology of Men and Masculinity, 5: 40-48
Gall, T.L. & Guirguis-Younger, M. (2013). Religious and spiritual coping: Current theory and
research. In: K.I. Pargament (Ed): APA Handbook of Psychology, Religion, and
Spirituality, vol. 1. APA, Washington D.C., 349-364. doi: 10.1037/14045-000
Gergen, K.J. (1991). The saturated self: Dilemmas of identity in contemporary life. New York:
Basic Books
Gorsuch, R.L. (1984). Measurement: The boon and the bane of investigating religion. American
Psychologist, 39: 228-236
Greenbaum, T. (2000). Moderating focus groups: A practical guide for group facilitation.
Thousand Oaks, CA: Sage
Halkier, B. (2006). Fokusgrupper. Roskilde Universitetsforlag
Hayes, N. (1997). Theory-led thematic analysis: social identification in small companies. In Hayes,
N. (ed): Doing qualitative analysis in psychology. Psychology Press
Hill, P.C. & Edwards, E. (2013). Measurement in the psychology of religiousness and spirituality:
Existing measures and new frontiers. In: Kenneth I. Pargament: APA Handbook of
psychology, religion and spirituality. Vol. 1.. American Psychological Association
Hood, R.W. (1999). American Psychology of Religion and the Journal of the Scientific Study on
Religion. Journal for the Scientific Study on Religion, 39 (4): 531-543
Hood, R. (2010). “Towards cultural psychology of religion: principles, approaches, and
applications”: an appreciative response to Belzen's invitation. Mental Health, Religion &
Culture, 13(4), 397-406.

25
Iversen, H.R. (2006). Secular Religion and Religious Secularism: A profile of the religious
development in Denmark since 1968. Nordic Journal of Religion and Society, 19 (2), pp.
75-92
Johnson, J. (1990). Selecting Ethnographic Informants. Sage, London
Krageloh, C. U., Chai, P. P., Shepherd, D., & Billington, R. (2010). How religious coping is used
relative to other coping strategies depends on the individual’s level of religiosity and
spirituality. Journal of Religion and Health. doi:10.1007/s10943-010-9416-x
Lüchau, P. (2005). Danskernes gudstro siden 1940’erne. In: M.T. Højsgaard & H.R. Iversen (Eds.),
Gudstro i Danmark (pp. 31-58). København: Anis.
Maynard, E. A., Gorsuch, R. L., & Bjorck, J. P. (2001). Religious coping style, concept of god, and
personal religious variables in threat, loss, and challenge situations. Journal for the
Scientific Study of Religion, 40(1), 65–74.
McGrath, A. E. (2004). The science of God: an introduction to scientific theology. London: T & T
Clark.
Miles, M.B. & Huberman, M. (1996). Qualitative data analysis. An expanded sourcebook. 2nd
edition. Sage Publications
Miller, W.R. & Thoreson, C.E. (2003). Spirituality, Religion and Health: An emerging research
field. American Psychologist, 58 (1): 24-35
Morgan, D. (1997). Focus groups as qualitative research. (2nd
. Ed.). Thousand Oaks, CA: Sage
Nelson, J.M. (2012). A history of psychology of religion in the West: Implications for theory and
method. Pastoral Psychology, 61: 685-710. doi: 10.1007/s11089-011-0407-y
Paloutzian, R. (1996). Invitation to the Psychology of Religion. Needham Heights, MA: Allyn &
Bacon, 2nd
ed.
26
Pargament, K.I. (1997). The psychology of religion and coping. Theory, research, practice. New
York: Guildford.
Pargament, K.I., Smith, B.W., Koenig, H.G., & Perez, L. (1998). Patterns of positive and negative
religious coping with major life stressors. Journal of the Scientific Study of Religion, 37 (4),
710-724.
Pargament, K.I., Mahoney, A., Exline, J.J., Jones, J.W., & Shafranske, E.P. (2013). Envisioning an
integrative paradigm for the psychology of religion and spirituality. In: Pargament, K.I.
(Ed). APA Handbook of Psychology, Religion, and Spirituality, vol. 1. 3- 19
Pedersen, H.F., Pedersen, C.G., Sinclair, A., Zachariae, R. (2010). Religious coping in a secular
society: A preliminary qualitative study of the content validity of R-COPE-14.
International Journal of Behavioral Medicine, 17 (1): 22
Sherman, A.C. & Simonton, S. (2001). Assessment of Religiousness and Spirituality in Health
Research. In: T.G. Plante & A.C. Sherman (Eds.), Faith and Health. Psychological
Perspectives: 139-166. The Guildford Press
Rosen, I. (2009). I’m a believer – but I’ll damned if I’m religious: Belief and religion in the greater
Copenhagen area – a focus group study. Lund Studies in Sociology of Religion, Lund
University
Selvam, S.G. (2011). Positive psychology as a theoretical framework for studying and learning
about religion from the perspective of psychology. A paper presentation at the BSA
Sociology of Religion Study Group -Teaching and Studying Religion Symposium.
London.
Silverman, D. (2010). Doing qualitative research. Third Edition. Sage Publications
Smith, C. & Denton, M.L. (2005). Soul searching: The religious and spiritual lives of American
teenagers. New York, NY: Oxford Press.
27
Spilka, B. (1981). "Faith and behavior: Religion in introductory psychology texts of the 1950s and
1970s."Teaching of psychology (0098-6283), 8 (3), p. 158-160.
Spilka, B. & McIntosh, D.N. (1999). Bridging religion, a psychology: the Hall-James generation as
transition from the “old” to the “new” psychology. In: Psychological perspectives and the
religious quest, edited by Lallene J. Rector and Weaver Santaniello, 7-39.Lanham, Md:
University Press of America
The Danish Value Survey, 2008. Originally conducted by prof. Peter Gundelach. Data was made
available by the Danish Data Archive (archive number DDA-21432)
Thuné-Boyle, I.C., Stygall, J.A., Keshtgar, M.R., & Newman, S.P. (2006). Do religious/spiritual
coping strategies affect illness adjustment in patients with cancer? A systematic review of
the literature. Social Science and Medicine, 63: 151-164.
Vail, K.E., III, Rothschild, Z.K., Weise, D.R., Solomon, S., Pyszczynski, T., & Greenberg, J.
(2010). A terror management analysis of the psychological functions of religion.
Personality and Social Psychology Review, 14, 84–94. doi:10.1177/1088868309351165
Williamson, W.P. & Ahmad, A. (2007). Survey research and Islamic fundamentalism: A question
about validity. Journal of Muslim Mental Health, 2:155-176.
Zuckerman, P. (2008). Society without God. What the least religious nations can tell us about
contentment. New York, NY: NYU Press.
Zwingmann, C., Wirtz, M., Müller, C., Körber, J., & Murken, S. (2006). Positive and negative
religious coping in German breast cancer patients. Journal of Behavioral Medicine, 29 (6):
533-547. doi: 10.1007/s10865-006-9074-3

