pharmacology of anesthesia 1
TRANSCRIPT
8/8/2019 Pharmacology of Anesthesia 1
http://slidepdf.com/reader/full/pharmacology-of-anesthesia-1 1/18
8/8/2019 Pharmacology of Anesthesia 1
http://slidepdf.com/reader/full/pharmacology-of-anesthesia-1 2/18

8/8/2019 Pharmacology of Anesthesia 1
http://slidepdf.com/reader/full/pharmacology-of-anesthesia-1 3/18

8/8/2019 Pharmacology of Anesthesia 1
http://slidepdf.com/reader/full/pharmacology-of-anesthesia-1 4/18

8/8/2019 Pharmacology of Anesthesia 1
http://slidepdf.com/reader/full/pharmacology-of-anesthesia-1 5/18
There are many theories, but none of them completely explain the mode of action of all anesthetics
The most recent one is: Affection of Synaptic Transmission
Decrease Synaptic Transmission rather than AxonalImpulse conduction.

8/8/2019 Pharmacology of Anesthesia 1
http://slidepdf.com/reader/full/pharmacology-of-anesthesia-1 6/18
This occurs by;
Presynaptic Mechanisms:- A
1- Activation of presynaptic K+ channelsTransmitter same as presynaptic inhibition.
2- Volatile agents & propofol (but not thiopental) glutamate.
Postsynaptic Mechanisms:-B
G.A. Depression of postsynaptic response.
Summary:In
G.A. act mainly at synaptic transmission rather thanaxonal impulse conduction.
8/8/2019 Pharmacology of Anesthesia 1
http://slidepdf.com/reader/full/pharmacology-of-anesthesia-1 7/18
M inimum Alveolar Concentration ( M AC)
Definition:
It is the Minimum Alveolar Concentration of theanesthetic at 1 atmosphere absolute that preventsmovement of 50% of the population to a standard
stimulus (e.g. surgical incision)
Types of M. A.C:1- M.A.C as above2- M.A.C awake 3- M.A.C 95%
4- M.A.C intubation
8/8/2019 Pharmacology of Anesthesia 1
http://slidepdf.com/reader/full/pharmacology-of-anesthesia-1 8/18
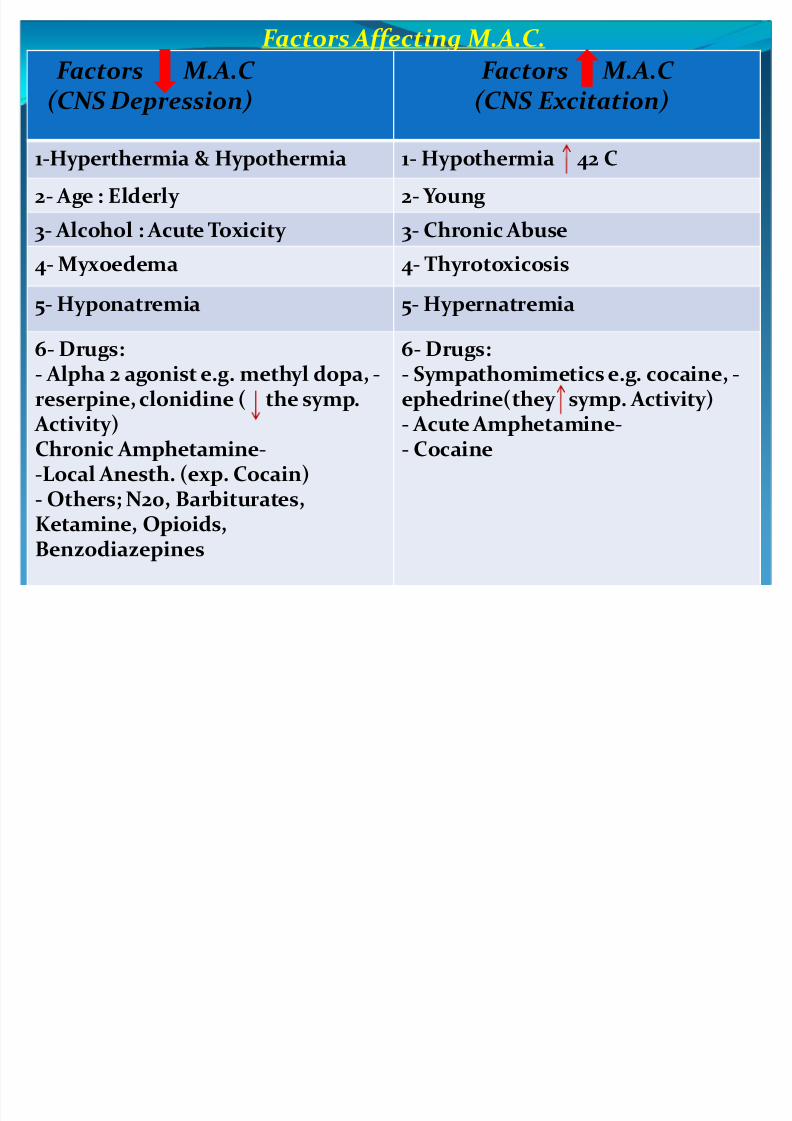
F actors Affecting M. A.C .
F actors M. A.C (CNS Excitation)
F actors M. A.C (CNS Depression)
1- Hypothermia 42 C1-Hyperthermia & Hypothermia
2- Young2- Age : Elderly
3- Chronic Abuse 3- Alcohol : Acute Toxicity
4- Thyrotoxicosis4- Myxoedema
5- Hypernatremia5- Hyponatremia
