pfapa 09.04.2013
TRANSCRIPT
7/27/2019 PFAPA 09.04.2013
http://slidepdf.com/reader/full/pfapa-09042013 1/17
Morning Report
September 4th, 2013
Carrie Johnson

7/27/2019 PFAPA 09.04.2013
http://slidepdf.com/reader/full/pfapa-09042013 2/17
HPI•
In Urgent Care in August• You see a 3 yo Caucasian female with fever,
sore throat and swollen lymph nodes for 2days
• Fever reach 104 on day of presentation
• Complaining of throat pain, discomfort withswallowing
• Decreased oral intake
• Also complains of generalized stomach ache;no vomiting or diarrhea
7/27/2019 PFAPA 09.04.2013
http://slidepdf.com/reader/full/pfapa-09042013 3/17
HPI continued
• Some body aches, head aches intermittently
• No altered mental status
•
No cough, congestion, rhinorrhea, ear pain, orsnoring.
• No joint pain, rash, night sweats, weight loss.
•
No dysuria, no back pain• Using ibuprofen which seems to help fevers,
pain

7/27/2019 PFAPA 09.04.2013
http://slidepdf.com/reader/full/pfapa-09042013 4/17
• PMH/PSH:
– Bilateral Grade III VUR, no prophylaxis, no history of UTI.
– Has had a few similar episodes of lymph nodeenlargement and fever “fairly regularly” throughoutpast year. Always with a negative strep test. Had bloodwork done at PCPs office, slight elevation of WBC (20-
21), normal differential, platelet, hemoglobin, normalUA/culture. Received a course of antibiotics eachtime. Between episodes feels well.
• Unremarkable social history and family history.
No sick contacts, no daycare.• No medication use other than Ibuprofen during
illness

7/27/2019 PFAPA 09.04.2013
http://slidepdf.com/reader/full/pfapa-09042013 5/17
Physical Exam• Temp 102° F, HR 110, RR 20, BP 86/52
• Wt: 73%ile for age, Ht: 84%ile for age• Gen: Well nourished, non-toxic
• HEENT: EOMI, no conjunctival injection, TMs normal, naresclear. Posterior OP with erythema, thin tonsillar exudate.No lesions, masses, or ulcerations. Discomfort with
swallowing. • Neck: Full ROM, tender bilateral submandibular lymph
node enlargement (1.5 cm). No overlying erythema
• CV: RRR, no murmurs, rub, or gallop. Good perfusion
•
Resp: CTAB, no wheezing or crackles, no increased WOB• Abd: soft, no tenderness to palpation, normoactive BS
• Extrem: full ROM, nontender
• Skin: no rashes
7/27/2019 PFAPA 09.04.2013
http://slidepdf.com/reader/full/pfapa-09042013 6/17
Differential
• 3 year old female with recurrent episodes of
fever and tender lymph node enlargement.
7/27/2019 PFAPA 09.04.2013
http://slidepdf.com/reader/full/pfapa-09042013 7/17
DifferentialID
Lymphadenitis
Pharyngitis
-Group A strep (carrier in home?)
- viral (rhinovirus, parainflu, coronavirus, adenovirus,coxsackievirus, Human metapneumovirus)
- H flu, M catarrhalis, streppneumo, mycoplasma
Retropharyngeal AbscessPrevertebral Abscess
Atypical mycobacterium
Bartonella Henselae
EBV/CMV/HIV
Onc
Lymphoma
Neuroblastoma
Heme
Cyclic Neutropenia
Rheum/Imm-Serum Sickness
-PFAPA
-Familial Mediterranean fever
-Tumor Necrosis Factor
Receptor-associated PeriodicSyndrome (TRAPS)
-Hyperimmunoglobulin D
Syndrome
-SLE
-Sarcdoidosis-Histiocytic necrotizing
lymphadenitis (Kikuchi Disease)

