pet and lung cancer
TRANSCRIPT

8/3/2019 Pet and Lung Cancer
http://slidepdf.com/reader/full/pet-and-lung-cancer 1/15
Positron Emission Tomography/Computed Tomographyin Lung Cancer Staging, Prognosis, and Assessment
of Therapeutic ResponseMylene T. Truong, MD, Chitra Viswanathan, MD, and Jeremy J. Erasmus, MD
Abstract: Positron emission tomography (PET)/computed tomo-graphic scanning, using 18F-2-deoxy-D-glucose, complementsconventional imaging evaluation of patients with lung cancer.The strength of PET scanning lies in the detection of nodal andextrathoracic metastases. PET scanning is also currently beingstudied in the assessment of prognosis and therapeutic response
and has the potential to alter management of oncologic patients.This review will discuss the role of PET/computed tomographicscanning in the diagnosis, staging, and evaluation of prognosis andtreatment response in patients with lung cancer.
Key Words: lung cancer, staging, positron emission tomography/
computed tomography
(J Thorac Imaging 2011;26:132–146)
Lung cancer is a common malignancy. The AmericanCancer Society estimated that 219,440 new cases were
diagnosed in the United States in 2009 (www.cancer.org)and that lung cancer accounted for 28% of all cancer
deaths in 2009. Imaging plays an integral role in thedetection, diagnosis, and staging of the disease, as wellas in the assessment of treatment response and in thesurveillance for tumor recurrence after therapy. Typically,imaging with computed tomographic (CT) scanning isused to assess the anatomic extent of the disease andto determine appropriate treatment. Positron emissiontomography (PET) using the radiopharmaceutical 18F-2-deoxy-D-glucose (FDG), a D-glucose analog labeled withfluorine-18, complements conventional radiologic assess-ment in the evaluation of patients with lung cancer andimproves the detection of nodal and extrathoracic meta-static disease. Metabolism of glucose is typically increasedin malignancies due to an overexpression of glucose
transporter receptors on the surface of tumor cells and anupregulation of hexokinase (a phosphorylating enzyme).Due to a downregulation of phosphatase, FDG is unable toenter intracellular glycolytic pathways and is sequestered intumor cells. The most common semiquantitative method of evaluating malignancies using PET is FDG standardizeduptake value (SUV) calculated as a ratio of tissue radio-tracer concentration (mCi/mL) and injected dose (mCi) atthe time of injection divided by body weight (in grams).Most factors that change SUV measurements affect the
measurement of the radioactivity concentration. Biologicalfactors, such as patient blood glucose level, uptake timeof the tracer, and respiratory motion, can impact SUVmeasurements. Technologic factors, such as variabilityamong different scanners, image acquisition and recon-struction parameters, and interobserver variability, can
impact SUV measurements as well.1
Thus, it is important tokeep as many of these factors as possible the same betweenbaseline and follow-up studies of a patient. An SUVthreshold of 2.5 has been used to differentiate benign frommalignant nodules.2 In the staging of lung cancer, imaginghas evolved from an anatomic basis with CT scanningalone to a combination of anatomic and functional datawith the introduction of PET scanning. Initially, PETscanning was performed separately from CT scanning,and the 2 studies were viewed side by side with visualcorrelation. This was succeeded by various software-basedalgorithms to fuse CT and PET scanning data once thestudies had been acquired separately.3 Finally, integratedwhole-body PET/CT imaging has enabled the acquisition
of coregistered, spatially matched functional data of PETscanning and anatomic data of CT scanning in a singleexamination. This review will discuss the current applica-tions of PET/CT scanning in the diagnosis, staging, andassessment of prognosis, treatment response, and tumorrecurrence in patients with lung cancer.
BACKGROUNDA typical whole-body PET scan is performed 60
minutes after the intravenous administration of FDG. Withan acquisition time of 4 to 6 minutes per bed position, thetotal imaging time is 30 to 40 minutes. When quantitativeassessment of FDG metabolism is needed, for example, forthe evaluation of the therapeutic response, correction
for soft tissue attenuation is important. To use CT scanningfor attenuation correction, the attenuation values of low-dose CT energies must be scaled to high-dose (511 keV)PET energies using scaling algorithms. CT-based attenua-tion correction in integrated PET/CT scanning results in alower noise emission scan and faster acquisition times, and,thus, fewer motion artifacts and a higher throughput. Withintegrated PET/CT scanners, the use of CT scanning forattenuation correction of the PET images has introducedartifacts and quantitative errors that can affect the emissionimage and lead to misinterpretation.4 These artifacts relateto patient respiration, the use of intravenous and oral CTcontrast media, and the presence of catheters and othermetal objects in the patients.5 For example, imaging during
different stages of the patient’s respiratory cycle mayintroduce a mismatch between the CT scan attenuationdata obtained during breathhold and the PET emissionCopyright r 2011 by Lippincott Williams & Wilkins
From the Division of Diagnostic Imaging, University of Texas M.D.Anderson Cancer Center, Houston, TX.
Reprints: Mylene T. Truong, MD, M.D. Anderson Cancer Center,Division of Diagnostic Imaging Unit 1478, 1515 Holcombe boulevard,Houston, TX 77030 (e-mail: [email protected]).
SYMPOSIA
132 | www.thoracicimaging.com J Thorac Imaging Volume 26, Number 2, May 2011

8/3/2019 Pet and Lung Cancer
http://slidepdf.com/reader/full/pet-and-lung-cancer 2/15
data obtained during quiet tidal breathing.6,7 In addition tolocalization errors, this misregistration may also result inincorrect attenuation coefficients applied to the PET datathat can affect the SUV, the most widely used parameter toquantify FDG uptake.6,8 Misregistration may lead to SUVbeing lower than expected and can potentially result in a
false-negative study. Strategies to reduce the respiratorymismatch between the CT and PET images include perform-ing the CT scanning at end expiration, which most closelyapproximates the lung volumes during PET data acquisitionat quiet tidal breathing. However, CT scans of the lungsat end expiration compromise anatomic detail and smallnodules may be obscured. A more recent approach suggeststhe use of respiratory-averaged CT scanning (CT cine imagesobtained over different portions of the respiratory cycle using4-dimensional CT scanning techniques) to improve SUVquantification.9 Respiratory-averaged CT scanning used forattenuation correction of a PET scan has shown SUVdifferences of more than 50% in some lesions, compared withthe standard method of CT attenuation using data obtained
in the mid-expiratory phase.9,10
DIAGNOSISAs many patients with early-stage lung cancer can
present with a solitary pulmonary nodule (SPN), animportant imaging goal is to accurately differentiatemalignant from benign lesions. The use of PET/CTscanning is established in the evaluation of SPNs. In ameta-analysis of 40 studies, PET scanning was found tooperate at a point on the summary receiver operatingcharacteristic curve corresponding to a sensitivity of 96.8%and a specificity of 78% for the detection of malignancyin nodules of 10mm or greater in diameter.11 Using a
threshold SUV of 2.5 and comparing with backgroundactivity in the mediastinum, Rohren and Lowe12 reported asensitivity of 95% and a specificity of 81% for malignancyby compiling data from 7 studies evaluating PET scansand pulmonary nodules. In a study comparing integratedPET/CT scans and helical dynamic CT scans in theevaluation of SPNs, PET/CT scanning was more sensitive(96% vs. 81%) and accurate (93% vs. 85%) than helicaldynamic CT scanning.13 A recent prospective integratedPET/CT scanning study evaluating 585 patients (496malignant and 89 benign nodules) showed that although anodule with high SUV (>4.1) was associated with a 96%likelihood of malignancy, a nodule with low SUV (<2.5)was also associated with a 25% likelihood of malignancy.14
This underscores the importance of accurate SUV measure-ments in PET/CT scan interpretation.
It is important to note that the high sensitivity andspecificity of PET scanning in the evaluation of SPNspertain to solid nodules of 10 mm or greater in diameter.In contrast, FDG uptake in malignant ground-glass andpartially solid nodules is variable and cannot be usedreliably to distinguish benign from malignant lesions (Fig. 1).In a recent study, 9 of 10 well-differentiated adenocarcino-mas presenting as ground-glass nodular opacities werefalsely negative on PET scanning, whereas 4 of 5 benignground-glass nodular opacities were falsely positive.15 Thesensitivity (10%) and specificity (20%) for ground-glassopacities in this study were significantly lower than those
for solid nodules (90% and 71%, respectively). Limitationsin spatial resolution can also result in false-negative studieswhen lesions <10 mm in diameter are evaluated.15,16 With
advances in PET technology, the evaluation of nodules of approximately 7 mm is possible.17 Thus, PET scanning isnot recommended in the routine evaluation of small lungnodules. Otherwise, false-negative PET scanning resultsare uncommon, but may occur with carcinoid tumors,bronchioloalveolar carcinomas, and early-stage disease.18–21
The lower positive predictive value (PPV) relates to the false-positive lesions due to infection and inflammation. False-positive lesions have been reported to include pulmonaryhamartoma, pneumonia, caseating granulomas, sarcoidosis,amyloidosis, talc pleurodesis, rounded atelectasis, pleuralfibrosis, and atherosclerosis.22
The usefulness of PET scanning in the evaluation of SPNs takes into consideration clinical risk factors such aspatient age, smoking history and history of malignancy,as well as imaging characteristics, to determine patientmanagement. For instance, in a patient with a low pretestlikelihood of malignancy (20%) being considered for serialimaging reassessment, a negative PET scan will reducethe likelihood of malignancy to 1% and would support
conservative management.11,23 However, in a patient with ahigh pretest likelihood of malignancy (80%), a negativePET scan will only reduce the likelihood of malignancy to14%.23,24 Accordingly, obtaining tissue for diagnosis withbiopsy or resection is recommended. Although the addi-tional benefit of PET scanning as a function of clinicalpretest risk assessment for malignancy has not been clearlyestablished, a recent cost-effectiveness analysis supports thisdiagnostic strategy.25
STAGINGIn patients with non-small cell lung cancer (NSCLC),
staging, the assessment of the anatomic extent of disease at
presentation determines treatment and prognosis. Patientsare typically staged according to the TNM (Tumor, Node,Metastasis) classification system. In 2009, the seventhedition of the TNM staging system for lung cancer waspublished by the International Union Against Cancer andthe American Joint Committee on Cancer, based onproposals from the International Staging Project of theInternational Association for the Study of Lung Cancer,which will be reviewed in depth in another section in thissymposium.
In terms of the T, N, and M descriptors, stagingevaluation is usually aimed at distinguishing resectablefrom unresectable disease (T4 or N3 or M1). Thedifferentiation of T1 to T3 from T4 lung cancer and the
detection of contralateral nodal (N3) and/or metastases(M1) are important, as these descriptors typically precludesurgical resection or require additional chemotherapy orradiotherapy. Recently, the American Society of ClinicalOncology (ASCO) published evidence-based guidelines forthe diagnostic evaluation of patients with NSCLC.26 Asstated in these guidelines, chest radiography and contrast-enhanced chest CT scanning, which includes the liver andadrenals, are performed in the initial staging of lung cancer.