6- Drugs:-- Sympathomimetics e.g. cocaine,
ephedrine(they symp. Activity)-- Acute Amphetamine
- Cocaine
6- Drugs:-- Alpha 2 agonist e.g. methyl dopa,
reserpine, clonidine ( the symp. Activity)
-Chronic Amphetamine-Local Anesth. (exp. Cocain)- Others; N20, Barbiturates,Ketamine, Opioids,
Benzodiazepines

8/8/2019 Pharmacology of Anesthesia 1
http://slidepdf.com/reader/full/pharmacology-of-anesthesia-1 9/18
I nhalational Anesthetic includes;
1- N2O2- Halothane
3- Ether
4- Methoxyfluran
5- Enflurane
6- Isoflurane7- Desflurane
8- Sevoflurane
8/8/2019 Pharmacology of Anesthesia 1
http://slidepdf.com/reader/full/pharmacology-of-anesthesia-1 10/18
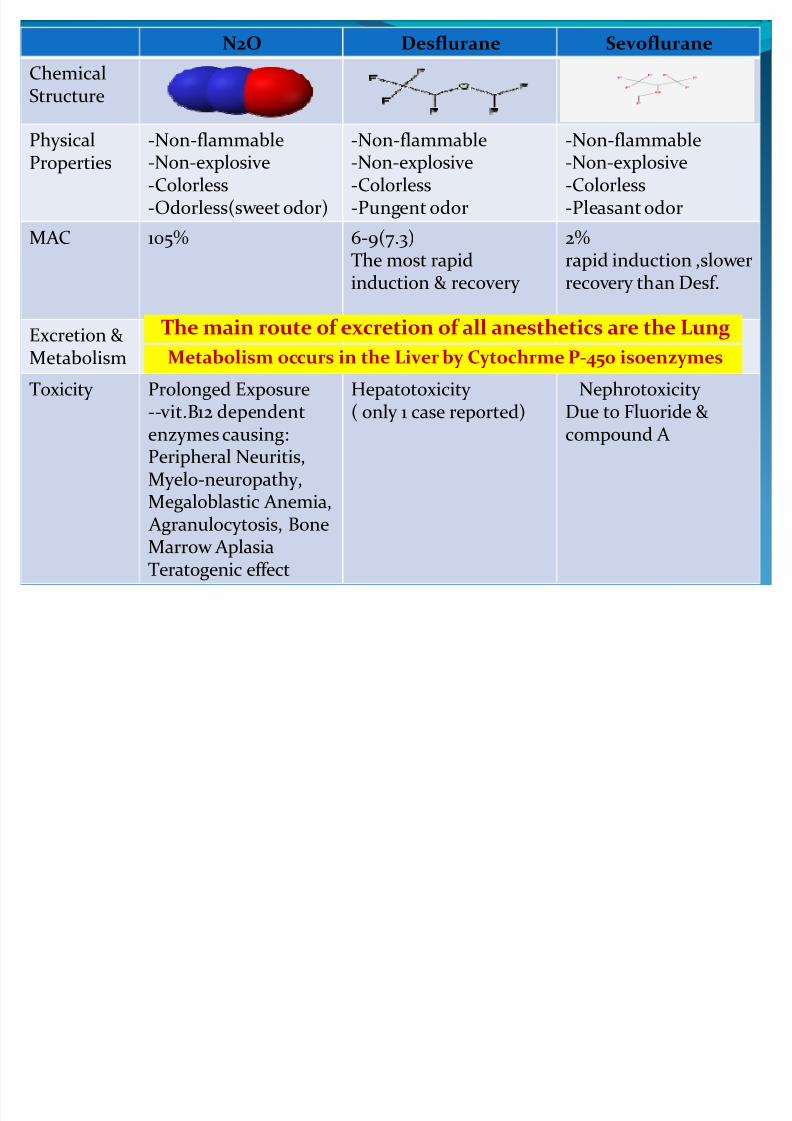
SevofluraneDesfluraneN2O
ChemicalStructure
-Non-flammable-Non-explosive-Colorless-Pleasant odor
-Non-flammable-Non-explosive-Colorless-Pungent odor
-Non-flammable-Non-explosive-Colorless-Odorless(sweet odor)
PhysicalProperties
2%rapid induction ,slower
recovery than Desf.
6-9(7.3)The most rapid
induction & recovery
105%MA C