28
Table 1: The Brief RCOPE and Brief SCOPE
Brief RCOPE Not
at
all
A
little
bit
Quite
a bit
A
great
deal
1 Looked for a stronger connection with God 0 1 2 3
2 Sought God’s love and care 0 1 2 3
3 Felt punished by God 0 1 2 3
4 Wondered whether God had abandoned me 0 1 2 3
5 Sought help from God in letting go of my anger 0 1 2 3
6 Tried to put my plans into action together with God 0 1 2 3
7 Asked for forgiveness for my sins 0 1 2 3
8 Wondered what I did for God to punish me 0 1 2 3
9 Tried to see how God might be trying to strengthen me
in this situation
0 1 2 3
10 Questioned God’s love for me 0 1 2 3
11 Wondered whether my religious community had
abandoned me
0 1 2 3
12 Focused on religion to stop worrying about my problems 0 1 2 3
13 Decided that an evil power (like the devil) made this
happen
0 1 2 3
14 Questioned the power of God 0 1 2 3
15 God granted me the strength to handle my
illness/situation
0 1 2 3
16 Thought God had a meaning with my illness/situation
after all
0 1 2 3

29
Brief SCOPE Not
at
all
A
little
bit
Quite
a bit
A
great
deal
1 Looked for a stronger connection though my faith/
spiritual conviction
0 1 2 3
2 Sought love and care through my faith/spiritual
conviction
0 1 2 3
3 Felt spiritually punished 0 1 2 3
4 Felt spiritually abandoned 0 1 2 3
5 Sought help through my faith/spiritual conviction to let
go of my anger
0 1 2 3
6 Tried to put my plans into action together with another
spiritual power
0 1 2 3
7 Sought spiritual purification 0 1 2 3
8 Wondered what I did for a spiritual power to punish me 0 1 2 3
9 Tried to see how another spiritual power might be trying
to strengthen me in this situation
0 1 2 3
10 Questioned spiritual love for me 0 1 2 3
11 Wondered whether my fellow believers had abandoned
me
0 1 2 3
12 Focused on my spiritual conviction to stop worrying
about my problems
0 1 2 3
13 Decided that a negative power made this happen 0 1 2 3
14 Questioned the spiritual 0 1 2 3
15 I felt an inner spiritual power and strength that helped
me cope with my illness/situation
0 1 2 3
16 Found spiritual meaning with my illness/situation 0 1 2 3