Whole-body PET scanning is an integral componentof NSCLC staging, as it improves the detection of nodaland distant metastases and frequently changes patientmanagement.27–32 PET scanning complements radiologicfindings, and the ASCO recommendations are that PET
scanning should be performed when there is no evidence of distant metastatic disease on CT scan.26 Integrated PET/CT scanning, with coregistration of PET and CT images,
J Thorac Imaging Volume 26, Number 2, May 2011 PET/CT in Evaluation of Lung Cancer
r 2011 Lippincott Williams & Wilkins www.thoracicimaging.com | 133

8/3/2019 Pet and Lung Cancer
http://slidepdf.com/reader/full/pet-and-lung-cancer 3/15
overcomes the limitations inherent in both modalities when
used separately. In fact, staging of NSCLC has beenreported to be more accurate with integrated PET/CTscanning than when using visual correlation of PET and CTimages taken separately.28,33
T Descriptor In the evaluation of the primary tumor (T descriptor),
the anatomic information provided by CT scanning compen-sates for the relatively poor spatial resolution of the PETscan. The CT scan is used to determine the characteristicsof the primary tumor, including size, location, and anatomicrelationship to adjacent structures such as the pleura,mediastinum, and bones, as well as for the detection of smallnodules in the same lobe (T3), same lung (T4), or contralateral
lung (M1a). PET/CT scanning has no real advantage over CTscanning for assessing chest wall or mediastinal invasion.However, for central tumors causing collapse of a lobe or alung, PET/CT scanning can differentiate tumor from adjacentlung atelectasis (Fig. 2). This aids in radiation therapy (RT)planning and reduces toxicity to the normal tissues.34 In arecent study, PET/CT scanning was found to be superior toCT scanning alone and PET scanning alone in T stagingaccuracy (82% vs. 68% vs. 55%).5
N Descriptor The most important prognostic factor in patients
with localized and resectable NSCLC is nodal disease
(N descriptor).35 Accurate lymph node staging is essential,
and CT scanning is generally used to evaluate hilar andmediastinal lymph nodes. Size is typically the only criterionused for differentiating normal from abnormal nodes with athreshold of 1 cm for the short-axis diameter. However,node size has not been shown to be a reliable parameter forthe evaluation of nodal metastatic disease in patients withNSCLC.36–38 Prenzel et al36 reported that in 2891 resectedhilar and mediastinal nodes in 256 patients with NSCLC,77% of the 139 patients with no nodal metastases had atleast 1 node >1 cm in diameter. With regard to the lymphnodes with histologic signs of metastases (405), 44% (180lymph nodes) were <1 cm.36 Furthermore, 12% of the 127patients with nodal metastases had no nodes >1 cm. Arecent meta-analysis of 20 studies (3438 patients) evaluating
CT scanning accuracy for staging the mediastinum yieldeda pooled sensitivity of 57% and a specificity of 82%.39
Interestingly, PET/CT scanning enhanced accuracyof nodal staging in patients with NSCLC and underlyingpulmonary fibrosis. Patients with pulmonary fibrosis have a5-fold to 14-fold increased risk of developing lung cancerand frequently have reactive mediastinal lymph nodeenlargement (55% to 93% of cases). PET/CT scanning inpatients with pulmonary fibrosis had similar sensitivity(60% vs. 60%), better specificity (91% vs. 47%) and betteraccuracy (83% vs. 50%) than CT scanning alone. This wascompared with sensitivity (63% vs. 40%), specificity (96%vs. 84%), and accuracy (88% vs. 73%) in patients withoutpulmonary fibrosis.40
FIGURE 1. A 62-year-old woman with chest and shoulder pain. CT scan (A) shows a 2.5cm right upper lobe lesion with mixedattenuation associated with an air bronchogram. Note the spiculated solid component (arrow) and the ground-glass component(arrowheads). PET/CT scan (B) and PET scan (C) show low-grade FDG uptake in the lung lesion (SUV, 1.6). Resection revealedadenocarcinoma with bronchioloalveolar features. False-negative PET scan may be due to slow cell proliferation or poor cellularity.
FIGURE 2. A 48-year-old man with hemoptysis and left upper lobe collapse due to central obstructing tumor. On contrast-enhanced CTscan (A), it is difficult to differentiate the tumor from the adjacent atelectatic lung. PET/CT scan (B) shows the FDG-avid 3 cm centraltumor (SUV, 11.8) within the nonhypermetabolic collapsed lung parenchyma. Delineation of the primary tumor is important for radiation treatment planning.
Truong et al J Thorac Imaging Volume 26, Number 2, May 2011
134 | www.thoracicimaging.com r 2011 Lippincott Williams & Wilkins

8/3/2019 Pet and Lung Cancer
http://slidepdf.com/reader/full/pet-and-lung-cancer 4/15
As the treatment decisions concerning surgery andpotential use of adjuvant therapy are dependent on patients’N descriptor, improvement in the accuracy of detection of nodal metastases is needed. PET scanning complements CTfindings and provides information on locoregional nodalstaging that can impact management.30,41,42 In a recent
meta-analysis of 17 studies (833 patients), PET scanning wassuperior to CT scanning in the detection of nodal metastaticdisease, with sensitivities of 83% versus 59% and specificitiesof 92% versus 78%.41 Recently, significant improvements inthe accuracy of overall staging have been reported whenusing integrated PET/CT scanning compared with CT andPET scanning when interpreted separately.33
In many institutions, mediastinoscopy and, morerecently, endoscopic ultrasound-guided and endobronchialultrasound-guided biopsy of nodes are performed toaccurately determine the presence and location of nodalmetastases in patients with NSCLC.30,43 The precise role of PET scanning with regard to invasive nodal staging isunclear, but should be considered an adjunct rather than
an alternative.26,30 In an attempt to determine the needfor mediastinoscopy after PET and CT imaging, a meta-analysis evaluated the association between the size of mediastinal lymph nodes and the probability of malig-nancy.44 In patients with a negative PET scan and lymphnodes of 10 to 15 mm in size on CT scanning, the posttestprobability for N2 disease was only 5%. Consequently, theresearchers suggest that these patients should proceeddirectly to thoracotomy. In patients with a negative PETscan and lymph nodes of >16 mm on CT scanning, theposttest probability for N2 disease was 21%, and theresearchers suggest that these patients should have medias-tinoscopy prior to thoracotomy (Fig. 3). In patients with T1lung cancer and good performance status, the finding of
PET-negative nodes of <10 mm in size on CT scanningwould favor surgical resection without preoperative in-vasive nodal sampling due to the high negative predictivevalue (NPV) of a PET scan. In patients with poorperformance status, the treatment is stereotactic orintensity-modulated RT without pretreatment invasivenodal sampling.
Although PET scanning for nodal staging is cost-effective and can reduce the likelihood that a patient withN3 disease would undergo attempted resection, decisionanalyses show that the number of false-positive resultsdue to infectious or inflammatory etiologies is too highto preclude mediastinoscopy.45,46 Consequently, invasive
sampling of FDG-avid nodes is recommended to confirmnodal metastatic disease in patients in whom accurateN staging may impact management. For example, if theipsilateral mediastinal nodes (N2 disease) are histologicallypositive for malignancy by invasive sampling, patients aretreated with chemotherapy and then possibly surgery. If the
contralateral nodes (N3 disease) are positive for malig-nancy, patients would receive chemotherapy and RT. In thelatter scenario, PET/CT scanning aids in the delineation of the radiation treatment planning for the primary tumor andthe nodal metastases.
M Descriptor Distant metastases (M1) occur in 21% of patients with
NSCLC.47 Common sites of metastases are the adrenalglands, liver, brain, bones, and abdominal lymph nodes.47
Imaging evaluation for metastatic disease is often deter-mined by clinical history and physical examination. Whole-body PET scanning is increasingly being used to improvethe accuracy of staging due to its strength in the detection
of metastases, some of which may be clinically occult. PETscanning has a higher sensitivity and specificity than CTscanning in detecting metastases to the adrenals, bones,and extrathoracic lymph nodes. The American College of Surgeons Oncology Trial reports a sensitivity, specificity,PPV, and NPV of 83%, 90%, 36%, and 99%, respectively,for M1 disease.30
Whole-body PET imaging stages intrathoracic andextrathoracic disease in a single examination, detects occultextrathoracic metastases in up to 24% of patients selectedfor curative resection, and has been shown to be cost-effective.27,30,32,48,49 Schrevens et al50 reported that aftera negative conventional staging, occult metastases werefound on PET scans in 5% to 29% of the patients.
MacManus et al49 reported that the incidence of occultmetastases increases with the increase in T and N staging,that is, 7.5% in early-stage disease compared with 24% inadvanced disease. A recent randomized controlled trialevaluating the role of PET scanning in early-stage lungcancer (>90% T1-2N0) showed that distant metastaseswere rarely detected (<5%), and the researchers concludedthat PET scanning improves the accuracy of staging andleads to more stage-specific therapy.51 In addition, 2 studieswith a higher proportion of more advanced lung cancers,considered resectable by conventional staging, showed thatthe addition of PET scanning prevented futile surgery in1 in 5 patients.30,48
FIGURE 3. A 61-year-old man with a 4-month history of cough. CT scan (A) shows a left upper lobe mass and right paratrachealadenopathy (asterisk) measuring 2 cm in short-axis diameter. PET/CT scan (B) shows FDG-avidity in the primary tumor (SUV, 15) and lefthilar adenopathy. However, the right paratracheal adenopathy (asterisk) has FDG uptake similar to that of the mediastinal blood pool.Mediastinoscopy confirmed N3 (contralateral nodal) disease from the primary lung cancer and the patient was treated palliatively.
A negative PET scan does not preclude biopsy of enlarged mediastinal lymph nodes.