Excretion &Metabolism
Nephrotoxicity
Due to Fluoride &compound A
Hepatotoxicity
( only 1 case reported)
Prolonged Exposure
--vit.B12 dependentenzymes causing:Peripheral Neuritis,Myelo-neuropathy,Megaloblastic Anemia, Agranulocytosis, Bone
Marrow AplasiaTeratogenic effect
Toxicity
The main route of excretion of all anesthetics are the Lung
Metabolism occurs in the Liver by Cytochrme P-450 isoenzymes
8/8/2019 Pharmacology of Anesthesia 1
http://slidepdf.com/reader/full/pharmacology-of-anesthesia-1 11/18
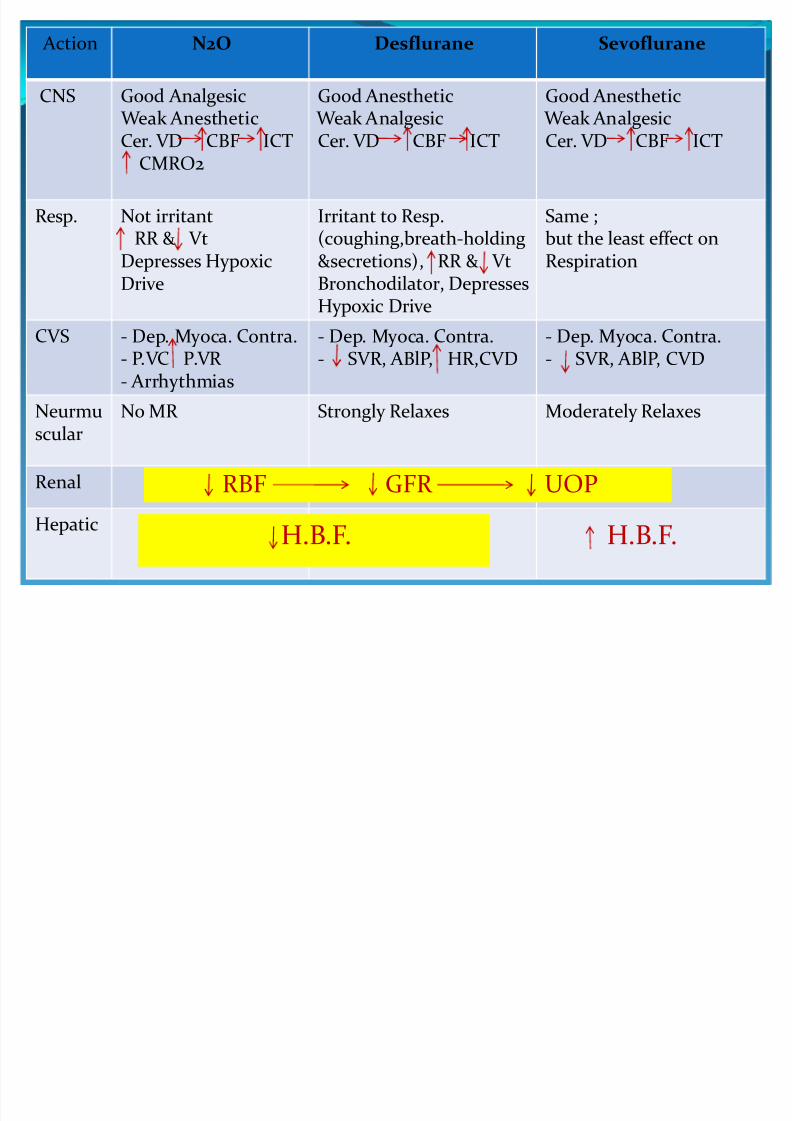
SevofluraneDesfluraneN2O Action
Good Anesthetic Weak Analgesic
Cer. VD CBF ICT
Good Anesthetic Weak Analgesic
Cer. VD CBF ICT
Good Analgesic Weak Anesthetic
Cer. VD CBF ICTCMRO2
CNS
Same ;but the least effect onRespiration
Irritant to Resp.(coughing,breath-holding&secretions), RR & Vt
Bronchodilator, DepressesHypoxic Drive
Not irritantRR & Vt
Depresses Hypoxic
Drive
Resp.
- Dep. Myoca. Contra.- SVR, ABlP, C VD
- Dep. Myoca. Contra.- SVR, ABlP, HR,C VD
- Dep. Myoca. Contra.- P.V C P.VR - Arrhythmias
