pharmacotherapy teaching/learning - ugentusers.ugent.be/~lvbortel/sunday_13.pdf · pharmacotherapy...
TRANSCRIPT

Pharmacotherapy teaching/learning
Theo PGM de Vries, MD PhDClinical Pharmacology and PharmacyVU University Medical Center AmsterdamGent/EACPT 2007 Amsterdam
Introduction
- Competence
- Learning
- Assessment
Conclusion

Still incompetence in choosing and prescribing drugs….

…despite increasing CP knowledge.

• Model status
diagnosistreatment
Pharmacotherapy competence
Goalcompetence
Methodlearning
Monitorassessment

1. Patiënt’s problem
2. Therapeutic objective
3. Treatment choice
a. standard (best evidence)
b. verify suitability for patient
4. Start treatment
5. Give patiënt information
6. Monitor treatment
Pharmacotherapy competenceWHO 6-step: the student/doctor is able to:
WHO 1994; Nierenberg 1990; Walley 1997; Maxwell 2003

WHO 6-step: Cogn. Comm. Mot.
1. Patient’s problem + + +
2. Therapeutic objective + + + + + +
3. Treatment choice
a. standard (best evidence) + + +
b. verify suitability for patient + + + + +
4. Start treatment + + + + + + +
5. Give patient inform./instr. + + + + + +
6. Monitor treatment + + + + + +
Pharmacotherapy competence

- physiology, pathophysiol. etc
- internal medicine etc.
- research methodology
!
!
answers
responsibilityspecific experiences + abstract theor. concepts
meaningful sets of connections (memory networks)
easy accessible “illness scripts”
condensation
Regehr 1996; Schmidt 1990

Symptoms & signs
diagnosis
Analyticslow, conscious, systematic, evidence based, novice
Non-analyticfast, unconscious, heuristic, experience based, expert
Illness script
Regehr 1996; Schmidt 1990; Eva 2005

- physiology, pathophysiology
- pharmacology
- internal medicine etc.
- research methodology
!
!
answers
responsibilityspecific experiences + abstract theor. concepts
meaningful sets of connections (memory networks)
easy accessible “treatment scripts”??
condensation
Regehr 1996; Schmidt 1990

Diagnosis Treatment
Analyticslow, conscious, systematic, evidence based, novice
Non-analyticfast, unconscious, heuristic, experience based, expert
Treatment script
Geyteman (review; subm. 2007)

Choosing (1)
An oven cloth
Conscious/analytical?
Unconscious/non-analytical?

Choosing (2)
A room
Conscious/analytical?
Unconscious/non-analytical?

Choosing (3): study
Students: presented several related items (oven cloths/rooms)
Dijksterhuis 2005
Group 2: instructed: carefull choice (conscious/analytical)
Group 3: distracted (unconscious/non-analytical)
Group 1: immediate choice
Which group made the best choice (reference)?

Complicated problems/many factors (rooms):
- unconscious/non-analytical thinking
- very large ‘brain’ capacity (‘hard disk’)
- role experience??
Less complicated problems/few factors (oven cloths):
- conscious/analytical thinking
- limited ‘brain’ capacity (‘working memory’)
Dijksterhuis 2005
Choosing (4): theory

Diagnosis Treatment
Analyticslow, conscious, systematic, evidence based, novice
Non-analyticfast, unconscious, heuristic, experience based, expert
Treatment script
Geyteman (review; subm. 2007)

Pharmacotherapy learning & assessment
Goalcompetence
Methodlearning
Monitorassessment

- physiology, pathophysiology
- pharmacology
- internal medicine etc.
- research methodology
!
!
answers
responsibilityspecific experiences + abstract theor. concepts
meaningful sets of connections (memory networks)
easy accessible “treatment scripts”??
condensation
Regehr 1996; Schmidt 1990

Context learning & assessment
Criteria:
1. Setting of future occupation
2. Responsibility and involvement
3. Feedback and reflection
4. Repeated cycle
Coles 1998, Ashley 2000, Lewkonia 2001, Branch 2002

Degree of reality of the setting
real practice
simulated practice
demonstration in practice
description of practice



Vollebregt 2006

Setting (‘OSCE’: 3 stations; 9 students)
D1 D2 D3
P1
A1
P2
A2
P3
A3D = doctor
P = patient
A = assessor
Vollebregt 2006
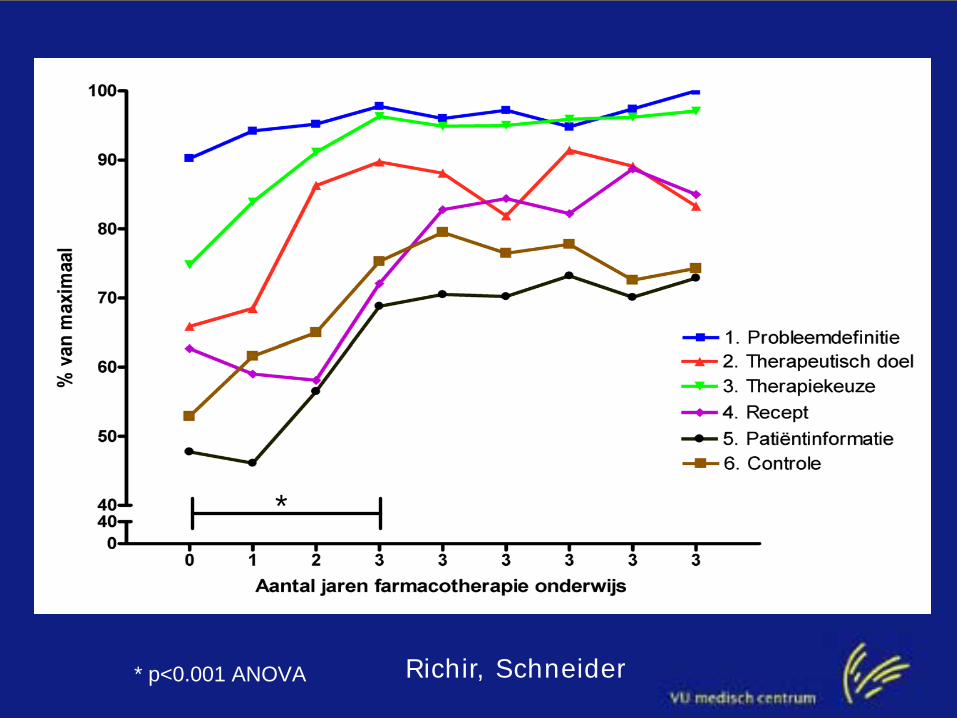
Geneesmiddelonderzoek
* p<0.001 ANOVA
*
Richir, Schneider

Miller 1990, Rethans 1991
(knows procedures)
(performance)
(competence)
Assessment:
- valid
- reliable
- predictive

Conclusion (1) Pharmacotherapy curriculum

because: Students remember:
20% of what they hear
30% of what they see
50% of what they hear and see
70% of what they teache
90% of what they experience

Tell me and I will forget,
show me, and I may not remember,
INVOLVE ME, and I will understand.
Ashley, 2000