J Thorac Imaging Volume 26, Number 2, May 2011 PET/CT in Evaluation of Lung Cancer
r 2011 Lippincott Williams & Wilkins www.thoracicimaging.com | 135
8/3/2019 Pet and Lung Cancer
http://slidepdf.com/reader/full/pet-and-lung-cancer 5/15
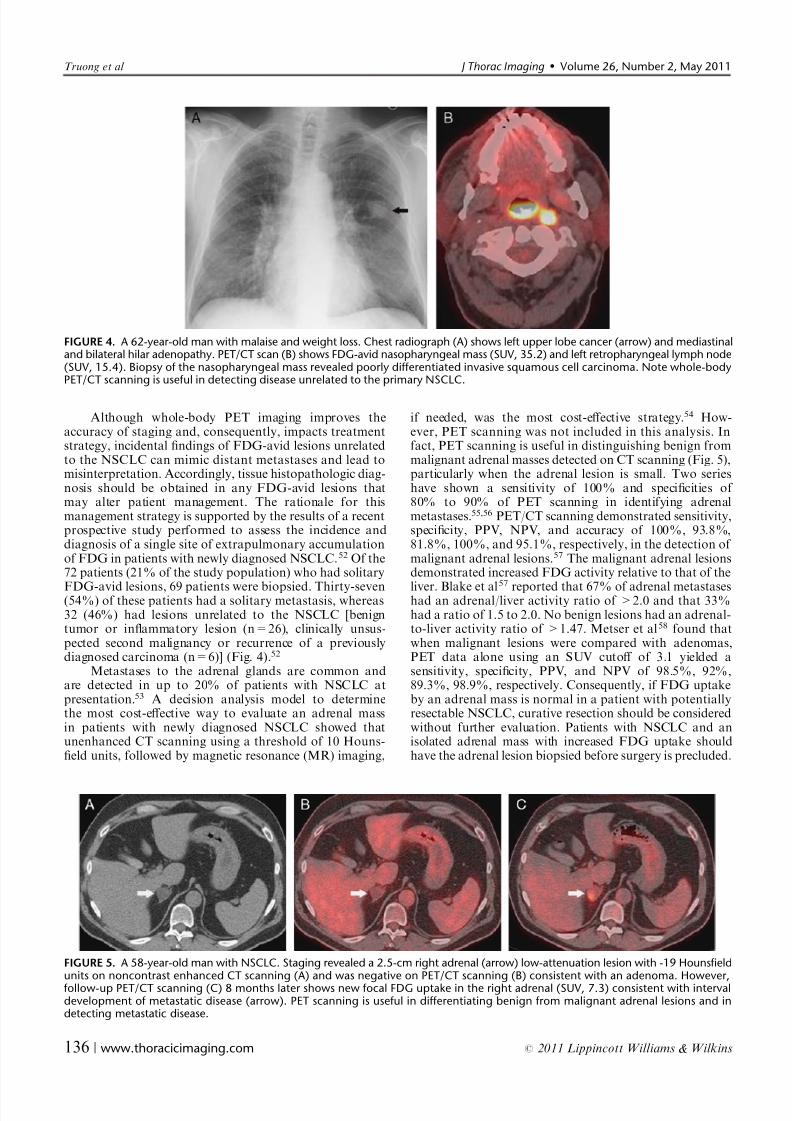
Although whole-body PET imaging improves theaccuracy of staging and, consequently, impacts treatmentstrategy, incidental findings of FDG-avid lesions unrelatedto the NSCLC can mimic distant metastases and lead tomisinterpretation. Accordingly, tissue histopathologic diag-nosis should be obtained in any FDG-avid lesions thatmay alter patient management. The rationale for thismanagement strategy is supported by the results of a recentprospective study performed to assess the incidence anddiagnosis of a single site of extrapulmonary accumulationof FDG in patients with newly diagnosed NSCLC.52 Of the72 patients (21% of the study population) who had solitary
FDG-avid lesions, 69 patients were biopsied. Thirty-seven(54%) of these patients had a solitary metastasis, whereas32 (46%) had lesions unrelated to the NSCLC [benigntumor or inflammatory lesion (n=26), clinically unsus-pected second malignancy or recurrence of a previouslydiagnosed carcinoma (n=6)] (Fig. 4).52
Metastases to the adrenal glands are common andare detected in up to 20% of patients with NSCLC atpresentation.53 A decision analysis model to determinethe most cost-effective way to evaluate an adrenal massin patients with newly diagnosed NSCLC showed thatunenhanced CT scanning using a threshold of 10 Houns-field units, followed by magnetic resonance (MR) imaging,
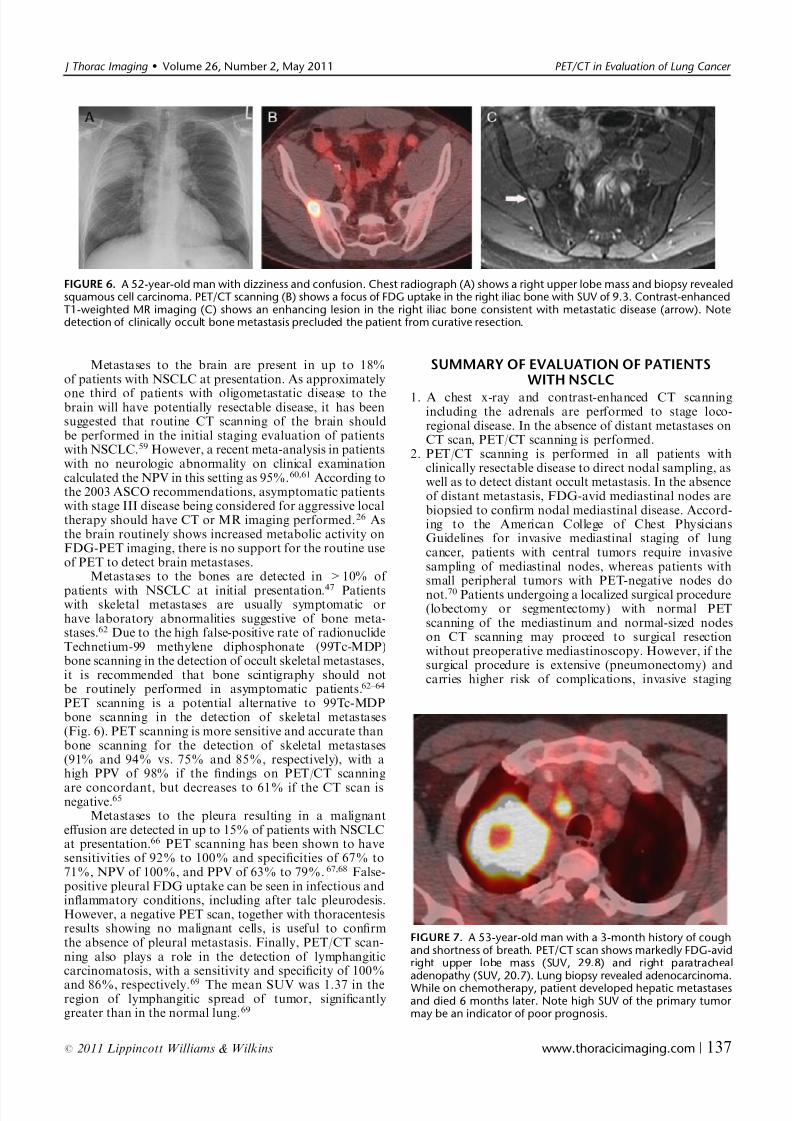
if needed, was the most cost-effective strategy.54 How-ever, PET scanning was not included in this analysis. Infact, PET scanning is useful in distinguishing benign frommalignant adrenal masses detected on CT scanning (Fig. 5),particularly when the adrenal lesion is small. Two serieshave shown a sensitivity of 100% and specificities of 80% to 90% of PET scanning in identifying adrenalmetastases.55,56 PET/CT scanning demonstrated sensitivity,specificity, PPV, NPV, and accuracy of 100%, 93.8%,81.8%, 100%, and 95.1%, respectively, in the detection of malignant adrenal lesions.57 The malignant adrenal lesionsdemonstrated increased FDG activity relative to that of the
liver. Blake et al57
reported that 67% of adrenal metastaseshad an adrenal/liver activity ratio of >2.0 and that 33%had a ratio of 1.5 to 2.0. No benign lesions had an adrenal-to-liver activity ratio of >1.47. Metser et al58 found thatwhen malignant lesions were compared with adenomas,PET data alone using an SUV cutoff of 3.1 yielded asensitivity, specificity, PPV, and NPV of 98.5%, 92%,89.3%, 98.9%, respectively. Consequently, if FDG uptakeby an adrenal mass is normal in a patient with potentiallyresectable NSCLC, curative resection should be consideredwithout further evaluation. Patients with NSCLC and anisolated adrenal mass with increased FDG uptake shouldhave the adrenal lesion biopsied before surgery is precluded.
FIGURE 4. A 62-year-old man with malaise and weight loss. Chest radiograph (A) shows left upper lobe cancer (arrow) and mediastinaland bilateral hilar adenopathy. PET/CT scan (B) shows FDG-avid nasopharyngeal mass (SUV, 35.2) and left retropharyngeal lymph node(SUV, 15.4). Biopsy of the nasopharyngeal mass revealed poorly differentiated invasive squamous cell carcinoma. Note whole-bodyPET/CT scanning is useful in detecting disease unrelated to the primary NSCLC.
FIGURE 5. A 58-year-old man with NSCLC. Staging revealed a 2.5-cm right adrenal (arrow) low-attenuation lesion with -19 Hounsfieldunits on noncontrast enhanced CT scanning (A) and was negative on PET/CT scanning (B) consistent with an adenoma. However,follow-up PET/CT scanning (C) 8 months later shows new focal FDG uptake in the right adrenal (SUV, 7.3) consistent with intervaldevelopment of metastatic disease (arrow). PET scanning is useful in differentiating benign from malignant adrenal lesions and indetecting metastatic disease.
Truong et al J Thorac Imaging Volume 26, Number 2, May 2011
136 | www.thoracicimaging.com r 2011 Lippincott Williams & Wilkins
8/3/2019 Pet and Lung Cancer
http://slidepdf.com/reader/full/pet-and-lung-cancer 6/15
Metastases to the brain are present in up to 18%of patients with NSCLC at presentation. As approximately
one third of patients with oligometastatic disease to thebrain will have potentially resectable disease, it has beensuggested that routine CT scanning of the brain shouldbe performed in the initial staging evaluation of patientswith NSCLC.59 However, a recent meta-analysis in patientswith no neurologic abnormality on clinical examinationcalculated the NPV in this setting as 95%.60,61 According tothe 2003 ASCO recommendations, asymptomatic patientswith stage III disease being considered for aggressive localtherapy should have CT or MR imaging performed.26 Asthe brain routinely shows increased metabolic activity onFDG-PET imaging, there is no support for the routine useof PET to detect brain metastases.
Metastases to the bones are detected in >10% of
patients with NSCLC at initial presentation.47 Patientswith skeletal metastases are usually symptomatic orhave laboratory abnormalities suggestive of bone meta-stases.62 Due to the high false-positive rate of radionuclideTechnetium-99 methylene diphosphonate (99Tc-MDP)bone scanning in the detection of occult skeletal metastases,it is recommended that bone scintigraphy should notbe routinely performed in asymptomatic patients.62–64
PET scanning is a potential alternative to 99Tc-MDPbone scanning in the detection of skeletal metastases(Fig. 6). PET scanning is more sensitive and accurate thanbone scanning for the detection of skeletal metastases(91% and 94% vs. 75% and 85%, respectively), with ahigh PPV of 98% if the findings on PET/CT scanning
are concordant, but decreases to 61% if the CT scan isnegative.65
Metastases to the pleura resulting in a malignanteffusion are detected in up to 15% of patients with NSCLCat presentation.66 PET scanning has been shown to havesensitivities of 92% to 100% and specificities of 67% to71%, NPV of 100%, and PPV of 63% to 79%.67,68 False-positive pleural FDG uptake can be seen in infectious andinflammatory conditions, including after talc pleurodesis.However, a negative PET scan, together with thoracentesisresults showing no malignant cells, is useful to confirmthe absence of pleural metastasis. Finally, PET/CT scan-ning also plays a role in the detection of lymphangiticcarcinomatosis, with a sensitivity and specificity of 100%
and 86%, respectively.69 The mean SUV was 1.37 in theregion of lymphangitic spread of tumor, significantlygreater than in the normal lung.69
SUMMARY OF EVALUATION OF PATIENTSWITH NSCLC
1. A chest x-ray and contrast-enhanced CT scanningincluding the adrenals are performed to stage loco-regional disease. In the absence of distant metastases onCT scan, PET/CT scanning is performed.
2. PET/CT scanning is performed in all patients withclinically resectable disease to direct nodal sampling, aswell as to detect distant occult metastasis. In the absenceof distant metastasis, FDG-avid mediastinal nodes arebiopsied to confirm nodal mediastinal disease. Accord-ing to the American College of Chest PhysiciansGuidelines for invasive mediastinal staging of lungcancer, patients with central tumors require invasivesampling of mediastinal nodes, whereas patients withsmall peripheral tumors with PET-negative nodes do
not.70 Patients undergoing a localized surgical procedure(lobectomy or segmentectomy) with normal PETscanning of the mediastinum and normal-sized nodeson CT scanning may proceed to surgical resectionwithout preoperative mediastinoscopy. However, if thesurgical procedure is extensive (pneumonectomy) andcarries higher risk of complications, invasive staging
FIGURE 6. A 52-year-old man with dizziness and confusion. Chest radiograph (A) shows a right upper lobe mass and biopsy revealedsquamous cell carcinoma. PET/CT scanning (B) shows a focus of FDG uptake in the right iliac bone with SUV of 9.3. Contrast-enhancedT1-weighted MR imaging (C) shows an enhancing lesion in the right iliac bone consistent with metastatic disease (arrow). Notedetection of clinically occult bone metastasis precluded the patient from curative resection.