C VS
Moderately RelaxesStrongly RelaxesNo MR Neurmuscular
Renal
Hepatic
RBF GFR UOP
H.B.F. H.B.F.
8/8/2019 Pharmacology of Anesthesia 1
http://slidepdf.com/reader/full/pharmacology-of-anesthesia-1 12/18
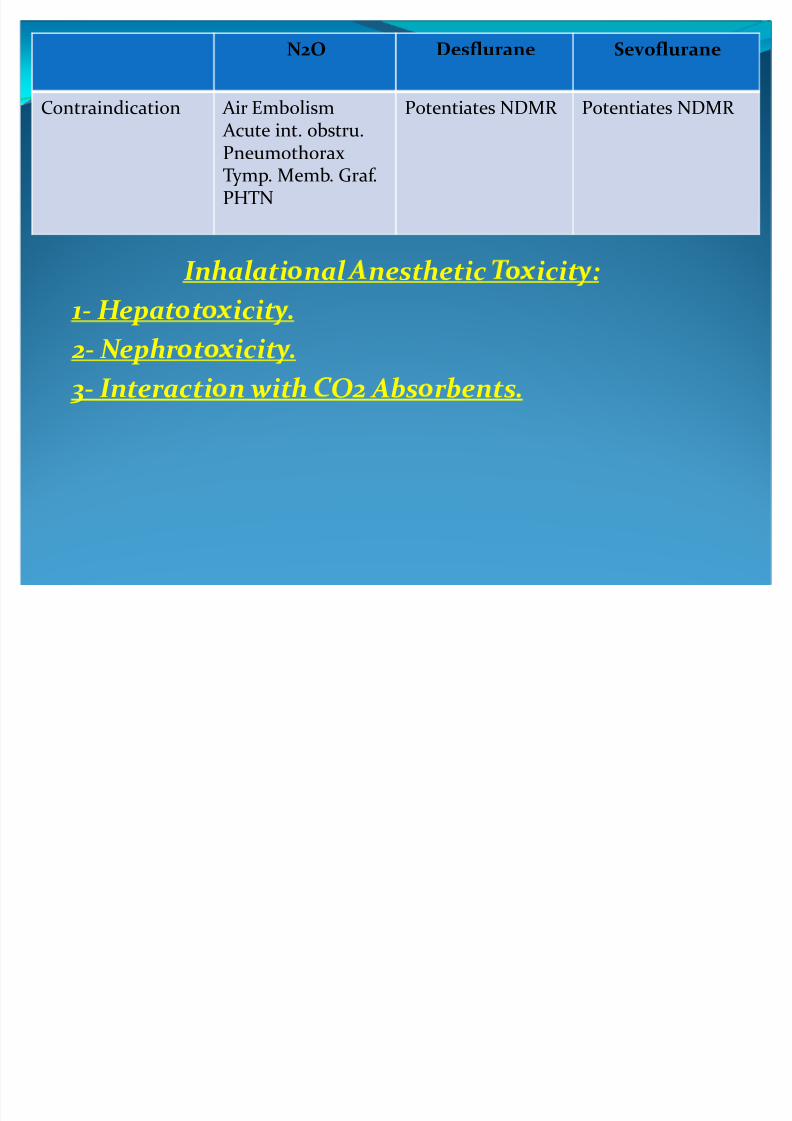
SevofluraneDesfluraneN2O
Potentiates NDMR Potentiates NDMR Air Embolism
Acute int. obstru.PneumothoraxTymp. Memb. Graf.PHTN
Contraindication
Inhal ati nal nesthetic icit :H epat t icit .- 1
. N ephr t icit- 2
Abs r bents. 2 Inter acti n with O- 3
8/8/2019 Pharmacology of Anesthesia 1
http://slidepdf.com/reader/full/pharmacology-of-anesthesia-1 13/18
P harmacokinetic of I .V. Anesthetics :
- A bsorption
- Distribution
- Metabolism (Biotransformation)
- Excretion
8/8/2019 Pharmacology of Anesthesia 1
http://slidepdf.com/reader/full/pharmacology-of-anesthesia-1 14/18
I .V. Anesthetics include :1- Thiopentone Sodium
2- Methohexitone Sodium
3- Propofol
4- Etomidate
5- KetamineOther i.v. agents used in anesthesia:
- Benzodiazepines
- Opioids- Neuroleptic Agents