7/27/2019 PFAPA 09.04.2013
http://slidepdf.com/reader/full/pfapa-09042013 8/17
More Past Medical History
• When digging through the chart more…
• First presented with similar illness with high fever andswollen lymph nodes nine months ago.
• Since then, doctor’s office visit every 4-8 weeks for
same symptoms.• Always with a negative rapid strep and culture. Often
diagnosed with Cervical lymphadenitis or AOM.Received 5 courses of antibiotics
•
Resolution of symptoms in between• Patient lovingly nicknamed her lymph nodes “my
rocks,” and anticipated their reappearance every 4-6weeks.
7/27/2019 PFAPA 09.04.2013
http://slidepdf.com/reader/full/pfapa-09042013 9/17
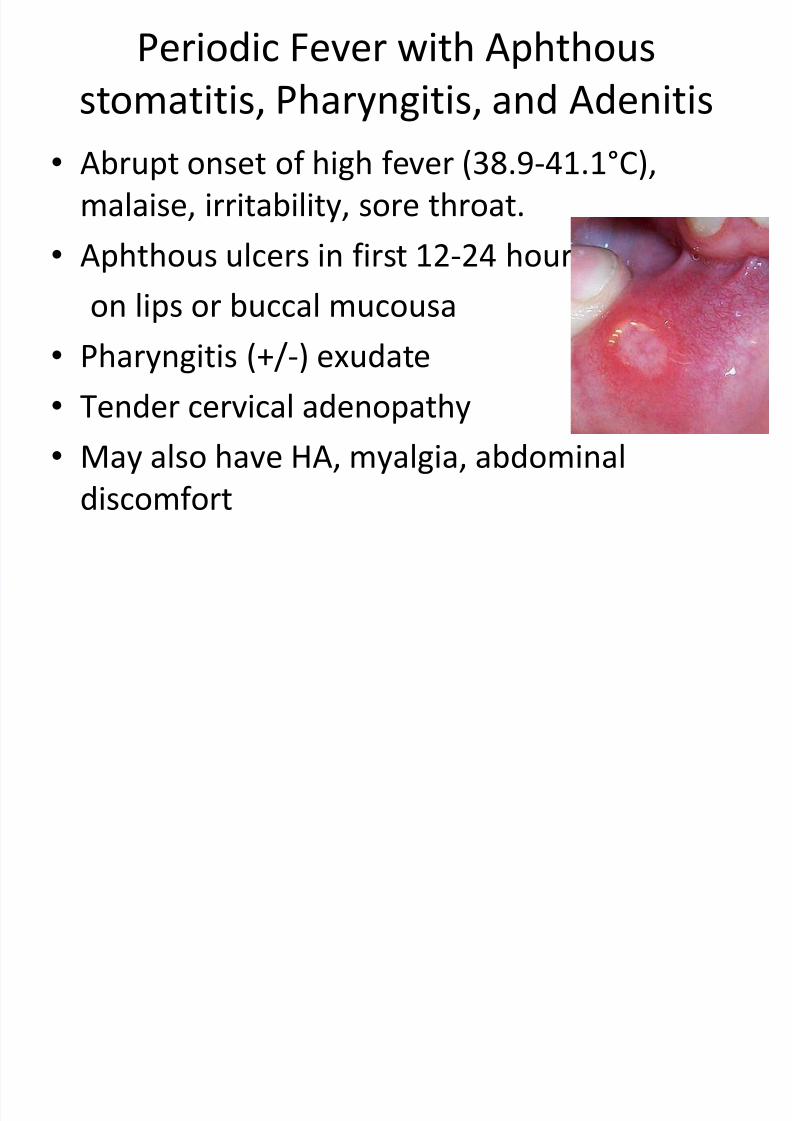
Periodic Fever with Aphthous
stomatitis, Pharyngitis, and Adenitis
• Abrupt onset of high fever (38.9-41.1°C),
malaise, irritability, sore throat.
• Aphthous ulcers in first 12-24 hours
on lips or buccal mucousa
• Pharyngitis (+/-) exudate
•
Tender cervical adenopathy• May also have HA, myalgia, abdominal
discomfort

7/27/2019 PFAPA 09.04.2013
http://slidepdf.com/reader/full/pfapa-09042013 10/17
Natural Course of Illness
• Onset age 2 to 5 years old
• Benign, self limited (unknown etiology)
• Mean duration of attacks ranges from 4.5 to 8
years.• With time, episodes are of shorter duration and
occur less frequently.
•
Within 5-7 years of onset, most childrenasymptomatic.
• Limited cases occurring in adulthood
7/27/2019 PFAPA 09.04.2013
http://slidepdf.com/reader/full/pfapa-09042013 11/17
Laboratory Findings
• May have mild leukocytosis (15-19), Elevation
of ESR ( 49 +/- 30 mm/hr), CRP increase (~ 2.5
to 7 mg/dl).
• No increased presence of ANA above baseline
population estimates ( 1 in 30 children)
• All lab values normalize between episodes
• Strep test should be negative.
– If positive may represent benign carriage

7/27/2019 PFAPA 09.04.2013
http://slidepdf.com/reader/full/pfapa-09042013 12/17
Diagnosis
Based on Clinical Presentation
• 3+ episodes of fever no more than 5 days at
regular intervals (on average Q 3-6 weeks)
• Pharyngitis + aphthous ulcers OR tender
cervical LAD
• Normal growth parameters, good health
between episodes (no B symptoms)
7/27/2019 PFAPA 09.04.2013
http://slidepdf.com/reader/full/pfapa-09042013 13/17
Treatment
• Optional
• NSAIDS, tylenol for fevers
• Tonsillectomy (Controversial) – Small study (N 39): Remission in 63%,
• Prednisone (benefit vs. harm) – Single dose of 1-2 mg/kg has dramatic response on fever, pharyngitis
within hours
– Repeated doses shorten the interval between attacks in 25% of cases
– Can try Colchicine to extend interval between attacks but effect isshort lived.
•Cimetidine (Case Reports) – 20-40 mg/kg divided BID
– May help with reducing or eliminating recurrent episodes
– Continue drug therapy for 6 months if initial benefit
7/27/2019 PFAPA 09.04.2013
http://slidepdf.com/reader/full/pfapa-09042013 14/17
PFAPA must be excluded when…
• Family history of recurrent fever (consider
hereditary autoinflammatory syndromes)
• Elevated CRP/ESR between attacks (suggests
chronic inflammation)
• Atypical symptoms (are not consistent with
previous pattern)
• Neutropenia (consider cyclic neutropenia)