FIGURE 7. A 53-year-old man with a 3-month history of coughand shortness of breath. PET/CT scan shows markedly FDG-avidright upper lobe mass (SUV, 29.8) and right paratrachealadenopathy (SUV, 20.7). Lung biopsy revealed adenocarcinoma.
While on chemotherapy, patient developed hepatic metastasesand died 6 months later. Note high SUV of the primary tumor may be an indicator of poor prognosis.
J Thorac Imaging Volume 26, Number 2, May 2011 PET/CT in Evaluation of Lung Cancer
r 2011 Lippincott Williams & Wilkins www.thoracicimaging.com | 137

8/3/2019 Pet and Lung Cancer
http://slidepdf.com/reader/full/pet-and-lung-cancer 7/15
with endobronchial ultrasound, endoscopic ultrasound,or mediastinoscopy is performed regardless of the size of mediastinal nodes or the degree of nodal FDG uptake.
3. All extrathoracic FDG-avid lesions suspicious formetastases in patients being considered for surgicalresection should be biopsied to obtain a histopathologic
diagnosis if confirmation of metastatic disease alterspatient management. If biopsy is not feasible, the lesionshould be further evaluated with additional imagingstudies (CT and/or MR imaging).
4. Brain CT or MR imaging is performed in patients withsigns or symptoms of central nervous system disease, aswell as in asymptomatic patients with stage III diseasebeing considered for aggressive local therapy (surgery orchemoradiation therapy).
PROGNOSISMultiple studies have observed that patients with lung
cancers that are highly metabolic as measured by the degree
of FDG uptake tend to have a more aggressive clinicalcourse than those with a low metabolic rate.71–78 Thisfinding has been reported across the various stages of lungcancer, from early-stage disease amenable to curativeresection to advanced inoperable disease. A recent meta-analysis performed by the European Lung Cancer WorkingParty for the International Association for the Study of Lung Cancer Staging Project concluded that metabolicactivity of the primary tumor as determined by the SUV onPET imaging is a prognostic indicator in patients withNSCLC.79 Berghmans et al79 identified a high SUV as apoor prognostic factor for survival (Fig. 7) and recom-mended a formal analysis of SUV with respect to stage andperformance status to determine the prognostic value of
PET imaging.Several studies have evaluated the potential role of
PET scanning as a prognostic indicator using the degreeof increased FDG uptake in the primary tumor at diagnosisto predict survival.71,72,76–78,80–83 The threshold SUV usedfor univariate analysis in these studies ranged from 3.3 to20. A review of the results of these studies will be presentedorganized according to disease stage.
For stage I disease, FDG uptake of the primary tumorat diagnosis was found to be predictive of disease-freesurvival.71,72 In a retrospective study of 136 patients withstage I NSCLC treated with curative surgical resection byGoodgame et al,72 an SUV threshold of 5.5 was used toassess prognostic significance. Thirty-two of 136 patients
developed recurrence of malignancy after a mean post-resection interval of 46 months. Patients with a primarytumor with high SUV (>5.5) were approximately 3 timesmore likely to have relapse.72 The 5-year estimates of recurrence rates for patients with high and low SUV were37% and 14%, respectively (P=0.002), with 5-year overallsurvivals of 53% and 74%, respectively (P=0.006). Inmultivariate analyses based on SUV, T descriptor, age,and histology, there were significant correlations betweenhigh SUV and recurrence (P=0.002) and high SUV andmortality (P=0.041).72
Similar results were reported by Hanin et al71 in aretrospective study evaluating the prognostic value of FDGuptake (using an SUV threshold of 7.8) in 96 patients with
stage I and II tumors that were completely resected. Themedian survival of stage I patients with low-SUV tumorswas significantly longer than those with high-SUV tumors
(127mo vs. 69mo, P=0.001). Although there was nostatistical difference seen in patients with stage II tumors(72 mo vs. 40mo), there was a trend toward reducedsurvival for high-SUV (>7.8) tumors. Disease-free survivalfor all patients with low-SUV tumors was longer than thosewith high-SUV tumors (96.1 mo vs. 87.7 mo, P=0.01).
The researchers of these 2 studies hypothesized thatPET imaging may be of potential use in selecting patientsfor postoperative adjuvant chemotherapy.71,72 The use of adjuvant chemotherapy in patients with stage I NSCLC isnot currently supported by evidence from clinical trials.However, there may be a subset of patients with highlymetabolic tumors with high risk for relapse who may havea survival benefit from postoperative adjuvant chemo-therapy. In the study by Ohtsuka et al77 using an SUVthreshold of 3.3 to evaluate the prognostic value of FDGuptake in patients with pathologic stage I adenocarcinomaswho underwent curative resection, patients with high-SUVstage IA and IB disease had shorter disease-free intervals,suggesting that these patients could be candidates for
adjuvant chemotherapy. Furthermore, none of the patientswith low-SUV stage IB disease developed recurrence of malignancy, suggesting that these patients may not benefitfrom adjuvant therapy.
In contrast, in a retrospective study by Cerfolio et al84
of 315 patients with complete resection for NSCLC,patients in the same stage with high-SUV tumors weremore likely to have tumor recurrence (significant for stagesIB and II) and shorter survival (significant for stage IB, II,and IIIA disease), compared with those with low-SUVtumors. Patients with stage IB and stage II disease with anSUV of greater than the median for their respective stageshad a lower disease-free survival at 4 years. The differencesin disease-free survival between groups with low-SUV
tumors versus high-SUV tumors were significant in patientswith stage IB (92% vs. 51%) and stage II (64% vs. 47%)disease. Stratified by stage, the 4-year survival for patientswith low-SUV tumors versus high-SUV tumors was 80%versus 66% for stage IB, 64% versus 32% for stage II, and64% versus 16% for stage IIIA. Results show that SUVwas an independent predictor of the likelihood of nodalinvolvement and distant metastases, that is, patients with ahigh SUV (>10) were more likely to have advanced stage.In fact, SUV was found to be the best predictor of disease-free survival and overall survival.
In inoperable stage III patients, a phase II study wasperformed in 31 patients using PET before and after 3cycles of neoadjuvant chemotherapy followed by consoli-
dation RT.85 All the tumors had a marked increase in FDGuptake (median SUV, 11.3) at baseline. After 3 cycles of neoadjuvant chemotherapy, 10 patients with completemetabolic response defined as an SUV of <2.5 showedbenefit compared with the patients with a posttherapy SUVof >2.5 (19.9 mo vs. 9.8 mo for time to progression and49 mo vs. 14.4 mo for overall survival).85
In addition, in a prospective study of the prognosticvalue of PET scanning after the completion of definitiveradiotherapy (n=10) or chemoradiotherapy (n=63) inpatients of various stages (13 patients with stage I, 14patients with stage II, and 46 patients with stage III),MacManus et al86 reported a significant correlationbetween the decrease in FDG uptake within the primary
tumor and mediastinal lymph nodes, and patient outcome.Furthermore, the study is also in agreement with previousreports of the superior prognostic value of PET scanning
Truong et al J Thorac Imaging Volume 26, Number 2, May 2011
138 | www.thoracicimaging.com r 2011 Lippincott Williams & Wilkins

8/3/2019 Pet and Lung Cancer
http://slidepdf.com/reader/full/pet-and-lung-cancer 8/15
compared with CT scanning after therapy.86 In fact, asingle early posttreatment PET scan was found to be abetter predictor of survival than CT scanning response,stage, or pretreatment performance status.
In contrast, data from a retrospective study of 214patients with advanced-stage NSCLC (stages IIIA, IIIB,
and IV) using a median SUV threshold of 11.1 at the timeof diagnosis did not show a survival benefit for patientswith low-SUV tumors (median survival of 16mo vs.12 mo).87 Seventy-four percent of the 214 patients died,and 56 patients were alive at 27 months (range, 3 to 140 mo)after the diagnosis of NSCLC. A possible explanation isthat the short survival time and high mortality rate inpatients with advanced-stage NSCLC may account for thelack of correlation between survival and FDG uptake inthe primary tumor. In summary, although PET imagingshows promise as a prognostic indicator in patientswith lung cancer, particularly in early-stage disease, multi-institutional prospective randomized trials are necessary tofully elucidate the role of PET scanning in patient treatment
algorithms.
RADIATION THERAPY PLANNINGRadiation therapy plays a central role in the manage-
ment of NSCLC, either alone or in combination withsurgery and/or chemotherapy. In curative RT, the targetvolume of tissue irradiated with a high dose mustencompass the entire tumor and any microscopic extensionsof disease. However, the target volume should be kept assmall as possible to minimize damage to adjacent normaltissues. Advances in computer-assisted 3-dimensional plan-ning, such as 3-dimensional conformal radiotherapy,intensity-modulated RT, and image-guided RT, enable
delivery of higher radiation doses to the tumor and improvenormal tissue sparing. Thus, accurate target delineation isessential. The gross tumor volume indicates palpable orvisible disease, which may be the primary tumor, metastaticlymph nodes, or other metastases. The clinical targetvolume (CTV) is defined as the gross tumor volume withthe addition of sufficient margins to account for subclinicaldisease extension. The planning target volume derives fromthe CTV and is a geometrical parameter that is obtained byadding adequate margins around the CTV to account forset-up errors and organ motion. With image-guided RT,treatment plans can be adjusted as needed on the basis of information from imaging modalities including therapy-induced tumor changes. This is the basis for adaptive RT.88
Due to its remarkable accuracy in staging and thedemonstration of a powerful effect on treatment volumes,there is a strong case for the routine use of PET/CTscanning in RT planning for NSCLC.89
Inclusion of PET scanning in staging evaluation hasproven to be more accurate than conventional staging forNSCLCs, and when available, PET scanning should beused to select patients with NSCLC for treatment withdefinitive RT. PET scanning detects unsuspected distantmetastasis (>20% of pre-PET stage III) and identifiespatients with very advanced locoregional disease notsuitable for radical RT.90 Inclusion of PET scanning inthe staging workup improves the apparent survival of patients treated with RT or chemoradiation therapy by
excluding incurable patients.91 In a large prospective study,30% of patients who were candidates for high-dose RT onthe basis of conventional staging received only palliative
therapy after PET scanning, because of unexpected distantmetastasis (20%) or very extensive intrathoracic disease(10%).92 In a prospective study, knowledge of preradiother-apy PET data caused treatment to be canceled or modifiedfrom curative to palliative in 15 patients (11%).93 Of the119 patients in whom radical radiotherapy was confirmed,
the treatment plan was modified in 37 patients (31%).93PET/CT scanning should be used for RT planning in
NSCLC because it more accurately images tumor extent thanCT scanning alone.94 This has been proven by the extensivesurgical literature on the accuracy of PET scanning in thelymph node staging of NSCLC. Despite its higher accuracy,the limitations of PET scanning should be remembered. Therate of false-negative lymph node station assessment (posttestprobability) in NSCLC RT candidates is 5% to 10%.95 The 2most important and consistent reasons cited in the literature96
for significant changes in target volumes in NSCLC withPET scanning were:
1. FDG-PET scanning significantly changed lymph nodestaging in the thorax, usually by showing more positive
nodes than CT scanning.2. In cases with atelectasis, PET scanning helped to
delineate the border between the tumor and thecollapsed lung, allowing a smaller volume of the lungto be treated.97
THERAPEUTIC RESPONSENSCLC commonly presents at an advanced stage of
disease, and chemotherapy plays a vital role in thetreatment of these patients. With initiation of chemother-apy, progression of disease may occur in up to one thirdof patients.98 Early recognition of therapeutic failure isimportant in patient management because it can lead to
cessation of ineffective treatment and institution of analternative regimen. Anatomic imaging alone using stan-dard World Health Organization or Response EvaluationCriteria in Solid Tumors is widely applied, but haslimitations in response assessment, as size measurementsmay not correlate with pathologic response or tumorviability. Furthermore, with the development of treatmentalternatives targeting tumor biology, such as tumor cellproliferation and invasion, angiogenesis, and metastasis,the effect in many of these novel regimens is cytostatic, notcytotoxic, and may not lead to regression in tumor size.In contradistinction, metabolic imaging with PET scanningmay allow an early and sensitive indication of theeffectiveness of chemotherapy, as FDG uptake is not only
a function of proliferative activity, but is also related toviable tumor cell number.99–102
Multiple studies have examined the role of PETscanning in assessing treatment response in patients withlocally advanced (stages IIIA and IIIB) NSCLC who havecompleted neoadjuvant therapy and are being consideredfor curative surgical resection.103–109 Because metabolicresponse to therapy may occur earlier and may be moreaccurate than anatomic response, PET imaging has thepotential to improve the assessment of residual tumor andcould be useful in selecting patients for resection. Althoughnot used in the routine evaluation of tumor response inpatients with NSCLC after neoadjuvant treatment, smallstudies suggest a promising role for PET scanning.