8/8/2019 Pharmacology of Anesthesia 1
http://slidepdf.com/reader/full/pharmacology-of-anesthesia-1 15/18
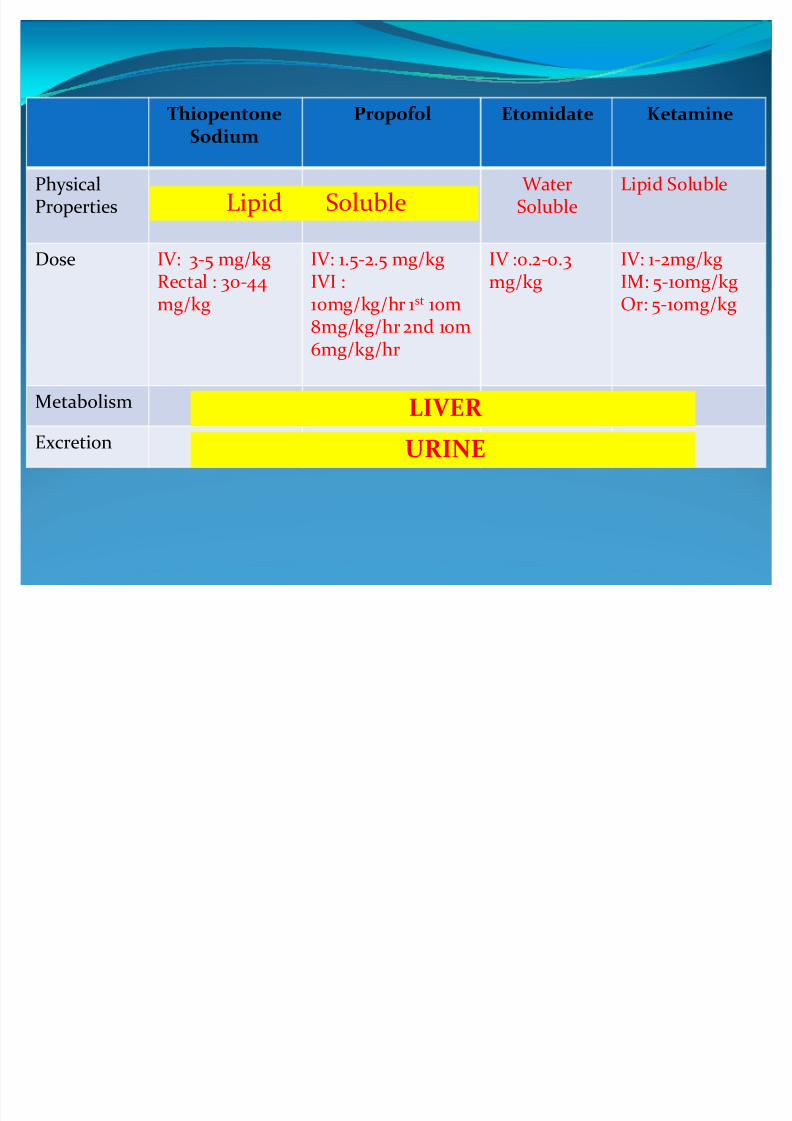
KetamineEtomidatePropofolThiopentone
Sodium
Lipid Soluble WaterSoluble
PhysicalProperties
IV: 1-2mg/kg
IM: 5-10mg/kgOr: 5-10mg/kg
IV :0.2-0.3
mg/kg
IV: 1.5-2.5 mg/kg
IVI :10mg/kg/hr 1st 10m8mg/kg/hr 2nd 10m6mg/kg/hr
IV: 3-5 mg/kg
Rectal : 30-44mg/kg
Dose
Metabolism
Excretion
Lipid Soluble
LIVER URINE

8/8/2019 Pharmacology of Anesthesia 1
http://slidepdf.com/reader/full/pharmacology-of-anesthesia-1 16/18
KetaminePropofolThiopentone SodiumPh.Action
Mech. of Action:Dissociativ Aneth.(dissociates thalamus
from cortex.Blocks NMDA Rs.- Clinically..- CNS (+)-EEG changes.- CMR
- PONV - ++ Excitatory Ph.
Mech. of Action: As Thiopentone ; but- Not Anticonvulsant
- Excitatory Ph.
Mech. of Action:Depresses RF in B.stemby GABA
unconscious.- CNS depresses- Anticonvulsant- CMR - No PONV - No Excitatory Ph.
CNS
1- Resp.(--)1- Resp.(--)1- Resp.(--)2- Bronchospasm3- Laryngeal spasm
Resp.