7/27/2019 PFAPA 09.04.2013
http://slidepdf.com/reader/full/pfapa-09042013 15/17
Cyclic Neutropenia
• Rare
• Onset in first year of life
• Recurring fevers and neutropenia ANC <200
(very consistent time frame for the individual;range 14-35 days)
• Familial pattern (AD inheritance)
• Symptoms: malaise, fever, aphthousstomatitis, gingival/mucosal infection,sub/cutaneous infections
7/27/2019 PFAPA 09.04.2013
http://slidepdf.com/reader/full/pfapa-09042013 16/17
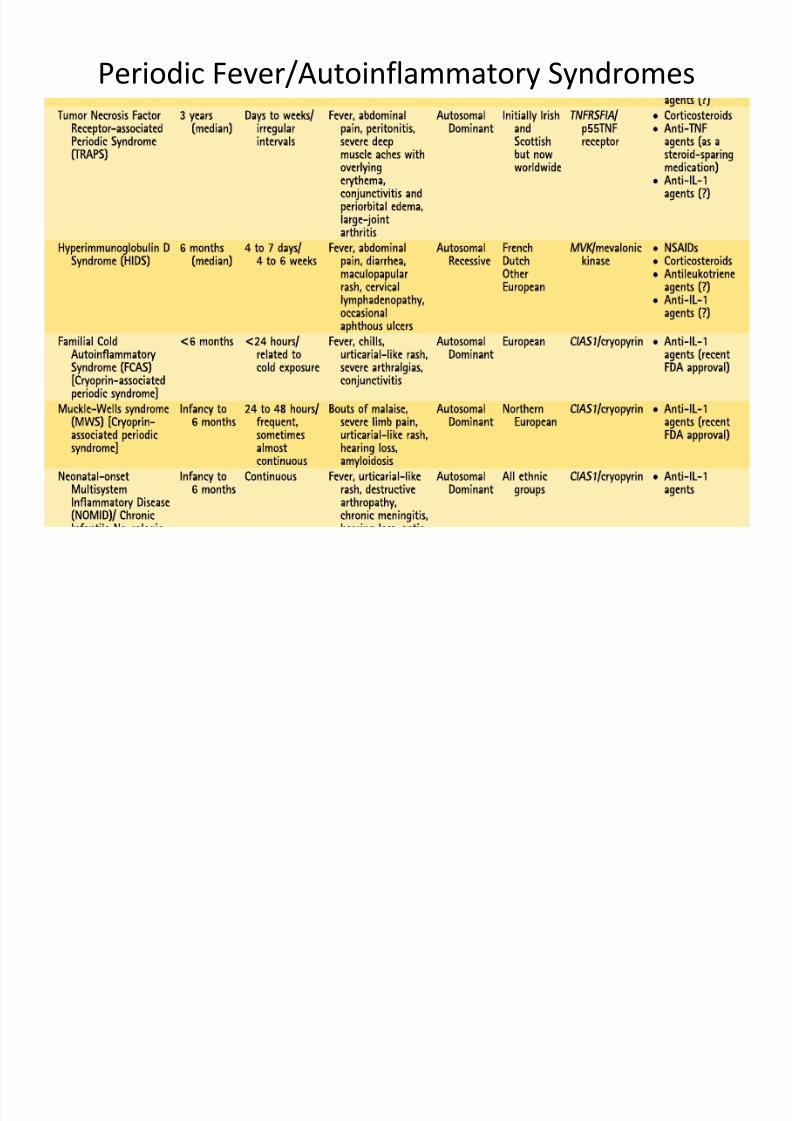
Periodic Fever/Autoinflammatory Syndromes

7/27/2019 PFAPA 09.04.2013
http://slidepdf.com/reader/full/pfapa-09042013 17/17
References
• Donald Goldsmith. Periodic Fever Syndromes.Pediatrics in Review Vol 30 No.5, May 2009.
• Shashi Sahai. Lymphadenopathy. Pediatrics in
Review 2013;34;216. DOI: 10.1542/pir.34-5-216• Thomas KT, Feder HM Jr, Lawton AR, Edwards
KM. Periodic Fever syndrome in children Journalof Pediatrics. 1999; 135: 15.
• Shai Padeh, MD. Periodic Fever with aphthousstomatitis, pharyngitis, and adenitis (PFAPAsyndrome). Uptodate.com