In a study by Eschmann et al109 of 70 patientswith advanced NSCLC (stage III) who had neoadjuvantchemoradiotherapy, the difference between initial FDG
J Thorac Imaging Volume 26, Number 2, May 2011 PET/CT in Evaluation of Lung Cancer
r 2011 Lippincott Williams & Wilkins www.thoracicimaging.com | 139

8/3/2019 Pet and Lung Cancer
http://slidepdf.com/reader/full/pet-and-lung-cancer 9/15
uptake and uptake after induction chemotherapy waspredictive of long-term survival. Patients with normalFDG uptake or an 80% or more decrease in tumor SUV
after therapy had a significantly longer survival than thosebelow this threshold (Fig. 8). Of note, the few patients withPET findings of progressive disease who underwent surgicalresection had only slightly longer survival than patientswho did not undergo surgery.109
In a prospective trial of 93 patients with NSCLC andbiopsy-proven stage IIIA N2 disease, the patients werestaged with mediastinoscopy, integrated PET/CT scanning,and CT scanning. Repeat evaluation was performed 4 to12 weeks after neoadjuvant chemoradiation therapy.107
PET/CT scanning was superior to CT scanning in assessingthese patients after neoadjuvant chemoradiation therapy.Receiver Operating Characteristic curve analysis showedthat a decrease of 75% or more in the SUV of the primary
tumor indicated a high likelihood of a complete response,and a decrease by more than 50% in the SUV of the N2node indicated a high likelihood of no residual disease. Thestudy reported that the median decrease in SUV in patientswith N2 disease and complete response was 87%, comparedwith 52% in patients with residual N2 disease.107 However,if the N2 nodes had a persistently high SUV, pathologicconfirmation of metastatic disease was recommended, asincreased FDG uptake did not reliably indicate residualdisease. This strategy is supported by the results of a smallstudy by Ohtsuka et al,110 which used PET scanning toassess pathologic tumor response and lymph node stagingafter neoadjuvant therapy in patients with NSCLC, and inwhom the sensitivity (0.61), specificity (0.69), PPV (0.36),
NPV (0.86), and accuracy (0.67) for lymph node stagingwere suboptimal.
The interpretation of SUV measurements after neo-adjuvant therapy (especially when radiotherapy has beenadministered) is problematic because of confoundingfactors including tumor cell differentiation and macrophageinfiltration. Animal studies have shown that up to 30%of the FDG uptake in a tumor may be caused by themacrophage/monocyte system and that some tumors mayretain high SUV measurements at the end of therapy evenwith histopathologic complete remission at the time of resection.110–113 Accordingly, PET scanning should not bethe sole determinant of eligibility for surgical resection ordose-escalated radiotherapy after neoadjuvant treatment of
NSCLC. This recommendation is supported by the resultsof a study by Poettgen et al,111 which correlated PET/CTscanning and histopathology after neoadjuvant therapy in
NSCLC. Forty-six patients with stage IIIA and IIIB diseasewho received neoadjuvant therapy underwent surgicalresection. Of the 19 patients with complete pathologic
response of the primary tumor, 44% had a postinductionSUV of >2.5, suggesting residual viable tumor.
There have been relatively few studies assessing thevalue of early PET scanning in assessing tumor responsewhile patients are still receiving therapy.104,114 A decline intumor SUV after 1 cycle of chemotherapy may predictoutcome, with survival benefit directly related to themagnitude of the decline. In a recent prospective study of 57 patients with stage IIIB or IV unresectable NSCLC whounderwent restaging PET scanning after only 1 cycle of platinum-based chemotherapy, a decline in SUV of 20% orgreater in the primary tumor was an independent predictorof long-term survival.114 This metabolic response correlatedhighly with the best response to therapy according to the
Response Evaluation Criteria in Solid Tumors as deter-mined on serial CT scans and was associated with a higheroverall survival than in nonresponders (median survival of 252 d vs. 151 d). Furthermore, in a prospective study of 47 patients with locally advanced but potentially resectablestage IIIA N2 NSCLC who were receiving neoadjuvantchemotherapy, a reevaluation PET scan performed after 1cycle of induction chemotherapy showed that a decrease inFDG uptake of 35% or greater correlated with improvedsurvival (P=0.03).104 In this study, PET scanning wassuperior to CT scanning in monitoring response and alsoenabled an early prediction of survival during the initiationof therapy.
A problematic issue in implementing the wide use
of PET scanning in the assessment of early therapeuticresponse in patients with NSCLC is that there is noconsensus on the timing of performance of PET imaging orthe most appropriate criteria for assessment. Furthermore,for SUV measurements to be comparable and reproducible,standardization of scanning methods, including time toimaging after FDG administration, is required. To addressthe issue of reproducibility of data, the European Organi-zation for Research and Treatment of Cancer PET StudyGroup and the Cancer Imaging Program of the NationalCancer Institute have issued guidelines for the use of PETscanning in the assessment of prognosis and response totherapy in oncologic studies.100,115 The use of PET scanningto determine selection of appropriate therapy and as a
marker of therapeutic efficacy in patients with NSCLCrequires that the recommendations pertaining to thestandardization of patient preparation, image acquisition
FIGURE 8. A 74-year-old man with shoulder pain and left apical lesion. PET/CT scan (A) shows FDG-avid lesion in the left apex (SUV,10.8) and biopsy confirmed adenocarcinoma. PET/CT scanning (B) after 2 cycles of carboplatin and pemetrexed showed completemetabolic response. Note there is generally a significant association between marked decrease in FDG uptake within the tumor andpatient outcome.
Truong et al J Thorac Imaging Volume 26, Number 2, May 2011
140 | www.thoracicimaging.com r 2011 Lippincott Williams & Wilkins

8/3/2019 Pet and Lung Cancer
http://slidepdf.com/reader/full/pet-and-lung-cancer 10/15
and reconstruction, and PET timing relative to therapy beimplemented.115 In addition, an agreement on the optimalthreshold levels for the determination of response isrequired for PET scanning to be comparable and widelyapplicable clinically. In this regard, a new framework forPET Response Criteria in Solid Tumors has been proposed.
This framework recommends assessing normal referencetissue values in a 3-cm-diameter region of interest in theliver, using a consistent PET protocol and a fixed smallregion of interest, about 1 cm3 in volume (1.2 cm diameter),in the most active region of metabolically active tumors tominimize statistical variability, assessing tumor size, treat-ing SUV lean measurements in the 1 (up to 5 optional) mostmetabolically active tumor focus as a continuous variable,and requiring a 30% decline in SUV for response. Thisframework should serve as a starting point for use inclinical trials and in structured quantitative clinical report-ing. Undoubtedly, subsequent revisions and enhancementswill be required as validation studies are performed.116
RECURRENT LUNG CANCEREarly detection of local tumor recurrence is important
as patients can be treated with repeat surgery, salvagechemotherapy, or radiotherapy.117–120 Symptoms of localrecurrence of lung cancer may not manifest until later, andthis can lead to delays in diagnosis and can limit retreatmentoptions. Findings on CT scanning or MR imaging areunreliable in distinguishing tumor from necrosis, posttherapyscarring, or fibrosis.121 PET scanning can detect localrecurrence of tumor after definitive treatment with surgery,chemotherapy, or radiotherapy earlier than conventionalimaging and has been reported to have a sensitivity of 98% to100% and specificity of 62% to 92% (Fig. 9).122–125 In a
recent prospective study of 62 patients who had undergonesurgical resection of NSCLC, PET scanning was able todetect tumor recurrence (sensitivity 93%, specificity 89%,and accuracy 92%) and predict which patients would benefitmost from surgical retreatment.126 Similarly, Keidar et al127
used PET/CT scanning to evaluate 42 patients with NSCLCat least 6 months after initial therapy (surgery, n=25; surgeryand radiotherapy or chemotherapy, n=15; radiotherapy andchemotherapy, n=2) who had an uncertain diagnosis of recurrent disease or its extent after routine clinical and CTevaluation. Twenty-five patients had recurrence of NSCLC,and the sensitivity, specificity, PPV, and NPV of PET/CTscanning for diagnosis of recurrence were 96%, 82%,89%, and 93%, respectively. Hicks et al124 also evaluated
patients with suspected relapse of more than 6 months after
definitive curative treatment (surgery, n=18; surgery andchemoradiotherapy, n=12; radical radiotherapy with orwithout concurrent chemotherapy, n =33). Forty-two of the 63 patients had tumor relapse. PET scanning waspositive in 41 patients (sensitivity 98%), whereas CTscanning indicated recurrence in all 42 patients. Seventeen
of the 63 patients (27%) had no evidence of relapse, andPET scanning was negative in 14 of these patients(specificity 82%). In contradistinction, CT scanning in-dicated recurrence of malignancy in 15 of the 17 patients.Of note, PET scanning resulted in a significant change inthe management of 40 patients (63%), including a changefrom curative to palliative therapy in 6 patients and frompalliative to curative therapy in 3 patients.
The high sensitivity and specificity of PET scanningfor the detection of recurrent malignancy may be related tothe timing of imaging. In Hicks’ study,124 PET scanningwas performed more than 6 months after therapy, thuslimiting the confounding effect of increased FDG uptakedue to therapy-induced inflammation and/or macrophage
infiltration that may occur when PET scanning isperformed soon after completion of radiotherapy. In arecent study of 73 patients with NSCLC, it was reportedthat the ability of PET scanning performed a median of 70 days (range, 39 to 123 d in 90% of patients) after thecompletion of radical radiotherapy to assess therapeuticresponse was not confounded by radiation-induced inflam-mation.128 Furthermore, PET scanning not only improvesthe detection of recurrent disease, but also providesprognostic information useful in selecting patients forrepeat surgical resection. In a study by Hellwig et al,126
patients who had tumor recurrence with SUV of <11 had alonger median survival (46 mo) compared with thosepatients with a higher SUV (3 mo).