1- ABP2- HR 3- CO +ve inotropic
1- ABP2- HR 3- CO maintained
1- ABP2- HR 3- CO maintained
C VS
N-M
8/8/2019 Pharmacology of Anesthesia 1
http://slidepdf.com/reader/full/pharmacology-of-anesthesia-1 17/18
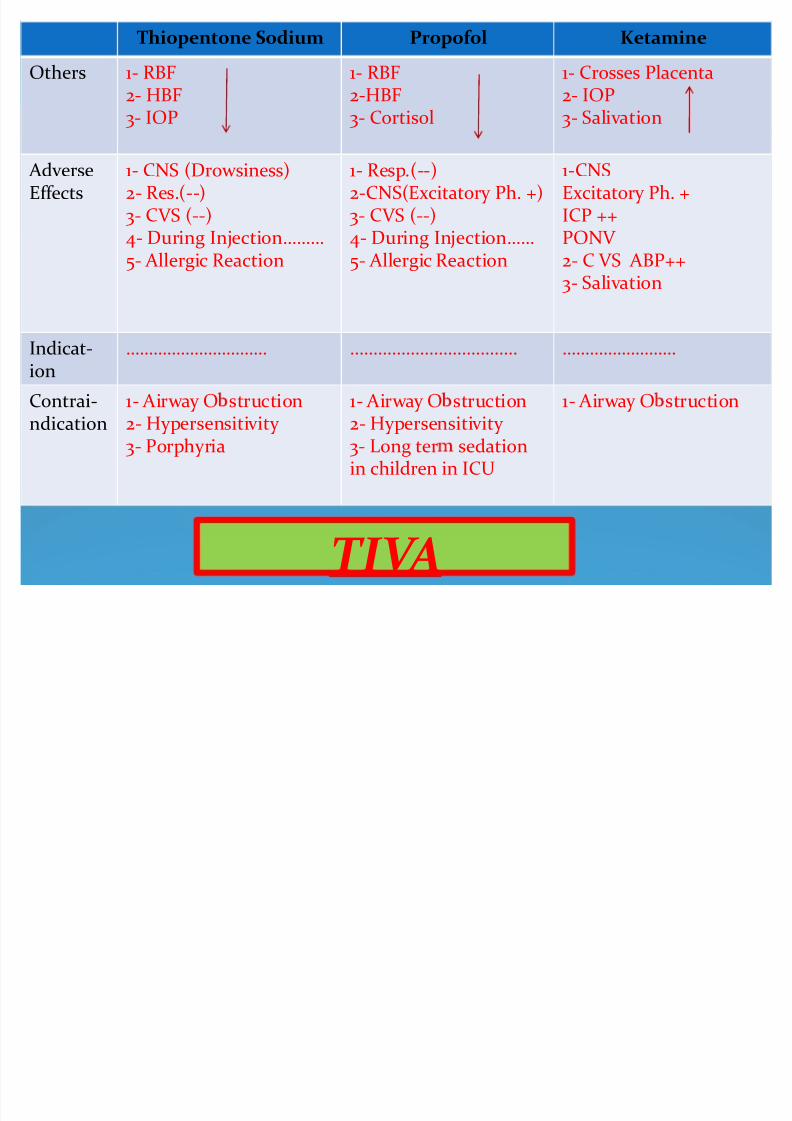
KetaminePropofolThiopentone Sodium
1- Crosses Placenta2- IOP3- Salivation
1- RBF2-HBF3- Cortisol
1- RBF2- HBF3- IOP
Others
1-CNSExcitatory Ph. +ICP ++PONV 2- C VS ABP++
3- Salivation
1- Resp.(--)2-CNS(Excitatory Ph. +)3- C VS (--)4- During Injection5- Allergic Reaction
1- CNS (Drowsiness)2- Res.(--)3- C VS (--)4- During Injection5- Allergic Reaction
AdverseEffects
......................................Indicat-ion
1- Airway O struction1- Airway O struction
2- Hypersensitivity 3- Long ter sedationin children in ICU
1- Airway O struction
2- Hypersensitivity 3- Porphyria
Contrai-
ndication
T I V A

8/8/2019 Pharmacology of Anesthesia 1
http://slidepdf.com/reader/full/pharmacology-of-anesthesia-1 18/18
THANK YOU