SMALL CELL LUNG CANCERIn contrast to the numerous studies evaluating
PET scanning in NSCLC, there are far fewer studies onits utility in small cell lung cancer (SCLC). SCLC accountsfor 15% to 20% of all lung cancers, and staging is basedon differentiating patients with limited disease from thosewith extensive disease. Limited disease is confined to thehemithorax of origin, including contralateral hilar andsupraclavicular nodes, which can be encompassed within atolerable RT portal, and patients are candidates for radicalconcurrent chemoradiotherapy (Fig. 10). Extensive diseasehas spread beyond the supraclavicular region or to distant
organs, and patients receive palliative chemotherapy alone.
FIGURE 9. A 51-year-old woman with a right upper lobe lung cancer treated with RT. Ten years later, contrast-enhanced CT scan (A)shows increased soft tissue within the area of radiation fibrosis (arrow). PET/CT scan (B) reveals intense focal FDG uptake with SUV of 10.4 suspicious for local recurrence of malignancy (arrow) and was useful in directing needle biopsy.
J Thorac Imaging Volume 26, Number 2, May 2011 PET/CT in Evaluation of Lung Cancer
r 2011 Lippincott Williams & Wilkins www.thoracicimaging.com | 141

8/3/2019 Pet and Lung Cancer
http://slidepdf.com/reader/full/pet-and-lung-cancer 11/15
Patients with malignant pleural effusions have an inter-mediate prognosis between limited and extensive disease.In a prospective study of 24 patients with SCLC consideredto have limited disease based on conventional workup,PET scanning correctly upstaged 8.3% of patients withsensitivity of 100% and specificity of 95.5% for detectingmetastatic disease.129 Furthermore, PET scanning can leadto a change in the radiation treatment plan in 25% of patients by detecting unsuspected locoregional nodaldisease.129 Brink et al130 reported that PET scanning causeda stage migration in 14 of 120 patients (including upstaging10 patients to extensive disease and downstaging 3 patientsby not confirming metastases of the adrenals suspected onCT scanning). PET scanning was superior to CT scanning
in the detection of extrathoracic nodal disease, with asensitivity of 100% versus 70% and a specificity of 98%versus 94%, respectively. Furthermore, PET scanning
showed superiority compared with CT scanning in thedetection of distant metastases (excluding the brain), with asensitivity of 98% versus 83% and a specificity of 92%versus 79%, respectively.
CONCLUSIONIntegrated PET/CT scanning complements conventional
imaging assessment in the staging of patients with lung cancerby improving the detection of nodal and extrathoracicmetastases. PET/CT scanning is also used for RT planningin NSCLC because it more accurately images tumor extentthan CT scanning alone. PET/CT scanning is currently beingstudied in the evaluation of prognosis and therapeutic
response and has the potential to provide more appropriateselection of patients for surgical resection and neoadjuvantand adjuvant therapy. Furthermore, this imaging modality
FIGURE 10. A 68-year-old man with a 6-month history of shortness of breath. PET/CT scanning shows FDG-avid mediastinaladenopathy in the aortopulmonary window (APW) and contralateral paratracheal region. Biopsy of the APW mediastinal lymph nodesrevealed small cell carcinoma. Note PET scanning is useful in assessing extent of disease; patients with limited disease (confined to 1hemithorax and contralateral mediastinal nodes) are treated with definitive chemoradiation therapy.
Truong et al J Thorac Imaging Volume 26, Number 2, May 2011
142 | www.thoracicimaging.com r 2011 Lippincott Williams & Wilkins

8/3/2019 Pet and Lung Cancer
http://slidepdf.com/reader/full/pet-and-lung-cancer 12/15
may impact patient management by allowing an earlierassessment of tumor response to chemotherapeutic regimens.Multi-institutional, prospective randomized controlled trialsand standardization of PET imaging protocols to accuratelymeasure the degree of FDG uptake are needed to fullyelucidate the clinical applications of PET scanning in the
management of patients with lung cancer.
REFERENCES
1. Adams MC TT, Wilson JM, Wong TZ. A systematic reviewof factors affecting accuracy of SUV measurements. Am J Roentgenol. 2010;195:310–320.
2. Lowe VJ, Hoffman JM, DeLong DM, et al. Semiquantitativeand visual analysis of FDG-PET images in pulmonaryabnormalities. J Nucl Med. 1994;35:1771–1776.
3. Costa DC, Visvikis D, Crosdale I, et al. Positron emission andcomputed X-ray tomography: a coming together. Nucl Med Commun. 2003;24:351–358.
4. Cook GJ, Wegner EA, Fogelman I. Pitfalls and artifacts in18FDG PET and PET/CT oncologic imaging. Semin Nucl
Med. 2004;34:122–133.5. De Wever W, Stroobants S, Coolen J, et al. Integrated
PET/CT in the staging of nonsmall cell lung cancer: technicalaspects and clinical integration. Eur Respir J. 2009;33:201–212.
6. Beyer T, Antoch G, Blodgett T, et al. Dual-modality PET/CTimaging: the effect of respiratory motion on combined imagequality in clinical oncology. Eur J Nucl Med Mol Imaging.2003;30:588–596.
7. Osman MM, Cohade C, Nakamoto Y, et al. Respiratorymotion artifacts on PET emission images obtained using CTattenuation correction on PET-CT. Eur J Nucl Med Mol Imaging. 2003;30:603–606.
8. Goerres GW, Burger C, Kamel E, et al. Respiration-inducedattenuation artifact at PET/CT: technical considerations.Radiology. 2003;226:906–910.
9. Pan T, Mawlawi O, Nehmeh SA, et al. Attenuation correctionof PET images with respiration-averaged CT images in PET/CT. J Nucl Med. 2005;46:1481–1487.
10. Truong MT, Pan T, Erasmus JJ. Pitfalls in integratedCT-PET of the thorax: implications in oncologic imaging.J Thorac Imaging. 2006;21:111–122.
11. Gould MK, Maclean CC, Kuschner WG, et al. Accuracy of positron emission tomography for diagnosis of pulmonarynodules and mass lesions: a meta-analysis. JAMA. 2001;285:914–924.
12. Rohren EM, Lowe VJ. Update in PET imaging of nonsmallcell lung cancer. Semin Nucl Med. 2004;34:134–153.
13. Yi CA, Lee KS, Kim BT, et al. Tissue characterization of solitary pulmonary nodule: comparative study between helicaldynamic CT and integrated PET/CT. J Nucl Med. 2006;47:
443–450.14. Bryant AS, Cerfolio RJ. The maximum standardized uptake
values on integrated FDG-PET/CT is useful in differentiatingbenign from malignant pulmonary nodules. Ann Thorac Surg.2006;82:1016–1020.
15. Nomori H, Watanabe K, Ohtsuka T, et al. Evaluation of F-18fluorodeoxyglucose (FDG) PET scanning for pulmonarynodules less than 3 cm in diameter, with special reference tothe CT images. Lung Cancer. 2004;45:19–27.
16. Lowe VJ, Fletcher JW, Gobar L, et al. Prospective investiga-tion of PET in lung nodules (PIOPILN). J Clin Oncol.1998;16:1075–1084.
17. Herder GJ, Golding RP, Hoekstra OS, et al. The performanceof (18)F-fluorodeoxyglucose positron emission tomographyin small solitary pulmonary nodules. Eur J Nucl Med Mol Imaging. 2004;31:1231–1236.
18. Erasmus JJ, McAdams HP, Patz JEF, et al. Evaluation of primary pulmonary carcinoid tumors using FDG PET. Am J Roentgenol. 1998;170:1369–1373.
19. Higashi K, Ueda Y, Seki H, et al. Fluorine-18-FDG PETimaging is negative in bronchioloalveolar lung carcinoma.J Nucl Med. 1998;39:1016–1020.
20. Sabloff BS, Truong MT, Wistuba II, et al. Bronchioalveolarcell carcinoma: radiologic appearance and dilemmas in theassessment of response. Clin Lung Cancer. 2004;6:108–112.
21. Cheran SK, Nielsen ND, Patz EF Jr. False-negative findings
for primary lung tumors on FDG positron emissiontomography: staging and prognostic implications. Am J Roentgenol. 2004;182:1129–1132.
22. Asad S, Aquino SL, Piyavisetpat N, et al. False-positive FDGpositron emission tomography uptake in nonmalignant chestabnormalities. Am J Roentgenol. 2004;182:983–989.
23. Tan BB, Flaherty KR, Kazerooni EA, et al. The solitarypulmonary nodule. Chest. 2003;123:89S–96S.
24. Gould MK, Ananth L, Barnett PG. A clinical model toestimate the pretest probability of lung cancer in patients withsolitary pulmonary nodules. Chest. 2007;131:383–388.
25. Gould MK, Sanders GD, Barnett PG, et al. Cost-effectivenessof alternative management strategies for patients with solitarypulmonary nodules. Ann Intern Med. 2003;138:724–735.
26. Pfister DG, Johnson DH, Azzoli CG, et al. American Society
of Clinical Oncology treatment of unresectable non-small-celllung cancer guideline: update 2003. J Clin Oncol. 2004;22:330–353.
27. Verboom P, Van Tinteren H, Hoekstra OS, et al. Cost-effectiveness of FDG-PET in staging non-small cell lungcancer: the PLUS study. Eur J Nucl Med Mol Imaging.2003;30:1444–1449.
28. Lardinois D, Weder W, Hany TF, et al. Staging of non-small-cell lung cancer with integrated positron-emission tomo-graphy and computed tomography. N Engl J Med. 2003;348:2500–2507.
29. Verhagen AF, Bootsma GP, Tjan-Heijnen VC, et al. FDG-PET in staging lung cancer: how does it change the algorithm?Lung Cancer. 2004;44:175–181.
30. Reed CE, Harpole DH, Posther KE, et al. Results of theAmerican College of Surgeons Oncology Group Z0050 trial:
the utility of positron emission tomography in stagingpotentially operable non-small cell lung cancer. J ThoracCardiovasc Surg. 2003;126:1943–1951.
31. Vansteenkiste JF, Stroobants SG, De Leyn PR, et al. Lymphnode staging in non-small-cell lung cancer with FDG-PETscan: a prospective study on 690 lymph node stations from 68patients. J Clin Oncol. 1998;16:2142–2149.
32. Pieterman RM, van Putten JW, Meuzelaar JJ, et al. Preopera-tive staging of non-small-cell lung cancer with positron-emissiontomography. N Engl J Med. 2000;343:254–261.
33. Antoch G, Stattaus J, Nemat AT, et al. Non-small cell lungcancer: dual-modality PET/CT in preoperative staging.Radiology. 2003;229:526–533.
34. van Baardwijk A, Baumert BG, Bosmans G, et al. Thecurrent status of FDG-PET in tumour volume definition in
radiotherapy treatment planning. Cancer Treat Rev. 2006;32:245–260.
35. Mountain CF, Dresler CM. Regional lymph node classifica-tion for lung cancer staging. Chest. 1997;111:1718–1723.
36. Prenzel KL, Monig SP, Sinning JM, et al. Lymph node sizeand metastatic infiltration in non-small cell lung cancer.Chest. 2003;123:463–467.
37. De Leyn P, Vansteenkiste J, Cuypers P, et al. Role of cervicalmediastinoscopy in staging of non-small cell lung cancerwithout enlarged mediastinal lymph nodes on CT scan. Eur J Cardiothorac Surg. 1997;12:706–712.
38. Choi YS, Shim YM, Kim J, et al. Mediastinoscopy in patientswith clinical stage I non-small cell lung cancer. Ann ThoracSurg. 2003;75:364–366.
39. Toloza EM, Harpole L, Detterbeck F, et al. Invasive stagingof non-small cell lung cancer: a review of the current evidence.
Chest. 2003;123:157S–166S.40. Jeon TY, Lee KS, Yi CA, et al. Incremental value of PET/CT
Over CT for mediastinal nodal staging of non-small cell lung
J Thorac Imaging Volume 26, Number 2, May 2011 PET/CT in Evaluation of Lung Cancer
r 2011 Lippincott Williams & Wilkins www.thoracicimaging.com | 143

8/3/2019 Pet and Lung Cancer
http://slidepdf.com/reader/full/pet-and-lung-cancer 13/15
cancer: comparison between patients with and without idiopathicpulmonary fibrosis. Am J Roentgenol. 2010;195:370–376.
41. Birim O, Kappetein AP, Stijnen T, et al. Meta-analysis of positron emission tomographic and computed tomographicimaging in detecting mediastinal lymph node metastases innonsmall cell lung cancer. Ann Thorac Surg. 2005;79:375–382.
42. Gould MK, Kuschner WG, Rydzak CE, et al. Test
performance of positron emission tomography and computedtomography for mediastinal staging in patients with non-small-cell lung cancer: a meta-analysis. Ann Intern Med. 2003;139:879–892.
43. Yasufuku K, Nakajima T, Motoori K, et al. Comparison of endobronchial ultrasound, positron emission tomography,and CT for lymph node staging of lung cancer. Chest.2006;130:710–718.
44. de Langen AJ, Raijmakers P, Riphagen I, et al. The size of mediastinal lymph nodes and its relation with metastaticinvolvement: a meta-analysis. Eur J Cardiothorac Surg. 2006;29:26–29.
45. Dietlein M, Weber K, Gandjour A, et al. Cost-effectivenessof FDG-PET for the management of potentially operablenon-small cell lung cancer: priority for a PET-based strategy
after nodal-negative CT results. Eur J Nucl Med. 2000;27:1598–1609.
46. Scott WJ, Shepherd J, Gambhir SS. Cost-effectiveness of FDG-PET for staging non-small cell lung cancer: a decisionanalysis. Ann Thorac Surg. 1998;66:1876–1885.
47. Quint LE, Tummala S, Brisson LJ, et al. Distribution of distant metastases from newly diagnosed non-small cell lungcancer. Ann Thorac Surg. 1996;62:246–250.
48. van Tinteren H, Hoekstra OS, Smit EF, et al. Effectiveness of positron emission tomography in the preoperative assessmentof patients with suspected non-small-cell lung cancer: the PLUSmulticentre randomised trial. Lancet. 2002;359:1388–1393.
49. MacManus MP, Hicks RJ, Matthews JP, et al. High rate of detection of unsuspected distant metastases by PET inapparent stage III non-small-cell lung cancer: implicationsfor radical radiation therapy. Int J Radiat Oncol Biol Phys.
2001;50:287–293.50. Schrevens L, Lorent N, Dooms C, et al. The role of PET scan
in diagnosis, staging, and management of non-small cell lungcancer. Oncologist. 2004;9:633–643.
51. Viney RC, Boyer MJ, King MT, et al. Randomized controlledtrial of the role of positron emission tomography in themanagement of stage I and II non-small-cell lung cancer.J Clin Oncol. 2004;22:2357–2362.
52. Lardinois D, Weder W, Roudas M, et al. Etiology of solitaryextrapulmonary positron emission tomography and com-puted tomography findings in patients with lung cancer.J Clin Oncol. 2005;23:6846–6853.
53. Oliver TW Jr, Bernardino ME, Miller JI, et al. Isolatedadrenal masses in nonsmall-cell bronchogenic carcinoma.Radiology. 1984;153:217–218.
54. Remer EM, Obuchowski N, Ellis JD, et al. Adrenal massevaluation in patients with lung carcinoma: a cost-effective-ness analysis. Am J Roentgenol. 2000;174:1033–1039.
55. Yun M, Kim W, Alnafisi N, et al. 18F-FDG PET incharacterizing adrenal lesions detected on CT or MRI.J Nucl Med. 2001;42:1795–1799.
56. Erasmus JJ, Patz EF, McAdams HP, et al. Evaluation of adrenal masses in patients with bronchogenic carcinoma byusing 18F-fluorodeoxyglucose positron emission tomography.Am J Roentgenol. 1997;168:1357–1360.
57. Blake MA, Slattery JM, Kalra MK, et al. Adrenal lesions:characterization with fused PET/CT image in patients withproved or suspected malignancy—initial experience. Radio-logy. 2006;238:970–977.
58. Metser U, Miller E, Lerman H, et al. 18F-FDG PET/CT inthe evaluation of adrenal masses. J Nucl Med. 2006;47:32–37.
59. Yokoi K, Kamiya N, Matsuguma H, et al. Detection of brainmetastasis in potentially operable non-small cell lung cancer:a comparison of CT and MRI. Chest. 1999;115:714–719.
60. Toloza EM, Harpole L, McCrory DC. Noninvasive staging of non-small cell lung cancer: a review of the current evidence.Chest. 2003;123:137S–146S.
61. Silvestri GA, Tanoue LT, Margolis ML, et al. The noninvasivestaging of non-small cell lung cancer: the guidelines. Chest.2003;123:147S–156S.
62. Salvatierra A, Baamonde C, Llamas JM, et al. Extrathoracic
staging of bronchogenic carcinoma. Chest. 1990;97:1052–1058.63. Michel F, Soler M, Imhof E, et al. Initial staging of non-small
cell lung cancer: value of routine radioisotope bone scanning.Thorax. 1991;46:469–473.
64. Silvestri GA, Littenberg B, Colice GL. The clinical evaluationfor detecting metastatic lung cancer: a meta-analysis. Am J Respir Crit Care Med. 1995;152:225–230.
65. Taira AV, Herfkens RJ, Gambhir SS, et al. Detection of bonemetastases: assessment of integrated FDG PET/CT imaging.Radiology. 2007;243:204–211.
66. Dwamena BA, Sonnad SS, Angobaldo JO, et al. Metastasesfrom non-small cell lung cancer: mediastinal staging in the1990’s: meta-analytic comparison of PET and CT. Radiology.1999;213:530–536.
67. Erasmus JJ, McAdams HP, Rossi SE, et al. FDG PET of
pleural effusions in patients with non-small cell lung cancer.Am J Roentgenol. 2000;175:245–249.
68. Schaffler GJ, Wolf G, Schoellnast H, et al. Non-small celllung cancer: evaluation of pleural abnormalities on CT scanswith 18F FDG PET. Radiology. 2004;231:858–865.
69. Prakash P, Kalra MK, Sharma A, et al. FDG PET/CT inassessment of pulmonary lymphangitic carcinomatosis. Am J Roentgenol. 2009;194:231–236.
70. Detterbeck FC, Jantz MA, Wallace M, et al. Invasivemediastinal staging of lung cancer: ACCP evidence-based clinicalpractice guidelines (2nd edition). Chest. 2007;132:202S–220S.
71. Hanin FX, Lonneux M, Cornet J, et al. Prognostic value of FDG uptake in early stage non-small cell lung cancer. Eur J Cardiothorac Surg. 2008;33:819–823.
72. Goodgame B, Pillot GA, Yang Z, et al. Prognostic value of preoperative positron emission tomography in resected stage I
non-small cell lung cancer. J Thorac Oncol. 2008;3:130–134.73. Davies A, Tan C, Paschalides C, et al. FDG-PET maximum
standardised uptake value is associated with variation insurvival: analysis of 498 lung cancer patients. Lung Cancer.2007;55:75–78.
74. Downey RJ, Akhurst T, Gonen M, et al. Preoperative F-18fluorodeoxyglucose-positron emission tomography maximalstandardized uptake value predicts survival after lung cancerresection. J Clin Oncol. 2004;22:3255–3260.
75. Borst GR, Belderbos JS, Boellaard R, et al. StandardisedFDG uptake: a prognostic factor for inoperable non-smallcell lung cancer. Eur J Cancer. 2005;41:1533–1541.
76. Higashi K, Ueda Y, Arisaka Y, et al. 18F-FDG uptake as abiologic prognostic factor for recurrence in patients withsurgically resected non-small cell lung cancer. J Nucl Med.
2002;43:39–45.77. Ohtsuka T, Nomori H, Watanabe K, et al. Prognostic
significance of [(18)F] fluorodeoxyglucose uptake on positronemission tomography in patients with pathologic stage I lungadenocarcinoma. Cancer. 2006;107:2468–2473.
78. Patz EF Jr, Connolly J, Herndon J. Prognostic value of thoracic FDG PET imaging after treatment for non-small celllung cancer. Am J Roentgenol. 2000;174:769–774.
79. Berghmans T, Dusart M, Paesmans M, et al. Primary tumorstandardized uptake value (SUVmax) measured on fluoro-deoxyglucose positron emission tomography (FDG-PET) isof prognostic value for survival in non-small cell lung cancer(NSCLC): a systematic review and meta-analysis (MA) by theEuropean Lung Cancer Working Party for the IASLC LungCancer Staging Project. J Thorac Oncol. 2008;3:6–12.
80. Ahuja V, Coleman RE, Herndon J, et al. The prognostic
significance of fluorodeoxyglucose positron emission tomo-graphy imaging for patients with nonsmall cell lung carcinoma.Cancer. 1998;83:918–924.
Truong et al J Thorac Imaging Volume 26, Number 2, May 2011
144 | www.thoracicimaging.com r 2011 Lippincott Williams & Wilkins

8/3/2019 Pet and Lung Cancer
http://slidepdf.com/reader/full/pet-and-lung-cancer 14/15
81. Vansteenkiste JF, Stroobants SG, Dupont PJ, et al.Prognostic importane of the standardized uptake value on(18)F-fluoro-2-deoxy-gluxose-positron emission tomographyscan in non-small-cell lung cancer. An analysis of 125 cases.Leuven Lung Cancer Group. J Clin Oncol. 1999;17:3201–3206.
82. Dhital K, Saunders CA, Seed PT, et al. [(18)F]Fluorodeoxy-
glucose positron emission tomography and its prognostic valuein lung cancer. Eur J Cardiothorac Surg. 2000;18:425–428.
83. Jeong HJ, Min JJ, Park JM, et al. Determination of theprognostic value of [(18)F] fluorodeoxyglucose uptake byusing positron emission tomography in patients with non-small cell lung cancer. Nucl Med Commun. 2002;23:865–870.
84. Cerfolio RJ, Bryant AS, Ohja B, et al. The maximumstandardized uptake values on positron emission tomographyof a non-small cell lung cancer predict stage, recurrence, andsurvival. J Thorac Cardiovasc Surg. 2005;130:151–159.
85. Decoster L, Schallier D, Everaert H, et al. Completemetabolic tumour response, assessed by 18-fluorodeoxyglu-cose positron emission tomography [(18)FDG-PET], afterinduction chemotherapy predicts a favourable outcome inpatients with locally advanced non-small cell lung cancer
(NSCLC). Lung Cancer. 2008;62:55–61.86. MacManus MP, Hicks RJ, Matthews JP, et al. Positron
emission tomography is superior to computed tomographyscanning for response-assessment after radical radiotherapyor chemoradiotherapy in patients with non-small-cell lungcancer. J Clin Oncol. 2003;21:1285–1292.
87. Hoang JK, Hoagland LF, Coleman RE, et al. Prognosticvalue of fluorine-18 fluorodeoxyglucose positron emis-sion tomography imaging in patients with advanced-stagenon-small-cell lung carcinoma. J Clin Oncol. 2008;26:1459–1464.
88. Aristei C FL, Palumbo B, Tarducci R. PET and PET-CT inradiation treatment planning for lung cancer. Expert RevAnticancer Ther. 2010;10:571–584.
89. MacManus M, Nestle U, Rosenzweig KE, et al. Use of PETand PET/CT for radiation therapy planning: IAEA expert
report 2006-2007. Radiother Oncol. 2009;91:85–94.90. Vansteenkiste J, Fischer BM, Dooms C, et al. Positron-
emission tomography in prognostic and therapeutic assess-ment of lung cancer: systematic review. Lancet Oncol. 2004;5:531–540.
91. Mac Manus MP, Wong K, Hicks RJ, et al. Early mortalityafter radical radiotherapy for non-small-cell lung cancer:comparison of PET-staged and conventionally staged cohortstreated at a large tertiary referral center. Int J Radiat Oncol Biol Phys. 2002;52:351–361.
92. Mac Manus MP, Hicks RJ, Ball DL, et al. F-18 fluorodeoxy-glucose positron emission tomography staging in radicalradiotherapy candidates with nonsmall cell lung carcinoma:powerful correlation with survival and high impact ontreatment. Cancer. 2001;92:886–895.
93. Pommier P, Touboul E, Chabaud S, et al. Impact of (18)F-FDG PET on treatment strategy and 3D radiotherapyplanning in non-small cell lung cancer: a prospective multi-center study. Am J Roentgenol. 2010;195:350–355.
94. Bradley J, Thorstad WL, Mutic S, et al. Impact of FDG-PETon radiation therapy volume delineation in non-small-celllung cancer. Int J Radiat Oncol Biol Phys. 2004;59:78–86.
95. Graeter TP, Hellwig D, Hoffmann K, et al. Mediastinallymph node staging in suspected lung cancer: comparison of positron emission tomography with F-18-fluorodeoxyglucoseand mediastinoscopy. Ann Thorac Surg. 2003;75:231–235;discussion 235–236.
96. Mac Manus MP, Hicks RJ. Impact of PET on radiationtherapy planning in lung cancer. Radiol Clin North Am. 2007;45:627–638, v.
97. Nestle U, Walter K, Schmidt S, et al. 18F-deoxyglucose
positron emission tomography (FDG-PET) for the planning of radiotherapy in lung cancer: high impact in patients withatelectasis. Int J Radiat Oncol Biol Phys. 1999;44:593–597.
98. Sekine I, Tamura T, Kunitoh H, et al. Progressive disease rateas a surrogate endpoint of phase II trials for non-small-celllung cancer. Ann Oncol. 1999;10:731–733.
99. Duhaylongsod FG, Lowe VJ, Patz EF Jr, et al. Lungtumor growth correlates with glucose metabolism measuredby fluoride-18 fluorodeoxyglucose positron emission tomo-graphy. Ann Thorac Surg. 1995;60:1348–1352.
100. Young H, Baum R, Cremerius U, et al. Measurement of clinical and subclinical tumour response using [18F]-fluoro-deoxyglucose and positron emission tomography: review and1999 EORTC recommendations. European Organization forResearch and Treatment of Cancer (EORTC) PET StudyGroup. Eur J Cancer. 1999;35:1773–1782.
101. Higashi K, Clavo AC, Wahl RL. Does FDG uptake measureproliferative activity of human cancer cells? In vitrocomparison with DNA flow cytometry and tritiated thymi-dine uptake. J Nucl Med. 1993;34:414–419.
102. Watanabe K, Nomori H, Ohtsuka T, et al. [F-18] Fluoro-deoxyglucose positron emission tomography can predictpathological tumor stage and proliferative activity determinedby Ki-67 in clinical stage IA lung adenocarcinomas. Jpn J ClinOncol. 2006;36:403–409.
103. Vansteenkiste JF, Stroobants SG, De Leyn PR, et al.Potential use of FDG-PET scan after induction chemother-apy in surgically staged IIIa-N2 non-small-cell lung cancer: aprospective pilot study. The Leuven Lung Cancer Group. AnnOncol. 1998;9:1193–1198.
104. Hoekstra CJ, Stroobants SG, Smit EF, et al. Prognosticrelevance of response evaluation using [18F]-2-fluoro-2-deoxy-D-glucose positron emission tomography in patientswith locally advanced non-small-cell lung cancer. J ClinOncol. 2005;23:8362–8370.
105. De Leyn P, Stroobants S, De Wever W, et al. Prospectivecomparative study of integrated positron emission tomogra-phy-computed tomography scan compared with remediasti-noscopy in the assessment of residual mediastinal lymph nodedisease after induction chemotherapy for mediastinoscopy-proven stage IIIA-N2 Non-small-cell lung cancer: a Leuven
Lung Cancer Group Study. J Clin Oncol. 2006;24:3333–3339.106. Eschmann SM, Friedel G, Paulsen F, et al. Repeat 18F-FDG
PET for monitoring neoadjuvant chemotherapy in patientswith stage III non-small cell lung cancer. Lung Cancer.2007;55:165–171.
107. Cerfolio RJ, Bryant AS, Ojha B. Restaging patients with N2(stage IIIa) non-small cell lung cancer after neoadjuvantchemoradiotherapy: a prospective study. J Thorac CardiovascSurg. 2006;131:1229–1235.
108. Pottgen C, Levegrun S, Theegarten D, et al. Value of 18F-fluoro-2-deoxy-D-glucose-positron emission tomography/computed tomography in non-small-cell lung cancer forprediction of pathologic response and times to relapse afterneoadjuvant chemoradiotherapy. Clin Cancer Res. 2006;12:97–106.
109. Eschmann SM, Friedel G, Paulsen F, et al. 18F-FDG PET forassessment of therapy response and preoperative re-evalua-tion after neoadjuvant radio-chemotherapy in stage III non-small cell lung cancer. Eur J Nucl Med Mol Imaging. 2007;34:463–471.
110. Ohtsuka T, Nomori H, Ebihara A, et al. FDG-PET imagingfor lymph node staging and pathologic tumor response afterneoadjuvant treatment of non-small cell lung cancer. AnnThorac Cardiovasc Surg. 2006;12:89–94.
111. Poettgen C, Theegarten D, Eberhardt W, et al. Correlation of PET/CT findings and histopathology after neoadjuvant therapyin non-small cell lung cancer. Oncology. 2007;73:316–323.
112. Kubota R, Yamada S, Kubota K, et al. Intratumoraldistribution of fluorine-18-fluorodeoxyglucose in vivo: highaccumulation in macrophages and granulation tissues studiedby microautoradiography. J Nucl Med. 1992;33:1972–1980.
113. Deichen JT, Prante O, Gack M, et al. Uptake of [18F]fluoro-deoxyglucose in human monocyte-macrophages in vitro. EurJ Nucl Med Mol Imaging. 2003;30:267–273.
J Thorac Imaging Volume 26, Number 2, May 2011 PET/CT in Evaluation of Lung Cancer
r 2011 Lippincott Williams & Wilkins www.thoracicimaging.com | 145

8/3/2019 Pet and Lung Cancer
http://slidepdf.com/reader/full/pet-and-lung-cancer 15/15
114. Weber WA, Petersen V, Schmidt B, et al. Positron emissiontomography in non-small-cell lung cancer: prediction of response to chemotherapy by quantitative assessment of glucose use. J Clin Oncol. 2003;21:2651–2657.
115. Shankar LK, Hoffman JM, Bacharach S, et al. Consensusrecommendations for the use of 18F-FDG PET as anindicator of therapeutic response in patients in National
Cancer Institute Trials. J Nucl Med. 2006;47:1059–1066.116. Wahl RL, Jacene H, Kasamon Y, et al. From RECIST to
PERCIST: evolving considerations for PET response criteriain solid tumors. J Nucl Med. 2009;50(suppl 1):122S–150S.
117. Campione A, Ligabue T, Luzzi L, et al. Late outcome andperioperative complications for surgery of locally recurrentbronchogenic carcinoma. J Cardiovasc Surg (Torino). 2005;46:515–518.
118. Watanabe Y, Shimizu J, Oda M, et al. Second surgicalintervention for recurrent and second primary bronchogeniccarcinomas. Scand J Thorac Cardiovasc Surg. 1992;26:73–78.
119. Milton DT, Miller VA. Advances in cytotoxic chemotherapyfor the treatment of metastatic or recurrent non-small celllung cancer. Semin Oncol. 2005;32:299–314.
120. Curran WJ Jr, Herbert SH, Stafford PM, et al. Should
patients with post-resection locoregional recurrence of lungcancer receive aggressive therapy? Int J Radiat Oncol Biol Phys. 1992;24:25–30.
121. Frank A, Lefkowitz D, Jaeger S, et al. Decision logic forretreatment of asymptomatic lung cancer recurrence based onpositron emission tomography findings. Int J Radiat Oncol Biol Phys. 1995;32:1495–1512.
122. Ryu JS, Choi NC, Fischman AJ, et al. FDG-PET in stagingand restaging non-small cell lung cancer after neoadjuvant
chemoradiotherapy: correlation with histopathology. LungCancer. 2002;35:179–187.
123. Inoue T, Kim E, Komaki R, et al. Detecting recurrent orresidual lung cancer with FDG-PET. J Nucl Med. 1995;36:788–793.
124. Hicks RJ, Kalff V, MacManus MP, et al. The utility of (18)F-FDG PET for suspected recurrent non-small cell lung cancer
after potentially curative therapy: impact on management andprognostic stratification. J Nucl Med. 2001;42:1605–1613.
125. Bury T, Corhay JL, Duysinx B, et al. Value of FDG-PET indetecting residual or recurrent nonsmall cell lung cancer. EurRespir J. 1999;14:1376–1380.
126. Hellwig D, Groschel A, Graeter TP, et al. Diagnosticperformance and prognostic impact of FDG-PET in sus-pected recurrence of surgically treated non-small cell lungcancer. Eur J Nucl Med Mol Imaging. 2006;33:13–21.
127. Keidar Z, Haim N, Guralnik L, et al. PET/CT using 18F-FDG in suspected lung cancer recurrence: diagnostic valueand impact on patient management. J Nucl Med. 2004;45:1640–1646.
128. Hicks RJ, Mac Manus MP, Matthews JP, et al. Early FDG-PET imaging after radical radiotherapy for non-small-cell lung
cancer: inflammatory changes in normal tissues correlate withtumor response and do not confound therapeutic responseevaluation. Int J Radiat Oncol Biol Phys. 2004;60:412–418.
129. Bradley JD, Dehdashti F, Mintun MA, et al. Positronemission tomography in limited-stage small-cell lung cancer:a prospective study. J Clin Oncol. 2004;22:3248–3254.
130. Brink I, Schumacher T, Mix M, et al. Impact of [18F]FDG-PET on the primary staging of small-cell lung cancer. Eur J Nucl Med Mol Imaging. 2004;31:1614–1620.
Truong et al J Thorac Imaging Volume 26, Number 2, May 2011
146 | th i i i r 2011 Li i tt Willi & Wilki